")
Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 11
The Impact of Obesity on the Outcomes of Adult Patients with Acute Lymphoblastic Leukemia – A Single Center Retrospective Study
Authors Liu Q, Major B, Le-Rademacher J, Al-Kali AA , Alkhateeb H, Begna K , Elliott MA, Gangat N, Hogan WJ, Hook CC, Kaufmann SH , Pardanani A, Patnaik MS, Tefferi A, Wolanskyj-Spinner AP , Wei W , Litzow MR
Received 6 September 2020
Accepted for publication 28 November 2020
Published 22 January 2021 Volume 2021:11 Pages 1—9
DOI https://doi.org/10.2147/BLCTT.S269748
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Wilson Gonsalves
Qiuju Liu,1 Brittny Major,2 Jennifer Le-Rademacher,2 Aref A Al-Kali,3 Hassan Alkhateeb,3 Kebede Begna,3 Michelle A Elliott,3 Naseema Gangat,3 William J Hogan,3 C Christopher Hook,3 Scott H Kaufmann,3 Animesh Pardanani,3 Mrinal S Patnaik,3 Ayalew Tefferi,3 Alexandra P Wolanskyj-Spinner,3 Wei Wei,4 Mark R Litzow3
1Department of Cancer Center, Division of Hematology, Jilin University, Changchun, Jilin, People’s Republic of China; 2Department of Health Sciences Research, Division of Biomedical Statistics and Informatics, Mayo Clinic, Rochester, MN, USA; 3Department of Internal Medicine, Division of Hematology, Mayo Clinic, Rochester, MN, USA; 4Department of Urology, Second Division, Jilin University, Changchun, Jilin, People’s Republic of China
Correspondence: Mark R Litzow
Division of Hematology, Mayo Clinic, 200 First St, Rochester, MN 55902, USA
Tel +1 507-284-2511
Email [email protected]
Introduction: Obesity is a worldwide problem that is related to cardiac disease, thrombosis and cancer. However, little is known about the impact of obesity on the outcomes of adult acute lymphoblastic leukemia (ALL) patients.
Methods: We retrospectively evaluated a cohort of 154 newly diagnosed adult ALL patients between 1994 and 2011 at Mayo Clinic (Rochester). According to the World Health Organization (WHO) international BMI classification, patients were stratified as underweight, normal weight, overweight, and obese. For some analyses, patients were also stratified according to a two-sided non-obese or obese classification.
Results: The median follow-up time was 8.37 years. Obese patients were more likely to be women (p=0.024) and ≥ 60 years old (p=0.003). Five-year mortality rates were higher in obese patients than non-obese [HR 95% CI: 1.60 (1.03– 2.50) p=0.035]. This was also the case in subgroup analysis among T-cell patients although the number of patients was small [HR 95% CI: 5.42 (1.84– 15.98) p< 0.001]. There was no difference in mortality among the B-cell patients. After adjusting for baseline variables, the difference in mortality remained in several models. There was no difference in EFS or cumulative incidence of relapse rates between obese and non-obese patients among the overall population.
Discussion: In conclusion, our study suggests that adult ALL patients with obesity have lower survival rates, especially in T-cell ALL.
Keywords: acute lymphoblastic leukemia, obesity, overweight, B cell, T cell
Introduction
Compared with children, the long-term survival rate for adult patients with acute lymphoblastic leukemia (ALL) is inferior, with 5-year overall survival of only 30%-40% for patients younger than 60 years, less than 15% for patients older than 60 years and less than 5% for patients older than 70 years.1 Significant advances, however, have been made in the treatment of ALL in adults in the last decade. With current treatment regimens, long-term survival is achieved by approximately 80% of patients with Burkitt’s leukemia,2 50% of patients with B-cell ALL (B-ALL),3 50% to 60% of patients with Philadelphia chromosome (Ph)–positive ALL,4 and 50% to 60% of patients with T-cell ALL (T-ALL).5 Current risk classification strategies are based primarily on age as well as the analysis of genetic abnormalities of leukemic blasts and careful monitoring of each patient’s response to therapy,6,7 both of which are used to adjust therapy. However, certain clinical features, such as obesity, which are not typically used for risk stratification, are also associated with outcomes of acute leukemia.8,9 Studies addressing the impact of obesity on outcomes of adult patients with ALL are rare and have been reported in only one other series.9 Thus, we examined the effects of obesity on treatment outcomes of adult patients with ALL at our center.
Methods
Patients and Treatments
This was a retrospective, single-center study of adult ALL patients. We analyzed data from 154 consecutive eligible patients 18 years of age or older diagnosed with newly diagnosed ALL between 1994 and 2011 at Mayo Clinic (Rochester) who had at least five years of follow-up. Patients with mixed phenotype acute leukemia, Burkitt lymphoma, palliative treatment only and those without initial body mass index (BMI) data were excluded. Weight and height were measured by trained personnel. The chemotherapy dose was calculated on the basis of actual body surface area (BSA). The study was approved by the Mayo Clinic Institutional Review Board. All patients gave their consent for their medical records to be utilized for research purposes.
