")
Back to Journals » Clinical Interventions in Aging » Volume 16
The Incidence, Characteristics, and Use of Suspected Nephrotoxic Drugs in Elderly Patients with Community-Acquired Acute Kidney Injury
Authors Hu W, Lian X, Lin J, Chen Y, Wu Y, Liu W, Yu F, Hao W
Received 16 October 2020
Accepted for publication 3 December 2020
Published 7 January 2021 Volume 2021:16 Pages 35—42
DOI https://doi.org/10.2147/CIA.S286660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Wenxue Hu,* Xingji Lian,* Jieshan Lin, Yuanhan Chen, Yanhua Wu, Wei Liu, Feng Yu, Wenke Hao
Department of Nephrology, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangdong Provincial Geriatrics Institute, Guangzhou 510080, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenke Hao
Department of Nephrology, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangdong Provincial Geriatrics Institute, 106th, Zhongshan Road II, Guangzhou 510080, People’s Republic of China
Tel + ± 8620-83827812-70811
Email [email protected]
Purpose: Acute kidney injury (AKI) is a major health problem with poor prognosis. However, little is known about elderly community-acquired-AKI (CA-AKI). This study aimed to investigate the incidence, clinical characteristics, outcomes and use of suspected nephrotoxic medications after CA-AKI in the elderly.
Materials and Methods: A total of 36,445 patients aged over 60 years were recruited from 2013 to 2016. Through an electronic database, we collected the demographic and medical history data, and admission lab results from all patients.
Results: A total of 2371 patients with CA-AKI were identified. The incidence of CA-AKI was 26.03% in the elderly. The proportion of CA-AKI patients with chronic comorbidities and Charlson comorbidity index score were higher than that of non-AKI patients. After CA-AKI, the proportions of exposure to non-steroidal anti-inflammatory drugs (NSAIDs), iodine contrast agent, angiotensin converting enzyme inhibitor (ACEI) or angiotensin II receptor blocker (ARB) were significantly decreased (p < 0.001). However, the proportion of other possible nephrotoxic drugs (including aminoglycosides, glycopeptide antibiotics, antifungal agents, beta lactam antibiotics, diuretic, ferralia, adrenergic receptor agonists and drugs for cardiac insufficiency therapy) still increased after CA-AKI (p < 0.001). Compared with non-AKI patients, CA-AKI patients had higher percentage of cardiogenic shock, multiple organ failure, transferring to intensive care unit, cardio-pulmonary resuscitation, hemodialysis, and mortality (p < 0.001). Moreover, CA-AKI patients had worse prognosis when more kinds of suspected nephrotoxic drugs were used (p < 0.001).
Conclusion: The incidence of CA-AKI in the elderly was high, with more complex chronic complications and poor clinical outcomes. The use of most suspected nephrotoxic drugs still increased and was associated with worse prognosis after CA-AKI.
Keywords: acute kidney injury, community-acquired acute kidney injury, elderly, prognosis, nephrotoxic drug
Introduction
Acute kidney injury (AKI) is a common clinical problem, particularly in the elderly.1 Studies showed that patients with AKI who were above 65-years-old were associated with higher mortality and morbidity.2 Older age is not only a risk factor for impaired recovery from AKI and progression to advanced stage chronic kidney disease (CKD), but also for death, and maintenance dialysis of patients with AKI.3
Community-acquired-AKI (CA-AKI) is identified when a patient had AKI that could be defined in community.4 Hospital-acquired-AKI has been researched for decades, while CA-AKI is relatively less studied, especially in elderly patients. A study in China showed that the mean age of patients with CA-AKI was 61.2 years and use of nephrotoxic drugs was one of the main causative factors of CA-AKI, accounting for 59.9%.5 By far, effective strategies for the improvement of clinical outcomes in patients with AKI have not been well built. Previous studies show that patients with AKI require avoiding exposure to nephrotoxic drugs and adjusting drug dosing due to buildup from decreased excretion and metabolism by the kidneys.6,7 However, the use of drugs and drug dosing were often inadequately estimated by clinicians.
Therefore, investigating clinical characteristics and use of nephrotoxic drugs after CA-AKI in the elderly is necessary for formulating drug management, and age-specific preventive and therapeutic strategies. In this study, we conducted a further analysis of 2371 older patients with CA-AKI, exploring the incidence, clinical characteristics, suspected nephrotoxic medications use after CA-AKI, and clinical outcomes.
Materials and Methods
Definition of Disease
AKI was defined by 2012 KDIGO AKI guidelines: an increase in serum creatine (Scr) level by 0.3 mg/dL within 48 hours or by 50% within 7 days (not including urine output criteria).
CA-AKI was defined by AKI apparent on their first Scr measured within 48 hours of admission to hospital. Baseline Scr values for patients with CA-AKI were determined through the review of all Scr values taken from the patient (from the hospital or the community) during the preceding 12 months. Moreover, patients with unknown baseline values had Scr values charted after AKI resolution, which further enabled approximation of baseline Scr and confirmation of true AKI.
The estimated glomerular filtration rate (eGFR) was calculated using a Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.8
Comorbid condition was classified by Charlson co-morbidity index (CCI).9
Study Population and Data Source
Inclusion criteria: Patients >60 years old with a diagnosis of CA-AKI. Exclusion criteria was the following: (1) patients who had pre-existing chronic kidney disease (CKD) stage 5 and those who underwent nephrectomy or kidney transplantation; (2) those who had peak Scr values <0.6 mg/dL or Scr level changes that could not be attributed to AKI (such as amputations); (3) patients with hospitalization for more than 30 days; (4) patients with missing data.
