")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 15
The Influence of an Unexpected Switch of Hemodialysis Facilities on the Quality of Life (QOL) in Hemodialysis Patients
Authors Shimizu Y , Wakabayashi K, Nakata J, Io H, Hamada C, Tomino Y, Suzuki Y
Received 18 January 2022
Accepted for publication 6 April 2022
Published 13 April 2022 Volume 2022:15 Pages 151—160
DOI https://doi.org/10.2147/IJNRD.S358915
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Yoshio Shimizu,1,2 Keiichi Wakabayashi,1 Junichiro Nakata,3 Hiroaki Io,4 Chieko Hamada,5 Yasuhiko Tomino,6 Yusuke Suzuki3
1Department of Nephrology, Juntendo University Shizuoka Hospital, Izunokuni-shi, 410-2211, Japan; 2Shizuoka Medical Research Center for Disaster, Izunokuni-shi, 410-2211, Japan; 3Division of Nephrology, Department of Internal Medicine, Juntendo University Faculty of Medicine, Tokyo, 113-8421, Japan; 4Division of Nephrology, Juntendo University Nerima Hospital, Tokyo, 117-8521, Japan; 5Juntendo University Faculty of Health Sciences and Nursing, Mishima-shi, 411-8787, Japan; 6Asian Pacific Renal Research Promotion Office, Medical Corporation SHOWAKI, Tokyo, 160-0023, Japan
Correspondence: Yoshio Shimizu, Division of Nephrology, Department of Internal Medicine, Juntendo University Shizuoka Hospital, 1129 Nagaoka, Izunokuni-shi, Shizuoka, 410-2211, Japan, Tel +81-55-948-3111, Fax +81-55-946-0858, Email [email protected]
Background: We experienced a sudden breakdown of hemodialysis system during a clinical study of dermal itch and serum BNP concentrations.
Patients and Methods: Forty-eight hemodialysis patients were enrolled in the itch-related study. It was intended to improve itch by lowering BNP with supportive communication between the patients and the dialysis staff. We planned to collect data, including visual analogue scale (VAS), dermatology life quality index (DLQI), blood samples and QOL score (KDQOL-SF), four times over a four week interval. The first data was obtained just prior to switching facilities due to a breakdown. The patients underwent hemodialysis in other facilities for two weeks and underwent determination of their clinical data, including QOL scores, three times.
Results: While mean blood pressure showed no significant differences, serum albumin, iron and phosphate levels were worsened significantly between pre- and post-relocation. Serum BNP and DLQI showed no significant changes. VAS was significantly worsened. The mean values of the cognitive function in the KDQOL-SF and sleep and the role-physical, role-emotional, social function, dialysis staff’s encouragement in SF-36 analysis were identified as statistically significant items by MANOVA. Both SF-12 physical and mental composites were also statistically significant. Although SF-12 physical composites were significant among the patients under 66 yrs of age (median), eight factors were significant among those over 66 yrs. Independent analyses revealed every item that was detected worsened significantly after the switch of facilities.
Conclusion: Unexpected switching of hemodialysis facilities severely impacts the QOL for a long duration as well as the patients’ symptom and laboratory data.
Keywords: KDQOL-SF, switch of hemodialysis facilities, dermal itch
Introduction
Most patients undergoing maintenance hemodialysis receive treatments at hemodialysis facilities close to their homes. Huge disasters including earthquakes, Tsunami, floods, hurricanes, etc., can force dialysis facilities to close and patients to evacuate from their living communities.1 After the Great East Japan Earthquake in 2011, following the Tsunami and Fukushima Daiichi nuclear power plant accident, about 10,000 hemodialysis patients evacuated from their hometowns and continued to undergo hemodialysis in surrogate facilities adjacent to their temporary housings.2,3 Those who have relocated after disasters tend to exhibit various physical and mental symptoms.4–6 The evacuated victims of the Great East Japan Earthquake undergoing hemodialysis also exhibited similar problems and lowering of their quality of life (QOL).7–9
While these studies have revealed the relationships between relocation of the living place and lowering of the QOL, the effects of unexpected changes of hemodialysis facilities have not been reported. We experienced an unexpected and temporal switching of hemodialysis patients to other facilities due to a sudden breakdown of the water supplying system. Just one week prior to this accident, we started a clinical study to examine the relationships between dermal itch and serum B-type natriuretic peptide (BNP). Visual analogue score (VAS) for itch, dermatology life quality index, blood samples, including BNP levels, and QOL score (KDQOL-SF) were obtained from each patient with the purpose of examining relationships between dermal itch, serum BNP and QOL.10 Two weeks after the accident, the patients returned to our facility and maintenance hemodialysis was reinitiated. According to the protocol, QOL scores were collected repeatedly three times over a one month interval.
