")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
The importance of early identification of infusion-related reactions to monoclonal antibodies
Authors Cáceres MC , Guerrero-Martín J , Pérez-Civantos D, Palomo-López P , Delgado-Mingorance JI, Durán-Gómez N
Received 11 February 2019
Accepted for publication 27 May 2019
Published 1 August 2019 Volume 2019:15 Pages 965—977
DOI https://doi.org/10.2147/TCRM.S204909
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Macarena C Cáceres,1 Jorge Guerrero-Martín,1 Demetrio Pérez-Civantos,2,3 Patricia Palomo-López,1 Juan Ignacio Delgado-Mingorance,4 Noelia Durán-Gómez1
1Department of Nursing, University of Extremadura, Badajoz, Spain; 2Department of Biomedicine, University of Extremadura, Badajoz, Spain; 3Intensive Care Medicine Department, University Hospital of Badajoz, Servicio Extremeño de Salud, Badajoz, Spain; 4Oncology Department, University Hospital of Badajoz, Servicio Extremeño de Salud, Badajoz, Spain
Abstract: Monoclonal antibodies constitute important and useful tools in clinical practice and biotechnology for diagnosing and treating infectious, inflammatory, immunological and neoplastic diseases. This article reviews evidence on the different acute adverse effects of monoclonal antibodies, specifically infusion-related reactions (IRRs), and on the measures that should be taken before and during crises. A literature search using key terms relating to IRRs produced by monoclonal antibodies was undertaken to generate a comprehensive narrative review of the information available. Immunomodulatory monoclonal antibodies may produce IRRs and hypersensitivity-related reactions. Strategies to avoid or minimize the appearance of IRRs depend on the monoclonal antibody and type of patient and reaction (pre-medication, slowing infusion rates, infusion interruption or desensitization, etc.). Considering the great number of available monoclonal antibodies in current practice and those which will soon be authorized, it is mandatory to have clear guidelines that can give support to practitioners and nurses to help them respond quickly and safely to the different IRRs related to the use of these therapeutic drugs.
Keywords: antibodies, monoclonal, drug-related side effects and adverse reactions, nurse practitioners
Introduction
Important recent advances in biomedical science have been associated with the development and clinical application of biological agents based on monoclonal antibodies (mAb).1 These have been used as important tools in clinical practice and biotechnology in diagnosing and treating infectious, inflammatory, immunological and neoplastic diseases, and also for examining the host/pathogen interaction, and for detecting and quantifying diverse molecules.2
Throughout the evolution from murine, chimeric, and humanized to completely human products, there has been a significant reduction in the immunogenic risks associated with mAbs that resemble endogenous human immunoglobulins more closely.3 Their high specificity enables achieving of very accurate targets that can determine various cellular changes. The clinical use of nearly human or completely human mAbs has increased their clinical tolerability.4 However, an inherent risk of generating adverse immune-mediated drug reactions in humans, such as infusion-related reactions (IRRs), cytokine storms, immunosuppression and autoimmunity has constituted a major obstacle for the development of an early clinical investigation of many of these immunomodulatory mAbs.5
In an analysis of FDA MedWatch safety alerts for mAbs therapeutics, Stanulovic et al (2011) showed that premarketing clinical trials can predict more than half of safety concerns.6 This means, however, that a high percentage of the adverse reactions that mAbs may present will be known through post-marketing notifications. Stanulovic et al (2015) expanded this analysis to assess whether predictable alerts are detected sooner than unpredictable alerts. It was demonstrated that placing the focus on such predictable reactions defined as potential risks may play a role in detecting important safety concerns earlier.7
In recent years, regulatory agencies have approved the merchandising of new mAbs, and many more will appear in the very near future. Nursing professionals, who are responsible for drug administration, should be aware of the most important characteristics of this type of therapeutic tools (mechanisms of action, adverse effects, etc.).8 As a rapid response and appropriate management of hypersensitivity reactions (HR) is vital for optimal patient outcomes, nurses dealing with infusion ought to be familiar with the signs and symptoms of the typical infusion reactions seen with monoclonal antibody treatments, as well as the symptoms of more severe HR.9
It is very important that any facility where mAbs are administered has all the required emergency resuscitation equipment and medication, and that rigorously trained staff are readily available. A basic emergency plan should be made, and each nurse must be familiar and at ease with the protocol.10
Although IRRs are the most common adverse effects of the majority of mAbs, these are usually easily manageable.11
This article reviews recent evidence on the different acute adverse effects of mAbs, and more specifically iIRRs, and on the measures that should be taken before and during crises to control them.
Methods
Different key terms relating to IRRs produced by mAbs were employed to undertake a literature search in order to generate a comprehensive narrative review of the information available. Hand-searching was carried out to find relevant papers from the reference lists of included articles. In addition, all the summaries of product characteristics12 of mAbs in which a possible presentation of IRRs is reported have been reviewed.
