")
Back to Journals » Vascular Health and Risk Management » Volume 19
The Impact of COVID-19 National Lockdown on Myocardial Infarction (MI) Hospitalizations in Northern Jordan
Authors Al-Kasasbeh A, Alghzawi AA , Ibrahim KS , Ababneh MJ , Ibdah R , Abusurrah O, Dweik K, Kheirallah KA
Received 31 August 2022
Accepted for publication 5 January 2023
Published 20 January 2023 Volume 2023:19 Pages 43—51
DOI https://doi.org/10.2147/VHRM.S387074
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Takashi Kajiya
Abdullah Al-Kasasbeh,1 Ahmad Abdalmajeed Alghzawi,2 Khalid S Ibrahim,3 Muhannad J Ababneh,1 Rasheed Ibdah,1 Obada Abusurrah,1 Khaled Dweik,1 Khalid A Kheirallah2
1Department of Internal Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Public Health, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 3Division of Cardiac Surgery, Department of General Surgery and Urology, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Abdullah Al-Kasasbeh, Department of Internal Medicine, Faculty of Medicine, Jordan University of Science and Technology, P.O. Box 3030, Irbid, 22110, Jordan, Tel +962798339500, Email [email protected]
Background: During COVID-19 lockdown periods, several studies reported decreased numbers of myocardial infarction (MI) admissions. The lockdown impact has not yet been determined in developing countries. The aim of this study was to investigate the impact that of the lockdown measures might have had on the mean number of MI hospital admissions in Northern Jordan.
Methodology: A single-center study examined consecutive admissions of MI patients during COVID-19 outbreak. Participants’ data was abstracted from the medical records of King Abdullah University Hospital between 2018 and 2020. Mean and percentages of monthly admissions were compared by year and by lockdown status (pre-lockdown, lockdown, and post-lockdown time intervals).
Results: A total of 1380 participants were admitted with acute MI symptoms: 59.2% of which were STEMI. A decrease in number of MI admissions was observed in 2020, from 43.1 (SD: 8.017) cases per month in 2019 to 40.59 (SD: 10.763) in 2020 (P < 0.0001) while an increase in the numbers during the lockdown was observed. The mean number during the pre-lockdown period was 40.51 (SD: 8.883), the lockdown period was 44.74 (SD: 5.689) and the post-lockdown was 34.66 (SD: 6.026) (P < 0.0001 for all comparisons). Similar patterns were observed when percentages of admissions were used.
Conclusion: Upon comparing the lockdown period both to the pre- and post-lockdown periods separately, we found a significant increase in MI admissions during the lockdown period. This suggests that lockdown-related stress may have increased the risk of myocardial infarction.
Keywords: COVID-19, myocardial infarction, lockdown, hospital admissions, Jordan, STEMI, NSTEMI
Introduction
Globally, cardiovascular diseases (CVDs) are among the most prevalent medical conditions,1 and among the most common causes of death, causing around a third of all deaths.2,3 Ischemic heart disease (IHD) is considered the most common type of CVDs.3 Several factors contribute to the increased risk of IHD, including stress and sedentary lifestyle.4 Jordan has a high prevalence of myocardial infarction (MI) compared to western countries.5–7 It is the most common cause of death in Jordan and comprises almost one-fifth of the total number of deaths.8
The ST-segment elevation myocardial infarction (STEMI), which usually results from rupture of atherosclerotic plaque and subsequent thrombosis and occlusion of a coronary artery, is considered a fatal cardiovascular emergency that requires prompt diagnosis and rapid reperfusion therapy.9 This puts the medical staff in dilemma, as performing primary percutaneous coronary intervention (PCI), which is considered the preferred reperfusion strategy recommended by most STEMI guidelines,10 for a patient whose COVID-19 status is not yet known which puts the health care workers and other hospitalized cardiovascular patients at risk especially that they are particularly vulnerable to develop severe acute respiratory syndrome -coronavirus-2 (SARS-CoV2) if got infected.11,12 On the other hand, screening these patients for COVID-19 takes time which might delay primary PCI and negatively affect patient prognosis. However, PCI as the standard treatment for STEMI patients during the pandemic is still recommended as the therapy of choice by the American College of Cardiology and the Society for Cardiac Angiography and Interventions (SCAI).13 Altough there have been numerous health care system strains put on by COVID-19, the disease affects a variety of health care settings, including catheterization laboratories.13
In order to halt the spread of an epidemic, two non-pharmaceutical intervention (NPI) strategies have been identified globally: mitigation and suppression. Mitigation aims to reduce the peak of healthcare demand and to protect at-risk groups, thereby slowing the spread of disease but not necessarily stopping it. On the other hand, in suppression, the goal is to arrest and reverse the progression of the epidemic, reduce the number of cases to a low level, and maintain that level for the long run.14 As part of the global response to combat the first wave of COVID-19, Jordan has followed strict (NPI) measures early on during the pandemic to protect people. The government took one of the most drastic measures by implementing a strict country-wide lockdown between March 22 and the end of April 2020 followed by gradual re-opening of selected sectors, such as out-patient clinics. The country declared a state of emergency on March 22 and enacted a national lockdown; during which, all institutions of the public and private sectors were completely shut down, and the government circulated a decision outlining the sectors that are excluded from the lockdown decision including the health sector and other vital sectors.14,15
