")
Back to Journals » Patient Preference and Adherence » Volume 12
The level of awareness and the attitude of patients recommended for use of compression stockings in Turkish society, and investigation of the factors affecting their use
Authors Manduz Ş , Ada F , Ada Y
Received 17 November 2017
Accepted for publication 31 December 2017
Published 16 March 2018 Volume 2018:12 Pages 399—407
DOI https://doi.org/10.2147/PPA.S157344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Şinasi Manduz,1 Fatih Ada,1 Yusuf Ada2
1Cardiovascular Surgery Department, Cumhuriyet University School of Medicine, Sivas, Turkey; 2Department of Business Administration, Cumhuriyet University Faculty of Economics and Administrative Sciences, Sivas, Turkey
Objective: The purpose of this study was to reveal the treatment outlook, usage habits, and factors affecting these habits, in addition to providing suggestions for solutions for patients who are frequently recommended the use of compression stockings as treatment for conditions such as chronic venous insufficiency, deep vein thrombosis, lymphedema, and pregnancy.
Methods: The study was conducted as a face-to-face questionnaire session with 1,004 patients who had previously registered at the cardiovascular surgeon’s polyclinic of Sivas Numune Hospital between March 29, 2017, and October 31, 2017. In the study, basic criteria such as the patients’ history, physical examination findings, and the use of compression stockings were evaluated. The survey was conducted in patients who were recommended compression stockings treatment for conditions such as chronic venous insufficiency, deep vein thrombosis, lymphedema, or pregnancy. The patients were asked about their demographics, characteristics of the compression stockings, whether compression stockings were used or not, and doctor evaluations related to the diagnosis.
Results: At the end of the study, it was found that 20.5% of the patients who were recommended compression stockings never bought them and only 11.5% of the patients regularly used them. Another surprising detail was that only 54.7% of the patients thought that the compression stockings were part of the treatment and 44.0% of the patients thought that they would benefit from using them.
Conclusion: In many guidelines, use of compression stockings is the cornerstone of treatment of venous diseases. However, when the treatment incompatibility of the patients is taken into account, many duties fall to the doctors. The first of these is to inform the patient about the treatment and to answer any questions from the patients. In addition, the socioeconomic and sociocultural status of patients should be considered by the doctors.
Keywords: venous insufficiency, varicose veins, pregnancy, compression therapy, compression stockings
Introduction
Compression stockings are recommended during pregnancy as well as in patients with diseases such as chronic venous insufficiency, deep vein thrombosis, and lymphedema, which are common worldwide.1–4 Compression stockings treatment is also widely recommended and used in clinical practice. However, the most crucial problem in this treatment is patient incompliance. This incompliance is often manifested as not applying the treatment, as well as discontinuation of treatment once it has been practiced, often only once or several times. It is not clear whether this incompliance is due to patients’ mind-set, the features of compression stockings, or the wrong compression stocking recommendation. In addition, compression stockings are either never reimbursed or only partly reimbursed by health insurers in Turkey. There are very few studies in the literature on the compliance of patients related to the use of compression stockings.5–7 Most of the studies in the literature have focused on the physiological effects of compression stockings, the use of compression stockings after surgery, and their use after sclerotherapy.8 The purpose of this study was to see the source of incompliance and to propose solutions.
Aims of the study
Primary aim
The purpose of this study was to try to reveal the treatment outlook, usage habits, and factors affecting these habits for the group of patients who are frequently recommended the use of compression stockings for treatment of conditions such as chronic venous insufficiency, acute–subacute–chronic deep vein thrombosis, lymphedema, and pregnancy.
Secondary aim
It is observed that in terms of the use of compression stockings in the clinic, these patient groups are very incompliant. The study aimed to promote the habits of usage and determine the causes of incompliance.
Methods
In the market, there are many types of and varying prices for compression stockings. However, patient incompliance is frequently encountered in treatment. A survey was conducted to investigate the causes of this incompliance and to proffer recommendations for solutions. The study was conducted as face-to-face interviews with 1,004 patients who had previously registered at the cardiovascular surgeon’s polyclinic of Sivas Numune Hospital between March 29, 2017, and October 31, 2017. In the study, basic criteria such as patients’ history, physical examination findings, Doppler ultrasonography results, lymphoscintigraphy results, beta human chorionic gonadotropin (hCG) results, pregnancy status, and compression stockings usage patterns were evaluated. The participants were neither charged any amount nor paid any fees. The proposed compression stockings were manufactured by all brands in the market. Clinical indications and disease stages of patients (often classified using the clinical, etiologic, anatomic, and pathophysiologic [CEAP] system) were diagnosed after physical examination and anamnesis evaluation by physicians specializing in cardiovascular surgery.
