")
Back to Journals » Infection and Drug Resistance » Volume 15
The Influence of Saudi National COVID-19 Preparedness Programs on Triage Decision-Making Skills of Healthcare Practitioners During the 2020 Peak of the 1st Wave of COVID-19
Authors Alzahrani FR, Al-Moteri M
Received 16 November 2021
Accepted for publication 10 February 2022
Published 8 March 2022 Volume 2022:15 Pages 925—932
DOI https://doi.org/10.2147/IDR.S347375
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Faisal Rashed Alzahrani,1,2 Modi Al-Moteri1
1Taif University, College of Applied Medical Sciences, Nursing Department, At Taif, 21944, Saudi Arabia; 2Ministry of Health, King Abdelaziz Hospital, At Taif, 21944, Saudi Arabia
Correspondence: Modi Al-Moteri, Email [email protected]; [email protected]
Background: As part of the national COVID-19 preparedness efforts in Kingdom of Saudi Arabia to overcome the crisis of the COVID-19 pandemic, emergency rooms’ (ERs) health-care providers were required by their health institutions to receive a triage training program (TTP) as well as involving on a disaster preparedness program (DPP) and/or participation in a mock drill towards disaster response. These efforts attempted to enhance skills of ER health-care providers to make triage decisions, and, consequently, improve patient flow in ERs during the COVID-19 pandemic. However, the influence of these hospitals’ educational efforts on the decision-making skills of ERs’ health-care providers has not yet been reported.
Purpose: To identify the effect of hospitals’ COVID-19 preparedness educational efforts on triage decisions by ERs’ health-care practitioners during the crisis of the COVID-19 pandemic.
Methods: A one-group posttest-only design was conducted in ERs of regional hospitals in which Triage Decision-Making Inventory (TDMI) was used to collect data.
Results: About 78%, 70% and 78% of participants had taken TTP, DPP or were involved in mock drills, respectively. Skills of triage decision-makers in critical thinking and confidence have higher mean scores than cognitive and intuition skills. A positive relationship was found between TTP and participants’ cognitive (p=0.01), critical thinking (p=0.03), confidence (p=0.01) and intuition (p=0.02) skills as pertained to triage decision-making. Also, a positive relationship was found between DPP and cognitive abilities (p=0.04), as well as those involved in mock drills and measures of confidence (p=0.03).
Conclusion: TTP may enhance triage decision-making abilities of health-care professionals and contribute in delivering rapid and safe care service during disasters.
Keywords: cognition, emergency, health practitioners, COVID-19, triage, decision-making
Introduction
During the coronavirus pandemic (COVID-19) that appeared first in Wuhan, China, 2019, hospital resources were stretched and Emergency Rooms (ERs) have been significantly impacted.1 ERs have played a critical role during COVID-19 pandemic. Indeed, ERs are the first place to detect and isolate patients infected with COVID-19. Researchers reported that the number of patients triaged and the acuity of their conditions in ERs increased during COVID-19 compared to the same period of time in the previous years.2
In Kingdom of Saudi Arabia (KSA), nurses and physicians working in ERs during the COVID-19 pandemic have faced a great challenge to not only provide timely care for COVID-19 patients with severe or mild symptoms, but also to deal with a large number of regular visits of patients and distinguish them from suspected COVID-19 patients. Studies conducted in KSA to investigate the influence of COVID-19 pandemic on the volume and acuity of patients presenting in ERs revealed an overall reduction in the total number of patients; however, a significant increase in the number of patients attending the ERs as higher acuity was also noticed.3,4 The increment of the number of patients with higher acuity was about 200% resulting in an overcrowding and delay in ERs services.4 This increase in the number of patients with a higher acuity has interfered with patient flow and put health-care providers and other patients at high risk of infection with the COVID-19 virus.5 Indeed, the COVID-19 is a highly infectious virus and can rapidly spread through droplets and interpersonal contact.