COVID-19 was reported to impact physical health and the general overall,16 with patients with chronic diseases severely affected, especially those who require routine regular visits to clinics to monitor their blood pressure and blood glucose levels.17 As a result of the lockdown, people have been less active and gained more weight, adversely affecting their health.18 The effect of COVID-19 on mental health is considered a big concern, during the lockdown, with reports that mental health has deteriorated compared to the period before the lockdown.19 Some also reported that the prevalence of mental health issues was on the rise since the lockdown.20
The effects of COVID-19-related lockdown on CVS and MI hospital admissions were reported. According to a multicentric study in Europe, the number of ER visits declined and the number of hospital admissions for CVDs has significantly decreased.21 A meta-analysis assessing the hospitalization of MI patients reported that the number of admissions for myocardial infarction declined during COVID-19 pandemic and during the lockdown.22 STEMI patients’ outcomes were also reported to be negatively affected by the lockdown,23 with some studies reporting a 2% increase in mortality rate.24 Other studies reported other findings, despite the decrease in ER visits, the mortality rate increased four folds, but a similar mortality rate for admitted patients with MI was observed as compared to the previous year.21 A rise in cardiac arrests occurring outside of the hospital was noted during the pandemic,25,26 and the number of cardiac deaths occurring outside of the hospital markedly increased.27
From within developing countries, where resources to combat the epidemic were scarce and shut down of almost all medical services was the norm, little is known about the effects of severe NPI measures on cardiovascular patients. In this study, we aimed at investigating the potential impact of strict NPI measures (lockdown) from Jordan on myocardial infarction patient’s admissions, including STEMI and NSTEMI cases.
Materials and Methods
Study Design
This is a retrospective single-center study conducted in King Abdullah University Hospital (KAUH), which is the largest tertiary healthcare provider in northern Jordan and the only center that offers percutaneous coronary interventional (PCI) service. KAUH serves approximately 3 million inhabitants.
All patients admitted with STEMI and NSTEMI in the period from January 1, 2018 to December 31, 2020 were included. Eligible patients were above the age of 18 years, not infected with COVID-19 during the first COVID-19 outbreak, and hospitalized with MI. MI was defined according to the fourth universal definition of MI; as an elevation or a drop of cardiac enzymes (troponin) above the 99th percentile of the upper reference limit in addition to at least one of the following; MI symptoms, new electrocardiogram (ECG) ischemic changes, pathological Q wave, or imaging evidence consistent with ischemia.28 STEMI was defined according to European Society of Cardiology (ESC) guidelines as follows:
At least two contiguous leads with ST-segment elevation of ≥2.5 mm in men < 40 years, ≥ 2 mm in men ≥40 years, or ≥1.5 mm in women in leads V2–V3 and/or ≥1 mm in the other leads, in the absence of left ventricular (LV) hypertrophy or left bundle branch block. (LBBB)10
Retrospective data were abstracted from the medical records for the period between January 1, 2018 and December 31, 2020. The mean values of the number of monthly admitted MI cases, the percentage of the admitted STEMI (STEMI/total MI cases), and the percentage of in-hospital mortality (mortality/total MI cases) were calculated and compared by lockdown status and by year.
Time segments for the lockdown status were categorized into three time intervals: pre-lockdown, lockdown, and post-lockdown. The lockdown period was considered to be between April 1 and June 30, 2020 (3 months). Pre-lockdown was considered the period between January 1. 2018 and March 21. 2020 (~27 months). Post-lockdown period was set between July 1 and December 31, 2020 (6 months). April 1 was set as the start point of recruitment in the lockdown period, rather than March 22nd, to facilitate comparing statistics for whole months.
The study was performed according to the principles of the declaration of Helsinki, 1975. The IRB committee’s policy waived the informed consent due to the retrospective nature of the study and the research could not be carried out practically without the waiver. In addition, the research does not involve more than minimal risk to the patients. Given the importance of the knowledge to be gained and that it will not adversely affect the rights or the privacy of the participants, the IRB committee approved it without consent.