Preparing the questionnaire
The questionnaire consists of demographic data of the patients, the medical reason for the recommendation of the compression stockings, the characteristics of the compression stockings, their usage pattern, and the period of compression stockings use. The most recent compression stockings usage period was characterized as follows:
- Compression stockings were suggested to the patient, but the patient may not have bought them.
- The patient was recommended compression stockings; the patient bought the stockings but did not use them within the recommended time frame or follow appropriate rules.
- The patient was recommended compression stockings; the patient bought the stockings, and used them within the recommended time frame and followed appropriate rules.
- The patient was recommended compression stockings; the patient bought the stockings and continues using them irregularly.
- The patient was recommended compression stockings; the patient bought the stockings and continues to use them regularly.
There are subsections in these 5 items. These subsections consist of 2 main headings. First among these included the following queries: why did you not ever buy them? Why did you use them irregularly and discontinue their usage? Why did you use them regularly and discontinue their usage? Why do you use them occasionally? Why do you use them regularly? The second heading consisted of questions with proposals for solutions.
Patient population
The survey was conducted as a face-to-face interview of 1,004 persons who had registered at the Polyclinic of Cardiovascular Surgery of Sivas Numune Hospital between March 29, 2017, and October 31, 2017 and the study was approved by the Ethics Committee of Non-invasive Clinical Investigations of Cumhuriyet University (number 2017-04/06). Written informed consent was obtained from all patients.
Inclusion criteria
- To be included in the study, patients should have had any one of the following: chronic venous insufficiency, acute–subacute–chronic deep vein thrombosis, lymphedema, or pregnancy.
- The patients diagnosed with these conditions should have been recommended compression stockings.
Exclusion criteria
- Patients who were not recommended compression stockings although having been diagnosed with one of the following: chronic venous insufficiency, acute–subacute–chronic deep vein thrombosis, lymphedema, or pregnancy.
- Patients who were diagnosed with chronic venous insufficiency, deep vein thrombosis, lymphedema, or pregnancy and for whom compression stockings were recommended and who had previously participated in the same questionnaire survey (patients coming as controls).
Statistical analysis
In the study, continuous variables were expressed as mean ± SD and categorical variables as frequency and percentage. SPSS 24 package statistical program (StataCorp LP, College Station, TX, USA) was used for descriptive statistics and CI calculations.
Results
A total of 1,004 patients were included in the study. Of these, 71.0% of the patients were women and 29.0% of the patients were men. The mean age of the participants was 47.24±13.69 years. The majority of the patients were in C2 and C3 stages according to the CEAP classification, and 78.8% had previously received medical treatment for venous insufficiency (Table 1). Mean duration of illness was 3,554.39±3,434.49 days; the mean usage time of compression stockings was 320.13±1,039.04 days, and the mean body mass index was 30.17±5.88 (Table 2). Moreover, 55.4% of the patients were primary school graduates and 61.0% were housewives (Tables 3 and 4). When the indications for compression stockings were examined, edema (52.6%) and varicose veins (50.5%) were found to be the first 2 indications and the last in the order was lymphedema (1.5%; Table 5). The most surprising result from the questionnaire was that only 54.7% of the patients who had compression stockings knew that the stockings were part of the treatment, 35.3% did not know, 10.1% did not have an opinion; furthermore, 44.0% thought that it contributed or would contribute to the treatment, 42.9% thought that it did not contributes and would not contribute, and 13.1% did not have an opinion. These percentages were not present in previous studies; in fact, these studies summarized data on patients, presenting either scanty or secondhand information as well as an overview of the treatment using compression stockings. The compression stockings recommended by the physicians included those with medium pressure on lap (42.7%), medium pressure mid-calf (22.9%), and pantyhose medium pressure stockings (18.9%). The stockings bought by the patients comprised the following types: 37.7% were medium pressure on lap, 27.4% were medium pressure mid-calf, and 19.9% were pantyhose medium pressure stockings (Table 6). The recommended stockings and different models that were bought were similar. Further, 75.1% of the patients were given training before buying stockings and 24.9% were not; 87.2% of the patients used leg measurements and 12.8% of them did not, while buying compression stockings; 83.8% of the patients stated that they wore compression stockings according to the rules (putting on immediately after waking up from bed and taking off when going to sleep in bed) and 16.2% did not wear them according to the rules. For the question on who gave the training for use of compression stockings, the responses were medical sales representative (91.6%), doctor (7.4%), and nurse (1%). When the frequency of use is considered, 11.6% of patients wore stockings once or several times a year, 11.0% once or several times a week, and 8.6% once or several times a month (Table 7). When the patients’ usage period of compression stockings was taken into account, 35.3% of the patients were first using stockings irregularly and thereafter discontinued use, while 20.5% of the patients were at the bottom of the group with no compression stockings use despite being recommended and 11.5% of patients continued to use it regularly (Figure 1).