Results
Infusion-related reactions
IRRs are common adverse drug reactions which happen when monoclonal antibodies are infused. Symptoms are related in time to drug administration and may range from symptomatic discomfort to fatalities.13 Death may occur rapidly; thus, when dealing with severe IRRs, it is essential that risks are understood and early signs and symptoms are recognized quickly. All clinical staff should know about and be well trained in managing acute adverse events.14
IRRs may be defined as “any signs or symptoms experienced by patients during the infusion of pharmacologic or biologic agents or any event occurring on the first day of drug administration.”14 Acute reactions can manifest within 24 hrs from the first administration of the mAbs, but they appear most frequently from 10 mins to 4 hrs after beginning the administration.15 Clinical manifestations of these reactions vary; Table 1 shows the IRRs reported in the technical files of all mAb drugs ordered according to the ATC classification.12,16
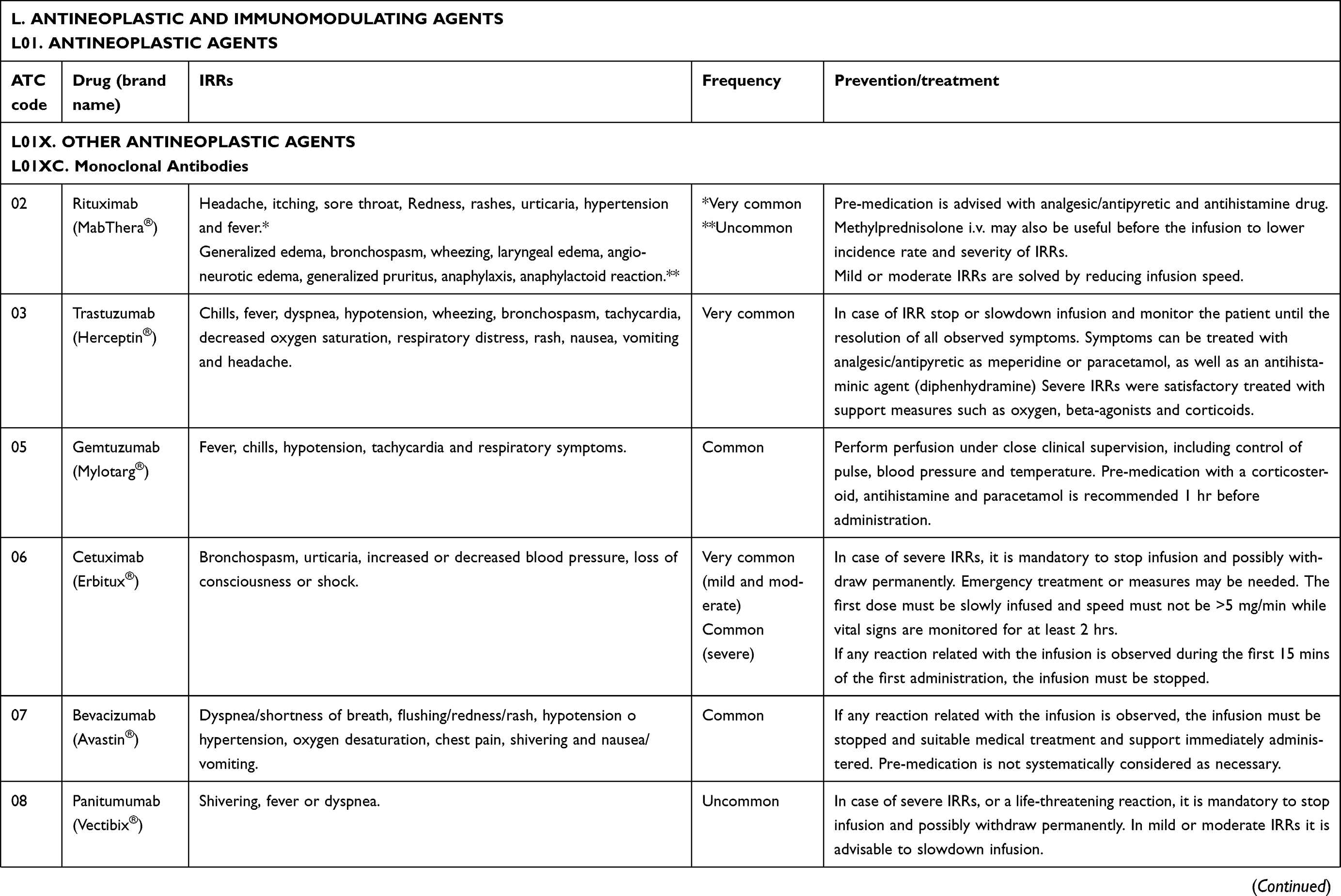 |
Table 1 IRRs reported in the technical files of all mAb drugs |
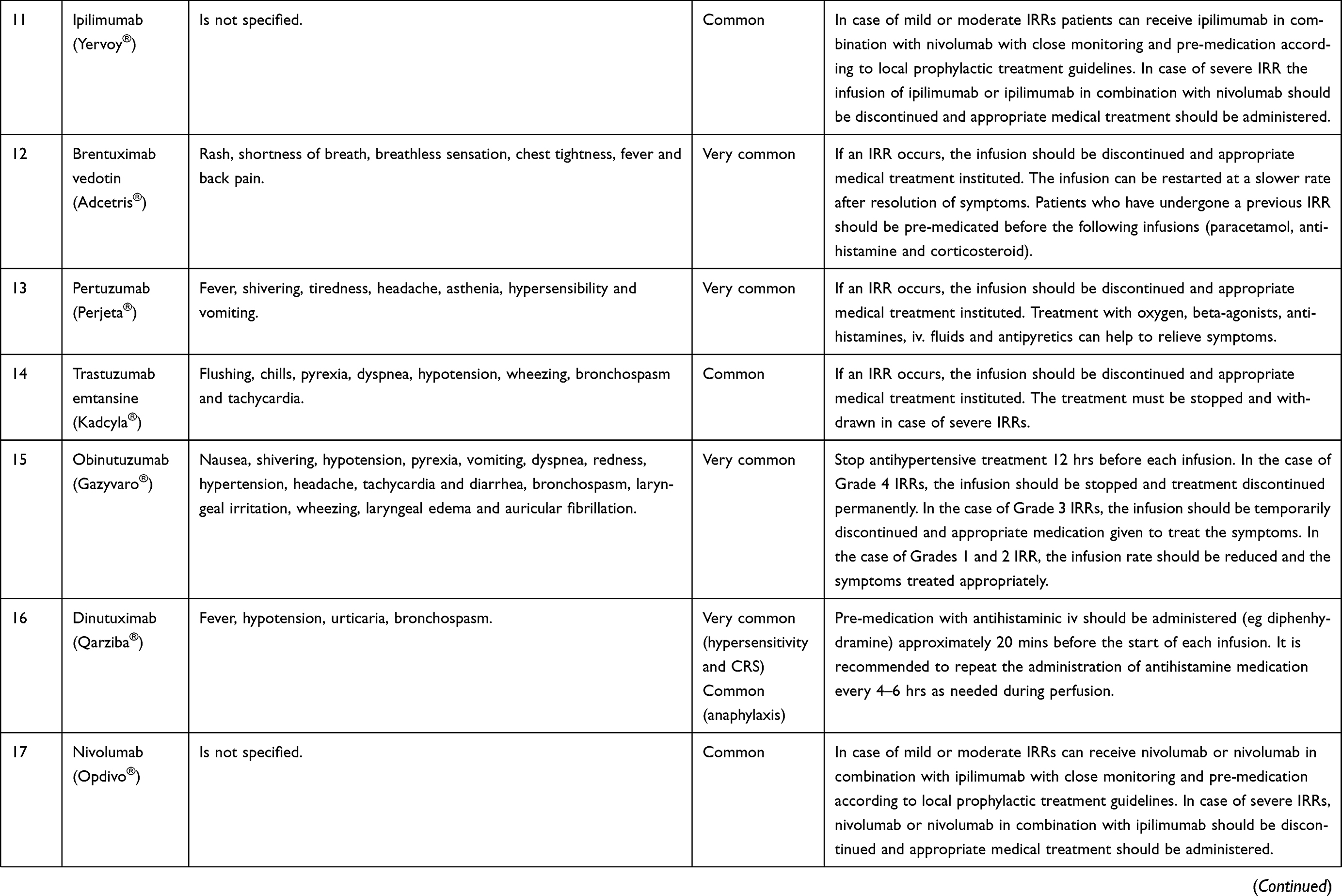 |
Table 1 (Continued). |
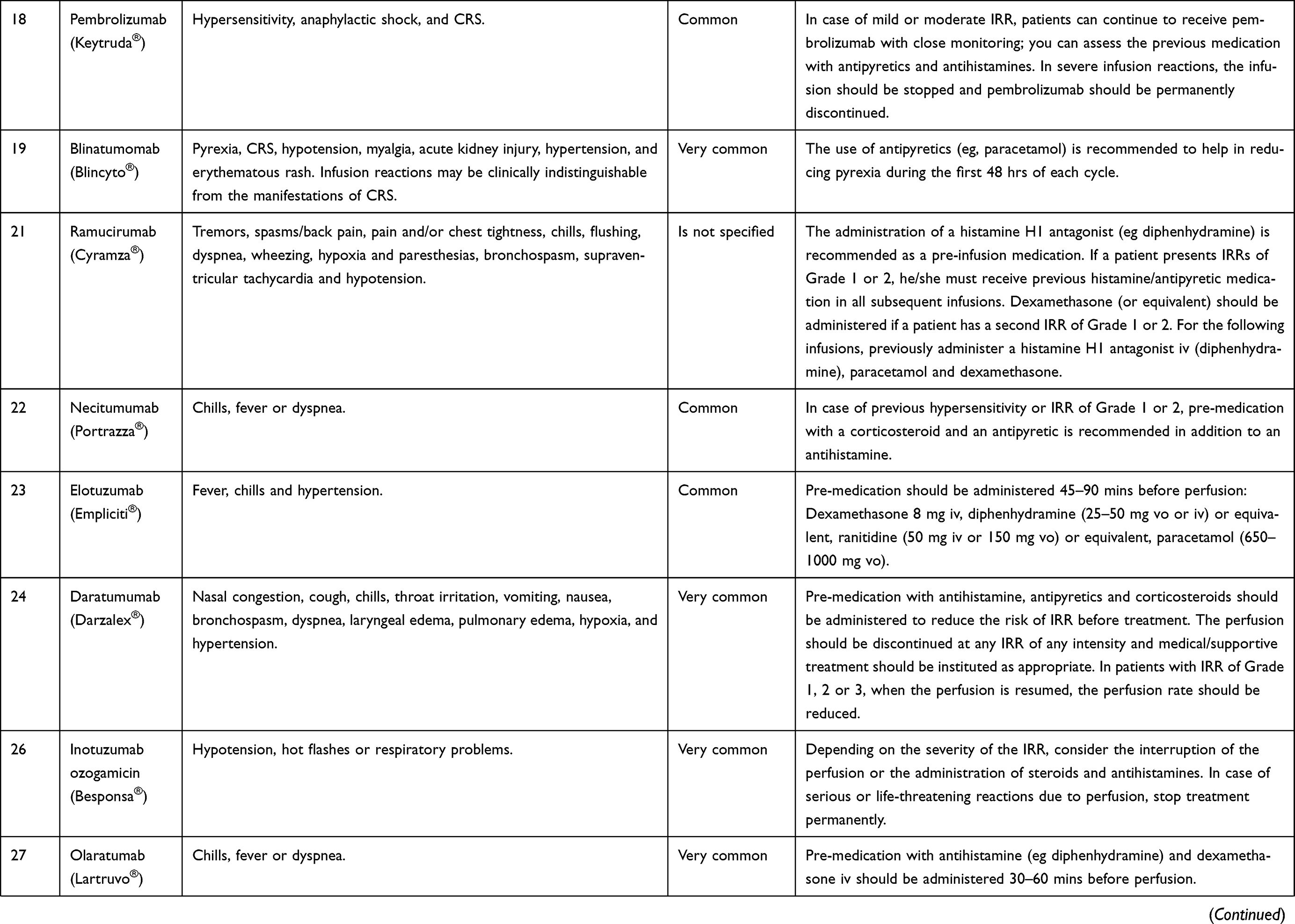 |
Table 1 (Continued). |
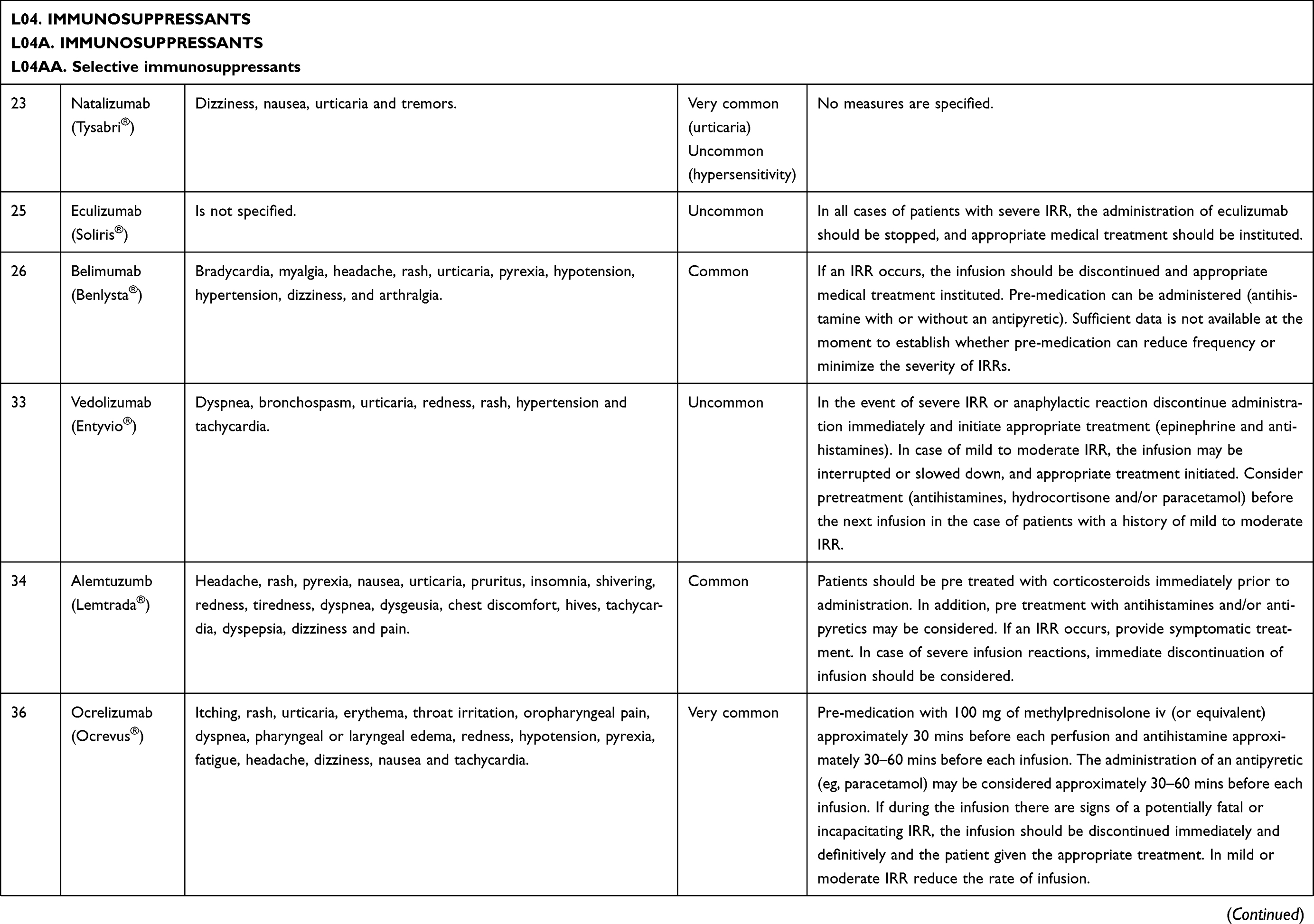 |
Table 1 (Continued). |
Immunomodulatory mAbs may also result in different HR that include IRRs, cytokine-release reactions, type I (IgE/non-IgE), type III and delayed type IV reactions.17 The symptoms of all types of immunologically mediated infusion reactions overlap, making it difficult to pinpoint the cause without additional laboratory work.5,14
Joint Task Force on Practice Parameters for drug allergy defined anaphylaxis as “an immediate systemic reaction that occurs when a previously sensitized individual is re-exposed to an allergen.”18 The characteristics of true anaphylactic reactions (type I IgE-mediated HR) are dyspnea and tightness of the chest, suffocation, hypotension, bronchospasm, and urticaria; in the absence of either of the latter two symptoms, it is unlikely