")
Back to Journals » International Journal of General Medicine » Volume 14
The Long-Term Survival of Intracranial Hemorrhage Patients Successfully Weaned from Prolonged Mechanical Ventilation
Received 3 February 2021
Accepted for publication 12 March 2021
Published 6 April 2021 Volume 2021:14 Pages 1197—1203
DOI https://doi.org/10.2147/IJGM.S304228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Chienhsiu Huang,1 Jin-cherng Chen2,3
1Department of Internal Medicine, Division of Chest Medicine, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan; 2Department of Surgery, Division of Neurosurgery, Dalin Tzu Chi Hospital, Chiayi, Taiwan; 3School of Medicine, Tzuchi University, Hualien, Taiwan
Correspondence: Chienhsiu Huang
Department of Internal Medicine, Division of Chest Medicine, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, NO. 2, Min-Sheng Road, Dalin Town, Chiayi, Taiwan
Email [email protected]
Background: Ninety-one intracranial hemorrhage prolonged mechanical ventilation patients were successfully weaned from the ventilator. No article had discussed the factors related to 1-year survival in successfully weaned prolonged mechanical ventilation patients with intracranial hemorrhage. This study aimed to evaluate the factors influencing the one-year survival of successfully weaned intracranial hemorrhage prolonged mechanical ventilation patients. The identification of patients with a poor long-term prognosis could guide long-term care decisions after discharge in such patients.
Patients and Methods: We performed this retrospective study on the respiratory care center of Dalin Tzu Chi hospital and enrolled all successfully weaned intracranial hemorrhage prolonged mechanical ventilation patients between 1 January 2012 and 31 December 2017. We analyzed data including age, gender, comorbidities, intracranial hemorrhage type, spontaneous or traumatic intracranial hemorrhage, location of intracerebral hemorrhage, presence or not of an intraventricular hemorrhage, Glasgow Coma Scale, receipt or not of intracranial hemorrhage surgery, receipt or not of tracheostomy, long-term survival, and end-of-life decisions.
Results: We had long-term follow-up data on 69 of these successfully weaned intracranial hemorrhage prolonged mechanical ventilation patients. The 1-year survival rate of successfully weaned patients was 43.5%. The factors unrelated to the 1-year survival rate were comorbidities, intracranial hemorrhage type, spontaneous or traumatic intracranial hemorrhage, location of the intracerebral hemorrhage, presence or not of an intraventricular hemorrhage, intracranial hemorrhage surgery, and tracheostomy. Four factors were independently associated with the 1-year survival rate of these patients: Glasgow Coma Scale score at discharge from the respiratory care center, age ≥ 65 years, signed do-not-resuscitate and do-not-intubate orders, and the absence of comorbidity.
Conclusion: This study emphasizes an important key factor in terms of the survival of successfully weaned intracranial hemorrhage prolonged mechanical ventilation patients. The patient’s Glasgow Coma Scale score at discharge from the respiratory care center is an important predictor of outcomes. These results can help physician better plan the clinical course for intracranial hemorrhage prolonged mechanical ventilation patients.
Keywords: prolonged mechanical ventilation, intracranial hemorrhage, respiratory care center, successfully weaned from ventilator, one-year survival rate
Introduction
The “Trial Plan for National Public Health Insurance Ventilator Dependent Patients Comprehensive Care System” began in Taiwan in July 2000 to resolve the intensive care unit bed shortage and was a step-down care procedure for prolonged mechanical ventilation (PMV) patients.1 This program covers mechanical ventilator care in the following settings: intensive care unit (ICU) (an acute stage for critical care), respiratory care center (RCC) (a subacute stage for patients receiving ventilator support for more than 21 days), respiratory care ward (RCW) (a chronic phase or long-term care), and home care service (a stable period during which the patient is cared for directly by family caregivers or by nursing home nurses). Patients were eligible for RCC admission if they met the Taiwan national health insurance requirements: (a) hemodynamic stability; (b) no vasoactive drug infusion needed; (c) stable oxygen condition (O2 saturation ⩾ 90% or PaO2 ⩾ 60 mmHg) with the requirement fraction of inspired oxygen less than 40% and positive end-expiratory pressure less than10 cm H2O; (d) no critical acute hepatic or renal failure; (e) no massive upper gastrointestinal bleeding; (f) no requirement for surgical intervention within the ensuing 2 weeks or no large open surgical wound; (g) no uncontrolled severe infectious diseases; (h) no life-threatening arrhythmia. We retrospectively studied 574 RCC patients and reported in 2019 the comprehensive clinical experience of those on PMV, including 109 whose intracranial hemorrhage (ICH) led them to require PMV.2 From these 109 ICH PMV patients, we gathered long-term follow-up data on patients who were successfully weaned from mechanical ventilator until December 31, 2018. This study aimed to evaluate the factors influencing the one-year survival of successfully weaned ICH PMV patients. The identification of patients with a poor long-term prognosis could guide long-term care decisions after discharge in such patients.
