")
Back to Journals » Clinical Ophthalmology » Volume 15
The in vitro Evaluation of the Activity of COVID-19 Antiviral Drugs Against Adenovirus
Authors Romanowski EG , Yates KA, Romanowski JE, Shanks RMQ, Kowalski RP
Received 22 September 2021
Accepted for publication 3 December 2021
Published 22 December 2021 Volume 2021:15 Pages 4787—4793
DOI https://doi.org/10.2147/OPTH.S340576
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Eric G Romanowski, Kathleen A Yates, John E Romanowski, Robert MQ Shanks, Regis P Kowalski
The Charles T. Campbell Ophthalmic Microbiology Laboratory, UPMC Eye Center, Ophthalmology and Visual Sciences Research Center, Department of Ophthalmology, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA
Correspondence: Eric G Romanowski
The Eye & Ear Institute, Room 1020, 203 Lothrop Street, Pittsburgh, PA, 15213, USA
Tel +1 412-647-2245
Fax +1 412-647-5880
Email [email protected]
Purpose: Presently, there is no approved antiviral therapy for adenovirus (HAdV) ocular infections. During the COVID-19 pandemic, increased attention has been focused on antiviral treatments. Remdesivir, hydroxychloroquine, ivermectin, and umifenovir (Arbidol) have been touted as potential antiviral treatments for COVID-19. The goal of the current study was to determine whether these potential COVID-19 antivirals produce in vitro antiviral activity against a panel of ocular adenovirus types.
Methods: The 50% effective concentrations (EC50) of remdesivir (REM), hydroxychloroquine (HCQ), ivermectin (IVM), umifenovir (UMF) and cidofovir (CDV) (positive antiviral control) were determined for the human HAdV types HAdV3, HAdV4, HAdV5, HAdV7a, HAdV8, HAdV19/64 and HAdV37 using standard plaque-reduction assays in A549 cells.
Results: The range of mean in vitro EC50 concentrations for each antiviral across the range of HAdV types is as follows: The positive antiviral control, CDV, ranged from 0.47 to 9.62 μM; REM ranged from 0.21 to 11.27 μM; UMF ranged from 3.72 to 64.8 μM; IVR ranged from 2.60 to 201.3 μM; and HCQ was > 10 μM for all Ad types because of toxicity to the A549 cells. REM produced lower EC50 concentrations than CDV for 6 of 7 HAdV types. Potency increases with lower EC50 concentrations.
Conclusion: REM demonstrated anti-adenovirus activity in a range similar to that demonstrated by cidofovir. UMF and IVR demonstrated larger ranges of antiviral activity than CDV and REM across the panel of HAdV types. The anti-adenovirus activity of HCQ could not be determined due to cytotoxicity. Further investigation of REM, UMF, and IVR as antivirals for adenovirus is indicated.
Keywords: adenovirus, remdesivir, ivermectin, umifenovir, in vitro, antiviral
Introduction
Human adenovirus (HAdV) eye infections are manifested in three major forms, epidemic keratoconjunctivitis [EKC], follicular conjunctivitis, and pharyngeal conjunctival fever. These eye infections are the most seen viral eye infections around the world.1,2 Currently, no antiviral agents have received regulatory approval to treat these infections.3
During the COVID-19 pandemic, there has been a great deal of attention paid by the lay media and in the scientific literature to several possible antiviral agents for the treatment of SARS-CoV-2 infections. Remdesivir, hydroxychloroquine, ivermectin, and umifenovir (Arbidol) have been publicized as potential COVID-19 therapies.
Remdesivir (REM) (Figure 1A) is an antiviral agent that has demonstrated in vitro antiviral activity against several RNA viruses including SARS-CoV-2.4 It is a monophosphoramidate nucleoside prodrug that undergoes intracellular metabolic conversion to its active metabolite nucleoside triphosphate form.4 Remdesivir triphosphate subsequently interacts with the viral RNA polymerase resulting in chain termination during RNA synthesis.4 Its antiviral effect on DNA viruses is unknown.
