")
Back to Journals » Cancer Management and Research » Volume 12
The Incidence Rate of Liver Cancer in Saudi Arabia: An Observational Descriptive Epidemiological Analysis of Data from the Saudi Cancer Registry (2004–2014)
Authors Alghamdi IG , Alghamdi MS
Received 26 September 2019
Accepted for publication 21 January 2020
Published 13 February 2020 Volume 2020:12 Pages 1101—1111
DOI https://doi.org/10.2147/CMAR.S232600
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lu-Zhe Sun
Ibrahim G Alghamdi,1 Mohamed S Alghamdi2
1University of Al-Baha, College of Applied Medical Sciences, Public Health Department, Al-Baha, Saudi Arabia; 2Ministry of Health, General Directorate of Health Affairs Al-Baha, Al-Baha, Saudi Arabia
Correspondence: Ibrahim G Alghamdi
University of Al-Baha, College of Applied Medical Sciences, Public Health Department, Prince Mohammad Bin Saud, Al-Baha 65527, Saudi Arabia
Tel +96 655 3777925
Email [email protected]
Objective: This study describes the epidemiological pattern of liver cancer in all regions of Saudi Arabia. It explores the frequency of cases diagnosed, the age-specific incidence rate (AIR), the crude incidence rate (CIR), and the age-standardised incidence rate (ASIR) stratified by age group, year of diagnosis, and region.
Methods: A retrospective descriptive epidemiological analysis of all liver cancer cases documented in the Saudi Cancer Registry (SCR) between 2004 and 2014 was performed. The data were analysed using descriptive statistics, t-test, Kruskal–Wallis, and sex ratio with the Statistical Package for the Social Sciences version 20.0 (SPSS).
Results: A total of 4723 liver cancer cases were registered in the SCR between January 2004 and December 2014. The highest overall ASIR of liver cancer among Saudi males was observed in the regions of Riyadh, Najran, and Tabuk at 10.4, 7.7, and 7.0 per 100,000 males, respectively. Furthermore, Riyadh, Eastern Region, and Tabuk recorded the highest overall ASIR among Saudi females at 4.9, 2.8, and 2.6 per 100,000 females, respectively. Jazan had the lowest overall ASIR (1.7 per 100,000 males) of liver cancer among male Saudis, while the Northern region and Baha had the lowest overall ASIR (0.6 and 0.9 per 100,000 females, respectively) of liver cancer among female Saudis. However, the overall ASIR of liver cancer was statistically higher in males than females (P-value < 0.05), and the overall male-to-female ratio in ASIR of liver cancer in Saudi Arabia was 2.4 per 100,000.
Conclusion: There was a slight increase in the CIRs and ASIRs of liver cancer in Saudi Arabia between 2004 and 2014. Riyadh, Najran, and Tabuk were the areas most affected by liver cancer among Saudi males, and Riyadh, Eastern Region, and Tabuk among female Saudis. The areas least affected by liver cancer were observed in Jazan among Saudi males, and the Northern region and Baha among Saudi females. The rates of liver cancer in Saudi Arabia were significantly higher among males compared with female Saudis.
Keywords: cancer epidemiology, liver cancer, Saudi cancer registry, hepatocarcinoma, incidence rate
Introduction
Liver cancer (LC) is considered the third most common malignancy in males, and the seventh in females, worldwide, accounting for more than 800,000 new cases per year.1–3 It is the leading cause of death in the United States (US) and worldwide, accounting for more than 700,000 deaths per year.3,4 In 2018, the two countries with the highest age-standardized incidence rates (ASIRs) of LC among both sexes were Mongolia and Egypt.5 However, LC consists of two types: primary and secondary LC. Primary LC originates in the liver, but secondary LC begins in other parts of the body such as cancers of the breasts, pancreas, colorectal area, ovary and lungs, and invades the liver due to metastases.6
The most common type of primary LC is Hepatocellular Carcinoma (HCC), which starts and develops in the main type of liver cells (hepatocyte).7,8 The well-known risk factors of HCC are chronic infection with hepatitis B virus (HBV), which considered the most important risk factor of HCC in many countries of Asia and Africa, or hepatitis C virus (HCV), which considered the strongest risk factor for HCC in Western countries. In addition, there are other risk factors that increase the chance of getting HCC, such as obesity or non-alcoholic fatty liver disease, diabetes, heavy alcohol use, tobacco smoking, and consumption of aflatoxins.7–9 Clinical presentation of HCC can vary from asymptomatic patients to other patients suffering from right upper quadrant pain, lethargy, jaundice, and weight loss.7
In the US, the American Cancer Society has estimated that 42,030 new patients (29,480 in males and 12,550 in females) are going to have LC diagnosed in 2019, while the number of liver cancer-related deaths is estimated at 31,780 persons (21,600 males and 10,180 females).3 In addition, the incidence rate of LC has more than tripled since 1980, and became three times higher in men than in women.3
In Saudi Arabia, the International Agency for Research on Cancer (IARC) estimated that the ASIR for LC was 4.5 per 100,000 population in 2018, and the age-standardised mortality rate (ASMR) was 4.2 per 100,000 population.10 Furthermore, in 2014, the Saudi Cancer Registry (SCR) reported that LC ranked sixth in cancer incidence among Saudi males, and ninth among Saudi females.11 The ASIR of LC in Saudi Arabia and Kuwait was slightly higher in comparison with other Arabian Gulf countries. For example, in 2018, the reported ASIR for Bahrain, Qatar, United Arab Emirates, and Oman, were lower than Saudi Arabia, at 3.4, 4.1, 4.2, and 4.4, respectively.10 The main objectives of this study were to investigate and describe the distribution of LC among the Saudi population by focusing on the CIR and ASIR stratified by year of diagnosis, region, and age group. Therefore, we intend to conduct an observational descriptive epidemiological study of the LC while considering the spatial/temporal distribution of registered cases in the SCR from 2004 to 2014.
