")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 15
The Lived Experience of Primary Family Caregivers of Patients on Hemodialysis Treatment in Southern Ethiopia: A Phenomenological Study
Authors Abebe A , Arba A , Paulos K , Abera W, Sidamo T , Shiferaw S, Abraham Z, Baza D , Nega B, Woldeyohannes S
Received 19 December 2021
Accepted for publication 16 February 2022
Published 22 February 2022 Volume 2022:15 Pages 41—52
DOI https://doi.org/10.2147/IJNRD.S353191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Pravin Singhal
Amene Abebe,1 Aseb Arba,2 Kebreab Paulos,3 Wogayehu Abera,4 Temesgen Sidamo,5 Shimelis Shiferaw,6 Zinabu Abraham,7 Daniel Baza,2 Banchialem Nega,3 Selamawit Woldeyohannes1
1Department of Public Health, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 2Department of Nursing, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 3Department of Midwifery, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 4Department of Anaesthesia, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 5Department of Pharmacy, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 6Department of Medical Laboratory Science, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 7Department of Surgery, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Amene Abebe, Email [email protected]
Background: Primary family caregivers of hemodialysis patients are the “hidden patients” who shoulder extraordinary care burdens. However, there is a dearth of studies in Ethiopia. The purpose of this study was to explore the lived experience of primary family caregivers of hemodialysis patients in Southern Ethiopia.
Methods: Qualitative phenomenological study design was employed in February 2021. A homogeneous purposive sampling technique was applied to select study participants. An in-depth interview using an interview guide and field notes were used to collect the required data. All interviews were recorded using a digital audio recorder. Data coding was assisted by Open code software version 4.03. Inductive thematic analysis was used to develop the emerged themes and sub-themes using Colaizzi’s 1978 seven-step phenomenological analysis method. The themes and sub-themes are described in detail in the respective heading and sub-headings.
Results: A total of twelve participants were involved in the present study. Bio-psychological experience, socio-economic impact, and healthcare provider-primary family caregiver relationships are the major themes that emerged from the data. The emotional responses, coping mechanisms, consequences on the family caregivers’ health, care fatigue, lifestyle change, economic burden, impact on social responsibility, social support, the role of the primary family caregiver, and trust and confidence in the service providers are the sub-themes defining primary family caregivers caring experience.
Conclusion: In this study, emotional instabilities and reactions, care fatigue, distortion of caregiver’s health, multiple economic and social damages are the major challenges faced by primary family caregivers.
Keywords: caregiver, hemodialysis, lived experience, patient, primary family caregiver
Introduction
Chronic Kidney Disease (CKD) involves a gradual loss of kidneys capacity of filtering wastes and excess fluids from the blood.1 In addition to supportive care, dialysis or a kidney transplant is a medical intervention to sustain the life of CKD patients.2 Globally, CKD is an increasing public health concern with an estimated prevalence of 5–10% and an annual increase rate of 8%.3–7 Hemodialysis (HD) has been proved to be the most common treatment modality in End-Stage Kidney Disease (ESKD) and more than three million patients all around the world are undergoing HD annually.8,9
Patients on dialysis face psychological, social, economic, sexual, and medical problems.10–12 Thus, the burden of care such as family isolation, reduced social interaction, and disturbance of family relationships are imposed on the family caregivers. Because of these facts, eventually, family caregivers are forced to give up the treatment.6,13,14
Globally, an estimated 349 million people including patients with ESKD are care-dependent.15 Patients with ESKD depend on unpaid family caregivers for their self-care needs.14 Unlike developed countries, in low and middle-income countries, the caregiving process for HD patients is highly challenging.16,17 Family caregivers share more than 20 hours per week care burdens.18,19
In low and middle-income countries including Ethiopia, due to the shift of lifestyle and urbanization, and the increased prevalence and incidence of diabetes mellitus and hypertension the burden of CKD is alarmingly increasing.20,21 Even though in Ethiopia, approximately 40% of the population is under the age of 15 years and nearly 60% is under 24,22 it is one of the three countries (Ethiopia, Niger, and Rwanda) where deaths attributable to CKD was steadily increased in the last 20 years which disproves the linearity of demographic and epidemiologic transitions.23
In the Sub-Saharan Africa region including Ethiopia, even though many patients with CKD initiate HD treatment, because of an inability to pay for ongoing dialysis; up to 85% of the patients are forced to withdraw from the HD treatment.23 In Ethiopia, due to unavailability, inaccessibility, and unaffordability of HD treatment, shortage of healthcare infrastructure, and adequately trained health personnel, an unacceptably high burden of care is laid on the shoulders of family caregivers.16,24
Before WSU-TRH HD center began giving service, there were five HD centers in Ethiopia; three in Addis Ababa (Zewditu Memorial, Saint Paulo’s Millennium Medical College, Tikur Anbessa) hospitals and two in northern Ethiopia (Bahir Dar Felege Hiwot, and University of Gondar comprehensive specialized) hospital HD centers.16
The Ethiopian health policy emphasizes the prevention of communicable diseases and health promotion.24 CKD patients in Ethiopia in general and in the study setting in particular do not receive any subsidies either from the government or other charity organizations. Besides, in the existing health insurance system, the care and treatment cost of chronic diseases like CKD is not covered.16
Exploring the holistic experience of family caregivers of HD patients has a paramount significance for the effective, continued, and desirable patient outcome.25 However, it is left unknown adequately and the few studies available also focused on the patient side challenges.26–28 Therefore, this study aimed to assess the lived experience of primary family caregivers of patients on HD in Wolaita Sodo University Teaching and Referral Hospital (WSU-TRH), Southern Ethiopia.
Methods and Materials
Study Design, Period, and Setting
A health facility-based qualitative phenomenological study design was conducted in February 2021. Qualitative phenomenological research investigates individuals’ lived experience of events such as the caring experience of patients on HD treatment. It describes the essence of the real meaning of lived experience. According to the 2007 Ethiopian population and census report, the total population of the Southern region is around 14,929,548 which was projected to be 25,297,354 in 2020.29 This study was conducted in the WSU-TRH HD center, Southern Ethiopia. The Hospital is located in the eastern part of Wolaita Sodo City, the capital of Wolaita Zone. It is 330 km far from the Ethiopian capital city, Addis Ababa, in the Southern direction.