Using electronic medical record databases in Guangdong Provincial People’s Hospital, we conducted a population-based retrospective cohort study. This study comprised elderly inpatients with CA-AKI who were aged over 60 years in Guangdong Provincial People’s Hospital, and these were patients in calendar years 2013–2016 with follow-up to December 31, 2016. Special populations and the elderly (aged ≥60 years) receive government-funded coverage of prescription medicines. The study was conducted in compliance with the Helsinki declaration and approved by the Ethical Committee of Guangdong Provincial People’s Hospital (GDREC2016327H; Guangdong, China). Requirements for written informed consent were waived because all personal data were deidentified before the analyses.
Statistical Analyses
Statistical analysis was carried out using SPSS software, version 19.0 (SPSS, Inc., Chicago, IL, USA). Categorical data were described as frequency and percentage and compared using a Pearson chi-squared test. Continuous variables were described using mean ± SD or median with interquartile range (IQR). A t-test and one-way ANOVA were used for analysis of normally distributed data. Data that were not normally distributed were analyzed using a Mann–Whitney U-test, Wilcoxon signed-rank test, and Kruskal–Wallis test. Variables that were significant in the univariate analysis or clinically important were included in the multivariable models. The adjusted odds ratio (OR) and 95% confidence interval (CI) were calculated. A p-value < 0.05 was considered to represent statistically significant differences.
Results
CA-AKI Incidence of the Elderly
During the 4 years of the study, a total of 36,445 patients aged over 60 years old were recruited, and they were all hospitalized in medical ward of Guangdong Provincial People’s Hospital. Of these, 7621 patients with AKI were identified, giving an overall AKI incidence of 20.91%. There were 2371 patients with CA-AKI and the overall incidence was 6.51% of all hospital admissions.
CA-AKI Characteristics of the Elderly
Mean age of patients with CA-AKI was 75 (67,81) years, and there was a male preponderance (62.84%). Preexisting CKD was observed in 8.6% (204 cases) of patients with CA-AKI. There were 143 patients (6.03%) involving the treatment of cardio-pulmonary resuscitation. The percentage of patients who transferred to intensive care unit (ICU) was 21.1% (501 cases). The percentage of patients who underwent dialysis was 10.4% (247 cases), and the in-hospital mortality rate was 9.70% (230 cases) The proportion of chronic comorbidities and Charlson comorbidity index score was higher in CA-AKI patients with than that of non-AKI patients (Table 1).