Patients and Methods
Patients
Forty-eight patients undergoing maintenance hemodialysis in the Juntendo University Hospital were enrolled in this study. This group consisted of 29 males and 19 females, with a mean age of 65-yrs. Seventeen patients (39.6%) suffered from diabetic kidney disease. Additional demographic data are summarized in Table 1.
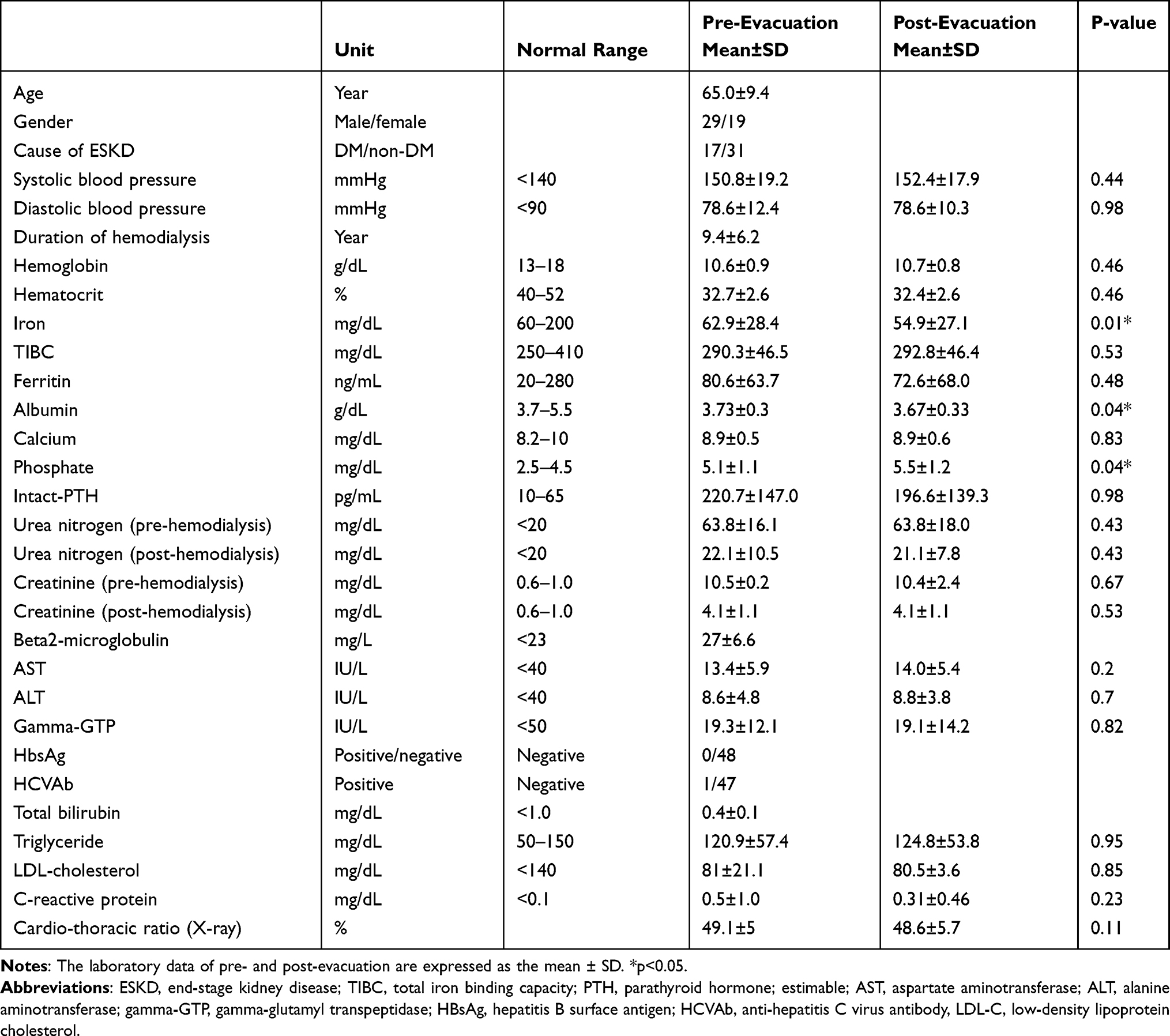 |
Table 1 Patient’s Background and Laboratory Data Pre- and Post- Evacuation |
Itch-Related Study
We previously reported that higher serum BNP concentrations were closely related to dermal itch in hemodialysis patients.11 As the next step, we intended to show causation by reducing the itch through attenuation of the serum BNP levels. Since serum BNP levels in hemodialysis patients are critical to body weight gain during dialysis interval and target dry weight settings, we planned a supportive communication method between patients and dialysis staff. An attending doctor and nursing staff were assigned to each patient. In each session, they reported the patient’s body weight and any gain between dialysis intervals. When the weight gain was above 5% of the target dry weight, the staff gave a “yellow card”, like in professional football games (Figure 1A). For those who exhibited elevated BNP concentrations, the staff attempted to reduce their target dry weight. The staff also discussed how the patients could improve their lifestyles, including diets, drinking and exercise. If necessary, they consulted experts, ie, nutritionists, physical therapists and clinical counselors. Thus, we enforced daily activities.
 |
Figure 1 (A) The yellow card. The patients whose pre-dialysis weight gained more than 5% of the target dry weight during the hemodialysis interval received this card. The card informed the patients that they had increased their body weight too much and exceeded the limit (5% of the target dry weight). (B) The time course of this study. The time course of the study that intended to weaken dermal itch by lowering the serum BNP concentration and timing of the accident with the water supply system. The collection of data, including VAS, DLQI, Blood sample and KDQOL-SF and movement of the patients, are shown. |