Patients and Methods
Details of Hospital
The Dalin Tzu Chi General Hospital is a tertiary-level teaching hospital. It has 600 acute care beds, and the intensive care unit contains 59 beds. We have a 10-bed ventilator weaning unit (respiratory care center) which is a weaning unit within an acute-care hospital, caters to PMV patients.
Participant Details
We performed this retrospective study on the respiratory care center of Dalin Tzu Chi hospital. We enrolled all successfully weaned ICH PMV patients consecutively admitted to respiratory care center between 1 January 2012 and 31 December 2017.
Definitions
A PMV patient was defined as one using a mechanical ventilator for at least six hours daily for ≥21 consecutive days. Successful weaning was defined as the patient being independent from the mechanical ventilator for five consecutive days and nights. On admission to the ICU, on admission to the RCC, and discharge from the RCC, each patient’s clinical condition was evaluated using the Glasgow Coma Scale (GCS). The delta GCS was the GCS score at discharge from the RCC minus the GCS score on admission to the RCC. The type of ICH was divided into epidural hemorrhage (EDH), subdural hemorrhage (SDH), subarachnoid hemorrhage (SAH), and ICH intracerebral hemorrhage. The location of the intracerebral hemorrhage was divided into supratentorial and infratentorial.
Comorbidities
The number of comorbidities was assessed. These included: cardiovascular disease (such as essential hypertension, decompensated heart failure, coronary atherosclerotic disease, acute myocardial infarction), chronic lung disease (such as COPD, asthma, bronchiectasis, interstitial lung disease), chronic kidney disease (CKD) (not requiring dialysis), end-stage renal disease (ESRD) (requiring dialysis before admission), neurologic disease (such as bed-ridden stroke survivors, or those with dementia or parkinsonism), chronic liver disease (chronic hepatitis, liver cirrhosis), metabolic disease (diabetes mellitus or other endocrine disorders requiring treatment), malignant diseases, and miscellaneous diseases.
Data Collection
We obtained data from the hospital’s clinical information systems and medical chart review. We obtained details on all ICH PMV patients who were successfully weaned from the ventilator, including age, gender, comorbidities, ICH type, spontaneous or traumatic ICH, location of intracerebral hemorrhage, presence or not of an intraventricular hemorrhage, GCS score on admission to the ICU, GCS score on admission to the RCC, GCS score at discharge from the RCC, receipt or not of ICH surgery, receipt or not of tracheostomy, duration of RCC stays, long-term survival, and end-of-life decisions.
Ethics Approval and Consent to Participate
Our study was a retrospective analysis of medical records. The study represented the lowest risk to the research subject and all information was made anonymous before being made available for research. The study was performed at the respiratory care center of Dalin Tzu Chi Hospital from January 2017 to December 2019. Details related to the methods of the study and the measurement of program outcomes are provided below.
The study conformed to the Declaration of Helsinki 1975, revised Hong Kong 1989. The project was approved by the Buddhist Dalin Tzu Chi General Hospital Research Ethics Committee (Approved IRB No.: B10802009), which exempted the study from the requirement for informed consent.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation or median (range), whereas categorical variables were expressed as frequencies and percentages. The differences in baseline characteristics, the location and type of ICH, number and type of comorbidities, GCS score on admission to the ICU, GCS score on admission to the RCC, GCS score at discharge from the RCC, delta of the GCS, duration of RCC stays, and end-of-life decisions were evaluated using the Student’s t-test for continuous variables and Pearson chi-square tests and Fisher’s exact test for categorical variables. Univariate analysis was used to analyze the difference in variables for those who survived <1 year and ≥1 year. Multivariate stepwise logistic regression models were used to assess the impact of each variable in patients who survived <1 year and ≥1 year. All statistical analyses were conducted using the statistical package SPSS for Windows (Version 17.0, SPSS, Inc., Chicago, IL), and a P value <0.05 was considered to show statistical significance.