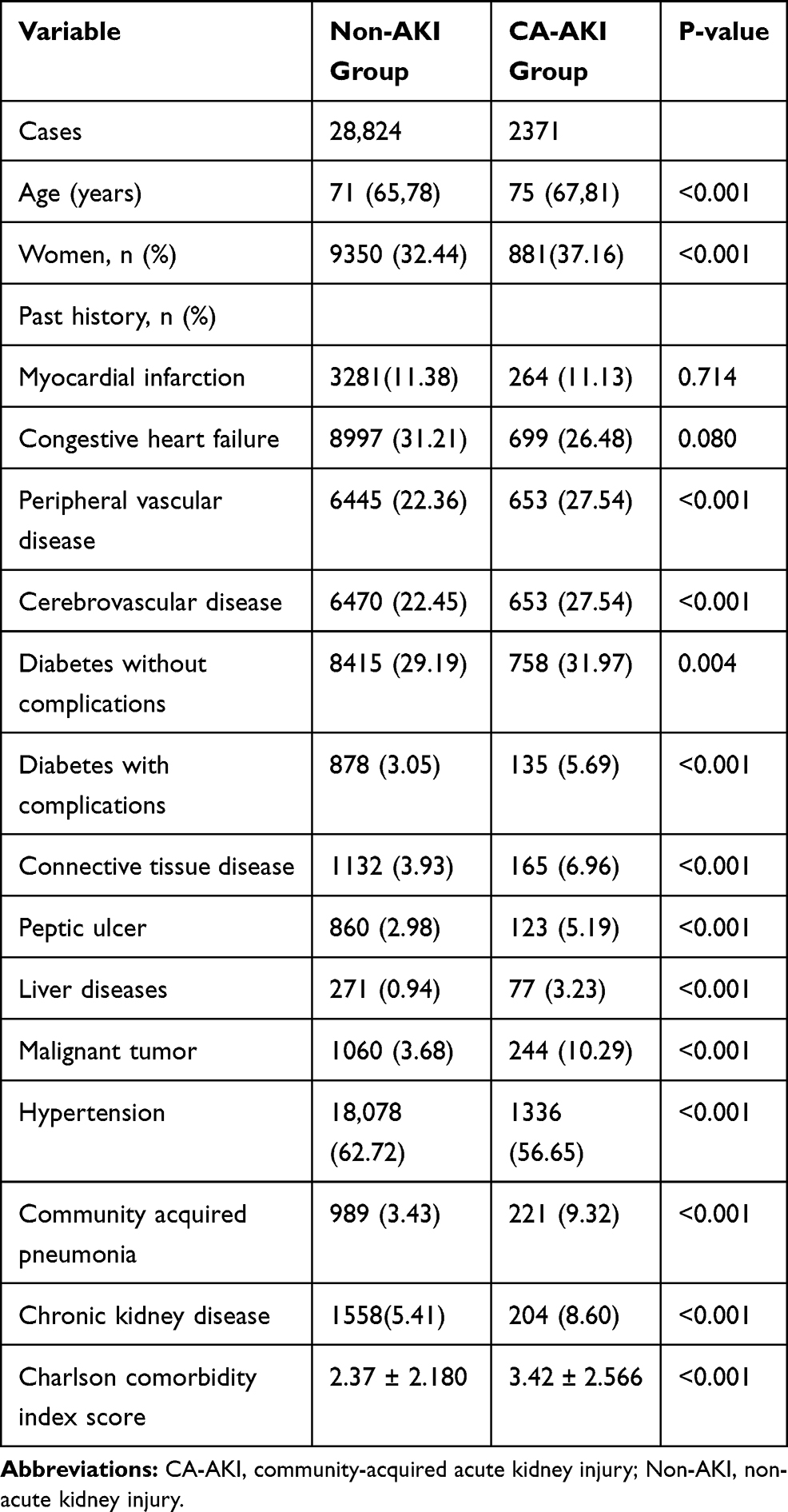 |
Table 1 The Baseline Characteristics of Elderly Patients with CA-AKI or Without AKI |
The Use of Suspected Nephrotoxic Drugs After CA-AKI in Elderly Patients
The prescription of suspected drugs induced nephrotoxicity after CA-AKI occurrence were analyzed (as shown in Table 2). The proportions of use for non-steroidal anti-inflammatory drugs (NSAIDs), iodine contrast agent and angiotensin converting enzyme inhibitor (ACEI) or angiotensin II receptor blocker (ARB) were significantly decreased in patients with CA-AKI when compared with non-AKI patients. However, the proportions of other possible nephrotoxic drugs in present study for concern (including glycopeptide antibiotics, aminoglycosides, antifungal agents, beta lactam antibiotics, diuretic, and dehydrating agents, ferralia, adrenergic receptor agonists and drugs for anti-heart failure) were still increased after CA-AKI occurred (p < 0.001). There was no difference of chemotherapeutic agents between 2 groups (p > 0.05). The number of types of suspected nephrotoxic drugs were also studied. Results showed use of one or two types of possible drugs for kidney injury decreased after CA-AKI occurred. But it was more popular in CA-AKI patients with three or more types of nephrotoxic medication (p < 0.001).
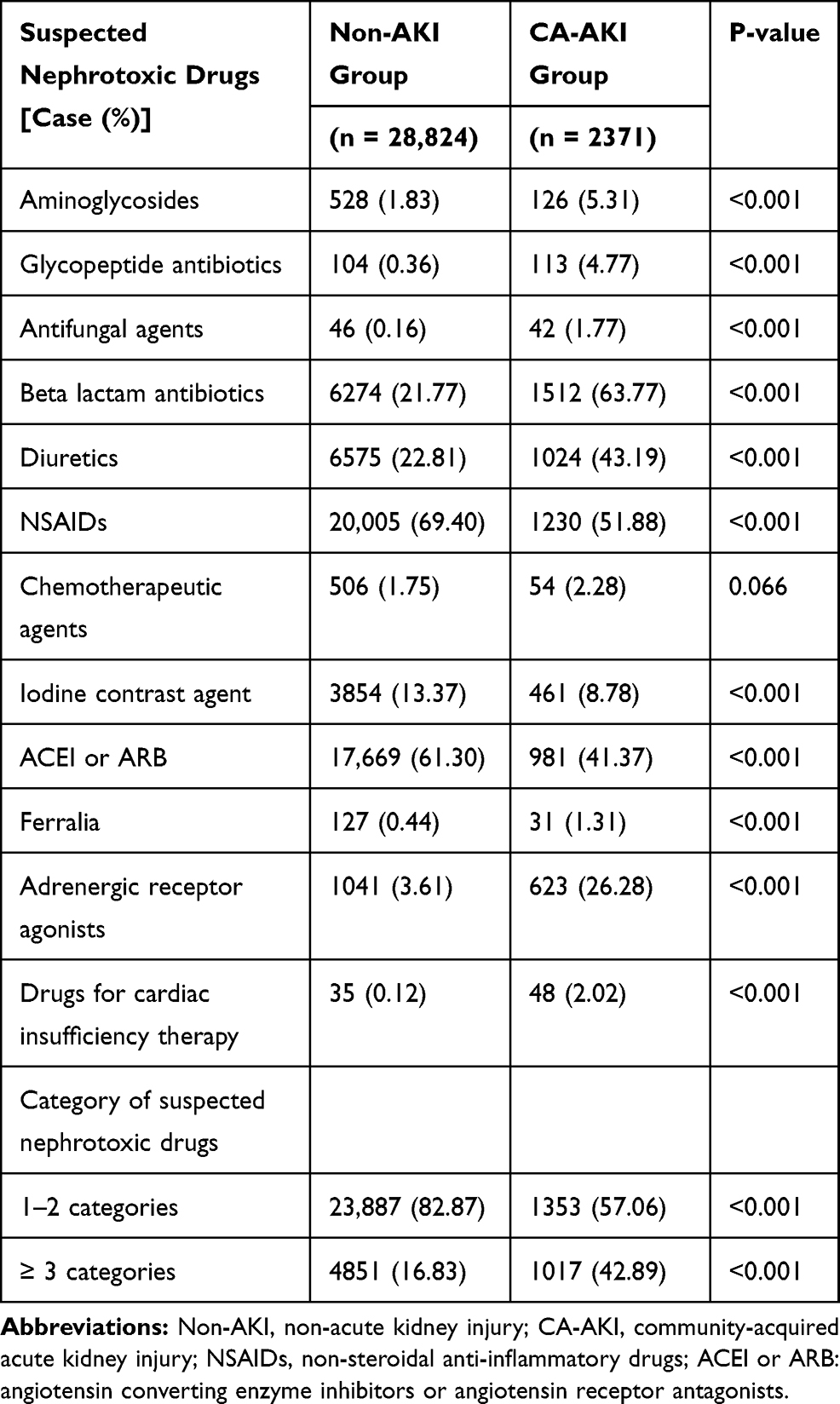 |
Table 2 Suspected Nephrotoxic Drugs Use in Post-CA-AKI or Non-AKI Elderly Patients |
Clinical Outcomes in Patients with CA-AKI
Clinical outcomes in patients with CA-AKI and non-AKI were shown in Table 3. Patients with CA-AKI had higher in-hospital all-cause mortality (9.71% versus 0.43% in non-AKI group; p < 0.001). Patients with CA-AKI also had longer length of hospital stay (14.46 ± 5.43 versus 8.30 ± 6.846, p < 0.001). Similarly, the cost of hospitalization was higher in patients with CA-AKI. Compared with non-AKI patients, the percentage of MODS (5.99% vs 0.04%) and cardiogenic shock (1.61% vs 0.05%) significantly increased in CA-AKI patients during hospitalization (p < 0.001). In addition, the proportion of patients with CA-AKI who needed to transfer to ICU (21.13% vs 4.27%), cardio-pulmonary resuscitation (6.03% vs 0.29%), dialysis (10.42% vs 0.01%) and intra-aortic balloon pump (IABP) (1.98% vs 0.27%) during hospitalization were higher than non-AKI patients (p < 0.001).