Data Collection
In December 20XX, VAS for dermal itch, DLQI, blood samples and kidney disease-specific QOL score (KDQOL-SF) responses were collected for the first time (test 0). Supportive communication to reduce body weight gain and serum BNP was initiated simultaneously. The following week, the dialysis center was closed after the hemodialysis fluid supplying system was severely damaged. Every patient had to undergo hemodialysis in another facility. One week later, the fluid supplying system was fixed and the treatments at the dialysis center resumed. The patients returned to start maintenance hemodialysis. One month after collecting the first responses for KDQOL-SF, the second survey (test 1) administered. The third (test 2) and fourth surveys (test 3) were administered in one month intervals. During the evacuation, a male patient died due to acute coronary syndrome in the surrogate clinic. Two patients decided to continue hemodialysis at the alternative facilities since they lived more than 50 km from the conventional facility. Another male patient died of heart failure between the second and third surveys. Four patients refused to take the third survey and other four patients took the fourth (Figure 1B).
The KDQOL-SF is a modified version of SF-36 that was developed specifically for the dialysis patients12 and was validated for Japanese patients.13 The KDQOL-SF contains eight evaluation items: symptoms or problems, effects of kidney disease on daily life, burden of kidney disease, work status, cognitive function, quality of social interaction, sexual function and sleep. Additionally, SF-36 health survey including physical function, physical role, pain, general health, emotional well-being, emotional role, social function and energy/fatigue can be evaluated. A non-health related QOL survey including social support, dialysis staff encouragement and patient satisfaction was administered simultaneously.
Short form QOL surveys (SF-12 physical composite and mental composite) were also administered. A better QOL was indicated by a higher score of the KDQOL-SF.