Materials and Methods
A retrospective observational descriptive epidemiological study of all LC cases diagnosed in all regions of Saudi Arabia between January 2004 and December 2014 was performed. The data regarding LC incidence in Saudi Arabia are publicly available and easily accessible through the SCR reports; therefore, no ethical approval was required for this observational descriptive epidemiological study. In addition, the data for this study are a population-based cancer registry that was established in 1994 by the Ministry of Health in Saudi Arabia. However, the first cancer report in Saudi Arabia was published in 2001, and the best accurate Saudi cancer reports were issued in the beginning of 2004. Therefore, this study will concentrate its efforts on exploring the epidemiological pattern of LC in Saudi Arabia from 2004 to 2014. Furthermore, the most recent available dataset from the SCR was in 2014.
Since 2001, the SCR has been reporting on the pattern of cancer in Saudi Arabia with the main objective of defining the epidemiological distribution of the disease. Based on these data, there are currently comprehensive reports for 13 administrative regions from 2004 to 2014 that provide the frequency with percentage of cases, the CIR and the ASIR, stratified by the provinces of Saudi Arabia, gender of patients, and the years of diagnoses. This study was conducted using these reports to critically gather all of the information from the SCR with the aim of presenting the descriptive epidemiology of LC in Saudi Arabia.
For data analysis, we used the Statistical Package for the Social Sciences (SPSS) version 20.0 (IBM Corporation, Armonk, NY, USA). The descriptive analysis of the epidemiological data was performed by calculating the overall percentage, the age-specific incidence rate, the CIR, and the ASIR stratified by gender, region, and year of diagnosis. The differences in the CIR and ASIR between the year 2004 and the year 2014 were calculated from the reports published by SCR, to investigate the pattern of LC among male Saudis in different regions. The independent sample t-test was used to compare the CIR and ASIR of LC among male and female Saudis. Furthermore, Kruskal–Wallis was used to compare the CIR and ASIR of LC among regions of Saudi Arabia. However, liver cancer sex ratio was calculated from the age-specific incidence rate, the CIR, and the ASIR stratified by age group, region, and year of diagnosis.
The overall percentage of stage distribution of LC among male and female Saudis was calculated from 2004 to 2014. The staging system that is used for all types of cancer in the SCR was classified into four categories: localized, regional, distant, and unknown stage. Localized stage means that the cancer is limited to the place where it started and has not spread to other parts of the body. Regional stage implies that the cancer has invaded to nearby lymph nodes, tissues, or organs, while the distant stage indicates that the cancer has spread to distant parts of the body. However, unknown category means there is not enough information to identify the stage of cancer.12
Results
Liver Cancer Among Male Saudis
A total of 3298 LC cases were documented in the SCR between January 2004 and December 2014. The frequency of the number of LC cases increased slightly from 2004 to 2014. In Figure 1A, it is shown that there were 231 cases in 2004 (7.0%). This figure decreased to 211 by 2005, representing a decline of 0.6%, and this was the lowest percentage stated by the SCR (2005). From 2005 to 2012, the number of LC cases increased from 211 to 344, representing an increase of 4%, this was the highest percentage stated by the SCR (2012). However, the overall number and percentage of LC from 2004 to 2014 among Saudi males was 300 cases (9.1%) per year.
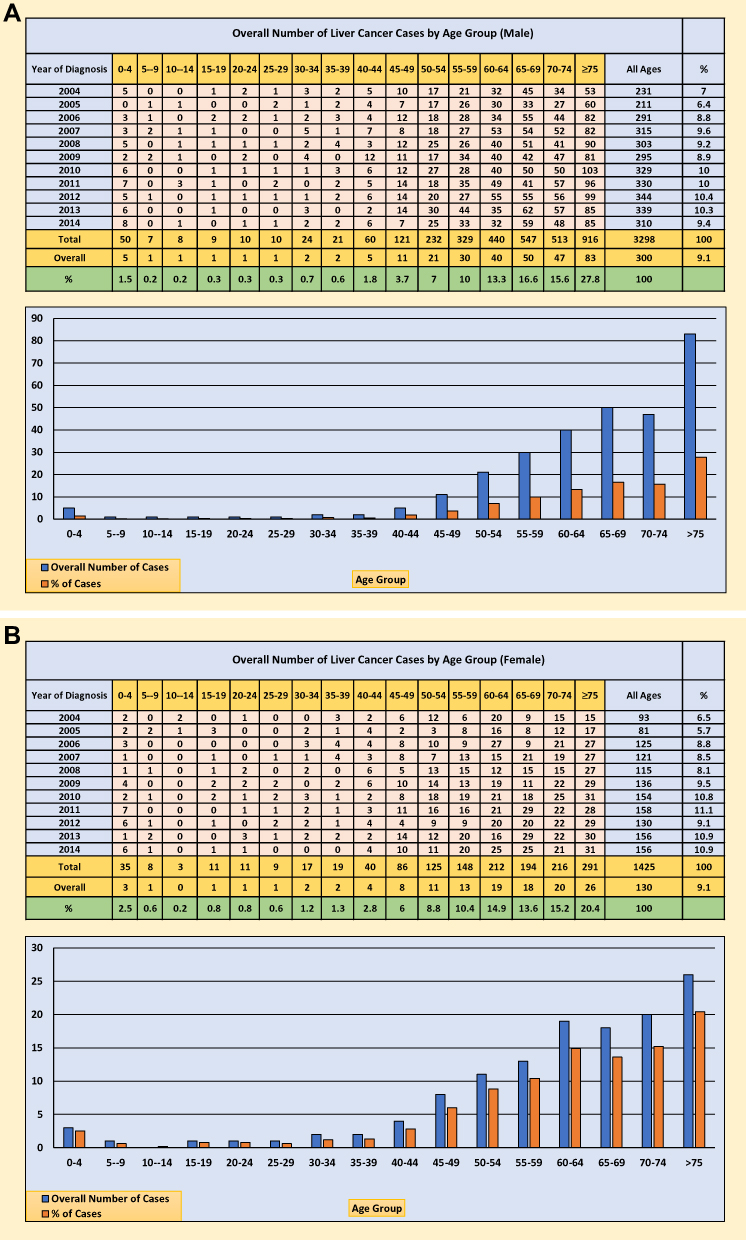 |
Figure 1 (A) Number and percentage of liver cancer cases among Saudi male between 2004 and 2014. (B) Number and percentage of liver cancer cases among Saudi female between 2004 and 2014. |
The average number and percentage of LC cases diagnosed between 2004 and 2014, stratified by age group of male Saudis, was calculated using the data from the SCR. The class width of the age groups was 5 years, starting from 0–4, 5–9, 10–14, 15–19, 20–24, and 75 years and over. From 2004 to 2014, Saudi men aged 75 years and over were most frequently diagnosed with LC, followed by those aged 65–69 years, representing 27.8% (83 overall cases per year) and 16.6% (50 overall cases per year) of the total number of LC cases, respectively. In contrast, the younger groups (aged 0–44 years) recorded the lowest overall number and percentage of LC cases (Figure 1A). In addition, the overall age-specific incidence rate of LC from 2004 to 2014 was high among Saudi males in the age groups 75 years and over, 70–74, 65–69, 60–64 at (70.4, 51.9, 44.4, and 24.6 per 100,000 males, respectively). However, the age-specific incidence male-to-female ratio of LC was higher among Saudi males aged from 45 to 75 years and over, while the age-specific incidence sex ratio was approximately similar for other age groups from 0 to 44 years (Figure 2).
