")
Back to Journals » Open Access Journal of Contraception » Volume 13
The Lived Experience of Women Using Bilateral Tubal Ligation Service in Rural Southern Ethiopia: A Phenomenological Study
Authors Tesfaw M, Abebe A , Bekele B, Baza D
Received 19 January 2022
Accepted for publication 24 April 2022
Published 3 May 2022 Volume 2022:13 Pages 49—60
DOI https://doi.org/10.2147/OAJC.S359120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Igal Wolman
Mihiret Tesfaw,1 Amene Abebe,2 Befekadu Bekele,3 Daniel Baza4
1Department of Reproductive Health, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 2Department of Reproductive Health and Human Nutrition, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 3Department of Public Health, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 4Department of Pediatrics and Neonatal Nursing, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Amene Abebe, Email [email protected]
Background: Bilateral tubal ligation is a highly safe and effective form of permanent contraception for couples who want no more children. However, it is the least known and used form of contraception in Ethiopia.
Objective: To explore the lived experience and perception of women using the bilateral tubal ligation method in Southern Ethiopia.
Methods: Qualitative phenomenological study design was employed. The study participants were recruited by purposive sampling. The data were collected through in-depth interviews and supportive field notes from March 25 to April 24, 2021. All Interviews with the participants were recorded using a digital audio recorder. Inductive thematic analysis was done using Colaizzi’s (1978) seven-step phenomenological analysis framework. Data coding was done using Open code software version 4.03.
Results: A total of fifteen participants were included in the study. Women’s satisfaction, male partner involvement, perception of women using bilateral tubal ligation, socio-cultural influences, client follow-up, and socio-economic impact of bilateral tubal ligation use are the major themes identified in the study. Findings revealed that most of the participants are satisfied with the method and became more productive and got the freedom to participate income-generating activities. The dominance of socio-cultural influences, male partner’s involvement, and client follow-up after the procedure are the common themes that emerged which determine the user’s experience.
Conclusion: Lack of supportive involvement of partners, community pressure, lack of women’s decision-making capacity and inadequate follow-up of women in the post bilateral tubal ligation use by healthcare workers are emergent experiences in the current study. Hence, promoting behavioral change communication for community members regarding bilateral tubal ligation use, empowerment of women’s economic, educational, and decision-making capability and healthcare workers’ follow-up of women in the post bilateral tubal ligation period are recommended.
Keywords: bilateral tubal ligation, phenomenology, perceptions, women, lived experience
Introduction
The world population had been estimated to be 7.8 billion in mid-2020 with an average fertility rate of 2.3 children per woman. Due to unplanned and low contraceptive service coverage, the least developed countries account for the highest birth and infant mortality rates. Maternal and child mortality is highly prevalent in areas where maternal and child healthcare services are not easily accessible.1
Unplanned childbearing restricts women and girls’ educational and economic opportunities that in turn limit their empowerment to attain and safeguard their families and community wellbeing. This further perpetuates the cycle of low utilization of contraceptives which leads to unwanted pregnancy, unsafe abortion, and the associated maternal and child health problems.2
Bilateral Tubal Ligation (BTL) is a permanent method of contraception for women who want no more children. The method involves blocking the fallopian tubes through a surgical procedure with a specially trained healthcare provider. BTL is done by mini-laparotomy with local anesthesia at an outpatient department. The procedure can be performed at any time of the menstrual cycle after pregnancy is ruled out and it has no interference with ovulation and hormonal mechanism in the reproductive system.3–7
Permanent contraceptive methods are commonly used in Asia and America, but women living in Sub-Saharan region including Ethiopia are not usually utilizing the methods.8 BTL could fasten maternal health and wellbeing through generating greater couple-years of protection (CYP) from pregnancy.9
The fertility rate of women of reproductive age in Ethiopia has shown a slight decline in the last decades from being 5.5% in 2000 to 4.6% in 2016. However, there has not been significant progress achieved among rural Ethiopian women which were 6% in 2000 and 5.5% in 2011.5,6 In Ethiopia, permanent contraceptive methods are the least known and used forms of contraception. Permanent contraceptive method utilization in Ethiopia accounts for only 0.4% in 2011 and 0.5% in 2016 which is still below 1% and only 0.2% of reproductive age women are using BTL as contraception means.10 Hence, this study aimed to come up with a detailed exploration and understanding of the lived experience, perception, and the challenges of BTL user women as a method of contraception in the Southern Ethiopia.
Methods and Materials
Study Setting, Design and Period
This study was conducted in Kamba Zuriya District, Gamo Zone Southern Ethiopia. It is located 605 kilometers south of Addis Ababa, the capital of Ethiopia, and Southwest of Arba Minch, the capital of Gamo Zone. Kamba Zuriya district is one of the 14 districts and 4 town administrations in the Gamo Zone. It comprises 29 kebeles (the lowest administrative level). The district has 5 health centers and 6 private health facilities. In Kamaba district, there are 26 health posts in which 46 Health Extension Workers (HEWs) are providing basic healthcare services. A qualitative phenomenological study design was employed from March 25 to April 24, 2021.
Participant Recruitment Procedure
Fifteen women of reproductive age who are currently using BTL in the study setting have participated. Women using BTL in selected kebeles (lowest administrative level in Ethiopia) of Balta health center, Kara health center, and Maze health center catchment of the district were recruited purposefully since these facilities provide BTL service.11 Participants had been traced through their contact addresses from medical records of respective health centers and health posts. HEWs in the respective health posts guided to trace participants. Reproductive age women who had used BTL for more than two years and willing to participate in the study were purposively included in the study.