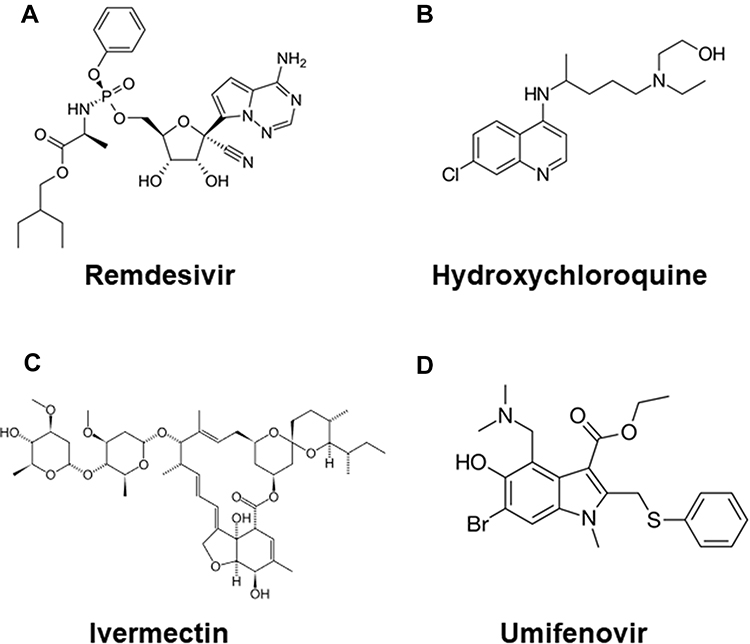 |
Figure 1 The chemical structures of the COVID-19 antivirals: (A) remdesivir; (B) hydroxychloroquine; (C) ivermectin; (D) umifenovir. Structures are courtesy of Wikipedia. |
Hydroxychloroquine (HCQ) (Figure 1B) is a synthetic antimalarial drug that was approved for use in 1955. It has been shown to have in vitro antiviral activity against SARS-CoV by an unknown mechanism of action.5
Ivermectin (IVM) (Figure 1C) was approved as a treatment for parasitic infections in animals in 1981, and subsequently to treat onchocerciasis (river blindness) in humans in 1987.6 Antiviral activity of IVR has been shown for the RNA viruses HIV-1, influenza, flaviviruses, and SARS-CoV-2, as well the DNA viruses pseudorabies, polyomavirus, and adenovirus.6 King et al demonstrated that IVR inhibits HAdV-5 early gene transcription, early and late protein expression and genome replication by disrupting the binding of the viral E1A protein to Imp-α without affecting the interaction between Imp-α and Imp-β1.7 This study also concluded that IVR also possesses antiviral activity against HAdV-3.7
Umifenovir (UMF; Arbidol) (Figure 1D) is an antiviral agent that has activity against both enveloped and non-enveloped viruses.8 UMF is used in Russia and China for the treatment of influenza but not in North America.8 UMF has been shown to prevent contact and penetration of viruses to host cells by inhibiting fusion of the virus to the cell membrane8 and it inhibits the release of SARS-CoV-2 from intracellular vesicles.8 UMF has demonstrated in vitro antiviral activity against HAdV7 when added after infection.9
With all the attention paid to these potential antivirals for SARS-CoV-2 and the fact that there were limited or no antiviral data for HAdV, we speculated whether these antivirals possessed antiviral activity against HAdV. This led us to the current study for which the goal was to determine whether remdesivir, hydroxychloroquine, ivermectin, and/or umifenovir possessed in vitro antiviral activity against a panel of common HAdV types that infect the eye and thus could be potential antivirals to treat HAdV eye infections. These agents are available as systemic medications and are not available as topical ocular formulations.