According to the information obtained from the hospital, WSU-TRH was established in 1927 as a district hospital, but now it is a teaching, referral hospital, and research institution. WSU-TRH provides curative and rehabilitative services to approximately 2.5 million people from Wolaita and neighboring Zones. The hospital has 374 beds and about 500 clients visit the hospital daily.
WSU-TRH is the only public HD center providing treatment for the population of the Southern and surrounding regions in Ethiopia. In the WSU-TRH HD center, approximately 12 CKD patients undergo hemodialysis daily but no documented evidence was found on the number of patients receiving HD nationally. Each patient in the WSU-TRH HD center receives two to three HD therapy per week and it costs about 5000 Ethiopian birrs for one session.
Participant Recruitment Procedure
Primary family caregivers of HD patients who provided care for at least 3 months were recruited for the study. Participants’ addresses, the duration of care, and the date of appointment for the next HD were obtained from the patients’ registration book. Based on the appointment date identified from the registration book, the patients were invited and negotiated to participate in the study. The place, date, and time of the interview were established with those who are a volunteer for participation. Owing to the time lapse between the invitation to participate and the negotiated date and time for the actual interview, all of the participants in the latter stages of the study were asked if they are still willing to be part of the study. Informed written consent was obtained from each of the participants before the interview. All participants who had initially consented to participate in the study were included.
Sample Size and Sampling Procedure
Twelve primary family caregivers for HD patients have participated in this study. A homogeneous purposive sampling technique was used to select the study participants. Caregivers who are registered as primary family caregiver, who has been caring for at least six months before the study, and are willing to participate were purposely selected. Initial estimation of the required sample size was determined by considering the experience of previous literature, recommendations of qualitative research books, and the phenomena of interest.30–32 However, information saturation was used as an indicator for the termination of further inclusion of participants. Selection continued to the point of redundancy, until new codes, sub-themes, or themes and explanations stop emerging from the data.
Data Collection Tools and Procedures
The required data were collected by the researchers. The researchers were trained, experienced, and certified in qualitative research methods. A semi-structured In-Depth Interview (IDI) guide with open-ended questions and supportive field notes were used to collect rich data in participants’ expressions and language. The IDI guide was used to maintain the sequence and flow of ideas and to stick to the aim of the study during interview sessions “Supplementary Material” Section 1. The interview was conducted at WSU-TRH. The private room was used to facilitate one-on-one communication. Probing was used to ensure the depth and clarification of the information provided during the interview. Further interviews were terminated when information saturation is achieved. All interviews were audiotaped and lasted on average 30 minutes.
Data Quality Management and Analysis
There are three possible methods for descriptive phenomenological data analysis in qualitative studies which include Colaizzi (1978), Giorgi (1985), and Van Kaam (1966). The basic outcome of all three methods is the description of the meaning of an experience. Colaizzi’s (1978) method, however, is the only one that calls for validation of results by returning to the study participants.31 To take this advantage, in the current study, Colaizzi’s (1978) seven-step phenomenological data analysis method was applied. After repeatedly listening to the audio-recorded data, audio transcripts were converted to text transcripts in the Amharic language. The text transcripts were translated to the English language for analysis by the researchers. Reading, and re-reading of the transcription and field notes were conducted to be familiarized with the data. The transcripts and field notes were converted into a rich text file and prepared to be imported into open code software. Data coding and management were assisted by using Open Code Software Version 4.03. Following the inductive thematic analysis approach themes and sub-themes emerged from the data. The potential themes and sub-themes were critically reviewed by the researchers and the finally agreed themes and sub-themes were developed “Supplementary Material” Section 3. The themes and sub-themes were compared with the codes and the data to check whether they appropriately represent the data.
Trustworthiness of the Study Findings
To ensure the rigor of the study, credibility, transferability, dependability, and conformability were maintained.
Credibility: recorded audio data and field notes, copies were kept safe and used as reference materials. Information validation was done by asking questions in different ways and cross-checking interview data with data from the patient registration book. Peer-debriefing was done with a similar status colleague who is out of the context of the study. Copy of the transcribed text and distribution of preliminary findings to study participants was conducted to check for any inconsistencies. All the participants provided with the preliminary findings confirmed all the themes and ideas listed were congruent with their lived experience.
Transferability of the findings: purposive selection of the study area and participants was done. A clear method of participant recruitment was employed to improve the transferability of the findings in similar settings and contexts. Direct verbatim quotations were used to explain the emergent themes.
Dependability: research design and implementation, methods, and approaches of data collection and reflective appraisal were clearly described to ensure the consistency of the study.
Confirmability: to ensure confirmability of the findings, a peer auditor was included to audit the process and product of the study. Preconceived beliefs and opinions about the phenomenon under scrutiny were held with abeyance.
Definition of Terms
Caregiving: is any help that may be in the form of aid and assistance provided to persons in need.33
Caregiver burden: is the physical, financial, and psycho-social hardships of caring for a loved one, usually for a family member struggling with a health problem.34
Family caregivers: are persons being responsible for the care of their patients without receiving any money.19
Primary family caregivers: are people who are registered and identified by the patient as being primary caregivers in the home and health facility setting.35
Phenomenology: is a philosophical discipline introduced by Edmund Husserl that deals with a direct investigation and description of phenomena.36
Results
Socio-Demographic Profile of the Study Participants
A total of 12 study participants with a mean age of 35.4 and an average family size of 6.4 participated in the study. The majority, 9 (75%) of the participants were females. As to the occupational status of participants, six (50%) government employees, 3 (25%) housewives, one farmer, one unemployed, and one student, and 8 (67%) were married. More than half, seven (58%) of the participants were protestant Christianity followers, 3 (25%) were Orthodox Christians and the remaining one is Islam religion followers. Regarding the duration of HD, it ranges from 6 months to 18 months “Table 1”.