that an acute reaction is anaphylactic, and it should thus be considered non-allergic.19,20 Since the first exposure to antigen is required for IgE sensitization, type I HR do not occur during the first administration of a mAbs infusion,21 except in rare cases where patients have pre-existing antibodies which cross-react with the drug.5,22
Non-IgE reactions are “immediate systemic reactions that mimic anaphylaxis but are caused by non-IgE-mediated release of mediators from mast cells and basophils.”18 These reactions can occur at the first exposure to an antigen and may be clinically indistinguishable from anaphylaxis. Unlike anaphylactic reactions, non-IgE reactions become milder upon repeated administration. However, there does not appear to be consensus as to whether non-IgE reaction is a separate entity from anaphylaxis.13
Complement activation-related pseudoallergy (CARPA)
CARPA is linked to adverse events evoked by several liposomal and micellar formulations, nanoparticles, radiocontrast agents, and therapeutic antibodies.23 It has been reported as:
a HR, the symptoms of which fit into the Coombs and Gell’s Type I category, which is not initiated or mediated by pre-existing IgE antibodies but arises as a consequence of activation of the complement system.24
MAbs activate the classical complement pathway by binding to the target antigen, allowing the binding of C1q, the recognition molecule of the activation initiator C1 complex, to the Fc part of the antibodies. MAb may provoke this feature and can be manipulated to enhance the effectiveness for avoiding certain adverse effects.25 CARPA typically appears within minutes after the start of the infusion. However, a delay is possible, particularly in pre-medicated patients. Almost all organs can be affected, the most often observed symptoms being flushing, rash, dyspnea, chest pain, back pain and subjective distress.13 All currently available mAbs can be considered to be potentially immunogenic, as their molecular size is large enough and their structure is different from endogenous proteins.25
