")
Back to Journals » Psychology Research and Behavior Management » Volume 15
The Influence of Stereotypes on Trust in Doctors from Patients’ Perspective: The Mediating Role of Communication
Authors Su F , Wang Y, Wu Q, Wang PJ, Chang X
Received 8 September 2022
Accepted for publication 29 November 2022
Published 15 December 2022 Volume 2022:15 Pages 3663—3671
DOI https://doi.org/10.2147/PRBM.S389202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Fan Su,1,* Yao Wang,2,* Qing Wu,2 Pei-Juan Wang,1 Xin Chang1
1School of Foreign Languages, Tongji University, Shanghai, People’s Republic of China; 2Faculty of Education, East China Normal University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xin Chang, School of Foreign Languages, Tongji University, Shanghai, 200092, People’s Republic of China, Email [email protected]
Purpose: To investigate the relationship among patients’ stereotypes of doctors, effectiveness of doctors’ communication skills evaluated by patients, and patients’ trust in doctors.
Patients and Methods: A cross-sectional survey with a total of 3289 patients from 103 hospitals in eastern, central and western China was conducted.
Results: There were strong correlations among patients’ stereotypes, patients’ evaluation on doctors’ communication skills, and patients’ trust (r = 0.50– 0.67, p < 0.01 for all). Patients’ trust was predicted by patients’ stereotypes directly (β = 0.32, 95% CI: 0.27– 0.37) and indirectly (β = 0.19, 95% CI: 0.16– 0.23) through patients’ evaluation on doctors’ communication skills.
Conclusion: Both patients’ stereotypes and patients’ evaluation on doctors’ communication skills have predictive effects on patients’ trust. Patients’ stereotypes are not only a direct predictor of patients’ trust but also an indirect predictor via doctors’ communication skills as a mediator. This national survey underlines the significance of patients’ stereotypes, and emphasizes the importance of developing doctors’ communication skills on patients’ trust. In order to build a more trustful doctor–patient relationship, there should be a joint effort at social and individual level to reinforce positive impression and suppress negative stereotypes of doctors. As far as communication skills are concerned, doctors are encouraged to use helpful verbal and nonverbal techniques that benefit their profession impression management.
Keywords: patients’ trust, patients’ stereotypes, doctors’ communication skills
Introduction
Doctor–patient relationship has been considered as a major sociological concern across world, China being no exception.1,2 Under post-pandemic era, medical conflicts still happen in a high frequency and even threaten doctors’ lives.3 For example, on January 26th, 2021, Dr. Hu, a cardiologist, was severely cut by his patient and did not survive after rescue. Just one day later, Dr. Zeng was vengefully stabbed by her inpatient with a syringe.3 Although it seems that in China there is a general increase in people’s trust in doctors after COVID-19,4–6 much evidence has been shown for medical disputes or violence against doctors.7,8 Furthermore, mistrust was indicated by Liu’s team to be one of patients’ factors in medical disputes.8 In other words, the loss of trust in doctors seems to have led to an increase in medical disputes and violence. In order to better resolve the problems between doctors and patients, it is high time to rethink patients’ trust, a promoting technology in the mechanism of the harmonious doctor–patient relationship.9,10 Patients’ trust can be defined as the optimistic acceptance of a vulnerable situation, in which patients believe their physician will care for their interests.11 If patients trust their doctors in vulnerable situations, they will feel less worried or anxious,12,13 enjoy more shared decision-making14 and adhere more to their doctors’ recommendations,15 which benefits doctor–patient relationship. On the contrary, a low degree of patient trust is likely to cause tension between doctors and patients, consequentially deteriorating the relationship between them.16 Therefore, patients’ trust has long been proposed as a key component in good doctor–patient relationship.17
Recent research has shown that, on influencing trust, one of the determinants is stereotype.18–20 A standard definition of stereotype is the belief about the characteristics, attributes, and behaviors of members of certain group.21 These beliefs are sometimes accurate representations of reality, but usually not accurate, particularly in relation to individual group members.22,23 In a medical context, doctors are vulnerable to patients’ stereotypes, as these preexisting beliefs can impact mutual trust and the related health care.24 For example, previous studies provided some evidence of the effect of doctors’ negative stereotypes (eg, ignorant) on older patients, so doctors often doubted elders’ willingness and ability to follow their advice, thus becoming cynical and distrustful of those patients.25–27 Similarly, patients also have stereotypes about doctors and these can affect their perceived trust and their intention to visit.24 Doctors as a profession are generally tagged by occupational stereotypes like “competent”, “warm”, but “unemotional” and these mixed stereotypes will bring about uncertain effects on patients’ trust level.28,29 Negative stereotypes are likely to keep patients defensive and vigilant, lower their trust, which in turn influences doctors’ behaviors, thus forming a vicious circle and maintaining the original negative stereotypes.30 Positive stereotypes held by patients, such as stereotypical traits of warmth and competence as doctor professionalism, are closely related to their perception of trustworthiness and preference for hospital selection.31