Patient flow can be maintained through sorting and triaging of patients.6,7 The triaging process is defined as arranging the patients according to the severity of their conditions while the process of prioritizing patients and deciding who should be treated first among others is called triage decision-making.8 The definition encompasses several processes: (a) selecting a patient among a group of patients, (b) separating (c) categorizing, and (d) prioritizing the categories.9 Triage decision-making is important and depends on ER staff experience. Further, cognitively processing the information available to take the best possible decisions is critical in everyday practice in emergency setting.10
Triage decisions are often made promptly, independently and under time restrictions, hence, it can critically influence the patients’ outcomes and flow. The literature has consistently shown that practitioners’ skills such as cognitive, critical thinking, confidence and intuition are key elements in maintaining the accuracy and promptness of triage decision-making and therefore patient’s safety.8–11 These skills can be enhanced by conducting tailored educational programs.12–14 In an attempt to enhance skills in triage decision-making for ER health-care providers in Saudi Arabia during the COVID-19 pandemic, hospitals’ COVID-19 preparedness plan which included three modes of training was conducted.
The hospitals’ COVID-19 preparedness and response plan was designed under the guidance of the Ministry of Health (MOH) in Saudi Arabia as a collaborative effort to face COVID-19 crisis. It involves training health-care providers to rapidly triage patients with suspected COVID-19 and distinguish them from the non-suspected. The hospitals’ COVID-19 preparedness plans also include preparing health-care providers to rapidly detect and effectively respond to the COVID-19 outbreak by teaching them the principles of disaster triage, the policies of infection control and prevention, transmission-based precaution, personal protective equipment (PPE), hand hygiene; and environment cleaning.15
Identifying the specific influence of these hospitals’ strategies on practitioners’ skills in making triage decisions during COVID-19 has not been reported. Hence, this study aims to identify the effect of hospitals’ COVID-19 preparedness educational efforts on the triage decision-making skills of ER health-care practitioners during the crisis of the COVID-19 pandemic.
Materials and Methods
A one-group posttest-only design was conducted from March to July 2020 in three main regional hospitals in the Kingdom of Saudi Arabia. A one-group posttest-only design was used because the participants already have been exposed to the hospitals’ COVID-19 preparedness educational program. The design has the same steps of the pre-post-test design, except that the pre-test step is omitted.
Participants
A convenience sampling technique was used in which all ER physicians and nurses were considered eligible and were invited to take part in the study. Prior to conducting the study, sample size was calculated to identify how many participants (physician and nurses) would be needed in the study. Using an online sample size calculator and with an alpha = 0.05 and power = 0.80, the estimated sample size needed was approximately N = 213 (45 physicians and 168 nurses).
Data Collection Instruments
Participants completed a demographic data questionnaire which included age, gender, professional qualification and work experience. In addition, the “Triage Decision-Making Inventory (TDMI)” (Cone, 2000) was employed. The TDMI is a self-reporting survey and includes 31 items measuring health-care professional decision-making skills in an ER setting on a 5-point, Likert scale (5 = Strongly agree; 4 = Agree; 3 = Undecided; 2 = Disagree, and 1 = Strongly disagree). The highest score to be obtained from the inventory is 155.
The inventory consists of four subscales as follows: (a) cognitive behaviours, (b) confidence, (c) intuition, and (d) critical thinking. The first subscale deals with the cognitive abilities and has six items that relate to organization, prioritization and judgment skills. The second subscale deals with the confidence and has eight items which assess the skills required to ask the correct questions in a triage setting. The third subscale deals with intuition and encompasses seven items that explain the inner feelings. The fourth and final subscale deals with critical thinking and has 10 items that assess the ability to communicate, collect and evaluate the required information to make decisions.
The tool has been found to be statistically valid and reliable.8 According to Cone,16 also reported in Aktaş and Alemdar (2017),9 the overall Cronbach’s alpha coefficient of the tool was found to be (α=0.95) indicating a high level of reliability and the Cronbach’s alpha coefficient for “the subscales” ranged from (α=0.84) to (α=0.89) indicating good level of reliability. The reliabilities for the four subscales were assessed also by Smith and Cone,8 and were found to be acceptable as follows: the Cronbach’s alpha coefficient for cognitive abilities, confidence, intuition, and critical thinking were, 0.91, 0.94, 0 87, and 0.86, respectively.