Materials and Methods
Experimental Drugs
Remdesivir was purchased from APExBIO, Houston, TX (Cat. No. B8398). Hydroxychloroquine sulfate was purchased from Sigma-Aldrich, St. Louis, MO (Cat. No. 90527). Ivermectin was also purchased from Sigma-Aldrich (Cat. No. PHR1380). Umifenovir hydrochloride was purchased from Biogems International, Inc., Westlake Village, CA (Cat. No. 131647). Powdered REM, IVR, and UMF were dissolved in DMSO to 20 mM and stored at −20°C prior to use. HCQ was dissolved in sterile water to 20 mM and was stored at −20°C until use. Cidofovir (CDV) was used as a positive control for antiviral in vitro activity against HAdV. A 20 mM stock solution CDV was prepared in saline from the 7.5% injectable form of cidofovir (Cidofovir Injection, Heritage Pharmaceuticals Inc., East Brunswick, NJ) and was stored at room temperature. All test drug concentrations were prepared in tissue culture media from their 20 mM stocks.
HAdV Isolates and Host Cells
HAdV isolates from a clinical repository of human HAdV types and species that were de-identified were used in this study. HAdV types HAdV3 (Species B), HAdV4 (Species E), HAdV5 (Species C), HAdV7a (Species B), HAdV8 (Species D), and HAdV19/64 (Species D) were isolated at the Charles T. Campbell Ophthalmic Microbiology Laboratory from patients presenting with HAdV eye disease. The isolate types were determined using serum neutralization. HAdV19/64 was found to be HAdV19 by serum neutralization. Recently, sequencing studies have determined that HAdV19 is actually HAdV64.10 For the purpose of this study, this isolate was designated HAdV19/64. No strains of HAdV37 (Species D) were isolated, therefore the ATCC (American Type Culture Collection, Manassas, VA) reference isolate of HAdV37 was used. A549 human lung carcinoma cells were purchased from ATCC and were used to prepare the virus stocks and for the in vitro Plaque Reduction Assays. It was determined that Institutional Review Board (IRB) approval was not necessary for this study.
In vitro Plaque Reduction Assay
These assays were done in 24-well multiplates containing A549 cell monolayers. One multiplate per virus isolate per antiviral was used. All wells of the 24-well multiplates were infected with approximately 100 PFU/well of the HAdV isolates. After 3 hours of adsorption, the virus inocula were removed from the wells. One mL of overlay media containing 0.001 µM, 0.01 µM, 0.1 µM, 1.0 µM, 10 µM, and 100 µM of antiviral was added to 3 wells each. To the remaining 6 wells, 1 mL of overlay media without antiviral was added. The plates were incubated at 37°C in 5% CO2 until plaque formation was visible in the negative control wells. At that time, the cells were fixed and stained with 0.5% gentian violet in formalin. The cells were dried and the number of plaques per well counted under a dissecting microscope. Two or three trials were performed for each antiviral. The Effective Concentration 50 (EC50; the concentration that inhibits plaque formation by 50%) for each virus isolate, antiviral, and trial was determined using the Fitted Line Plot regression analysis (Minitab, State College, PA). The mean ± standard deviation (SD) EC50 concentrations for each test drug and HAdV type were determined.
Results
The results from the Plaque Reduction Assays are displayed in Table 1 as the mean and standard deviations of the EC50 (µM) from duplicate or triplicate assays. The mean EC50 concentrations for the positive antiviral control, CDV ranged from 0.47 to 9.62 µM among the 7 HAdV types tested in our panel. Cidofovir was used as an experimental positive control as it has previously demonstrated antiviral activity against adenovirus in vitro11–13 and in vivo.12–19 In vitro antiviral activity that is similar to CDV provides an indication that the comparator antiviral could demonstrate anti-adenoviral activity in vivo.