Except patients’ stereotypes of doctors, it is noted that doctors’ communication skills play a vital role in building patient trust.32 A doctor’s communication skills involve the ability to gather information with the purpose of accurate diagnosis, appropriate counseling, effective therapeutic instructions, and caring relationships with patients.33 Evidence showed that skillful and adequate communication can in the long run produce better health outcomes and in the short run influence health outcomes via the indirect route of patient trust.34,35 Other studies also found correlations between doctors’ communication skills and patient trust.36,37 For example, a study showed that doctors’ communication skills are positively associated with patients’ trust. In this study, patients were asked to take a “trust game” and rate four aspects of doctors’ communication skills during the consultation (greeting them, looking at them while speaking, providing information, and telling them when to return). Results demonstrated that higher levels of trust were found for doctors with better communication skills.36
As mentioned above, it is worth noting that both patients’ stereotypes and doctors’ communication skills were suggested to be factors that may influence patients’ trust. Additionally, some studies have further discussed the association of patients’ stereotypes and patients’ evaluation on doctors’ communication skills. One of the studies on patients’ stereotypes of surgeons as both warm and competent suggested that these positive stereotypes may lead patients to interpret doctors’ paternalistic communication (eg, “do as I say and you will be healed”) as a sign of confidence and concern for patient well-being, rather than arrogance or lacking empathic concern.38 Besides, it has been proposed that communication styles are related to patients’ stereotypes of doctors: male doctors obtain good patient outcomes when verbally expressing patient-centeredness, whereas female doctors have patients who report better outcomes when they adapt nonverbal communication to patients’ different needs.39
Studies above suggested that there may be the complicated relationship between patients’ stereotyping of doctors, patients’ evaluation on doctors’ communication skills and patients’ trust: patients’ stereotypes of doctors may influence doctor–patient communication style and adjust patient trust level.39 However, to the best of our knowledge, no studies had explored the relationship among patient stereotypes of doctors, doctors’ communication skills, and patient trust. Therefore, the current study for the first time takes doctors as a whole professional group to explore the relationship among patients’ stereotypes, doctors’ communication skills, and patients’ trust. We hypothesize that both patients’ stereotypes and doctors’ communication skills impact patients’ trust, and patients’ evaluation on doctors’ communication skills plays a mediating role in the association between patients’ stereotypes and patients’ trust.
Materials and Methods
Participants
From September 2019 to February 2020, a nationwide cross-sectional survey was conducted among 3289 patients from 103 hospitals in 28 provinces of China, including Heilongjiang, Jiangsu, Zhejiang, Anhui, Shanghai, Hunan, Yunnan, etc. The survey included eastern developed regions, central sub-developed regions and western underdeveloped regions, covering primary, secondary and tertiary hospitals. Patients provided oral informed consent before they participated in the survey. They filled questionnaires online at their convenience inside hospitals during their visit or afterwards. Questionnaires were distributed and collected by hospital managers. In the procedure, some patients did not fill out all the questions due to reduced time or lacking interest. Invalid questionnaires (extreme values, missing values and same answers) being excluded, a total of 2256 valid questionnaires (68.6% response rate) were at last obtained for follow-up data analysis. All data were collected anonymously and kept confidential. The study was implemented with the permission of the Ethics Committee of Shanghai Normal University.
Measures
Questionnaires used in the current study are as follows:
The self-developed measurement tool for stereotypes of doctor role perception compiled by Qu and Ye was used as the questionnaire to study patients’ stereotypes in role perception of doctors.40 It contained 24 items in 3 domains: professional image (1–9), professional self-discipline (10–17), and professional accomplishment (18–24). The total score of this scale ranges from 24 to 120. Higher scores reflect more positive stereotypes of doctors as a professional group. With good reliability and validity, the scale can be applied in studying patients’ stereotypes of doctors in different groups and different regions in China.40 In this study, the Cronbach’s α was 0.980.
The Chinese Version of SEGUE Framework (C-SEGUE) was adapted to study doctors’ communication skills.41 The original SEGUE Framework is a research-based checklist of medical communication tasks, which has been the most widely used structure for communication skills teaching and assessment in North America.42 It encompasses 5 general areas with 25 items, ie, Set the stage (5 items), Elicit information (10 items), Give information (4 items), Understand the patient’s perspective (4 items), End the encounter (2 items). Each item is scored on a five-point Likert scale (1 = never, 2 = occasionally, 3 = sometimes, 4 = mostly, 5 = all the time). The total score of C-SEGUE ranges from 5 to 125. The higher the total score is, the better communication skills are possessed by doctors. In the present study, this scale was used among patients, which showed patients’ evaluation on doctors’ communication skills. The Cronbach’s α was 0.970.
The Chinese Version of Wake Forest Physician Trust Scale (C-WFPTS) was based on the Wake Forest Physician Trust Scale (WFPTS), a 10-item unidimensional scale that performs well in internal consistency, variability, and discriminability. WFPTS is strongly correlated with satisfaction, desire to remain with a physician, willingness to recommend to friends and not seeking second opinions.43 In 2012, researchers investigated C-WFPTS for evaluating patients’ trust in their physicians in China.44 It consists of two factors labeled “benevolence” and “technical competence”, each having 5 items. Each item uses a five-point Likert scale from “strongly disagree” to “strongly agree”. The total score of C-WFPTS ranges from 10 to 50. Higher scores indicate greater patients’ trust. In this study, the Cronbach’s α was 0.791.
