")
Back to Journals » Journal of Inflammation Research » Volume 16
The Levels of Anti-SARS-CoV-2 Spike Protein IgG Antibodies Before and After the Third Dose of Vaccination Against COVID-19
Authors Łysek-Gładysińska M, Starz M, Borowiec-Sęk A, Sufin I, Wieczorek A, Chrapek M , Zarębska-Michaluk D , Sufin P, Głuszek S , Adamus-Białek W
Received 3 November 2022
Accepted for publication 21 December 2022
Published 11 January 2023 Volume 2023:16 Pages 145—160
DOI https://doi.org/10.2147/JIR.S394760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Adam D Bachstetter
Małgorzata Łysek-Gładysińska,1 Magdalena Starz,2 Agnieszka Borowiec-Sęk,2 Iwona Sufin,2 Anna Wieczorek,1 Magdalena Chrapek,3 Dorota Zarębska-Michaluk,4 Patrycja Sufin,2 Stanisław Głuszek,4 Wioletta Adamus-Białek4
1Institute of Biology, Jan Kochanowski University, Kielce, Poland; 2Meduniv Sp. z o.o, Kielce, Poland; 3Department of Mathematics, Jan Kochanowski University, Kielce, Poland; 4Institute of Medical Sciences, Jan Kochanowski University, Kielce, Poland
Correspondence: Wioletta Adamus-Białek, Jan Kochanowski University, Institute of Medical Sciences, IX Wieków Kielc 19a, Kielce, 25-516, Poland, Tel +48 788 860 604, Email [email protected]
Purpose: The COVID-19 pandemic has been going on for almost three years, and so far, many preventive and therapeutic strategies have been developed. The issue of subsequent booster vaccinations is currently being discussed. We aimed to analyze how the third dose of vaccination against COVID-19 correlates with the dynamics of IgG anti-SARS-CoV-2 spike protein antibody levels in a group of healthy people.
Patients and Methods: The prospective study included 93 participants before and after a second booster of COVID-19 vaccination, from whom 4 blood samples were collected at intervals. The levels of IgG anti-SARS-CoV-2 in serum were identified using the chemiluminescent immunoassay specific for the receptor-binding domain (RBD) of the S1 protein. The analysis of the results was performed using appropriate statistical methods, considering p < 0.05 as a statistically significant value.
Results: The IgG levels were significantly higher and less diverse after the same follow-up time from the second booster vaccination compared to the first booster. The antibody levels were positively correlated with female, healthcare workers, the elderly and participants with a negative COVID-19 history. Furthermore, the increase in IgG antibodies after the second booster vaccination correlated inversely with the baseline level of antibodies before the vaccination. The latest results showed that antibody levels dropped 1.5-fold after approx. 10 months from the second booster vaccination but still remained at a protective level.
Conclusion: Booster vaccinations seem to better stimulate immune memory, and in the case of borderline IgG level induces the greatest increase in antibodies. It is worth considering the individual parameters of patients and measuring antibodies before vaccination.
Keywords: pandemic, virus, infection, immune response
Introduction
Since the end of 2019, the whole world has been focused on developing effective prophylaxis and therapeutic methods that would help stop the epidemic and effectively combat the symptoms of COVID-19 caused by a new strain of β-coronavirus SARS-CoV-2.1,2 The disease was first discovered in December 2019 in China in the city of Wuhan, probably originated from zoonotic source, and then it spread rapidly around the world through direct and contact transmission, causing the WHO to declare a global pandemic on 11 March 2020.3,4 The clinical features of COVID-19 vary, ranging from an asymptomatic or mild, self-limiting respiratory tract condition to a severe progressive pneumonia and an acute respiratory distress syndrome (ARDS) with a multiorgan dysfunction.5–7 WHO reported over 600 million confirmed cases of COVID-19 and over 6 million COVID-19 deaths until autumn 2022.8
The key guidelines for preventive proceedings have been introduced because of the spreading rate of pandemic and insufficient treatment. These include: an early diagnosis, timely isolation of infected subjects, quarantine of contact suspects, social distancing and use of masks.9 Most countries in the world including Poland have adapted to these procedures despite initial social resistance.10 About a year after the pandemic started, several research teams successfully completed their research and developed vaccines against SARS-CoV-2. Mass vaccination programs started immediately, which gave hope for an effective fight against the virus. Several vaccines against COVID-19 have been approved for use by the WHO. Due to their short production times, mRNA vaccines (Pfizer-BioNTech COVID-19 Vaccine known as Comirnaty and Moderna COVID-19 Vaccine known as Spikevax) were first to appear.1 However, their rapid development raised a great deal of controversy and conspiracy theories among those unaware that scientists had been working on mRNA vaccines for three decades before the pandemic broke out.11,12 The variation in the number of people vaccinated in different countries are mostly due to public trust in the government, medical staff and scientists, but also sociodemographic features, personal beliefs, and attitude toward vaccination have important influence.13,14 Nevertheless, 13,008,560,983 vaccine doses were administered in the world to date.8 Numerous studies have proved that these mRNA-based vaccines are completely safe and very effective.1,15 Protein S has been selected as an important target for vaccine and antiviral development. Its subunit, the receptor-binding domain (RBD) is a key determinant of infectivity and thus is considered to be the main antigenic component that is responsible for inducing a host immune response.2 It is a principal target of neutralizing antibodies generated following an infection by SARS-CoV-2 and a component of both mRNA and adenovirus-based vaccines.1,16,17 IgG antibodies constitute a predominant type of antibody found in blood circulation (approx. 75% of all antibodies) and they have the longest serum half-life of all immunoglobulin types. They participate in the secondary immune response as an important component of the host defense system.18 Therefore, anti-SARS-CoV-2 IgG antibodies are used to detect a past infection (also asymptomatic or mild symptomatic) or to determine degree of immunogenic response to vaccination.1,19 These tests enable long-term monitoring of the humoral immune system response in individual patients, which is especially important in the case of vaccination. The knowledge of the dynamics of changes in antibody titers, and thus the length of the protective period, allows for improvement in the vaccination schedule and a rational decision on booster vaccinations.1,19,20 Information about the antibody titer can be an important indicator of the organism’s current readiness to fight infection.
We aimed to analyze the dynamics of anti-SARS-CoV-2 spike IgG antibodies before and after the third dose of vaccination against COVID-19. We also aimed to verify whether age, sex, previous COVID-19 history, and medical professions had an impact on the level of antibodies in the studied group of people. Advanced statistical tools were used to observe patterns and changes in the dynamics of these IgG antibody levels.
Materials and Methods
Study Design and Population
Participants of the project were volunteers from the Świętokrzyskie Voivodeship, Poland, who gave an informed consent to participate in the project and fulfilled the inclusion and exclusion criteria. They are described in Table 1. We did not exclude treated patients with chronic diseases without acute symptoms, such diseases as diabetes, hypertension, arthrosis, hyperthyroidism and hypothyroidism, Hashimoto’s, allergies. The total of 235 individuals were selected to the analysis and serum samples were collected for the first analysis. However, during the project many individuals were excluded for not receiving the 3rd dose of the vaccine or/and not donating blood. In the end, 100 people were fully involved in the project, but 7 individuals who declared COVID-19 in a questionnaire during the project were analyzed separately. Also, 31 individuals declared COVID-19 history in the questionnaire, but not earlier than 27 weeks from the start of the project and they were not excluded from the project. Finally, 93 participants were analyzed firstly as a whole group and next they were divided based on the following factors: age ≤49 (n = 43) and ≥50 (n = 50), sex – males (n = 23) and females (n = 70), COVID-19 history – COVID-19-positive (n = 31) and COVID-19-negative (n = 62), profession – medical (n = 44, mostly clinicians and nurses working in contact with patients) and non-medical (n = 49, other people). The participants were vaccinated with BNT162b2 (n = 73), AZD1222 (n = 17), mRNA-1273 (Moderna, n = 2) or JNJ-78436735 (Johnson & Johnson, n = 1), the IgG antibodies levels were not significantly different (t-test two tailed, p > 0.05, data not shown). All participants were informed about the purpose of the project, the research planned, and gave their informed consent to participate in the project. Table S1 presents anonymized project members with detailed characteristics. During the project implementation, blood samples were collected from the participants at four time points depending on when a participant had planned the third dose of the vaccine against COVID-19. The first blood samples were collected no longer than 2 weeks before the third dose of COVID-19 vaccine (IgG_1), next blood samples were collected after the third dose of vaccine against COVID-19: 2nd blood sample (IgG_2): 10–12 weeks (approx. 3 months), 3rd blood sample (IgG_3): 18–20 weeks (approx. 5 months), 4th blood sample (IgG_4): 24–26 weeks (approx. 6 months).