Clinical Data Collection
Clinical data of the patients, including age, gender, cause of end-stage kidney disease, and blood samples were collected from the electronic medical record system in the Juntendo University Hospital. Blood pressure and laboratory data, including hemoglobin, iron, total iron binding capacity (TIBC), ferritin, calcium, phosphate, intact-PTH, urea nitrogen, creatinine, AST, ALT, gamma-GTP, triglyceride, LDL-cholesterol and C-reactive protein (CRP), from blood samples at the time of first survey (test 0) and one month later (test 1) were also collected for statistical analysis. All blood samples were taken at the beginning of hemodialysis on Monday or Tuesday two days after the last session. Serum BNP was measured in samples obtained post-dialysis.
Statistical Analyses
Data are expressed as the mean ± standard deviation (SD). The data from blood samples between test 0 and test 1 were compared by paired- student’s t test. The mean values between the four surveys were compared by multivariate analysis of variance (MANOVA). Dunnett’s test was applied for each test separately in the analyses of the differences between control data, the first survey (test 0) and the other tests. To examine the effect of age, independent analyses were performed using all patients, patients under 66-yrs of age (median) and over 66-yrs. Statistical significance was considered at p<0.05. All statistical analyses were performed using JMP 7.02 (SAS Institute Inc., Cary, NC) software.
Results
Laboratory Data
The mean blood pressure of the patients did not change after switching of the dialysis facilities. Serum albumin, iron and phosphate levels were worsened between pre- and post-switch of hemodialysis facilities (Table 1).
Itch Related Study
Although supportive communication was maintained to control the patient’s weight gain, except for during the evacuation period, serum BNP levels did not change significantly. Skin condition QOL score (DLQI) showed no significant change throughout the whole studying period. While VAS for itch suggested a significant change, it was worsened after evacuation until test 2 (Table 2, Figure 2)
 |
Table 2 Analyses of Dermal Itch-Related Values |
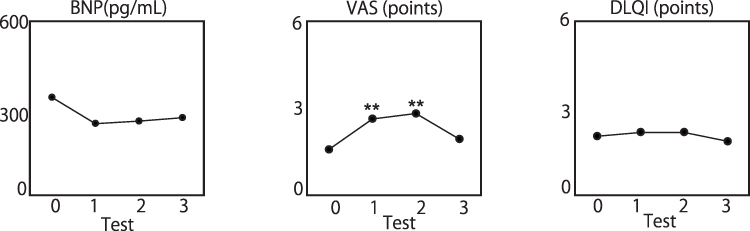 |
Figure 2 Controlling BNP and itch was failed. The mean values of each test is shown and tests 1, 2 and 3 were compared with the pre-relocated data, test 0 using MANOVA (**p<0.01). The supportive method did not change the patient’s serum BNP concentration or DLQI scores. VAS was worsened after switching facilities. |
MANOVA of KDQOL-SF
Among the kidney disease-specific QOL items, the mean values of cognitive function and sleep were significantly different (0.031, 0.045, respectively). The SF-36 health survey revealed that the values of role- physical (p=0.029), pain (p=0.018), role emotional (p=0.039), social function (p=0.038) changed significantly during the surveys. Among the items of the non-health related QOL surveys, dialysis staff encouragement revealed significant changes. Both of the SF-12 physical and the mental composite revealed any significant changes of the patients’ QOL (p=0.013, p=0.034) (Table 3).