Cytokine-release syndrome (CRS) is “a potentially life-threatening systemic inflammatory reaction which is observed after the infusion of agents targeting different immune effectors.”26 CRS can manifest itself with a variety of symptoms that range from mild, flu-like symptoms to severe life-threatening occurrences of the overshooting inflammatory response. Starting out with fever and unspecific symptoms, CRS might impact the majority of organ systems (Grades III–IV cases shows signs of life-threatening cardiovascular, pulmonary, renal involvement or neurotoxicity).27 Because events manifest during or after the first exposure to a “new” drug, a differentiation from anaphylaxis may be difficult. There are few allergy-specific symptoms such as urticaria or glottis edema which could guide an allergic diagnosis here.26 In order to get a differential diagnosis, it could be of help to obtain several samples of serum to know the plasmatic level of tryptase (tryptase test), it has to be done at 30 mins of the event, at 2 hrs and at 24 hrs. If this test results positive, it can indicate the activation of mastocytes, and in case of negative, it could be compatible with a CRS or tumoral lysis.28
Health care practitioners must differentiate between the terms “infusion reaction” and “anaphylaxis” and give a clear definition of which symptoms are to be labeled as “infusion-related reaction.” “Infusion reactions” usually represent symptoms that occur within a close time-related relationship to an infusion and are not necessarily linked to anaphylaxis or even hypersensitivity.13 In any case, it may be difficult to differentiate between various types of reactions at the onset of symptoms. Anaphylactic reactions occur within the first few minutes of the infusion, so documenting the time of the onset of symptoms is highly important.10
The latest version of Common Terminology Criteria for Adverse Events by The US Department of Health and Human Services of the National Cancer Institute (National Institute of Health) depicts a differentiation of all these concepts, using a grading scale of adverse events (Table 2).29