Patients were treated with chemotherapy regimens that were categorized into two broad categories,1) BFM-based regimens including the UKALLXII/E2993 protocol10 and the CALGB 9111 protocol11 or utilizing the 2) HyperCVAD12 regimen. For patients who were BCR-ABL1 positive, a tyrosine kinase inhibitor (TKI), including imatinib or dasatinib, was added when available.
The BMI was calculated as weight at diagnosis in kilograms divided by height in square meters – BMI (kg/m2) = Weight (kg)/[height (m)]2. According to the World Health Organization (WHO) international BMI classification, patients were stratified as follows: underweight (BMI < 18.5), normal weight (BMI 18.5 to <25), overweight (BMI 25 to <30), and obese (BMI ≥30). For some analyses, patients were more simply classified into two categories: non-obese (BMI <30) or obese (BMI ≥30).
Follow-up was complete on all patients with a minimum of five years of follow-up in all cases.
Criteria for Treatment Outcomes
The objective of the study was to evaluate the impact of obesity on the outcomes of adult patients with acute lymphoblastic leukemia. Outcomes include overall survival (OS), event-free survival (EFS), and relapse. OS time was defined as the time interval from diagnosis to death from any cause. EFS time was defined as the time interval from diagnosis to BMT, relapse or death whichever comes first. Relapse time was calculated from the date of diagnosis until the first relapse with death as the competing risk and censored at the time of BMT or the last follow-up for those alive and disease-free.
Statistical Analysis
Baseline characteristics were compared between BMI groups using Chi-Square test. OS and EFS were estimated for each BMI classification using the Kaplan–Meier estimator. The cumulative incidence of relapse in obese and non-obese patients, adjusted for the competing risk of death, was estimated using the cumulative incidence function and compared using Gray’s test. Cox proportional hazards models were used to estimate the effect of BMI on outcomes. BMI was included in all models as the main effect. Other covariates considered in the multivariable Cox models include patient age at diagnosis (18–40 vs 40–60 vs ≥60), type of ALL (B-cell vs T-cell), gender, hyperleukocytosis (white blood cell >30×109/L in B cell ALL, and >100×109/L in T cell ALL) at diagnosis, ECOG score, cytogenetic risk group (MRC-ECOG risk stratification: standard, intermediate, high), central nervous system involvement at diagnosis and type of induction regimen (HyperCVAD or BFM-based). Statistical analyses were performed using SAS Version 9.3 (SAS Institute, Cary NC, USA) and R Version 3.3.1 (R Foundation for Statistical Computing, Vienna, Austria). A p-value <0.05 was considered statistically significant and all statistical tests were two-sided.
Results
Patient Demographics
A total of 154 patients were analyzed in this study. The median age was 42.5 years (range 18–82 years). Median follow-up was 8.4 years. Overall, median BMI was 27.9 kg/m2 (range, 19.04–49.58). According to BMI WHO classification, among the 154 patients, 41 (26.6%) were classified as normal weight, 59 (38.3%) as overweight, and 54 (35.1%) as obese. There were no underweight patients. Ages varied among the BMI groups. Normal weight patients were younger than overweight patients, who in turn were younger than obese patients (P=0.002). Because there was no significant difference in all analyses between normal and overweight patients, they were grouped into one BMI category, ie, non-obese (101 patients, 65.5%). Obese patients were more likely to be women (p=0.024) and to be ≥60 years of age (p=0.003) (Table 1). Patient characteristics are summarized in Table 1. Forty nine of the 100 (49%) non-obese patients received a blood or marrow transplant (with the median time from diagnosis to BMT of 5.8 months (range 2–162 months)). Fifteen out of 54 (28%) obese patients received a BMT with the median time from diagnosis to BMT of 7.4 months (range 2–46 months).