Data Analysis
Data analysis was performed with SPSS Version 23.0. The main variables (patients’ stereotypes, patients’ evaluation on doctors’ communication skills, and patients’ trust) were analyzed with descriptive statistics, and correlations among them were analyzed by Pearson correlation. All the analyzed variables were standardized by z-score transformation. Then, a mediation analysis was conducted to test the mediating effect. We used PROCESS macro, models 4. The process macro provides confidence intervals (CI) using a bootstrap method to assess significance.45 The mediating effect of doctors’ communication skills is significant if 95% CI does not contain the value zero.
Results
Participant Characteristics
Out of 2256 valid questionnaires, 963 (42.7%) were answered by male patients. The age range for participants was 18–95 years old (M = 43.2, SD = 15.9). Patients’ demographic characteristics are summarized in Table 1.
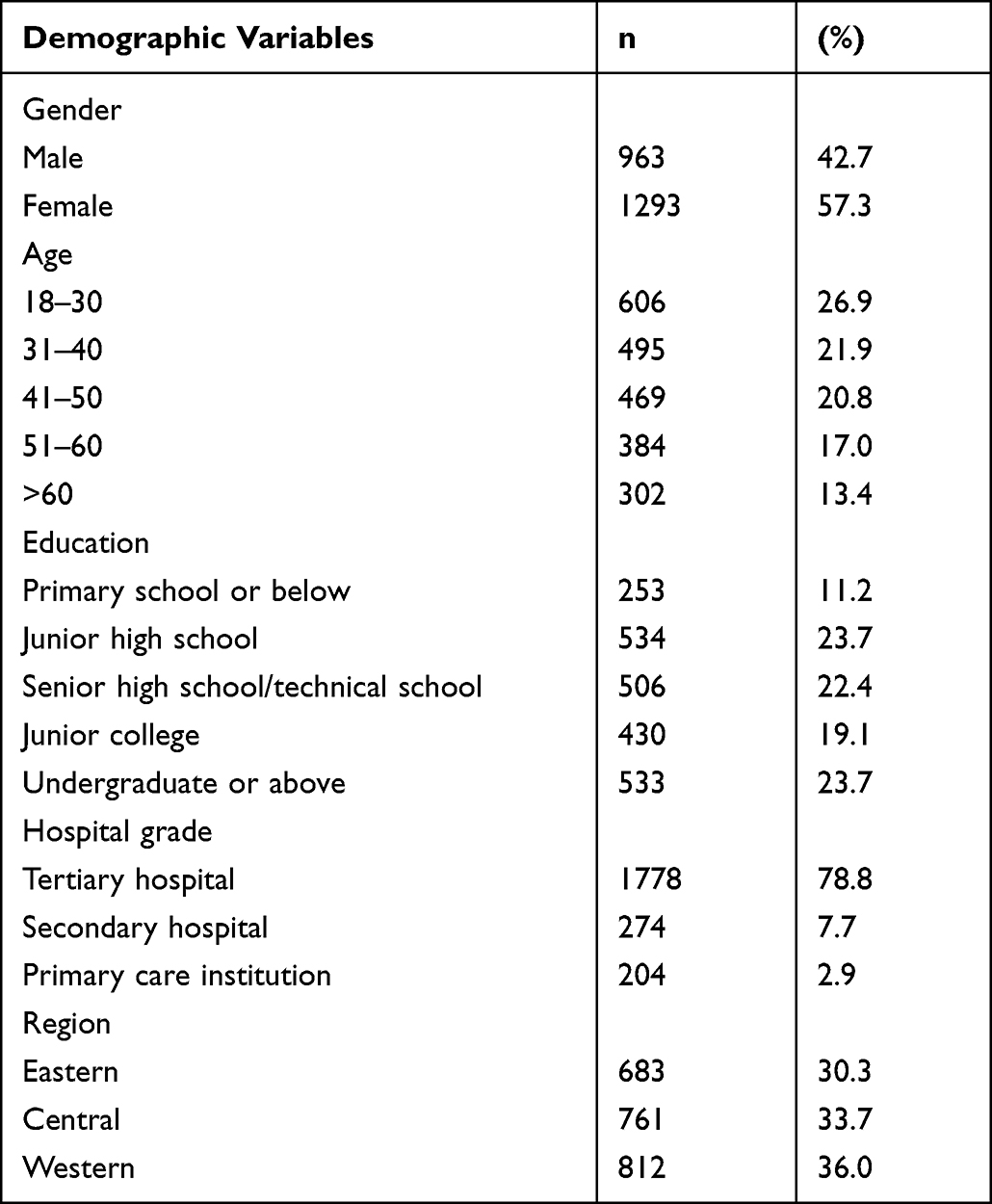 |
Table 1 Demographic Characteristics of Patients (n = 2256) |
Descriptive Statistics and Correlations
Mean scores, standard deviations, and correlations of the three main variables are presented in Table 2. The average score of patients’ overall stereotypes of doctors was 99.48 (SD = 13.18), indicating that patients held moderately positive stereotypes. Again, the mean scores for C-SEGUE 101.11 (SD = 16.32) and for C-WFPTS 38.10 (SD = 5.09) respectively showed the comparatively good current state of doctors’ communication skills and trust from patients’ perspective. As for the relationship among the three variables, results showed that all correlations across these main variables were significantly positive (r = 0.50–0.67, p < 0.01 for all). Specifically, patients’ stereotypes were strongly associated with doctors’ communication skills (r = 0.67, p < 0.01) as well as patient trust (r = 0.52, p < 0.01). Doctors’ communication skills were positively correlated with patients’ trust (r = 0.50, p < 0.01).
