")
Back to Journals » International Journal of Women's Health » Volume 14
The Influence of Lifestyle Variables on Primary Dysmenorrhea: A Cross-Sectional Study
Authors Al-Husban N , Odeh O, Dabit T , Masadeh A
Received 10 September 2021
Accepted for publication 24 November 2021
Published 13 April 2022 Volume 2022:14 Pages 545—553
DOI https://doi.org/10.2147/IJWH.S338651
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Naser Al-Husban,1 Omar Odeh,2 Tala Dabit,2 Aya Masadeh2
1Obstetrics and Gynecology Department, School of Medicine, The University of Jordan, Amman, Jordan; 2School of Medicine, The University of Jordan, Amman, Jordan
Correspondence: Naser Al-Husban, Obstetrics and Gynecology Department, The University of Jordan, P O Box 2194, Amman, 11941, Jordan, Tel +962-772086080, Fax +96264643217, Email [email protected]
Background: Primary dysmenorrhea is a common and often debilitating, gynaecological condition.
Objective: To investigate the effects of specific lifestyle variables on the prevalence and severity of primary dysmenorrhea.
Materials and Methods: A cross-sectional study of Jordanian women aged between 18– 25 years old utilized a questionnaire as the main instrument of the study.
Results: Primary dysmenorrhea was reported by 660 women out of 1988. It was found that approximately two thirds of them were students. Overall, 54.5% of the participants reported severe dysmenorrhea. A statistically significant correlation was found between severe dysmenorrhea and smoking at p value ˂0.001, sleeping less than 7 hours per 24 hours at p = 0.005, holding a university degree at p = 0.032, non-alcohol consumption at p = 0.044, frequent energy, fizzy, tea, coffee drinks and sugar intake. Interestingly, we found that severe dysmenorrhea was statistically significantly associated with women who never eat meat at p ˂0.001, cereals and fish consumers and with those who take less than 3 servings of fruit or none at all per week at p = 0.006. In addition to the previous variables, water intake of less than 1.0 litre a day, irregular cycles, non-OCP use and positive family history were found significantly associated with severe dysmenorrhea. Severe dysmenorrhea was significantly related to working less hours per week, higher stress level and longer bleeding duration at p = 0.021, 0.017 and 0.008, respectively. On the other hand, there was no statistically significant difference found between severe dysmenorrhea and the following variables: age, body mass index (BMI), weekly studying hours and age of menarche.
Conclusion: Primary dysmenorrhea is prevalent in the Jordanian population. To overcome severe dysmenorrhea, women should increase their intake of fish and fresh fruits, drinking water and use of oral contraceptive pills. The study concluded that smoking, frequent sugar intake, fizzy drinks, coffee, tea and energy drinks were associated with severe dysmenorrhea. It is also worth mentioning that alcohol consumption had a positive impact on dysmenorrhea.
Trial Registration: Registered in Clinicaltrial.gov (ID: NCT04583943).
Keywords: dysmenorrhea, menstruation, painful, menstrual, lifestyle, variables
Introduction
Primary dysmenorrhea is a common condition, and often debilitating in the absence of pelvic pathology. It is a gynaecological condition that affects between 45% and 95% of menstruating women.1 Therefore, the prevalence of dysmenorrhea worldwide is also difficult to be measured in different countries, but it can generally reach up to 90%.2
Dysmenorrhea pain can be considerably disabling, and is associated with a restriction of physical and daily activities3 In support of this view, a study of 623 female students4 reported that dysmenorrhea was a common health problem that has negative effects on health-related quality of life (HRQoL). Despite the high prevalence of dysmenorrhea, young women usually fail to consult a health professional or seek medical care. They are also incapable of applying alternative effective therapies to relieve their menstrual pain. This research hence highlights the significance of understanding this issue and investigating the risk factors that have been extensively studied in other populations but not in the Jordanian context. So further, this study aims to investigate the prevalence and severity of primary dysmenorrhea in Jordanian females aged between 18–25. It also studies the effect of lifestyle on the prevalence and severity of dysmenorrhea among this group of women. Results of this study may contribute to providing recommendations to the Jordanian or international communities by providing instructions to modify women’s lifestyle.
Materials and Methods
The study employed a cross-sectional approach that was conducted in all Jordanian governorates, namely, Amman, Irbid, Madaba, Zarqa, Balqa, Mafraq, Ajloun, Jerash, Karak, Tafileh, Maan, and Aqaba.