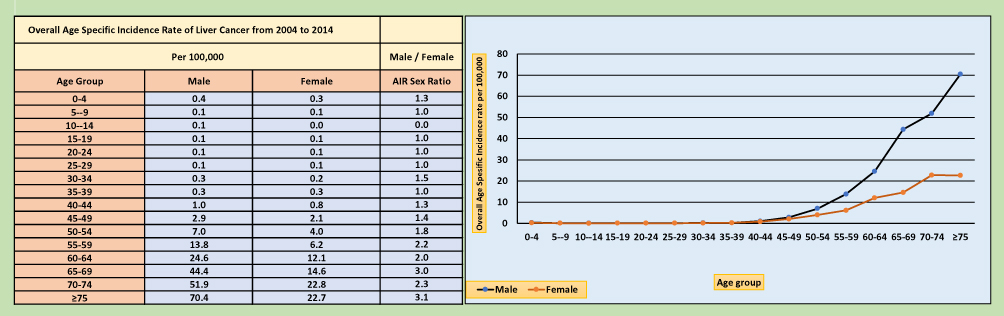 |
Figure 2 Overall age-specific incidence rate of liver cancer cases among Saudi male and female from 2004 to 2014. |
The CIRs of LC cases among males in Saudi Arabia, stratified by the year of diagnosis from 2004 to 2014 per 100,000 males, indicate a slight decrease from 2004 to 2005, and a slight increase from 2006 to 2007, then remain stable from 2008 to 2014. According to Figure 3, a CIR of 2.8 per 100,000 males was estimated in 2004. In 2007, the CIR of 3.6 per 100,000 males was the highest rate recorded by SCR. In addition, the overall CIR of LC among Saudi males from 2004 to 2014 per 100,000 males was 3.2 (95% CI, 3.0 to 3.4). The result of the two independent sample t-test indicated that the CIR of LC was significantly higher among Saudi males than females t(20) = 15.514, P < 0.001). However, the overall crude incidence male-to-female ratio from 2004 to 2014 per 100,000 males was 2.3. The overall CIR of LC stratified by the region of Saudi Arabia from 2004 to 2014 per 100,000 males was also calculated from the SCR, as shown in Figure 4. The regions of Riyadh and Najran in Saudi Arabia had the highest overall CIRs for LC among Saudi males, at 4.8 and 3.8 per 100,000 males, respectively, and the analysis of Kruskal–Wallis used for data not normally distributed was statistically significant for these regions compared with other parts of Saudi Arabia, χ2(12, N=143) =72.587, P < 0.001). In addition, the highest crude incidence male-to-female ratio per 100,000 males was documented in Najran at 4.8, and Baha at 4.4. The lowest overall CIR was observed in Jazan at 1.1, the Northern region at 1.2, and Jouf at 1.4 (Figure 4).