 |
Table 1 Cohort Characteristics, Inclusion and Exclusion Criteria |
Anti-SARS-CoV-2 IgG Testing
The Access SARS-CoV-2 IgG (1st IS) chemiluminescent immunoassay (Beckman Coulter Eurocenter S.A., Switzerland) was used for a quantitative and qualitative detection of IgG antibodies to SARS-CoV-2 in human serum. After collecting about 3 mL of whole blood to sample tube S-Monovette with clot activator (SARSTEDT AG & Co. KG; Germany), the serum was isolated immediately by 15-minute centrifugation at approximately 1000 x g. The 100 μL of serum was used for the analysis according to the manufacturer’s protocol, by Access 2 (Beckman Coulter, Switzerland). A sample was added to a reaction vessel with buffer, and paramagnetic particles coated with recombinant SARS-CoV-2 protein specific for the RBD of the S1 protein. The amount of analyte in the sample was determined from a stored, multi-point calibration curve. The measurement error limit according to the manufacturer is 3.1–4.8%, which was also confirmed by the analysis of the same 3 samples in three individual replications. The values ≥30 IU/mL SARS-CoV-2 IgG (1st IS) were interpreted as positive results (the value reactive for SARS-CoV-2 IgG antibodies) according to the manufacturer’s protocol.
Statistical Analysis
Normality of distributions was assessed by Shapiro–Wilk test. In the case of non-normality, Mann–Whitney or Wilcoxon signed rank test was used to compare unpaired and paired groups as appropriate, otherwise unpaired, or paired t-tests were applied. The study includes dependent variable: the level of IgG in a given measurement (1, 2, 3 and 4) and independent variables: age, gender, profession, COVID-19 history. The study may be unrepresentative by overrepresenting people with a positive COVID-19 history or women. Analyzes performed in subgroups (eg separately for male and female) and appropriately adjusted statistical tools excluded the bias of the observed relationships.
The analysis of the dynamics of the level of antibodies was proposed by determining the trajectory of changes: decrease (D), increase (I) and constant (C) of IgG in relation to the previous IgG value of the measurements at 4 time points: 1st, 2nd, 3rd, 4th. There are 27 possible IgG trajectory patterns, the first symbol (D, I or C) relates to the comparison of the levels of IgG_2 versus IgG_1 antibody, the second - IgG_3 vs IgG_2, the third - IgG_4 vs IgG_3. The analysis of increase, decrease or constant value was defined in relation to the previous measurement, but considering 5% measurement error, in the case of the difference below 5% the value was considered constant, while above 5% - a decrease or an increase.
IgG trajectory patterns as well as distributions of other categorical variables for independent groups were compared by chi-square test or Fisher’s exact test depend on whether expected values were above and below 5. Due to significant non-normality, the correlations between IgG antibodies levels at 1st, 2nd, 3rd, 4th time points were assessed by Spearman’s rank correlation coefficients. A two-tailed p-value <0.05 was considered statistically significant.
All statistical computations were performed using R (version 4.0.3; The R Foundation for Statistical Computing, Vienna, Austria), and GraphPad Prism, version 6 (San Diego, CA, USA) were used for the derivation of figures.
Results
Preliminary Analysis
Primarily, 235 participants were selected for the study according to the inclusion and exclusion criteria. The first blood sample was taken, and the level of anti-SARS-CoV-2 IgG was tested in the isolated serum. All the participants had received the 2nd dose of vaccination against COVID-19 approximately 6 months and were expected to receive the third dose of the same vaccine, the median of their IgG anti-SARS-CoV-2 level was 89.88 of IU/mL. During the project, more than half of the participants were excluded (due to not taking the 3rd dose of vaccination, not donating blood for the study). Consequently, the four measurements of antibody levels included 100 participants. During the project, seven participants developed COVID-19, after the infection an increased level of IgG (mean value 871 of IU/mL) was observed, so they were excluded from the subsequent analysis. The remaining participants (n = 93) showed a slightly lower median of IgG value from the first measurement (72.60 of IU/mL) to all the primarily enrolled participants (not statistically significant difference, Mann–Whitney, two tailed, p > 0.05; data not shown). Finally, subsequent analysis concerned 93 members. The dynamics of the antibody levels (4 measurements at intervals) of the studied participants (n = 93) was analyzed as a whole, as well as in relation to age, sex, previous COVID-19 (before the IgG measurement), and medical or non-medical profession.
General Analysis of IgG
The median IgG anti-SARS-CoV-2 levels of the four measurements (IgG_1, 2, 3, 4) were sequentially 72.60; 338.0; 345.0; 328.6 of IU/mL (Figure 1). The lowest IgG level was 2.12; 42.27; 37.28 and 25.98 of IU/mL respectively, and the highest level of IgG was 1635; 2448; 2444 and 2433 of IU/mL respectively, according to the following measurements. The median level of IgG antibodies was 4.65 times higher at 10–12 weeks after the third dose of the vaccine in comparison to 25 weeks after the second dose of the vaccine. The next two measurements revealed also similar, statistically significantly higher IgG levels than the first one. The last measurement (IgG_4) showed a statistically significant decrease in the level of antibodies in comparison to the previous measurement (IgG_3) (Figure 1). Detailed analysis showed that during the first measurement, 27.9% (n=26/93) of the participants did not have sufficient IgG levels to be protected against COVID-19 (IgG < 30 IU/mL; based on the manufacturer’s information) and 36.5% (n=34/93) of participants had IgG level below 40 IU/mL. Among these participants, IgG level increased 14 times (from median 13.23 to median 190,4 of IU/mL) after 3 months of the third dose of vaccination. As mentioned above, most participants (95%) revealed an increased level of IgG, except for five participants who had a decreased level of IgG after the 3rd vaccination. Interestingly, these peoples showed a decrease in IgG antibody levels with each subsequent measurement, they belonged to the younger group (<50 years of age), and four of them had COVID-19 in the past. They had also a high level of IgG in the first measurement (median IgG: 508 IU/mL). Almost all the participants revealed a sufficient level of IgG until the last measurement, which was approximately 6 months after the last dose of vaccination. Only three participants had an insufficient level of IgG antibodies at the last measurement (28.6; 29.95; 25.98 of IU/mL), they had also a very low IgG level at the first measurement (3.48; 15.29; 6.28 of IU/mL respectively). After a significant relative increase in IgG_2 (in relation to IgG_1), there were decreases in IgG in subsequent periods, but the relative magnitude of these decreases was not as large as the increase between IgG_2 and IgG_1, and at the end of the observation period the level of IgG_4 among 75% of the participants was at least 1.5 times higher than IgG_1 value, and 25% of the participants had values at least 9.5 times higher than the IgG_1 value.
