")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
The Impact of COVID-19 on Supplies of Routine Childhood Immunization in Oromia Regional State, Ethiopia: A Mixed Method Study
Authors Adilo TM, Endale SZ , Demie TG , Dinka TG
Received 18 August 2022
Accepted for publication 19 November 2022
Published 13 December 2022 Volume 2022:15 Pages 2343—2355
DOI https://doi.org/10.2147/RMHP.S386717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jongwha Chang
Takele Menna Adilo, Samson Zegeye Endale, Takele Gezahegn Demie, Temesgen Geleta Dinka
School of Public Health, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Takele Menna Adilo, Department of Epidemiology and Biostatistics, School of Public Health, St Paul’s Hospital Millennium Medical College, P.O. Box 1271, Addis Ababa City Administration, Addis Ababa, Ethiopia, Tel +251 911-134934, Fax +251112774787, Email [email protected]
Background: Globally, national immunization programs are at risk of disruption due to severe health system constraints caused by the ongoing Corona Virus Disease 2019 (COVID-19) pandemic.
Objective: To assess the impact of COVID-19 on the availability of supplies of routine childhood immunization in the Oromia Regional State in Ethiopia.
Methods: A health facility-based mixed-methods of study design was conducted. Both quantitative and qualitative data were collected using pre-tested questionnaires and key informant interview question guides, respectively. Descriptive statistics such as frequencies, means, and standard deviations were performed. Binary logistic regression analysis was employed to assess the associations between the COVID-19 pandemic and the availability of vaccine-related supplies at health facilities in study area. The qualitative data were analyzed using a thematic content analysis approach.
Results: Of the total 448 study participants, 214 (47.8%) reported that COVID-19 has disrupted childhood vaccines availability. A significant proportion of participants agreed with the disruption of BCG (62.1%), OPV (48%), IPV (40.4%), and PENTA (36.9%) vaccine availabilities. These findings were also supported with key informant interviews. Fear of not maintaining physical distance (71.4%) followed by government lockdown (68.1%) and inadequate supply by local providers/suppliers (62.4%) were the most frequently reported likely causes for the observed disruptions. A large proportion of participants (87.7% and 81.7%) reported disruptions in the supply of face masks and hand gloves, respectively. As to the binary logistic regression analysis, the study participants from hospitals were 1.72 (1.01, 2.68; 95% CI) times more likely to report the impacts of COVID-19.
Conclusion: Corona Virus Disease − 19 significantly disrupted the availability of supplies of childhood immunization in the Oromia region. The most disrupted vaccines and related supplies were BCG, OPV, IPV, PENTA, facemasks, and hand gloves. An effective vaccine supply management is crucial to prevent disruptions during pandemics such as COVID-19.
Keywords: availability of supplies, childhood vaccines, disruption, impact of COVID-19, Ethiopia
Introduction
Globally, vaccination prevents between 2 and 3 million deaths every year.1,2 It plays a crucial role in achieving 14 of the 17 Sustainable Development Goals (SDGs). 1,3–5 While vaccines save millions of lives each year, an estimated 1.5 million under-five children die from vaccine-preventable diseases (PVDs) due to low coverages in low- and middle-income countries in the globe.6,7
Although there has been unprecedented progress in preventing childhood mortality from infectious diseases through vaccination in this twenty-first century, the Corona Virus Disease 2019 (COVID-19) pandemic has disrupted routine childhood immunization for many vaccine-preventable diseases at the global, regional, and national levels.8 As reports indicated global vaccination coverage dropped from 86% in 2019 to 83% in 2020 and the proportion of children who completed the required childhood vaccinations was 69.21% in East Africa including Ethiopia.6,9
Worldwide, national immunization programs are at risk of disruption due to the severe health system constraints caused by the ongoing COVID-19 pandemic.10 The COVID-19 pandemic caused the most widespread and largest global disruption of routine childhood immunization services in 20206,11 In addition, maternal, neonatal, child, and sexual and reproductive health services were all impacted by the restrictions imposed by the government in response to COVID-19 including childhood immunization.12,13 A decline in vaccine coverage, in general, has been reported worldwide.14 According to a WHO and UNICEF estimate, globally at least 80 million children are at risk of Vaccines Preventable Disease due to the COVID-19 pandemic.14,15
The ongoing COVID-19 impact on routine child immunization is higher in lower-income countries with limited health-care resources and fragile health systems.16,17 For instance, the utilization of vaccination services at the national level decreased by 31% in Lebanon.18 Disruption of immunization services, even for brief periods, will result in increased numbers of susceptible individuals and raise the likelihood of an outbreak of vaccine-preventable diseases (VPDs) such as measles.19
The reasons for disrupted services vary. Some parents are reluctant to leave home because of restrictions on movement, lack of information, or because they fear infection with the COVID-19 virus. In addition, many health workers are unavailable because of restrictions on travel, or redeployment to COVID response duties, as well as lack of personal protective equipment. Transport delays of vaccines are exacerbating the situation.15,20,21
The access to and supply for vaccination are more likely to have been affected by the lockdown measures.21,22 The possible factors for the effects on the coverages and supplies of childhood immunization during the COVID-19 pandemic are fear of contracting severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) infection by the population due to interruptions in public transport or economic difficulties; and reduction in the health-care workers due to lack of protective equipment or reassignment to the assistance and management of patients affected by COVID-19.15
Vaccine stocks are running dangerously low in some low-income countries as supply chains have been disrupted by travel bans and canceled flights23 The pool of unimmunized children is expanding during the lockdown, leaving them susceptible to VPDs and also the occurrence of a disease outbreak at a population level. This highlights the need for mitigation, tailored to promote immunization and safe service delivery, as soon as possible.24 Improving immunization coverage requires creating a reliable supply of vaccines, training and incentivizing health workers, and strategies to improve the demand for immunization.25
In many developing countries, inefficiencies in the supply chain for the WHO’s Expanded Program on Immunization (EPI) vaccines are of concern. These inefficiencies result in thousands of people not being fully immunized and create a significant risk of disease epidemics.26,27
As the findings of a systematic review and meta-analysis study showed, only about 50% of 12–23 months old children in Ethiopia were fully vaccinated with significant disparities among regions.27,28
Understanding the level of immunization coverages and availabilities of childhood vaccine-related supplies is vital to designing appropriate interventions.28 The current immunization service models of COVID-19 pandemic require adaptation, including physical distancing measures, personal protective equipment, and good hygiene practices for infection control at the vaccination clinics.10 Continuous and timely assessment of vaccine coverages as well as availabilities of related supplies can play pivotal roles in responding to potentially volatile changes during the COVID-19 pandemic.29 Furthermore, the impacts of COVID-19 on the vaccine supplies of childhood vaccines in the Oromia region, Ethiopia are not yet studied. Oromia region is not only the largest region in Ethiopia in both surface area and population, but also with very diversified ethnic groups which makes it somewhat representative to the population of the country. The main aim of this study, therefore, was to assess the impact of COVID-19 on the availability of supplies of routine childhood immunization at the Oromia Regional State in Ethiopia.