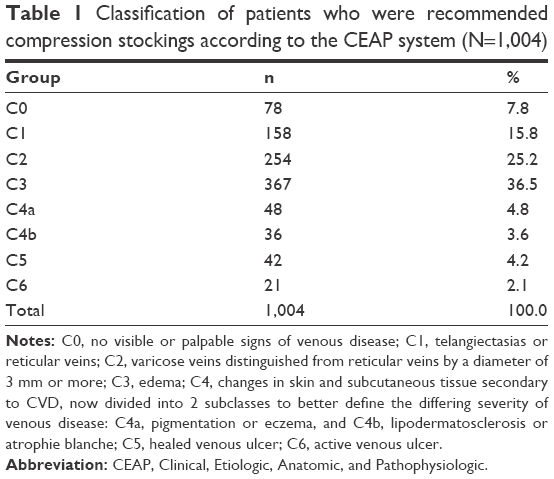 | Table 1 Classification of patients who were recommended compression stockings according to the CEAP system (N=1,004) |
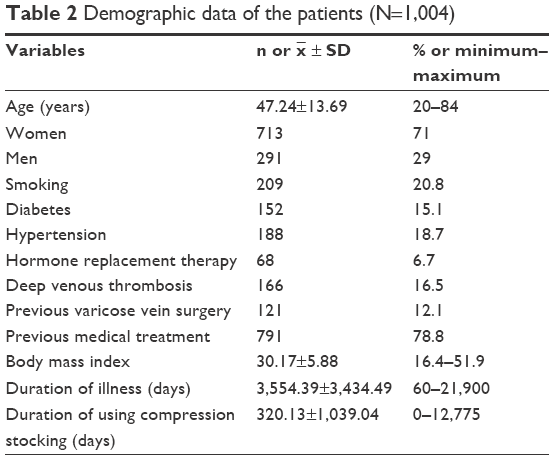 | Table 2 Demographic data of the patients (N=1,004) |
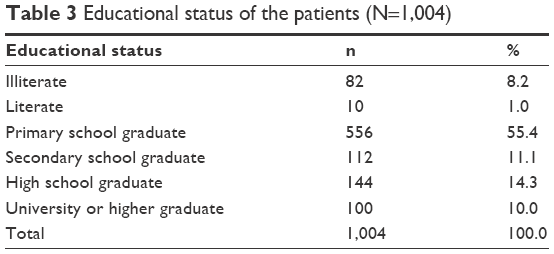 | Table 3 Educational status of the patients (N=1,004) |
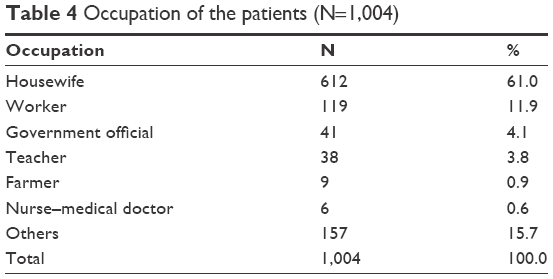 | Table 4 Occupation of the patients (N=1,004) |
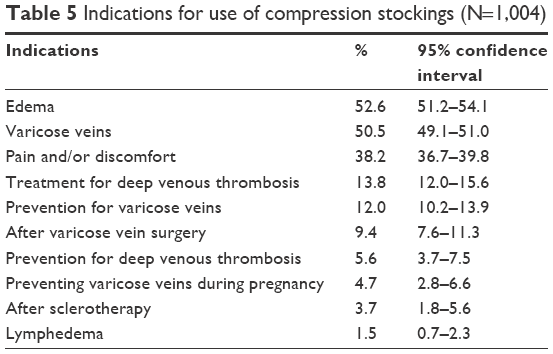 | Table 5 Indications for use of compression stockings (N=1,004) |
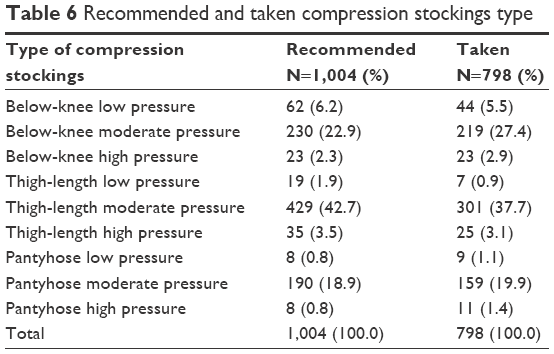 | Table 6 Recommended and taken compression stockings type |
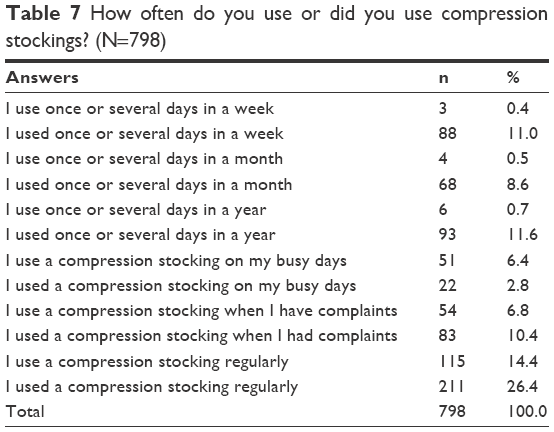 | Table 7 How often do you use or did you use compression stockings? (N=798) |
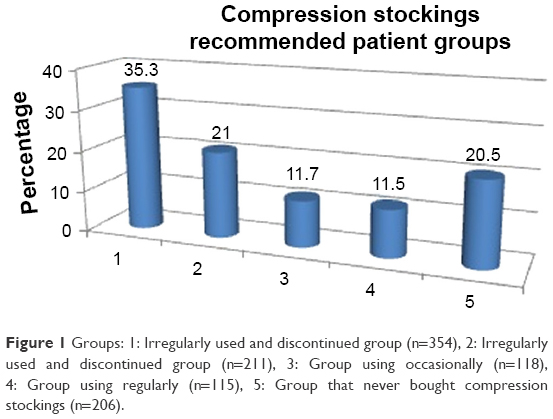 | Figure 1 Groups: 1: Irregularly used and discontinued group (n=354), 2: Irregularly used and discontinued group (n=211), 3: Group using occasionally (n=118), 4: Group using regularly (n=115), 5: Group that never bought compression stockings (n=206). |
After this step, 5 periods of use are presented at the end of each period; part A determined the reason for using or not using in each period and part B consisted of the solution recommendations.