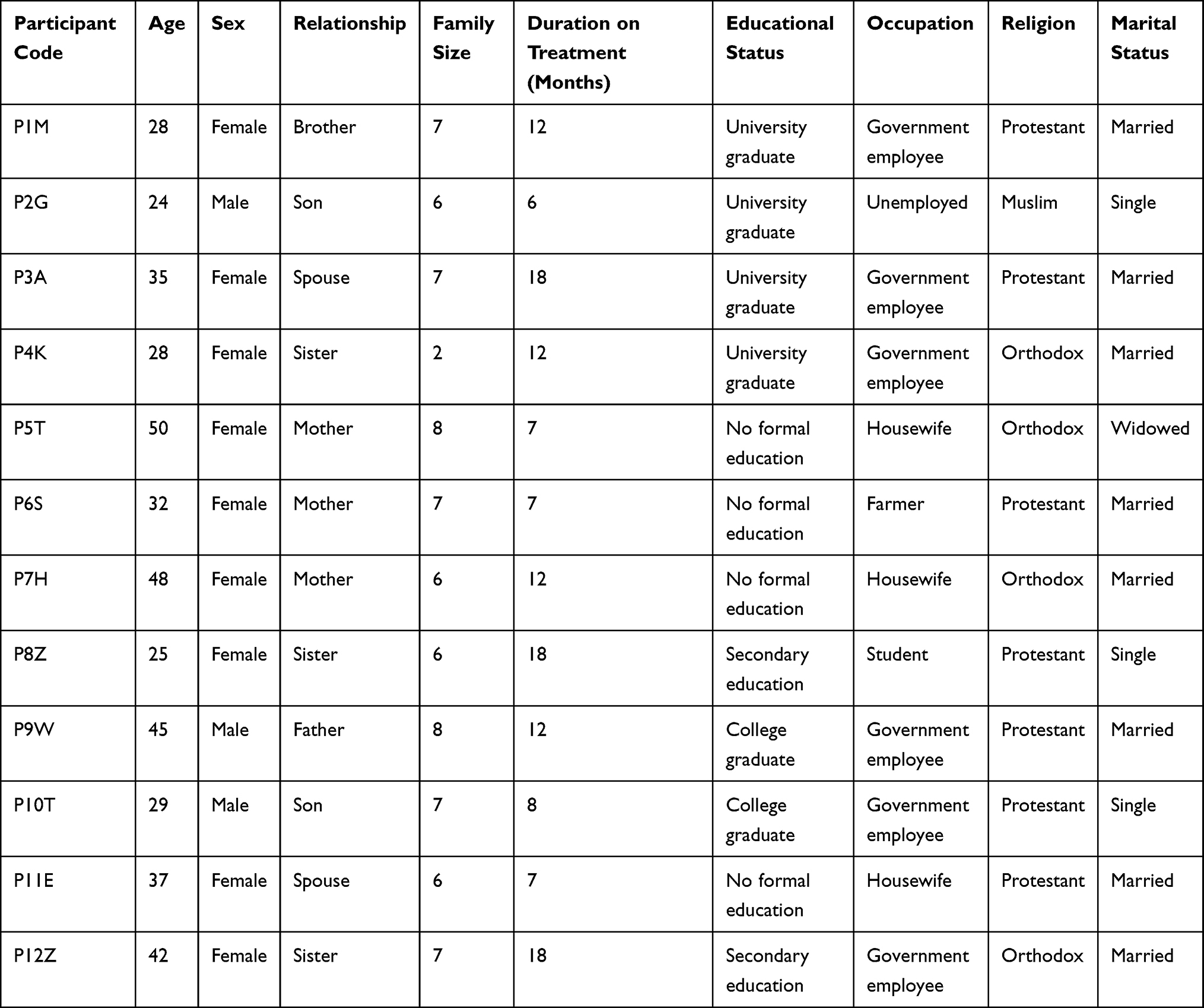 |
Table 1 Socio-Demographic Profile of Primary Family Caregivers Wolaita Sodo University Hemodialysis Centre, February 2021 |
In the current study, three major themes and ten sub-themes emerge from the data. The three major themes include bio-psychological experience, socio-economic impact, and healthcare provider-primary family caregiver relationships. The ten sub-themes identified are emotional responses, coping mechanisms, consequences on the family caregivers’ health, care fatigue, lifestyle change, economic burden, impact on social responsibility, social support, the role of the primary family caregiver, and trust and confidence in the service provision. All of the reported results are derived inductively from the study participant’s responses “Table 2”.