The study sample included females between the age of 18 and 25, living in Jordan and medically fit. The ethnicity and religion of the participants were not included as part of the survey items since they were out of the scope of the research and could be specifically studied in future research. The exclusion criteria were: females out of the age range 18–25, Jordanian women living overseas, women having any chronic or gynecological illnesses, women taking food supplements including vitamin D and oil fish, and participants failing to provide consent to take part in the study. The instrument of the study utilized a structured self-report questionnaire distributed online (see Supplementary File 1) The survey was initially used by a Spanish study. After obtaining the approval and consent of using the survey in the present study, it was then translated into Arabic.
(see Supplementary File 1) It was the main tool used in this research. There were no interviews or direct contact with the participants. The survey was randomly distributed between different groups of Jordanian citizens on social media. The participants have given their consent before filling-up the questionnaire (see Supplementary File 1) ensuring their confidentiality and anonymity without imposing any financial expenses for participation.
The questionnaire (see Supplementary File 1) contained the following variables: occupation, smoking, sleeping habits, education level, consumption of alcohol, fast food ingestion, consuming energy drinks, fizzy drinks water, tea, coffee, sugar, cereals intake, eating meat, fish, and fruits, cycle duration and regularity, family history, use of oral contraceptive pills (OCP). We then studied mild versus severe dysmenorrhea in relation to these lifestyle variables in addition to age, body mass index (BMI), duration of study per week in hours (for students), daily hours of work for those who were employed, stress level, age of menarche and cycle duration of bleeding. The study concluded that dysmenorrhea is considered severe when it causes severe pain that requires regular oral analgesics at home, parenteral analgesics at hospital, emergency visits or frequent absences from school, college, or work.
The questionnaire (see Supplementary File 1) was sent online by using different social media applications and emails. Additionally, it was also printed out and distributed in different areas, including fifth year medical students at the University of Jordan. Data was collected anonymously. Participants were not asked about their names, phone numbers or their addresses. They were also required to grant their consent. Furthermore, they had the right to withdraw from the questionnaire (see Supplementary File 1) at any time without repercussions. All participants were informed about the purpose of the survey, which was conducted in accordance with the Declaration of Helsinki.
The study obtained an institutional review board (IRB) approval at Jordan University Hospital (decision number 280/2020 dated 17/11/2020). It is registered in Clinicaltrial.gov (ID; NCT04583943).
In terms of data sharing, the authors intend to share all individual de-identified participants’ data upon a reasonable request from the corresponding author (email address; [email protected] and [email protected]). The questionnaire can also be shared in the same way. So, data will be available for one year after publication.
Statistical Analysis
Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) version 20. To analyse continuous variables between females with severe and mild dysmenorrhea, we included the mean (M), standard deviation (SD), and used an independent sample t-test. P value less than 0.05 was considered significant. These variables were BMI, age, hours of study per week for students, hours of work for employees, stress level, age of menarche, and days of bleeding.
Chi-Square test of independence was used to analyse the difference between female with severe and mild dysmenorrhea. The results were displayed in categories. P values less than 0.05 were considered significant. These variables were smoking, hours of sleep, education level, consumption of alcohol, fast food, energy drinks, fizzy drinks, tea, coffee, sugar, meat, cereal, fish, 3 servings of fruits, water intake, regular cycle, family history, cycle duration, and use of oral contraceptive pills.
In categorical variables, different p values which test the difference between females with severe and mild dysmenorrhea were given for each category. For example, the difference in smokers had a p-value while the difference in non-smokers had a different p-value. In continuous variables, the mean value in people with severe dysmenorrhea was compared with the mean value in people with mild dysmenorrhea, and the p-value was obtained.
Results
Out of 1988 respondents, the study found that 660 women suffered from primary dysmenorrhea. Around two thirds of them were students. The prevalence among students was 65.3%. Severe dysmenorrhea was reported by 360 women (54.5%). Most of the study population was non-smokers 84.4%, more than two thirds (70.8%) used to sleep from 7 to 9 hours per 24 hours and around one fifth (20.6%) consumed alcohol.
Table 1 shows the prevalence of primary dysmenorrhea impacted by different lifestyle variables.