Methods and Materials
Study Design and Setting
This health-facility-based mixed methods research design was conducted from May to June 2021 to assess the impact of COVID-19 on the availabilities of supplies of routine childhood immunization in the Oromia Regional State, Ethiopia. Oromia is the largest and the most populous region in the country. As to the national population and housing census report of 2007 of Ethiopia, the projected population of Oromia Regional State for the year 2020 was about 38.2 million, which comprises about 35% of the population of the country. Administratively, the Oromia region is divided into 21 zones 19 town administrations, and 317 Woredas (districts).31–33
Study Participants and Sampling
The study units were those purposively selected health institutions in ten zones of Oromia. We randomly selected health workers, who directly involve in vaccine supply chain management from 10 zonal health departments, 20-district health offices (DHOs), 7 hospitals and 23 health centers to participate in this study. The 10 zones selected to participate in this study among the 21 in Oromia Regional State were: 1) Arsi Zone, 2) Bale Zone, 3) East Shewa Zone, 4) East Wollega Zone, 5) Jimma Zone, 6) North Shewa Zone, 7) Southwest Shewa Zone, 8) West Arsi Zone, 9) West Shewa Zone and 10) Oromia Special Zone Surrounding Finfinne. These ten zones were believed to represent the whole region as they were selected from different areas in the region.
In addition, 450 health-care workers (15 randomly selected from each of the 7 hospitals and 23 health centers) were taken as the study participants. Primary and secondary data were collected from all the selected health institutions using both quantitative and qualitative data collection methods. Quantitative and qualitative data sources and methods were triangulated in order to increase the validity of the study.
For qualitative data collection, 60 key informant interviews (KIIs), ie, 6 KIIs from each of the selected 10 zones were conducted. The key informants were health workers who directly involved in the vaccine supply chain management, ie, zonal supply chain managers, district health offices supply chain managers, pharmacy heads, respective immunization unit heads, focal health workers in respective hospitals and HCs. The participants for KIIs were purposively selected using the criterion purposive sampling technique.
Data Collection and Quality Control
Primary and secondary data were collected from all the selected health institutions and their respective health workers using both quantitative and qualitative data collection methods. Structured questionnaires were used to collect the required primary quantitative data from all selected health workers in selected health institutions, ie, from seven hospitals and 23 HCs in the study area. The KII question guides were used to collect the KIIs. The guides included all the required information to assess the likely effects of COVID-19 on the availability of supplies of childhood immunization in the study area. The information generated from the KIIs helped to understand the problems in detail from each participant’s perspective.
Both data collection tools (questionnaire and KII question guide) were prepared in English and translated into local languages, Amharic and Afan Oromo. All data collection tools were pre-tested to assess their completeness in capturing all the variables required as per the specific objectives of the study. Quality assurance audits were carried out during the data collection process by field supervisors as well as the research team members by themselves. All the data collected, documents and reports were subject to regulatory audits and inspections without hindering confidentiality. Three days of training were given to both data collectors and supervisors by the researchers. The training included a discussion on the objectives of the study, contents of the data collection tools, data collection techniques, and maintaining the confidentiality of the responses. Moreover, the completeness of the filled questionnaires and checklists was checked by supervisors on a daily basis.
Data Management and Analysis
The collected quantitative data were first entered and cleaned using Epi Info version 7.2 statistical software and then exported to SPSS software version 25.0 for analyses. Various statistical methods like descriptive statistics such as frequencies mean and standard deviations (SDs) and also binary logistic regression tests were employed to identify the predictors for the impacts of COVID-19 on the availabilities of the supplies of childhood immunizations.
Qualitative data were first recorded using an audio recorder and then transcribed verbatim, translated, and exported into NVivo version 12.0 software for analysis. A thematic-content method was used for qualitative data analysis.
Results
Results of the Quantitative Data Analysis from the Survey
A total of 10 zones, 20 districts, and 30 health facilities in the Oromia Regional State of Ethiopia were included in this study. Of the 30 public health facilities, 7 were hospitals, and the remaining 23 were health centers. Fifteen health workers from each of the selected 30 health facilities participated in this study.
From the total 448 study participants, 214 (47.8%) reported that COVID-19 has disrupted the availability of childhood vaccines in their respective health institutions. Of those 214 respondents 198 (92.5%) reported that at least one of the childhood vaccine availability was disrupted in their respective health facilities due to COVID-19 pandemic.
A large proportion of participants, 62.1% (123/198) expressed the disruption of BCG vaccine whereas the lowest (29.8%) disruption was reported as the rotavirus vaccine. The rate of identifying BCG disruptions (69.1% or 38/55) was highest among hospital staff compared with that of health center staff (59.4% or 85/143). The rate of PENTA disruptions was about 9% higher among health centers (39.2%) than that of hospitals (30.9%). The rates for BCG and OPV disruptions were higher among health centers than hospitals. However, among the 214 study subjects who reported as childhood vaccines are disrupted due to the COVID-19 pandemic, 16 (7.5%) did not specify the kind of vaccine that was disrupted (Table 1).
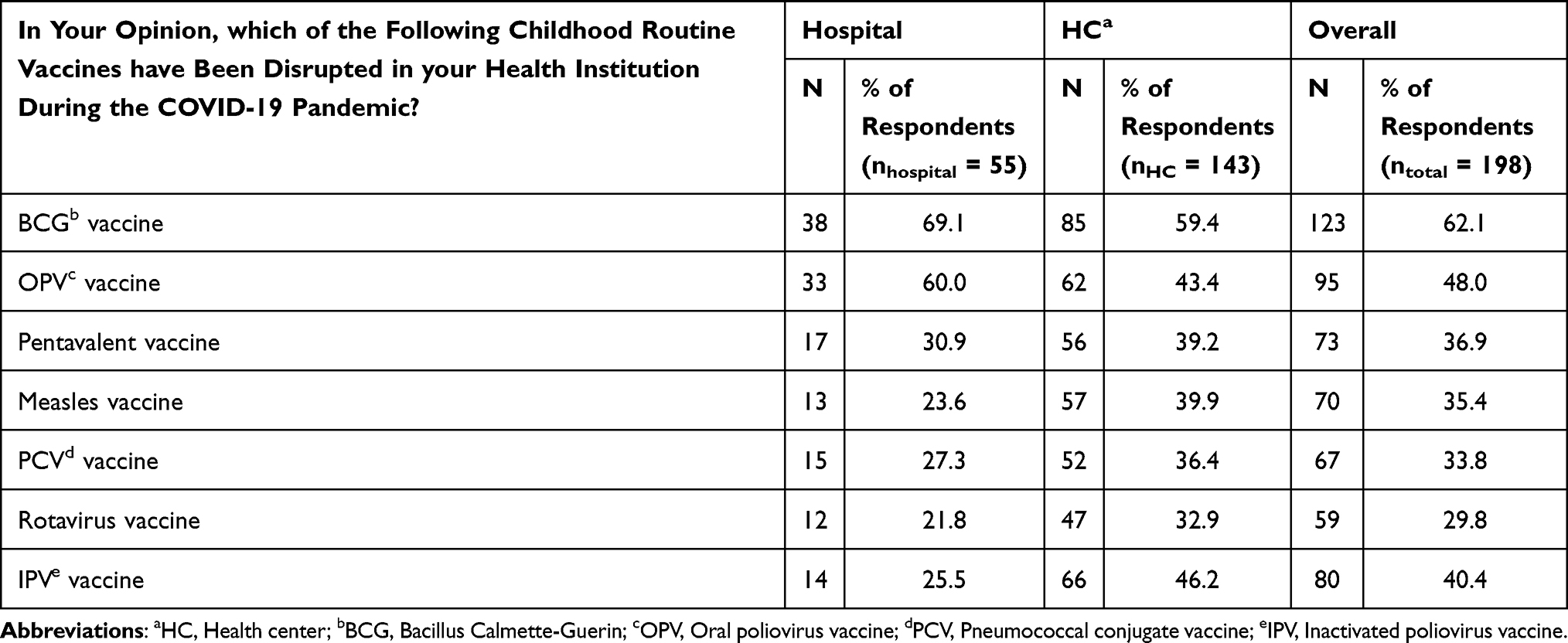 |
Table 1 Proportions of Childhood Vaccines Disrupted in Hospitals Compared to Health Centers, Oromia Region, Ethiopia, May 2021 (n = 198) |
Fear of not maintaining physical distance, 71.4% (152/213) was reported as the main reason for the disruptions during COVID 19 followed by government lockdown decision (68.1%), and inadequate supply by local providers/suppliers (62.4%). Distance of health institutions; poor cold chain management system; fear to maintain physical distances and government lockdowns were reported as more likely causes in hospitals compared to health centers. Whereas the inadequate number of health workers, inadequate supplies from local providers and international donors; and inability to purchase vaccines were reported as more likely causes in health centers compared to hospitals. The rate for poor supply management system was reported somewhat in equal proportions from both types of health facilities, ie, 34% (health centers) versus 35% (hospitals) (Table 2).