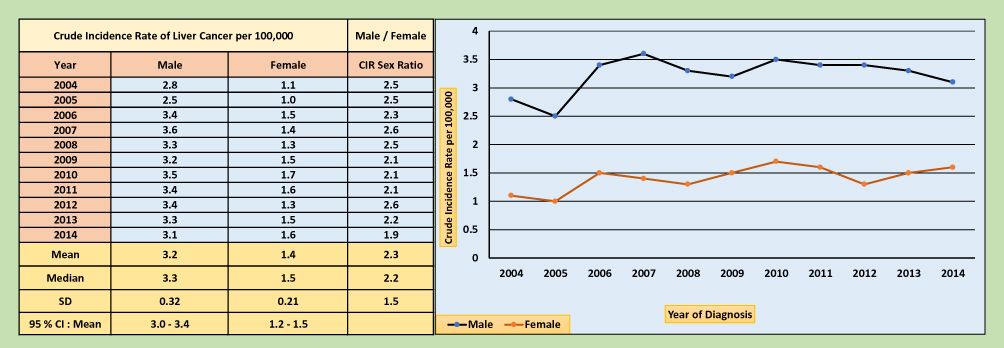 |
Figure 3 Crude incidence rate of liver cancer cases among Saudi male and female from 2001 to 2008. |
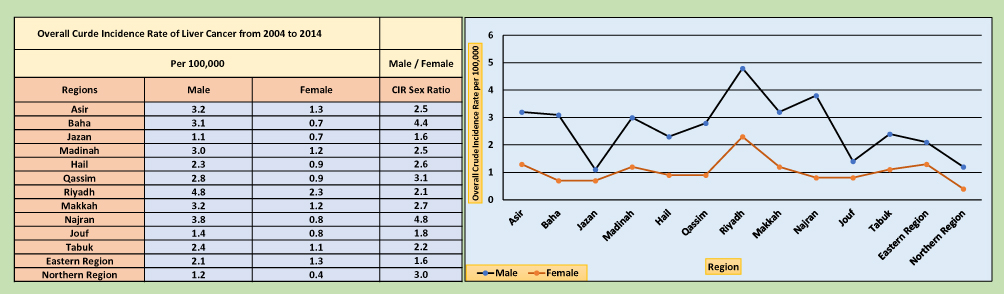 |
Figure 4 Overall crude incidence rate of liver cancer cases among Saudi male and female stratified by region of Saudi Arabia from 2004 to 2014. |
The ASIR of LC stratified by the year of diagnosis in Saudi Arabia, from 2004 to 2014 per 100,000 males, was calculated from the SCR (Figure 5). Similarly, there was a slight decrease from 2004 to 2005, and slight increase in 2006, then a steady decrease from 2007 to 2014. The highest ASIR of LC was recorded in 2006 at 7.5 per 100,000 males, with the lowest being in 2014 at 4.8 per 100,000 males. In addition, the overall ASIR of LC among Saudi males from 2004 to 2014 per 100,000 males was 6.0 (95% CI, 5.5 to 6.5). The results of the two independent sample t-tests indicated that the ASIR of LC was significantly higher among Saudi males than females t(20) = 13.169, P < 0.001). However, the overall age-standardised incidence male-to-female ratio from 2004 to 2014 per 100,000 males was 2.4. The overall ASIR of LC stratified by the region of Saudi Arabia from 2004 to 2014 per 100,000 males was also calculated from the SCR, as shown in Figure 6. The region of Riyadh in Saudi Arabia had the highest overall ASIR for LC at 10.4 per 100,000 males, followed by Najran at 7.7, and the analysis of Kruskal–Wallis was statistically significant for these regions compared with other parts of Saudi Arabia, χ2(12, N=143) =71.758, P < 0.001). In addition, the highest age-standardised incidence male-to-female ratio per 100,000 males was documented in Najran at 4.8, the Northern region at 5.0 and Baha at 4.6, respectively. Alternatively, the lowest overall ASIRs was documented in Jazan at 1.7, and the Northern region at 3.0 (Figure 6).
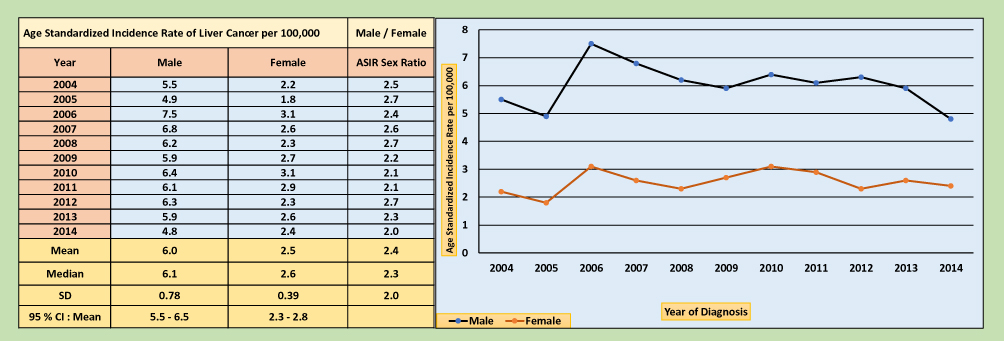 |
Figure 5 The age-standardised incidence rate of liver cancer cases among Saudi male and female during the year 2004 to 2014. |
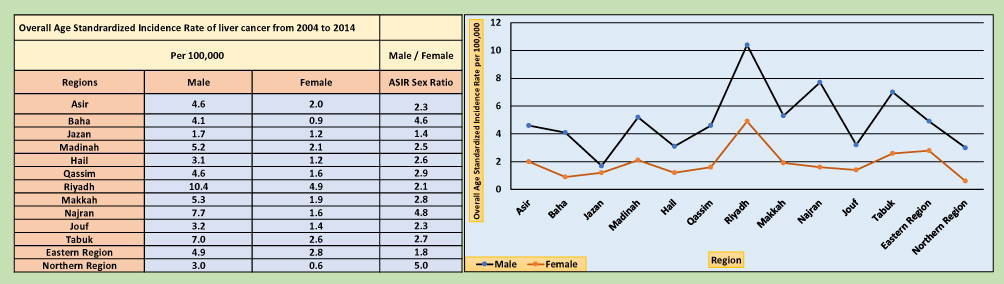 |
Figure 6 Overall age-standardised incidence rate of liver cancer cases among Saudi male and female stratified by region of Saudi Arabia from 2004 to 2014. |
The differences in the CIRs and ASIRs between 2004 and 2014 were calculated to examine the pattern of LC among Saudi males in the different regions of Saudi Arabia (Figure 7). The highest changes in rates were observed in the region of Najran among male Saudis (CIR, 3.6; ASIR, 6.7), and the lowest changes in the rates of LC among male Saudis were detected in the region of Tabuk (CIR, −1.6; ASIR, −6.3) and Hail (CIR, −2.5; ASIR, −4.5). However, these data indicate up-trending rates of LC among Saudi males living in Najran, and down-trending rates for Saudi males living in Tabuk and Hail.