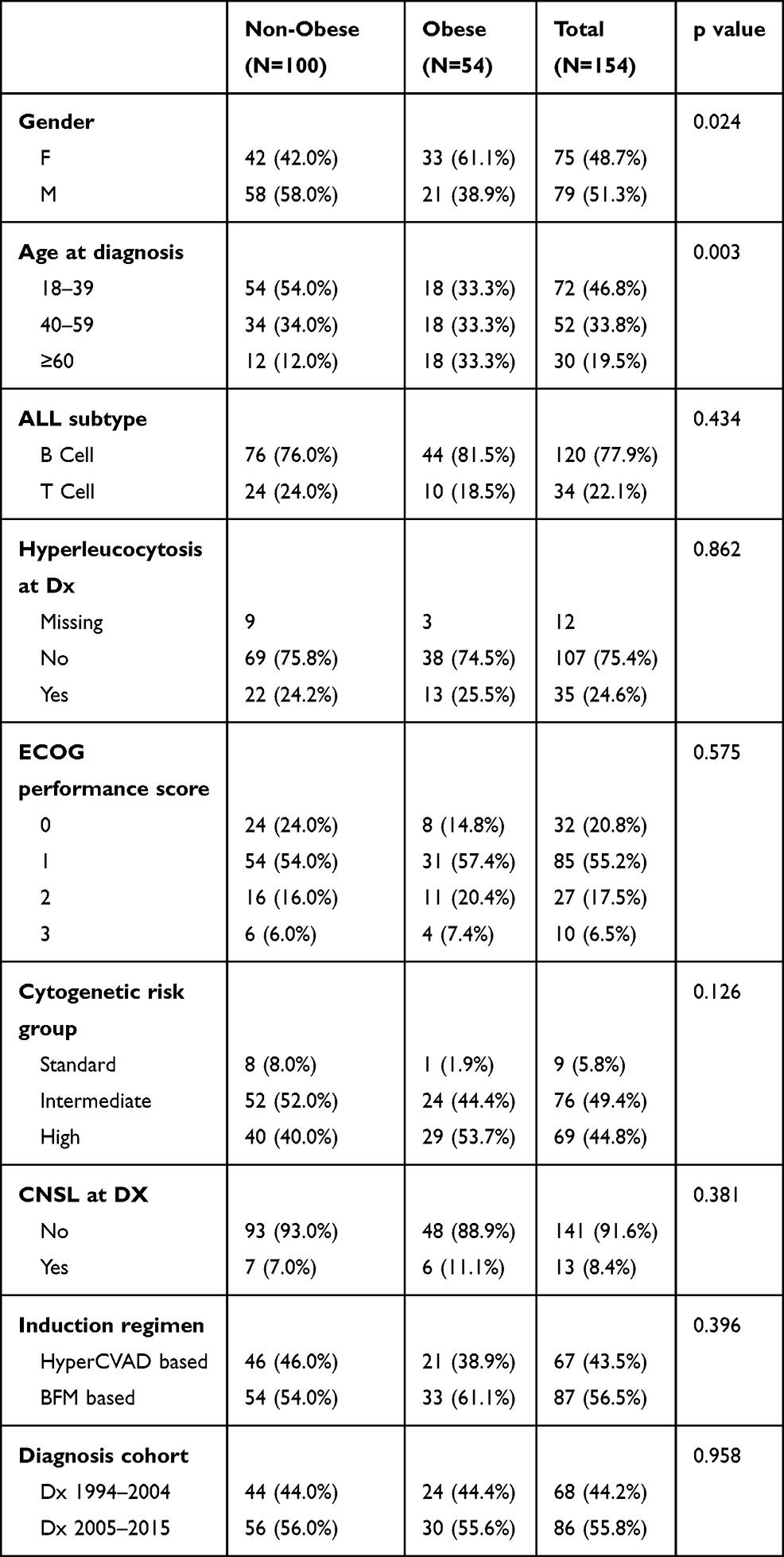 |
Table 1 Demographics by Obese/Non-Obese |
Relationship Between BMI and Survival: EFS and OS
The rate of complete remission and complete remission with incomplete count recovery (CR/CRi) did not differ between the obese and non-obese patients (Figure 1). The risk of mortality was higher in obese patients compared to non-obese patients [HR 95% CI: 1.60 (1.03–2.50) p=0.035 Figure 2A]. After adjusting for baseline variables, the difference in mortality remained in several models as shown in Table 2. There was no difference in EFS (Figure 2B) or relapse (Figure 2C) between obese and non-obese patients. In an additional analysis by ALL subtype, among T-ALL patients (obese n=10, non-obese n=24), obesity was associated with a lower OS [HR 95% CI: 5.42 (1.84–15.98) p<0.001] (Figure 3A) and with EFS, [HR 95% CI: 2.5 (1.00–6.21), P = 0.042] (Figure 3B). In contrast, no difference in OS or EFS was seen between obese (n=44) and non-obese (n=76) B-ALL patients (Figure 4A and B). Causes of death included relapse in 52 patients, non-relapse mortality in 27 patients (mostly related to post-transplant complications and was unable to be determined in 10 patients).