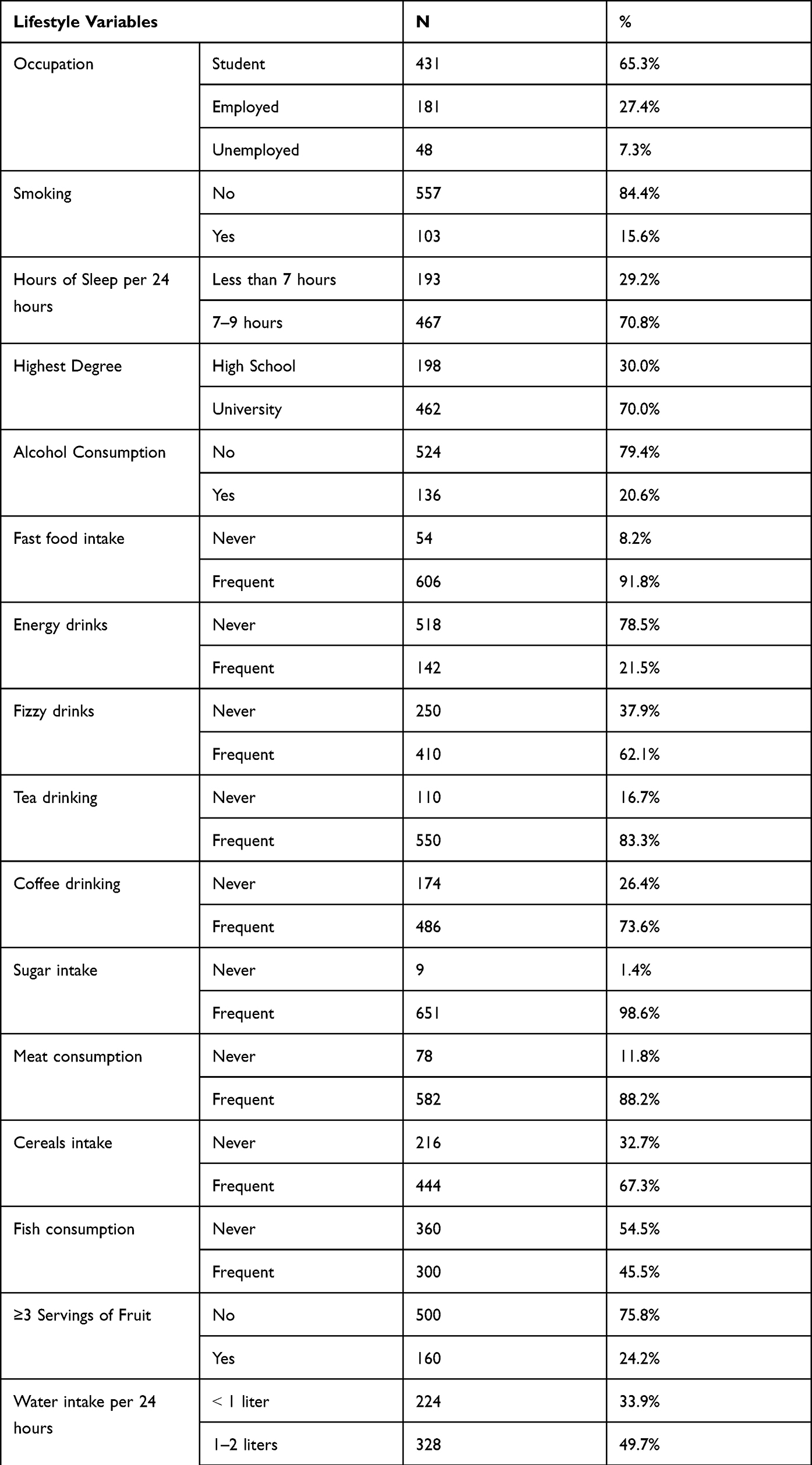 |
Table 1 Prevalence of Primary Dysmenorrhea Among Different Lifestyle Variables |
We then studied the relationship between the different lifestyle variables and the severity of primary dysmenorrhea. The study found that there was a statistically significant correlation between severe dysmenorrhea and smoking at p ˂0.001, sleeping less than 7 hours per 24 hours at p = 0.005, holding a university degree at p = 0.032, non-alcohol consumption at p = 0.044, frequent energy, fizzy, tea, coffee drinks and sugar intake (Table 2). Interestingly, the study found that severe dysmenorrhea was statistically associated with non-meat eaters at p ˂0.001, cereals and fish consumers and with those who used to take less than 3 servings of fruits or none at all per week at p = 0.006 (see Table 2).