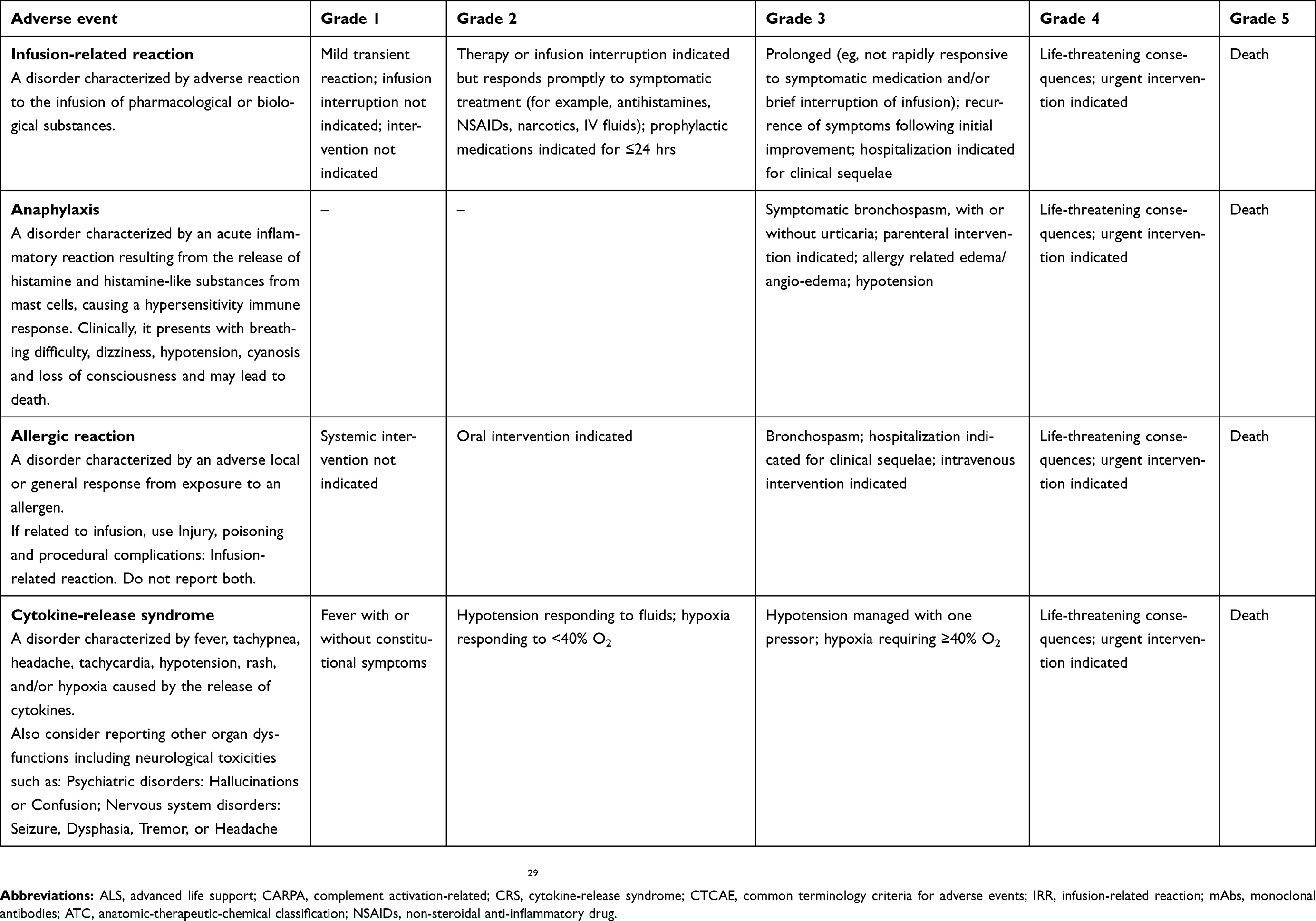 |
Table 2 Extracts from the Common Terminology Criteria for Adverse Events v5.0 (CTCAE) |
Due to the fact that current reporting practices are predominantly based on clinical presentation, researchers, health care professionals and pharmaceutical companies are not employing consistent terminology for reporting IRRs, which leads to under-reporting or over-reporting of allergic reactions, in particular, anaphylaxis.13 Terminology differs between package inserts (eg, allergic reactions, hypersensitivity and infusion reaction) which is a real obstacle. The grading criteria used to measure the severity of the reaction are often unclear. Inserts are vague concerning the exact timing of the reaction. Defining terminology is essential. Similar impediments often seen in clinical practice and medical literature include variations in terminology, inadequate documentation about time of onset of the reaction, inconsistency in grading, lack of documentation on when the reaction occurred, record of pre-medications (if any), and inadequate citation of management actions and effectiveness.10
Infusion-related reactions: prevention and treatment
Considering the varied nature of infusion reactions, nurses and other health care practitioners must recognize the underlying nature of these events for a clear identification of patients at risk and for providing optimal prophylactic measures and management of symptoms.30 Nursing professionals must be aware of different strategies to tackle with MAb HR. They have to register the onset time of reaction and symptoms, vital signs and rate of infusion at the time of the event. A rapid initiation of emergency measures must be taken. As initial clinical measures are similar to all type of reactions and the knowledge of a standard protocol is mandatory. We provide an algorithm (Figure 1) that shows a daily-practice guide to manage the use of mAbs, in agreement with the Departments of Intensive Care, Oncology and Allergy of the University Hospital, Badajoz (Health Service of Extremadura, Spain).