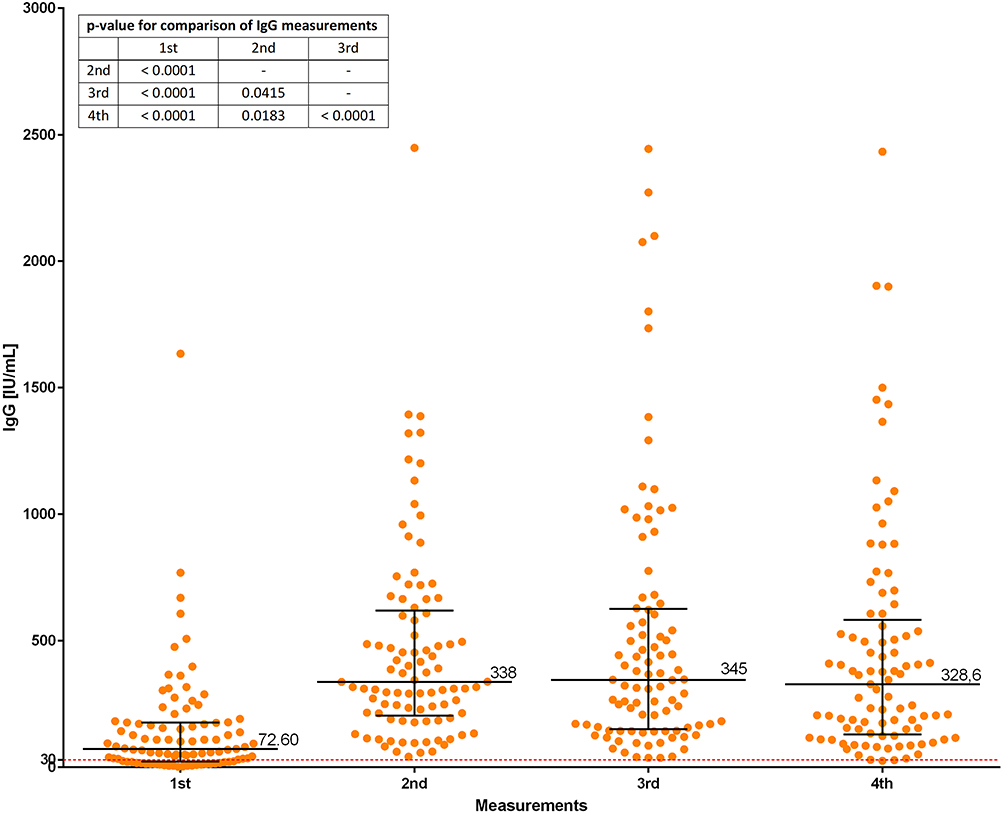 |
Figure 1 Comparison of anti-SARS-CoV-2 IgG levels [IU/mL] among the examined participants. Notes: The participants (n = 93) were tested at 4 time points (measurements) in relation to the third dose of COVID-19 vaccination (1st – approx. 2 weeks before vaccination, 2nd - approx. 3 months after vaccination, 3rd - approx. 5 months after vaccination, 4th - approx. 6 months after vaccination), dots – participants, red dots – outliers; error bars lines: bottom and top - quartiles Q1, Q3; middle - median of IgG levels; statistical significance (p < 0.05) was measured by Wilcoxon signed rank test; p-values for pairwise comparisons were all less than 0.0001, exception 2nd vs 3rd (p = 0.0415) and 2nd vs 4th (p = 0.0183). |
Furthermore, we grouped the participants according to baseline IgG antibody levels – from the lowest to the highest. The individuals were divided into 4 groups including limit values of IgG_1 [IU/mL]: <40 (2.12–39.3), 40≤100 (43.47–95.04), 100≤200 (102.28–191.66), >200 (211.3–1635). We observed that a relative increase in antibodies levels approximately 3 months after the vaccination (IgG_2) was inversely proportional to the baseline antibody level (IgG_1) among the participants – the lower baseline antibody level, the greater increase, and vice versa (Figure 2). The medians of the IgG_2 to IgG_1 ratio in individual groups of participants were: 12.44, 5.11, 2.69 and 1.71 respectively, the differences were statistically significant (Mann Whitney exact test, two-tailed, unpaired) except for differences between group <200 and <1635.
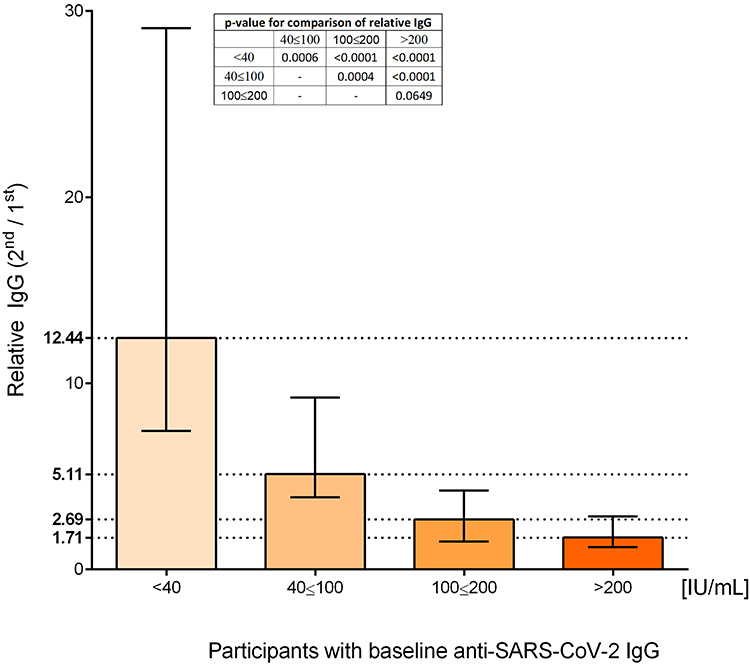 |
Figure 2 Comparison of relative increase of anti-SARS-CoV-2 IgG levels. Notes: The relative IgG was the ratio between value of IU/mL of IgG_2/IgG_1; the participants grouped according to four baseline IgG levels [IU/mL] ranges: <40 (2.12–39.3), 40≤100 (43.47–95.04), 100≤200 (102.28–191.66), >200 (211.3–1635); medians with interquartile range of relative IgG, the differences were measured by Mann Whitney exact test, two-tailed, unpaired (statistically significant p < 0.05). |
Moreover, Spearman’s rank correlation coefficients between individual measurements increased systematically and amounted to 0.465 between the measurements of IgG_2 and IgG_1, 0.756 between the measurements of IgG_3 and IgG_2 and 0.945 between the measurements of IgG_4 and IgG_3. This means that in the first measurement, the levels of IgG antibodies of the tested participants were very differentiated and changed not directly (increased/decreased) in the next measurement (IgG_2), but in the case of subsequent measurements, the levels of antibodies changed more and more pro-proportionally, assuming a linear relationship.
We also included the analysis of the trajectory of the dynamics of IgG antibodies depending on consecutive measurements. Of the 27 possible trajectories, 9 were observed, but none of these patterns occurred statistically more frequently compared to the others. However, the dominant pattern of changes in the level of IgG was an increase in IgG_2 (in relation to IgG_1), followed by a decrease in IgG_3 (in relation to IgG_2) and a decrease in IgG_4 (in relation to IgG_3) – such fluctuations in the level of IgG were observed in 46.2% of the participants (IDD pattern - increase, decrease, decrease). The second most frequent pattern of changes of IgG levels was IID in subsequent measurements (17.2% of participants). In addition, the following patterns were also observed: III (8.6% of participants), IDC (8.6% of participants), IDI (7.5% of participants), DDD (5.5% of participants), ICD (4.3% of participants), IIC (1.1% of participants) and ICC (1.1% of participants).
We would like to present our latest results – approximately after 10 months of the third dose of vaccination against COVID-19. These results include only 20 participants, the previous median of IgG levels was 431.96 of UI/mL and these values decreased 1.5 times (median IgG is 286.67 of IU/mL). Among 3 individuals (IgG was 80.55, 86.64, and 97.79 IU/mL), the antibody levels increased, so they were probably infected with COVID-19.