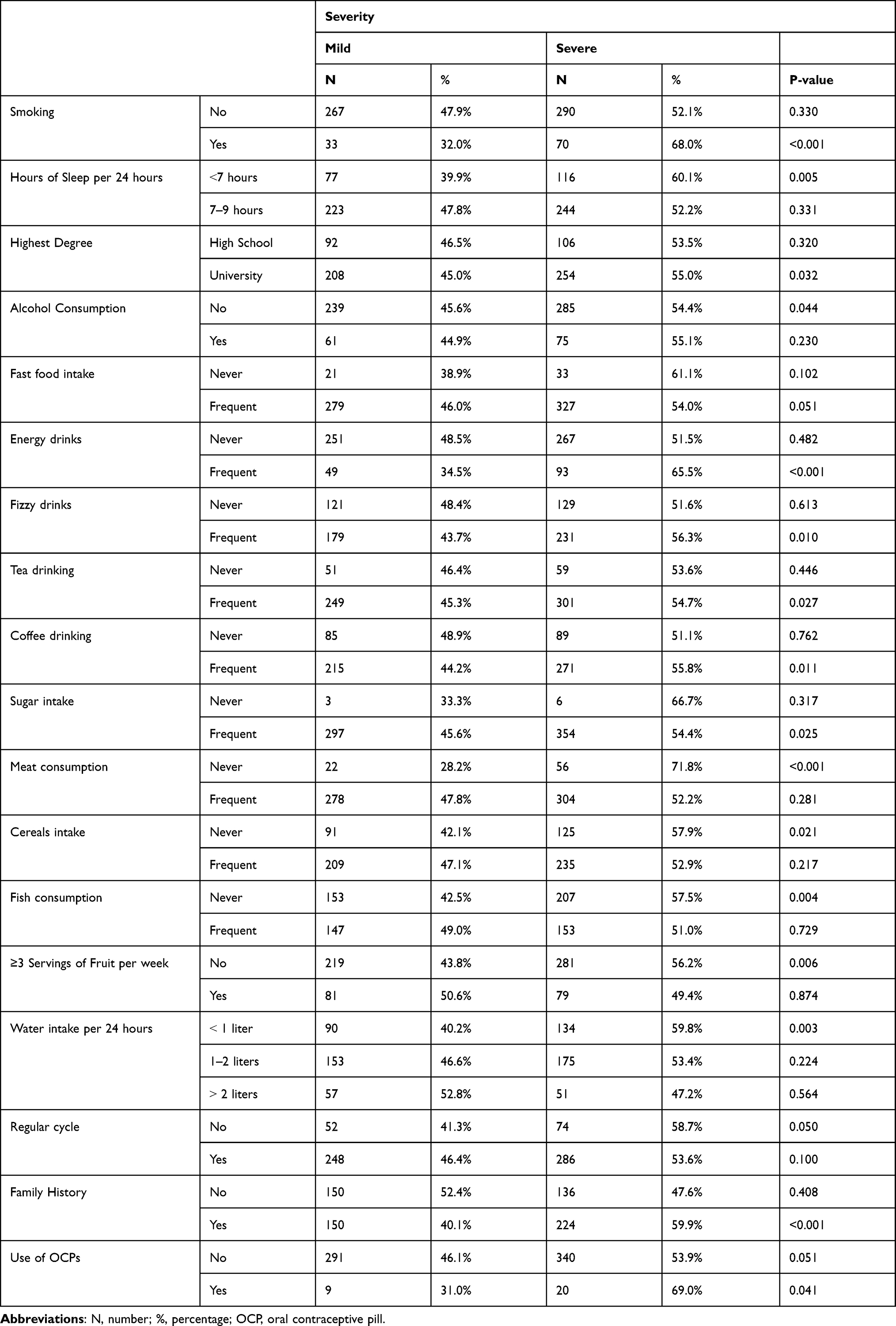 |
Table 2 Severity of Dysmenorrhea in Relation to Different Lifestyle Variables |
Water intake of less than 1.0 litre per 24 hours, irregular cycles, non-OCP use and positive family history were significantly associated with severe dysmenorrhea (see Table 2).
Severe dysmenorrhea was significantly associated with less working hours per week, higher stress level and longer bleeding duration at p= 0.021, 0.017 and 0.008, respectively (see Table 3). However, there was no statistically significant difference found in severity regarding age, BMI, weekly studying hours and age of menarche (see Table 3).