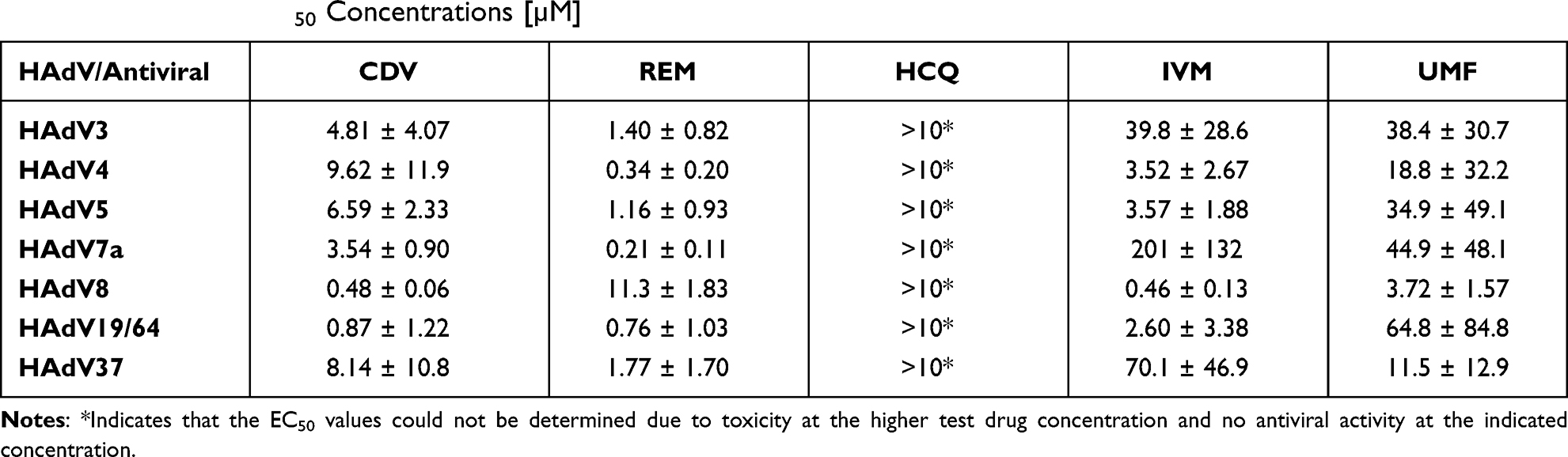 |
Table 1 Mean ± SD EC50 Concentrations [µM] |
Among the COVID-19 antivirals, REM demonstrated the lowest mean EC50 and tightest range of EC50 values from 0.21 to 11.27 µM across the panel of 7 HAdV types. This range of mean EC50 concentrations is similar to that produced by CDV. In fact, REM produced lower mean EC50 concentrations than CDV for 6 of 7 HAdV types. The mean EC50 concentrations for UMF ranged from a low concentration of 3.72 µM to a much higher EC50 than that of REM at 64.8 µM. IVR produced a lower concentration to the mean EC50 range than UMF at 2.60 µM, but its high mean concentration among the HAdV types was more than 3X greater than UMF and 17.8X greater than REM at 201.3 µM. We could not determine any EC50 concentrations for HCQ because of toxicity to the A549 cells demonstrated at the 100 µM concentration and plaque numbers at 10 µM were not less than 50% of the negative control for all HAdV types. Therefore, the EC50 for HCQ was considered as >10 µM for all 7 HAdV types tested.
Discussion
An antiviral treatment for adenoviral ocular infections would fulfill an unmet medical need in ophthalmology. Many antivirals have been evaluated for activity against adenovirus both in vitro and in vivo, but to date, none have received regulatory approval for use. Therefore, the search continues for a safe and effective topical treatment for these infections.
Recently, there has been a suggestion of using a repurposing approach for components of and/or the ophthalmic medications themselves as potential antiviral agents for treatments of viral infections with no available treatments.20 Among those agents suggested in that article, povidone-iodine,21–28 benzalkonium chloride (BAK),29–31 and polyhexamethylene biguanide (PHMB)32 have been formally evaluated against adenovirus in vitro or in patients. In fact, povidone-iodine has been evaluated in several formal clinical trials for the treatment of adenoviral conjunctivitis (ClinicalTrials.gov Identifier: NCT03055065, NCT01481519, NCT01179412, NCT03749317, NCT02998541, NCT02472223, NCT02998554, NCT04169919). The repurposing of agents used systemically to treat bacterial and viral infections is a strategy that has been long used in ophthalmology for the topical treatment of both bacterial and viral eye infections.