Results
Over six years, 109 patients had ICH that caused acute respiratory failure that led to patients requiring PMV. Of these, 91 (83.5%) ICH PMV patients were weaned from the ventilator. We had long-term follow-up data on 69 of these ICH PMV patients. Of these, 39 survived <1 year (56.5%) and 30 survived ≥1 year (43.5%) as of December 31, 2018. Thirty-nine were male and 30 were female with a mean age of 66.2 years. The mean age differed significantly between patients who survived <1 year and ≥1 year (71.15 vs 59.77 years, P=0.001). Of the 40 ICH PMV patients aged ≥65 years, 28 survived <1 year and 12 survived ≥1 year (P=0.013, odds ratio [OR]=0.262). Table 1 shows the clinical variables of demographic data and comorbidities of these successfully weaned ICH PMV patients.
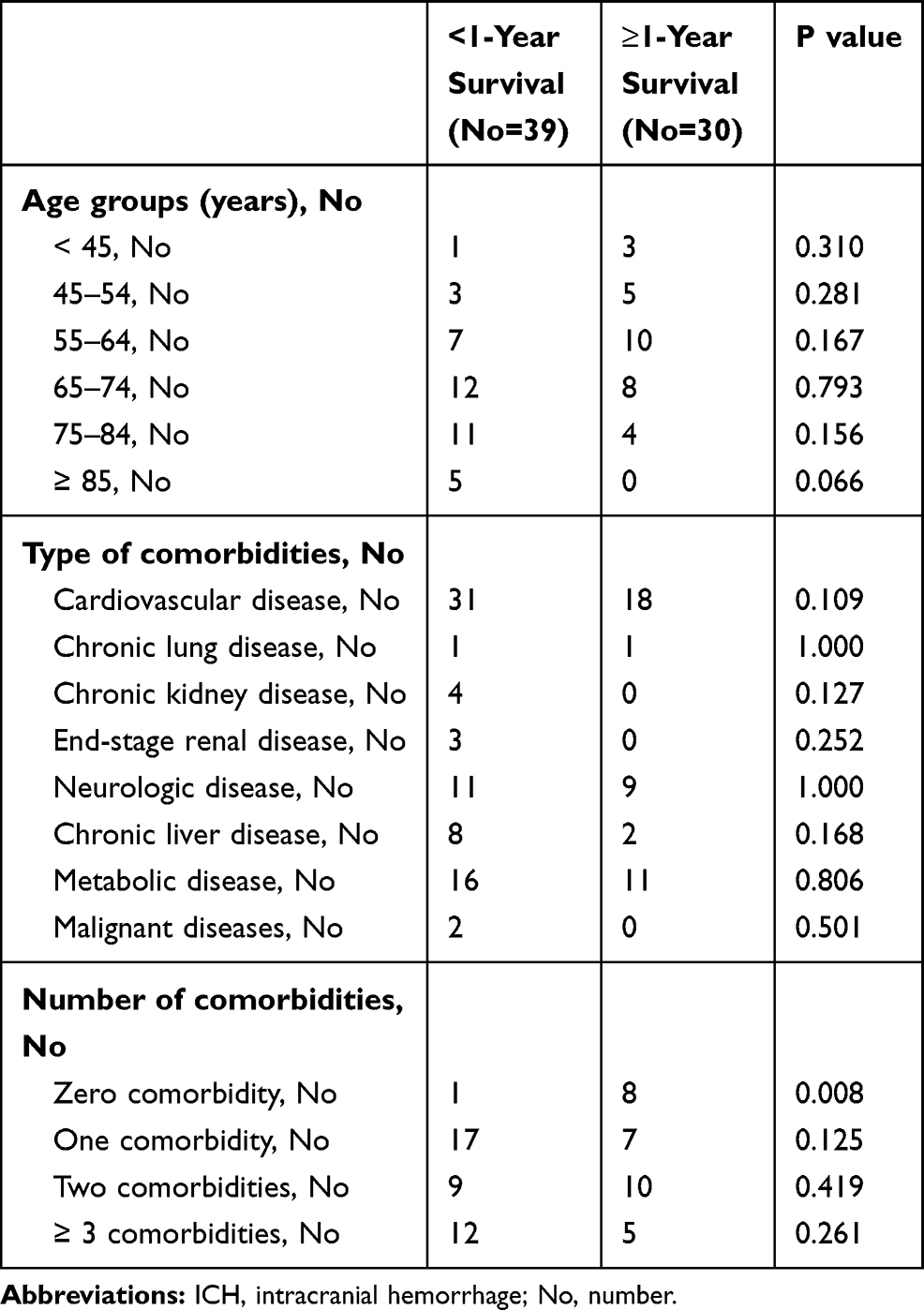 |
Table 1 Comparison of Clinical Variables of Demographic Data and Comorbidities Between Successfully Weaned ICH Prolonged Mechanical Ventilation Patients |
Table 2 shows the types of intracranial hemorrhage, GCS scores, treatment outcomes, duration of RCC stays, and end-of-life decisions for successfully weaned ICH PMV patients. The presence of an ICH surgical intervention and signed DNR and DNI orders were significantly different between patients who survived <1 year and ≥1 year. The GCS score between patients who survived <1 year and ≥1 year showed that GCS ≥7 on admission to the RCC, GCS ≥10 at discharge from the RCC, and delta GCS ≥3 were significantly different between the two groups.