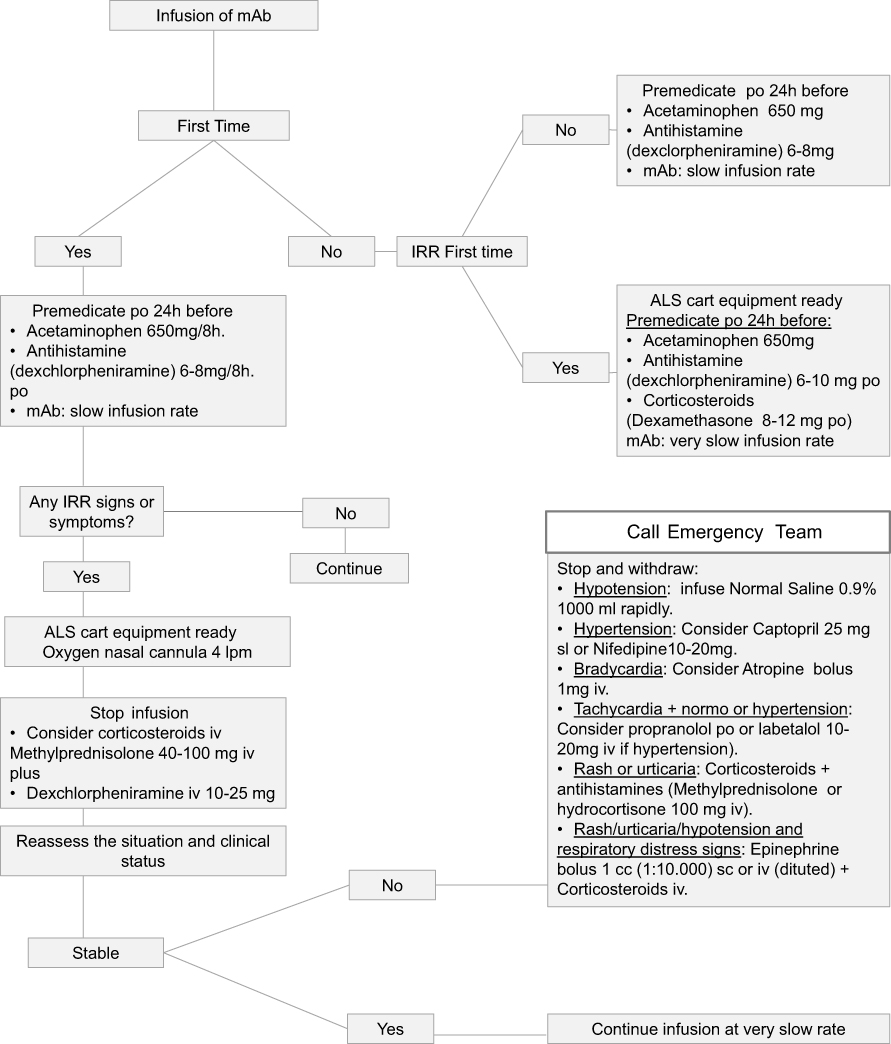 |
Figure 1 Algorithm proposed as a daily-practice guide to manage the use of mAb.Abbreviations: IRR, infusion-related reaction; ALS, advanced life support; mAbs, monoclonal antibodies; po, per oral; iv, intravenous; sl, sublingual; sc, subcutaneous. |
Readministration strategies to avoid or minimize the appearance of IRRs depending on the mAb and type of patient and reaction may include pre-medication (paracetamol, NSAIDs antihistamines, and corticosteroids) to reduce incidence or mitigate the symptoms. In addition, it may be necessary to slowdown infusion rates, or interrupt infusion, and in some cases, it could be necessary to reinitiate the treatment. This depends on the type of mAb and the severity of the IRR. Other measures could be to induce pharmacological desensitization and temporary immune tolerance15 or to fractionate the dose.13,18
Most technical files agree that the majority of mild or moderate IRRs are generally solved by slowing down the speed of infusion. Nevertheless, in case of a severe IRR, infusion must be stopped and reintroduction of treatment needs to be assessed. The decision to recommence an infusion will depend on the nature of the reaction and the choices made by the clinician. Each case must be considered separately, taking onboard the severity of the initial reaction, comorbidities, the aims of the therapy, and the risk of rechallenge versus the potential benefits of successful treatment.10
Although the information available in technical files with regard to the pharmacologic treatment of IRRs varies, there is some agreement on the need to establish symptomatic medical treatment, which can be the use of oxygen, beta-agonist agents, corticosteroids, intravenous fluid therapy or even antipyretics. The re-establishment of the mAb treatment may require the use of pre-medication.
Many studies have valued the efficacy of pre-medication to reduce or diminish symptoms of acute reactions due to mAbs. In the vast majority of the technical files, this is specifically recommended (with some exceptions as in the case of bevacizumab where the use of pre-medication is not systematically recommended).
Dotson et al (2016) carried out a study of which the main objective was to assess the safety and feasibility of a 60-min rituximab rapid infusion protocol (in B cell non-Hodgkin’s lymphoma patients) in the outpatient infusion center of a comprehensive cancer center. The conclusion of the study was that infusions can be safely administered over 60 mins and without steroid pre-medication in an experienced outpatient infusion center where patients are appropriately screened. The more rapid infusions can reduce the use of resources and increase satisfaction among nursing personnel.31
Ikegawa et al (2017) evaluated IRRs associated with cetuximab combination chemotherapy comprising an H1-receptor antagonist plus dexamethasone as anti-allergy pre-medications for patients with head and neck cancer. They reported that the occurrence of IRRs was lower compared with previous studies. Dexamethasone combined with an H1-receptor antagonist was useful for preventing allergic responses.32
When evaluating the first dose of trastuzumab, IRRs happened more commonly when patients were not administrated pre-medication compared to those who were. Previously unknown risk factors associated with the development of trastuzumab-associated IRRs have also been identified, more specifically the issues of obesity and advanced stage breast cancer, which may enable clinicians to identify patients at high risk for IRRs who could potentially benefit from pre-medication, although this hypothesis needs to be further validated.33
In patients with IRRs observed during previous obinutuzumab infusions, pre-medication with an oral analgesic such as acetaminophen or paracetamol and antihistamine before obinutuzumab treatment is required. In addition, pre-medication with corticosteroids should be considered as an option in patients with a high risk of severe IRRs.11,34
In dermatologic subjects with mild to moderate infusion reactions to infliximab, the prophylactic treatment of oral diphenhydramine and paracetamol should be administered at subsequent infusions, 90 mins before the start of each infusion. In patients who have manifested severe infusion reactions, pre-medication with IV hydrocortisone acetate 100 mg 20 mins before the infusion or with oral prednisone the day before the infusion is optional, according to the opinion of the clinician involved.19 Bartoli et al (2016) led a study which aimed to evaluate the incidence of IRRs in patients with joint inflammatory diseases (rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis) receiving treatment with infliximab with and without pre-medication. The combination of paracetamol, hydroxyzine, 6-methylprednisolone and ranitidine was more effective than paracetamol, esomeprazole, hydrocortisone, and chlorpheniramine maleate combination protocol to reduce the number of IRRs due to infliximab.35
Pre-medications are considered as standard procedure for keeping the risk for IRRs with mAbs to a minimum. However, due to the fact that most infusion reactions with mAbs take place following the first or second infusion, the value of pre medication on subsequent infusions may decrease.