Statistical Analysis
Data were analyzed by time (year and lockdown status) as stated above. The mean values for the number of monthly admitted MI cases and percentages were presented and compared using ANOVA. Post-hoc comparisons were conducted when appropriate using Tukey’s test. Sub-analyses were conducted for STEMI cases only. Data were presented as means (SD) and numbers/percentages as appropriate. Alpha level was set at 5%. IBM SPSS Statistical software application (version 28) was used for the analysis.
Results
Our study sample included 1380 participants who were admitted with acute myocardial infarction (MI) symptoms over the course of 3 years (January 1, 2018 to December 31, 2020). Males represented 85.7% of the study population. Overall mean age was 57.24 years (SD: 11.98) (for males= 56.15 years (SD: 11.66) and for females = 63.72 years (SD: 11.79) years (P<0.0001)). STEMI patients represented 59.2% (n=817) of the total sample. Other demographic and clinical characteristics are presented in Table 1.
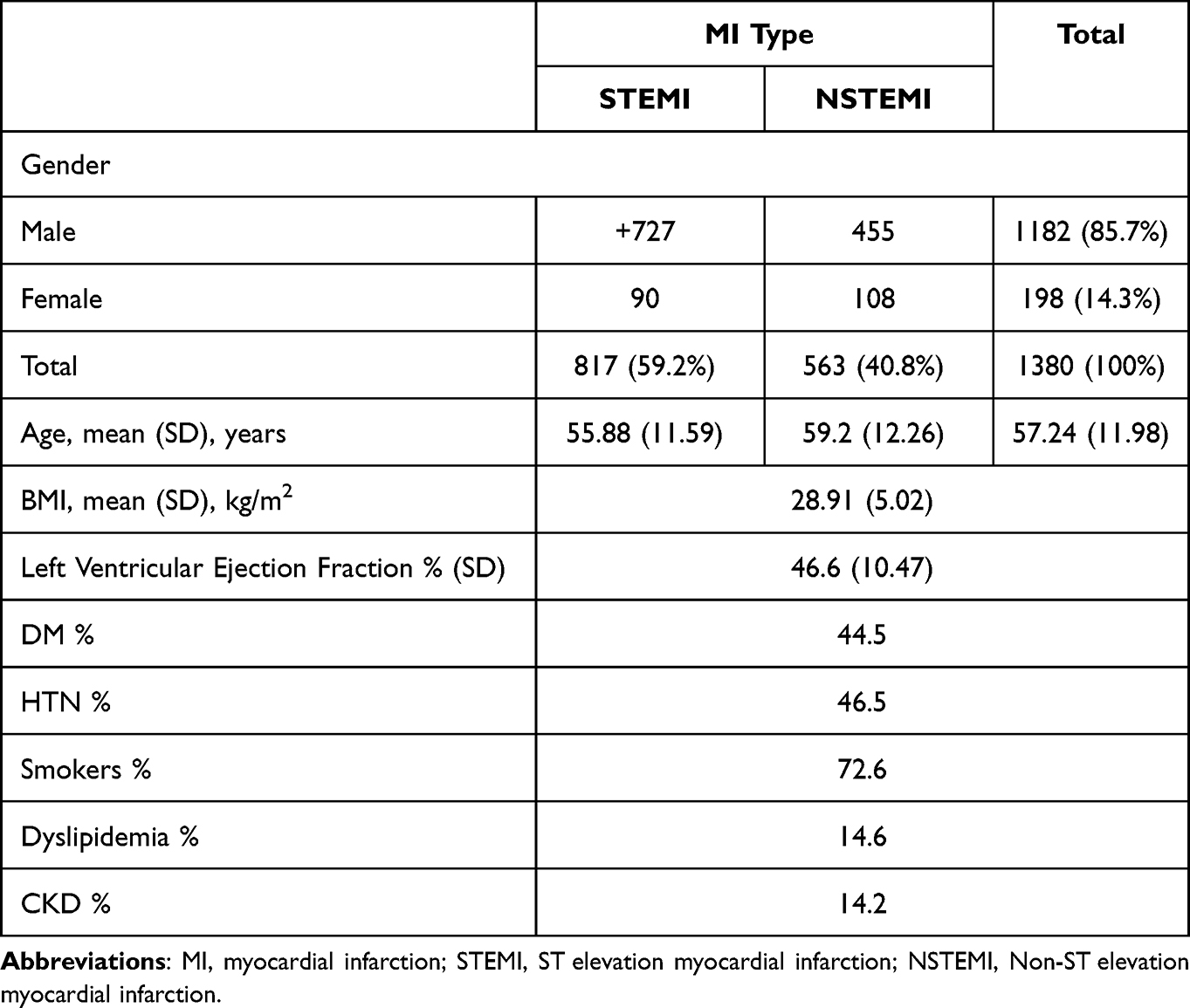 |
Table 1 Distribution of Study Participants by Gender and Mean Age and by MI Type |
The mean number of monthly admitted MI cases increased by 19.9% in 2019 compared to 2018; from 35.95 (SD: 3.9) cases per month in 2018 to 43.1 (SD: 8.02) cases per month in 2019 (P < 0.0001), before dropping by 5.8% in 2020 compared to 2019; 40.59 (SD: 10.76) (P < 0.0001).