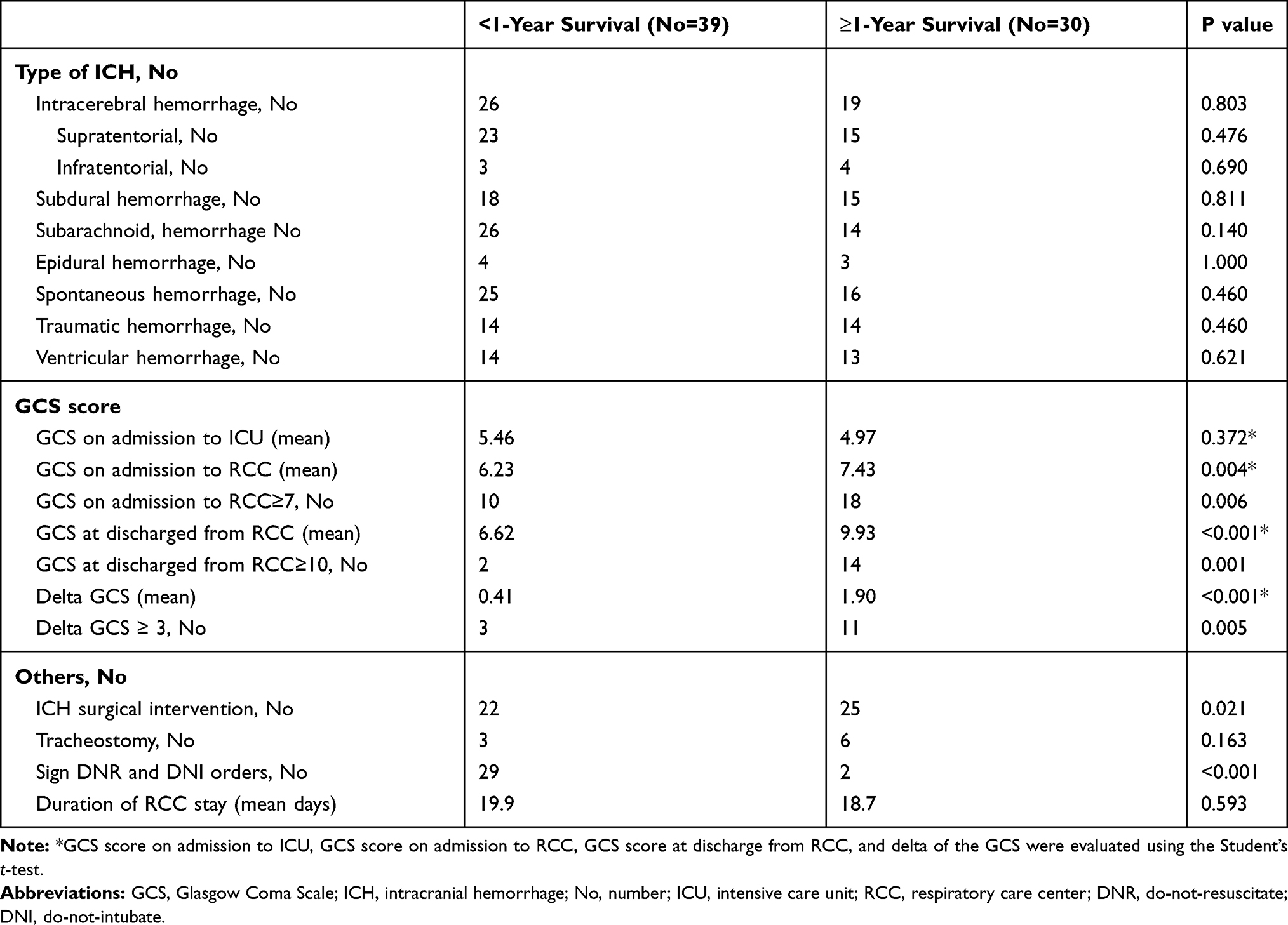 |
Table 2 Comparison of Intracranial Hemorrhage Type, GCS Score, Treatment Outcome, and End-of-Life Decisions Variables Between Successfully Weaned ICH Prolonged Mechanical Ventilation Patients |
Multivariate analysis of the difference in clinical characteristics and outcome between patients who survived <1 year and ≥1 year is shown in Table 3. Only age ≥65 years, GCS ≥10 at discharge from the RCC, signed DNR and DNI orders, and no comorbidity were significantly different between the two groups.