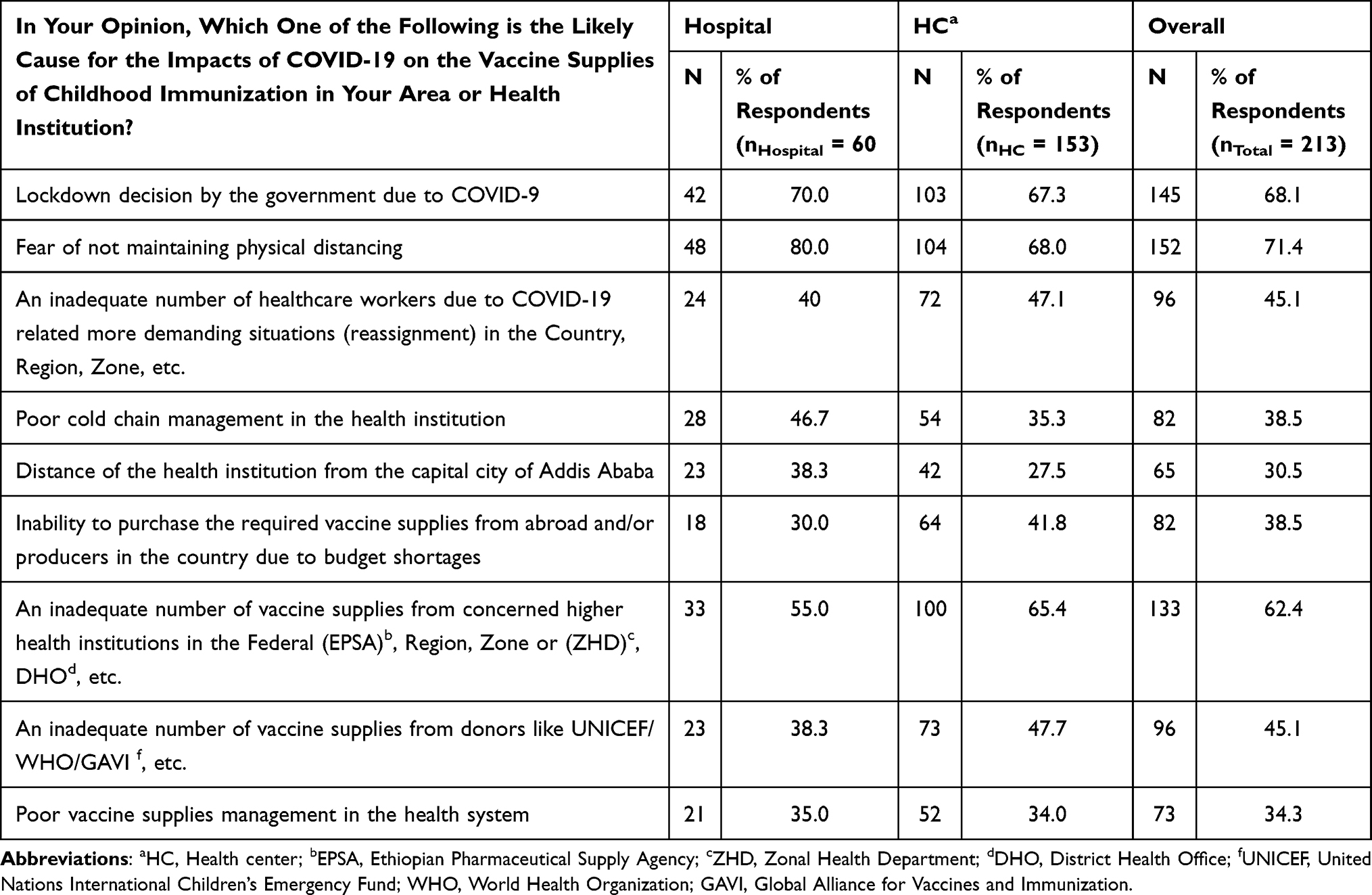 |
Table 2 Likely Causes for the Impact of COVID-19 on Childhood Vaccine Supplies in Hospitals Compared with That of Health Centers in the Oromia Region, Ethiopia, May 2021 (n = 213) |
Of those 284 (63.4% of the total study participants), who reported the disruption of at least one vaccine-related supply due to COVID-19, a large proportion of participants, 87.7% (249/284) reported disruptions of face masks, followed by hand gloves (81.7%). Except for face masks, the percentages of disruptions for other vaccine-related supplies were higher in health centers compared to hospitals. Except for syringes and needles, where the reported agreement was lower in proportion, the proportion of participants who agreed on disruptions of other vaccine-related supplies was high. However, a very insignificant number of participants responded that they did not know (Table 3).