Sample Size and Sampling Procedure
Fifteen women who had used BTL participated in this study. The sample size required for the study was determined by considering the experience of previous literature, the recommendation of different research books, and the phenomena of interest. However, information saturation was used as an indicator for termination of further inclusion of participants during the interview.12–14
The women who had shared and meaningful experience with the phenomena of interest were purposely selected. A homogeneous purposive sampling technique was used to select the study participants from the kebeles of the three health centers (Balta health center, Kara health center, and Maze health center) catchment area. Health Extension Workers (HEWs) were used as a community guide to tracing the study participants in their residential address in their respective kebeles.
Data Collection Tools and Procedures
Data were collected by two trained healthcare professionals who had previous experience in qualitative in-depth interview (IDI) data collection. A semi-structured IDI guide with open-ended questions was used to explore rich data based on participants’ expressions and language “Supplementary Material” Section 1 The actual interview was conducted at health posts and the participant’s home. The private room was used to facilitate one-on-one communication. Probing was used to ensure the depth and clarification of the information collected during the interview. The further interview was terminated after reaching the information saturation. The IDI guide was used to secure the sequence and flow of ideas and to stick to the aim of the study during interview sessions. All interviews were audiotaped and supportive field notes were also used. The interview last on average 29 minutes.
Data Quality Management and Analysis
After repeatedly listening to the audio recorded data for an accurate understanding of the message, audio transcripts were changed to the text transcripts in the local language. The text transcripts were translated to the English language for analysis by the same person who is a native speaker of the local language (Gamogna) and an expert in English. The transcripts and field notes were converted into a rich text file and prepared to be imported into Open Code software. Data coding and management were assisted by using Open Code Software Version 4.03. Inductive thematic analysis method using Colaizzi’s (1978) seven-step phenomenological data analysis framework was followed during data analysis and development of the sub-themes and themes;15 step 1: Read all protocols to acquire a feeling for them (Reading, and re-reading of the transcription and field notes were conducted to be familiarized with the data.), step 2: Review each protocol and extract significant statements (identified relevant data from the transcripts explaining the phenomenon of interest), step 3: Spell out the meaning of each significant statement (ie, formulate meanings /significant meanings were spelled out holding the researchers own experiences and background knowledge in abeyance and developed the potential themes) ‘Supplementary Material’ Section 2, step 4: Organize the formulated meanings into clusters of themes (comparative analysis of clusters of themes with themes, themes with codes and codes with codes and codes with the data were done to validate whether the meaning are exactly developed from the data and negative case analysis was done to note any discrepancies among or between the various clusters) ‘Supplementary Material’ Section 3, step 5: Integrate results into an exhaustive description of the phenomenon under study (visual model (thematic framework) have been developed to illustrate the level of integration of the developed themes), step 6: Formulate an exhaustive description of the phenomenon under study in as unequivocal a statement of identification as possible (thick description of the themes and sub-themes developed was done which are supported by direct verbatim quotations from the data) and step 7: Ask participants about the findings thus far as a final validating (preliminary findings as well as the final results were made member checks for final validation).
Trustworthiness
To ensure the rigor of the study, Credibility, transferability, dependability, and conformability were maintained. Recorded audio data and field notes copies were kept safe and used as reference materials. Triangulation of data was conducted by asking interview questions in different ways, using various data sources and methods. Peer-debriefing was done with a similar status colleague who is out of the context of the study. Copy of the transcribed text and distribution of preliminary findings to study participants was conducted to check for any inconsistencies. All the participants provided with the preliminary findings confirmed all the themes and ideas listed were congruent with their lived experience. Purposive selection of the study area and participants was done. A clear method of participant recruitment was employed to improve the transferability of the findings in similar settings and context. To ensure the consistency of the study, sections devoted to the research design and implementation, methods, and approaches of data collection, and reflective appraisal evaluating the effectiveness of the process of inquiry was clearly described. To provide readers with an accurate mental picture of the process of the study, copies of field notes and audio records are kept. An audit trial was conducted by a senior qualitative researcher.
Definition of Key Terms
Bilateral tubal ligation -is a surgical method of permanent contraception for women who want no more children.6
Phenomenology – is a philosophical discipline introduced by Edmund Husserl which deals with a direct investigation and description of phenomena.16
Perceptions- is the way of gathering, organizing, and interpreting sensory information to act to external stimuli.17
Results
Socio-Demographic and Economic Characteristics of Participants
A total of 15 rural-dwelling women who are currently using the BTL method in the Kamba Zuriya district participated in the study. The mean age of the participants is 36.5 years. The mean age of the women at BTL use was 30 years. Most of the participants, 14 (93%) were housewives and the remaining one was a merchant. Thirteen participants (86.7%) are protestant Christianity followers while the remaining 2 (13.3%) are Orthodox Christians Table 1.