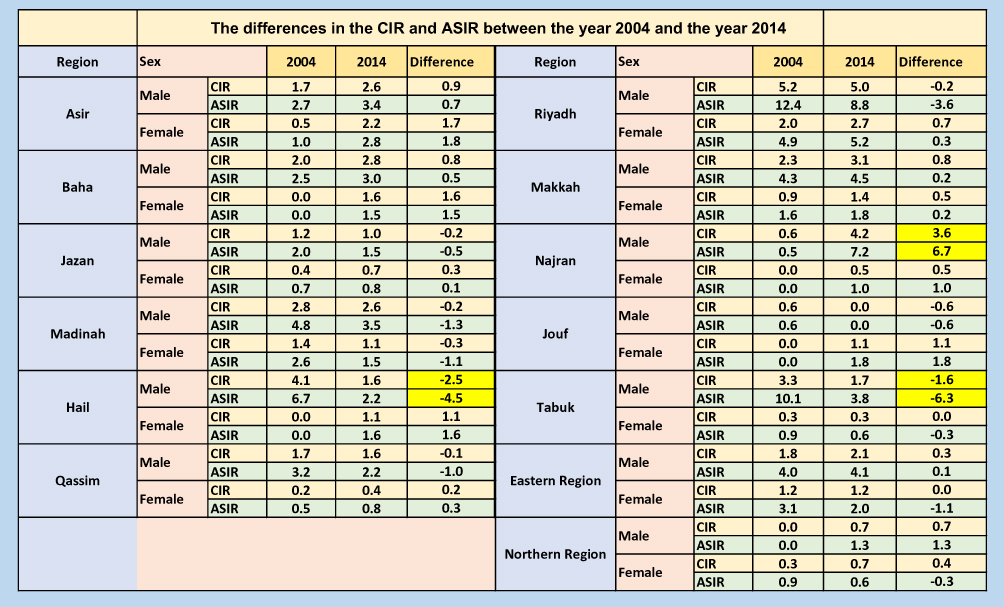 |
Figure 7 The differences in the CIR and ASIR between the year 2004 and the year 2014. |
The overall percentage of stage distribution of LC among male Saudis was calculated from 2004 to 2014. LC was diagnosed among Saudi men overall more often at the localized stage 31.4%, followed by distant and regional stages representing 18.4% and 12.1%, while unknown stage of LC was the highest percentage recorded by SCR from 2004 to 2014 at 37.8% (Figure 8A)
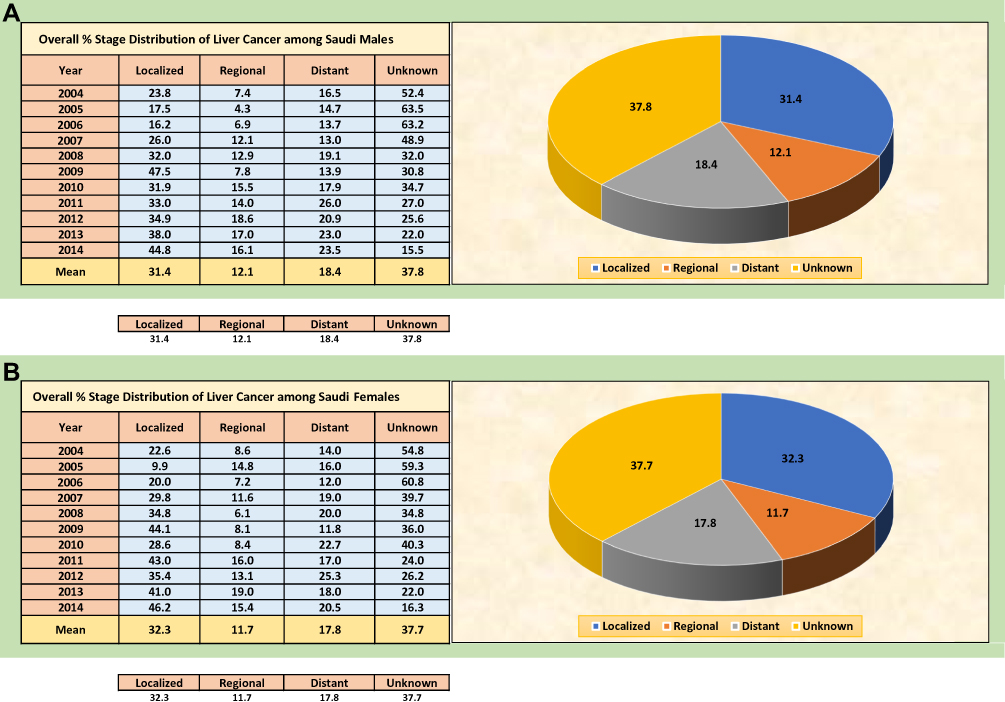 |
Figure 8 (A) Overall % stage distribution of liver cancer among Saudi males from 2004 to 2014. (B) Overall % stage distribution of liver cancer among Saudi females from 2004 to 2014. |
Liver Cancer Among Female Saudis
A total of 1425 LC cases were documented in the SCR between January 2004 and December 2014. The frequency of the number of LC cases increased slightly from 2004 to 2014. In Figure 1B, it is shown that there were 93 cases in 2004 (6.5%). This figure decreased to 81 by 2005, representing a decline of 0.8%, and this was the lowest percentage stated by the SCR (2005). From 2005 to 2011, the number of LC cases increased from 81 to 158, representing an increase of 5.4%, this was the highest percentage stated by the SCR (2011). However, the overall number and percentage of LC from 2004 to 2014 among Saudi females was 130 cases (9.1%) per year.
The average number and percentage of LC cases, stratified by age group of female Saudis, was obtained from the SCR. From 2004 to 2014, Saudi women aged 75 years and over were most frequently diagnosed with LC, followed by those aged 70–74 years, representing 20.4% (26 overall cases per year) and 15.2% (20 overall cases per year) of the total number of LC cases, respectively. In contrast, the younger groups (aged 0–44 years) recorded the lowest overall number and percentage of LC cases (Figure 1B). In addition, the overall age-specific incidence rate of LC from 2004 to 2014 was high among Saudi females in the age groups of 75 years and over, 70–74, 65–69, 60–64 at (22.8, 22.7, 14.6, and 12.1 per 100,000 females) (Figure 2).