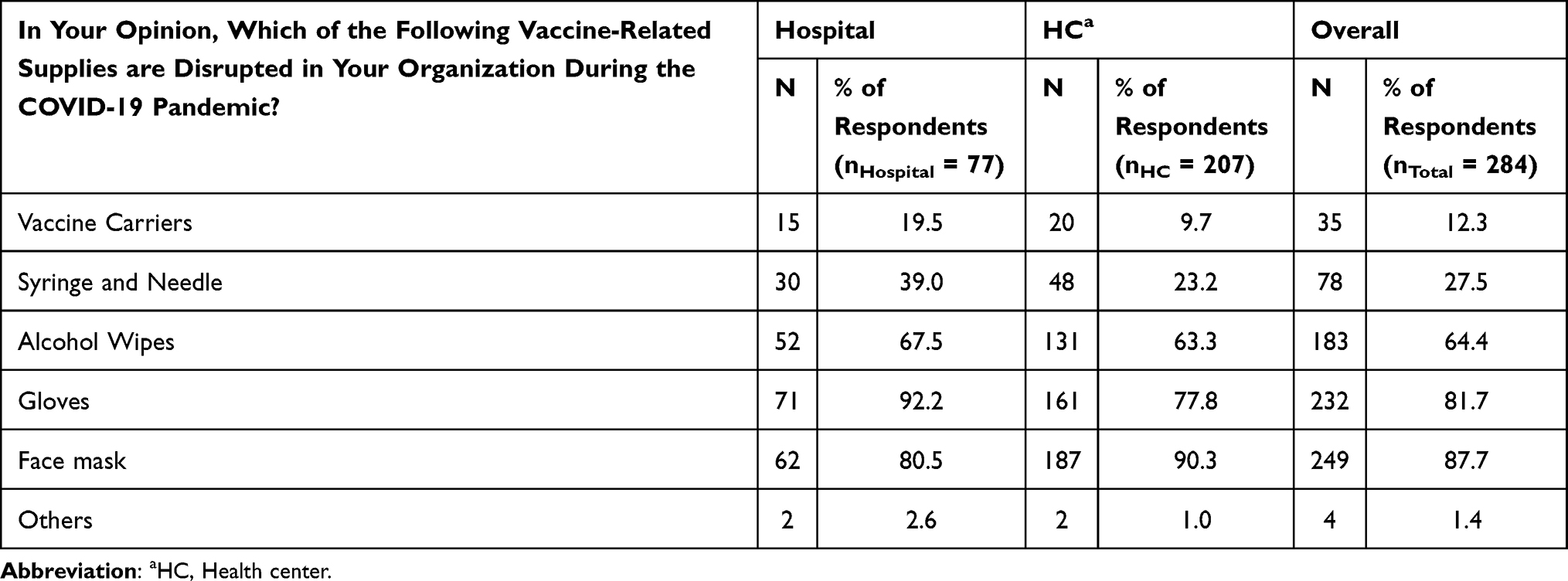 |
Table 3 Percentages of Vaccine-Related Supply Disruptions as Reported by the Study Participants from Selected Hospitals Compared to Health Centers in the Oromia Region, Ethiopia, May 2021 (n = 284) |
Fear of not maintaining physical distance, 67.3% (179/278) was the main likely cause reported by the study participants, followed by government lockdown (64.4%). Except for the rate for inadequate health workers, which is similar in both institutions 39.3% (health centers) versus 39.0% (hospitals), the rate of likely cause of the impacts of COVID-19 on the availability of childhood immunization-related supplies was higher in hospitals compared with health centers (Table 4).
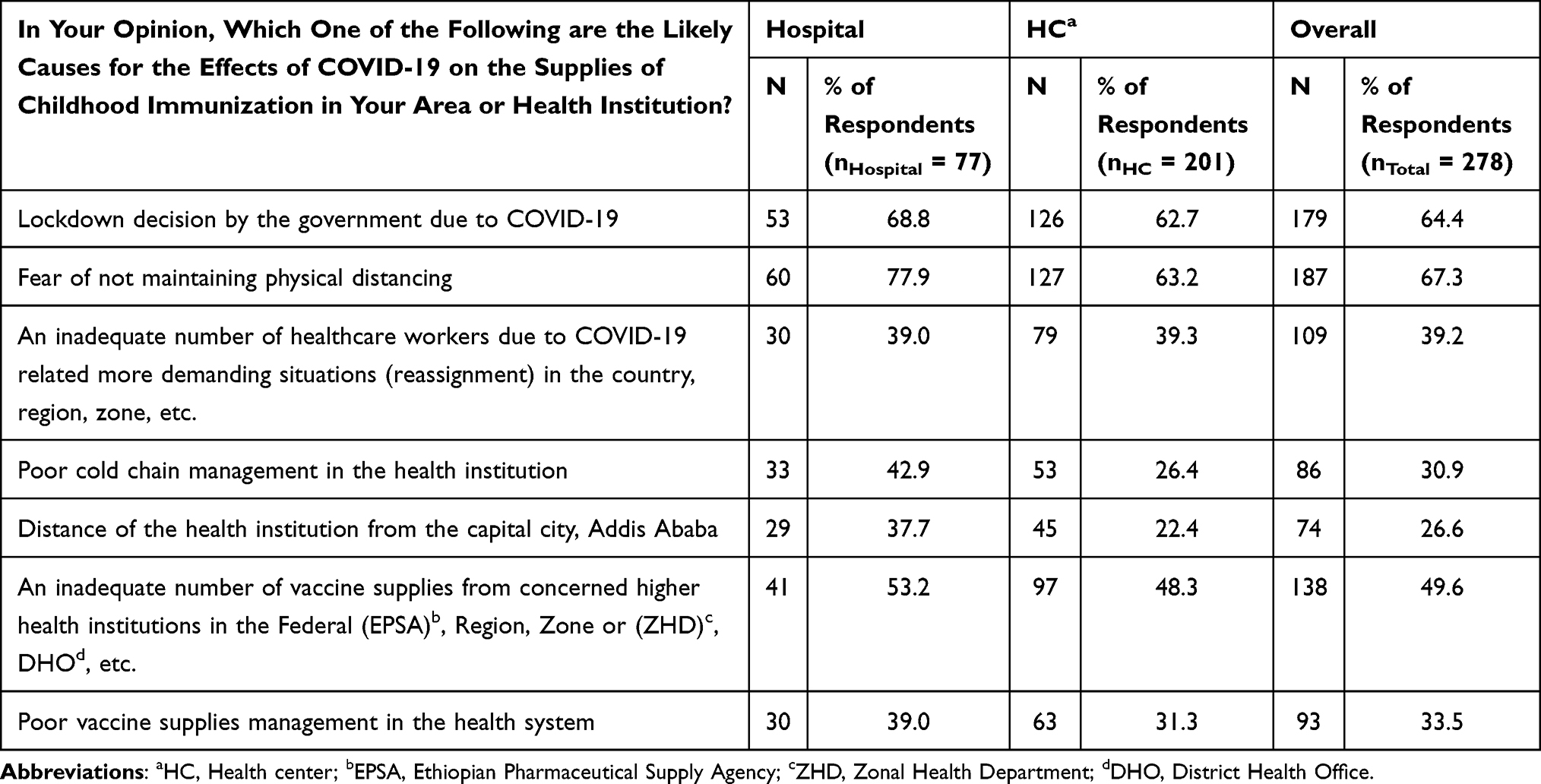 |
Table 4 Likely Causes of the Impact of COVID-19 on Childhood Immunization at Hospitals Compared with That of Health Centers in Oromia Region, Ethiopia, May 2021 (n = 278) |
In order to look for the associations between the impacts of the COVID-19 pandemic and the availabilities of childhood vaccines and vaccine-related supplies in the study area independently with the type of health institutions, a binary logistic regression model was employed. Results of the binary logistic regression revealed that types of health institutions have shown statistically significant association with the impact of COVID-19 on childhood vaccines and vaccine-related supplies (p-value <0.05).