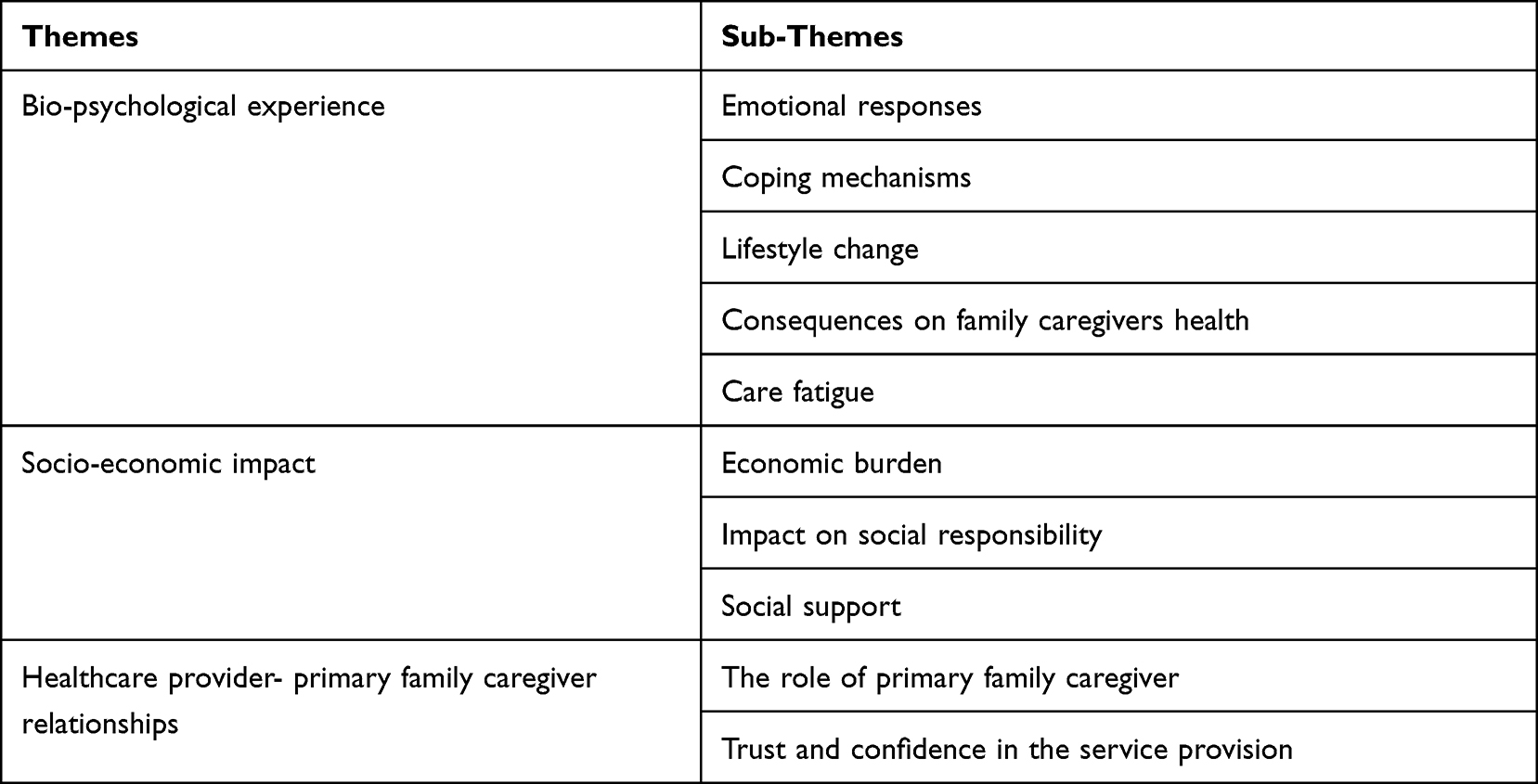 |
Table 2 The Themes and Sub-Themes Developed from the Data, February 2021 |
Theme One: Bio-Psychological Experience
Bio-psychological experience is the first major theme inductively developed from the participant responses. This theme developed from participant responses that explain attributes related to the biological and psychological impact of the HD on the family caregivers. The theme is comprised of five basic sub-themes which include emotional responses, coping mechanisms, consequences on family caregivers’ health, care fatigue, and lifestyle change.
Sub-Theme One: Emotional Responses
This sub-theme is developed from participant responses related to their emotional reactions at the moment when the decision to begin HD was disclosed and in the continuum of the caregiving process. Participants of this study expressed their emotional responses in various ways. The emotional responses identified during data analysis include crying, confusion, denial, hopelessness, fear, frustration, yelling, the anticipation of misfortune, and emotional lability. This notion is well explained by a 28-year-old female primary family caregiver who was caring for her brother in the following ways:
It was very difficult to accept. I was almost near to faint, he is the only brother for me, no other brothers. Previously, I heard the presence of HD treatment for kidney patients. However, I did not expect it would happen in my family. When I heard about it, I could not accept and I felt like my world is falling apart. In addition to that, I did not expect he would be alive any longer, I anticipated he would die immediately. I do not have words to explain the feeling at that moment. I think you can imagine, how much difficult it is, for someone who visited the health facility just for a headache and without prior illness when told his both kidneys are no more functional. Psychologically, it hurt us badly, both me and him. P1M
Sub-Theme Two: Coping Mechanisms
Faith in God and prayers for healing, talking and sharing the patient’s condition and the challenges to their friends, relatives, healthcare workers, colleagues, and talking to self were the participants coping mechanisms identified in this study. A verbatim quotation obtained from a 24-year-old male participant who was a primary family caregiver for his father well explains this result in the following manner:
I did not tell my father’s condition for anybody else at the moment I heard as he is going to receive HD treatment other than to God; neither could I tell other people because I was in distress. I just talked to God inside, even with no voice, because I believe God understand what I wanted to tell him. P2G
Additionally, a 35-year-old woman primary family caregiver for her husband mentioned that she discussed the challenges with her family members. This idea is well expressed in the following verbatim quotation received from her:
We have been talking about his condition in our home. We discussed this with my elder brother and family. P3A
Sub-Theme Three: Lifestyle Change
Lifestyle change is a new and challenging form of way of life which the participants were forced to assume due to a highly burdensome patient care role. Being cautious about their health and changes in their perspectives or outlook on the renal disease were among the mentioned lifestyle changes. A 25-year-old female participant explained this result in the following manner:
Previously I do not have an idea about kidney disease. I realized how much kidney disease is a serious problem only after my brother became ill with it. After the assessment of my brother’s health status, the healthcare workers told him that his both kidneys were failed. Eventually, we continued with the HD treatment and I have come to realize that it is impossible to know how much your kidney may be affected in normal life. The healthcare workers said that the “kidneys can function normally until 25% of the kidney is unaffected”. This means you cannot know before your kidneys are damaged permanently and become a serious health threat. P8Z
The data also shows that being the primary family caregiver of the patient on HD alarmed them to think about their renal status and lifestyle modifications. In this regard, lifestyle changes identified include engagement of the participants in preventive activities such as physical exercises, making renal function tests, changes in feeding and drinking habits. This view is captured in the following excerpt from a 29-year-old male study participant:
After I observed my father is undergoing HD treatment and unbearable suffering from the disease, my view of kidney health has changed. I have come to know that like hypertension and diabetes mellitus, kidney failure also may be inherited genetically. Hence, I decided to prevent the risk by doing preventive activities and modifying my eating and drinking habits, I begin working out with regular exercise. P10T
This study also identified that the self-care practices of the primary family caregivers had been distorted after they assume the patient caring duty. Personal hygiene, dressing, meal, and drinking habits were affected. A 45-year-old primary family caregiver who was caring for his son explained this concept in the following manner:
The caring responsibility for HD patients demands shifting your previous lifestyle. When someone enters into this situation, he would no longer think about himself. For instance, I do not eat meals adequately and regularly, I do not know how I dressed and I do not think or I do not have time to keep my hygiene. P9W
Sub-Theme Four: Consequences on Family Caregivers Health
According to this study, the health status of the participants was compromised after they assume the caring duty. The health and related problems identified in the study include infections, admissions, frequent visits to a health facility, and feeling sick with/without treatment. A 37-year- old female primary family caregiver stated this view in the following ways:
Because of my husband’s illness, on many occasions, I spent several sleepless nights just sitting or standing. As a result, I became sick. Recently, even I felt pain and abnormality in my kidneys. The pain in my neck because of a tumor is also being aggravated since I began caring for him. I got treatment before 8 years and I was better after the treatment, but now it seems my neck pain is relapsing. P11E
Sub-Theme Five: Care Fatigue