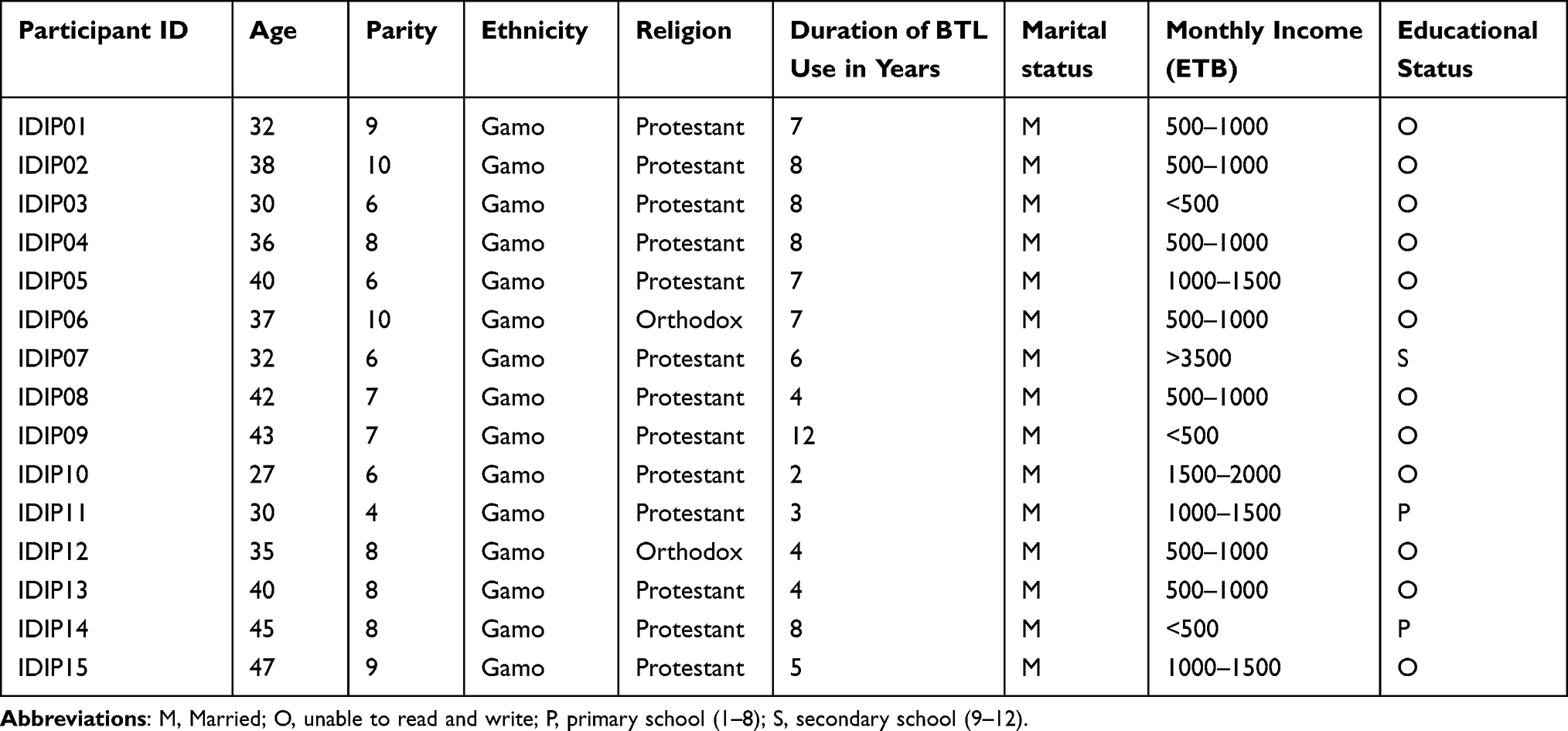 |
Table 1 Socio-Demographic and Economic Characteristics of the Study Participants in Kamba Zuriya District Southern Ethiopia, 2021 |
The Major Themes of the Study
Six major themes and thirteen sub-themes are developed from the participant responses in the current study. The identified themes include women’s satisfaction on BTL use, male partner involvement on BTL use, perception of women using BTL, socio-cultural influences against BTL use, Client follow-up after BTL use, and socio-economic impact of BTL use “Figure 1”.
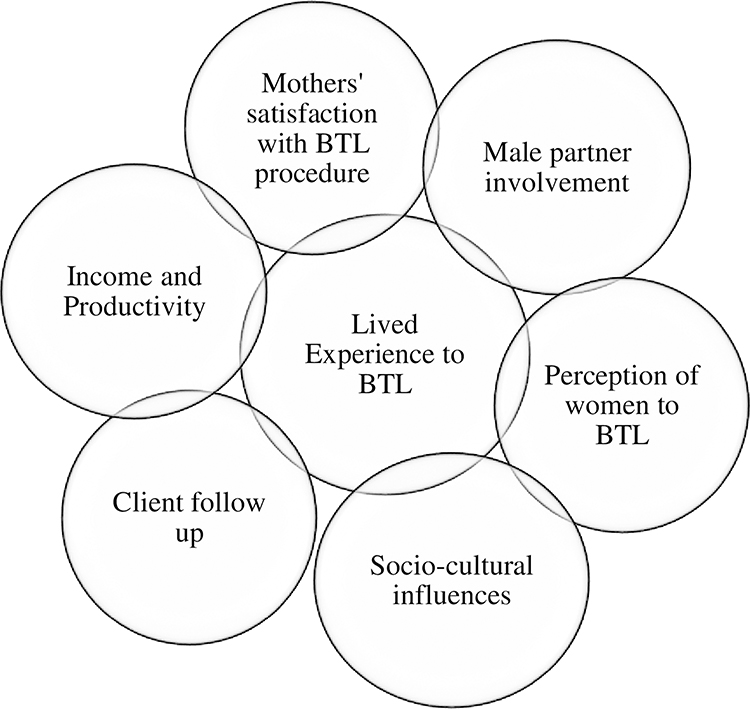 |
Figure 1 A thematic linkages of major themes among women using bilateral tubal ligation contraceptive method. |
Theme One: Women’s Satisfaction on Bilateral Tubal Ligation Use
Women’s satisfaction with BTL use is the first major theme inductively developed from the participant responses. This theme developed from participant responses that explain attributes related to the study participants’ perceived satisfaction with BTL use and pain experienced during the BTL procedure. This theme comprises one sub-themes which is pain experience with BTL procedure.