Participants working in hospitals were 1.72 times more likely than health center staff to report the impacts of COVID-19 on childhood vaccine availability (COR = 1.72; 95% CI, 0.01, 2.68) at p-value 0.016. That was to say the impacts of COVID-19 on disrupting childhood vaccine supplies increased by 72% in hospital settings than health centers. Moreover, those study subjects working in hospitals are 1.98 times more likely than health center staff to report the impacts of COVID-19 on disrupting vaccine-related supplies (COR = 1.98; 95% CI, 1.20, 3.26) at p-value 0.007. That was to say the effects of COVID-19 on disrupting vaccine-related supplies increased by 98% in hospitals compared to health centers. The chance of vaccine-related supplies in hospitals being affected by COVID-19 was almost double compared to health centers.
Findings of Qualitative Data Analyses from KIIs
Main Theme and Sub-Themes
The main theme identified during the qualitative data analyses was changes during COVID-19 and it comprises seven sub-themes including stock status for both vaccines and related supplies, most affected vaccines and related supplies, demand for immunization, and reasons (likely causes) for decreased number of vaccines and related supplies during COVID-19 pandemic. The findings are summarized here below.
Changes in Childhood Vaccines and Related Supplies During COVID-19 and the Likely Reasons
Some KIs reported that COVID-19 had an effect on immunization services in the first three months, but it has had no effect on the stock status of the vaccines. Children dropped out or defaulted from PENTA 3 and Measles due to parents’ fear of contracting COVID-19.
…During the early COVID-19 outbreak, children have defaulted or dropped out of immunization due to fear of infection by the community. Specifically, Measles and PENTA 3 dropout was observed.
The findings of KIIs also showed that there is variation in responses to the question “whether there have been changes in demand for immunization during COVID-19”. Most of KIs observed a decrease in demand for immunization from the mother’s (parents) side because of fear of contracting COVID-19 especially at the beginning of the pandemic and during the lockdown. In addition, during the lockdown health professionals were also not available at health facilities to provide services. But this happened for only a very brief period at the start of the lockdown. This change in demand affected the number of vaccines to order because monthly vaccine ordering depends on the number of vaccines consumed and stock at hand. Since less is consumed at the beginning of the COVID-19 pandemic and lockdown, fewer vaccines were ordered as one of the KI described below:
…. There was a decline as compared to the regular service. The vaccine users said that they feared coming to the town after everything was locked down. The number of vaccinated children and the number of vaccines decreased as compared to the regular one. Hence, we request the minimum amount as we had enough supply balance on hand.
Because of a range of responses against the COVID-19 pandemic, the observed effects of COVID-19 and the demand for childhood vaccines were not significant. Some of the KIs stated that both the Federal and Regional Governments continued providing the support they needed during the pandemic and it had no effect. Some others said that the COVID-19 pandemic has affected immunization services. Fear of the health workers against contracting COVID-19 has an impact on forecasting and ordering of supplies. Fewer children were receiving the service due to the COVID-19 pandemic as reported by some of the KIs. Among the likely causes are fear of parents contracting the infection from health institutions or fear of not maintaining physical distance, lockdown decisions by the government, and few number of health professionals working at health institutions due to COVID-19- related more demanding situations in the country, region or zone. Children could not continue their vaccines according to their schedule as their families have a high fear of COVID-19 infection. In addition, they have also stated that lack of transportation for vaccines and the acquisition of expired or near to expire OPV vaccines. There has been high wastage, shortage of budget to obtain the required amount of vaccines, lack of enough functional refrigerators, and less amount of vaccines received from donors or EPSA.
…Fear of physical distancing was one of the first contributing factors at the time [during the early stages of COVID-19]. The community is afraid to meet with health professionals because they believe COVID-19 can easily be contracted from health professionals. The other is a health professional-related challenge, and there was an inadequate number of health workers because they were afraid of the disease and were absent from work…
Additionally, an MCH coordinator from Chancho Hospitals reported decreased demand or client flow than the interruption of vaccines and immunization supplies by COVID-19.
No effects on vaccine supplies but client flow to hospital decreased which resulted in decreased demand for vaccines and supplies and this, in turn, caused a high number of defaulters.
Similarly, a KI from Olenchite HC reported a decrease in demand and service utilization.
The number of children taking the vaccines during the first outbreak of COVID-19 greatly decreased as it had a great impact on this service. Accordingly, the number of vaccine requests decreased. However, there was no problem related to the supply and the vaccination service.
To sum up, most of the KIs reported that there were changes in ordering, receiving, and using both vaccines and related supplies as well as in immunization service coverages in the Oromia region during the COVID-19 pandemic especially at the beginning of the pandemic mainly due to the national lockdown decision.
Some of the KIIs of this study reported that there was no shortage of vaccines or related supplies, such as personal protective equipment (PPE), glove, disposable gloves, and face masks during COVID-19. This can be supported with the following response by a KI an EPI focal person from Oromia Special Zone Surrounding:
Yes, COVID-19 has made society not come and use the services. The problem was not with the supply; there was low number of clients coming to health facilities to get immunization service. Moreover, there was a problem with the supply of COVID-19 personal protective equipment for the staff.
Moreover, a KI from East Shewa ZHD expressed the impact of COVID-19 pandemic on childhood immunization services as stated below:
Yes, there were huge challenges regarding immunization during lockdown due to the COVID-19 pandemic. Healthcare professionals were not fully serving in health facilities. The immunization demand (the number of children) declined to some extent though it needs to refer to the actual data. The decreased number of children directly influences the number of vaccines to be requested because we initiate order based on the balance of vaccine at hand.
Moreover, some key informants who were working at the district level of health-care delivery systems like Toke Kutaye and Adaba, districts reported that there were interruptions or shortages of vaccine such as BCG, polio, PCV, Pentavalent, and Rota, particularly during the first months of COVID-19 case reporting. In support of these realities, the following expressions can be taken from a KI from Toke Kutaye, Dodota, and Lume districts health offices, respectively.
There was no interruption to vaccine supplies before the COVID-19 pandemic. But during the COVID-19 emergency, there was a one-month interruption to OPV, PCV, and Penta vaccines.
It has effects on immunization; it leads to drop-out of children from immunization. Particularly, polio and BCG vaccination were highly affected.
There was a shortage of polio vaccine for two months which created unexpected re-visit of children due to interrupted vaccination schedule. Children couldn’t continue their vaccine according to their schedule as their family has high fear of COVID-19 infection. The stored vaccines expired, resulting in high levels of wastage.