The CIRs of LC cases among females in Saudi Arabia, stratified by the year of diagnosis from 2004 to 2014 per 100,000 females, indicate a steady decrease from 2004 to 2005, then remain stable from 2006 to 2014. According to Figure 3, a CIR of 1.1 per 100,000 females was estimated in 2004. In 2010, the CIR of 1.7 per 100,000 females was the highest rate recorded by SCR. In addition, the overall CIR of LC among Saudi females from 2004 to 2014 per 100,000 females was 1.4 (95% CI, 1.2 to 1.5). Furthermore, the overall CIR of LC stratified by the region of Saudi Arabia from 2004 to 2014 per 100,000 females was also calculated from the SCR, as shown in Figure 4. The region of Riyadh had the highest overall CIR for LC at 2.3 per 100,000 females, followed by the Eastern region and Asir at 1.3 per 100,000 females, and the result of Kruskal–Wallis was statistically significant for these regions compared with other parts of Saudi Arabia, χ2(12, N=143) =52.789, P < 0.001). The lowest overall CIR was observed in the Northern region at 0.4, and Jazan and Baha at 0.7 per 100,000 females, respectively (Figure 4).
The ASIRs of LC stratified by the year of diagnosis in Saudi Arabia, from 2004 to 2014 per 100,000 females, were obtained from the SCR (Figure 5). Similarly, there was a slight decrease from 2004 to 2005, and a slight increase in 2006, then they remained stable from 2007 to 2014. The highest ASIRs of LC were recorded in 2006 and 2010 at 3.1 per 100,000 females, while the lowest were in 2014 at 4.8 per 100,000 females. In addition, the overall ASIR of LC among Saudi females from 2004 to 2014 per 100,000 females was 2.5 (95% CI, 2.3 to 2.5). The overall ASIR of LC stratified by the region of Saudi Arabia from 2004 to 2014 per 100,000 females was also calculated from the SCR, as shown in Figure 6. The region of Riyadh in Saudi Arabia had the highest overall ASIR for LC at 4.9 per 100,000 females, followed by the Eastern region, and Tabuk at 2.8 and 2.6 per 100,000 females, respectively, and the Kruskal–Wallis test was statistically significant for these regions compared with other parts of Saudi Arabia, χ2(12, N=143) =65.242, P < 0.001). The lowest overall ASIRs were observed in the Northern region and Baha at 0.6, and 0.9 per 100,000 females, respectively (Figure 6).
The overall percentage of stage distribution of LC among female Saudis was calculated from 2004 to 2014. LC was diagnosed among Saudi women overall more often at the localized stage 32.3%, followed by distant and regional stages representing 17.8% and 11.7%, while unknown stage of LC was the highest percentage recorded by SCR from 2004 to 2014 at 37.7% (Figure 8B).
Discussion
The CIRs and ASIRs of LC cases among the Saudi population are essential to be monitored and updated for all regions in Saudi Arabia. In this study, we intended to investigate the pattern of the CIR and ASIR of LC in Saudi Arabia during the years from 2004 to 2014. Notably, this study is considered to be the first descriptive epidemiological study on the spatial/temporal distribution of LC among men and women in different regions of Saudi Arabia, based on the PubMed database. It investigates the real situation of the LC trend and explores the significance of the disease in the entire population of Saudi Arabia.
In this study, we have observed that the highest overall ASIRs for LC among male Saudis, from 2004 to 2014, were documented in the regions of Riyadh, Najran and Tabuk. The most likely reasons for these rising ASIRs are that most male Saudis in Riyadh, Najran, and Tabuk were highly exposed to the risk factors of LC compared with other Saudi males in different regions. Furthermore, the impact of environmental life factors, lifestyle habits, and genetic risk factors may be associated with the increase of ASIRs of LC among male Saudis in Riyadh and Najran.
According to the risk factors of LC, it was seen that almost 50% of HCC cases worldwide are associated with HBV infections and 25% are related to HCV infections.13 The risk that a person will develop HCC is 100-fold higher for patients infected with HBV than for those who are not infected.14 A systematic review and meta-analysis for 36 published studies in Saudi Arabia from 1965 to 2013 found a 3.2% prevalence of HBV, which was slightly lower than the worldwide prevalence of 3.6%.15
In Saudi Arabia, obesity and instances of being overweight are increasing with an overall rate of 35.5%.16,17 The region of Riyadh is considered one of the most highly affected areas with obesity in Saudi Arabia, with a 35% prevalence of obesity.18 Therefore, the rate of LC was significantly higher in Riyadh than in other parts of Saudi Arabia. In contrast, the areas least affected by LC were observed in the region of Jazan, which recorded the lowest rate of obesity in Saudi Arabia at 2%.18
The most epidemiological studies have suggested that diabetes mellitus is a risk factor for HCC. The incidence of HCC is approximately three times higher in diabetic patients than in those who do not have diabetes mellitus. Furthermore, the increasing prevalence of diabetes mellitus may contribute to the increase of HCC.11 In 2013, the Saudi Ministry of Health conducted a large national survey to investigate chronic diseases, health behaviours, and risk factors among adults aged (at least 15 years old) in all regions of Saudi Arabia. They observed that the prevalence of diabetes mellitus in the region of Riyadh is 20 times higher than in Jazan. Therefore, our results indicate that the region of Riyadh in Saudi Arabia had the highest overall ASIR of LC among Saudi males and females, and the region of Jazan had the lowest overall ASIR of LC among Saudi males and females, which means that presence of diabetes may contribute to the increase of ASIR of LC in the region of Riyadh, and contribute to the decrease of LC in the region of Jazan.18 However, it is very difficult to give a good explanation for the increase of ASIR of LC in the regions of Riyadh and Najran without conducting analytic epidemiological studies that help to investigate the real association between exposures and outcome. Therefore, a case-control study should be conducted to identify the most important risk factors of LC among Saudi males living in the regions of Riyadh and Najran. Researchers in the field of cancer epidemiology may observe the association between risk factors in Riyadh and Najran that contribute to the increase in the incidence of LC in Saudi Arabia.