Because the “TDMI” is a self-report that focuses on triage decision-making specific skills such as cognition, critical thinking, confidence and intuition use, rather than on particular proficiency abilities, diseases, or guideline and protocols, the tool can be used in any context of health-care professionals working inside an ER.
Hospitals COVID-19 Preparedness Plan
As a part of the hospitals’ COVID-19 preparedness and response plan at the beginning of the COVID-19 pandemic, hospitals offered a one-day online triage training program (TTP) or a disaster preparedness program (DPP) as well as mock drills. All health-care providers were recommended to attend at least two of these educational and training programs. The aim of the TTP is to provide health-care providers with the required knowledge to appropriately prioritize patients during the disaster to enhance patient flow and care process. DPP aimed to provide health-care providers with an introduction to national emergencies and the essential role that they play during the time of the disaster. Mock drills were provided only for the first responders (ER health-care practitioners) to practice emergency procedures.
Data Collection Procedure
Due to the COVID-19 social restrictions, the “TDMI” was distributed electronically to physicians and registered nurses through their official emails, following the hospital review board approval (HAP-2-T-067:453). All health-care practitioners [(N=263) (61 physicians and 202 nurses)] working in three main regional hospitals received an invitation to contribute to the current study as an “electronic notice”. The participants were able to read the invitation, the study information and the consent form. If the participant wished to participate, he/she was able to access the link and complete the demographic data, complete the “TDMI”, and click the submit icon.
Prior to the data collection process, the research team set a target for the unacceptable percentage of missing data. Less than 20% of missing data was acceptable.17 Of the 263 eligible participants, 228 surveys were returned. Of those returned surveys, 15 were discarded, nine (9) due to missing data (>20% are missed) and six (6) were considered inattentive responders and were removed.
Data Analysis
Data analysis was performed using Statistical Package for the Social Science (SPSS) Version 22. Descriptive analysis was used to describe sample characteristics. One-way ANOVA test and two tail t-test were used to determine if there were statistically significant differences between the groups relevant to particular variables. Specifically, to compare the sociodemographic characteristics of the ER health-care professionals with their mean TDMI subscale scores in the status of receiving hospitals’ COVID-19 preparedness educational program (TTP, DPP, Mock Drills). The value of p < 0.05 was accepted as being statistically significant.
Results
The Demographic Variables
A total of 213 participants (Physician n = 45 and Registered Nurses n = 168) agreed to take part in this study. Of these, 67% (n = 143) were female and 33% (n = 70) were male. The mean age of the participants was 35 years (±7.19 years). At the time of the study 60% (n = 129) of participants had work experience in ER of more than five years and 40% (n = 84) of participants had work experience of less than five years.
The Hospitals COVID-19 Preparedness Plans and TDMI Subscale
Out of the 213 participants, 78% (n = 165) had taken TTP and 70% (151) had taken DPP offered by their institution. Seventy-eight per cent (n = 165) of participants had been involved in mock drills and training sessions towards disaster response. The mean and standard deviation of TDMI subscale score of the ER professionals is presented in Table 1.