The 3 most frequent reasons for irregular use and discontinuation are as follows: they are very tight (50.3%), they prevented performing ablutions (29.1%), and they are hard to use (24.3%). Solution recommendations yielded the following responses: I would continue if they were more useful (57.9%); I would continue if they did not prevent me from performing ablutions (26.8%), and I would continue if they were physically more comfortable (14.1%; Table 8A and B).
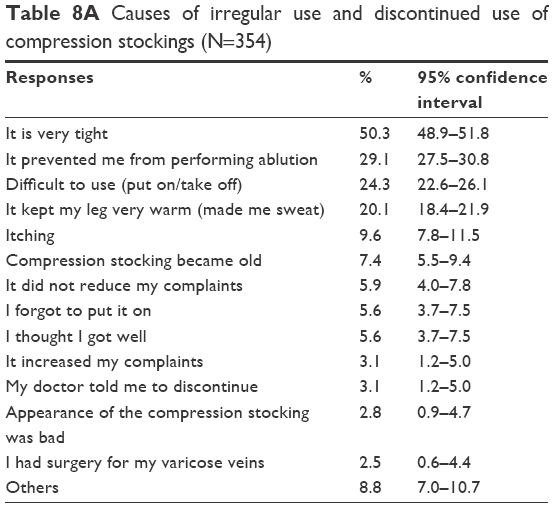 | Table 8A Causes of irregular use and discontinued use of compression stockings (N=354) |
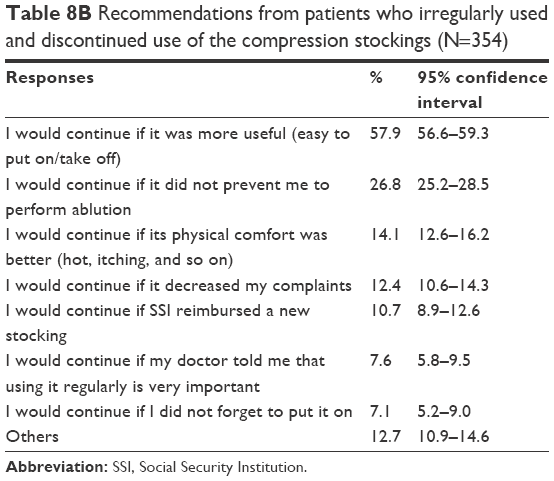 | Table 8B Rrecommendations from patients who irregularly used and discontinued use of the compression stockings (Nn=354) |
According to this study, the 3 most frequent reasons in the regularly using and discontinued groups are as follows: 30.3%, stockings are very tight; 26.6%, compression stockings became old; 19.0%, stockings are hard to use. In terms of solution recommendations, 41.2% said that they would continue if it was more useful, 28.4% that they would continue if Social Security Institution (SSI) would reimburse a new stocking, and 25.6% reported that they would continue if their doctor told them that using it regularly is very important (Table 9A and B).