Sub-Theme One: Pain Experience with Bilateral Tubal Ligation
This sub-theme was developed in reference to the participant’s responses about their pain experience with the BTL procedure. The participant’s data of this study expressed their pain experience in a contradicting manner. For some study participants, the procedure was painless and comfortable but for some others it is painful and not comfortable.
For instance, a 27- year-old woman of 6 children who used BTL for 2 years expressed her positive experience in the following ways:
GOD blessed me with a healthy life after the operation. Um—, it was very nice, and there was no pain during the procedure as I anticipated before. After getting this service supplied by our government, my life is completely changed in all aspects. Since I started using the method, my overall physical appearance improved and my health has returned to normal. [IDIP10]
However, for others, the pain experience was the opposite of what had been noted above. Another BTL using woman of age 42-year-old who has 9 children, the participant felt pain around the incision site following BTL procedure. The following verbatim quotation received from the woman supports the idea:
I felt pain for 2 months at the incision site after the procedure. The pain is also aggravated whenever I try to lean forward, while I walk and perform different activities. [IDIP08]
Theme Two: Male Partner Involvement in Bilateral Tubal Ligation
This theme is developed from participant data related to the male partner involvement in contraception in general and BTL use in particular. In this study, the participant responses revealed that the male partners have had varying levels of involvement in permanent contraceptive methods such as BTL. The theme developed to include two sub-themes: male Partners supportive involvement and male partners discouraging involvement.
Sub-Theme One: Male Partners Supportive Involvement
This sub-theme is emerged from the data regarding the recognition and support of male partners’ contribution for better planning, to determine family size and choice of contraception. This notion was well explained by a 27-year-old mother of 6 children who had been using BTL for 2 years in the following ways:
Both I and my husband did not want to have more children but the community perception regarding the permanent method of contraception is not supportive. However, I overcome the challenges and decided to use the method because of the encouragement and support of my husband in all aspects. [IDIP10]
The community members not only influence the woman using BTL but also influence the husband of the user and other family members too. The same participant stated how her supportive husband reacted against the community influence as follows:
We have been hearing a lot of back-talks against my use of the method. However, on one occasion the community members and the close friends of my husband asked him why he allowed me to use the method. He responded to them as to why are you worried about our life; she is my wife, we decided to improve our living conditions, it is all our matter. Why did it become an agendum for you? Even I and my wife may decide to have a single child but currently, we have six. Stop talking about our life, you may make it your problem if I ask you to give more children, leave us alone, this is only our private issue. [IDIP10]
Sub-Theme Two: Male Partners Discouraging Involvement
The male partners discouraging involvements identified in the data include refusal of the use of the method from the beginning and an attempt to control all the decisions of their wives. Due to fear of their partner’s discouragement, some women decided to use BTL on their own without knowledge of their partner and they are facing different forms of oppression. If the women decide alone to use the method, their partners correlate it as the cause of illness if they get ill. This idea is well explained by a mother of age 40-years who have 8 children as follows:
I used the method without getting my husband’s permission. As he did not know that I am using permanent contraception, I and my husband continuously get into conflict. He checks my arms whether I am using the contraceptive which is buried in the arms (implants). However, I try to convince him to lie; GOD has finished giving children; my mother also stopped bearing children at my age but he continued oppressing me, he does not care about me and he still forces me to give birth to another child. [IDIP13]
Theme Three: Perception of Women Using Bilateral Tubal Ligation
Perception towards BTL use was among the major themes developed from the data. The perception was developed as a theme in reference to the participant data related to participants’ outlooks on BTL use. This theme includes sub-themes such as the beliefs of BTL users, perceived benefits of using BTL, community pressure and BTL users’ reaction.
Sub-Theme One: The Beliefs of the Bilateral Tubal Ligation Method Users
This study revealed that BTL is expected as a solution for rural women to control birth because of the inaccessibility of other methods of contraception at the right time.