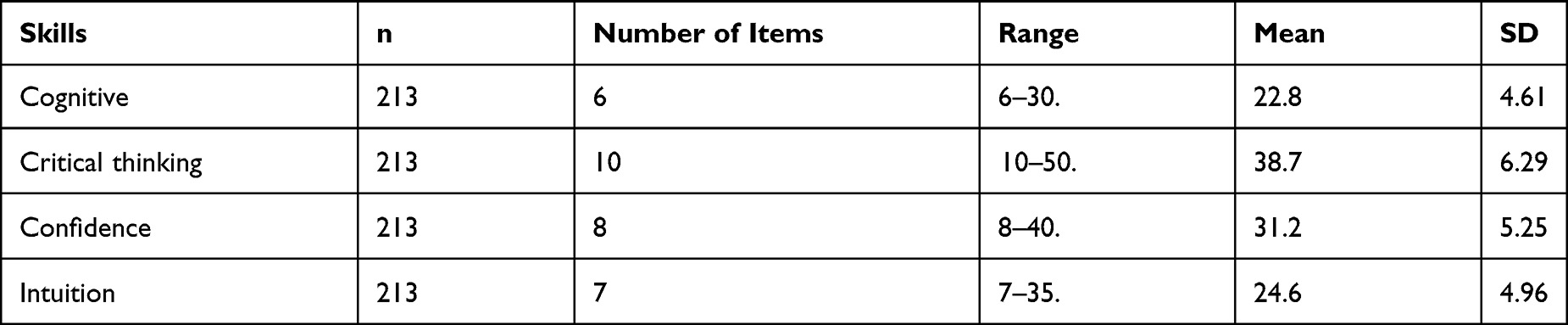 |
Table 1 Mean Scores of TDMI Subscales |
The Association Between Demographic Variables and TDMI Subscale Scores
When the demographic variables of the ER participants were analysed in relation to the mean of TDMI subscale scores irrespective of the method used for the training, it was determined that there was a significant difference in cognitive abilities among different age (p=0.025) and professional experience groups (p=0.02) of ER participants. Similarly, the mean score of the confidence subscale showed significant difference among different age (p=0.02) and professional experience groups (p=0.01) of ER participants. A statistically significant difference was found between intuition and being a physician (p=0.03) and years of work experience (p=0.01) (see Table 2).
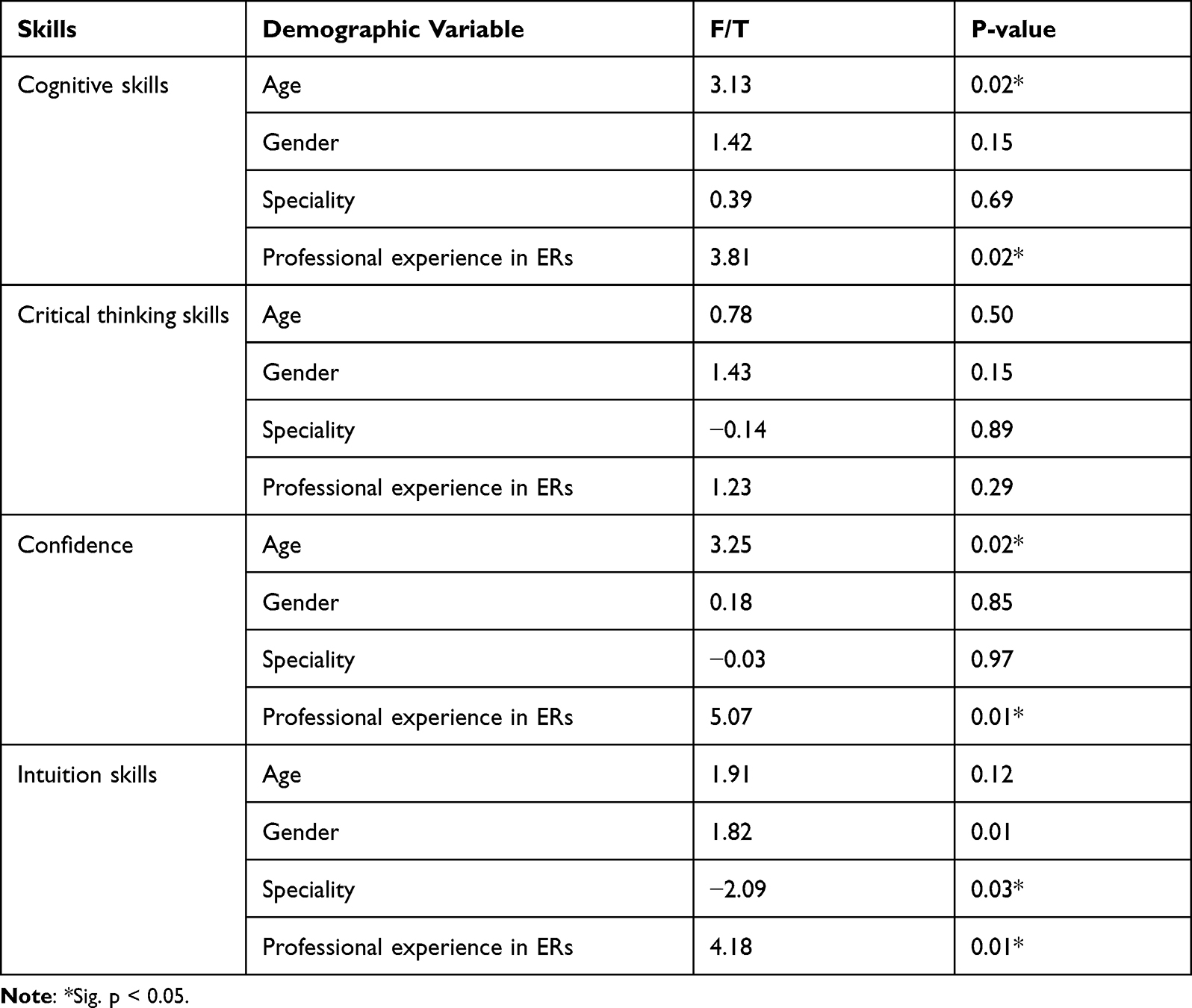 |
Table 2 TDM Skills in Relation to Demographic Data |
The Association Between Hospitals COVID-19 Preparedness Efforts and TDM Skills
Out of 213, 78% (n = 165) and 70% (n = 151) of participants had been involved in a TTP and DPP, respectively, and 78% (n = 165) of participants had participated in a Mock Drill. There is a statistically significant association between all the triage skills – cognitive (p=0.01), critical thinking (p=0.035), confidence (p=0.01) and intuition (p=0.02) and having participated in a TTP. Meanwhile, a significant association was found only between cognitive abilities (p=0.04) and DPP. Further, a significant difference was found between the confidence subscale and the status of having been involved in mock drills and training sessions towards disaster response (p=0.03) (see Table 3).
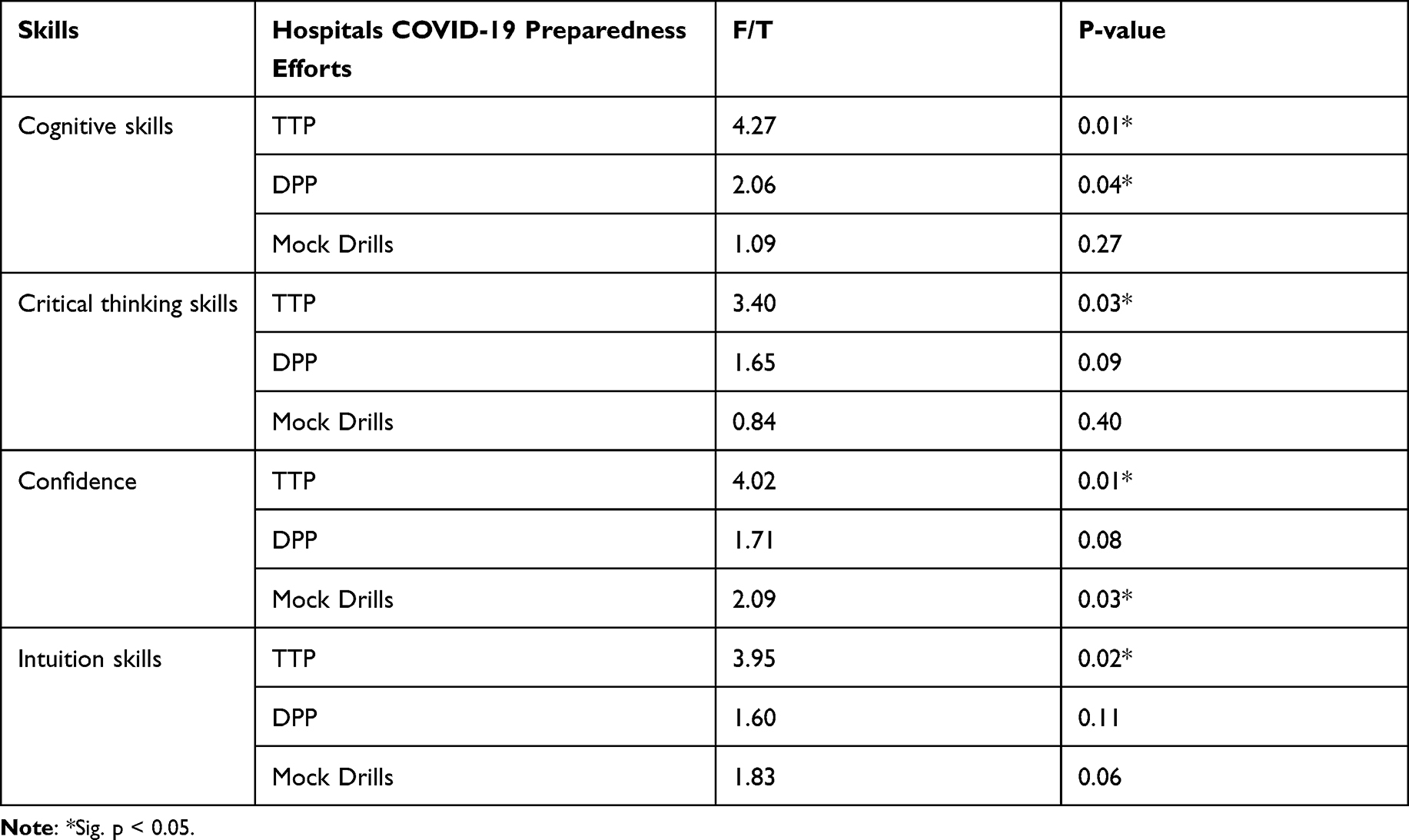 |
Table 3 TDM Skills in Relation to Hospitals COVID-19 Preparedness Efforts |
Discussion