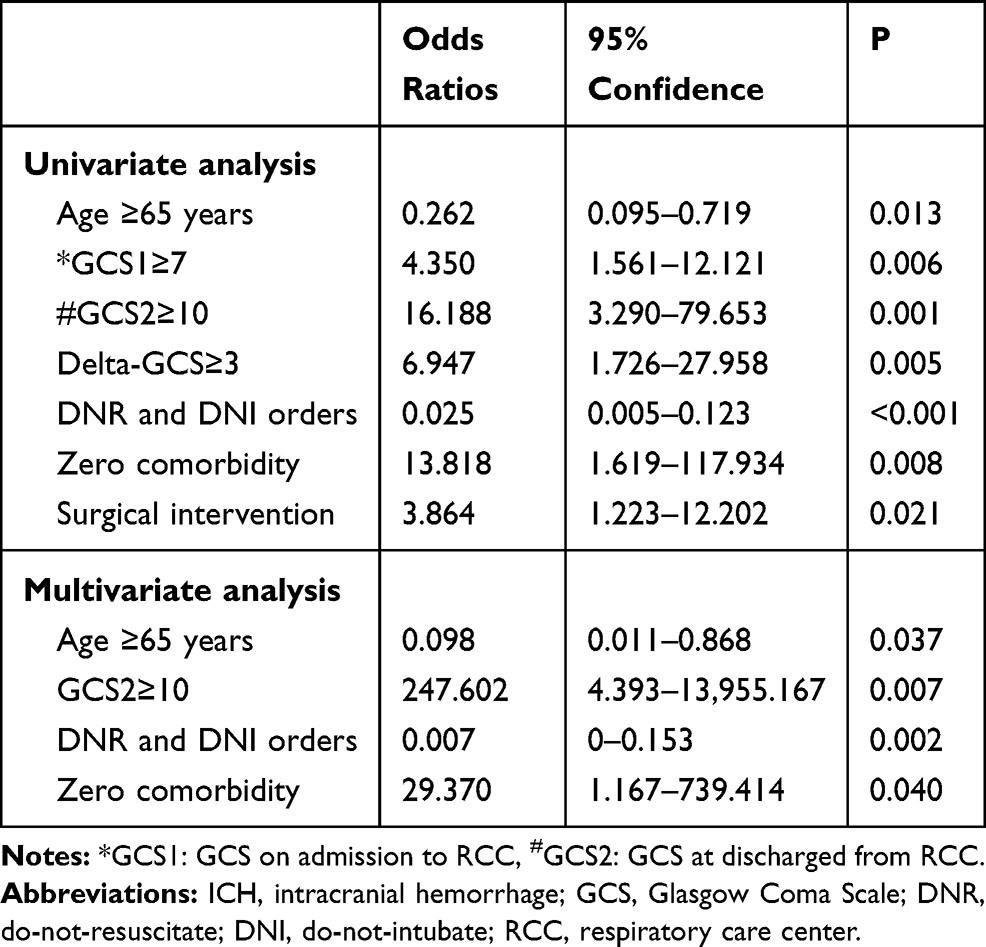 |
Table 3 The Difference in Clinical Characteristics and Outcome Variables Between Successfully Weaned ICH Prolonged Mechanical Ventilation Patients Who Survived <1 Year and Those Who Survived ≥1 Year |
Discussion
The many indications for mechanical ventilation in ICH patients include early neurologic impairment, neurologic deterioration with an inability to protect the airway, status epilepticus, need for a surgical procedure, and cardiopulmonary deterioration. Although some articles have explored the long-term outcome in patients with intracerebral hemorrhage who require mechanical ventilation,3–10 to our knowledge, no one has discussed the factors related to 1-year survival in successfully weaned PMV patients with spontaneous and traumatic ICH (including EDH, SDH, SAH, and intracerebral hemorrhage). Therefore, we reported the long-term survival of successfully weaned ICH PMV patients with the intention of discovering the factors related to improved long-term care of these patients.