For the type of patients that receive treatment with mAbs, a change or swift to second-line drugs after a HR can have a negative impact for their quality of life and life expectancy.36 New guidelines in the management and treatment of reactions, creating a new standard of care for mAb desensitization.17 There exist different protocols for desensitization that even allow a single day outpatient performance with trained 1-to-1 nursing. The protocol of Brenann et al (2009) proposes single day outpatient desensitization performed in a hospital associated infusion center with specially trained 1-to-1 nursing.37 Until now, it has been successfully desensitized mAb HSR to rituximab, ofatumumab, obinutuzumab, trastuzumab, cetuximab, tocilizumab, infliximab, etanercept, adalimumab, golimumab, certolizumab, brentuximab, bevacizumab and omalizumab.38
Conclusion
To conclude, mAbs can give rise to HR, such as anaphylaxis, IRRs, CRS or CARPA. Nurses responsible for the administration of mAbs should be able to promptly identify and grade IRRs, and to rapidly manage any adverse reaction linked with the use of these drugs in order to prevent dangerous risks for patients.
Although recommendations or published protocols exist on the management of IRRs caused by some mAbs, such as infliximab in dermatologic patients,19 obinutuzumab in chronic lymphocytic leukemia patients,34 natalizumab in multiple sclerosis,9 much remains to be known about the correct way to manage IRRs. In addition to this, the lack of uniform terminology entails an obstacle for clinical practice.
Considering the great number of mAbs available in current practice and those which will soon be authorized, it is mandatory to have clear guidelines that can give support to practitioners and nurses to help them respond quickly and safely to the different IRRs related to the use of these therapeutic drugs.
Acknowledgments
This work was partially financed by a grant of the Regional Goverment of Extremadura; European Regional Development Fund (FEDER; IB18101).
The collaboration of Dr Pedro Bobadilla from the Badajoz University Hospital, Allergology Department, is gratefully acknowledged.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lushova A, Biazrova M, Prilipov A, Sadykova G, Kopylov T, Filatov A. Next-generation techniques for discovering human monoclonal antibodies. Mol Biol. 2017;51(6):782–787. doi:10.1134/S0026893317060103
2. Machado NP, Tèllez GA, Castaño JC. Anticuerpos monoclonales: desarrollo físico y perspectivas terapéuticas [Monoclonal antibodies: physical development and therapeutic perspectives]. Infectio. 2006;10(3):186–197.
3. Cui Y, Cui P, Chen B, Li S, Guan H. Monoclonal antibodies: formulations of marketed products and recent advances in novel delivery system. Drug Dev Ind Pharm. 2017;43(4):519–530. doi:10.1080/03639045.2017.1278768
4. Merino AG. Anticuerpos monoclonales. aspectos básicos. [Monoclonal antibodies. Basic aspects]. Neurología. 2011;26(5):301–306. doi:10.1016/j.nrl.2010.10.005
5. Brennan FR, Morton LD, Spindeldreher S, et al. Safety and immunotoxicity assessment of immunomodulatory monoclonal antibodies. mAbs. 2010;2(3):233–255. doi:10.4161/mabs.2.3.11782
6. Stanulovic V, Zelko R, Kerpel-Fronius S. Predictability of serious adverse reaction. Int J Clin Pharmacol Ther. 2011;49(3):185–190. doi:10.5414/cp201497
7. Stanulovic V, Kadlecova P, Zelko R, Kerpel-Fronius S. Earlier identification of risks: cumulative probability analysis of time to safety alerts for therapeutic monoclonal antibodies. Int J Clin Pharmacol Ther. 2015;53(7):499–503. doi:10.5414/CP202283
8. Cáceres MC, Durán-Gómez N, Guerrero-Martín J, Pérez Civantos DV, Carreto-Lemus MA, Postigo-Mota S. Interés para la enfermera de los nuevos anticuerpos monoclonales. una revolución terapéutica. Revista Rol De Enfermera. 2017;40(7–8):524–530.
9. Namey M, Halper J, O’leary S, Beavin J, Bishop C. Best practices in multiple sclerosis: infusion reactions versus hypersensitivity associated with biologic therapies. J Infus Nurs. 2010;33(2):98–111. doi:10.1097/NAN.0b013e3181cfd36d
10. Vogel WH. Infusion reactions: diagnosis, assessment, and management. Clin J Oncol Nurs. 2010;14(2):E10. doi:10.1188/10.CJON.E10-E21
11. Korycka-Wołowiec A, Wołowiec D, Robak T. The safety profile of monoclonal antibodies for chronic lymphocytic leukemia. Expert Opin Drug Saf. 2017;16(2):185–201. doi:10.1080/14740338.2017.1264387
12. Cima (aemps); 2018. Available from: https://cima.aemps.es/cima/publico/home.html.
13. Doessegger L, Banholzer ML. Clinical development methodology for infusion-related reactions with monoclonal antibodies. Clin Transl Immunol. 2015;4(7):e39. doi:10.1038/cti.2015.14
14. Kang SP, Saif MW. Infusion-related and hypersensitivity reactions of monoclonal antibodies used to treat colorectal cancer – identification, prevention, and management. J Support Oncol. 2007;5(9):451–457.