This sub-theme is developed from the data referring to the physical and emotional exhaustion that primary family caregivers experience in the continuum of care. The caregivers run out of energy or motivation to continue with the treatment as a result of drained resources in terms of cash and kind/assets like land, house, cattle, and so on. The most common experience of care fatigue identified in the data includes chronic exhaustion of emotional and physical capacity, reduced feeling of sympathy or empathy, anxiety, insomnia, not eating well, anorexia, poor work and life balance, diminished sense of career fulfillment, and so forth. For instance, the following verbatim quotation taken from a 28- year-old female participant well explains this notion:
Today, I told the health professionals regarding our family’s inability to continue with the treatment. I bought all prescribed medications for today’s treatment but I told them this episode is the last session. Then the health care professionals replied, if you are not able to continue with the treatment, we can do nothing, it is up to you to decide. But, we will show you what will happen and the fate of the patient. You will put your signature on against medical advice form and you can terminate the treatment. When they say this, I had no words to reply, rather I kept silent, and I said to myself, I will not get him back if he dies once, so I promised to myself to pay whatever sacrifice and to bring him for the treatment back but I do not know where to go. I do not know the end date of the treatment which always makes me sick and hopeless. P4K
Theme Two: Socio-Economic Impact
The long-term caring process of patients on HD treatment caused multiple social and economic damages to the caregivers and their families. This theme is comprised of three basic sub-themes which include: economic burden, social support, and impact on social responsibility.
Sub-Theme One: Economic Burden
HD is palliative care for which the caregiver is expected to pay per session. It is an economically deranging treatment modality that affects the overall life status of the caregivers and overall family. The economic burden identified were loss of financial capability and other assets like loss of job due to absenteeism, inability to pay school fees for self and children, incapacity to purchase essential household consumables like food items, cloth, sanitary equipment, inability to pay for house rent, selling house and farmland, and dependency and seeking support from others. This result is well captured by a 48-year-old woman who was a primary family caregiver of her son in the following ways:
Currently, I and my family are facing unbearable economic challenges. It is now one year since we began HD treatment for my son. I do not have money, let alone to pay for the HD treatment which costs approximately 4000 ETB (Ethiopian Birr) in one session, I cannot pay transportation and food costs. He has been ordered to get two HD sessions per week. Imagine how costly it is. We have exploited all options of money for the treatment. We had land which we inherited from our late parents but now we sold it. We already have finished everything we have had. We can no more afford the treatment, we are now planning how to terminate the treatment. P7H
Sub-Theme Two: Social Support
Several participants mentioned that they lacked social support. Participants specifically expected financial, psycho-social, and moral supports. The expected sources of social support were individuals and organizations like churches, relatives, volunteers, colleagues, support groups like non-government organizations, and/or government organizations. However, they are not getting any support that they desperately desire and deserve to get it. The participants specifically expected financial, psychological, and moral empathy from individuals and organizations which match their situation. Even though they get some pity support from their relatives and friends but not get any support that can resolve the challenges. For instance, a 35- year- old woman who was a primary caregiver for her husband stated the above result as follows:
We are not getting any support that matches the situation currently we are encountering. Our kids are not yet grown and cannot support me. The whole burden is laid upon me. Initially, our friends and families were providing us moral and spiritual support but now it has ceased. Because they are exhausted. We do not blame them for doing so, since we understand that our situation is challenging and it is not known when it comes to an end. It is a year and a half since the treatment began, I exploited all the resources we have and I no longer afford the cost of the treatment. For the current session, I got the money from his mother. She sold her single dairy cow and offered it for his treatment. When I think about the fate of his mother, it also disturbs me, because her source of income is from the dairy products of that cow. P3A
Sub-Theme Three: Impact on Social Responsibility
Social responsibilities such as attending churches, Edir and Epub (local social organizations), funeral service, wedding service, and spending time with neighbors, engaging in local ceremonies and the works, and taking care of other members of the families had been jeopardized due to the burden of care of the HD patient. This concept was well explained by a 50-year-old woman who was a primary family caregiver of her son in the following ways:
It is too difficult to take additional responsibilities rather than caring for him. For example, whenever I bring him to the center, I begin the journey early in the morning and stay the whole day with him there. I do not have time to care for other members of the family. I have children but I do not have time to look after them. It has also affected my job, I left all my jobs, my entire life became caring for him. Previously, we had Edir (a local social organization) in 3 places but now I quit 2 of them. The leaders tried to convince me not to quit but as I see my current situation, let alone three, I cannot afford the one. P5T
Theme 3: Healthcare Provider- Primary Family Caregiver Relationship
To be successful with the caring responsibility and attain a desirable patient outcome, both the role of the family caregivers and the healthcare workers is required to be smooth. In this regard, the role of primary family caregivers and trust and confidence in the service providers were the sub-themes identified.