The above opinion is supported by the verbatim quotation received from a woman who is using BTL for 4-years, a mother of 7 children, and aged 36- years in the following manner:
I think using BTL is a better option for a rural woman. Using other contraceptives which are kept in our left hand (by pointing the area in her arm) requires time and access for a woman. Then on removing when it expires, umm … then again it requires going for another insertion, this way it covers all potential areas of insertion on the user’s hands. Sometimes the health care providers are not willing to remove the contraceptive (implant); the women might make a repeated visit to the health facilities. Because of this reason, using uterine inversion (BTL) is a better option to stop bearing children than facing this all burden. [IDIP8]
Sub-Theme Two: Perceived Benefits of Using Bilateral Tubal Ligation
This study confirmed that up-taking of BTL has numerous perceived advantages. From the participant’s viewpoint, it has improved their health status by relieving them from problems related to pregnancy, labor, and childbirth, resolved menstrual problems and irregularities. This result is espoused by the verbatim quotation taken from a woman of age 32-years, a mother of 7 children, and who is using BTL for 7 years as follows:
Umm—-, it (BTL) is a good method for those who want to be healthy. I decided to use the method, I know my problems and the challenges I faced during pregnancy, childbirth, and while caring and feeding many children. This method (BTL) saved me from such exhaustion. Now I am encouraging those who want to use this method. The use of this method helped me to be healthy. [IDIP01]
Another woman of 38-year-old, who is the mother of 10 children and who had been using BTL for 10 years echoed the above advantages of BTL in the following ways:
I think it (BTL) is a good option for women who decided to terminate the pregnancy. It saved me from dying from complications of pregnancy, labor, and delivery. However, overcoming the pressure exerted by the community on permanent contraceptive users is not easy; it is too much stress. Religious leaders are playing an important positive role in the community, they share the grievances and stress that users of the method are facing. For instance, I faced a huge challenge because of my use of the method (BTL) but when I got the religious fathers, they prayed for me and I got relief. [IDIP 06]
The above notion is further supported by a verbatim quotation obtained from a 42-year-old mother of 9 children as follows:
It (BTL use) makes me happy; before I use the method, my monthly bleeding was irregular and whenever it appears; it stays for many days but now it is regular per month. It (BTL use) also shortened the duration of bleeding to less than three days. [IDIP08]
Sub-Theme Three: Community Pressure on the Bilateral Tubal Ligation Users
In this study, the data further shown that BTL users are facing various direct and indirect negative pressures about using BTL. This result is evidenced by a 27-year-old mother of 6 children who had been using BTL for 3 years in the following ways:
Our community members are usually making an agendum which is not their concern. Some members of our community say that “women in your age are not even married but you are telling us you decided to stop childbearing”. Some others reproach my husband for my use of the method, they say that “Your husband is a mad person, he does not want to have children and he does not know children are gifts from the GOD. [IDIP10]
The other participant enlightened that the husbands of other women in the community attempt even to restrict my relationship with their wives. They fear that if their spouse makes a relationship with me, I may inform or convince them using the method. This result is well stated in the verbatim quotation received from the mother of 9 children, used the method for 7 years and aged 32 years as follows:
Some husbands of the community members even warn me not to be together with their wives. If you make a relationship with our spouses, you would inform and convince them to use the method. [IDIP02]
Sub-Theme Four: Bilateral Tubal Ligation User’s Reaction Towards Community Pressure
This study revealed that the community members exert negative and unnecessary pressure on the users of the BTL method. Women who are using BTL after overcoming all the pressure they face from the community are able to defend their decision in all possible ways. One of the participants of this study who are using BTL for 6 years, at the age of 32 years and a mother of 6 children elaborated how she is defending the discouraging comments of the community regarding her BTL use as follows:
When our community members begin to forward discouraging comments regarding my use of the method, I respond to them by saying giving birth is so simple, but the difficult task is caring and safeguarding the children appropriately. Whenever, we meet in social gatherings like wedding ceremonies, or funeral or mourning services, they begin to challenge me by asking questions and even some of the community members make opposing comments. However, I always educate and tell them the truth, how the use of this method improved my health, and the freedom I am getting from the use of the method. I also encourage those who want to have no more children to decide to use the method in the meantime. [IDIP07]
Theme Four: Socio-Cultural Influences Against Bilateral Tubal Ligation
Socio-cultural perspectives and influences of the community are some of the major themes developed from the data in this study. The theme describes the socio-cultural influences of the community regarding the use of BTL use. The theme comprises two logically coherent sub-themes: the myths and misconceptions towards BTL use and gossips (rumors and back-talks) about BTL use.
Sub-Theme One: Myths and Misconceptions Towards Bilateral Tubal Ligation
Those community members have information and awareness regarding the availability of BTL, they think that the method is for only women of old age. The following verbatim quotation obtained from a 32-year- old woman, who have 9 children and used the method for 7 years elaborates this statement:
The community members label me as a fool woman saying you are using this method which is designed for only old-age women while you are in your adulthood age. [IDIPO01]
Sub-Theme Two: Gossips Related to Bilateral Tubal Ligation Use
In communities with diversified culture, religion, and socio-cultural aspects like Ethiopia, permanent contraceptive users are a victim of different Gossips and back talks related to BTL use. This sub-theme is developed from the participant’s information regarding back-talks, rumors, and conversations about the use of BTL. This finding is well expressed by one of the women who had been using BTL for 4 years who have 9 children and at the age of 42 years as follows:
I frequently heard that the community members make a back-talk by saying that “she cannot even control her urine after this using the method; she urinates in public. [IDIP08]
Theme Five: Client Follow-Up After Bilateral Tubal Ligation Use
Client follow-up is one of the major themes that emerged from the data. This theme included two conceptually inter-related subthemes: Lack of follow up after BTL use and Expectations of the BTL users after the procedure.