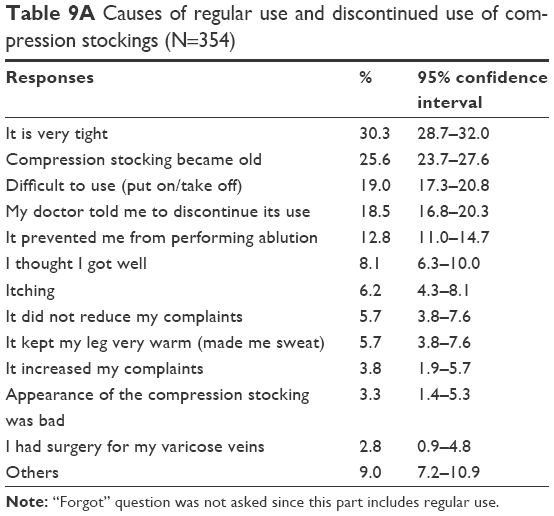 | Table 9A Causes of regular use and discontinued use of compression stockings (N=354) |
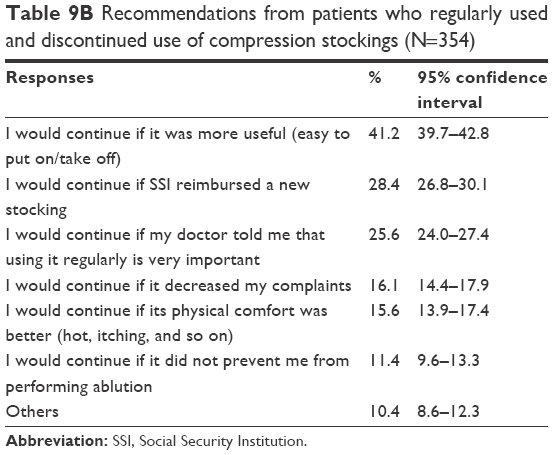 | Table 9B Recommendations from patients who regularly used and discontinued use of compression stockings (N=354) |
The 3 most frequent causes in the occasional-use group are as follows: very tight (49.2%), hard to use (29.7%), and prevention from performing ablutions (19.5%). In terms of solutions, the responses were as follows: I would continue if it was more useful (39.8%), I would continue if it was physically more comfortable (21.2%), and I would continue if it does not prevent me from performing ablutions (16.9%; Table 10A and B).