A key informant from Bekoji HC reported disruption of the Penta vaccine, “It didn’t result in significant impacts. But the supply of Penta vaccine was seriously influenced due to stockout of Penta at a higher level.” A KI from Obora HC also reported BCG and Penta as the most impacted vaccines
COVID-19 had an effect. There was a condition when some vaccines become ‘overstock’ while others become ‘understock’. The most impacted vaccines were ‘BCG’ and ‘Penta’. We had asked for them repeatedly, but we couldn’t get them for two to three rounds.
Furthermore, the disruptions of vaccine-related supplies for a few months during the early outbreak of COVID-19 were reported by KIs from some HCs. For instance, a KI from Tulubollo HC said, “There was a shortage of immunization supplies such as sanitizer, examination gloves, and alcohol” while a KI from Ejere HC added, “Yes, there was an interruption to vaccine supply as a whole at the beginning of the pandemic.”
As reported by the KIs from multiple HCs, there are shortages of supplies like gloves and face masks, alcohol swabs, needles, cold box, and refrigerators. Serious scarcities of vaccine carriers, pads, and refrigerators were also reported from a few HCs. The greatest logistical challenge of the region for childhood immunization was shortages of refrigerators as reported by some KIs.
Discussions
The Impacts of COVID-19 on the Availability of Vaccine Supplies in the Region
This health-institution-based mixed methods study design was conducted among selected health workers from different public health institutions in the Oromia regional state of Ethiopia to assess the impacts of COVID-19 on the availability of supplies of childhood immunization in the region. Nearly forty-eight percent (47.8%) of the study participants' health workers from the total 448 reported that the COVID-19 pandemic has disrupted the availability of vaccine supplies at their respective health institutions. The above finding on the childhood vaccines disruptions in the study area is in agreement with the findings of other sources of data of the same study aimed at triangulating the main findings.
A large proportion of participants, 62.1% responded as BCG vaccine availability was disrupted whereas the lowest (29.8%) responded as the Rota vaccine was disrupted. Except for BCG, disruption of other vaccines is below 50%. The rate of BCG disruptions (69.1%) reported from hospitals was higher than that of the health centers (59.4%). However, the rate of PENTA disruptions was about 9% higher among health centers (39.2%) than that of hospitals (30.9%). The rates for BCG and OPV disruptions were higher among hospitals than health centers, while they were the opposite for the other vaccines.
The above findings regarding the impacts s of COVID-19 on the supplies of child immunizations were supported by the reports from previous studies conducted elsewhere. Various studies conducted in different countries reported that one of the consequences of the COVID-19 pandemic is its impact on the delivery of important health services, including immunizations and vaccine supplies to populations residing in low- and middle-income countries.33,34 As it was reported the national immunization programs globally are at risk of suspension or disruption due to the severe health system constraints caused by the ongoing COVID-19 pandemic and the physical distancing measures to mitigate the outbreak.10 The routine immunization services faced stark challenges in 2020, with the COVID-19 pandemic causing the most widespread and largest global disruption in recent history.9 Furthermore, in the era of COVID-19, as that in many social services, the routine childhood immunization service in Ethiopia is believed to have serious challenges due to shortages of basic supplies. The COVID-19 pandemic continues to disrupt essential health services in more than 90% of countries across the globe.11
The Impacts of COVID-19 on the Availability of Vaccine-Related Supplies in the Region
As the survey data findings revealed the most disrupted vaccine-related supplies for which the disruption was agreed by the study participants were, face masks (85% of participants agreed), hand gloves (79.5%), alcohol wipes (62.7%), and syringes and needles (26.7%). These findings are also in agreement with the qualitative data results of our study as shown in the following expressions of the KIIs participants from various selected health institutions. For instance, an EPI focal person from Dodola General Hospital reported:“Yes, it caused a big challenge, due to lack of timely requesting the supplies. All supplies were impacted”; A key informant from Tulubollo HC said:“There were shortages of immunization supplies such as sanitizer, hand gloves, and alcohol”.
A key informant from Ejere HC also said the following, “Yes, there was an interruption to vaccine supplies as a whole at the beginning of the pandemics.”A key informant from Olanchite hospital reported, Vaccine supplies like PPE, gloves and masks are not received. Especially, there are critical shortages of disposable gloves and face masks. A key informant from Jawe HCs also said:
With regard to the immunization supplies (alcohol wipes, vaccine carriers, gloves, face masks, etc.), the major problem is the inability to get these supplies when needed.
The above findings that showed the impact of COVID-19 on childhood vaccine-related supplies are in agreement with the reports from GAVI. As GAVI reported, fear of contracting SARS-CoV-2 infection by the population or due to interruptions in public transport or to economic difficulties and reduction in the health-care workers who can be employed in vaccination services due to lack of protective equipment are factors for the decrease in childhood immunization during COVID-19 pandemic.15
As reported by the KIs from different HCs, there are shortages of supplies like gloves and face masks, alcohol swabs, needles, cold box and refrigerators. Serious scarcities of vaccine carriers, pads, and refrigerators are also reported from a few HCs. In general, improving immunization coverage requires creating a reliable supply of vaccines and immunization supplies, trained and incentivized health workers, and strategies to improve the demand for immunization.25
A successful vaccination program can only occur when vaccine-related supplies are present at the same time. This implies the importance of each of them as the absence of any one of the supplies immediately results in missed vaccination opportunities. Moreover, among the required childhood vaccine-related supplies syringes, needles, vaccine carriers, ice packs, and hand gloves and sanitizers can be taken as mandatory.
The Likely Causes for the Impacts of COVID-19 on the Availability of Vaccine and Vaccine-Related Supplies in the Region
As the survey data findings showed among the 292 respondents who reported that COVID-19 disrupted the availability of vaccine-related supplies in their institution, 95% reported at least one likely cause for the observed impacts of COVID-19 on childhood immunization. Fear of not maintaining physical distance (67.3%) was the main likely cause reported by the study participants, followed by government lockdown (64.4%). Inadequate numbers of vaccine supplies and health-care workers were also among the significant causes that played roles for the observed impacts of COVID19 on the supplies of childhood vaccines as this study findings showed.
The above reported likely causes are supported by the findings from the qualitative data analysis or KIIs of this study as can be seen from the following expressions. A study participant said
…Fear of physical distancing was one of the first contributing factors at the time [during the early stages of COVID-19]. The community is afraid to meet with health professionals because they believe they could easily contract COVID-19 from health professionals. The other is a health professional-related challenge, and there was an inadequate number of health workers because they are afraid of the disease and are absent from work…
The greatest logistical challenge of the region for childhood immunization was shortages of refrigerators as reported by some KIs.