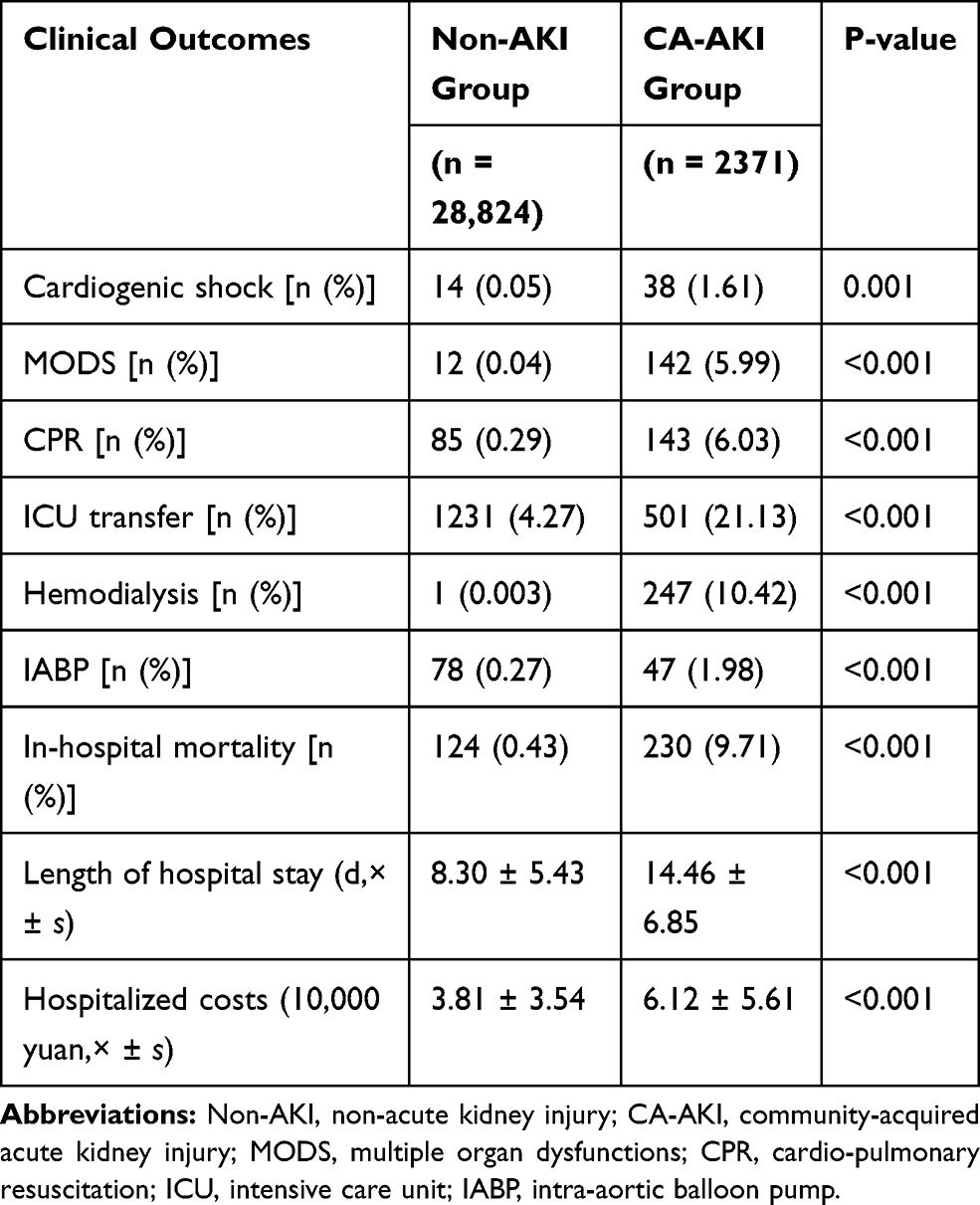 |
Table 3 Clinical Outcomes in Patients with CA-AKI or Without AKI |
The Association of Clinical Outcomes and Suspected Nephrotoxic Drug Use After CA-AKI
As shown in Table 4, there was a worse trend of clinical outcomes with exposure to a number of drugs with possible nephrotoxicity after CA-AKI occurred. CA-AKI patients had higher all-cause mortality, longer length of hospital stay and more hospitalization expenses with exposure to more kinds of suspected nephrotoxic drugs (p < 0.001). Moreover, the proportions of patients who needed to transfer to ICU, cardio-pulmonary resuscitation, or dialysis significantly increased when more kinds of suspected nephrotoxic drugs were used (p < 0.001). In addition, the hospitalization day and expenses, proportion of dialysis and transferring to ICU and all-cause in-hospital mortality was highest for those who use ≥3 drugs (p < 0.05).