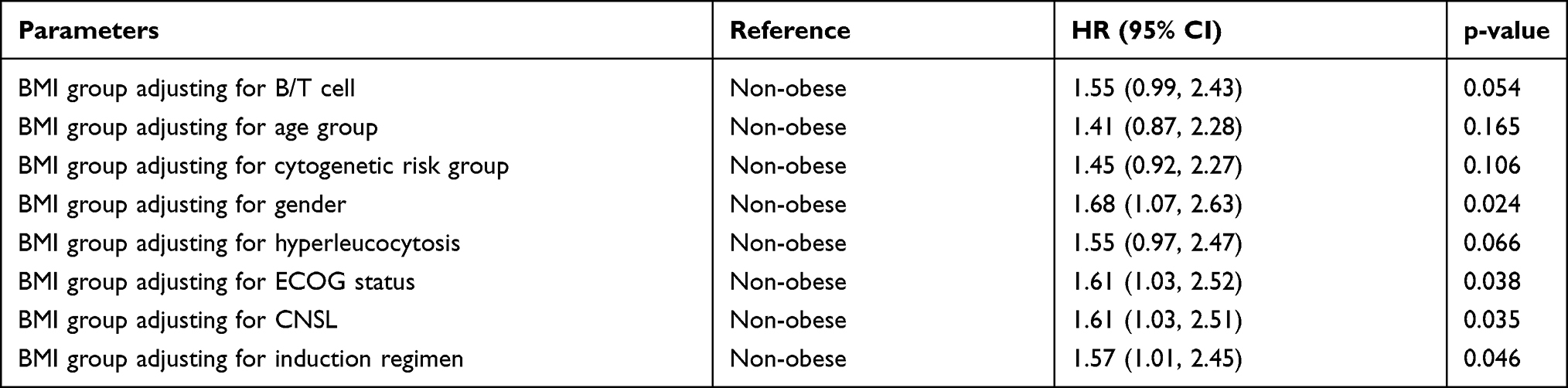 |
Table 2 Cox Proportional Hazards Models-Time to Death Comparing BMI Groups Adjusting for Baseline Variables |
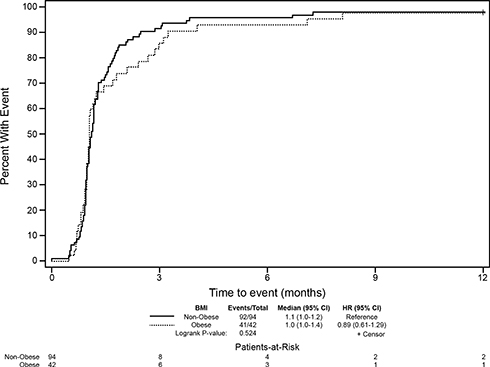 |
Figure 1 Time to complete response (1 year). |
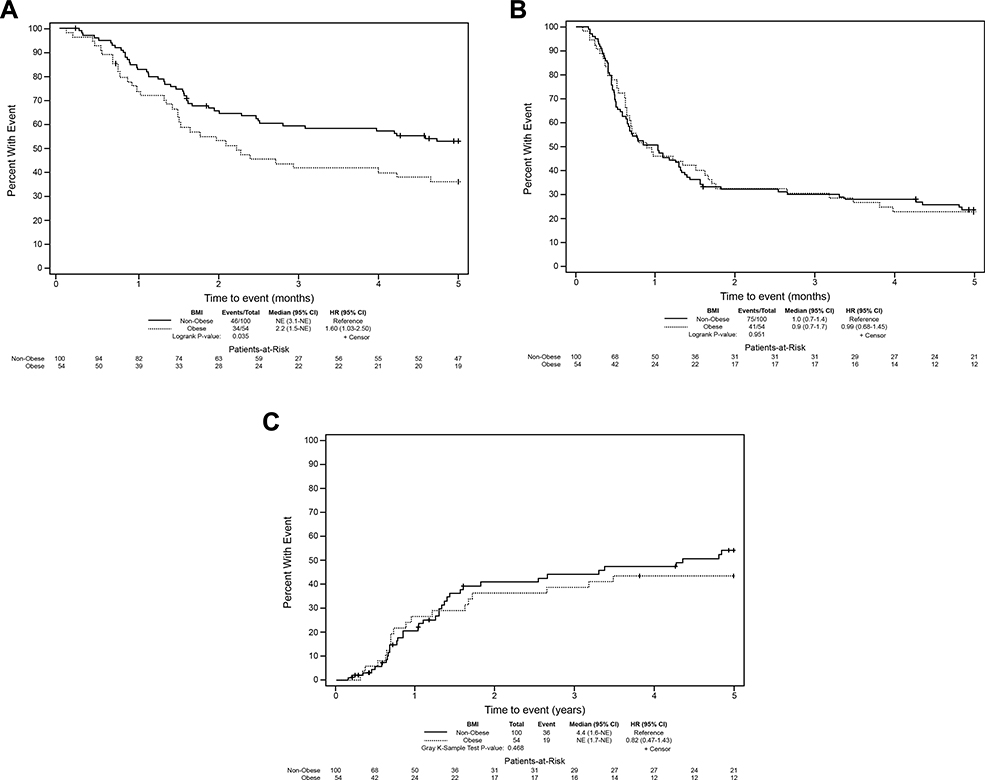 |
Figure 2 (A) Overall survival by BMI group (non-obese vs obese). (B) Event-free survival by BMI group (non-obese vs obese). (C) Relapse by BMI group (non-obese vs obese). Patients with prior BMT are censored. |
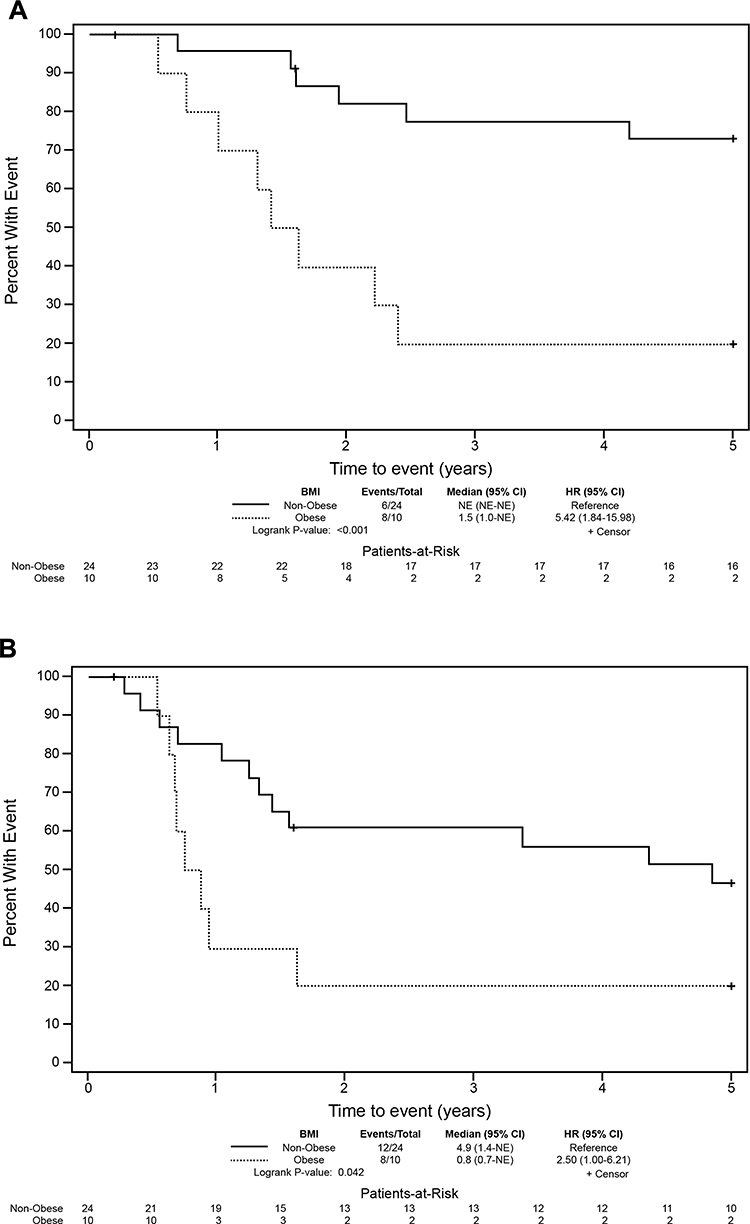 |
Figure 3 (A) T-cell ALL overall survival by BMI group (non-obese vs obese). (B) T-cell ALL event-free survival by BMI group (non-obese vs obese). |
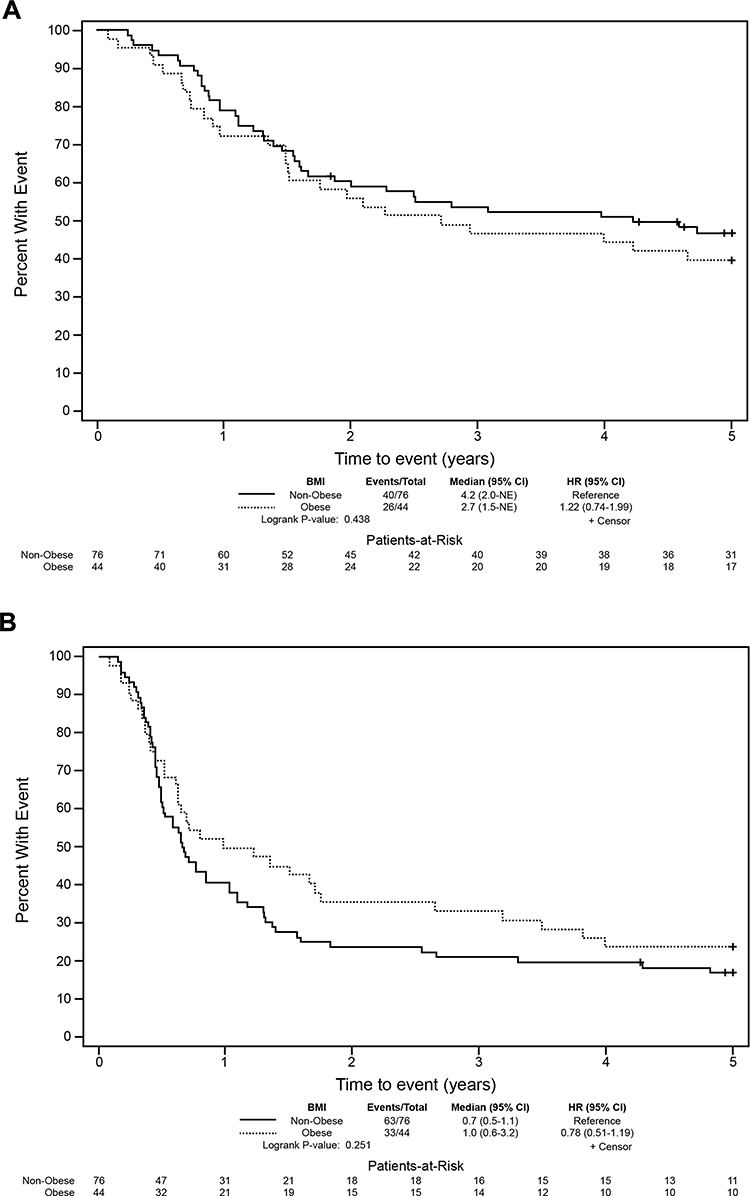 |
Figure 4 (A) B-cell ALL overall survival by BMI group (non-obese vs obese). (B) B-cell ALL event-free survival by BMI group (non-obese vs obese). |
Discussion
Obesity is now an alarming problem worldwide. Globally, the prevalence of overweight and obesity increased by 28% in adults and 47% in children between 1980 and 2013. Current estimates suggest that there are nearly 2.1 billion people in the world who are either overweight or obese.13 In the United States, data from the National Health and Nutrition Examination Surveys (NHANES) collected between 2011 and 2012 suggest that 35% of adults are obese.14 Aside from well-known long-term complications, obesity may also affect cancer incidence and cure.15 Here, we report the relationship between obesity and outcomes in adult patients with ALL and show that obese patients had a higher mortality overall with decreased overall survival that was not related to relapse.