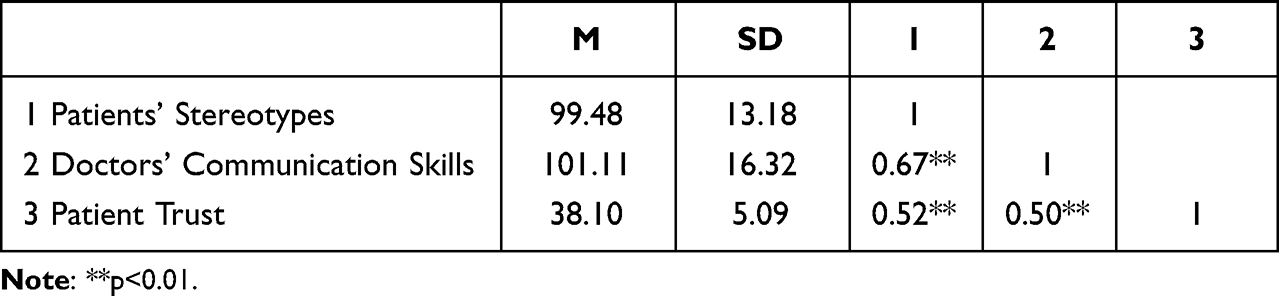 |
Table 2 Mean, Standard Deviations, and Correlations of Three Variables |
Mediation Analysis
A mediation analysis was conducted to test whether the effect of patients’ stereotypes on patients’ trust was mediated by their evaluation on doctors’ communication skills. Results in Table 3 suggested that patients’ stereotypes had significant effect on both doctors’ communication skills (M1) and patients’ trust (M3). When doctors’ communication skills were taken as a mediator in regression equation, both patients’ stereotypes and doctors’ communication skills were still significant predictors of patients’ trust (M2). Figure 1 illustrates a mediational model of the main variables. It was found that patients’ stereotypes had both direct (β = 0.32, p < 0.01) and indirect (β = 0.19, p < 0.01) effect on patients’ trust (F = 509.05, r² = 0.31). The total standardized effect of patients’ stereotypes was strong (β = 0.52, p < 0.01), of which the mediating effect of doctors’ communication skills accounted for 37%. Patients’ stereotypes had greater impact on patients’ trust compared with the intermediate variable, doctors’ communication skills.
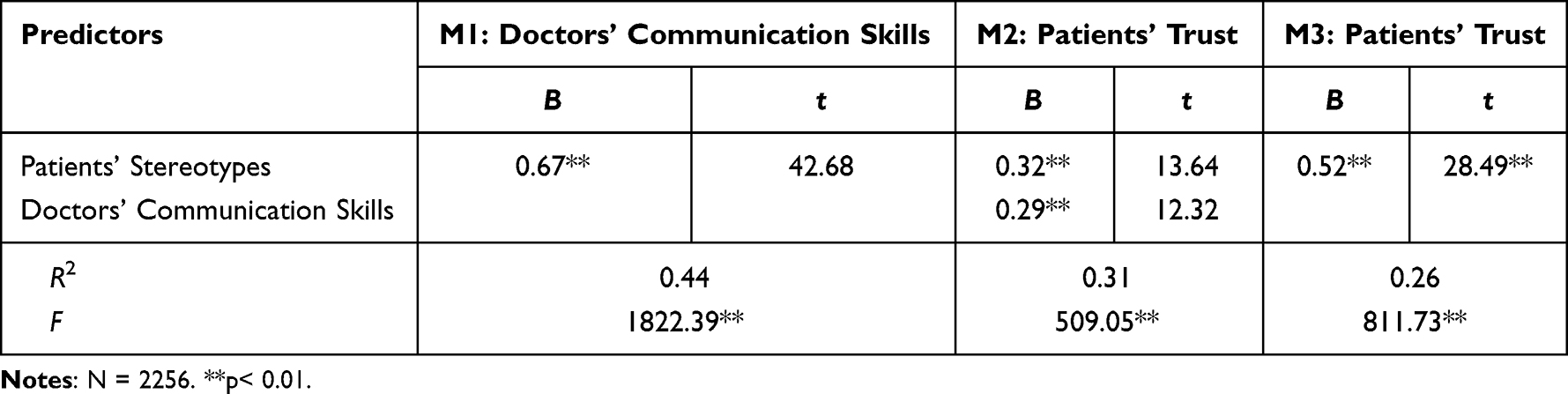 |
Table 3 Mediation Analysis |
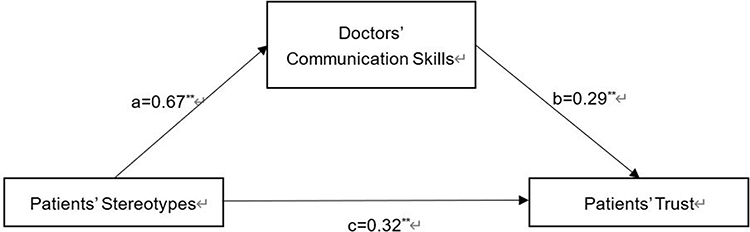 |
Figure 1 Mediating effect of patients’ stereotypes on patients’ trust through doctors’ communication skills. All paths are presented in standardized regression coefficients. The indirect path ab is a product of path a and path b. Direct effect = c: β = 0.32, SE = 0.02, 95% CI [0.27–0.37]. Indirect effect = ab: β = 0.19, SE = 0.02, 95% CI [0.16–0.23]. Total effect = ab+c: β = 0.52, SE = 0.00, 95% CI [0.48–0.55]. **p < 0.01. |
Discussion
The current research examined a new predictor of patients’ trust, patients’ stereotypes of doctors, with patients’ evaluation on doctors’ communication skills as a mediator. In particular, we found that patients’ trust can be strongly predicted by patients’ stereotypes, both directly and indirectly through patients’ evaluation on doctors’ communication skills. The results agree well with our hypothesis.