A great deal of media and political attention has been paid to possible antiviral therapies for COVID-19 infections. Older drugs such as hydroxychloroquine and ivermectin have been touted as possible treatments.5,6 A new drug, remdesivir, which was being developed for the treatment of emerging viral infections caused by Ebola, Marburg, SARS, and MERS has shown promise.4 A lesser-known drug outside of China and Russia, umifenovir (Arbidol) has also demonstrated efficacy in COVID-19 patients.8 Little, if any data exists regarding the antiviral activity of the above-mentioned antivirals against adenovirus. Therefore, we sought to determine whether these antivirals possessed antiviral activity against adenovirus using a traditional antiviral assay.
In this study, we used a panel of common ocular HAdV isolates to evaluate the antivirals. This panel represents HAdV species and types that are commonly associated with eye infections. Adenovirus types HAdV3, HAdV4, and HAdV7a are associated with pharyngeal conjunctival fever and follicular conjunctivitis, HAdV8, HAdV19/64, and HAdV37 cause EKC, and HAdV5 is associated with follicular conjunctivitis and is used in the Ad5/NZW rabbit ocular replication model to evaluate in vivo antiviral activity of topical antiviral treatments. It is important to show similar antiviral activity against the range of HAdV types and species since it has been shown previously that antivirals can have variable activity across HAdV types and species.33 Should all HAdV types show similar activity as HAdV5, it can be used as a surrogate for all HAdV types in the Ad5/NZW rabbit ocular replication model used to evaluate antivirals.
The results of the current study demonstrated that REM produced the lowest mean EC50 among the COVID-19 antivirals (0.21 µM for HAdV7a) and the narrowest range of mean EC50 concentrations (0.21–11.27 µM) across the panel of HAdV types. This range compares favorably to that produced by CDV, the positive antiviral control (0.47–9.62 µM). Among the HAdV types tested, REM produced mean EC50 concentrations lower than CDV for 6 of the 7 types tested. The only HAdV type for which REM produced a higher mean EC50 concentration than CDV was for HAdV8. REM produced its highest mean EC50 against HAdV8, whereas CDV produced its lowest against HAdV8. This could be an important finding since HAdV8 is the most commonly occurring HAdV type in the USA.34 The potential clinical relevance of this finding must be determined. Nevertheless, REM demonstrated broad-spectrum activity across the HAdV species and types tested, which is paramount when treating HAdV eye infections that can be caused by numerous HAdV types. Further, in vitro studies should be conducted with REM to determine whether the EC50 concentration produced for HAdV8 was isolate dependent. This is the first report of remdesivir demonstrating antiviral activity against a DNA virus and adenovirus in particular.
UMF demonstrated a range of mean EC50 concentrations of 3.72–64.8 µM. The range is larger than those produced by CDV and REM with the highest mean EC50 concentration being 6.74X greater than CDV and 5.73X greater than REM. UMF did not produce any mean EC50 concentrations that were lower than CDV and only 1 vs REM (HAdV8). Overall, there was antiviral activity demonstrated across the HAdV panel, but UMF does not appear to be as active as CDV and REM.
IVR produced the highest mean EC50 concentration demonstrated in our study against HAdv7a, which was 56.8X greater than that produced by CDV and 957X greater than that produced by REM. However, IVR demonstrated mean EC50 concentrations lower than CDV for 3/7 isolates, whereas only 1/7 EC50 concentrations were lower than REM (HAdV8). In contrast to the other test antivirals, EC50 concentrations could not be determined for HCQ due to cytotoxicity to the A549 cells and therefore does not appear to be a candidate for further investigation.
Overall, the COVID-19 touted antivirals remdesivir, umifenovir (Arbidol), and ivermectin demonstrated antiviral activity against a panel of ocular HAdV species and types. Remdesivir appears to be the most active of the three, followed by umifenovir and ivermectin. Remdesivir compared favorably to the positive antiviral control, cidofovir. While some of the antivirals demonstrated higher mean EC50 concentrations than others, and among the HAdV types, this does not preclude them from further investigation. Higher effective antiviral concentrations can be achieved in ocular tissue with topical dosing by high drug concentrations in the bottle, more frequent dosing, and/or vehicle manipulations. Our group has demonstrated the proof of concept that achieving high antibiotic corneal concentrations can overcome bacterial resistance to antibiotics with topical antibiotic dosing.35–38 Pharmacokinetic and pharmacodynamic studies are necessary to determine what safe and effective ocular tissue concentrations of the antivirals can be achieved after topical dosing.