Age
The participants ranged from 21 to 61 years old, they were divided into two groups: younger (age ≤49, n = 43) and older (age ≥50, n = 50). For both groups, no statistically significant differences were observed between IgG_2 and IgG_3. In both groups, there was a statistically significant decrease in the value of IgG_4 versus IgG_3, however, in the case of the “older” group the decrease was smaller. We can see a tendency to lower immunological response in the case of the younger people (Figure 3); however, the difference between younger and older participants was not statistically significant (Table 2). There has been shown 9 different trajectories of changes in antibody levels, however, of the most people, both younger and older ones, showed a decrease in antibodies in the third and fourth measurement (Table 3). Participants showing a continuous decrease in the level of antibodies (DDD) occurred only in the younger group, and in the measurement of IgG_4 a more frequent increase in IgG was observed in the older group (IDI).
 |
Table 2 Comparison of the Medians (with Quartiles Q1, Q3) of the Anti-SARS-CoV-2 Spike IgG Antibodies Values [IU/mL] Among the Studied Participants (n = 93) Based on Specific Parameters (Age, Sex, COVID-19 History, Profession) |
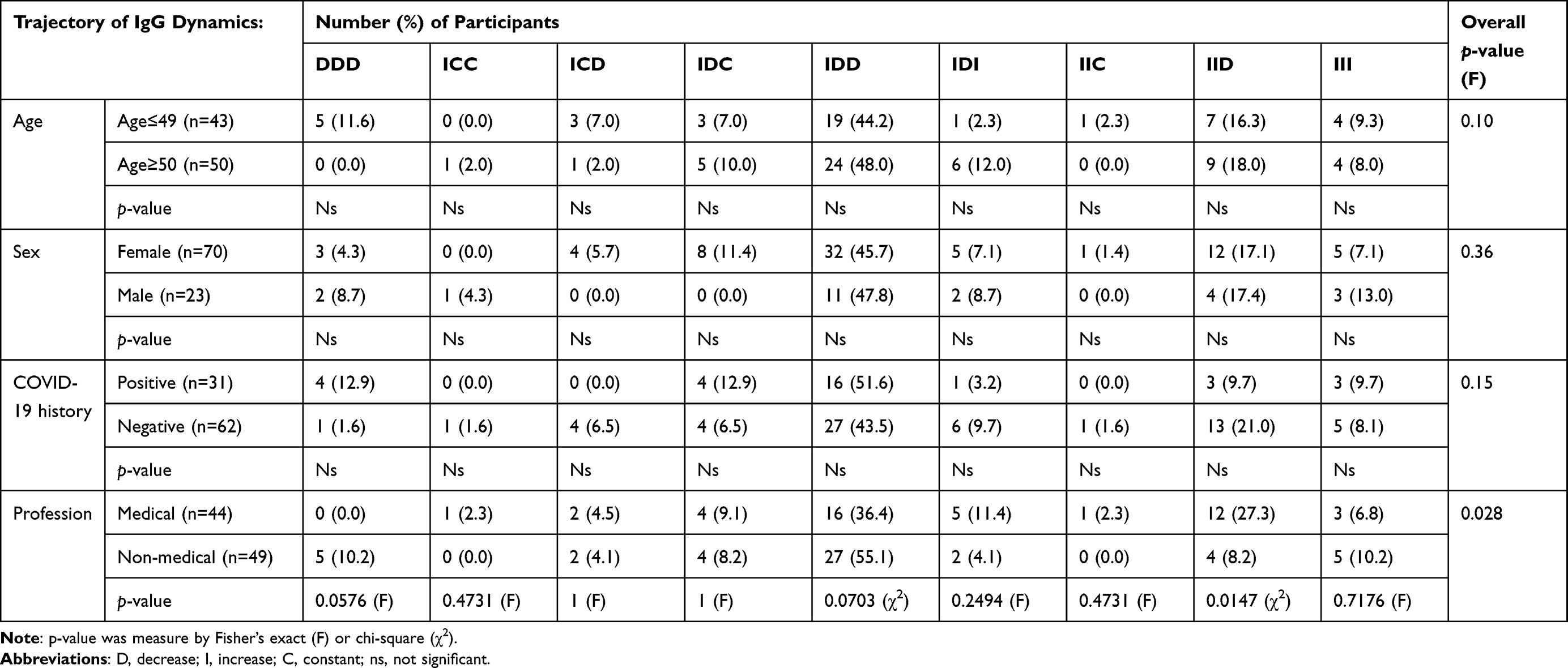 |
Table 3 Number (%) of Participants Grouped According to Particular Parameters (Age, Sex, COVID-19 History, Profession) Showing Specific Patterns of Trajectory of IgG Antibody Dynamics Between Consecutive Measurements |
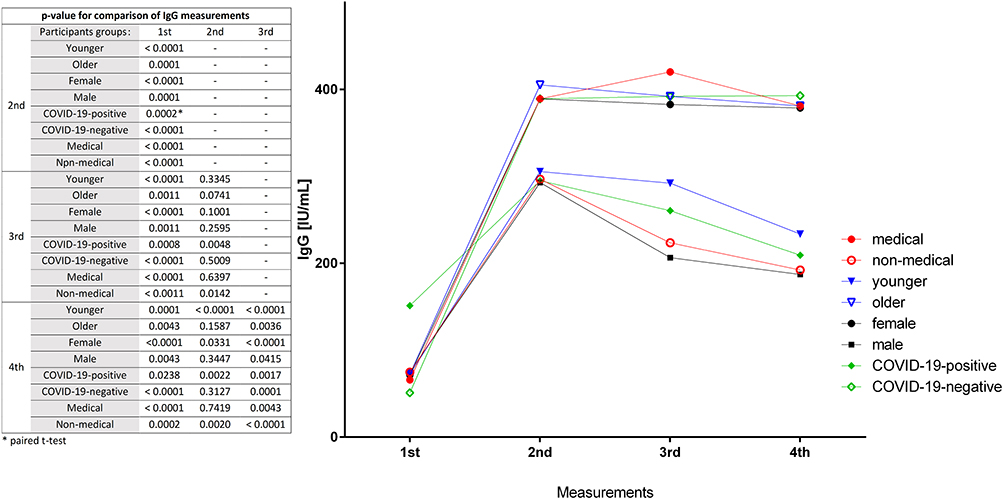 |
Figure 3 Dynamics of anti-SARS-CoV-2 IgG of the participants according to age, sex, COVID-19 history and profession. Notes: The dots represent the median levels of IgG at 4 measurements (1st – approx. 2 weeks before vaccination 3rd dose of vaccination, 2nd - approx. 3 months after vaccination, 3rd - approx. 5 months after vaccination, 4th - approx. 6 months after vaccination), the differences were measured by Wilcoxon signed rank test (statistically significant p < 0.05). |
Sex
The participants were grouped according to sex: female (n = 70) and male (n = 23) and the differences between the median levels of IgG antibodies were presented in Figure 3. Both among male and female participants, the level of IgG_1 was significantly lower than the level at each of the other measurement points (IgG_2, 3 and 4). For both groups, no statistically significant change was observed between IgG_2 and IgG_3. In both groups, there was a statistically significant decrease in the value of IgG_4 versus IgG_3. Generally, a decrease in IgG level in male participants was revealed (Figure 3). The median level of antibodies in the first measurement was very similar for both female and male, but already in the second and third measurement, a statistically significantly higher level of antibodies (1.3 and 1.85 times higher respectively) was detected among female participants (Table 2). The trajectory of IgG changes did not show statistically significant differences between male and female subjects (Table 3): most of both female and male participants showed a decrease in IgG levels during the 3rd and 4th measurements (IDD pattern).
COVID-19 in the Past
Of all the members, 31 (33%) had COVID-19 in the past (more than 6 months before). The differences between the median levels of IgG antibodies are presented in Figure 3. Both among positive and negative histories of the COVID-19, the level of IgG_1 was significantly lower than the level at each of the other measurement points (IgG_2, 3 and 4). Interestingly, a consistently significant decrease in the level of antibodies was observed after about 5 months post vaccination (third measurement), in contrast to the group of people who did not have COVID-19 – this was observed scarcely at the last measurement. Generally, the participants which had COVID-19 in the past showed a decrease in antibodies, even though at the beginning (IgG_1) they had statistically more antibodies than those who had not been infected before. The IgG_1 level of COVID-19-positive group was 3 times higher in comparison to the other participants (Table 2). The next measurements did not reveal any statistically significant differences, but we can see a lower median level of IgG among the COVID-19-positive group. On the other hand, the relative increase of IgG antibodies level between the first and next measurements (relative value between IgG _2/1, IgG_3/1, IgG_4/1) was statistically significantly higher in the COVID-negative group in comparison to the COVID-positive group (data not shown, Mann–Whitney, two tailed, p < 0.0001, except IgG_4/1 p = 0.0001). The trajectory of IgG changes did not show statistically significant differences between these groups (Table 3). Most of the participants showed a decrease in IgG levels during the 3rd and 4th measurements (IDD pattern). There was no statistically significant relationship with sex in the COVID-19-positive and COVID-19-negative groups (p = 0.395, chi-square test).