Previous studies have shown that in the early stages of a relationship, the building of trust is on the basis of cross-group friendship, which is strongly affected by cognitive motivators, such as stereotypes, and affective indicators of intergroup attitudes, such as positive or negative evaluations.46 It is probably not surprising that stereotypes affect intergroup relations. For example, one study on Asian immigrants found that minority group’s perceived stereotype toward the majority group (British citizens) affects their willingness to interact with the outgroup members.47 When people focus on stereotypes, they may act as “detached observers” during cognitive judgment.
In the present study, patients’ stereotypes yielded more association with trust than did patients’ evaluation on doctors’ communication skills. One possible explanation is that Chinese people have more positive stereotypes about doctors in Chinese culture,48 which is also a finding of this study. People have much respect to doctors. Doctors are quite often called “baiyitianshi” (angels in white) as warm, benevolent, and authoritative. Patients who hold these stereotypes tend to assume that doctors are able to show empathy for their sufferings, and they always communicate in a serious and professional manner.49
The current study firstly demonstrates that patients’ evaluation on doctors’ communication skills can mediate their stereotypes’ influence on trust. Consistent with this view, Wang and his team found that communication frequency between doctors and patients has mediating effect on patients’ stereotypes of doctors, especially in the starting stage of information transmission.50 This result showed a necessity for doctor–patient adequate communication for ingroup positive stereotype transmission. Therefore, to reduce medical disputes and conflicts, doctors should avoid casual or relaxed styles during communication and make interactions with patients more patient-centered. Trying to regard patients as a source of knowledge, inviting patients to tell their story, and expressing a basic respect for patients with recognition will all contribute to stereotype elimination and effective communication.51
Furthermore, as aforementioned, patients’ evaluations are concerned with their emotions and feelings. During medical interactions, patients particularly value doctors’ communication skills of emotional support. Findings showed that while informational and decision-making support may be more important to patients’ trust in the early course of treatment, emotional support from doctors may be more important to maintain the trust.52 This highlights emotional support’s importance in developing communication skills for doctors’ good self-impression management. Emotional support can be facilitated from the perspective of linguistics.53 Some linguistic markers, such as affiliation words, can positively predict patients’ perception of their health providers’ compassionate care. Meanwhile, health providers’ use of first-person singular pronouns, causation and differentiation words, and clout words are positively related to perceived shared decision-making.53 These concrete communication behaviors can provide doctors with useful techniques in medical interactions. In addition to verbal communication, researchers also claimed that nonverbal communication, such as eye contact, has effect on breast cancer patients’ trust.37 By using these verbal and nonverbal techniques, doctors can not only build better impression and maintain patients’ positive stereotypes but at the same time suppress patients’ negative stereotypes, both of which facilitating trustful doctor–patient relationship. Therefore, it is important for doctors to focus on their impression self-management because their impression management helps to better match patients’ positive stereotypes, which can be exploited to convey a particular impression.54
This study investigated patients’ stereotypes on a wide range, as a practical implication it could be applied to patients across China as the geographic restriction to the distribution is small. Patients of males and females were of many different ages, varied as to region and education level, and the grade of hospitals where they received consultation was surveyed closely. Taken together, the information illustrates that our study sample is representative of the Chinese patient population. Results also support a need to build doctors’ positive impression at both social and individual level. At social level, the government should give high honor to doctor profession and appeal for more respect for this group. Social media should work harder on guiding and managing people’s impression of doctors. Stereotypes of doctor profession are spread through social media and that social media also might represent an avenue for improving messaging and disseminating more positive attitudes toward doctors.55 Much evidence has shown that social media always affect patients’ trust during COVID-19.56,57 For example, a recent study on Turkish public service advertisements by the Ministry of Health found that fictional perfect characters may help to shape a more positive stereotype toward doctors. After watching those fictional doctors, the audience were more likely to believe their miraculous abilities, and great trust could be formed at public level.57 At individual level, there should be a joint effort from both patients and doctors. Patients need to deepen understanding toward doctors, thus discarding excessive expectation and correcting biased perception. They need to put themselves in doctors’ shoes and see doctors’ difficulty such as time and energy limitation. This will help to rectify the mismatched situation of stereotypes and doctors’ real figure. Doctors also need to focus on impression management during medical encounters, which should be noticed in early age as they are medical students. Medical schools and hospitals are responsible for offering courses to let these future doctors know how to effectively manage self-impression. After training doctors can present themselves more professional in front of patients and leave them with a more positive impression. Publicity strategies are also recommendable, such as hospitals’ Open Day and online consultation that can provide channels for increasing the transparency of treatment, at the same time, providing patients with more convenience. In addition, proper communication skills are a blessing to doctors’ self-impression management. Doctors need to receive training on how to work with their patients and involve them meaningfully during medical communication. With useful verbal and nonverbal techniques, doctors can maintain and improve their positive impression, show their good characteristics and professionalism to patients, together contributing to a more trustful doctor–patient relationship.