Sub-Theme One: The Role of Primary Family Caregivers
The roles and responsibilities known in the data include assisting the patient in travels (taking and bringing) from the center, assisting the patient when he/she receive medications, making payments and searching for additional financial sources, buying prescribed drugs, feeding and providing basic cares such as bath, oral, and hair care. A verbatim quotation obtained from a 42-year-old woman who was a primary family caregiver for her brother well describes this result:
As a primary caregiver for my brother, I have many responsibilities. For example, during his hospital stay, I go to the bank and withdraw money, make payments for his medical expenses and closely follow the HD central catheter. When we go back to our home, I make different home cares; you know he cannot eat all food we eat, when I buy a foodstuff, I select items which are suitable for him. In addition to that, I make hair care, give him a bed bath, make his bed and keep his oral hygiene. Besides, comforting him. Even my father even do not know from where the money comes for the treatment. P12Z
Sub-Theme Two: Trust and Confidence in the Service Provision
Trust and confidence in the healthcare institution, professionals, and service delivery system are enabling factors for the continuity of patient care. The caregiver’s trust and confidence in the healthcare service dimensions such as counseling, prescriptions, empathy, HD procedure, and satisfaction with the overall service were stated in the data. This notion is well captured in the following verbatim quotation received from a 32-year-old woman who was a primary family caregiver for her daughter as follows:
In this center, I can say, they (healthcare workers) are the reason for the continuity of the life of my daughter apart from God. They went beyond their responsibility to support us. Previously, I stopped the treatment but I continued it again. When something falls short, they do their best to fill the gap and render their compassionate care at any cost. P6S
Another male study participant of age 29-year-old who is a primary family caregiver for his son further strengthened the above result in the following ways:
The health status of anyone who receives the treatment in this center (Wolaita Sodo University Hospital, dialysis center), improves faster and can go for his routine activities earlier than expected. The healthcare professionals in this center are very compassionate and respectful. For instance, one day, I asked them whether I could stop the HD treatment because I could not afford the cost and they told me in detail what will happen to my son if I decide to stop. I did not ask them anymore because I trusted them and they are experienced in treating patients next to God. P10T
Discussion
This study tried to explore the extremely burdensome experience of primary family caregivers caring for patients on HD in WSU-TRH, Southern Ethiopia. In the current study, three major themes and ten sub-themes emerge from the data. The three major themes include bio-psychological experience, socio-economic impact, and healthcare provider-primary family caregiver relationships. The ten sub-themes identified were emotional responses, coping mechanisms, consequences on the family caregivers’ health, care fatigue, lifestyle change, economic burden, impact on social responsibility, social support, the role of the primary family caregiver, and trust and confidence in the service provision.
Results of this study revealed that emotional instabilities and reactions are common experiences among primary family caregivers of a patient on HD. The identified emotional responses include crying, confusion, denial, hopelessness, fear, frustration, yelling, and anticipation of misfortune. This finding is consistent with the results of similar studies done in Iran, Greece, and Saudi Arabia where family caregivers of HD patients were prone to a variety of psycho-social and emotional responses.5,10,13,37
In the current study, the coping mechanisms were mainly based on talking either to important others or self. Talking and sharing the patient’s status and the challenges to friends, relatives, healthcare workers, colleagues, and talking to self were among the coping mechanisms primary caregivers experienced. This result is not similar to the study report done in Britain where the coping mechanism to caregiving stress was mainly based on individualized actions such as distraction of attention with other activities, mental stimulation with leisure activities such as physical exercise or reading books, emotional release by either crying or dancing, looking for the positive aspects of caregiving, and disengaging from stressful thoughts.38 The difference might be due to socio-cultural variation and the patient’s medical character.
The current study also shows that most of the participants have a strong religious foundation. They believe that the treatment they are obtaining from HD center was blessing of the medical technology. Because HD helped them to see their loved ones alive. Several other participants expressed that the unbearable suffering due to the endless HD treatment and supportive care burden was a punishment for their sin and hopelessly accept God’s decision. This finding is corroborated by another similar study in northwest Ethiopia where religion and spirituality were reported as both the blessing and punishment.39
According to this study, the caregiving role of the participants alarmed them to make many health promotive and disease preventive lifestyle changes. The lifestyle changes identified include changes in the perspectives or outlook on renal disease, engagement in preventive activities such as physical exercises, making renal function tests, changes in feeding and drinking habits. This result is not mentioned in other similar studies where giving care for a HD patient is reported as only burdensome which distorts the caregivers habituated self-care practices such as personal hygiene, dressing, meal, and drinking habits.8,10,25,37
The economic burden identified in the recent study includes loss of financial capability and other assets like loss of job due to absenteeism, inability to pay school fees for self and children, incapacity to purchase essential household consumables like food items, cloth, sanitary equipment, inability to pay for house rent, selling house and farmland, and dependency and seeking support from others. This finding is supported by studies done in Iran, Jordan, Saudi Arabia, Nigeria, and Ethiopia.10,13,16,37,40
Most of the participants expressed that they have decreased frequency of treatment appointments. Eventually they planned to terminate treatment due to financial hardships to cover the treatment costs. A similar result was reported in the global burden of diseases study where the patients with CKD in the low and middle-income countries particularly in Sub-Saharan Africa initiate HD treatment but 85% of patients are forced to withdraw from this life-sustaining treatment.23
The long-term care of the patient on HD leads to a lack of social support and an inability to fulfill social responsibilities. The results of this study show that the caregivers are not getting any financial, psycho-social, and moral supports that match their situation from individuals and/or organizations. This result is also reported similarly in other studies done in Ethiopia and Nigeria.16,40 This finding is contrasting to the study reports from developed countries where the government and other organizations provide financial and other needed social support.38,41,42
The present study confirmed that social responsibilities such as attending churches, Edir and Epub (local social organizations), funeral service, wedding service, spending time with neighbors, engaging in local ceremonies and their jobs, and taking care of their families had been jeopardized due to burden of care. This result is corroborated by the study findings from Nigeria and the USA where the study reported that family caregivers were caught in between competing social responsibilities.40,43
The success and desired treatment outcome of the patient depends on the smooth relationship between family caregivers and the treatment team. This study verified that the primary family caregivers and the treatment team of the hospital are effectively executing their roles and responsibilities. This finding is in line with the study finding done in Iran where the study reports the healthcare teams doing their duties based on defined job descriptions enhances confidence and trust of family caregivers. Thus, it eases the burden of care for the family caregivers and promotes the care process.44
Strengths of the Study
In this study, data collection, analysis, and interpretation are guided by the emergence of ideas from the data but not on preconceived information. An open and emerging approach was followed. Face-to-face interaction with participants was used to capture important non-verbal cues.