For STEMI cases, only (n=817) the mean number of monthly admitted STEMI cases significantly increased, by 26.4%, from 19.63 (SD: 3.63) cases per month in 2018, to 26.68 (SD: 5.61) cases per month in 2019 (P < 0.0001), before dropping 2.43% in 2020, to 26.03 (SD: 7.8) cases. This difference is not statistically significant comparing to the year 2019 (P=0.524). The mean STEMI-only monthly percentage (STEMI/total MI cases) of the admitted cases was compared between the 3 years. The mean monthly percentage of the admitted STEMI cases increased from 54.91% in 2018 (SD: 9.00) to 62.13% in 2019 (SD: 7.29) (P < 0.0001), it further increased to 63.62% in 2020 (SD: 9.74) (P =0.093).
The mean number of monthly admitted MI cases during the lockdown period was compared with pre-lockdown period and with the post-lockdown period. The mean number of monthly admitted MI cases increased by 9.45% in the lockdown period compared to the pre-lockdown period; from 40.51 (SD: 8.88) cases per month to 44.74 (SD: 5.69) cases per month (P<0.0001), followed by a 22.53% decrease in the post-lockdown period to 34.66 (SD: 6.03) (P<0.0001).
Regarding STEMI cases only, the mean number of monthly admitted STEMI cases increased 20.75% in the lockdown period compared to the pre-lockdown period; from 24.01 (SD: 6.18) cases per month to 30.3 (SD: 5.301) cases per month, followed by a decrease by 25.18% in the post-lockdown period to 22.67 (SD: 8.214) cases per month. Differences in the mean number of monthly admitted MI cases were statistically significant between the lockdown, in one hand, and the pre-lockdown (P < 0.0001) and post-lockdown (P < 0.0001) on the other hand. The difference between the pre-lockdown and post-lockdown was statistically insignificant (P = 0.092). The mean STEMI-only monthly percentage (STEMI/total MI cases) of the admitted cases increased from 59.42% in the pre-lockdown period (SD: 8.94) to 65.2% in the lockdown period (SD: 4.74) (P < 0.0001), before dropping to 62.47% in the post-lockdown period (SD: 12.63) (P=0.065).
In a sub-analysis, when conducting the same analysis for the year 2020 only and with considering the pre-lockdown period between January 1 and March 21, 2020, the lockdown from April 1 to June 30 and the post lockdown as the period from July 1 to September 30, the mean monthly percentage of the admitted STEMI cases increased by 5.17% in the lockdown period (66.85%, SD: 3.45), compared to the pre-lockdown period (61.68%, SD: 8.48) (P = 0.002), followed by a 4.37% decrease in the post-lockdown period (62.47%, SD: 12.63) (P = 0.003).
In a trial to eliminate any seasonal effect on admissions and mortality related to MI, the lockdown period (April–June) was compared between the 3 consecutive years (2018, 2019 and 2020). The mean number of monthly admitted MI cases in 2018 was 35.57 (SD: 2.89) cases per month, this number increased to 40.51 (SD: 7.4) cases per month in 2019 (P < 0.0001). While in 2020, the number of cases increased to 44.74 (SD: 5.69) cases per month (P < 0.0001) (Figure 1). There was an increase in the mean number of monthly percentages of admitted STEMI cases from 51.89% (SD: 11.73) in 2018 to 68.91% (SD: 6.62) in 2019, followed by a drop to 66.67% in 2020. The difference in percentage was statistically significant between 2019 and 2018 (P < 0.0001). On the other hand, the difference in percentages was not statistically between 2019 and 2020 (P = 0.097) (Figures 2 and 3).