Some limitations must be noted in the present study. First, since we used the cross-sectional survey to demonstrate the correlations among the main variables, the causality is not yet determined. Future research could either conduct intervention studies or obtain longitudinal data to test the causal relationship. Second, although this study put forward a new predictor, patients’ stereotypes, these stereotypes were not associated with category-based processes like negative and positive stereotypes. In the future, we recommend researchers conduct their studies within the context of the negativity and positivity of their content and consequences, especially under theoretical models, like Stereotype Content Model58,59 as sound explanations to discuss dimensions like warmth and competence. Third, future studies may involve more variables, such as satisfaction and compliance, to get a more detailed image for patients’ stereotypes, thus drawing a comprehensive picture of the impact mechanism of doctor–patient trust.
Conclusion
Through this study, we found relationships among patients’ trust, patients’ stereotypes of doctors, and patients’ evaluation on doctors’ communication skills. Our study suggests that patients’ trust can be predicted by patients’ stereotypes of doctors not only directly but also indirectly through the mediating effect of doctors’ communication skills. Both the direct and the mediating-effect-based correlations should be addressed so as to foster patients’ trust. Patients’ stereotypes and doctors’ communication skills are both associated with patients’ trust, which underlines the importance of shaping doctors’ positive impression and improving communication skills to maintain their good impression, in expectation of building a more trustful doctor–patient relationship.
Ethics Approval and Informed Consent
This study complies with the Declaration of Helsinki. The verbal consent was approved by the ethics committee in our revised manuscript.
Consent for Publication
Details of any images, videos, recordings, etc. can be published, and that the person(s) providing consent have been shown the article contents to be published.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by major bidding projects for National Social Sciences Fund of China (17ZDA327).
Disclosure
Fan Su and Yao Wang are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Lupton D. Doctors on the medical profession. Sociol Health Illn. 1997;19(4):480–497. doi:10.1111/j.1467-9566.1997.tb00414.x
2. Han Q, Liu Z, Gao M, Fang J. Deep and multiple thoughts on the doctors-patients relationship induced by the SARS event. Chin Med Ethics. 2003;06:11–12.
3. Medical violence. Available from: https://www.gpbctv.com/jrrd/202104/165522.html.
4. Zhou YA, Chen SB, Liao YH, et al. General perception of doctor-patient relationship from patients during the COVID-19 Pandemic in China: a cross-sectional study. Front Public Health. 2021;2021:9646486.
5. Hu LM, Bai LJ, Zhao SY, Lu RJ. Analysis of doctor-patient relationship in post-COVID-19 period: perspective differences between citizen and medical staff. Inquiry. 2021;2021:5800469580211060300.
6. Shang-xin C, Jun-hang C, Shi-jia L. Public trust in medical staff during COVID-19 epidemic in China: a cross-sectional survey. Chin J Public Health. 2021;37(12):1783–1787.
7. Basis F, Moskovitz K, Tzafrir S. Did the events following the COVID-19 outbreak influence the incidents of violence against hospital staff? Isr J Health Policy Res. 2021;10(1):36. doi:10.1186/s13584-021-00471-z
8. Liu Y, Wang P, Bai YH. The influence factors of medical disputes in Shanghai and implications-from the perspective of doctor, patient and disease. BMC Health Serv Res. 2022;22(1):1128. doi:10.1186/s12913-022-08490-5
9. Zhao J, Sun M, Zou D, et al. Rethinking the relationship between doctors and patients under the COVID-19 and post-epidemic era. Chin Hosp. 2022;26(02):24–26.