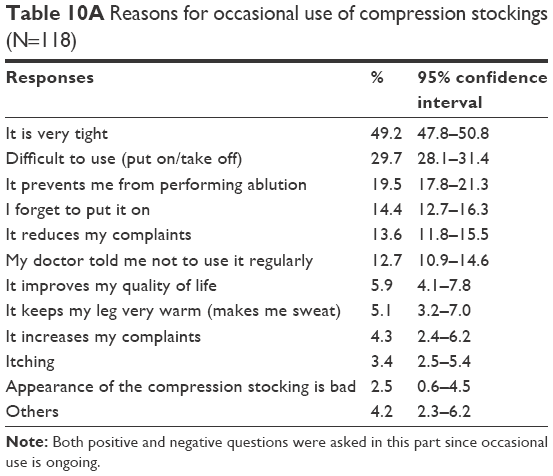 | Table 10A Reasons for occasional use of compression stockings (N=118) |
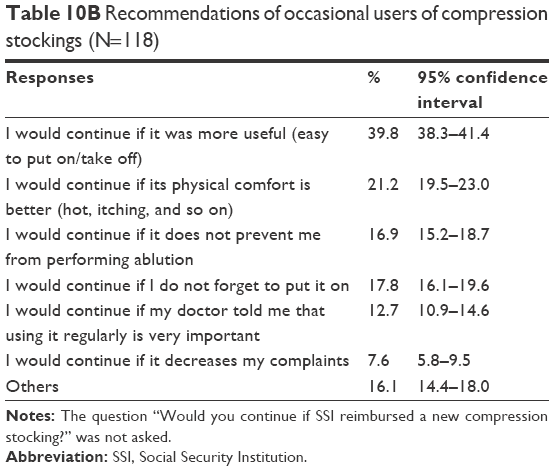 | Table 10B Recommendations of occasional users of compression stockings (N=118) |
The group that continued to use stockings regularly was asked the reason for their continued regular use and their recommendations. The reasons received are: they reduce my complaints (73.9%), my doctor tells me to use them regularly (47.8%), and they improve the quality of my life (10.4%). In terms of recommendations, the responses were they would be better if they were more useful (47.8%); they would be better if they did not prevent me performing ablutions (29.6%), and they would be better if made in a different color, in a different model, and with different materials (25.2%; Table 11A and B).
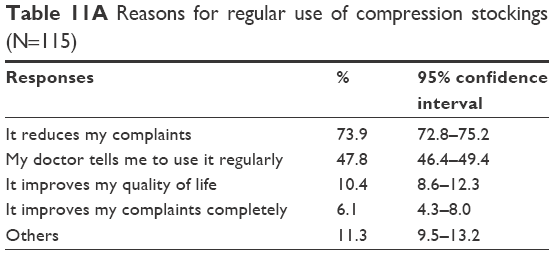 | Table 11A Reasons for regular use of compression stockings (N=115) |
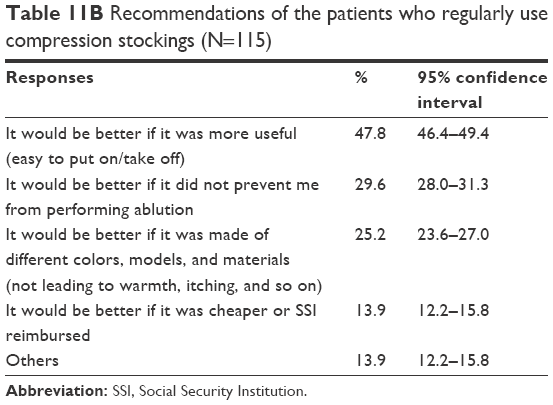 | Table 11B Recommendations of the patients who regularly use compression stockings (N=115) |
The patients in the group that did not buy any compression stockings were asked why they never bought the stockings and their recommendations. The following responses were obtained: I thought it would be difficult to use it (38.3%); it was expensive (27.2%); and those who used it told me that it was useless (22.3%). The recommendations obtained were as follows: I would buy it if it was cheaper or if SSI reimbursed the expense (40.3%), I would buy it if I knew I could use it (39.3%), and I would buy it if I knew it would not make me feel very hot and was not very tight (17.5%; Table 12A and B).
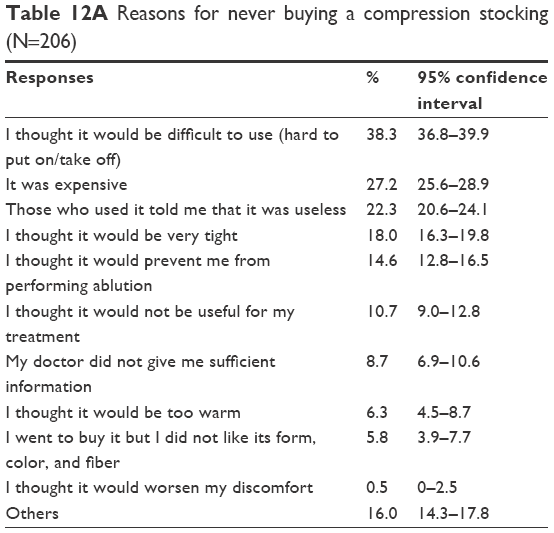 | Table 12A Reasons for never buying a compression stocking (N=206) |
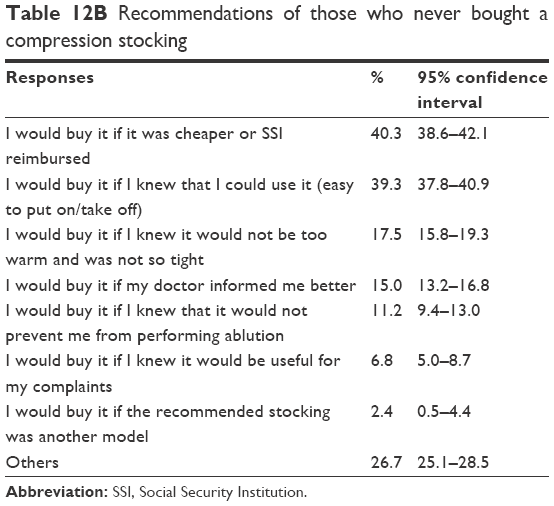 | Table 12B Recommendations of those who never bought a compression stocking |
Discussion
With this study, data on the treatment and the use of compression stockings in Turkish society were obtained. First, 79.5% of the patients who were recommended compression stockings bought them and 20.5% of them did not buy them. Considering the usage proportions, it seems that treatment with compression stockings is accepted by the vast majority of patients. This ratio is close to that of Cataldo et al (89.3%), but the difference can be explained by the economic and cultural differences between the 2 countries.9 Most of the patients were female, housewives, had low educational level, and were obese or morbidly obese. These rates were similar in a study conducted by Yilmaz et al in Turkey.10 This result can be explained by the sedentary living and feeding habits in the working population. In our study, the most common indications for the recommendation of compression stockings to patients were edema, varicose veins, and pain, as well as discomfort.
One of the interesting aspects of the data obtained in this study is the incredible difference between the total duration of illness and the total duration of compression stockings use. A similar rate has not been found in previous studies: the mean duration of illness was 3,554.39±3,434.49 days and the average duration of compression stockings use was 320.13±1,039.04 days. There is incompatibility of >10 times between them. It is obvious that not using the treatment in the recommended time frame will contribute to the progress of the disease, but it also increases unnecessary hospital admissions.