In conclusion, remdesivir demonstrated in vitro anti-adenovirus activity in a range similar to that demonstrated by cidofovir, the positive antiviral control. Umifenovir and ivermectin also demonstrated anti-adenovirus activity across the range of HAdV types and species, but the antiviral activity for some HAdV types was less than what was demonstrated by cidofovir and remdesivir. The anti-adenovirus activity of hydroxychloroquine could not be accurately determined due to drug cytotoxicity.
To our knowledge, this is the first study to demonstrate that remdesivir possesses antiviral activity against adenovirus, a DNA virus, as well as a panel of adenovirus types that commonly infect the eyes. We have also demonstrated that both ivermectin and umifenovir possess antiviral activity against that same panel of ocular adenovirus types. Further investigation of remdesivir, umifenovir, and ivermectin as antivirals for adenovirus ocular infections is indicated.
Acknowledgments
The study was supported by The Charles T. Campbell Ophthalmic Microbiology Laboratory, Pittsburgh, PA; NIH CORE Grant for Vision Research EY08098; The Eye & Ear Foundation of Pittsburgh, Pittsburgh, PA; and an unrestricted grant to the University of Pittsburgh Department of Ophthalmology from Research to Prevent Blindness, New York, NY. The Charles T. Campbell Laboratory participated in the design of the study, the conduct of the study, data collection, data management, data analysis, interpretation of the data, preparation, review, and approval of the manuscript. This study was presented at the ARVO 2021 virtual conference as a poster presentation. The abstract was published in Investigative Ophthalmology & Visual Science 2021;62:411.
Disclosure
The authors report no financial interests or conflicts of interest in this work.
References
1. King D, Johnson B, Miller D, et al. Adenovirus-associated epidemic keratoconjunctivitis outbreaks—Four States 2008–2010. Morb Mortal Wkly Rep. 2013;62:637–641.
2. Garcia-Zalisnak D, Rapuano C, Sheppard JD, Davis AR. Adenovirus ocular infections: prevalence, pathology, pitfalls, and practical pointers. Eye Contact Lens. 2018;44:S1–S7. doi:10.1097/ICL.0000000000000226
3. Hoffman J. Adenovirus: ocular manifestations. Community Eye Health. 2020;33:73–75.
4. Malin JJ, Suárez I, Priesner V, Fätkenheuer G, Rybniker J. Remdesivir against COVID-19 and other viral diseases. Clin Microbiol Rev. 2021;34:e00162–20.
5. Keyaerts E, Vijgen L, Maes P, Neyts J, Van Ranst M. In vitro inhibition of severe acute respiratory syndrome coronavirus by chloroquine. Biochem Biophys Res Commun. 2001;323:264–268. doi:10.1016/j.bbrc.2004.08.085
6. Jans DA, Wagstaff KM. The broad spectrum host-directed agent ivermectin as an antiviral for SARS-CoV-2? Biochem Biophys Res Commun. 2021;538:163–172. doi:10.1016/j.bbrc.2020.10.042
7. King CR, Tessier TM, Dodge MJ, Weinberg JB, Mymryk JS. Inhibition of human adenovirus replication by the importin α/β1 nuclear import inhibitor ivermectin. J Virol. 2020;94:e00710–20. doi:10.1128/JVI.00710-20
8. Nojomi M, Yassin Z, Keyvani H, et al. Effect of Arbidol (Umifenovir) on COVID-19: a randomized controlled trial. BMC Infect Dis. 2020;20:954. doi:10.1186/s12879-020-05698-w