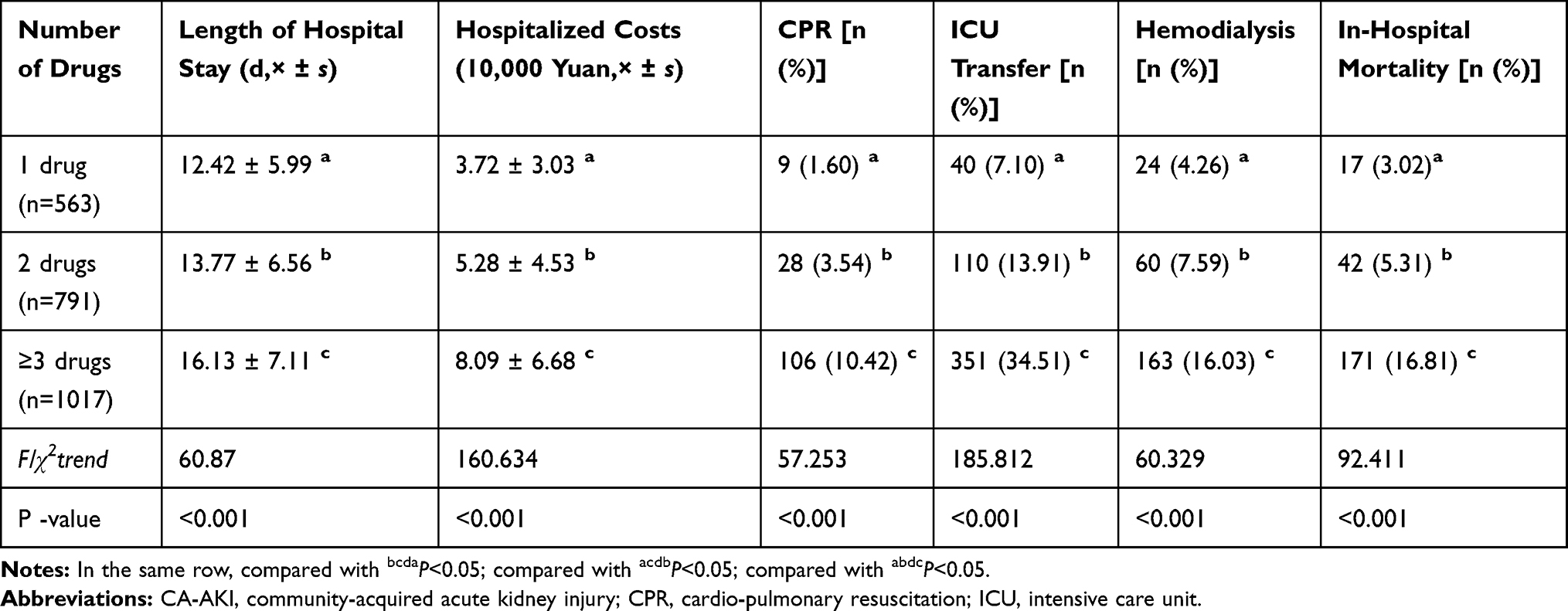 |
Table 4 The Association of the Number of Suspected Nephrotoxic Drugs Use and Clinical Outcomes After CA-AKI in Elderly Patients |
After adjusting for other potential risk factors (gender, age, MODS, shock, myocardial infarction, community acquired pneumonia, liver disease and cancer), exposure to nephrotoxic drugs after CA-AKI remained an independent risk factors for in-hospital mortality (adjust OR=1.60, 95% CI, 1.50–1.72, P<0.001), and the use of more ≥3 drugs showed stronger association (adjust OR=3.31, 95% CI, 2.76–3.97, P<0.001) (Table 5).