Limitations of the Study
Though the study quite surely achieved the study objectives, it has some general and specific limitations. Since this study is used a purposely selected small sample size, the generalizability of the findings to other larger populations is not possible and the aim of the study. Translation of the data to English for analysis and write-up might have introduced deviation in some contextual expressions of the participants.
Conclusion
Primary family caregivers are experiencing extraordinary care burdens due to prolonged and demanding caring responsibility for HD patients. This study disclosed that emotional instabilities and reactions, care fatigue, distortion of caregiver’s health, multiple economic and social damages are the major obstacles faced by primary family caregivers. Therefore, free professional psycho-social counseling and health care services provision, reduction of cost of HD and medications through health insurance coverage and/or involving charity organizations, strengthening assistance of significant others like families and friends, expansion of HD treatment centers, and free transportation, accommodation, and food service for primary family caregivers are recommended.
Abbreviations
CKD, Chronic Kidney Disease; HD, Hemodialysis; IDI, In-depth Interview; WSU-TRH, Wolaita Sodo University Teaching and Referral Hospital.
Data Sharing Statement
The dataset analyzed for the findings of this particular study is available with the corresponding author and can be accessed upon reasonable request.
Ethical Considerations
Ethical clearance was obtained from the Institutional Review Board of Wolaita Sodo University College of Health Science and Medicine. The necessary communication was made with respective WSU-TRH administrative bodies. Before data collection, the nature of the study, its relevance, and participant rights were explained to the study participants. The willingness of participants was asked before conducting the interview. Informed written consent was obtained from each participant before data collection “Supplementary Material” Section 2. To ensure confidentiality, participants’ data and each verbatim quotation are described using codes.
Acknowledgment
Our gratitude goes to the WSU-TRH administrative bodies, study participants, and clinical staff of the WSU-TRH HD center for their irreplaceable contributions to the successful completion of the study.
Author Contributions
All authors equally contributed to this work beginning from the conception, study design, execution, acquisition of data, analysis, and interpretation. Authors of this work took part in the drafting, revising, and/or critically reviewing of the article and finally agreed on the journal to which the article was submitted. All authors are also reviewed and agreed on all versions of the article before submission, during revision, and the final version is accepted for publication and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Mayo C. Chronic kidney disease; 1998–2022.
2. California Uo. Chronic Kidney Disease (CKD). Clinical practice recommendations for primary care physicians and healthcare providers. Divisions of nephrology & hypertension and general internal medicine; 2011.
3. Alebiosu CO, Ayodele OE. The global burden of chronic kidney disease and the way forward. Ethn Dis. 2005;15(3):418–423.
4. Al-Shdaifat EA, Manaf MR. The economic burden of hemodialysis in Jordan. Indian J Med Sci. 2013;67(5–6):103–116. doi:10.4103/0019-5359.122734
5. Hawamdeh S, Almari AM, Almutairi AS, Dator WLT. Determinants and prevalence of depression in patients with chronic renal disease, and their caregivers. Int J Nephrol Renovasc Dis. 2017;10:183–189. doi:10.2147/IJNRD.S139652
6. Shahgholian N, Yousefi H. Supporting hemodialysis patients: a phenomenological study. Iran J Nurs Midwifery Res. 2015;20(5):626–633. doi:10.4103/1735-9066.164514
7. Nobahar M, Tamadon MR. Barriers to and facilitators of care for hemodialysis patients; a qualitative study. J Ren Inj Prev. 2016;5(1):39–44. doi:10.15171/jrip.2016.09
8. Griva K, Li ZH, Lai AY, Choong MC, Foo MWY. Perspectives of patients, families, and health care professionals on decision-making about dialysis modality–the good, the bad, and the misunderstandings! Perit Dial Int. 2013;33(3):280–289. doi:10.3747/pdi.2011.00308
9. Shaw C, Pruthi R, Pitcher D, Fogarty D. UK renal registry 15th annual report: chapter 2 UK RRT prevalence in 2011: national and centre-specific analyses. Nephron Clin Pract. 2013;123(Suppl. 1):29–54. doi:10.1159/000353321
10. Salehitali S, Ahmadi F, Hasanpour Dehkordi A, Noorian K, Fereidooni-Moghadam M, Zarea K. Progressive exhaustion: a qualitative study on the experiences of Iranian family caregivers regarding patients undergoing hemodialysis. Int J Nurs Sci. 2018;5(2):193–200. doi:10.1016/j.ijnss.2018.01.005
11. Fredman L, Cauley JA, Hochberg M, Ensrud KE, Doros G; For the study of osteoporotic F. Mortality associated with caregiving, general stress, and caregiving-related stress in elderly women: results of caregiver-study of osteoporotic fractures. J Am Geriatr Soc. 2010;58(5):937–943. doi:10.1111/j.1532-5415.2010.02808.x
12. Khaira A, Mahajan S, Khatri P, Bhowmik D, Gupta S, Agarwal SK. Depression and marital dissatisfaction among Indian hemodialysis patients and their spouses: a cross-sectional Study. Ren Fail. 2012;34(3):316–322. doi:10.3109/0886022X.2011.647291
13. Alnazly EK. Burden and coping strategies among Jordanian caregivers of patients undergoing hemodialysis. Hemodial Int. 2016;20(1):84–93. doi:10.1111/hdi.12318
14. Suri RS, Larive B, Garg AX, et al. Burden on caregivers as perceived by hemodialysis patients in the Frequent Hemodialysis Network (FHN) trials. Nephrol Dial Transplant. 2011;26(7):2316–2322. doi:10.1093/ndt/gfr007
15. WHO. Integrated care for older people (ICOPE). Guidelines on community-level interventions to manage declines in intrinsic capacity Evidence profile: caregiver support; 2017.