9. Shi L, Xiong H, He J, et al. Antiviral activity of arbidol against influenza A virus, respiratory syncytial virus, rhinovirus, coxsackie virus and adenovirus in vitro and in vivo. Arch Virol. 2007;152:1447–1455. doi:10.1007/s00705-007-0974-5
10. Zhou X, Robinson CM, Rajaiya J, et al. Analysis of human adenovirus type 19 associated with epidemic keratoconjunctivitis and its reclassification as adenovirus type 64. Invest Ophthalmol Vis Sci. 2012;53:2804–2811. doi:10.1167/iovs.12-9656
11. Gordon YJ, Romanowski EG, Araullo-Cruz T, et al. Inhibitory effect of (S)-HPMPC, (S)-HPMPA, and 2ʹ-nor-Cyclic GMP on different ocular adenoviral serotypes in vitro. Antiviral Res. 1991;16:11–16. doi:10.1016/0166-3542(91)90054-U
12. Romanowski EG, Yates KA, Gordon YJ. The in vitro and in vivo evaluation of ddC as a topical antiviral for ocular adenovirus infections. Invest Ophthalmol Vis Sci. 2009;50:5295–5299. doi:10.1167/iovs.08-3286
13. Romanowski EG, Hussein ITM, Cardinale SC, et al. Filociclovir is an active antiviral agent against ocular adenovirus isolates in vitro and in the Ad5/NZW rabbit ocular model. Pharmaceuticals. 2021;15:294. doi:10.3390/ph14040294
14. Gordon YJ, Romanowski EG, Araullo-Cruz T, De Clercq E. Pre-treatment with topical 0.1% S-HPMPC inhibits adenovirus type 5 replication in the NZ rabbit ocular model. Cornea. 1992;11:529–533. doi:10.1097/00003226-199211000-00008
15. Gordon YJ, Romanowski EG, Topical A-CT. HPMPC inhibits adenovirus type 5 in the New Zealand rabbit ocular replication model. Invest Ophthalmol Vis Sci. 1994;35:4135–4143.
16. Romanowski EG, Gordon YJ. Efficacy of topical cidofovir on multiple adenoviral serotypes in the New Zealand rabbit ocular model. Invest Ophthalmol Vis Sci. 2000;41:460–463.
17. Romanowski EG, Yates KA, Teuchner B, Nagl M, Irschick EU, Gordon YJ. N–Chlorotaurine is an effective antiviral agent against adenovirus in vitro and in the Ad5/NZW rabbit ocular model. Invest Ophthalmol Vis Sci. 2006;47:2021–2026.
18. Nwanegbo EC, Romanowski EG, Gordon YJ, Gambotto A. Efficacy of topical immunoglobulins (IG) against experimental adenoviral ocular infection. Invest Ophthalmol Vis Sci. 2007;48:4171–4176. doi:10.1167/iovs.07-0491
19. Romanowski EG, Yates KA, Paull JRA, Heery GP, Shanks RMQ. Topical astodrimer sodium, a non-toxic polyanionic dendrimer, demonstrates antiviral activity in an experimental ocular adenovirus infection model. Molecules. 2021;26:3419. doi:10.3390/molecules26113419
20. Napoli PE, Mangoni L, Gentile P, Braghiroli M, Fossarello M. A panel of broad-spectrum antivirals in topical ophthalmic medications from the drug repurposing approach during and after the coronavirus disease 2019 era. J Clin Med. 2020;9:2441. doi:10.3390/jcm9082441
21. Isenberg SJ, Apt L, Valenton M, et al. A Controlled Trial of Povidone–Iodine to Treat Infectious Conjunctivitis in Children. Am J Ophthalmol. 2002;134:681–688. doi:10.1016/S0002-9394(02)01701-4
22. Sauerbrei A, Sehr K, Brandstädt A, et al. Sensitivity of human adenoviruses to different groups of chemical biocides. J Hosp Infect. 2004;57:59–66. doi:10.1016/j.jhin.2004.01.022
23. Monnerat N, Bossart W, Thiel MA. Povidone-iodine for treatment of adenoviral conjunctivitis: an in vitro study. Klin Monatsbl Augenheilkd. 2006;223:349–352. doi:10.1055/s-2006-926633