15. Calogiuri G, Ventura MT, Mason L, et al. Hypersensitivity reactions to last generation chimeric, umanized and human recombinant monoclonal antibodies for therapeutic use. Curr Pharm Des. 2008;14(27):2883–2891.
16. WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2019. Available from: http://www.whocc.no/atc_ddd_index/.
17. Isabwe GAC, Neuer MG, de Las Vecillas Sanchez L, Lynch D, Marquis K, Castells M. Hypersensitivity reactions to therapeutic monoclonal antibodies: phenotypes and endotypes. J Allergy Clin Immunol. 2018;142(1):
18. Joint Task Force on Practice Parameters, American Academy of Allergy, Asthma and Immunology, American College of Allergy, Asthma and Immunology, Joint Council of Allergy, Asthma and Immunology. Drug allergy: an updated practice parameter. Ann Allergy Asthma Immunol. 2010;105(4):259–273. doi:10.1016/j.anai.2010.08.002
19. Puig L, Sáez E, Lozano MJ, et al. Reacciones a la infusión de infliximab en pacientes dermatológicos. [reactions to infliximab infusions in dermatologic patients: consensus statement and treatment protocol]. Actas Dermo-Sifiliográficas. 2009;100(2):103–112.
20. Cheifetz A, Smedley M, Martin S, et al. The incidence and management of infusion reactions to infliximab: A large center experience. Am J Gastroenterol. 2003;98(6):1315–1324. doi:10.1111/j.1572-0241.2003.07457.x
21. Maggi E, Vultaggio A, Matucci A. Acute infusion reactions induced by monoclonal antibody therapy. Expert Rev Clin Immunol. 2011;7(1):55–63. doi:10.1586/eci.10.90
22. Chung CH, Mirakhur B, Chan E, et al. Cetuximab-induced anaphylaxis and IgE specific for galactose-α-1, 3-galactose. N Engl J Med. 2008;358(11):1109–1117. doi:10.1056/NEJMoa074943
23. Szebeni J. Complement activation-related pseudoallergy caused by liposomes, micellar carriers of intravenous drugs, and radiocontrast agents. Crit Rev Ther Drug Carrier Syst. 2001;18(6):567–606.
24. Szebeni J. Complement activation-related pseudoallergy: a new class of drug-induced acute immune toxicity. Toxicology. 2005;216(2):106–121. doi:10.1016/j.tox.2005.07.023
25. Fülöp T, Mészáros T, Kozma G, Szebeni J, Józsi M. Infusion reactions associated with the medical application of monoclonal antibodies: the role of complement activation and possibility of inhibition by factor H. Antibodies. 2018;7(1):14. doi:10.3390/antib7010014
26. Kroschinsky F, Stölzel F, von Bonin S, et al. New drugs, new toxicities: severe side effects of modern targeted and immunotherapy of cancer and their management. Crit Care. 2017;21(1):89. doi:10.1186/s13054-017-1686-1
27. Shimabukuro-Vornhagen A, Gödel P, Subklewe M, et al. Cytokine release syndrome. J Immunother Cancer. 2018;6(1):56. doi:10.1186/s40425-018-0343-9
28. Cardona V, Cabañes N, Chivato T, De la Hoz B, Fernández Rivas M, Gangoiti Goikoetxea I. Guía de actuación en anafilaxia: Galaxia 2016 [Anaphylaxis Action Guide: Galaxia]. Available from: https://www.aepnaa.org/recursos/publicaciones-archivos/5851f6dd835b9ffc3f32220233dc3eca.pdf. Spanish.
29. US Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. national institutes of health, national cancer institute; 2017.
30. Chung CH. Managing premedications and the risk for reactions to infusional monoclonal antibody therapy. Oncologist. 2008;13(6):725–732. doi:10.1634/theoncologist.2008-0012
31. Dotson E, Crawford B, Phillips G, Jones J. Sixty-minute infusion rituximab protocol allows for safe and efficient workflow. Support Care Cancer. 2016;24(3):1125–1129. doi:10.1007/s00520-015-2869-4
32. Ikegawa K, Suzuki S, Nomura H, et al. Retrospective analysis of premedication, glucocorticosteroids, and H1-antihistamines for preventing infusion reactions associated with cetuximab treatment of patients with head and neck cancer. J Int Med Res. 2017;45(4):0300060517713531.
33. Thompson LM, Eckmann K, Boster BL, et al. Incidence, risk factors, and management of infusion-related reactions in breast cancer patients receiving trastuzumab. Oncologist. 2014;19(3):228–234. doi:10.1634/theoncologist.2013-0286
34. Snowden A, Hayden I, Dixon J, Gregory G. Prevention and management of obinutuzumab‐associated toxicities: Australian experience. Int J Nurs Pract. 2015;21(S3):15–27. doi:10.1111/ijn.12412
35. Bartoli F, Bruni C, Cometi L, et al. Premedication prevents infusion reactions and improves retention rate during infliximab treatment. Clin Rheumatol. 2016;35(11):2841–2845. doi:10.1007/s10067-016-3351-5
36. Sloane D, Govindarajulu U, Harrow-Mortelliti J, et al. Safety, costs, and efficacy of rapid drug desensitizations to chemotherapy and monoclonal antibodies. J Allergy Clin Immunol. 2016;4(3):497–504. doi:10.1016/j.jaip.2015.12.019
37. Brennan PJ, Bouza TR, Hsu FI, Sloane DE, Castells MC. Hypersensitivity reactions to mAbs: 105 desensitizations in 23 patients, from evaluation to treatment. J Allergy Clin Immunol. 2009;124(6):1259–1266. doi:10.1016/j.jaci.2009.09.009
38. Bonamichi-Santos R, Castells M. Diagnoses and management of drug hypersensitivity and anaphylaxis in cancer and chronic inflammatory diseases: reactions to taxanes and monoclonal antibodies. Clin Rev Allergy Immunol. 2018;54(3):375–385. doi:10.1007/s12016-016-8556-5
39. Guidelines for preparing core clinical-safety information on drugs second edition – report of CIOMS working groups III and V • COUNCIL FOR INTERNATIONAL ORGANIZATIONS OF MEDICAL SCIENCES; 1999. Available from: https://cioms.ch/shop/product/guidelines-preparing-core-clinical-safety-information-drugs-second-edition-report-cioms-working-groups-iii-v/.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.