Demographic Data and Comorbidity of Successfully Weaned ICH PMV Patients
Burtin et al showed that hemorrhagic stroke patients who required mechanical ventilation and those aged ≥75 years had increased mortality.3 Steiner et al revealed that the independent predictor of death at 2 months was age >65 years in stroke patients undergoing mechanical ventilation.4 Gujjar et al reported that older age predicted higher mortality in intracerebral hemorrhage patients requiring mechanical ventilation.5 Roch et al reported that the probability of death after discharge significantly increased if age at admission was >65 years for intracerebral hemorrhage patients requiring mechanical ventilation.7 In our series too, older age was associated with survival <1 year in successfully weaned ICH PMV patients.
Another factor related to survival <1 year in successfully weaned PMV patients with ICH is the number of comorbidities. To our best knowledge, ours is the first study thus far to analyze the relationship of the number of comorbidities to long-term survival in successfully weaned ICH PMV patients. In fact, only one patient who survived <1 year had no comorbidity versus eight patients who survived ≥1 year.
Some studies have discussed the relationship of various medical comorbidities with the risk of death from intracerebral hemorrhage. The study of Arnone et al found that only congestive heart failure was significantly associated with death from intracerebral hemorrhage.11 Burtin’s et al study showed that mechanical ventilator use for hemorrhagic stroke patients with chronic heart failure and malignancy was associated with increased mortality.3 However, Gujjar et al did not find that comorbidities influenced the outcomes of stroke patients requiring mechanical ventilation.5 In our series, the type of comorbidities was not significantly associated with survival ≥1 year in successfully weaned ICH PMV patients.
The ICH Type and Clinical Management of Successfully Weaned ICH PMV Patients
The type of ICH, location of the intracerebral hemorrhage, spontaneous or traumatic ICH, and the presence of intraventricular hemorrhage had no effect on whether successfully weaned PMV ICH patients survived ≥1 year in our series. In the study of Gujjar e al., the stroke location did not influence the outcomes for stroke patients requiring mechanical ventilation.5 Roch et al showed the location of the intracerebral hemorrhage (supratentorial or infratentorial) of patients requiring mechanical ventilation was not a factor influencing survival.7
It is still unclear whether surgical removal of an ICH will improve the outcome.12–14 In randomized trials of surgical treatment for ICH patients, surgical intervention offered little advantage over conservative treatment.15–17 Roch et al demonstrated that tracheostomy at discharge was a factor influencing survival.7 In our multivariate analysis, no significant difference was observed between successfully weaned ICH PMV patients who had undergone either a tracheostomy or surgical treatment for ICH.
End-of-Life Decisions in Successfully Weaned PMV ICH Patients
In our study, 50 patients (72.5%) signed the DNR order, including 31 patients (44.9%) who signed both the DNR and DNI orders. This result means that, at most, 55.1% of the survivors were willing to receive mechanical ventilation again. The presence of an end-of-life decision (ie, signed DNR and DNI orders) showed significant differences between successfully weaned PMV ICH patients who survived <1 year and ≥1 year. Why did patients’ families sign the DNR and DNI orders for these patients? Despite being successfully weaned from the mechanical ventilator, these patients still had severe neurological deficits. Patients’ families believed that palliative therapy provided a greater benefit to these patients than having to undergo mechanical ventilation again.