Considering the ratios of bought compression stockings to recommended compression stockings, it was seen that a large proportion of the patients bought the compression stockings recommended by the physicians. One interesting aspect is that most of the patients bought compression stockings and used these stockings only once, or all the time. This contributes to the inadequacy of treatment, as well as the destruction of both the country’s economy and the individual assets.
One of the main aims of this study was to find answers to some of the questions regarding why some patients continue to use compression stockings on a regular basis, while others never buy them, or why patients discontinue after using them for a while. Therefore, the participants were divided into 5 groups and each group was asked to put forward the major problems and the solution recommendations for the problems.
The group with irregular users from these groups accounted for 35.3% of the patients who were recommended compression stockings, and this was the highest proportion among the 5 groups. Almost half of the patients complained that the compression stockings were very tight, 1 in 3 patients stated that it prevented performing ablutions, 1 in 4 patients stated the difficulty of use, and 1 in 5 patients complained about keeping the legs warm. In the solution recommendation, in the first place was the availability of a stocking that was easier to put on and take off; a stocking that did not prevent performing ablutions was in the third place; availability of a stocking that is not itchy and does not keep legs warm was also present. It was seen that this group supported irregular use and part of the solution recommendation. It may be a logical choice for this group to regularly use the prescription of lower-pressure, open-toe compression stockings and nonallergic compression stockings, as well as the use of apparatuses that help to put these on.
The second group, comprising regularly using and patients who had discontinued use, accounted for 21.0% of the patients who were recommended compression stockings and was in second place among all groups. The most important complaints in this group were compression stockings are tight, are old, are difficult to use, and the doctor suggested discontinuing it. In this group, 12.8% of the respondents said that it prevented performing ablutions. In the solution recommendations, the most important solutions included the manufacture of a more useful compression stockings, replacement of the old stocking with the new ones by the SSI, and doctor’s recommendation to continue using it. Considering the reasons for discontinuing its use in this group and considering the solution proposal, excess stockings pressure was seen as the main problem, but it was seen that the economic reasons and the results of the physician’s recommendations were influential.
The third group consisted of patients who were still using it on an intermittent basis. This group accounted for 11.7% of all patients. The main problem in this group was that the compression stockings were very tight. The subsequent problem was the stocking being difficult to wear and preventing the performance of ablutions. The percentage of those who stated that they did not use stockings regularly because they forgot to wear them was 14.4%. Solutions with the top rankings included stockings being more useful, stockings with good physical comfort, and a stocking that would not prevent ablutions. Regarding the ratios of groups that continued to use these intermittently and the irregular-user group, both the complaints and the solutions suggested were similar.