There are scarce data in the literature about the impact of obesity on outcomes of adult ALL patients. The present study shows that obese patients with ALL have a higher risk of overall mortality. This adverse effect of obesity on mortality remained after adjusting for demographic and baseline clinical factors, while the rates of refractory leukemia, relapse and EFS were nearly identical across different weight categories. In the subgroup of patients with T-cell ALL, obesity was associated with a 5-fold increase in overall mortality. In our data, obese patients were older, which may explain the slight decrease in the adverse risk of obesity after adjusting for age group. Another retrospective analysis of two GIMEMA studies reached a similar conclusion with EFS in adults with BCR-ABL-negative ALL.16 However, a study from France did not find any relationship between BMI and outcome in adult ALL, but an increased BMI (>25) appeared associated with a better outcome in terms of leukemia free survival (LFS) (3-year LFS, 76% vs 13%; P = 0.005) and OS (3-year OS, 78% vs 41%; P =0.04) in T-ALL,9 which contradicts our findings. However, they were not able to confirm their results in a validation cohort of 211 T-ALL patients.
In pediatric ALL, reports of the effect of BMI on patient outcome are conflicting. A study from the Children’s Cancer Group (CCG) highlighted that obesity at diagnosis was an independent predictive factor of relapse and remission in adolescent patients.8 In contrast, a study from St. Jude Children’s Research Hospital found no differences in overall survival, event-free survival, or relapse rates among four BMI groups (underweight: BMI ≤ 10th percentile; normal: 10th to 85th percentile; at risk of overweight: BMI 85th to 95th percentile; overweight: BMI ≥ 95th percentile).17 Our current study suggests that adult obese patients with ALL have a worse survival, and suggests that their prognosis is unfavorable even in the context of contemporary supportive care.
In contrast, in adult, acute myeloid leukemia (AML) studies showed that obesity was not associated with worse survival or toxicities.18,19 However, in acute promyelocytic leukemia (APL), increasing BMI was strongly associated with worsening outcomes that were not seen with other subtypes of AML.20 Another study of children and adults with APL showed that overweight/obese patients had a significantly higher relapse rate and incidence of differentiation syndrome.21 Recently, a pooled analysis from four Cancer and Leukemia Group B (CALGB) (now the Alliance) studies also showed that obesity has significant prognostic value for DFS and OS in APL patients, but not for non-APL AML patients.22 These results may suggest a relationship between obesity-related metabolic mediators and the pathogenesis of APL.
There are limitations to our study. Due to the retrospective nature of this study, some data were missing for patients. Also, while BMI is the most widely used standard for classifying obesity, it may not be the best indicator of obesity in patients with chronic diseases because of its failure to distinguish between adipose tissue and lean muscle mass.23 Obesity is defined as an excess accumulation of body fat. To measure fat content in the body accurately is difficult, and no method is easily available for routine clinical use. Not only is the total amount of fat an individual carries important but also where the fat is distributed in the body. Fat in a central or upper body (android) distribution is most related to health risk. The most accurate way to measure central obesity is by magnetic resonance imaging or computer-assisted tomography scanning, but this approach is too expensive for routine use. Simple anthropometric measurements can be used, such as waist circumference. A waist circumference of greater than 1020 mm in men and 880 mm in women is a risk factor for insulin resistance, diabetes mellitus and cardiovascular disease.24 So it may be better if we can combine other indices such as waist circumference to identify obesity. Additionally, we were not able to determine the variations of BMI during patient follow-up.
Our study showed obese ALL patients had inferior survival compared to non-obese patients. Some data may explain this result. Typical obesity is characterized by hyperleptinemia,25 and current studies indicate the plasma and bone marrow leptin levels were significantly higher in ALL patients and there were positive significant correlations between bone marrow blast cells percentage, total white blood cells counts, serum lactate dehydrogenase and plasma leptin levels.26 These findings suggest the possibility that leptin might play a role in the pathophysiology of leukemia.27 However, studies on leptin receptor expression have not been consistent in vivo and in vitro. One study revealed that leukemic blasts from children ALL patients did not express the leptin receptor on the leukemia cell surface, whereas surrounding lymphocytes exhibited strong staining.28 In ALL cell lines, B-cell-derived cells exhibited very low, even absent leptin receptor expression, compared with relative higher expression of T-cell-derived cells, especially in Jurkat cells.29 This may indicate the leptin and its receptor play a different role in T versus B-lymphoblastic cells.