Medical Profession
The last analysis included comparison of the IgG levels between medical (n = 44) and non-medical (n = 49) participants. Generally, a higher level and a weaker decline of IgG anti-SARS-CoV-2 were observed in the medical group (Figure 3). Both among medical and non-medical groups, the level of IgG_1 was significantly lower than the level at each of the other measurement points (IgG_2, 3 and 4). In case of the non-medical group each next measurement revealed statistically significant differences to the previous measurement, in the medical group the significant decrease of IgG levels detected also between IgG_4 and IgG_3. The median level of antibodies in the first measurement was similar for both control and medical groups, but in subsequent measurements the differences deepened. A statistically significantly higher level of antibodies during the third and fourth measurements (1.8 and 1.98 times higher respectively) was detected in medical group (Table 2). Generally, a statistically significant relative higher increase or lower decrease in IgG antibodies level between the measurements was observed among the medical group in comparison to the non-medical group (data not shown, Mann–Whitney, two tailed, p < 0.05). The trajectory of IgG changes showed statistically significant differences between these two groups (Table 3). Significantly more participants from the medical group showed a decrease only in the last measurement (IgG_4) as compared to the non-medical group. More participants of the non-medical group showed a faster decline in antibodies compared to the medical group, also no individual showed a pattern of a continuous decline (DDD) in antibodies in the medical group, in contrast to the non-medical one. However, most of the participants (medical: 36.4%, non-medical: 55.1%) revealed an IgG decrease in 3rd and 4th measurements.
There was no evidence of an effect of sex (chi-square test, p = 0.0617) and age (Mann Whitney test, p = 0.1463) of participants on IgG antibody levels in the medical and non-medical groups.
Discussion
Despite the developed guidelines, how to proceed in the event of a pandemic, the COVID-19 pandemic has surprised not only human population but also clinicians, and scientists. It introduced many changes in medical diagnostics and chaos in the economic and social life. The knowledge about the virus SARS-CoV-2 and the COVID-19 disease is growing rapidly. Moreover, scientists were prepared for the emergence of the virus and several safe vaccines against COVID-19 were approved quickly, just one year after the outbreak of the epidemic (December 2020).12,21–25 Technologies of Pfizer/BioNTech and Moderna turned out to be the most effective they use virus’s mRNA fragment encoding the spike (S) protein. This protein attaches the virion to the host cell’s membrane26 and its S1 subunit contains an immunologically relevant RBD, which is a key antibody target. During COVID-19, the human body also produces other specific antibodies against different SARS-CoV-2 structures, but the spike protein appears to be the most immunogenic,27,28 however, the immune response to COVID-19 is still poorly understood. Currently, the pathophysiology of infection and the course of the disease are well understood and quite predictable, but potential long-term repercussions remain a mystery.29 The host’s immune system plays a key role in defense against SARS-CoV-2 infection and regulates the course of the disease. A further course of the COVID-19 pandemic will depend on widespread immunity of the population acquired through infection or vaccination.
Analysis of the Dynamics of IgG Anti-SARS-CoV-2 Spike Protein Before and After the Third Dose of Vaccination
Screening trials showed that protective levels of antibodies after the second dose of the vaccine maintained for at least 6 months but at different levels and with dynamics of maintenance.1,30–32 It is known that many internal and external parameters can be associated with these observations, but still little is known about how immunity develops after vaccination. There is much controversy and conflicting discussions to whether subsequent doses of the vaccine should be taken. The cellular and humoral immunity is triggered in response to exposure to viral antigens after contracting COVID −19, but the level of neutralizing IgG anti-S antibodies strongly correlate with the severity of illness33 In our project, we present the dynamics of IgG anti-SARS-CoV-2 spike protein after the next booster mRNA vaccination against COVID-19 (mostly BNT162b2) in human participants of Polish population. The observation of particular individuals lasted about 6 months, and each person was examined 4 times. We also analyzed the IgG levels associations with typical clinical parameters like age, sex, and prior COVID-19, as well as with the medical profession. The results revealed that about 6 months after the second dose of vaccination, the antibody level in most participants was enormously low (the median was only twice the protective cutoff value of 30 IU/mL of IgG), and 36.5% of participants had IgG level below 40 IU/mL (Figure 1). A similar significant decrease in antibodies after the second dose of COVID-19 vaccine mRNA was presented by Tretyn et al1 after 4 month the antibodies levels in all participants decreased below the administration of the second dose. This has also been observed in other countries described in the metanalysis by Notarte et al34 Đaković Rode et al35 reported a decline in antibodies 6 months after the second dose of vaccination but these levels were still considered positive for protection against COVID-19, it was in line with our results. The next measurement (IgG_2) after approximately 3 months from the 3rd dose of vaccination indicated in most of the participants that the antibody level was 4.6 higher compared to the previous measurement. Such a high level was mostly maintained until the last measurement (IgG_4) – up to 6 months from the 3rd dose of vaccination, similar observations are described by others,20,36–41 on this basis we can generally conclude that the 3rd booster dose of vaccination has an enhancing effect of longer-lasting immune protection against COVID-19. We also observed an interesting association: individuals who showed lower antibody levels at baseline responded better to the vaccine in comparison to the participants with higher baseline IgG level (Figure 2). This was also confirmed using the Spearman’s rank correlation coefficients – the increase in IgG levels was disproportionate at the beginning, and later the changes were linear. This may mean that the mobilization of the immune system is variable and highly dependent on the level of antibodies present in the body.
The analysis of the trajectory of the antibody levels’ dynamics also revealed many interesting observations. In most of the participants, a decrease in the level of IgG was detected in the 3rd and 4th measurements, but the level was still very high, what is more, 22.6% of the participants showed a decrease only on the last measurement. This confirms a correct, strong effect of the vaccine in most of the studied people.29,36,40 It should be noted that some individuals (5% of studied group) did not respond to the vaccine (their trajectory of IgG level dynamics was DDD), but they had very high levels of antibodies on the baseline measurement and maybe that is why the vaccine did not induce immunity. Three participants had below the cutoff level of reactive IgG antibodies at last measurement, and they had also a very low IgG level at the baseline measurement. Individual features or other reasons may have influenced this, but it did not significantly affect the overall conclusions. Also, among 9.7% of the participants the untypical dynamics of antibodies level (the IDI trajectory) was revealed. Such a pattern of IgG dynamics may indicate a recent COVID-19, which we could not detect with the applied test. It should also be emphasized that all atypical trajectories do not significantly change the conclusion that the median antibody level in each measurement was significantly higher than in the baseline measurement.
Our preliminary results (23 participants) show a 1.5-fold decrease in IgG anti-SARS-CoV-2 approximately 10 months after the last (third) dose of vaccination against COVID-19 and suggest a longer duration of antibodies in the Polish population compared to other reports.29,42
We are obligated to mention some limitations in our project. Participants who reported COVID-19 during the study were excluded from the project, but we do not know if there were more patients suffering from COVID-19, the applied test does not differentiate the COVID-19 and SARS-CoV-2 IgG. Some individuals may have had an asymptomatic course of COVID-19, or they might have thought it was a different infection. However, it should be considered that the risk of the infection was also before the first measurement, what is more, the risk was higher due to higher number of infections.8 The analyzed antibody levels could have been modified to the same extent by prior infection with each measurement, so the observed significant differences in IgG levels are independent of the infection.