The above findings can be supported by the following previous findings that were reported from elsewhere in the globe. A study on estimating global and national disruptions to routine childhood vaccine reported that the national immunization programs globally are at risk of suspension or disruption due to the severe health system constraints caused by the ongoing COVID-19 pandemic and the physical distancing measures to mitigate the outbreak.11
Various other studies from different countries such as Pakistan showed disrupted access to maternal and child health services including immunization services in countries with strict lockdowns.6,8,29,35,36
It was also reported that childhood immunization in Africa was directly affected by the lockdown as it discourages caregivers from visiting health facilities for routine immunization. Vaccine logistics and the supply chain are interrupted. Furthermore, community mobilization activities would decrease which in turn would cause a decrease in mass vaccination campaigns.13 The pool of unimmunized children are expanding during the lockdown, leaving them susceptible to VPDs and also occurrence of disease outbreak at a population level. This highlights the need for mitigation, tailored to promote immunization and safe service delivery, as soon as possible.13 The access and supply side of vaccination was more likely to have been affected by the lockdown measures.21,22
Fear of contracting SARS-CoV-2 infection by the population or due to interruptions in public transport or to economic difficulties and reduction in the health-care workers who can be employed in vaccination services due to the lack of protective equipment or relocation to the assistance and management of patients affected by COVID-19 are factors for the decrement in childhood immunization during COVID-19 pandemic.6
Lastly, as the findings of this study revealed, the chance for the impacts of COVID-19 on childhood vaccines and related supplies in hospitals was higher compared to health centers in the Oromia Region. This could be due to the reason that the immunization service is primarily provided at health centers and health post levels in the Ethiopian health-care delivery system. Consequently, the health centers and health posts have better chances to get more vaccines and related supplies compared with that of the hospitals. In addition, as some of the hospitals were supposed to be COVID-19 centers during the first few months of the outbreak, the probability of health-care workers’ temporary transfers from immunization service units of the hospitals to the newly established COVID-19 centers could be the likely reason for the observed more impacts of COVID-19 on the vaccine and related supplies disruptions in hospitals comparing to health centers in the study area.
Limitations of the Study
This study is not without limitations. First, to the knowledge of the researchers, this is the first innovative research. Thus, it was so difficult to find the results of any other similar studies done elsewhere, in order to compare and contrast the current findings with those previously reported or known elsewhere; and that might be considered as a limitation that may lead us to use the findings with care. Secondly, the private health institutions and health workers in the training and education settings were not included due to resource constraints. Moreover, the cross-sectional study is not strong to identify the true causality or effects of COVID-19 on the supplies of childhood immunization in the study area and that might be also taken a limitation. Nevertheless, to bridge the gap, it was triangulated with data from KIIs. We also addressed almost half of the zones in the region. Furthermore, the quantitative and qualitative data sources and methods were triangulated in order to increase the validity of the findings.
Conclusions
The impacts of COVID-19 on the vaccine and related supplies of childhood immunization at the Oromia region in Ethiopia became evident. As the findings of this study showed, nearly half of the study participants reported that COVID-19 affected vaccines and related supplies of childhood immunization. Even though there were variations from health facilities to other health facilities as reported by KIs, the most affected vaccines were BCG, OPV, IPV, PENTA, and measles. Whereas, the facemasks, hand gloves, alcohol wipes, and syringes and needles were the most frequently reported vaccine-related supplies that were affected by COVID-19 in the region. Moreover, the fear of community and health-care workers not to be infected by COVID-19, the lockdown decision by the government, inability to purchase adequate supplies from designated organizations, and poor supply chain management were the reported likely causes for the observed impacts of COVID-19 on supplies of childhood vaccines. Hence, the health institutions in the study region and their stakeholders should strengthen the current interventions against COVID-19. There is also a need for large-scale or nationwide studies with more representative sample sizes to consolidate much needed empirical evidence on COVID-19 impacts among health institutions in the country.
Abbreviations
BCG, Bacillus Calmette-Guérin; COVID-19, Corona virus Disease 2019; DHOs, District health offices; DPT, Diphtheria-Tetanus-Pertussis Vaccine; EDHS, Ethiopian Demographic and Health Survey; EPI, Expanded Program on Immunization; EFY, Ethiopian Fiscal Year; ETB, Ethiopian Birr; FGDs, Focus group Discussions; FDRE, Federal Democratic Republic of Ethiopia; FMOH, Federal Ministry of Health; HIMS, Health Management Information System; HPV, Human Papilloma Virus; HPs, Health Posts; IRB, Institutional Review Board; KIs, Key informant(s); KIIs, Key informant interview(s); MMR, Measles, Mumps, Rubella; MPH, Masters of Public Health; NOK, Norwegian Kroner; OPV, Oral Polio Vaccine; PHC, Primary Health Care; PHCU, Primary Health Care Unit; PCV, Pneumococcal Conjugate Vaccine; PPE, Personal Protective Equipment; RCN, Research Council of Norway; SARS, Severe Acute Respiratory Syndrome; SD, Standard Deviations; SPHMMC, St. Paul’s Hospital Millennium Medical College; SPSS, Statistical Package for Social Sciences; VPD, Vaccine preventable diseases; WHO, World Health Organization; ZHDs, Zonal health department(s).
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Ethical clearance and approval of the research protocol was obtained from the Institutional Review Board (IRB) of St. Paul’s Hospital Millennium Medical College (SPHMMC) and a formal support letter was written from SPHMMC to all concerned federal health institutions as well as to Oromia Regional State Health Bureau. The regional health bureau has written a letter of support to all concerned regional level health institutions, zonal health departments, district health offices, and health facilities according to the administrative hierarchies in the region. Furthermore, written informed consents were obtained from both the participant health institutions and all health professionals. Moreover, the participants’ informed consent included publication of anonymized responses. All the personal data concerning study participants kept were strictly confidential, and all the details of participants were anonymous during database preparation, ie, all the study subjects were coded with pseudo names. Furthermore, even during the data management and report drafting periods, ethical considerations were maintained. In general, the authors are pleased to inform that this study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
First, our gratitude goes to St. Paul’s Hospital Millennium Medical College, School of Public Health, and BI Norwegian Business School for their provision of the chance to participate in the MIA project-COVID-19 Supply Chain Research Group and to conduct this research work. Secondly, our gratitude goes to the Research Council of Norway (RCN) for funding the research project. Last, but not least, we are grateful for those who participated actively and positively from the inception up to the final report of the research project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Research Council of Norway (RCN) in collaboration with BI Norwegian Business School funded this research (Project no: 312715). The funding body had no role in the design of the study, data acquisition, analysis, and interpretation of data, and in writing the manuscript.
Disclosure
The authors declare that they have no potential conflicts of interest in this work.
References
1. United Nations Children’s Fund. Leaving No One Behind, All Children Immunized and Healthy; 2019: 1–4.
2. World Health Organization. Coronavirus disease (COVID-19). World Health Organization. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
3. World Health Organization. Introduction of Pneumococcal Vaccine A Handbook for District and Health Facility Staff World Health Organization; 2013:1–20.
4. Gavi.org. Sustainable development goals. Available from: https://www.gavi.org/our-alliance/global-health-development/sustainable-development-goals.