GCS Score on Admission to the ICU, GCS Score on Admission to the RCC, and GCS Score at Discharge from the RCC
In view of the GCS score, our study reflects the following conditions. The GCS score on admission to the ICU was not an influencing factor of long-term survival of successfully weaned PMV ICH patients. Successfully weaned PMV ICH patients who survived <1 year had more neurologic impairment when they were admitted to the RCC than those who survived ≥1 year. In addition, the successfully weaned PMV ICH patients who survived <1 year had less neurologic improvement while in the RCC than those who survived ≥1 year. Finally, successfully weaned PMV ICH patients who survived <1 year had more neurologic impairment upon RCC discharge than those who survived ≥1 year.
Factors Affecting Survival ≥1 Year in Successfully Weaned ICH PMV Patients
Roch et al reported long-term outcomes after mechanical ventilation for patients with intracerebral hemorrhage. Their conclusion was that the probability of death after discharge significantly increased if the age at admission was >65 years and if the GCS score at discharge was <15.7 In the study of Burtin et al, age ≥75 years, malignancy, and chronic heart failure were associated with increased mortality for hemorrhagic stroke patients requiring mechanical ventilation.3 In the report of Gujjar et al on intracerebral hemorrhage patients undergoing mechanical ventilation, older age predicted higher mortality.5 These studies discussed the long-term survival of ICH patients undergoing mechanical ventilation but did not focus on successfully weaned ICH PMV patients. Our study showed that four independent factors influenced the one-year survival rate of successfully weaned ICH PMV patients, namely GCS score at discharge from RCC, age ≥65 years, signed the DNR and DNI orders, absence of comorbidity. These results emphasized the following key points in terms of the survival of successfully weaned ICH PMV patients. First, patients who were older and those who had signed the DNR and DNI orders had poorer long-term survival. Older age is an unsurprising influencing factor for reduced mortality. In addition, a signed DNR and DNI order may indicate poorer health status and the family’s recognition that survival is likely difficult. The second key point is that the patient’s GCS score at discharge from the RCC (GCS≥10) is an important predictor of outcome, as the GCS score represents the real recovery of neurologic function in ICH patients. The final neurologic function was closely related to the patient’s long-term survival. Finally, ICH patients with no comorbidity had a better long-term survival rate owing to their previously healthy status. These independent risk factors can help physicians better plan the clinical course for ICH PMV patients.
Limitations of Our Study
This study focused on the long-term survival of ICH patients successfully weaned from PMV. We did not collect patients’ laboratory data, respiratory parameters, Acute Physiology and Chronic Health Evaluation II scores, or other similar relevant variables. We were, therefore, unable to determine which of these measures, if any, were related to the long-term survival of successfully weaned ICH PMV patients. The ICH patients’ laboratory data are essential to the acute stage of ICH patients and less important to understand the patients’ long-term survival. The respiratory parameters are related to whether or not patients successfully weaning in prolonged mechanical ventilation. Our patients in this study are all successfully weaning patients. The evaluation of ICH patient severity score at admission in our surgical ICU is GCS, which is the most important severity score for ICH patients. Acute Physiology and Chronic Health Evaluation II scores is less important for ICH. Intracranial hemorrhage was the second leading cause of PMV patients in our hospital because these patients were transferred to our hospital for an operation with ICH. The numbers of patients are limited in our study. While limited, there are no other articles discussed the long-term survival of ICH patients successfully weaned from PMV before. Our study provides the largest series of ICH PMV patients in the literature. The results of our study can provide an advanced long-term survival of ICH successfully weaned PMV patients to the medical community. The result of our study on long-term outcomes of successfully weaned PMV ICH patients must be interpreted with care, since they derive only from our retrospective single-unit study. We expect that additional studies on long-term survival in successfully weaned successfully weaned ICH PMV patients will yield additional insights.
Conclusions
In this study, 69 ICH PMV patients were successfully weaned from mechanical ventilation. The one-year survival rate of successfully weaned patients was 43.5%. The factors unrelated to the one-year survival rate were type of comorbidities, ICH type, spontaneous or traumatic ICH, location of the intracerebral hemorrhage, presence or absence of an intraventricular hemorrhage, ICH surgery, tracheostomy, GCS score on admission to the ICU, and GCS score on admission to the RCC. Four factors were independently associated with the one-year survival rate of these patients: GCS score at discharge from the RCC (GCS≥10), age≥65 years, signed DNR and DNI orders, and the absence of comorbidities. We expect that these results will help patients’ families understand the prospects for the long-term survival of PMV ICH patients and help clinicians to improve the quality of medical treatment received by these patients.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Not applicable.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There was no funding for this study.