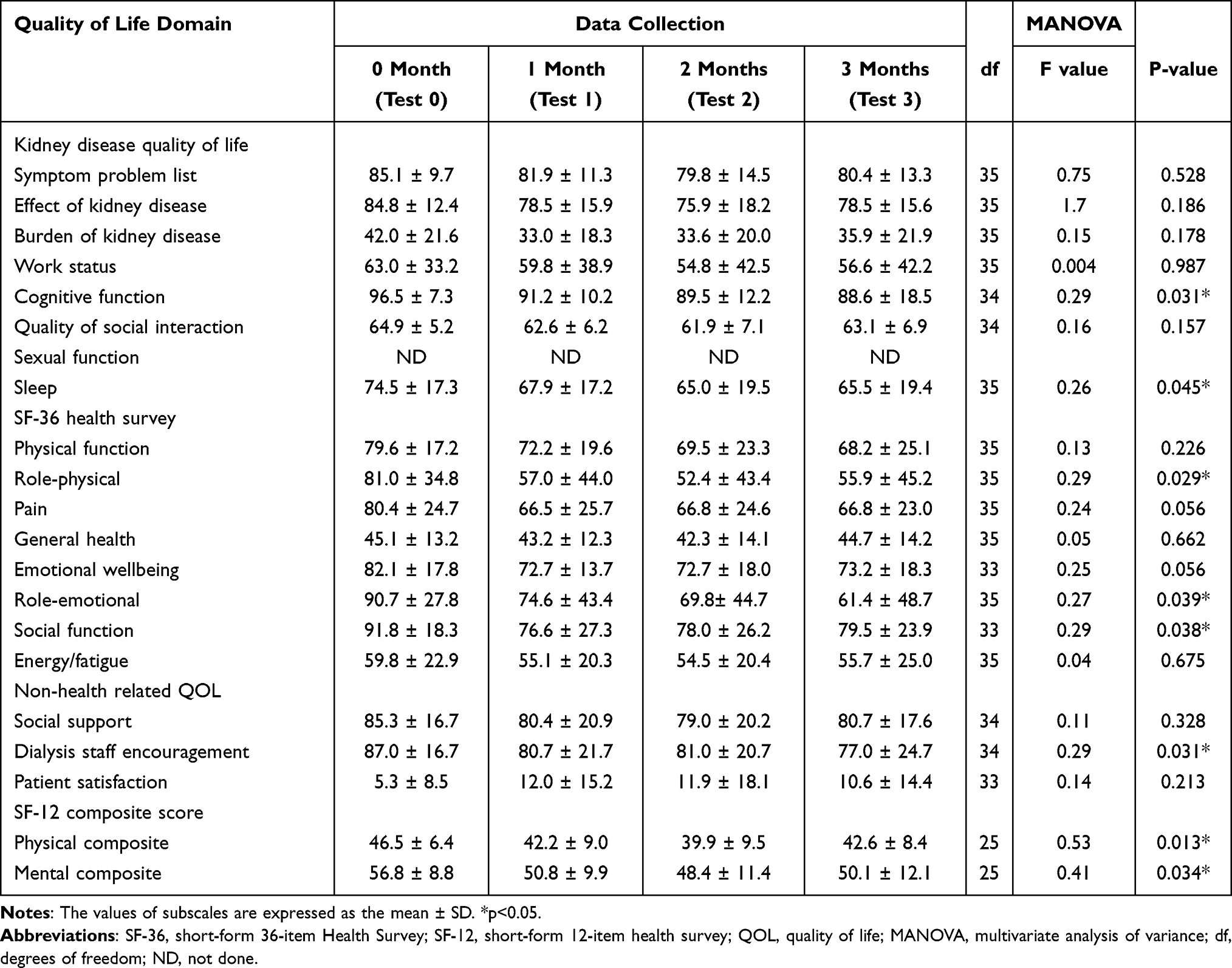 |
Table 3 Chronological Changes in Subscales of KDQOL-SF |
Independent Analyses
All of the items for patients’ QOL selected by MANOVA showed that the scores worsened after the first survey. All of the patient’s values for sleep, role-physical, social function, SF-12 physical and mental composite in tests 1, 2, 3 were significantly lower than those of test 1. The scores of cognitive function, role-emotional and dialysis staff encouragement were gradually reduced and showed significant lowering two or three months after evacuation (Figure 3A).
 |
Figure 3 Significantly changed subscales of KDQOL-SF during the study. The mean values of each test are shown. The values of tests 1, 2, 3 were compared with test 0 using MANOVA (*p<0.05, **p<0.01). (A) The analyzed data from all of the patients. (B) The analyzed data from the patients under 66 years (median) old. Only SF-12 Physical composite was significantly different. (C) The analyzed data from the patients over 66 years old. |
The patients under 66-yrs of age exhibited significant reduction of the SF-12 physical composite. The scores of test 3 were recovered and showed reduced significance compared to those of test 0 (Figure 3B).