Study of the Age and Sex Influence on the IgG Anti-SARS-CoV-2 Spike Protein Antibody Level
During the study, we verified if the pre-retirement age (age of 50–61 years) correlates with the IgG anti-SARS-CoV-2 (Figure 3). It turned out that the group of older participants tended to have significantly higher levels of antibodies at each stage of the measurements, and the younger group (age between 21 and 49 years) showed a greater downward trend between the last two measurements. This observation is in line with Soeorg et al and Yang et al,43,44 which can be associated with many factors specific for older individuals like: more severe symptoms during COVID-19, expanded catalog of memory B and T cells through accumulated immunological memory and higher level of cytokines associated with comorbidities what can stimulate the SARS-CoV-2 humoral response. What is more, older people suffer from COVID-19 more often,45 which might not have been noted in our data, but it influenced the level of tested antibodies. On the other hand, Barda et al46 revealed that people over 60 years of age suffered less from COVID-19 after the 3rd dose of vaccination compared to younger age groups. The answer to our observations would be to conduct a test differentiating the immune response after vaccination and post-infection. Generally, most reports indicate negative correlation of IgG levels with age,47–49 nevertheless, there is still no clear studies.
In the case of gender – our findings are similar to those of others:1,36,50–52 Females have statistically higher and more stable level of IgG anti-SARS-CoV-2 in comparison to males, even if they started with similar IgG levels.45 The phenomenon of stronger immunological response among women is commonly observed also in contact with other pathogenic antigens and can be modified by many genetic, hormonal, and environmental factors.53 A scoring metric for immunological aging also revealed that men exhibit significantly higher immune-aging scores than women.54
Study of the COVID-19 Influence on the IgG Anti-SARS-CoV-2 Spike Protein Antibody Level
Some participants (33%) reported COVID-19 at least 6 months before the baseline measurement and they showed 3 times higher level of IgG antibodies than the rest. Moreover, they all had sufficient antibody levels at least twice as high as the cutoff (median 151.34 (Q1; Q3: 60.36; 250.50) of IU/mL). These observations are in line with others1,36,55–57 that infection promotes longer maintenance of SARS-CoV-2 antibodies after the second dose of vaccination against COVID-19. However, with longer observations up to 6 months after the 3rd dose of vaccination, COVID-19-positive individuals revealed a quicker decrease in IgG antibodies, and the median of IgG levels were almost twice lower in comparison to individuals previously unaffected by COVID-19, these findings are also consistent with Pellini et al.52 Also, Tretyn et al1 observed that in patients without prior COVID-19, stable antibody level lasted longer than in patients with prior COVID-19. Our thesis is confirmed again – people with lower levels of antibodies are better immunized by the vaccine. This phenomenon may be also related to the amnesty response to exposure to the virus, however there is no confirmation of this.58 Schwarzkopf et al59 revealed that among convalescent patients immunity may be mediated through T cells. Moreover, Greaney et al25 proved that a vaccine can provide a better protection against a mutating virus than a disease itself – a better match of antibody-virus binding produced after immunization with the vaccine. Romero-Ibarguengoitia et al36 also describe that after the administration of the third BNT162b2 booster, the increase in quantitative SARS-CoV-2 spike 1–2 IgG antibody was twice as high among participants with a negative SARS-CoV-2 infection in comparison to participants with COVID-19 positive history, nevertheless, the raw data show higher levels of antibodies in COVID-19 positive participants. These divergent results require further investigation. Generally, a higher level of antibodies is described in people with a positive COVID-19 history, but many factors should be taken into account - The time of the analysis in relation to the previous infection and vaccination, the test method, the individual conditions of the subjects and the fact that the virus produces various proteins that can stimulate a variety of immune response pathways.60,61
Study of the Medical Profession Influence on the IgG Anti-SARS-CoV-2 Spike Protein Antibody Level
The last analysis involved comparison of the IgG levels between medical and non-medical participants. Generally, a higher level and a weaker decline of IgG anti-SARS-CoV-2 was observed in the medical group, which is in line with other observation.62 We showed that the medical profession correlated with almost twice the antibody level after about 5–6 months of baseline measurement, although the median of baseline values was similar in both groups but less varied in the medical staff. This suggests that exposure to continuous or more frequent contact with the SARS-CoV-2 virus or its antigens stimulates the immune system and allows the body to maintain antibody levels longer and more stable.52 Despite this, a group of healthcare workers 6 months after the second vaccination also had very low levels of antibodies, much lower (almost threefold) than those who had COVID-19 at least six months ago. On the other hand, Đaković Rode et al35 presented much more optimistic data among healthcare workers in Croatia. Although they used a different method of IgG measurement, the relative level of antibodies was on average 20 times higher than the cutoff value of positive test (50 AU/mL of IgG) 6 months after the 2nd dose of vaccination. We would like to underline the correlations described above are independent of each other, and the statistical tools used allow for their apart interpretation, which gives the basis for searching for an explanation of these phenomena.
To sum up, we would like to mention the limitations of the work. An important issue is the lack of differentiation into post-vaccination and post-infection IgG antibodies in the applied method. This would allow for a precise answer regarding the level of antibodies depending on vaccination and/or possible asymptomatic COVID-19. We also did not confirm the presence of SARS-CoV-2 RNA in the participants to exclude ongoing infection, we only relied on declarations, which could affect the higher levels of antibodies levels. Another limitation is the small number of respondents, which makes it difficult to obtain stronger correlations between the distinguished groups, especially in the case of distribution of women and men. Also, the presence of chronic diseases could modify the level of antibodies, but it was practically impossible to select a study group without chronic diseases. Therefore, we excluded the occurrence of severe diseases and people in the acute phase of the disease and untreated. We would like to emphasize that the mentioned limitations of the project do not present false correlations, but the observed statistically significant differences could be more pronounced. We would like to mention that it would also be interesting to study the age group over 61 and children, which could provide more interesting observations.
Our greatest achievement in this work is providing evidence that vaccination mobilizes the immune system to production of specific neutralizing IgG against SARS-CoV-2. Moreover, a greater number of boosters correlates with a longer duration of immune memory against COVID-19. An interesting observation is also that it is better to vaccinate people with borderline levels of antibodies, then the mobilization of the immune system is more long-lasting. In this work, we also indicated which features of participants correlate with weaker immune system in relation to SARS-CoV-2. This can be useful for developing guidelines for the timing of booster doses.
Conclusion
The research presents the dynamics of anti-SARS-CoV-2 IgG-S antibodies after the 2nd and 3rd dose of the vaccine against COVID-19 and provide interesting correlations about selected clinical parameters. The main finding of our research was that IgG-S levels lasted about 2 months longer after the second booster vaccination in comparison to the first booster vaccination, which confirms that vaccinations enhance immune memory, not impairs it. What more, our findings indicate a weaker effect of vaccinations among individuals with a higher level of IgG. This suggests that patients should be tested for IgG levels prior to vaccination. We observed also a stronger and less diverse immune response in the case of people who are more exposed to the virus (medical staff), women, people without previous COVID-19 and the elderly (over 49 years of age). Administration of booster vaccinations should be carried out with greater care, but their continuation is certainly justified even in the case of subsequent SARS-CoV-2 mutations. Recent studies indicate a slightly reduced immune response, but they show the effectiveness of currently used vaccines against other variants of the SARS-CoV-2 virus.63,64
Ethics Approval and Informed Consent
The study complies with the Declaration of Helsinki. The study was approved by the Bioethics Committee of the Jan Kochanowski University in Kielce (Resolution No. 69/2021 UJK). All participants were informed about the purpose of the project and the planned research tasks. Participants gave the informed consent to participate in the project. Table S1 presents anonymized project members with detailed characteristics.
Acknowledgments
We would like to thank all the blood donors who agreed to this scientific study.
Funding
Project financed under the program the Minister of Education and Science called “Regional Initiative of Excellence” in the years 2019–2023, project no. 024/RID/2018/19, amount of financing11999000,00 PLN.