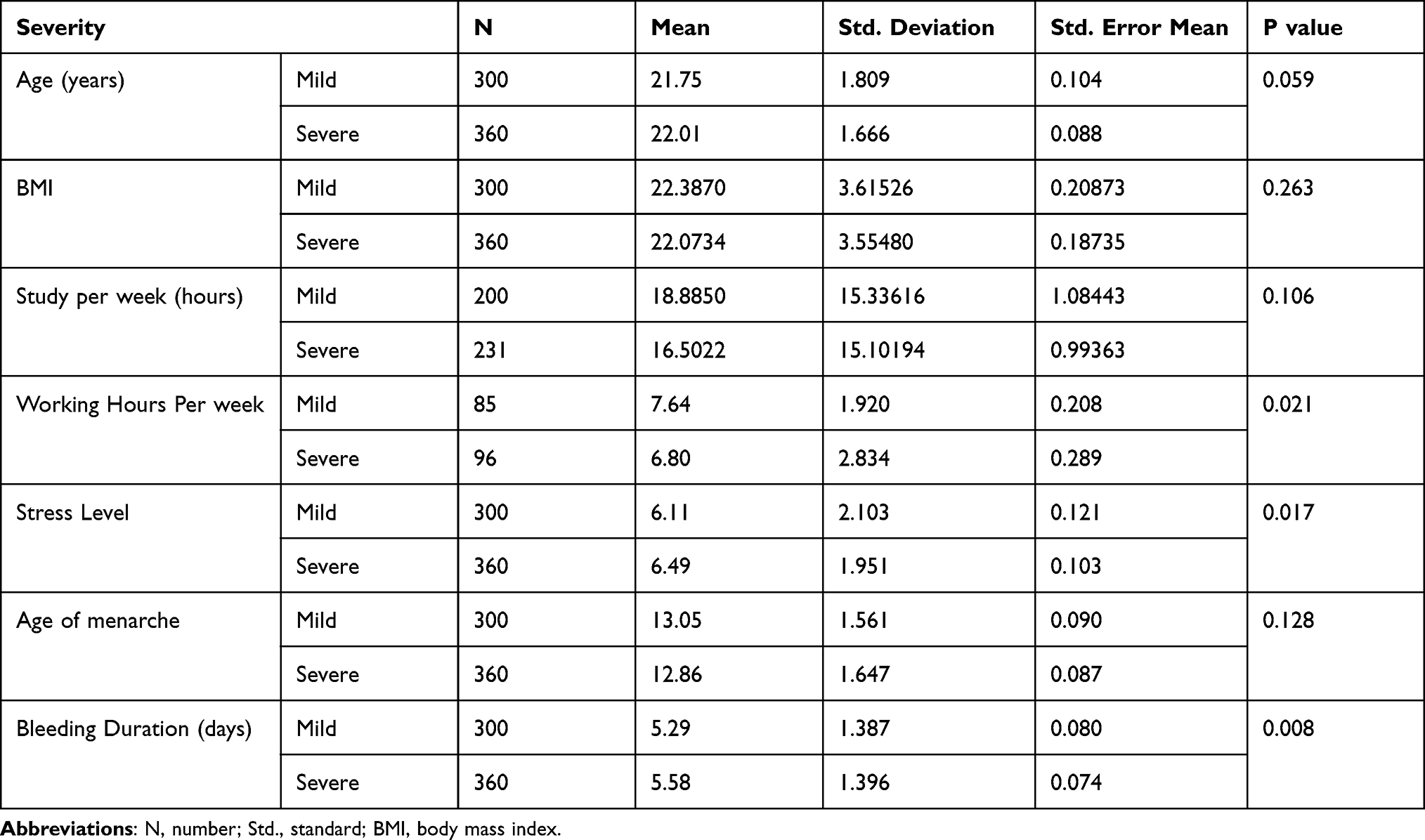 |
Table 3 Severity of Dysmenorrhea in Relation to Lifestyle Variables |
Discussion
The results of the study illustrates that the high prevalence of severe dysmenorrhea is particularly more evident among students, consumers of frequent sugar intake, women with irregular menstrual cycle, women who have heavy bleeding and family history. These findings were consistent with the study of Muluneh et al.5 Unlike the present study, their sample of study included ethnically different population. Furthermore, they also found an association with sexual intercourse which is considered a sensitive issue to explore in our conservative society.
The authors found that smoking, high stress level and less working hours were significantly associated with severe dysmenorrhea.