16. Kassa D, Abebe S, Kebede A, Gebremedhin T. Cost of hemodialysis treatment and associated factors among end-stage renal disease patients at the tertiary hospitals of Addis Ababa City and Amhara Region, Ethiopia. Clinicoecon Outcomes Res. 2020;12:399–409. doi:10.2147/CEOR.S256947
17. Okafor C, Kankam C. Future options for the management of chronic kidney disease in Nigeria. Gend Med. 2012;9(1):S86–93. doi:10.1016/j.genm.2011.10.002
18. Lin IF, Fee HR, Wu H-S. Negative and positive caregiving experiences: a closer look at the intersection of gender and relatioships. Fam Relat. 2012;61(2):343–358. doi:10.1111/j.1741-3729.2011.00692.x
19. Caqueo-Urízar A, Gutiérrez-Maldonado J, Miranda-Castillo C. Quality of life in caregivers of patients with schizophrenia: a literature review. Health Qual Life Outcomes. 2009;7(1):84. doi:10.1186/1477-7525-7-84
20. Xie Y, Bowe B, Mokdad AH, et al. Analysis of the Global Burden of Disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int. 2018;94(3):567–581. doi:10.1016/j.kint.2018.04.011
21. Tolossa T, Fetensa G, Regassa B, et al. Burden and determinants of chronic kidney disease among diabetic patients in Ethiopia: a systematic review and meta-analysis. Public Health Rev. 2021;42(3). doi:10.3389/phrs.2021.1603969.
22. Mundi I. Ethiopia demographics profile; 2021.
23. Bikbov B, Purcell CA, Levey AS, et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020;395(10225):709–733. doi:10.1016/S0140-6736(20)30045-3
24. Tuso PJ. SERVE Ethiopia. Perm J. 2009;13(3):51–64. doi:10.7812/TPP/08-082
25. Eslami AA, Rabiei L, Shirani M, Masoudi R. Dedication in caring of hemodialysis patients: perspectives and experiences of Iranian family caregivers. Indian J Palliat Care. 2018;24(4):486–490. doi:10.4103/IJPC.IJPC_204_17
26. Low J, Smith G, Burns A, Jones L. The impact of end-stage kidney disease (ESKD) on close persons: a literature review. NDT Plus. 2008;1(2):67–79. doi:10.1093/ndtplus/sfm046
27. Cook WL, Jassal SV. Functional dependencies among the elderly on hemodialysis. Kidney Int. 2008;73(11):1289–1295. doi:10.1038/ki.2008.62
28. Mashayekhi F, Pilevarzadeh M, Rafati F. The assessment of caregiver burden in caregivers of hemodialysis patients. Mater Sociomed. 2015;27(5):333–336. doi:10.5455/msm.2015.27.333-336
29. Agency CS. Population and housing census of Ethiopia: statistical report for Southern Nations, Nationalities and Peoples’ Region; 2007.
30. JW C. Research Design: Qualitative, Quantitative and Mixed Methods Approaches.
31. Polit DF, Beck CT. Nursing Research – Generating and Assessing Evidence for Nursing Practice.
32. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. 2018;18(1):148–166. doi:10.1186/s12874-018-0594-7
33. Brown RM, Brown SL. Informal caregiving: a reappraisal of effects on caregivers. Soc Issues Policy Rev. 2014;8(1):74–102. doi:10.1111/sipr.12002
34. Garlo K, O’Leary JR, Van Ness PH, Fried TR. Burden in caregivers of older adults with advanced illness. J Am Geriatr Soc. 2010;58(12):2315–2322. doi:10.1111/j.1532-5415.2010.03177.x
35. Lobchuk MM, Kristjanson L, Degner L, Blood P, Sloan JA. Perceptions of symptom distress in lung cancer patients: i. Congruence between patients and primary family caregivers. J Pain Symptom Manage. 1997;14(3):136–146. doi:10.1016/S0885-3924(97)00022-5
36. R-N K$. “Edmund Husserl ’ s theory of image consciousness, aesthetic consciousness, and art; 2014.
37. Eirini G, Georgia G. Caregivers of patients on haemodialysis. Caregiving Home Care. 2017;14:75.
38. Epiphaniou E, Hamilton D, Bridger S, et al. Adjusting to the caregiving role: the importance of coping and support. Int J Palliat Nurs. 2012;18(11):541–545. doi:10.12968/ijpn.2012.18.11.541
39. Tadesse H, Gutema H, Wasihun Y, et al. Lived experiences of patients with chronic kidney disease receiving hemodialysis in Felege Hiwot comprehensive specialized hospital, Northwest Ethiopia. Int J Nephrol. 2021;2021:6637272. doi:10.1155/2021/6637272
40. Oyegbile YO, Brysiewicz P. Exploring caregiver burden experienced by family caregivers of patients with end-stage renal disease in Nigeria. Int J Afr Nurs Sci. 2017;7:136–143. doi:10.1016/j.ijans.2017.11.005
41. Northouse LL, Katapodi MC, Schafenacker AM, Weiss D. The impact of caregiving on the psychological well-being of family caregivers and cancer patients. Semin Oncol Nurs. 2012;28(4):236–245. doi:10.1016/j.soncn.2012.09.006
42. Cohen LM, Germain MJ. Caregiver burden and hemodialysis. Clin J Am Soc Nephrol. 2014;9(5):840–842. doi:10.2215/CJN.02690314
43. Byrd J, Spencer SM, Goins RT. Differences in caregiving: does residence matter? J Appl Gerontol. 2010;30(4):407–421. doi:10.1177/0733464810371098
44. Salehitali S, Ahmadi F, Zarea K, Fereidooni-Moghadam M. The role of heath team in coping process of family caregivers with patients under hemodialysis: a qualitative study. Jundishapur J Chronic Dis Care. 2018;7(1):e63304.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.