One important issue in regard to this topic is the impact of obesity on the pharmacokinetics and pharmacodynamics of chemotherapy drugs. There are limited data on this issue and the results available are conflicting, as in the case of doxorubicin. One earlier study suggested that doxorubicin had lower clearance and longer half-life in the most obese patients, resulting in a larger area-under-the-curve and more exposure, although the pharmacokinetics of doxorubicinol, an active metabolite, did not differ among patient groups.30 Another study did not come to the same conclusion.31 Pharmacokinetics is affected by multiple factors such as plasma protein binding capacity, water- or lipid-solubility of the compound, liver metabolism, and the function of the excretion pathway. Hijiya et al17 showed that intracellular levels of thioguanine nucleotides and methotrexate polyglutamates, as well as systemic clearance of methotrexate, teniposide, etoposide, and low-dose cytarabine, did not differ between different BMI groups of patients with pediatric ALL. Prospective pharmacokinetic studies of medications used in ALL, especially corticosteroids, cytarabine, anthracycline, cyclophosphamide, and methotrexate are needed in adult ALL patients. At our center, we do not modify the chemotherapy dosing on the basis of body surface area. It could be, however, that pharmacokinetic-guided dosing might reduce toxicity in those ALL patients with an abnormal BMI.
In conclusion, our study suggests that obesity is associated with lower survival rates in adult ALL patients, especially in T-cell ALL. Further studies would be warranted to confirm this finding and determine the underlying pathophysiologic mechanisms.
Acknowledgments
This work was supported in part by grants from the National Science Foundation of China (81302860, to Q.L.).
Disclosure
Dr Scott H Kaufmann reports grants from National Cancer Institute, Eli Lilly, Cyteir Therapeutics, Stand Up to Cancer/Entertainment Industry Foundation/AACR, and Minnesota Partnership for Biotechnology and Medical Genomics; non-financial support from ProLynx LLC, outside the submitted work. In addition, Dr Scott H Kaufmann has EP Patent No. 1682131 issued to Wyeth/Pfizer, US Patent No. 8530172 issued, US Patent No. 8729048 issued, US Patent No. 62/149873 pending, US Patent No. 62/312115 pending, and US Patent No. 62/668508 pending. The authors report no other conflicts of interest in this work.
References
1. Sive JI, Buck G, Fielding A, et al. Outcomes in older adults with acute lymphoblastic leukaemia (ALL): results from the international MRC UKALL XII/ECOG2993 trial. Br J Haematol. 2012;157:463–471. doi:10.1111/j.1365-2141.2012.09095.x
2. Hoelzer D, Walewski J, Dohner H, et al. Improved outcome of adult Burkitt lymphoma/leukemia with rituximab and chemotherapy: report of a large prospective multicenter trial. Blood. 2014;124:3870–3879. doi:10.1182/blood-2014-03-563627
3. Thomas DA, O’Brien S, Faderl S, et al. Chemoimmunotherapy with a modified hyper-CVAD and rituximab regimen improves outcome in de novo Philadelphia chromosome–negative precursor B-lineage acute lymphoblastic leukemia. J Clin Oncol. 2010;28:3880–3889. doi:10.1200/JCO.2009.26.9456
4. Fielding AK, Rowe JM, Buck G, et al. UKALLXII/ECOG2993: addition of imatinib to a standard treatment regimen enhances longterm outcomes in Philadelphia positive acute lymphoblastic leukemia. Blood. 2014;123:843–850. doi:10.1182/blood-2013-09-529008
5. Jain P, Kantarjian H, Ravandi F, et al. The combination of hyper- CVAD plus nelarabine as frontline therapy in adult T-cell acute lymphoblastic leukemia and T-lymphoblastic lymphoma: MD Anderson Cancer Center experience. Leukemia. 2014;28:973–975.
6. Giebel S, Krawczyk-Kulis M, Kyrcz-Krzemien S, et al. Could cytogenetics and minimal residual disease replace conventional risk criteria in adults with Ph-negative acute lymphoblastic leukaemia? Br J Haematol. 2009;144:970–972.
7. Van Dongen JJ, van der Velden VH, et al. Minimal residual disease diagnostics in acute lymphoblastic leukemia: need for sensitive, fast, and standardized technologies. Blood. 2015;125:3996–4009. doi:10.1182/blood-2015-03-580027
8. Butturini AM, Dorey FJ, Lange BJ, et al. Obesity and outcome in pediatric acute lymphoblastic leukemia. J Clin Oncol. 2007;25:2063–2069. doi:10.1200/JCO.2006.07.7792
9. Heiblig M, Elhamri M, Nicolini FE, et al. Effect of initial body mass index on survival outcome of patients with acute leukemia: a single-center retrospective study. Clin Lymphoma Myeloma Leuk. 2015;15(Suppl):S7–13. doi:10.1016/j.clml.2015.02.005
10. Ramanujachar R, Richards S, Hann I, et al. Adolescents with acute lymphoblastic leukaemia: outcome on UK national paediatric (ALL97) and adult (UKALLXII/E2993) trials. Pediatr Blood Cancer. 2007;48(3):254–261. doi:10.1002/pbc.20749
11. Larson RA, Dodge RK, Linker CA, et al. A randomized controlled trial of filgrastim during remission induction and consolidation chemotherapy for adults with acute lymphoblastic leukemia: CALGB study 9111. Blood. 1998;92(5):1556–1564.