This study aimed to evaluate the influence of hospitals’ COVID-19 preparedness educational efforts on the dimensions of triage decision-making processes of health-care practitioners working in the emergency departments. Enhancement of ERs’ health-care practitioners’ decision-making skills is essential to improve patient flow.
In normal circumstances, triage decision-making is an important part of ER care as it categorizes patients according to their acuity in order to manage patient flow,9 yet, during the COVID-19 pandemic, managing patient flow becomes more difficult for health practitioners. This study evaluated the specific skills of health practitioners’ triage decision-making skills in ERs during COVID-19 pandemic, to correlate them with specific national COVID-19 preparedness efforts.
Triage decision-making depends on cognitive critical thinking, confidence and intuition.16 In this study, it was found that the participants’ mean score of perceived critical thinking skills and confidence in triage decision-making was higher than cognitive and intuition skills among general health practitioners working in emergency rooms. Perhaps, the reason that the critical thinking skills of the health practitioners’ triage decision-making in the study was high is due to the triage training courses. Indeed, developing critical thinking skills is influenced by the learning environment, approach of training and the trainers’ competence.18
In this study, 78%, 71% and 78% of the health-care professionals were determined to have been involved in hospitals’ COVID-19 preparedness educational programs, TTP, DPP and mock disaster exercise, respectively. Researchers have confirmed the need for ongoing education and training.9,19,20