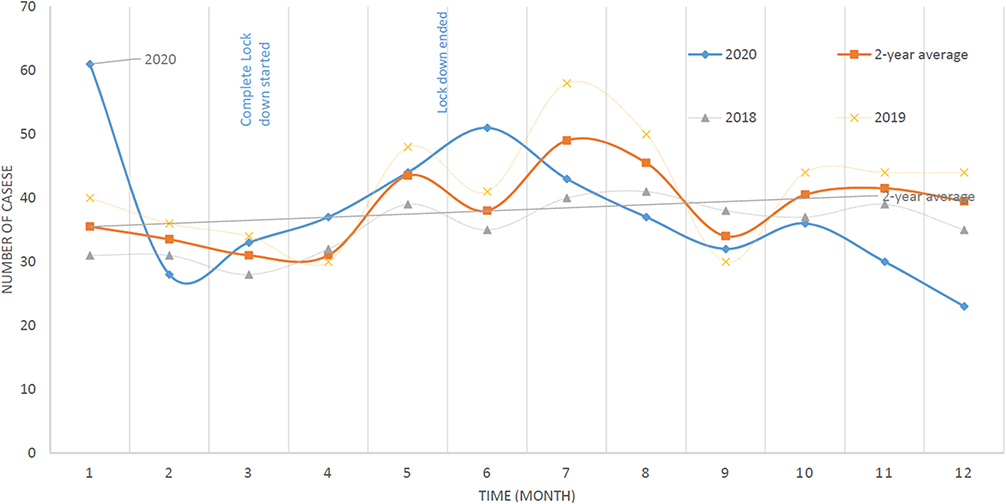 |
Figure 1 Number of MI cases (2020 vs 2019–2018 average). |
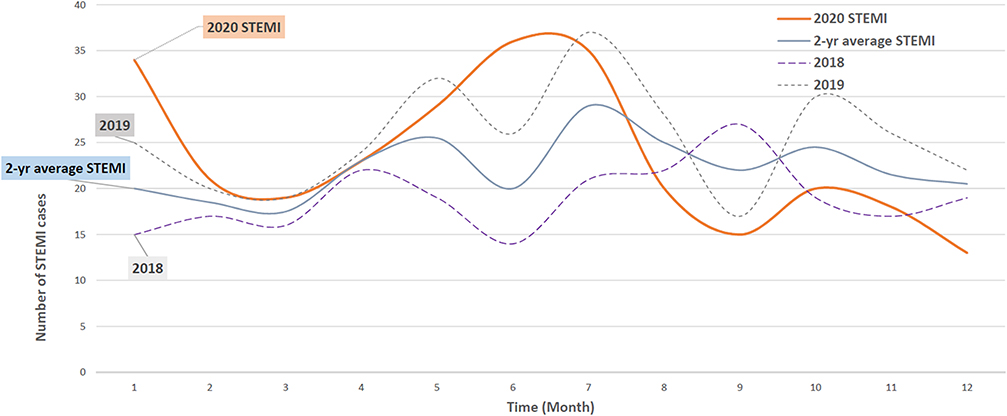 |
Figure 2 Number of STEMI cases (2020 vs 2019–2018 average). |
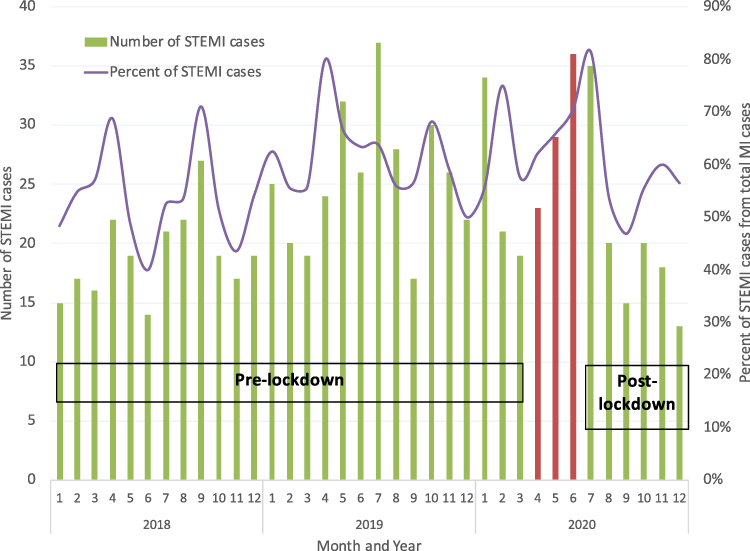 |
Figure 3 The number of STEMI cases and the percentage of STEMI cases out of the total cases for the 3-year period. |
There was a statistically significant decrease in the mean monthly percentage of in-hospital MI mortality cases between 2018 (6.17 (SD: 3.68)) and 2019 (5.29 (SD: 2.47)) (P = 0.002), which was followed by a further decrease in 2020 (4.62 (SD: 2.92)) (P < 0.0001). In STEMI cases only, the mean monthly percentage of in-hospital mortality cases was the same as that of the total MI cases. The mean monthly percentage of in-hospital mortality cases was compared by lockdown level. The mean monthly percentage of in-hospital mortality cases decreased by 1.36% in the lockdown period (4.61% (SD: 1.28)) compared to the pre-lockdown period (5.97% (SD: 3)) (P < 0.0001), followed by a further decrease by 2.12% in the post-lockdown period (2.49% (SD: 2.53)) (P < 0.0001). In STEMI cases only, the mean number of monthly in-hospital mortality cases was almost the same as that of total MI cases (Table 2).