12. Rytting ME, Jabbour EJ, O’Brien SM, et al. Acute lymphoblastic leukemia in adolescents and young adults. Cancer. 2017;123(13):2398–2403. doi:10.1002/cncr.30624
13. Fleming NGM, Robinson T, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–781. doi:10.1038/leu.2013.312
14. Ogden CL, Carrol MD, Kit BK, et al. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA. 2014;311:806. doi:10.1001/jama.2014.732
15. De Pergola G, Silvestris F. Obesity as a major risk factor for cancer. J Obes. 2013;23:1–10. doi:10.1155/2013/291546
16. Butturini A, Vignetti M, Gubbiotti S, et al. Obesity independently affects event free survival (EFS) in adults with BCR-ABL-negative acute lymphoblastic leukemia (ALL): a retrospective analysis of two GIMEMA studies. Blood. 2005;106 Abstract 520a.
17. Hijiya N, Panetta JC, Zhou Y, et al. Body mass index does not influence pharmacokinetics or outcome of treatment in children with acute lymphoblastic leukemia. Blood. 2006;108:3997–4002. doi:10.1182/blood-2006-05-024414
18. Medeiros BC, Othus M, Estey EH, et al. Impact of body-mass index in the outcome of adult patients with acute myeloid leukemia. Haematologica. 2012;97:1401–1404. doi:10.3324/haematol.2011.056390
19. Lee HJ, Licht AS, Hyland AJ, et al. Is obesity a prognostic factor for acute myeloid leukemia outcome? Ann Hematol. 2012;91:359–365. doi:10.1007/s00277-011-1319-8
20. Estey E, Thall P, Kantarjian H, et al. Association between increased body mass index and a diagnosis of acute promyelocytic leukemia in patients with acute myeloid leukemia. Leukemia. 1997;11:1661–1664. doi:10.1038/sj.leu.2400783
21. Breccia M, Mazzarella L, Bagnardi V, et al. Increased BMI correlates with higher risk of disease relapse and differentiation syndrome in patients with acute promyelocytic leukemia treated with the AIDA protocols. Blood. 2012;119:49–54. doi:10.1182/blood-2011-07-369595
22. Castillo JJ, Mulkey F, Geyer S, et al. Relationship between obesity and clinical outcome in adults with acute myeloid leukemia: a pooled analysis from four CALGB (alliance) clinical trials. Am J Hematol. 2016;91:199–204. doi:10.1002/ajh.24230
23. Warner JT, Cowan FJ, Dunstan FD, et al. The validity of body mass index for the assessment of adiposity in children with disease states. Ann Hum Biol. 1997;24:209–215. doi:10.1080/03014469700004942
24. Pi-Sunyer FX. Obesity: criteria and classification. Proc Nutr Soc. 2000;59:505–509. doi:10.1017/S0029665100000732
25. Farr OM, Gavrieli A, Mantzoros CS. Leptin applications in 2015: what have we learned about leptin and obesity? Curr Opin Endocrinol Diabetes Obes. 2015;22:353–359. doi:10.1097/MED.0000000000000184
26. Aref S, Ibrahim L, Azmy E, Al Ashary R. Impact of serum adiponectin and leptin levels in acute leukemia. Hematology. 2013;18:198–203. doi:10.1179/1607845412Y.0000000059
27. Han TJ, Wang X. Leptin and its receptor in hematologic malignancies. Int J Clin Exp Med. 2015;8:19840–19849.
28. Wex H, Ponelis E, Wex T, et al. Plasma leptin and leptin receptor expression in childhood acute lymphoblastic leukemia. Int J Hematol. 2002;76:446–452. doi:10.1007/BF02982810
29. Mouzaki A, Panagoulias I, Dervilli Z, et al. Expression patterns of leptin receptor (OB-R) isoforms and direct in vitro effects of recombinant leptin on OB-R, leptin expression and cytokine secretion by human hematopoietic malignant cells. Cytokine. 2009;48:203–211. doi:10.1016/j.cyto.2009.07.006
30. Rodvold KA, Rushing DA, Tewksbury DA. Doxorubicin clearance in the obese. J Clin Oncol. 1988;6:1321–1327. doi:10.1200/JCO.1988.6.8.1321
31. Sparreboom A, Wolff AC, Mathijssen RH, et al. Evaluation of alternate size descriptors for dose calculation of anticancer drugs in the obese. J Clin Oncol. 2007;25:4707–4713. doi:10.1200/JCO.2007.11.2938
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.