It was noticed in the current study that the cognitive abilities, critical thinking skills, confidence and intuition were high in the health-care providers that had been involved in and completed the TTP. Lack of TTP among emergency health-care providers was found to be associated with lack of the accuracy of triage decisions.9,20 Meanwhile, DPP was found to influence the cognitive abilities of health practitioners only. Perhaps, this is because cognitive skills refer to prioritization skills and knowledge (Smith and Cone, 2010).8 These findings show the importance of training in triage and disaster for health-care practitioners in ERs.21
In the current study, health practitioners’ characteristics such as years of work experience and receiving a training session on triage decision-making were found to influence participants’ cognitive skills, confidence and intuition. These findings are consistent with the Aktaş and Alemdar,9 study that found a positive relationship between health practitioners with triage care certificates and triage decision cognitive skills, confidence and intuition. Triage decision-making is made by nurses and physicians; however, intuition was found to be high among physicians who had more years of work experience in ERs. This might be related to the type of intuition. Nurses describe their intuition as a “gut feeling”, or their ability to feel that something is going wrong with the patient or their worry about the patient condition,22 while physicians describe their intuition as a “recognition”, their ability to make a quick decision despite a lack of information.23
The ability to make quick decisions is very critical in ERs. Hence, the development of a triage decision-making educational plan for health-care professionals who work in ERs will contribute in improving patient flow and consequently patients’ outcomes.