Sub-Theme One: Lack of Follow Up by Healthcare Workers Following BTL Use
Post-procedure client follow-up is an opportunity to assess the experience and overall health status of women using BTL. However, participant responses of this study show that post-operative client follow-up by the healthcare workers is a neglected duty. The following direct verbatim quotation taken from a 32-year-old who has 9 children and using BTL for 7 years supports this concept:
During the procedure, the healthcare workers promised to visit and assess my health condition but no one visited me since I use the method. After they provide the service, I was left alone. (IDIP01)
Sub-Theme Two: Health Care Provider and BTL Users’ Relationship
This sub-theme has emerged from the data in reference to the client’s expectation following their BTL use. The findings of this study show that healthcare workers are not keeping their words which they promised during the BTL procedure to visit and monitor their health condition. A verbatim quotation obtained from a mother of age 32 years, having 6 children, and who had used BTL for 6 years described this statement as follows:
I think it is better to get follow-up care and monitor our health condition after using the method. My message for healthcare workers is please do not let the woman alone after she uses this method. For example, no healthcare worker visited me since I started using the method. It is for the first time you come today for an interview since I used the method. We should be under the close supervision of health care providers and the government. (IDIP07)
Theme Six: Socio-Economic Impact of Bilateral Tubal Ligation Use
Income and productivity of BTL use are among the main themes that emerged from the data. The theme is developed from participant responses after coherently and logically linking concepts related to the contribution of BTL use in social engagements and improvement of family income. The theme comprises two sub-themes: Improvement of fulfilling social responsibilities and productivity of the users.
Sub-Theme One: Improvement of Fulfilling Social Responsibilities by Bilateral Tubal Ligation Users
This study revealed that BTL is a unique permanent birth control method that played an important role in the improvement of societal engagement and the social status of the users. The use of the method enabled the women to fulfill appropriately their social responsibilities. This result is well described in the following verbatim quotation received from a mother of age 27-year-old, who had been using BTL for 2 years and having 6 children in the following ways:
Before I begin using this method, I could not fulfill my social responsibilities. I had not sufficient time to be engaged with social organizations such as attending church services, edir and equb (social organizations), funeral services, and wedding ceremonies because I had the additional burden of looking after my small children. If I became pregnant it was also impossible to be engaged. (IDIP10)
Sub-Theme Two: Improvement in the Productivity of the Bilateral Tubal Ligation Users
The data revealed that BTL use created a good opportunity to work hard and earn more income which further paved the way to provide adequate care and support for existing children. One of the study participants, aged 32-year-old, having 6 children, and who had been using BTL for 6 years described the above notion as follows:
After I use this method, I can run wherever for our business. In terms of income, previously, I could not earn enough money, leave alone get extra; sometimes even I face a lack of money to buy a coffee. After I became a user of this method, I got time for farming activities and also I am earning money to purchase the needed from the market. Currently, we (she and her husband) are planning to build a house with an iron roof. I am also able to buy a drench for our cows. These all-important things are due to my use of the method which gave me all the freedom to work hard. When I evaluate the advantages of using this method even I regret why I did not use it earlier. (IDIP07)
Another woman of age 35-year-old, who has 8 children and had been using the BTL for 3 years further explained the above result in the following manner:
Since I began using this method (BTL), I got the opportunity to go anywhere I needed, you know (the interviewer) if I had a child, even I cannot meet with you today. Now, I am free of childbearing, I farm vegetables like Sidama onion, Cabbage, and potatoes in my backyard. (IDIP12)
Discussion
This study attempted to investigate the multidimensional and complex experience of women using the BTL method in the rural Kamba district, Southern Ethiopia. This study revealed that the use of BTL had a direct and positive impact on the users’ overall satisfaction with the use of the method. Menstrual irregularities and pain during menstruation among the participants returned to normal. This result is in contrast with the study findings in the USA and South Africa where the studies show the participants had developed a sense of hopelessness and regret after getting a forced sterilization.18–20 This difference might be due variability of the study participants, the setting, and socio-cultural aspects where in the previous studies coerced sterilization of HIV positive women in the health facilities and cross-sectional study design was implemented.
The present study also confirmed that the pain experience of the participants with the BTL procedure is contradicting, for some of the study participants, the procedure was painless and comfortable but for some others, it is painful and not comfortable This finding is consistent with the study result in Kaziba, Congo, where the study reported somatic symptoms after the BTL procedure was varied from woman to woman.21
Partner collaboration in decision-making on family planning, in general, influences the acceptance and rejection of the methods. The current study shows partners of the study participant women make positive and negative involvement about their BTL use. The data from participant responses show approximately an equal portion of the participant’s partners making supportive and discouraging involvement. This finding is corroborated with other study findings which were conducted in India and Ethiopia where the studies reported that partner’s approval or rejection had an enormous impact on the women’s contraceptive method choice and its use.22–25
The overall perception of BTL users in the current study was developed from the data in reference to participants’ beliefs about the method, perceived advantages of using BTL, and their reaction and defense mechanisms regarding the decision to use BTL. The data from the participant responses show participants’ belief that the use of the BTL method is a solution for rural women who want no more children. This result is consistent with the study result of Southwest Nigeria and Catholic Hospitals in the USA, where the studies reported that the majority of the participants’ believe the use of BTL is an important permanent family planning choice for women who want no more children and the studied ob-gyns disagreed with the churches strict prohibition of sterilization service in favor of BTL use respectively.26,27 However, this finding is not supported by the study result of Usmanu Danfodiyo University Teaching Hospital Sokoto, Nigeria where the study reported the study participant’s belief against the use of the BTL method.26 The possible reason for the difference might be the difference in the study setting and design where the previous studies done using facility based cross-sectional design on antenatal care clinic followers.