The patients over 66-yrs of age showed significant worsening in multiple subscales of KDQOL-SF. Most of the scales for test 1 were significantly lower than test 0. Dialysis staff encouragement showed a pattern similar to that of all of the patients. With the exception of the effect of kidney disease, the values of test 3 remained significantly lower compared to those of test 0 (Figure 3C).
Discussion
Since we read a report that BNP was a candidate of stimulator for itch transmission,14 we have studied the relationships between BNP and itch in hemodialysis patients.11 Our observational study suggested serum hyper-BNP related daytime itch in non-diabetic patients. Then, we attempted to control itch by lowering serum BNP. By ethical restriction, we could perform the supportive communication method and the protocol was approved by ethics committee of the Juntendo University. Unfortunately, owing to water-supply system breakdown, our hemodialysis unit was closed just after starting study. But the member of our group adhered to the protocol.
Returned patients showed lowering serum albumin, iron and elevated phosphate. Most of the surrogate facilities have close relationships and collaborate with ours. Every patient’s protocol of hemodialysis was sent and the records from surrogate facilities showed that the patients were given adequate dialysis. The change of serum albumin and phosphate might be driven by changing dietary habits. It was possible that lowering iron was due to stopping supplementation.
Our plan for reducing weight gain and serum BNP was failed. Patient’s itch was worsened. These phenomena might reveal the limitation of the supportive methods or shortage of study period. While the itch was worsened, DLQI was not changed. Although the VAS score significantly elevated after the switch of dialysis facilities, the patients had mild itch with mean VAS score was 1.6 at the beginning of the study. The elevated mean VAS score was 2.7 (Table 2). Previous validation studies revealed that the heavier intensity of itch gave the more impact on patient’s QOL scores.15,16 Thus, the increase of the VAS score influenced subtle impact on DLQI. DLQI limits to show the impact of skin troubles on QOL, the dissociation between DLQI and KDQOL suggests the impact of sudden switch of dialysis facilities.
The 36-items which show functioning and well-beings were assessed by KDQOL-SF. Among whole patients, they were significantly disturbed in cognitive function, sleep, role-physical, role-emotional, social function, dialysis staff encouragement, SF-12 physical and social composites (Figure 3A). The role-physical and role-emotional reflect the interference on the job and daily activities by physical and mental troubles, respectively. Social function suggests the effect on the relationships among the patients and their family members, neighbors and friends. SF-12 physical and mental composites are summarized the change of QOL by physical and mental disturbances.12 The physical and mental dimensions between SF-12 and SF-36 exhibit excellent correlation.17
Older patients (>66-yrs) significantly interfered on Effect of kidney disease, burden of kidney disease, physical functioning, pain, role-emotional, social function and SF-12 mental composite (Figure 3C). The effect means the direct effect of kidney disease on daily life. “Burden” does time, money or efforts of patients and families to maintain daily life. The decrease of the physical functioning suggested the patients felt more difficulty for daily activities including taking a bath, changing clothes etc.12 They showed long physical and mental interference while social function gradually improved. This suggested the effect of returning to the home facility.
We learned that there are six infrastructures that are indispensable to maintaining daily hemodialysis: 1) buildings, 2) hemodialysis equipment, 3) electrical power supply, 4) water supply, 5) dialysis materials and 6) dialysis workforce, after the experiences of the Great East Japan Earthquake on March 11, 2011.18 If one of these essential infrastructures is lacking, the patients cannot receive adequate treatment. Especially, a lack of electric power or water supply can put a hemodialysis center out of order for a long time.18 In this situation, transient switching of dialysis facilities is one of the solutions for continuing treatment.