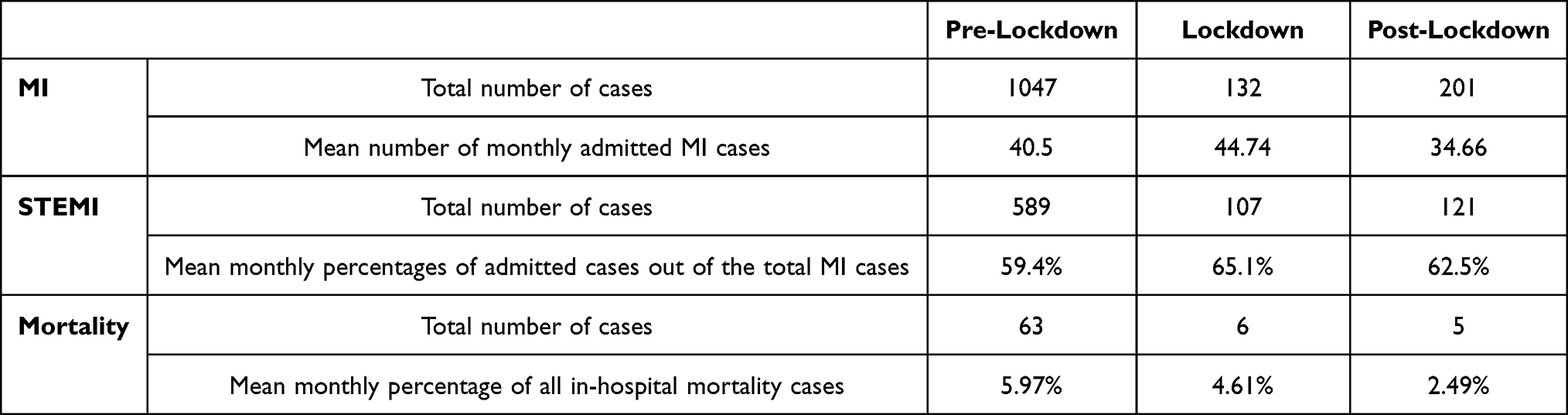 |
Table 2 Cases Number and Monthly Percentage in Lockdown Levels |
Discussion
The effect of COVID-19 lockdown on cardiovascular diseases, especially MI, has been previously reported in western countries. Patients with cardiovascular diseases were adversely affected by the lockdown that was implemented during the COVID-19 pandemic.23,29,30 Yet, evidence from developing country settings is scarce. This study was conducted to investigate the potential impact of strict NPI measures in Jordan, particularly lockdown, on myocardial infarction admissions, including STEMI and NSTEMI.
Our results suggest that the number of myocardial infarction cases, STEMI and NSTEMI, in 2020 was lower than that in 2019. The mean number of monthly admitted MI cases decreased by 5.8%. This finding is consistent with similar results in France, where a 6% decline in MI cases admission was observed in 2020.31 Other studies reported 30% reduction of MI cases admission.24 Regarding STEMI-only cases, we observed an increase of 7.22% in the mean STEMI-only monthly percentage of the admitted cases between 2018 and 2019, followed by an insignificant increase by 1.49% in 2020. Different results were observed in other studies, although there was a 30% decrease in acute coronary syndrome admissions in Europe. Compared to 2019, STEMI cases increased from 32% to 37% of all admitted cases in 2020, whereas NSTEMI cases decreased.21
The observed difference in monthly cases by year could be attributed to the fear of COVID-19 infection while in the hospital. This is especially true as the hospital setting under investigation was the main healthcare setting for COVID-19 patients in Northern Jordan. With such fear, patients may have avoided seeking medical care. Such explanation was previously reported.21,24,32
By comparing the mean number of monthly admitted MI cases by lockdown status, our results suggest that MI cases increased 9.5% during the lockdown period, followed by a 22.5% drop after the lockdown ended. Regarding STEMI cases, there is a 5.78% increase during the lockdown period as compared to the pre-lockdown period, followed by a 2.73% decrease after the lockdown. Compared with previous published studies, our results are conflicting in which the number of admitted MI cases were fewer during the COVID-19 lockdown with a decrement of about 17% compared to the pre-lockdown period, and no difference in number of cases between the pre-lockdown and the post-lockdown periods.22,32 Our results can be explained by the increased effect of risk factors during the lockdown such as psychological factors, sedentary lifestyle, and loss of chronic illness follow-up. Acute MI is significantly affected by psychological factors.33 During the lockdown, adults experienced more stress, anxiety, social isolation, and psychological distress.34 Individuals at risk for MI can be affected by lockdown-related stress.35 Also, depression was exacerbated by lockdown-related stress.36 Chronic depression is considered as one of the most important predictors of poor outcomes in MI patients.33 A study conducted in Jordan indicated that stress and loneliness are the most reported triggering factors for MI during the lockdown, followed by stress and hardship related to finances, fluctuating incomes, and loss of employment.35 CVD risk increases by 50% when social isolation and loneliness were present.33
Other risk factors were affected by the lockdown, the level of physical activity among adults decreased during quarantine and their sedentary behavior increased.34 Patients with chronic diseases require diagnostic tests and routine check-ups by physicians. Those patients’ health and routine life have been affected due to inability to get appropriate follow-up during the lockdown.17 Several studies have shown that the lockdown period caused patients’ glycemic values to worsen and weight/BMI to rise.37 It is possible that all these factors together could have increased the number of MI cases observed during the lockdown period.