The current study shows BTL users experienced different community-level influences. Myths and misconceptions and gossips (rumors and back-talks) are the commonest influences towards women using the method. There are many unresolved community influences on BTL uptake which have a significant role in discouraging the use of BTL by others who want to use it. The commonest myth and misconception about BTL use are assuming the number of children ever born as a precondition for BTL uptake compromising all appropriate age women freedom of contraceptive method choice. Insults in front of community gatherings attempt to convince the husbands of BTL users to dump them out reasoning BTL user women as useless since they stopped childbearing and putting pressure on their husbands to go for other women were among the common community-level influences identified. This finding is reported similarly in studies done in Uganda, in central and eastern provinces of Kenya and Kwara State, Nigeria where the studies reported that socio-cultural influences as the main determinants of BTL uptake.22,28–30
According to WHO recommendation, emergency preparedness, and complication readiness should be implemented before, during, and after the BTL procedure for those who underwent BTL.31 However, according to the current study, this recommendation is not fulfilled. Participant responses of this study show that post-operative client follow-up by the healthcare workers is a neglected duty. The findings also show that healthcare workers are not keeping their words which they promised during the BTL procedure to visit and monitor the user’s health condition.
This study revealed that BTL is a unique permanent birth control method that played an important role in the improvement of societal engagement and the social status of the users. The use of the method enabled the women to fulfill appropriately their social responsibilities and created a good opportunity to work hard and to be productive. According to this study, the use of the BTL method provided change on the routine responsibilities of women which are staying at home, and bearing and caring for their children. The use of BTL ensured the women’s freedom of working out of home as they wish to work. After the use of BTL, they can participate in social and economic activities such as attending churches, participating in social services like wedding and funeral services, and income-generating activities like cultivating different vegetables on their land and caring for cattle respectively. This finding is in contrast with the study finding conducted in Kaziba district, Congo where the study reported that the use of BTL decreased the productivity of women and made them unable to go to the field due to illness after the procedure.21 The possible reason for the dissimilarity of the results might be the perception about pain control, healthcare seeking behaviours of the mothers and the follow-up methods of the healthcare workers.
According to this study findings, policy makers, governmental and non-governmental organizations and other stakeholders should emphasize on improvement of males positive impact on BTL use, increasing healthcare workers follow-up post BTL use, improve behavioral change communication for community members on the BTL use, empowerment of women’s economic, educational, and decision-making capability and healthcare workers’ and health facilities’ capacity are recommended. Furthermore, we recommend to make further studies by using mixed methods, using different participants and setting.
Strengths of the Study
In this study, data collection and analysis were not limited based on predetermined variables; an open thematic approach was followed. Face-to-face interaction with participants was used to monitor relevant non-verbal cues and clarify terms that were not understandable for the participants.
Limitations of the Study
The main purpose of this study was to explore, describe and investigate the lived experience of women using BTL in Kamba district, South Ethiopia. The study quite surely achieved the study objectives. However, it also has some general and specific limitations. This study is conducted using a purposely selected small sample size, generalizability of the findings to other larger populations is not possible. Personal differences between the two data collectors might create a difference in the responses of the participants. Translation of the data to English for analysis and write-up might introduce deviation in some too local and contextual expressions of the participants.
Conclusion
Women who underwent bilateral tubal ligation had a positive impression and are satisfied with the method. Supportive involvement of partners plays an important role in the women’s decision-making capacity about bilateral tubal ligation use. Follow-up of women’s by healthcare workers after the use of the method emerges as a neglected task in the study. Many socio-cultural influences are discouraging women from using the bilateral tubal ligation method in the study area. The use of the BTL has enabled the women to fulfill appropriately their social responsibilities and created a good opportunity to work hard and to be productive.
Abbreviations
BTL, Bilateral Tubal Ligation; IDI, In-depth Interview; IDIP, In-Depth Interview Participant; WHO, World Health Organization.
Data Sharing Statement
The dataset analyzed for the findings of this particular study is available with the corresponding author and can be accessed upon reasonable request.
Ethics Approval and Informed Consent
This study was conducted following the declaration of Helsinki for studies involving human participants. Ethical clearance was obtained from the Institutional Review Board of Wolaita Sodo University College of Health Science and Medicine. The necessary communication was made with Gamo Zone Health Department and Kamba Zuriya District health office sequentially. Before data collection from participants; the nature of the study, its relevance, and participant rights were explained. The willingness of participants was asked before conducting the interview session. Informed written consent was obtained from each participant. To keep the confidentiality and anonymity of the participants’ code labels of participants was used. The study participants also agreed to publish their anonymized responses in scientific journals for better dissemination of the results “Supplementary Material” Section 4.
Acknowledgment
Our gratitude goes to the research supervisors, data collectors, study respondents, Gamo Zone Health Department, District Health Officer, and the Kebeles and Health Center Administrators for their valuable contribution.
Author Contributions
All authors equally contributed to this work beginning from the conception, study design, execution, acquisition of data, analysis, and interpretation. Authors of this work took part in the drafting, revising, and/or critically reviewing of the article and finally agreed on the journal to which the article was submitted. All authors are also reviewed and agreed on all versions of the article before submission, during revision, and the final version is accepted for publication and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Population Reference Bureau. World population data sheet 2020; 2020. Available from: https://interactives.prb.org/2020-wpds/#.
2. UNFPA. State of world population 2019; 2019. Available from: https://www.unfpa.org/state-world-population-2019.
3. Fathalla M. Contraceptive technology and safety. IPPF Medical Bulletin. 1987;21(1):1–4.
4. World Health Organization. A Guide to Family Planning for Community Health Workers and Their Clients. World Health Organization; 2012.