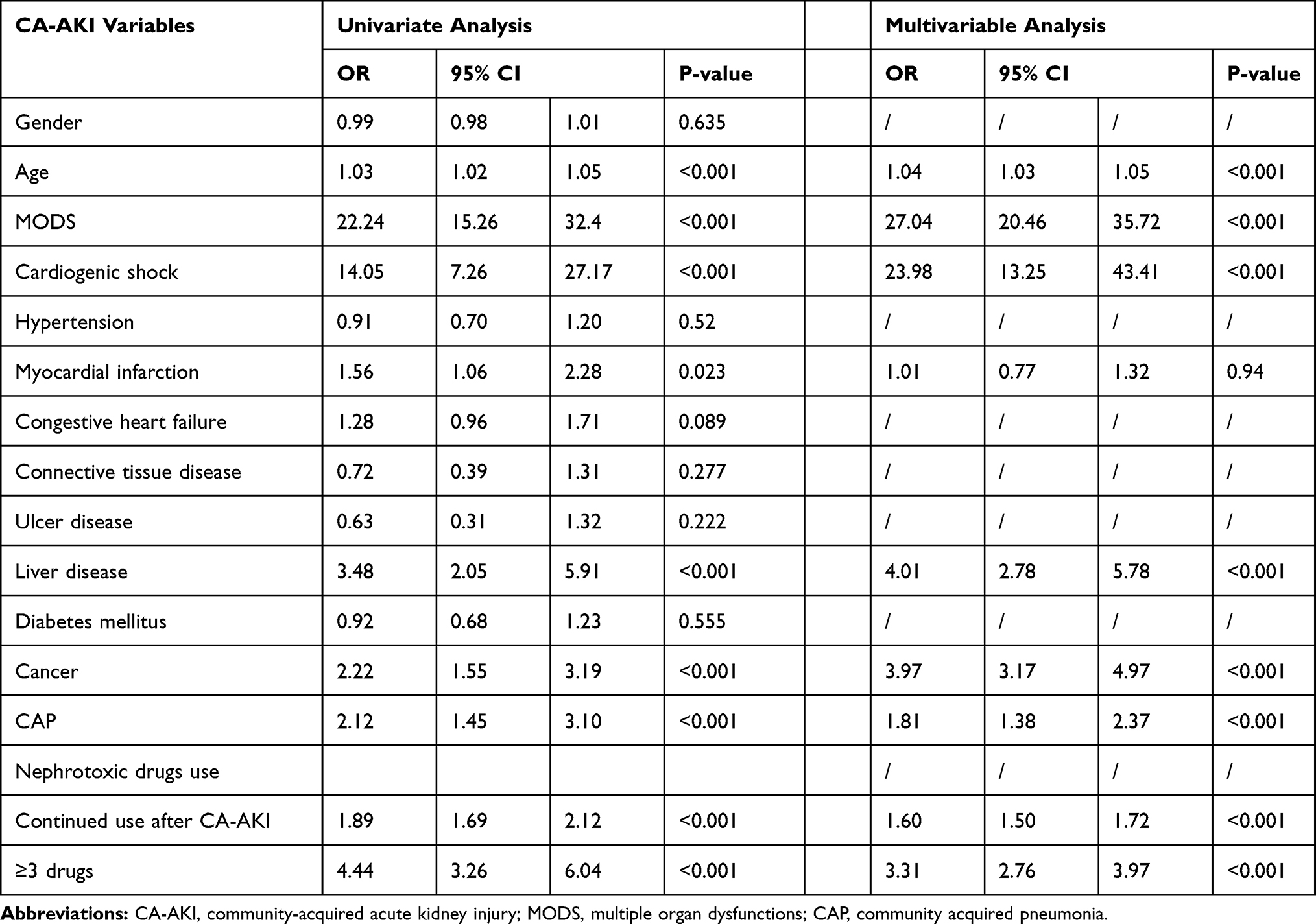 |
Table 5 Univariate and Multivariate Analysis of Risk Factors for in-Hospital Mortality |
Discussion
In the current study, we identified 2371 elderly patients with CA-AKI from 36,445 patients who were hospitalized in medical ward. The overall incidence of CA-AKI was 6.51%. We found that the proportion of use for NSAIDs, iodine contrast agent and ACEI or ARB were significantly decreased in patients with CA-AKI when compared with non-AKI patients. However, the proportion of other possible nephrotoxic drugs used in present study group were still increased after CA-AKI occurred. Moreover, patients with CA-AKI had higher all-cause mortality, longer length of hospital stay and other worsen clinical outcomes. In addition, a worse trend of clinical outcomes as long with the exposure to number of drugs with possible nephrotoxicity after CA-AKI.
Two previous studies showed that the incidences of CA-AKI of adults were 1.1% and 4.3%, respectively.4,10 Another study in Africa showed the incidence of AKI in hospitalized patients ranges from 0.3 to 1.9% in adults, and between 70 and 90% of cases of AKI are community acquired.11 In our study, incidence of CA-AKI in elderly patients was 6.51%. These data indicated that CA-AKI may be more prevalent in older patients. The following data in our study cloud provide the explanations for higher incidence of CA-AKI in elderly patients. Firstly, older adults have more chronic and comorbid illnesses. Pre-existing CKD, hypertension, diabetes, peripheral vascular diseases, cerebrovascular diseases, connective tissue diseases, peptic ulcer, liver diseases, malignant tumors and community acquired pneumonia were significantly higher in CA-AKI patients. The CCI scores were much higher in these patients when compared with the older patients without AKI. Secondly, the more chronic diseases and complications the older patients have, more chances to use medications and iodine contrast agent. Previous study in China showed that use of nephrotoxic drugs was one of main causative factors for CA-AKI, accounting for 59.9% of all AKI patients.4 These factors may be the reasons for high prevalence of CA-AKI in older patients.
Currently, treatments for established CA-AKI are limited and supportive care is required. Among the strategies for AKI, reducing exposure to nephrotoxic drugs may be critical in improving the clinical outcomes of the elderly patient.12,13 Therefore, we analyzed the prescription of suspected drugs induced nephrotoxicity after CA-AKI occurred. Our results showed that the proportion of use for NSAIDs, iodine contrast agent and ACEI or ARB were significantly decreased in patients with CA-AKI. Nash et al showed that use of NSAID was associated with a higher 30-day risk of AKI in the elderly and the incidence of NSAID-related AKI was 0.82%.14 Iodinated contrast, which has well-known renal toxicities, were often used to obtain accurate imaging of many diseases.15 The National Cardiovascular Data Registry Cath-PCI (985,737 patients who underwent elective and urgent percutaneous coronary intervention [PCI]) reported 69,658 (7.1%) cases of contrast-induced AKI (Scr rise ≥ 0.3 mg/dL) and 3005 (0.3%) cases of AKI requiring dialysis.16 ACEI and ARB are extensively use in the treatment of hypertension, cardiac failure, significant proteinuria, etc. However, patients who received an ACEI or ARB had a higher risk of AKI and the effect of them on glomerular perfusion (by reducing hyperfiltration) is the main mechanism.17,18 The three types of drugs mentioned above are common drugs inducing kidney injury and well-known by non-nephrologists, so they were decreased in patients with after CA-AKI occurred.