Implications
Enhancing triage decision-making in all health practitioners is essential to improve patient flow and consequently patients’ outcomes, particularly during a disaster. Triage decision-making is recognised as a cognitive practice to make the best decision for the consequent intervention steps to take place. The findings of the current study imply the importance of providing health practitioners with educational programs and training courses in triage to improve skills of “triage decision-making”. Further studies are required to identify the reasons behind the lack of the influence of disaster preparedness programs on triage decision-making skills.
Limitations
The study has several limitations. First, the study was conducted in a single region. Further studies are suggested including in emergency services from other locations. The social, cultural, and economic status of Saudi Arabia differs from other countries; the results cannot be transferred, and similar studies should be carried out in other countries. Second, a considerable number of participants had two or three types of training modes simultaneously; hence, there was an overlap in terms of the specific impact of the various training sessions. This has made it difficult for the researchers to know if a particular skill was gained from one mode or more than one mode of training. This kind of methodological limitation can only be managed early during the construction of the demographic part of the survey. Future researchers should consider this deficiency and include this missing element. Third, this study used a one group posttest only design. It is difficult to infer a causal relationship between the national preparedness program and outcomes; a pre-post experimental design is required.
Conclusions
In this study, it was found that DPP may increase participants’ cognitive abilities and confidence, while TTP may increase participants’ cognitive, critical thinking, confidence and intuition abilities. Involvement in mock drills and training sessions was found to increase participants’ confidence. The cognitive abilities, confidence and intuition skills were higher in health-care professionals who had more years of work experience in ERs and the usage of intuition was higher among physicians. Understanding factors influencing the triage decision-making skills of health professionals may facilitate an understanding of their training needs.
Institutional Review Board Statement
Ethical approval was granted from the Ethics Review Committee (ERC) of the Ministry of Health number (HAP-2-T-067:453). Participants were informed that their participation was entirely voluntary and that any information resulting from the study would be treated with confidentiality.
Data Sharing Statement
Data available on request from the corresponding author due to privacy/ethical restrictions.
Acknowledgments
The authors would like to acknowledge Taif University for supporting this study through the University Research Supporting Project number (TURSP-2020/194). The authors wish also to express their gratitude to the participants for their significant contribution.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; have drafted, written, and critically reviewed the article; have agreed on the journal to which the article has been submitted; reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage; agree to take responsibility and be accountable for the contents of the article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Remuzzi A, Remuzzi G. COVID-19 and Italy: what next? Lancet. 2020;395(10231):1225–1228. doi:10.1016/S0140-6736(20)30627-9
2. Gutiérrez MÁ, Domínguez JA, Barriocanal MB, et al. Impact of the COVID-19 pandemic on emergency department: early findings from a hospital in Madrid. An Pediatr. 2020;93(5):313–322.
3. Abdelhadi A. The effects on the number of patients visiting the emergency units: comparison study before and during COVID-19 pandemic in Saudi Arabia. J Multidiscip Healthc. 2021;14:1207. doi:10.2147/JMDH.S314191
4. Alharthi S, Al-Moteri M, Plummer V, Al Thobiaty A. The impact of COVID-19 on the service of emergency department. In: Healthcare. Vol. 9. Multidisciplinary Digital Publishing Institute; 2021:1295.
5. Dzinamarira T, Mhango M, Dzobo M, et al. Risk factors for COVID-19 among healthcare workers. A protocol for a systematic review and meta-analysis. PLoS One. 2021;16(5):e0250958. doi:10.1371/journal.pone.0250958
6. Imperato J, Morris DS, Sanchez LD, Setnik G. Improving patient satisfaction by adding a physician in triage. J Hosp Adm. 2014;3(1):7–13.