Our results indicate that Jazan and Northern region had the lowest overall ASIRs for LC among male Saudis, from 2004 to 2014. The most likely explanation for the decrease of ASIRs is that most male Saudis in Jazan and Northern region were highly exposed to specific protective factors of LC compared to other Saudi males living in Riyadh and Najran. Furthermore, cancer researchers may also investigate the relationship between the protective factors in Jazan and Northern region that play a big role in the decline in the incidence of LC in Saudi Arabia. However, it is also essential to conduct analytical epidemiological studies such as case-control studies to determine the relationship between the protective factors and LC cases among Saudi males living in Jazan and Northern region.
The most important changes in the CIR and ASIR of LC were analysed among Saudi males in different regions of Saudi Arabia, in the year 2001 and the year 2014. The highest changes in rates were observed in the region of Najran among Saudi males, which means that the LC cases diagnosed increased the CIR by 3.6 cases per 100,000 males, and the ASIR increased by 6.7 cases per 100,000 males. However, these data indicate an up-trending rate in these regions and the likely explanation for the differences in CIR and ASIR suggests that male Saudis living in Najran were affected more by LC over an 11-year period (2004–2014). In addition, our findings indicate that the lowest changes in the CIR and ASIR of LC were observed in the region of Tabuk and Hail among Saudi males. It means that the LC cases diagnosed in Tabuk and Hail decreased the CIR by 1.6 and 2.5 cases per 100,000 males, and the ASIR decreasing by 6.3 and 4.5 cases per 100,000 males. However, these data indicate a down-trending rate and show that male Saudis living in Tabuk and Hail were less affected by LC over an 11-year period (2004–2014).
In 2018, the International Agency for Research on Cancer (IARC) estimated that the ASIR for LC in Saudi Arabia among both sexes of all ages was 4.5 per 100,000 individuals, which is considered slightly low in comparison with other countries, including the Arabian Gulf countries.7 Egypt had the highest ASIR of LC among both sexes of all ages at 49 per 100,000 individuals; this figure was 11-fold greater than Saudi Arabia’s (Figure 9A). In addition, the most recent age-standardised mortality rate (ASMR) of LC among both sexes, all ages were reported in Saudi Arabia at 4.2 per 100,000 individuals.7 This rate was relatively low compared to those of other countries, including Arabian Gulf countries. Furthermore, Egypt had the highest ASMR of LC among both sexes of all ages at 31.8 per 100,000 individuals; this figure was 7.5-fold greater than Saudi Arabia’s. However, Iraq had the lowest ASIR and ASMR of LC among both sexes of all ages at 2.7 per 100,000 individuals (Figure 9B).7 The pattern and trend of LC among male and female Saudis should not be neglected because of the low ASIRs and ASMRs.
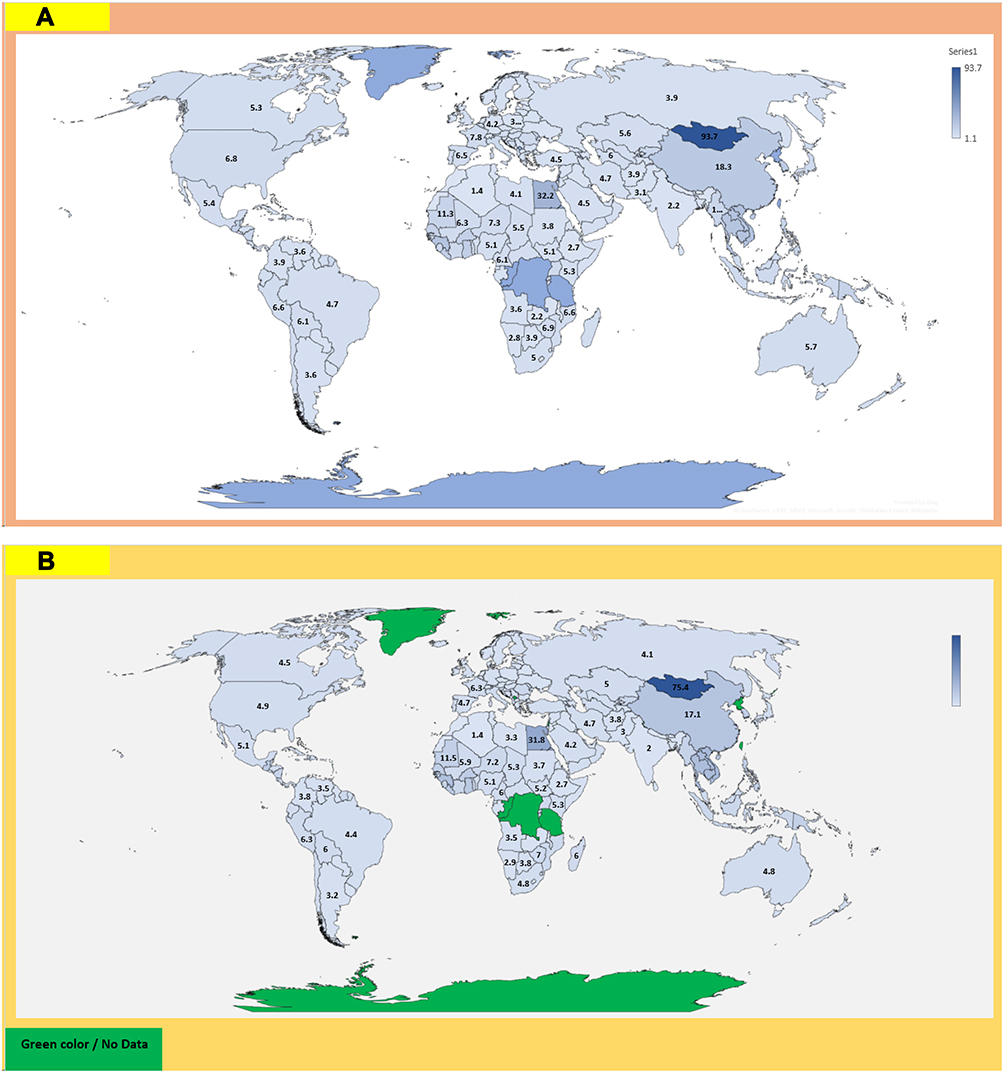 |
Figure 9 (A) Age-standardised incidence rate of liver cancer (World) in 2018, both sexes, all ages. (B) Age-standardised mortality rate of liver cancer (World) in 2018, both sexes, all ages. |
The strengths of descriptive epidemiological studies are generally their speed, inexpensiveness and ease of conducting. Furthermore, they allow the researcher to study the independent variables without considering any specific cause or hypotheses. These studies often do not need ethical approval, except if the information required is of a confidential nature. Furthermore, descriptive studies help generate a new hypothesis regarding the cause of disease, which can be tested using more complex study design. However, these studies are born with some limitations, which include there being no comparison group and that the statistical association between variables cannot be tested.19 In this study, the overall mortality rates of LC in different regions of Saudi Arabia were not calculated, because the reports of SCR had no data related to the number of deaths from LC. Despite the unavailable data related to the geographic distribution of LC among male and female Saudis, except for the SCR reports, we intended to clarify the real patterns of LC in different regions during the years from 2004 to 2014. Therefore, the findings of our study are very significant to the researchers and decision makers in Saudi Arabia.