A big decline in cases can be observed in the post-lockdown period, the possible explanation is that patients with high risk to develop MI have undergone a big stressful conditions and got under exaggerated risk factor during the lockdown period; this large effect accelerated the infarction event, resulting in decreased number of cases following the lockdown period.
In 2020, the total number of MI cases declined, which resulted in a significant decrease in MI mortality compared with previous years. Our results suggest that there is a 0.67% decrease in the mean number of monthly percentage of in-hospital mortality cases in 2020 compared to 2019. In STEMI cases, the mean number of monthly in-hospital mortality cases was nearly the same as that for MI overall. The inpatient mortality rate appeared to be similar to what was seen in 2019 according to other studies.21
The mean number of monthly percentage of in-hospital mortality cases in 2020 were compared by lockdown level for MI cases, although the number of MI cases increased in the lockdown period, the mean number of monthly in-hospital mortality cases decreased 1.36% compared with the pre-lockdown period, this finding can be explained by the excellent and fast health care provided for MI patients, although the total lockdown that was implemented in the country was strict and included governmental and non-governmental organizations, vital sectors were not included.15 Health sector was not included in the lockdown, health services were suspended for non-emergent conditions,14 By taking these measures, the health sector has been able to provide good and fast health care to emergency cases. Alternatively, a possible explanation for this finding is that more high-risk patients died out-of-hospital, in Denmark, the total deaths in 2020 during the lockdown period was the same as that of 2019 in the same period, but in-hospital mortality decreased and out-of-hospital mortality increased, this was explained by patients’ fear of acquiring the disease.38 Due to such fear, patients may have avoided seeking medical care, which may have led to advanced diseases. This explanation was previously reported.21,24,32
Other literature indicates that there is no significant increase in inpatient mortality among MI patients during the lockdown.31 In STEMI cases, the mean number of monthly percentage of in-hospital mortality cases was nearly the same as that for MI overall. The mean number of monthly percentage of in-hospital mortality cases continued to significantly decline after the lockdown.
Conclusion
Upon comparing the lockdown period both to the pre- and post-lockdown periods separately, we found a significant increase in MI admissions during the lockdown period. This suggests that lockdown-related stress may have increased the risk of myocardial infarction.
Recommendations
During pandemics, certain steps should be taken to reduce the risk of myocardial infarction. Despite the lockdown, chronically ill patients need to continue to receive their medical care, whether through telehealth or by adapting and developing certain programs to help patients receive appropriate health care and reduce in-person contact at the same time. In addition, the mental health effects of lockdown measures should be considered when establishing policies to slow the pandemic spread. This is due to the fact that they are considered a potential cause of myocardial infarction.
Acknowledgments
The authors would like to thank all workers at KAUH for their efforts during COVID-19 in Jordan.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roser M, Ritchie H. Burden of disease - our world in data. OurWorldInData.org; 2018. Available from: https://ourworldindata.org/burden-of-disease.
2. World Health Organization. WHO reveals leading causes of death and disability worldwide: 2000–2019 - PAHO/WHO. Pan Am Health Organ. 2020;1:2019–2022.
3. Khan MA, Hashim MJ, Mustafa H, et al. Global epidemiology of ischemic heart disease: results from the global burden of disease study. Cureus. 2020;12(7). doi:10.7759/CUREUS.9349
4. Shah PK. Risk Factors in Coronary Artery Disease. StatPearls Publishing; 2006. doi:10.3109/9781420014570
5. Mohannad N, Mahfoud Z, Kanaan MN, Balbeissi A. Prevalence and predictors of non-fatal myocardial infarction in Jordan. East Mediterr Health J. 2008;14(4):818–830.