The fourth group was still continuing to use stockings regularly; the group included the least patients (11.5%). In this group, the reason for the regular usage in spite of the complaints and the characteristics that were better in compression stockings were investigated. Thus, 73.9% of the patients stated that they used it because it reduced their complaints, 47.8% said they continued to use it because their doctor recommended to them to continue using it, and 10.4% use it because it increased the quality of their lives. Only 6.1% of the patients reported that their complaints had completely gone through use of compression stockings. A compression stocking that is easier to wear and take off, a stocking that does not prevent performing ablutions, and a stocking in various models were the most important suggestions.
The fifth group was the second largest group, and although the compression stockings were suggested, they never bought them. The remarkable fact here is that 20.5% of the group never bought it, meaning that 1 in 5 patients never gets treatment and this is a fairly high ratio. The most common reason was that the patients most often thought that it would be difficult to put on and take off; next was that the stockings were expensive and that people who used them said that they did not work at all. “I would buy them if the stockings were cheaper or if the SSI reimburses them” was the response in the first place, and “I would buy it if it was easier to put them on and take off” was the answer in the second place. In this group, the reasons for not buying were more of an economic nature. In fact, if we were to interpret it in comparison with other groups, even if these patients bought compression stockings, a very high rate of them would probably stop using them soon.
Currently, billions of people from many different races, beliefs, and nations live together. These unifications propel us to be able to learn many different cultures.
In Muslim societies, ablution is a prerequisite for prayer/worship. One of the requirements of ablution is to wipe both feet up to the heel 3 times. Considering that this prayer is made at least 5 times a day, it is a big mistake to expect compliance to compression stockings. Therefore, if there is no medical necessity, suggestions of either open-ended or zippered compression stockings by the physicians will be appropriate for Muslim patients.
While each group has its own reasons and recommendations, it is seen that the 3 most important factors in general are economic situation, patient information, and sociocultural status of patients. In addition, physicians should pay particular attention to pressure when prescribing compression stockings; it may be more effective to use lower pressure stockings in the beginning phase or for protection purposes.
Conclusion
Thus, treatment of patients by physicians with compression stockings should consider many factors. It is necessary to evaluate the stage of the disease, economic status, beliefs, habits, allergic nature, geography and climate of residence, and many other factors collectively by the physician and patient and thereafter make the choice of the right compression stockings by consensus.
Acknowledgments
We would like to thank all participants for their patience and sincerity in cooperating as a working team. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
Nicolaides A, Allegra C, Bergan J, et al. Management of chronic venous disorders of the lower limbs guidelines according to scientific evidence. Int Angiol. 2008;27(1):1–59. | ||
Wittens C, Davies AH, Bækgaard N, et al. Management of chronic venous disease: clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2015;49(6):678–737. | ||
Marsden G, Perry M, Kelley K, Davies AH; Guideline Development Group. Diagnosis and management of varicose veins in the legs: summary of NICE guidance. BMJ. 2013;347:f4279. | ||
Partsch H, Flour M, Smith PC; International Compression Club. Indications for compression therapy in venous and lymphatic disease consensus based on experimental data and scientific evidence. Under the auspices of the IUP. Int Angiol. 2008;27(3):193–219. | ||
Ziaja D, Kocełak P, Chudek J, Ziaja K. Compliance with compression stockings in patients with chronic venous disorders. Phlebology. 2011;26(8):353–360. | ||
Carpentier PH, Becker F, Thiney G, Poensin D, Satger B. Acceptability and practicability of elastic compression stockings in the elderly: a randomized controlled evaluation. Phlebology. 2011;26(3):107–113. | ||
Allegra C, Antignani PL, Will K, Allaert F. Acceptance, compliance and effects of compression stockings on venous functional symptoms and quality of life of Italian pregnant women. Int Angiol. 2014;33(4):357–364. | ||
Ashby RL, Gabe R, Ali S, et al. Clinical and cost-effectiveness of compression hosiery versus compression bandages in treatment of venous leg ulcers (Venous leg Ulcer Study IV, VenUS IV): a randomised controlled trial. Lancet. 2014;383(9920):871–879. | ||
Cataldo JL, De Godoy JM, De Barros N. The use of compression stockings for venous disorders in Brazil. Phlebology. 2012;27(1):33–40. | ||
Yilmaz S, Yaylaci S, Diken AI, et al. Compression stockings and the factors that affect their use in lower extremity venous insufficiency treatment. Damar Cer Derg. 2015;24(1):47–53. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.