Conclusion
This study revealed a slight increase of the CIR and ASIR of LC among the Saudi population. Riyadh and Najran had the highest overall ASIRs of LC among males, and Riyadh, Eastern region, and Asir among Saudi females, while the Northern region, Baha, and Jazan recorded the lowest rates among male and female Saudis. The overall age-standardised incidence male-to-female ratio from 2004 to 2014 per 100,000 males was approximately more than double that of the female Saudi population. Further analytical studies are needed to identify the potential risk factors for LC among the Saudi population.
Ethical Statement
The authors declare that the paper does not raise any ethical concern. The data regarding liver cancer incidence in Saudi Arabia are publicly available and easily accessible through the Saudi Cancer reports; therefore, no ethical approval was required for this observational descriptive epidemiological study.
Acknowledgment
I would like to thank Deanship of Scientific Research in University of Al-Baha for its financial support of this research.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Fitzmaurice C, Dicker D, Pain A, et al. Global burden of disease cancer collaboration. JAMA Oncol. 2015;1:505–527. doi:10.1001/jamaoncol.2015.0735
2. Pian L, Shao-Hua X, Shaobo H, et al. Age-specific sex difference in the incidence of hepatocellular carcinoma in the United States. Oncotarget. 2017;8(40):68131–68137. doi:10.18632/oncotarget.19245
3. Ali A, Zubair K, Abdurahman A, et al. Hepatocellular Carcinoma: Molecular Mechanisms and Targeted Therapies. Medicina (Kaunas). 2019;55(9):526.
4. Paulo S, Karen E, Patrica D, et al. Liver cancer: a leading cause of cancer death in the United States and the role of the 1945–1965 birth cohort by ethnicity. JHEP Rep. 2019. doi:10.1016/j.jhepr.2019.05.008
5. American institute for cancer research. Liver cancer statistics; 2018. Available from: https://www.wcrf.org/dietandcancer/cancer-trends/liver-cancer-statistics.
6. Shen Q, Fan J, Yang XR, et al. Serum DKK1 as a protein biomarker for the diagnosis of hepatocellular carcinoma: a large-scale, multicenter study. Lancet Oncol. 2012;13:817–826. doi:10.1016/S1470-2045(12)70233-4
7. Dimitrios D, Chistos D, Serena V, et al. From diagnosis to treatment of hepatocellular carcinoma: an epidemic problem for both developed and developing world. World J Gastroenterol. 2017;23(29):5282–5294.
8. Ayman AA, Mazen H, Abdulrahman A, et al. Saudi guidelines for the diagnosis and management of hepatocellular carcinoma: technical review and practice guidelines. Ann Saudi Med. 2012;32(2):174–199. doi:10.5144/0256-4947.2012.174
9. Dafina J, Viktorija CI, Vlado J. Hepatocellular carcinoma: risk factors, diagnosis and treatment. Open Access Maced J Med Sci. 2015;15(4):732–736.
10. GLOBOCAN (IARC). Section of cancer information; 2018. Available from: http://globocan.iarc.fr/.
11. Saudi Cancer Registry. Cancer Incidence Report in Saudi Arabia. Ministry of Health; 2014.
12. National Cancer Institute. Cancer staging; 2015. Available from: https://www.cancer.gov/about-cancer/diagnosis-staging/staging.
13. Gurtsevitch VE. Human oncogenic viruses: hepatitis B and hepatitis C viruses and their role in hepatocarcinogenesis. Biochem (Mosc). 2008;73(5):504–513. doi:10.1134/S0006297908050039
14. Alan D, Herbst BA, Reddy KR. Risk factors for hepatocellular carcinoma. Clin Liver Dis. 2012;1(6):180–183. doi:10.1002/cld.111
15. Abdulrahman AA, Mohamed B, Almoataz H, et al. Hepatitis B care pathway in Saudi Arabia: current situation, gaps and actions. Saudi J Gastroenterol. 2019;25(2):73–80. doi:10.4103/sjg.SJG_421_18
16. Al-Nozha MM, Al-Mazrou YY, Al-Maatouq MA, et al. Obesity in Saudi Arabia. Saudi Med J. 2005;26(5):824–829.
17. Saad MA. A review of prevalence of obesity in Saudi Arabia. J Prevalence Obes Saudi Arabia. 2016;2:2–25.
18. Saudi Ministry of Health. Saudi Health Interview Survey (SHIS); 2013. Available from: http://www.healthdata.org/ksa/projects/saudi-health-interview-survey.
19. Rakesh A, Priya R. Study designs: Part 2 – Descriptive studies. Perspect Clin Res. 2019; 10(1):34-36. doi: 10.4103/picr.PICR_154_18
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.