French L6 found that nulliparity, heavy menstrual flow, smoking, and depression were risk factors that were relevant to dysmenorrhea. The less working hours in our study could be the result of severe dysmenorrhea rather than an underlying aetiology. In support of this view, Ortiz et al7 found that dysmenorrhea had a prevalence at 48.4% and was the cause of school absences for 24% of the affected students. By the same token, De Sanctis et al8 added that prevalence of primary dysmenorrhea in adolescents vary between 16% and 93% compared to 65.3% in our study. One-third to one-half of females with primary dysmenorrhea were missing school or work at least once per cycle, and more frequently affected from 5% to 14% of them.8 They also illustrated that earlier age of menarche, long menstrual periods, heavy menstrual flow, smoking and positive family history were risk factors. They reported that young women using oral contraceptive pills (OCP) experienced less severe dysmenorrhea. Our study showed that only 4.4% of OCP users reported dysmenorrhea compared to 95.6% of non-OCP users. This result was statistically significant at p =0.041. In a randomized controlled trial by Uysal et al,9 they found two types of OCP to be effective for relieving pain. The present study did not specify the type of OCP used by Jordanian women which is one of the limitations that future study may consider investigating. However, OCP in our study could have been prescribed as treatment for some women. In a prospective observational cohort study, Grandi et al10 found that different OCPs reduced similar primary dysmenorrhea and one of them also reduced withdrawal bleedings.
Our findings of less sleeping hours, smoking and dietary effect on the prevalence and severity of dysmenorrhea were evident. In a cross-sectional study by Gagua et al11 family history of dysmenorrhea was a risk factor for dysmenorrhea. The prevalence of dysmenorrhea was significantly higher among smokers versus non-smokers, increased sugar intake reported a marked increase of dysmenorrhea compared to women who reported no daily sugar intake.
Alcohol intake was not correlated with dysmenorrhea. Despite that only 136 women in our study reported alcohol consumption, we found a statistically significant increase of severe dysmenorrhea among those who did not drink alcohol. Yet, it is worth to mention that there was no significant difference in severity among those who used to drink alcohol. This finding clarifies the impact that the alcohol consumption has on menstruation. Huang et al12 found that A. Officinarum 80% alcohol extract can significantly relieve primary dysmenorrhea.
Additionally, Parazzini et al13 found that the relative risk of dysmenorrhea was increased by smoking and decreased among alcohol drinkers. In consistency with this result, a meta-analysis of observational study conducted by Qin et al14 found a significant association between cigarette smoking (both current and former smoking) and dysmenorrhea. Another meta-analysis conducted by Jenabi et al15 found a significant association between smoking and dysmenorrhea.
Frequent intake of coffee, tea, energy and fizzy drinking, drinking less than 1.0 litre of water per 24 hours were found in our study to be associated with severe dysmenorrhea. The present study reported that there was no significant difference in the severity of dysmenorrhea among women who consumed fresh fruits. However, there was a statistically significant increase in severe dysmenorrhea among women who did not consume fruits. Zeru et al16 in a case control study found that thyme tea-drinking, consumption of vegetables and fruits had a relieving effect while coffee drinking was positively associated with primary dysmenorrhea. In a study conducted in Kuwait involving a similar ethnicity to ours, Al-Matouq et al17 found that there was a significant association between drinking coffee and dysmenorrhea.
Another important variable was fish consumption by Jordanian women which was not a well-established dietary habit. In the present study, severe dysmenorrhea was statistically significantly as seen more in non-fish consumers. On the other hand, among frequent fish consumers, there was no significant difference between mild and severe dysmenorrhea suggesting a relieving impact of fish consumption on dysmenorrhea. Fatty acids had shown to be beneficial factor on depressive disorder, behaviour, mood, pre-menstrual syndrome and dysmenorrhea.18 Omega-3 was also found to be more effective than calcium for primary dysmenorrhea.19 In the same vein, Rahbar et al20 found that omega-3 fatty acids supplements reduced the symptom intensity of primary dysmenorrhea and decreased the dose of ibuprofen needed. In a review conducted by Saldeen et al21 omega-3 fatty acids were associated with several health benefits for women.
Fernández-Martínez et al22 found that the risk factors for mild and moderate dysmenorrhea among Spanish university students to be not using OCP, long duration of bleeding, family history (first degree) of dysmenorrhea, drinking cola drinks and eating meat Similarly the present study showed that severe dysmenorrhea was significantly associated with non-meat consumers. Those who consumed meat frequently, in our population, showed no significant difference in the severity of dysmenorrhea. This difference could possibly be due to different study population, different ethnicity and differences in the quality of consumed meat, and preparation or sources between Spain and Jordan.