24. Rutala WA, Peacock JE, Gergen MF, Sobsey MD, Weber DJ. Efficacy of hospital germicides against adenovirus 8, a common cause of epidemic keratoconjunctivitis in health care facilities. Antimicrob Agents Chemother. 2006;50:1419–1424. doi:10.1128/AAC.50.4.1419-1424.2006
25. Pelletier JS, Stewart K, Trattler W, et al. A combination povidone-iodine 0.4%/dexamethasone 0.1% ophthalmic suspension in the treatment of adenoviral conjunctivitis. Adv Ther. 2009;26:776–783. doi:10.1007/s12325-009-0062-1
26. Clement C, Capriotti JA, Kumar M, et al. Clinical and antiviral efficacy of an ophthalmic formulation of dexamethasone povidone-iodine in a rabbit model of adenoviral keratoconjunctivitis. Invest Ophthalmol Vis Sci. 2011;52:339–344. doi:10.1167/iovs.10-5944
27. Trinavarat A, Atchaneeyasakul L. Treatment of epidemic keratoconjunctivitis with 2% povidone-iodine: a pilot study. J Ocul Pharmacol Ther. 2012;28:53–58. doi:10.1089/jop.2011.0082
28. Yates KA, Shanks RMQ, Kowalski RP, Romanowski EG. The in vitro evaluation of povidone-iodine against multiple ocular adenoviral types. J Oc Pharm Ther. 2019;35:132–136. doi:10.1089/jop.2018.0122
29. Wood A, Payne D. The action of three antiseptics/disinfectants against enveloped and non-enveloped viruses. J Hosp Infect. 1998;38:283–295. doi:10.1016/S0195-6701(98)90077-9
30. Béleca L, Tevi-Benissana C, Bianchic A, et al. In vitro inactivation of Chlamydia trachomatis and of a panel of DNA (HSV-2, CMV, adenovirus, BK virus) and RNA (RSV, enterovirus) viruses by the spermicide benzalkonium chloride. J Antimicrob Chemother. 2000;46:685–693. doi:10.1093/jac/46.5.685
31. Romanowski EG, Yates KA, Shanks RMQ, Kowalski RP. Benzalkonium chloride demonstrates concentration dependent antiviral activity against adenovirus in vitro. J Oc Pharm Ther. 2019;35:311–314. doi:10.1089/jop.2018.0145
32. Romanowski EG, Yates KA, O’Connor KE, Mah FS, Shanks RMQ, Kowalski RP. The evaluation of polyhexamethylene biguanide (PHMB) as a disinfectant for adenovirus. JAMA Ophthalmol. 2013;131:495–498. doi:10.1001/jamaophthalmol.2013.2498
33. Morfin F, Dupuis-Girod S, Mundweiler S, et al. In vitro susceptibility of adenovirus to antiviral drugs is species-dependent. Antivir Ther. 2005;10:225–229.
34. Lee CS, Lee AY, Akileswaran L, et al. BAYnovation Study Group. Determinants of outcomes of adenoviral keratoconjunctivitis. Ophthalmology. 2018;125(9):1344–1353. doi:10.1016/j.ophtha.2018.02.016
35. Romanowski EG, Mah FS, Yates KA, Kowalski RP, Gordon YJ. The successful treatment of gatifloxacin-resistant Staphylococcus aureus keratitis with Zymar® (Gatifloxacin 0.3%) in a NZW Rabbit Model. Am J Ophthalmol. 2005;139:867–877. doi:10.1016/j.ajo.2005.01.021
36. Kowalski RP, Romanowski EG, Mah FS, Shanks RMQ, Gordon YJ. Topical levofloxacin 1.5% overcomes in vitro resistance in rabbit keratitis models. Acta Ophthalmol. 2010;88:e120–125. doi:10.1111/j.1755-3768.2010.01897.x
37. Kowalski RP, Romanowski EG, Yates KA, Romanowski JE, Grewal A, Bilonick RA. Is there a role for topical penicillin treatment of Staphylococcus aureus keratitis based on elevated corneal concentrations? J Clin Ophthalmol Optom. 2018;2:103.
38. Romanowski JE, Romanowski EG, Yates KA, Kowalski RP. The successful treatment of experimental methicillin-resistant Staphylococcus aureus (MRSA) keratitis with topical penicillin. Ophthalmol Res Rep. 2018;3:ORRT–128.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.