On the other hand, the results of the present study showed the proportion of other possible nephrotoxic drugs of concern that were still increased after CA-AKI occurred. These drugs were previously reported in literature, including beta lactam antibiotics, glycopeptide antibiotics, aminoglycosides, antifungal agents, diuretic ferralia, adrenergic receptor agonists and drugs for cardiac insufficiency therapy.19,20 There may be several explanations for increasing use of suspected nephrotoxic drugs for elderly patients. Firstly, elderly patients often have more comorbidities and infections are common and serious.21 Therefore, the use of antibiotics (lactam antibiotics, glycopeptide antibiotics, aminoglycosides, antifungal agents) is more prevalent in older patients.22–24 Secondly, studies have shown diuretics are one of the most common drugs inducing AKI and dose of exposure should be minimized in higher risk patients, like older patients.25 However, older patients often have problems in overloaded fluid and diuretics are needed to used, which may be the reason for increasing use of diuretic drugs in patients with CA-AKI. Thirdly, the incidence and prevalence of heart failure increase strikingly with age and make heart failure the most common reason for hospitalization among older adults.26 So that use of drugs for cardiac insufficiency therapy is very necessary and common in them. In a word, the drugs mentioned above are popular among old patients even if these patients with CA-AKI. Lastly, AKI is not considered by non-nephrologists and treatment strategies are not involved the impaired renal function. Therefore, clinician should pay high attention to avoid use of suspected nephrotoxic drugs, reduce doses, monitor renal function in older patients with CA-AKI.
Our study demonstrated that patients with CA-AKI had higher all-cause mortality, longer length of hospital stay and higher cost of hospitalization compared with non-AKI inpatients. This result was similar to another study, which had demonstrated that an episode of community acquired acute kidney injury markedly increases the risk of CKD, and moderately increases the risk of death in adults.27 The poor outcomes among older patients with CA-AKI may have been due in part to the physicians in charge being less likely to refer patients to nephrologists and economic reasons for patients to forgo RRT.
Moreover, Compared with non-AKI patients, CA-AKI patients were with higher incidence of MODS and cardiogenic shock during hospitalization. In addition, the proportion of these patients who needed to transfer to ICU, cardio-pulmonary resuscitation, dialysis, and intra-aortic balloon pump were significantly higher. These findings are novel and not described before. Therefore, our research provided more evidence for poor prognosis of CA-AKI patients. Clinicians should pay high attention to CA-AKI in the elderly and give preventive strategies to these patients. When CA-AKI occurs, more treatment measures should be taken. What’s more, our results also showed these patients had worse prognosis when more kinds of suspected nephrotoxic drugs were used, and the hospitalization days and expenses, proportion of dialysis and transferring to ICU and all-cause in-hospital mortality were highest for those who use ≥3 drugs. These findings call for heightened concern on early diagnosis and suspected nephrotoxic drugs are avoided using as much as possible after CA-AKI in the elderly.
In this study, we conducted a research on CA-AKI with large sample of elderly patients and some significant findings were discovered. However, our study also has following limitations. Firstly, this is a retrospective study and the causes of CA-AKI were not involved. Secondly, the subjects of this study were patients admitted in hospital, while outpatients with CA-AKI were not included. Therefore, our data only reflected the condition of these inpatients with more severe CA-AKI. Lastly, the follow-up duration was in hospital and no long follow up. Further prospective studies are needed with large patient groups and long follow up to establish more reliable conclusions.
Conclusion
CA-AKI in elderly patients is very common, with more complex chronic complications and poor clinical outcomes. Except for NSAIDs, iodine contrast agent, ACEI or ARB, most suspected nephrotoxic drugs use still increased and was associated with worse prognosis after CA-AKI. These results highlight the importance of early recognition of CA-AKI, avoiding use of suspected nephrotoxic drugs and taking renal protective strategies in elderly patients.
Abbreviations
AKI, acute kidney injury; CA-AKI, community-acquired-AKI; Scr, serum creatine; eGFR, estimated glomerular filtration rate; CKD-EPI, chronic kidney disease epidemiology collaboration equation; CCI, Charlson co-morbidity index; CKD, chronic kidney disease; IQR, interquartile range; NSAIDs, non-steroidal anti-inflammatory drugs; ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin II receptor blocker; IABP, intra-aortic balloon pump; MODS, multiple organ dysfunctions.
Data Sharing Statement
Restrictions apply to the availability of data generated or analyzed during this study to preserve participant confidentiality. The corresponding author will on request detail the restrictions and any conditions under which access to some data may be provided.
Ethics Approval and Informed Consent
The study was conducted in compliance with the Helsinki declaration and approved by the Ethical Committee of Guangdong Provincial People’s Hospital (GDREC2016327H; Guangdong, China). Requirements for written informed consent were waived because all personal data were deidentified before the analyses.
Acknowledgment
We acknowledge the role of all patients, investigators, and support staff in performing the study.
These authors are considered as co-first authors: Wenxue Hu and Xingji Lian.
Funding
This study was supported by grants from the Natural Science Foundation of Guangdong Province, China (NO. 2019A1515011594).
Disclosure
The authors report no conflicts of interest for this work.