After the Great East Japan Earthquake, many hemodialysis patients in Tohoku district were evacuated from their hometown to Niigata, Hokkaido, Chiba and Tokyo and underwent hemodialysis in unfamiliar environments.2 The patients worried about their families who were left behind, their homes, evacuating methods, financial costs, the duration and joining unfamiliar patients when they were told the necessities of evacuation.19 Relocation after disasters is considered to be associated with increased mental health problems.20 Studies among the earthquake survivors have reported various symptoms, including post-traumatic stress disease (PTSD), PTSD-like and depression.21,22 Relocation after disasters is also considered to be associated with increased mental health problems.20 Post-traumatic stress and depression are negatively associated with QOL after disaster.23
Compared to these studies, our experience is unique since the cause of the physical and mental distress was limited to the unexpected switching of hemodialysis facilities. Every patient received adequate treatment and did not experience home re-location. The most severe impact on each of the patient’s mental condition might be induced by a lack of human communication with the dialysis staff and other patients. One study examining satisfaction with dialysis treatment and QOL revealed that communication between the care provider and the patients plays a favorable role for the QOL.24 Test separately study of KDQOL-SF subscales toward the patients over or under 66-yrs old showed aging related vulnerability for sudden change of surrounding circumstances.
Recent studies have revealed that social networking services enable hemodialysis patients and their families to share information in managing dialysis.25 For young people suffering from mental health problem, social networking service-based interventions were found to be useable, engaging and supportive.26 The lack of communication between the patients and care-providers can be overcoming by developing various communication tools. As such, user-friendly devices are anticipated.
Conclusion
The unexpected switching of hemodialysis facilities severely impacts the patient’s QOL for a long duration as well as the patients’ symptom and laboratory data.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, YS. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Ethics Approval Statement
This study was approved by the Ethics Committee of the Juntendo University Hospital with declaration of Helsinki (No. 14-124). Written informed consent was obtained from the patients.
Acknowledgments
We are indebted to the nephrologists, nursing staff and the patients at the Juntendo University Hospital for their collaboration and participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in conception, study design, execution, acquisition data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the JSPS KAKENHI grants numbered 26461238 and 17K09039. Shizuoka Medical Research Center for Disaster, Juntendo University is supported in part by a Grant-in-Aid for Special Research in Subsidies for ordinary expenses of private schools from The Promotion and Mutual Aid Corporation for Private Schools of Japan.
Disclosure
The authors declare no conflicts of interest associated to this manuscript.
References
1. Ochi S, Hodgson S, Landeg O, Mayner L, Murray V. Disaster-driven evacuation and medication loss: a systematic literature review. PLoS Curr. 2014;18:6.
2. Nangaku M, Akizawa T. Diary of a Japanese nephrologist during the present disaster. Kidney Int. 2011;79:1037–1039. doi:10.1038/ki.2011.106
3. Kazama J, Narita I. Earthquake in Japan. Lancet. 2011;377:1652–1653. doi:10.1016/S0140-6736(11)60673-9
4. Hashimoto S, Nagai M, Fukuma S, et al.; Fukushima Health Management Survey Group. Influence of post-disaster evacuation on incidence of metabolic syndrome. J Atheroscler Thromb. 2017;24:327–337. doi:10.5551/jat.35824
5. Ishiki A, Okinaga S, Tomita N, et al. Changes in cognitive functions in the elderly living in temporary housing after the great East Japan earthquake. PLoS One. 2016;11:e0147025. doi:10.1371/journal.pone.0147025
6. Orui M, Suzuki Y, Maeda M, Yasumura S. Suicide rates in evacuation areas after the fukushima daiichi nuclear disaster. Crisis. 2018;39:353–363. doi:10.1027/0227-5910/a000509
7. Haga N, Hata J, Yabe M, et al. The Great East Japan Earthquake affected the laboratory findings of hemodialysis patients in Fukushima. BMC Nephrol. 2013;14:239. doi:10.1186/1471-2369-14-239
8. Hyre AD, Cohen AJ, Kutner N, et al. Psychosocial status of hemodialysis patients one year after Hurricane Katrina. Am J Med Sci. 2008;336(2):94–98. doi:10.1097/MAJ.0b013e318180f1f1
9. Nishikawa Y, Ozawa Y, Tsubokura M, et al. Long-term vulnerability of access to hemodialysis facilities in repopulated areas after the Fukushima Nuclear Disaster: a case report. Oxf Med Case Rep. 2018;2018(7):omy040. doi:10.1093/omcr/omy040
10. Fukuhara S, Lopes AA, Bragg-Gresham JL, et al. Worldwide Dialysis Outcomes and Practice Patterns Study. ShareHealth-related quality of life among dialysis patients on three continents: the Dialysis Outcomes and Practice Patterns Study. Kidney Int. 2003;64:1903–1910. doi:10.1046/j.1523-1755.2003.00289.x
11. Shimizu Y, Sonoda A, Nogi C, et al. B-type (brain) natriuretic peptide and pruritus in hemodialysis patients. Int J Nephrol Renovasc Dis. 2014;7:329–335. doi:10.2147/IJNRD.S65929
12. Hays RD, Kallich JD, Mapes DL, Coons SJ, Carter WB. Development of the kidney disease quality of life (KDQOL) instrument. Qual Life Res. 1994;3:329–338.