5. Chin EL. Visualizing mini-laparotomy tubal ligation under local anesthesia: effective skills acquisition for health care workers in developing countries. Baltimore, Maryland; 2016.
6. Republic of the Philippines,Department of Health. Bilateral tubal ligation by minilaparotomy under local anesthesia. Participant’s Handbook. 2016. Available from : https://doh.gov.ph/sites/default/files/publications/BTL_by_MLLA_Training_Manual_participants_handbook.pdf. Accessed April 28,2022.
7. Commission FPaC. Summary and statistical report of the 2007 population and housing census: population size by age and sex. Addis Ababa; 2008.
8. Oliveira I, Dias JG, Padmadas SS. Dominance of sterilization and alternative choices of contraception in India: an appraisal of the socioeconomic impact. PLoS One. 2014;9(1):e86654. doi:10.1371/journal.pone.0086654
9. United Nations, Department of Economic and Social Affairs . World Family Planning - Highlights. United Nations; 2017.
10. CSA CSACEaI. Ethiopia Demographic and Health Survey. Addis Ababa: CSA and ICF; 2016.
11. Departement GZH. Sexual and reproductive health performances by district: permanent method of contraception in gamo zone. Arbaminch; 2020.
12. Creswell JW, Creswell JD. Research Design: Qualitative, Quantitative and Mixed Methods Approaches.
13. Polit DB, Beck CT. Nursing Research – Generating and Assessing Evidence for Nursing Practice.
14. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. 2018;18(1):148–166. doi:10.1186/s12874-018-0594-7
15. Morrow R, Rodriguez A, King N. Colaizzi’s descriptive phenomenological method. Psychologist. 2015;28(8):643–644.
16. Kurg RN. Edmund Husserl’s theory of image consciousness, aesthetic consciousness art [Dissertation]. University of Fribourg; 2014.
17. GO Unumeri, HT Ayo. Perception and Conflict. Nigeria: National Open University of Nigeria; 2009.
18. Shreffler KM, Greil AL, McQuillan J, Gallus KL. Reasons for tubal sterilisation, regret and depressive symptoms. J Reprod Infant Psychol. 2016;34(3):304–313. doi:10.1080/02646838.2016.1169397
19. Strode ZEa A. ‘I feel like half a woman all the time’: the impacts of coerced and forced sterilisations on HIV-positive women in South Africa. Agenda. 2012;26(2):24–34. doi:10.1080/10130950.2012.708583
20. Jahanian Sadatmahalleh SH, Ziaei S, Kazemnejad A, Mohamadi E. Evaluation of influencing factors on tubal sterilization regret: a cross-sectional study. Int J Fertil Steril. 2018;12(3):200–206. doi:10.22074/ijfs.2018.5272
21. Lutala JFH PM, Luhiriri LN. Psychosocial implications of tubal ligation in a rural health district: a phenomenological study. Reprod Health. 2011;8(1):38. doi:10.1186/1742-4755-8-38
22. Nagapurkar S, Santpure A, Giri P, Bhanap P. Study of biosocial factors affecting laparoscopic tubal ligation in rural Maharashtra, India. Int J Reprod Contracept Obstet Gynecol. 2016;5:4461–4465. doi:10.18203/2320-1770.ijrcog20164363
23. Abraham W, Adamu A, Deresse D. The involvement of men in family planning an application of transtheoretical model in Wolaita Soddo Town South Ethiopia. Asian J Med Sci. 2010;2(2):44–50.
24. Chekole MK, Kahsay ZH, Medhanyie AA, Gebreslassie MA, Bezabh AM. Husbands’ involvement in family planning use and its associated factors in pastoralist communities of Afar, Ethiopia. Reprod Health. 2019;16(1):33. doi:10.1186/s12978-019-0697-6
25. Bayray A. Assessment of male involvement in family planning use among men in south eastern zone of Tigray, Ethiopia. J Med. 2012;2:1–10.
26. Sagir T, Abubakar Panti A, Garba J, Funtua A, Chappa A, Markus M. Perception and acceptability of bilateral tubal ligation among women attending antenatal clinic at Usmanu Danfodiyo university teaching hospital Sokoto. Int J Reprod Contracept Obstet Gynecol. 2020;9:1636. doi:10.18203/2320-1770.ijrcog20201237
27. Stulberg DB, Hoffman Y, Dahlquist IH, Freedman LR. Tubal ligation in Catholic hospitals: a qualitative study of ob-gyns’ experiences. Contraception. 2014;90(4):422–428. doi:10.1016/j.contraception.2014.04.015
28. Anita P, Nzabona A, Tuyiragize R. Determinants of female sterilization method uptake among women of reproductive age group in Uganda. Contracept Reprod Med. 2020;5(1):25. doi:10.1186/s40834-020-00131-8
29. Mbugua KK Factors influencing uptake of bILATERAL tubal ligation among women who have completed family size in eastern and central provinces of Kenya. University of Nairobi; 2013.
30. Onifade OA, Adigun JO, Abikoye AI, Abiola OO, Aliyu S. Socio-cultural factors influencing choice of bilateral tubal ligation among women attending University of Ilorin teaching hospital. KIU J Soc Sci. 2017;3(1):37–46.
31. World Health Organistation. Female Sterilization: A Guide to Provision of Services. Geneva, Switzerland: World Health Orgnization; 1996.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.