10. Sun L, Wang P. Theory construction on the psychological mechanism of the harmonious doctor-patient relationship and its promoting technology. Adv Psychol Sci. 2019;27:951–964. doi:10.3724/SP.J.1042.2019.00951
11. Hall MA, Dugan E, Zheng B, Mishra AK. Trust in physicians and medical institutions: what is it, can it be measured, and does it matter? The Milbank Quarterly. 2001;79(4):613–639. doi:10.1111/1468-0009.00223
12. Bernstein M, Potvin D, Martin DK. A qualitative study of attitudes toward error in patients facing brain tumour surgery. Can J Neurol Sci. 2004;31(2):208–212. doi:10.1017/S0317167100053841
13. Knifed E, July J, Bernstein M. Neurosurgery patients’ feelings about the role of residents in their care: a qualitative case study. J Neurosurg. 2008;108(2):287–291. doi:10.3171/JNS/2008/108/2/0287
14. Charles C, Gafni A, Whelan T. Self-reported use of shared decision-making among breast cancer specialists and perceived barriers and facilitators to implementing this approach. Health Expect. 2004;7(4):338–348. doi:10.1111/j.1369-7625.2004.00299.x
15. Sharf BF, Stelljes LA, Gordon HS. “A little bitty spot and I’m a big man”: patients’ perspectives on refusing diagnosis or treatment for lung cancer. Psycho-Oncology. 2005;14(8):636–646. doi:10.1002/pon.885
16. Qiao TT, Fan YC, Geater AF, Chongsuvivatwong V, McNeil EB. Factors associated with the doctor-patient relationship: doctor and patient perspectives in hospital outpatient clinics of Inner Mongolia Autonomous Region, China. Patient Prefer Adherence. 2019;13:1125–1143. doi:10.2147/PPA.S189345
17. Thom DH, Campbell B. Patient-physician trust: an exploratory study. J Fam Pract. 1997;44(2):169–176.
18. Kong DT. Trust toward a group of strangers as a function of stereotype-based social identification. Pers Individ Dif. 2018;120:265–270. doi:10.1016/j.paid.2017.03.031
19. Gorbunova LA, Ambrasat J, von Scheve C. Neighborhood stereotypes and interpersonal trust in social exchange: an experimental study. City Commun. 2020;14(2):206–225. doi:10.1111/cico.12112
20. Li X, Liu Q. Warmth and competence: how social stereotypes of volunteers versus paid workers affect client trust. Voluntas. 2021;32(6):1332–1345. doi:10.1007/s11266-021-00406-x
21. Hilton JL, vonHippel W. Stereotypes. Ann Rev Psychol. 1996;47:237–271. doi:10.1146/annurev.psych.47.1.237
22. Hamilton DL, Gifford RK. Illusory correlation in interpersonal perception: a cognitive basis of stereotypic judgments. J Exp Soc Psychol. 1976;12(4):392–407. doi:10.1016/S0022-1031(76)80006-6
23. Judd CM, Park B. Definition and assessment of accuracy in social stereotypes. Psychol Rev. 1993;100(1):109–128. doi:10.1037/0033-295X.100.1.109
24. Jain P. The stereotype content model as an explanation of biased perceptions in a medical interaction: implications for patient-provider relationship. Health Commun. 2022;37(1):64–73. doi:10.1080/10410236.2020.1816311
25. Meisner BA. Physicians’ attitudes toward aging, the aged, and the provision of geriatric care: a systematic narrative review. Crit Public Health. 2012;22(1):61–72. doi:10.1080/09581596.2010.539592
26. Chrisler JC, Barney A, Palatino B. Ageism can be hazardous to women’s health: ageism, sexism, and stereotypes of older women in the healthcare system. J Soc Issues. 2016;72(1):86–104. doi:10.1111/josi.12157
27. Montplaisir ML, Dufour Y. THE ATTITUDES TOWARD AGING AND THE ELDERLY PEOPLE. UNION MEDICALE DU CANADA. 1982;111(8):716–718.
28. Hareli S, David S, Hess U. Competent and warm but unemotional: the influence of occupational stereotypes on the attribution of emotions. J Nonverbal Behav. 2013;37(4):307–317. doi:10.1007/s10919-013-0157-x
29. Qu XP, Wu J, Ye XC. Research progress of stereotype and its enlightenment on physician-patient relationship. J Nurs Admin. 2012;12(4):264–266.
30. Su Y. Stereotypes and doctor-patient relationship. Chin Med Human Rev. 2012;2012:18–22.
31. Drevs F. How patients choose hospitals: using the stereotypic content model to model trustworthiness, warmth and competence. Health Services Manag Res. 2013;26(2–3):95–101. doi:10.1177/0951484813513246
32. Thom DH. Training physicians to increase patient trust. J Eval Clin Pract. 2000;6(3):245–253. doi:10.1046/j.1365-2753.2000.00249.x
33. Ha JF, Anat DS, Longnecker N. Doctor-patient communication: a review. Ochsner J. 2010;10(1):38–43.
34. Stewart M, Brown JB, Boon H, Galajda J, Meredith L, Sangster M. Evidence on patient-doctor communication. Cancer Prev Control. 1999;3(1):25–30.