13. Green J, Fukuhara S, Shinzato T, et al. Translation, cultural adaptation, and initial reliability and multitrait testing of the Kidney Disease Quality of Life instrument for use in Japan. Qual Life Res. 2001;10(1):93–100. doi:10.1023/A:1016630825992
14. Mishra SK, Hoon MA. The cells and circuitry for itch responses in mice. Science. 2013;340(6135):968–971. doi:10.1126/science.1233765
15. Gergely LH, Gáspár K, Brodszky V, et al. Validity of EQ-5D-5L, Skindex-16, DLQI and DLQI-R in patients with hidradenitis suppurativa. Eur Acad Dermatol Venereol. 2020;34(11):2584–2592. doi:10.1111/jdv.16642
16. Warlich B, Fritz F, Osada N, et al. Health-related Quality of Life in chronic pruritus: an analysis related to disease etiology, clinical skin conditions and itch intensity.dermatology. 2015;231(3):253–259. doi:10.1159/000437206
17. Lacson E Jr, Xu J, Lin SF, Dean SG, Lazarus JM, Hakim RM. A comparison of SF-36 and SF-12 composite scores and subsequent hospitalization and mortality risks in long-term dialysis patients. Clin J Am Soc Nephrol. 2010;5:252–260. doi:10.2215/CJN.07231009
18. Ikegaya N, Seki G, Ohta N. How should disaster base hospitals prepare for dialysis therapy after earthquakes? Introduction of double water piping circuits provided by well water system. Biomed Res Int. 2016;2016:9647156. doi:10.1155/2016/9647156
19. Motomiya H. Assessment of nursing care during East Japan great earthquake. J Japan Acad Nephrol Nurs. 2012;14:131–134. Japanese.
20. Norris FH, Friedman MJ, Watson PJ. 60,000 disaster victims speak: Part II. Summary and implications of the disaster mental health research. Psychiatry. 2002;65:240–260. doi:10.1521/psyc.65.3.240.20169
21. Bland SH, Valoroso L, Stranges S, Strazzullo P, Farinaro E, Trevisan M. Long-term follow-up of psychological distress following earthquake experiences among working Italian males: a cross-sectional analysis. J Nerv Ment Dis. 2005;193:420–423. doi:10.1097/01.nmd.0000165297.49452.41
22. Watanabe C, Okumura J, Chiu TY, Wakai S. Social support and depressive symptoms among displaced older adults following the 1999 Taiwan earthquake. J Trauma Stress. 2004;17:63–67. doi:10.1023/B:JOTS.0000014678.79875.30
23. Siqveland J, Nygaard E, Hussain A, Tedeschi RG, Heir T. Posttraumatic growth, depression and posttraumatic stress in relation to quality of life in tsunami survivors: a longitudinal study. Health Qual Life Outcomes. 2015;13:18. doi:10.1186/s12955-014-0202-4
24. Cirillo L, Toccafondi A, Cutruzzulà R, et al. Association between satisfaction with dialysis treatment and Quality of Life: a Cross-Sectional Study. Blood Purif. 2020;1–8. doi:10.1159/000509787
25. Ahmed S, Haines-Saah RJ, Afzal AR, et al. User-driven conversations about dialysis through Facebook: a qualitative thematic analysis. Nephrology. 2017;22:301–307. doi:10.1111/nep.12780
26. Ridout B, Campbell A. The use of social networking sites in mental health interventions for young people: systematic review. J Med Internet Res. 2018;20(12):e12244. doi:10.2196/12244
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.