Disclosure
The authors declare no conflicts of interest in relation to this work and that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Tretyn A, Szczepanek J, Skorupa M., et al. Differences in the Concentration of Anti-SARS-CoV-2 IgG Antibodies Post-COVID-19 Recovery or Post-Vaccination. Cells. 2021;10(8):1952. doi:10.3390/cells10081952
2. Zhang S, Xu K, Li C, et al. Long-Term Kinetics of SARS-CoV-2 Antibodies and Impact of Inactivated Vaccine on SARS-CoV-2 Antibodies Based on a COVID-19 Patients Cohort. Front Immunol. 2022;13:48.
3. Cucinotta D, Vanelli M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020;91(1):157–160. doi:10.23750/abm.v91i1.9397
4. Umakanthan S, Sahu P, Ranade AV, et al. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad Med J. 2020;96(1142):753–758. doi:10.1136/postgradmedj-2020-138234
5. Zeng H, Ma Y, Zhou Z, et al. Spectrum and Clinical Characteristics of Symptomatic and Asymptomatic Coronavirus Disease 2019 (COVID-19) With and Without Pneumonia. Front Med. 2021;8:645651. doi:10.3389/fmed.2021.645651
6. Trybek A, Lichota P, Wilczynski J, Zieliński R. Neck phlegmon in COVID-19 patients. Med Studies. 2021;37(4):349–353. doi:10.5114/ms.2021.112392
7. Pabjan P, Błoniarczyk P, Stępień PM, Garbat A, Włosek M, Zarębska-Michaluk D. Pulmonary embolism complicating the course of COVID-19 – an underestimated condition? Med Studies. 2020;36(3):206–210. doi:10.5114/ms.2020.99542
8. WHO Coronavirus (COVID-19) Dashboard. Available from: https://covid19.who.int.
9. Gianfagna F, Veronesi G, Baj A, et al. Anti-SARS-CoV-2 antibody levels and kinetics of vaccine response: potential role for unresolved inflammation following recovery from SARS-CoV-2 infection. Sci Rep. 2022;12(1):385. doi:10.1038/s41598-021-04344-y
10. Miralles O, Sanchez-Rodriguez D, Marco E, et al. Unmet needs, health policies, and actions during the COVID-19 pandemic: a report from six European countries. Eur Geriatr Med. 2021;12(1):193–204. doi:10.1007/s41999-020-00415-x
11. Dolgin E. The tangled history of mRNA vaccines. Nature. 2021;597(7876):318–324. doi:10.1038/d41586-021-02483-w
12. Turner JS, O’Halloran JA, Kalaidina E, et al. SARS-CoV-2 mRNA vaccines induce persistent human germinal centre responses. Nature. 2021;596(7870):109–113. doi:10.1038/s41586-021-03738-2
13. Umakanthan S, Bukelo MM, Bukelo MJ, Patil S, Subramaniam N, Sharma R. Social Environmental Predictors of COVID-19 Vaccine Hesitancy in India: a Population-Based Survey. Vaccines. 2022;10(10):1749. doi:10.3390/vaccines10101749
14. Umakanthan S, Patil S, Subramaniam N, Sharma R. COVID-19 Vaccine Hesitancy and Resistance in India Explored through a Population-Based Longitudinal Survey. Vaccines. 2021;9(10):1064. doi:10.3390/vaccines9101064
15. Kowalzik F, Schreiner D, Jensen C, Teschner D, Gehring S, Zepp F. mRNA-Based Vaccines. Vaccines. 2021;9(4):390. doi:10.3390/vaccines9040390
16. Dai L, Gao GF. Viral targets for vaccines against COVID-19. Nat Rev Immunol. 2021;21(2):73–82. doi:10.1038/s41577-020-00480-0
17. Harvey WT, Carabelli AM, Jackson B, et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat Rev Microbiol. 2021;19(7):409–424. doi:10.1038/s41579-021-00573-0
18. Schroeder HW, Cavacini L. Structure and Function of Immunoglobulins. J Allergy Clin Immunol. 2010;125(2):S41–S52. doi:10.1016/j.jaci.2009.09.046
19. Higgins V, Fabros A, Kulasingam V. Quantitative Measurement of Anti-SARS-CoV-2 Antibodies: analytical and Clinical Evaluation. J Clin Microbiol. 2021;59(4):e03149–20. doi:10.1128/JCM.03149-20
20. Skorupa M, Szczepanek J, Goroncy A, et al. The Dynamics of Changes in the Concentration of IgG against the S1 Subunit in Polish Healthcare Workers in the Period from 1 to 12 Months after Injection, Including Four COVID-19 Vaccines. Vaccines. 2022;10(4):506. doi:10.3390/vaccines10040506
21. Sahin U, Muik A, Derhovanessian E, et al. COVID-19 vaccine BNT162b1 elicits human antibody and T.sub.H1 T cell responses. Nature. 2020;586(7830):594–600. doi:10.1038/s41586-020-2814-7
22. Mulligan MJ, Lyke KE, Kitchin N, et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature. 2020;586(7830):589–593. doi:10.1038/s41586-020-2639-4
23. Polack FP, Thomas SJ, Kitchin N, et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Eng J Med. 2020;383(27):2603–2615. doi:10.1056/NEJMoa2034577
24. Baden LR, El Sahly HM, Essink B, et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N Engl J Med. 2021;384(5):403–416. doi:10.1056/NEJMoa2035389
25. Greaney AJ, Loes AN, Gentles LE, et al. Antibodies elicited by mRNA-1273 vaccination bind more broadly to the receptor binding domain than do those from SARS-CoV-2 infection. Sci Transl Med. 2021;13(600):eabi9915. doi:10.1126/scitranslmed.abi9915
26. Ashour HM, Elkhatib WF, Rahman MM, Elshabrawy HA. Insights into the Recent 2019 Novel Coronavirus (SARS-CoV-2) in Light of Past Human Coronavirus Outbreaks. Pathogens. 2020;9(3):186. doi:10.3390/pathogens9030186
27. Piccoli L, Park YJ, Tortorici MA, et al. Mapping Neutralizing and Immunodominant Sites on the SARS-CoV-2 Spike Receptor-Binding Domain by Structure-Guided High-Resolution Serology. Cell. 2020;183(4):1024–1042.e21. doi:10.1016/j.cell.2020.09.037
28. Salazar E, Kuchipudi SV, Christensen PA, et al. Convalescent plasma anti-SARS-CoV-2 spike protein ectodomain and receptor-binding domain IgG correlate with virus neutralization. J Clin Invest. 2020;130(12):6728–6738. doi:10.1172/JCI141206
29. Lo Sasso B, Agnello L, Giglio RV, et al. Longitudinal analysis of anti-SARS-CoV-2 S-RBD IgG antibodies before and after the third dose of the BNT162b2 vaccine. Sci Rep. 2022;12(1):8679. doi:10.1038/s41598-022-12750-z
30. Doria-Rose N, Suthar MS, Makowski M, et al. Antibody persistence through 6 months after the second dose of mRNA-1273 vaccine for Covid-19. N Engl J Med. 2021;384(23):2259–2261. doi:10.1056/NEJMc2103916
31. Fiolet T, Kherabi Y, MacDonald CJ, Ghosn J, Peiffer-Smadja N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: a narrative review. Clin Microbiol Infect. 2022;28(2):202–221. doi:10.1016/j.cmi.2021.10.005
32. Levin EG, Lustig Y, Cohen C, et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N Eng J Med. 2021;385(24):e84. doi:10.1056/NEJMoa2114583
33. Chen X, Pan Z, Yue S, et al. Disease severity dictates SARS-CoV-2-specific neutralizing antibody responses in COVID-19. Signal Transduction Targeted Therapy. 2020;5. doi:10.1038/s41392-020-00301-9