35. Street RL, Makoul G, Arora NK, Epstein RM. How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Educ Couns. 2009;74(3):295–301. doi:10.1016/j.pec.2008.11.015
36. Kovacs RJ, Lagarde M, Cairns J. Measuring patient trust: comparing measures from a survey and an economic experiment. Health Econ. 2019;28(5):641–652. doi:10.1002/hec.3870
37. Hillen MA, De Haes H, van Tienhoven G, et al. All eyes on the patient: the influence of oncologists’ nonverbal communication on breast cancer patients’ trust. Breast Cancer Res Treat. 2015;153(1):161–171. doi:10.1007/s10549-015-3486-0
38. Ashton-James CE, Tybur JM, Griesser V, Costa D. Stereotypes about surgeon warmth and competence: the role of surgeon gender. PLoS One. 2019;14(2):e0211890. doi:10.1371/journal.pone.0211890
39. Mast MS, Kadji KK. How female and male physicians’ communication is perceived differently. Patient Educ Couns. 2018;101(9):1697–1701. doi:10.1016/j.pec.2018.06.003
40. Qu XP, Ye XC. Development and evaluation research of measurement tools for stereotypes of doctor role perception. Chin Hosp Manag. 2014;34(02):48–50.
41. Li J. Using the SEGUE Framework to Assess Chinese Medical Students’ communication skills in History-Taking [Thesis]. Shenyang: China Medical University; 2008.
42. Makoul G. The SEGUE framework for teaching and assessing communication skills. Patient Educ Couns. 2001;45(1):23–34. doi:10.1016/S0738-3991(01)00136-7
43. Hall MA, Zheng B, Dugan E, et al. Measuring patients’ trust in their primary care providers. MCRR. 2002;59(3):293–318. doi:10.1177/1077558702059003004
44. Dong E, Bao Y. Reliability and validity of the Chinese version of Wake Forest Physician Trust Scale. Chin Ment Health J. 2012;26(03):171–175.
45. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. Guilford Publications; 2017.
46. Davies K, Tropp LR, Aron A, Pettigrew TF, Wright SC. Cross-group friendships and intergroup attitudes: a meta-analytic review. Personal Soc Psychol Rev. 2011;15(4):332–351. doi:10.1177/1088868311411103
47. Rast DE, Gaffney IAM, Yang FL. The effect of stereotype content on intergroup uncertainty and interactions. J Soc Psychol. 2018;158(6):711–720. doi:10.1080/00224545.2017.1407285
48. Wang JH-Y, Adams IF, Pasick RJ, et al. Perceptions, expectations, and attitudes about communication with physicians among Chinese American and non-Hispanic white women with early stage breast cancer. Support Care Cancer. 2013;21(12):3315–3325. doi:10.1007/s00520-013-1902-8
49. Siu JYM. Communicating with mismatch and tension: treatment provision experiences of primary care doctors treating patients with overactive bladder in Hong Kong. BMC Fam Pract. 2015;2015:16160.
50. Wang P, Yin Z, Luo X, Ye X, Bai Y. The impact of doctor-patient communication frequency on the stereotype of the doctor. Stud Psychol Behav. 2018;16(1):119–124.
51. Undeland M, Malterud K. Diagnostic interaction: the patient as a source of knowledge? Scand J Prim Health Care. 2008;26(4):222–227. Pii 902579083. doi:10.1080/02813430802325086
52. Arora NK, Gustafson DH. Perceived helpfulness of physicians’ communication behavior and breast cancer patients’ level of trust over time. J Gen Intern Med. 2009;24(2):252–255. doi:10.1007/s11606-008-0880-x
53. Zhou YM, Callejas MLA, Li YW, MacGeorge EL. What does patient-centered communication look like?: Linguistic markers of provider compassionate care and shared decision-making and their impacts on patient outcomes. Health Commun. 2021;1–11. doi:10.1080/10410236.2021.1989139
54. Vartanian LR, Herman CP, Polivy J. Consumption stereotypes and impression management: how you are what you eat. Appetite. 2007;48(3):265–277. doi:10.1016/j.appet.2006.10.008
55. Johnsen JAK, Eggesvik TB, Rorvik TH, Hanssen MW, Wynn R, Kummervold PE. Differences in emotional and pain-related language in tweets about dentists and medical doctors: text analysis of twitter content. Public Health Surveill. 2019;5(1):22–30. e10432. doi:10.2196/10432
56. Niu ZM, Qin Z, Hu PW, Wang TT. Health beliefs, trust in media sources, health literacy, and preventive behaviors among high-risk Chinese for COVID-19. Health Commun. 2022;37(8):1004–1012. doi:10.1080/10410236.2021.1880684
57. Deveci A, Cesur AA. Your doctor speaking: the representation of doctor characters in COVID-19 public service advertisements. Turkiye Iletisim Arastirmalari Dergisi. 2021;2021:(37):254–273.
58. Fiske ST, Cuddy AJ, Glick P. Universal dimensions of social cognition: warmth and competence. Trends Cogn Sci. 2007;11(2):77–83. doi:10.1016/j.tics.2006.11.005
59. Fiske ST, Cuddy AJC, Glick P, Xu J. A model of (often mixed) stereotype content: competence and warmth respectively follow from perceived status and competition. J Pers Soc Psychol. 2002;82(6):878–902. doi:10.1037/0022-3514.82.6.878
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.