References
1. Lewington AJ, Cerda J, Mehta RL. Raising awareness of acute kidney injury: a global perspective of a silent killer. Kidney Int. 2013;84(3):457–467. doi:10.1038/ki.2013.153
2. Lafrance JP, Miller DR. Acute kidney injury associates with increased long-term mortality. J Am Soc Nephrol. 2010;21(2):345–352. doi:10.1681/ASN.2009060636
3. Clark EG, Hiremath S, Sood MM, et al. WITHDRAWN: death and recovery of kidney function among patients continued on dialysis after discharge from hospital stays complicated by acute kidney injury: a cohort study. Am J Kidney Dis. 2019:. doi:10.1053/j.ajkd.2019.03.429.
4. Wang Y, Wang J, Su T, Qu Z, Zhao M, Yang L. Community-acquired acute kidney injury: a nationwide survey in China. Am J Kidney Dis. 2017;69(5):647–657. doi:10.1053/j.ajkd.2016.10.034
5. Hsu CY, McCulloch CE, Fan D, Ordonez JD, Chertow GM, Go AS. Community-based incidence of acute renal failure. Kidney Int. 2007;72(2):208–212. doi:10.1038/sj.ki.5002297
6. Cox ZL, McCoy AB, Matheny ME, et al. Adverse drug events during AKI and its recovery. Clin J Am Soc Nephrol. 2013;8(7):1070–1078. doi:10.2215/CJN.11921112
7. Matzke GR, Aronoff GR, Atkinson AJ
8. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
9. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
10. Wonnacott A, Meran S, Amphlett B, Talabani B, Phillips A. Epidemiology and outcomes in community-acquired versus hospital-acquired AKI. Clin J Am Soc Nephrol. 2014;9(6):1007–1014. doi:10.2215/CJN.07920713.
11. Adu D, Okyere P, Boima V, Matekole M, Osafo C. Community-acquired acute kidney injury in adults in Africa. Clin Nephrol. 2016;86:48–52. doi:10.5414/CNP86S121
12. Welch HK, Kellum JA, Kane-Gill SL. Drug-associated acute kidney injury identified in the united states food and drug administration adverse event reporting system database. Pharmacotherapy. 2018;38(8):785–793. doi:10.5414/CNP86S121
13. Levey AS, James MT. Acute kidney injury. Ann Intern Med. 2017;167(9):Itc66–itc80. doi:10.7326/AITC201711070
14. Nash DM, Markle-Reid M, Brimble KS, et al. Nonsteroidal anti-inflammatory drug use and risk of acute kidney injury and hyperkalemia in older adults: a population-based study. Nephrol Dial Transplant. 2019;34(7):1145–1154. doi:10.1093/ndt/gfz062
15. McCullough PA, Choi JP, Feghali GA, et al. Contrast-induced acute kidney injury. J Am Coll Cardiol. 2016;68(13):1465–1473. doi:10.1016/j.jacc.2016.05.099
16. Tsai TT, Patel UD, Chang TI, et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: insights from the NCDR Cath-PCI registry. JACC Cardiovasc Interv. 2014;7(1):1–9. doi:10.1016/j.jcin.2013.06.016
17. Palmer SC, Mavridis D, Navarese E, et al. Comparative efficacy and safety of blood pressure-lowering agents in adults with diabetes and kidney disease: a network meta-analysis. Lancet. 2015;385(9982):2047–2056. doi:10.1016/S0140-6736(14)62459-4
18. Brar S, Ye F, James MT, Hemmelgarn B, Klarenbach S, Pannu N. Association of angiotensin-converting enzyme inhibitor or angiotensin receptor blocker use with outcomes after acute kidney injury. JAMA Intern Med. 2018;178(12):1681–1690. doi:10.1001/jamainternmed.2018.4749
19. Khan S, Loi V, Rosner MH. Drug-induced kidney injury in the elderly. Drugs Aging. 2017;34(10):729–741. doi:10.1007/s40266-017-0484-4
20. Pierson-Marchandise M, Gras V, Moragny J, et al. The drugs that mostly frequently induce acute kidney injury: a case - noncase study of a pharmacovigilance database. Br J Clin Pharmacol. 2017;83(6):1341–1349. doi:10.1111/bcp.13216
21. High KP, Bradley SF, Gravenstein S, et al. Clinical practice guideline for the evaluation of fever and infection in older adult residents of long-term care facilities: 2008 update by the infectious diseases society of America. Clin Infect Dis. 2009;48(2):149–171. doi:10.1086/595683
22. Rutter WC, Burgess DR, Talbert JC, Burgess DS. Acute kidney injury in patients treated with vancomycin and piperacillin-tazobactam: A retrospective cohort analysis. J Hosp Med. 2017;12(2):77–82. doi:10.12788/jhm.2684
23. Ong LZ, Tambyah PA, Lum LH, et al. Aminoglycoside-associated acute kidney injury in elderly patients with and without shock. J Antimicrob Chemother. 2016;71(11):3250–3257. doi:10.1093/jac/dkw296
24. Ramos-Martinez A, Vicente-Lopez N, Sanchez-Romero I, et al. Epidemiology and prognosis of candidaemia in elderly patients. Mycoses. 2017;60(12):808–817. doi:10.1111/myc.12677
25. Vanmassenhove J, Kielstein J, Jorres A, Biesen WV. Management of patients at risk of acute kidney injury. Lancet. 2017;389(10084):2139–2151. doi:10.1016/S0140-6736(17)31329-6
26. Dharmarajan K, Rich MW. Epidemiology, pathophysiology, and prognosis of heart failure in older adults. Heart Fail Clin. 2017;13(3):417–426. doi:10.1016/j.hfc.2017.02.001
27. Soto K, Campos P, Pinto I, et al. The risk of chronic kidney disease and mortality are increased after community-acquired acute kidney injury. Kidney Int. 2016;90(5):1090–1099. doi:10.1016/j.kint.2016.07.018
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.