7. Reay G, Rankin JA. The application of theory to triage decision-making. Int Emerg Nurs. 2013;21(2):97–102. doi:10.1016/j.ienj.2012.03.010
8. Smith A, Cone KJ. Triage decision-making skills: a necessity for all nurses. J Nurses Prof Dev. 2010;26(1):E14–9.
9. Aktaş YY, Alemdar DK. Triage decision-making levels of healthcare professionals working in emergency departments. Eurasian J Emerg Med. 2017;16(3):92. doi:10.5152/eajem.2017.96168
10. Noon AJ. The cognitive processes underpinning clinical decision in triage assessment: a theoretical conundrum? Int Emerg Nurs. 2014;22(1):40–46. doi:10.1016/j.ienj.2013.01.003
11. Kerie S, Tilahun A, Mandesh A. Triage skill and associated factors among emergency nurses in Addis Ababa, Ethiopia 2017: a cross-sectional study. BMC Res Notes. 2018;11(1):1–6. doi:10.1186/s13104-017-3088-5
12. Brinjee D, Al Thobaity A, Almalki M, Alahmari W. Identify the disaster nursing training and education needs for nurses in Taif City, Saudi Arabia. Risk Manag Healthc Policy. 2021;14:2301. doi:10.2147/RMHP.S312940
13. Van der Linden MC, van der Linden NN. The impact of a multimodal intervention on emergency department crowding and patient flow. Int J Emerg Med. 2019;12(1):1. doi:10.1186/s12245-019-0238-7
14. Fathoni M, Sangchan H, Songwathana P. Relationships between triage knowledge, training, working experiences and triage skills among emergency nurses in East Java, Indonesia. Nurse Media J Nurs. 2013;3(1):511–525.
15. Griffin KM, Karas MG, Ivascu NS, Lief L. Hospital preparedness for COVID-19: a practical guide from a critical care perspective. Am J Respir Crit Care Med. 2020;201(11):1337–1344. doi:10.1164/rccm.202004-1037CP
16. Cone KJ. The Development and Testing of an Instrument to Measure Decision Making in Emergency Department Triage Nurses. [unpublished doctoral dissertation]. Saint Louis University; 2000.
17. Dong Y, Peng CY. Principled missing data methods for researchers. SpringerPlus. 2013;2(1):1–7. doi:10.1186/2193-1801-2-222
18. Gul R, Cassum S, Ahmad A, Khan S, Saeed T, Parpio Y. Enhancement of critical thinking in curriculum design and delivery: a randomized controlled trial for educators. Procedia Soc Behav Sci. 2010;2(2):3219–3225. doi:10.1016/j.sbspro.2010.03.491
19. Elkum NB, Barrett C, Al-Omran A-OH. Canadian Emergency DepartmentTriage and Acuity Scale: implementation in a tertiary care center in Saudi Arabia. BMC Emerg Med. 2011;11(1):1–5. doi:10.1186/1471-227X-11-3
20. Considine J, Botti M, Thomas S. Do knowledge and experience have specific roles in triage decision‐making? Acad Emerg Med. 2007;14(8):722–726. doi:10.1197/j.aem.2007.04.015
21. Sherafat A, Vaezi AA, Vafaeenasab M, Ehrampoush MH, Fallahzadeh H, Tavangar H. Evaluation of emergency nurses’ knowledge and performance about hospital triage. J Pharm Res Int. 2019;22:1–7. doi:10.9734/jpri/2019/v27i530182
22. Douw G, Schoonhoven L, Holwerda T, et al. Nurses’ worry or concern and early recognition of deteriorating patients on general wards in acute care hospitals: a systematic review. Crit Care. 2015;19(1):1. doi:10.1186/s13054-015-0950-5
23. Vanstone M, Monteiro S, Colvin E, et al. Experienced physician descriptions of intuition in clinical reasoning: a typology. Diagnosis. 2019;6(3):259–268. doi:10.1515/dx-2018-0069
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.