Although Khalid et al23 found that dysmenorrhea was significantly associated with body mass index and age, those two factors were not found to affect the severity of dysmenorrhea in our study. However, Çinar et al24 found that increased BMI increased the tendency to have less severe pain.
Our study strength involves women from all over the country with different social and cultural backgrounds. These findings represent a platform for managing this common condition in our society and will help health providers counsel and approach these patients.
This research recommends studying the influence of lifestyle variables’ interventions on the severity of dysmenorrhea.
Conclusion
Primary dysmenorrhea is prevalent among Jordanian population. The study concluded that severe dysmenorrhea could be treated by increasing consumption of fish and fresh fruits, water drinking and use of oral contraceptive pills. Clearly, smoking, frequent intake of sugar, fizzy drinks, coffee, tea and energy drinks are associated with severe dysmenorrhea. Drinking alcohol, on the other hand, has a beneficial impact on dysmenorrhea.
Abbreviations
OCP, oral contraceptive pill; BMI, body mass index; HRQoL, health-related quality of life; IRB, institutional review board; SPSS, Statistical Package for Social Sciences.
Registration Number
NCT04583943
Ethics Approval and Consent to Participate
The study obtained an institutional review board (IRB) approval at Jordan University Hospital (decision number 280/2020 dated 17/11/2020).
To obtain consent from participants, the following statement was included at the beginning of the questionnaire in Arabic and English (see Supplementary File 1): “Please note, your participation in this survey is completely voluntary. All the data recorded through this survey will be maintained confidential and the identity of the participant will be kept anonymous.
All participants were informed about the purpose of the survey, and that it was conducted in accordance with the Declaration of Helsinki.
The respondent read; I grant permission for the data generated from this survey to be used in the researcher’s publications on this topic;
Yes
No
Only participants who responded with “Yes” were included in this research.
Consent for publication: Consent was granted from participants to use their responses in the researcher’s publication on the topic.
Availability of data and materials: The datasets generated and/or analysed during the current study are not publicly available due to the consent given by the participants. The data to be used in the researcher’s publication on this topic only, but data can be made available by the corresponding author upon a reasonable request.
It is registered in Clinicaltrial.gov (ID: NCT04583943).
Acknowledgment
The authors thank all participants for taking the time to complete the questionnaire.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Iacovides S, Avidon I, Baker FC. What we know about primary dysmenorrhea today: a critical review. Hum Reprod Update. 2015;21(6):762–778. PMID: 26346058. doi:10.1093/humupd/dmv039
2. Hu Z, Tang L, Chen L, Kaminga AC, Xu H. Prevalence and risk factors associated with primary dysmenorrhea among Chinese female university students: a Cross-sectional Study. J Pediatr Adolesc Gynecol. 2020;33(1):15–22. doi:10.1016/j.jpag.2019.09.004
3. Chantler I, Mitchell D, Fuller A. Actigraphy quantifies reduced voluntary physical activity in women with primary dysmenorrhea. J Pain. 2009;10:38–46. doi:10.1016/j.jpain.2008.07.002
4. Unsal A, Ayranci U, Tozun M, Arslan G, Calik E. Prevalence of dysmenorrhea and its effect on quality of life among a group of female university students. Ups J Med Sci. 2010;115(2):138–145. PMID: 20074018; PMCID: PMC2853792. doi:10.3109/03009730903457218
5. Muluneh AA, Nigussie T, Gebreslasie K, et al. Prevalence and associated factors of dysmenorrhea among secondary and preparatory school students in Debremarkos town, North-West Ethiopia. BMC Women’s Health. 2018;57:18. doi:10.1186/s12905-018-0552-x
6. French L. Dysmenorrhea. Am Fam Physician. 2005;71(2):285–291. PMID: 15686299.
7. Ortiz MI, Rangel-Flores E, Carrillo-Alarcón LC, Veras-Godoy HA. Prevalence and impact of primary dysmenorrhea among Mexican high school students. Int J Gynecol Obstet. 2009;107(3):240–243. doi:10.1016/j.ijgo.2009.07.031
8. De Sanctis V, Soliman A, Bernasconi S, et al. Primary dysmenorrhea in adolescents: prevalence, impact and recent knowledge. Pediatr Endocrinol Rev. 2015;13(2):512–520. PMID: 26841639.