34. Notarte KI, Guerrero-Arguero I, Velasco JV, et al. Characterization of the significant decline in humoral immune response six months post-SARS-CoV-2 mRNA vaccination: a systematic review. J Med Virol. 2022;94(7):2939–2961. doi:10.1002/jmv.27688
35. Đaković Rode O, Bodulić K, Zember S, et al. Decline of Anti-SARS-CoV-2 IgG Antibody Levels 6 Months after Complete BNT162b2 Vaccination in Healthcare Workers to Levels Observed Following the First Vaccine Dose. Vaccines. 2022;10(2):153. doi:10.3390/vaccines10020153
36. Romero-Ibarguengoitia ME, Rivera-Salinas D, Hernández-Ruíz YG, et al. Effect of the third dose of BNT162b2 vaccine on quantitative SARS-CoV-2 spike 1–2 IgG antibody titers in healthcare personnel. PLoS One. 2022;17(3):e0263942. doi:10.1371/journal.pone.0263942
37. Cromer D, Steain M, Reynaldi A, et al. Neutralising antibody titres as predictors of protection against SARS-CoV-2 variants and the impact of boosting: a meta-analysis. Lancet Microbe. 2022;3(1):e52–e61. doi:10.1016/S2666-5247(21)00267-6
38. Yavuz E, Günal Ö, Başbulut E, Şen A. SARS-CoV-2 specific antibody responses in healthcare workers after a third booster dose of CoronaVac or BNT162b2 vaccine. J Med Virol. 2022;94(8):3768–3775. doi:10.1002/jmv.27794
39. Kontopoulou K, Nakas CT, Belai C, Papazisis G. Antibody titers after a third dose of the SARS-CoV-2 BNT162b2 vaccine in immunocompromised adults in Greece: is a fourth dose necessary? J Med Virol. 2022;94(10):5056–5060. doi:10.1002/jmv.27954
40. Irsan A, Mardhia M, Rialita A. Evaluation of Humoral Response of Emergency Unit Healthcare Workers after Third Dose of COVID-19 Vaccination. Muhammadiyah Med J. 2022;3(1):27–32. doi:10.24853/mmj.3.1.27-32
41. Simon B, Rubey H, Gromann M, et al. SARS-CoV-2 Antibody and T Cell Response after a Third Vaccine Dose in Hemodialysis Patients Compared with Healthy Controls. Vaccines. 2022;10(5):694. doi:10.3390/vaccines10050694
42. Eliakim-Raz N, Stemmer A, Ghantous N, et al. Antibody Titers After a Third and Fourth SARS-CoV-2 BNT162b2 Vaccine Dose in Older Adults. JAMA Netw Open. 2022;5(7):e2223090. doi:10.1001/jamanetworkopen.2022.23090
43. Soeorg H, Jõgi P, Naaber P, Ottas A, Toompere K, Lutsar I. Seroprevalence and levels of IgG antibodies after COVID-19 infection or vaccination. Infect Dis. 2022;54(1):63–71. doi:10.1080/23744235.2021.1974540
44. Yang HS, Costa V, Racine-Brzostek SE, et al. Association of Age With SARS-CoV-2 Antibody Response. JAMA Network Open. 2021;4(3):e214302. doi:10.1001/jamanetworkopen.2021.4302
45. Ishaq SE, Abdulqadir SZ, Khudhur ZO, et al. Comparative study of SARS-CoV-2 antibody titers between male and female COVID-19 patients living in Kurdistan region of Iraq. Gene Reports. 2021;25:101409. doi:10.1016/j.genrep.2021.101409
46. Barda N, Dagan N, Cohen C, et al. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: an observational study. Lancet. 2021;398(10316):2093–2100. doi:10.1016/S0140-6736(21)
47. Alharbi NK, Al-Tawfiq JA, Alwehaibe A, et al. Persistence of Anti-SARS-CoV-2 Spike IgG Antibodies Following COVID-19 Vaccines. IDR. 2022;15:4127–4136. doi:10.2147/IDR.S362848
48. Anastassopoulou C, Antoni D, Manoussopoulos Y, et al. Age and sex associations of SARS-CoV-2 antibody responses post BNT162b2 vaccination in healthcare workers: a mixed effects model across two vaccination periods. PLoS One. 2022;17(4):e0266958. doi:10.1371/journal.pone.0266958
49. Wei J, Stoesser N, Matthews PC, et al. Antibody responses to SARS-CoV-2 vaccines in 45,965 adults from the general population of the United Kingdom. Nat Microbiol. 2021;6(9):1140–1149. doi:10.1038/s41564-021-00947-3
50. Demonbreun AR, Sancilio A, Velez ME, et al. COVID-19 mRNA Vaccination Generates Greater Immunoglobulin G Levels in Women Compared to Men. J Infect Dis. 2021;224(5):793–797. doi:10.1093/infdis/jiab314
51. Pang NYL, Pang ASR, Chow VT, Wang DY. Understanding neutralising antibodies against SARS-CoV-2 and their implications in clinical practice. Military Med Res. 2021;8(1):47. doi:10.1186/s40779-021-00342-3
52. Pellini R, Venuti A, Pimpinelli F, et al. Initial observations on age, gender, BMI and hypertension in antibody responses to SARS-CoV-2 BNT162b2 vaccine. EClinicalMedicine. 2021;36:100928. doi:10.1016/j.eclinm.2021.100928
53. Flanagan KL, Fink AL, Plebanski M, Klein SL. Sex and Gender Differences in the Outcomes of Vaccination over the Life Course. Annu Rev Cell Dev Biol. 2017;33:577–599. doi:10.1146/annurev-cellbio-100616-060718
54. Alpert A, Pickman Y, Leipold M, et al. A clinically meaningful metric of immune age derived from high-dimensional longitudinal monitoring. Nat Med. 2019;25(3):487–495. doi:10.1038/s41591-019-0381-y
55. Ali H, Alahmad B, Al-Shammari AA, et al. Previous COVID-19 Infection and Antibody Levels After Vaccination. Front Public Health. 2021;9:778243. doi:10.3389/fpubh.2021.778243
56. Manisty C, Otter AD, Treibel TA, et al. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet. 2021;397(10279):1057–1058. doi:10.1016/S0140-6736(21)00501-8
57. Guo J, Li L, Wu Q, et al. Detection and predictors of anti-SARS-CoV-2 antibody levels in COVID-19 patients at 8 months after symptom onset. Future Virol. 2021;16(12):795. doi:10.2217/fvl-2021-0141
58. Purushotham JN, van Doremalen N, Munster VJ. SARS-CoV-2 vaccines: anamnestic response in previously infected recipients. Cell Res. 2021;31(8):827–828. doi:10.1038/s41422-021-00516-7
59. Schwarzkopf S, Krawczyk A, Knop D, et al. Cellular Immunity in COVID-19 Convalescents with PCR-Confirmed Infection but with Undetectable SARS-CoV-2-Specific IgG. Emerg Infect Dis. 2021;27(1):122–129. doi:10.3201/2701.203772
60. Arya R, Kumari S, Pandey B, et al. Structural insights into SARS-CoV-2 proteins. J Mol Biol. 2021;433(2):166725. doi:10.1016/j.jmb.2020.11.024
61. Shah VK, Firmal P, Alam A, Ganguly D, Chattopadhyay S. Overview of Immune Response During SARS-CoV-2 Infection: lessons From the Past. Front Immunol. 2020;11:11. doi:10.3389/fimmu.2020.00011
62. Huțanu A, Dobreanu M. Antibody Response After Sars-Cov-2 mRNA Vaccine In Naïve And Previously Infected Healthcare Workers. Health Problems Civilization. 2021;16(1):48–56. doi:10.5114/hpc.2021.111783
63. Wang Z, Schmidt F, Weisblum Y, et al. mRNA vaccine-elicited antibodies to SARS-CoV-2 and circulating variants. Nature. 2021;592(7855):616–622. doi:10.1038/s41586-021-03324-6
64. Xie X, Liu Y, Liu J, et al. Neutralization of SARS-CoV-2 spike 69/70 deletion, E484K and N501Y variants by BNT162b2 vaccine-elicited sera. Nat Med. 2021;27(4):620–621. doi:10.1038/s41591-021-01270-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.