5. Gavi. Immunization and the sustainable development goals; 2019.
6. Causey K, Fullman N, Sorensen RJD, et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020, a modelling study. Lancet. 2021;398(10299):522–534. doi:10.1016/S0140-6736(21)01337-4
7. Wondimu A, Cao Q, Wilschut JC, Postma MJ. Factors associated with the uptake of newly introduced childhood vaccinations in Ethiopia, the cases of rotavirus and pneumococcal conjugate vaccines. BMC Public Health. 2019;19(1):1656. doi:10.1186/s12889-019-8002-8
8. Rana MS, Ikram A, Salman M, Usman M, Umair M. Negative impact of the COVID-19 pandemic on routine childhood immunization, experience from Pakistan. Nat Rev Immunol. 2021;21(11):689–690. doi:10.1038/s41577-021-00627-7
9. Tesema GA, Tessema ZT, Tamirat KS, Teshale AB. Complete basic childhood vaccination and associated factors among children aged 12-23 months in East Africa, a multilevel analysis of recent demographic and health surveys. BMC Public Health. 2020;20(1):1837. doi:10.1186/s12889-020-09965-y
10. Abbas K, Procter SR, Zandvoort K, Clark A, Funk S, Mengistu T Routine childhood immunization during the COVID-19 pandemic in Africa, a benefit-risk analysis of health benefits versus excess risk of SARS-CoV-2 infection. Lancet Glob Heal. 2020;8:1264–1272.
11. World Health Organization. COVID-19 Continues to Disrupt Essential Health Services in 90% of Countries; 2021. Available from: https://www.who.int/news/item/23-04-2021-covid-19-continues-to-disrupt-essential-health-services-in-90-of-countries.
12. Masresha BG, Jr LR, Shibeshi ME, et al. The performance of routine immunization in selected African countries during the first six months of the COVID-19 pandemic. Pan Afr Med J. 2020;37(Suppl1):12. doi:10.11604/pamj.supp.2020.37.12.26107
13. Adamu AA, Jalo RI, Habonimana D, Wiysonge CS. COVID-19 and routine childhood immunization in Africa, leveraging systems thinking and implementation science to improve immunization system performance. Int J Infect Dis. 2020;98:161–165. doi:10.1016/j.ijid.2020.06.072
14. Chiappini E, Parigi S, Galli L, et al. Impact that the COVID‐19 pandemic on routine childhood vaccinations and challenges ahead, a narrative review. Acta Paediatr. 2021;110(9):2529–2535. doi:10.1111/apa.15949
15. WHO and UNICEF. At least 80 million children at risk of disease as COVID-19 disrupts vaccination efforts, warn Gavi. Gavi.org; 2020. Available from: https://www.gavi.org/news/media-room/least-80-million-children-risk-disease-covid-19-disrupts-vaccination-efforts.
16. Unicef. Immunization services begin slow recovery from COVID-19 disruptions, though millions of children remain at risk from deadly diseases – WHO, UNICEF, Gavi. Available from: https://www.unicef.org/press-releases/immunization-services-begin-slow-recovery-covid-19-disruptions-though-millions.
17. Chandir S, Siddiqi DA, Mehmood M, et al. Impact of COVID-19 pandemic response on uptake of routine immunizations in Sindh, Pakistan, an analysis of provincial electronic immunization registry data. Vaccine. 2020;38(45):7146–7155. doi:10.1016/j.vaccine.2020.08.019
18. Mansour Z, Arab J, Said R, et al. Impact of COVID-19 pandemic on the utilization of routine immunization services in Lebanon. PLoS One. 2021;16(2):E0246951. doi:10.1371/Journal.Pone.0246951
19. World Health Organization. Guiding Principles for Immunization Activities During the COVID-19 Pandemic, Interim Guidance. World Health Organization; 2020. Available from: Https://apps.who.int/iris/handle/10665/331590.
20. Montoya J, Ballesteros SM, Constanza J, Sotelo R, Lucia C, Cervera B. Impact of the COVID-19 pandemic on routine childhood immunisation in Colombia. BMJ. 2021;2021(28):1–6.
21. Chandir S, Siddiqi DA, Setayesh H, Khan AJ. Impact of COVID-19 lockdown on routine immunisation in Karachi, Pakistan. Lancet Glob Health. 2020;8(9):e1118–e1120. doi:10.1016/S2214-109X(20)30290-4
22. Ogundele OA, Omotoso AA, Fagbemi AT. COVID-19 outbreak, a potential threat to routine vaccination programme activities in Nigeria. Hum Vaccin Immunother. 2021;17(3):661–663. doi:10.1080/21645515.2020.1815490
23. UNICEF. Disruption of childhood vaccination in South Asia poses an urgent threat to children’s health. Unicef.org. Available from: https://www.unicef.org/press-releases/disruption-childhood-vaccination-south-asia-poses-urgent-threat-childrens-health.
24. Burt JF, Ouma J, Lubyayi L, et al. Indirect effects of COVID-19 on maternal, neonatal, child, sexual and reproductive health services in Kampala, Uganda. BMJ Glob Health. 2021;6(8):e006102. doi:10.1136/bmjgh-2021-006102
25. Gooding E, Spiliotopoulou E, Yadav P. Impact of vaccine stockouts on immunization coverage in Nigeria. Vaccine. 2019;37(35):5104–5110. doi:10.1016/j.vaccine.2019.06.006
26. Chen SI, Norman BA, Rajgopal J, Assi TM, Lee BY, Brown ST. A planning model for the WHO-EPI vaccine distribution network in developing countries. IIE Trans. 2014;46(8):853–865. doi:10.1080/0740817x.2013.813094
27. Nour TY, Farah AM, Ali OM, Abate KH. Immunization coverage in Ethiopia among 12-23 month old children, systematic review and meta-analysis. BMC Public Health. 2020;20(1):1134. doi:10.1186/s12889-020-09118-1
28. Tamirat KS, Sisay MM. Full immunization coverage and its associated factors among children aged 12-23 months in Ethiopia, further analysis from the 2016 Ethiopia demographic and health survey. BMC Public Health. 2019;19(1):1019. doi:10.1186/s12889-019-7356-2
29. Mcdonald HI, Tessier E, White JM, Woodruff M, Knowles C, Bates C. Early impact of the coronavirus disease (COVID-19) pandemic and physical distancing measures on routine childhood vaccinations in England. Eurosurveillance. 2020;25(19):2000848
30. ORHB. Oromia Regional Health Bureau 2012 EFY (2019/2020) Annual Report; 2020.
31. UNICEF. Situation Analysis of Children and Women, Oromia Region; 2019.
32. Oromia Regional Health Bureau. Available from: File:/Https://www.orhb.gov.Et/.
33. Nelson R. COVID-19 disrupts vaccine delivery. Lancet Infect Dis. 2020;20(5):546. doi:10.1016/S1473-3099(20)30304-2
34. Santoli JM, Lindley MC, Desilva MB, Kharbanda EO, Daley MF, Galloway L. Morbidity and Mortality Weekly Report Effects, Effects of the COVID-19 Pandemic on Routine Pediatric Vaccine Ordering and Administration. United States; 2020.
35. Center for Global Development. Balancing the COVID-19 response with wider health needs, key decision-making considerations for low- and middle-income countries; 2020:1–12.
36. Lassi ZS, Naseem R, Salam RA, et al. COVID-19 disrupts vaccine delivery, the impact of the ongoing pandemic of coronavirus 2019 on immunization campaigns in low-and middle-income countries is concerning. Int J Environ Res Public Health. 2020;18:988.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.