9. Uysal G, Akkaya H, Cagli F, Tutus S, Tayyar AT. A comparison of two different oral contraceptives in patients with severe primary dysmenorrhoea. J Obstet Gynaecol. 2018;38(6):828–832. PMID: 29537325. doi:10.1080/01443615.2017.1410533
10. Grandi G, Napolitano A, Xholli A, Tirelli A, Di Carlo C, Cagnacci A. Effect of oral contraceptives containing estradiol and nomegestrol acetate or ethinyl-estradiol and chlormadinone acetate on primary dysmenorrhea. Gynecol Endocrinol. 2015;31(10):774–778. PMID: 26291811. doi:10.3109/09513590.2015.1063118
11. Gagua T, Tkeshelashvili B, Gagua D. Primary dysmenorrhea: prevalence in adolescent population of Tbilisi, Georgia and risk factors. J Turk Ger Gynecol Assoc. 2012;13(3):162–168. PMID: 24592031; PMCID: PMC3939234. doi:10.5152/jtgga.2012.21
12. Huang L, Zhang JQ, Li YB, et al. Effect of Alpinia officinarum Hance alcohol extracts on primary dysmenorrheal. Asian Pac J Trop Med. 2016;9:882–886. PMID: 27633303. doi:10.1016/j.apjtm.2016.07.012
13. Parazzini F, Tozzi L, Mezzopane R, Luchini L, Marchini M, Fedele L. Cigarette smoking, alcohol consumption, and risk of primary dysmenorrhea. Epidemiology. 1994;5(4):469–472. PMID: 7918820. doi:10.1097/00001648-199407000-00016
14. Qin LL, Hu Z, Kaminga AC, et al. Association between cigarette smoking and the risk of dysmenorrhea: a meta-analysis of observational studies. PLoS One. 2020;15(4):e0231201. PMID: 32294123; PMCID: PMC7159229. doi:10.1371/journal.pone.0231201
15. Jenabi E, Khazaei S, Veisani Y. The relationship between smoking and dysmenorrhea: a meta-analysis. Women Health. 2019;59(5):524–533. PMID: 30481133. doi:10.1080/03630242.2018.1508541
16. Zeru AB, Muluneh MA. Thyme tea and primary dysmenorrhea among young female students. Adolesc Health Med Ther. 2020;11:147–155. PMID: 33117031; PMCID: PMC7585774. doi:10.2147/AHMT.S280800
17. Al-Matouq S, Al-Mutairi H, Al-Mutairi O, et al. Dysmenorrhea among high-school students and its associated factors in Kuwait. BMC Pediatr. 2019;19(1):80. PMID: 30885151; PMCID: PMC6421654. doi:10.1186/s12887-019-1442-6
18. Kidd PM. Omega-3 DHA and EPA for cognition, behavior, and mood: clinical findings and structural-functional synergies with cell membrane phospholipids. Altern Med Rev. 2007;12(3):207–227. PMID: 18072818.
19. Mehrpooya M, Eshraghi A, Rabiee S, Larki-Harchegani A, Ataei S. Comparison the effect of fish-oil and calcium supplementation on treatment of primary dysmenorrhea. Rev Recent Clin Trials. 2017;12(3):148–153. PMID: 28356030. doi:10.2174/1574887112666170328125529
20. Rahbar N, Asgharzadeh N, Ghorbani R. Effect of omega-3 fatty acids on intensity of primary dysmenorrhea. Int J Gynaecol Obstet. 2012;117(1):45–47. PMID: 22261128. doi:10.1016/j.ijgo.2011.11.019
21. Saldeen P, Saldeen T. Women and omega-3 Fatty acids. Obstet Gynecol Surv. 2004;59(10):
22. Fernández-Martínez E, Onieva-Zafra MD, Parra-Fernández ML. Lifestyle and prevalence of dysmenorrhea among Spanish female university students. PLoS One. 2018;13(8):e0201894. PMID: 30096156; PMCID: PMC6086430. doi:10.1371/journal.pone.0201894
23. Khalid M, Jamali T, Ghani U, Shahid T, Ahmed T, Nasir T. Severity and relation of primary dysmenorrhea and body mass index in undergraduate students of Karachi: a cross sectional survey. J Pak Med Assoc. 2020;70(7):1299–1304. PMID: 32799302. doi:10.5455/JPMA.18303
24. Çinar GN, Akbayrak T, Gürşen C, et al. Factors related to primary dysmenorrhea in Turkish women: a multiple multinomial logistic regression analysis. Reprod Sci PMID: 32780360. 2020;28:381–392. doi:10.1007/s43032-020-00289-1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.