Disclosure
The authors declare that they have no competing interests.
References
1. Bureau of National Health Insurance. Prospective payment system of ventilator dependents managed care demonstration. Available from: https://www.nhi.gov.tw/Resource/webdata/13988_1_1050002331-1.pdf.
2. Huang CH. How PMV is a negligent disease in chest medicine – a study of PMV based on six years’ experience in Taiwan. Ther Adv Respir Dis. 2019;13:1–11. doi:10.1177/1753466619878552
3. Burtin P, Bollaert PE, Feldmann L, et al. Prognosis of stroke patients undergoing mechanical ventilation. Intensive Care Med. 1994;20:32–36. doi:10.1007/BF02425052
4. Steiner T, Mendoza G, De Georgia M, Schellinger P, Holle R, Hackeet W. Prognosis of stroke patients requiring mechanical ventilation in a neurological critical care unit. Stroke. 1997;28:711–715. doi:10.1161/01.STR.28.4.711
5. Gujjar AR, Deibert E, Manno EM, Duff S, Diringeret MN. Mechanical ventilation for ischemic stroke and intracerebral hemorrhage: indications, timing, and outcome. Neurology. 1998;51:447–451. doi:10.1212/WNL.51.2.447
6. Mayer SA, Copeland D, Bernardini GL, et al. Cost and outcome of mechanical ventilation for life-threatening stroke. Stroke. 2000;31:2346–2353. doi:10.1161/01.STR.31.10.2346
7. Roch A, Michelet P, Jullien AC, et al. Long-term outcome in intensive care unit survivors after mechanical ventilation for intracerebral hemorrhage. Crit Care Med. 2003;31:268. doi:10.1097/01.CCM.0000094222.57803.B4
8. Rabinstein AA, Wijdicks EF. Outcome of survivors of acute stroke who require prolonged mechanical ventilatory assistance and tracheostomy. Cerebrovasc Dis. 2004;18(4):325–331. doi:10.1159/000080771
9. Fukuhara T, Aoi M, Namba Y. Mechanical ventilation for comatose patients with inoperative acute intracerebral hemorrhage: possible futility of treatment. PLoS One. 2014;9:e103531. doi:10.1371/journal.pone.0103531
10. Busl KM, Ouyang B, Boland TA, Pollandt S, Temes RE. Prolonged mechanical ventilation is associated with pulmonary complications, increased length of stay, and unfavorable discharge destination among patients with subdural hematoma. J Neurosurg Anesthesiol. 2015;27:31–36. doi:10.1097/ANA.0000000000000085
11. Arnone GD, Esfahani MW, Wonais M, et al. Surgery for cerebellar hemorrhage: a national surgical quality improvement program database analysis of patient outcomes and factors associated with 30-day mortality and prolonged ventilation. World Neurosurg. 2017;106:543–550. doi:10.1016/j.wneu.2017.07.041
12. Auer LM, Deinsberger W, Niederkorn K, et al. Endoscopic surgery versus medical treatment for spontaneous intracerebral hematoma: a randomized study. J Neurosurg. 1989;70:530–535. doi:10.3171/jns.1989.70.4.0530
13. Broderick J, Brott T, Tomsick T, Tew J, Duldner J, Huster G. Management of intracerebral hemorrhage in a large metropolitan population. Neurosurgery. 1994;34:882–887. doi:10.1227/00006123-199405000-00015
14. Hankey GJ, Hon C. Surgery for primary intracerebral hemorrhage: is it safe and effective? A systematic review of case series and randomized trials. Stroke. 1997;28:2126–2132. doi:10.1161/01.STR.28.11.2126
15. Juvela S, Heiskanen O, Poranen A, et al. The treatment of spontaneous intracerebral hemorrhage. A prospective randomized trial of surgical and conservative treatment. J Neurosurg. 1989;70:755–758. doi:10.3171/jns.1989.70.5.0755
16. McKissock W, Richardson A, Taylor J. Primary intracerebral hæmorrhage. Lancet. 1961;278(7196):221–226. doi:10.1016/S0140-6736(61)90353-1
17. Batjer HH, Reisch JS, Allen BC, Plaizier LJ, Su CJ. Failure of surgery to improve outcome in hypertensive putaminal hemorrhage. A prospective randomized trial. Arch Neurol. 1990;47:1103–1106. doi:10.1001/archneur.1990.00530100071015
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.