6. Manuel DG, Lim JJY, Tanuseputro P, Stukel TA. How many people have had a myocardial infarction? Prevalence estimated using historical hospital data. BMC Public Health. 2007;7(1):1–12. doi:10.1186/1471-2458-7-174
7. Bhatnagar P, Wickramasinghe K, Williams J, Rayner M, Townsend N. The epidemiology of cardiovascular disease in the UK 2014. Heart. 2015;101(15):1182–1189. doi:10.1136/heartjnl-2015-307516
8. CDC. CDC in Jordan; 2013. Available from: http://www.cdc.gov/globalhealth/countries/jordan.
9. Zhang Y, Yu B, Han Y, et al. Protocol of the China ST-segment elevation myocardial infarction (STEMI) Care Project (CSCAP): a 10-year project to improve quality of care by building up a regional STEMI care network. BMJ Open. 2019;9(7):e026362. doi:10.1136/BMJOPEN-2018-026362
10. Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393
11. Rodriguez-Leor O, Cid-Alvarez B. ST-segment elevation myocardial infarction care during COVID-19. JACC Case Rep. 2020;2(10):1625–1627. doi:10.1016/j.jaccas.2020.04.011
12. Driggin E, Madhavan MV, Bikdeli B, et al. Cardiovascular considerations for patients, health care workers, and health systems during the COVID-19 pandemic. J Am Coll Cardiol. 2020;75(18):2352–2371. doi:10.1016/j.jacc.2020.03.031
13. Welt FGP, Shah PB, Aronow HD, et al. Catheterization laboratory considerations during the coronavirus (COVID-19) pandemic: from the ACC’s interventional council and SCAI. J Am Coll Cardiol. 2020;75(18):2372–2375. doi:10.1016/j.jacc.2020.03.021
14. Kheirallah KA, Alsinglawi B, Alzoubi A, et al. The effect of strict state measures on the epidemiologic curve of COVID-19 infection in the context of a developing country: a simulation from Jordan. Int J Environ Res Public Health. 2020;17(18):1–11. doi:10.3390/IJERPH17186530
15. Khassawneh AH, Alrabadi N, Al-Mistarehi AH, Obeidat N, Kheirallah KA. The role of non-state actors in combating COVID-19 spread in Northern Jordan. Ann Med Surg. 2020;60:484–486. doi:10.1016/j.amsu.2020.11.005
16. Dai J, Sang X, Menhas R, et al. The influence of COVID-19 pandemic on physical health–psychological health, physical activity, and overall well-being: the mediating role of emotional regulation. Front Psychol. 2021;12:3005. doi:10.3389/fpsyg.2021.667461
17. Saqib MAN, Siddiqui S, Qasim M, et al. Effect of COVID-19 lockdown on patients with chronic diseases. Diabetes Metab Syndr. 2020;14(6):1621–1623. doi:10.1016/j.dsx.2020.08.028
18. Dor-Haim H, Katzburg S, Revach P, Levine H, Barak S. The impact of COVID-19 lockdown on physical activity and weight gain among active adult population in Israel: a cross-sectional study. BMC Public Health. 2021;21(1). doi:10.1186/s12889-021-11523-z
19. Pierce M, Hope H, Ford T, et al. Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population. Lancet Psychiatry. 2020;7(10):883–892. doi:10.1016/S2215-0366(20)30308-4
20. Gualano MR, Lo Moro G, Voglino G, Bert F, Siliquini R. Effects of COVID-19 lockdown on mental health and sleep disturbances in Italy. Int J Environ Res Public Health. 2020;17(13):1–13. doi:10.3390/ijerph17134779
21. Sokolski M, Gajewski P, Zymliński R, et al. Impact of Coronavirus Disease 2019 (COVID-19) outbreak on acute admissions at the emergency and cardiology departments across Europe. Am J Med. 2021;134(4):482–489. doi:10.1016/j.amjmed.2020.08.043
22. Baumhardt M, Dreyhaupt J, Winsauer C, et al. The effect of the lockdown on patients with myocardial infarction during the COVID-19 pandemic–a systematic review and meta-analysis. Dtsch Arztebl Int. 2021;118(26):447–453. doi:10.3238/ARZTEBL.M2021.0253
23. Rattka M, Stuhler L, Winsauer C, et al. Outcomes of patients with ST-segment elevation myocardial infarction admitted during COVID-19 pandemic lockdown in Germany – results of a single center prospective cohort study. Front Cardiovasc Med. 2021:256. doi:10.3389/FCVM.2021.638954
24. Mesnier J, Cottin Y, Coste P, et al. Hospital admissions for acute myocardial infarction before and after lockdown according to regional prevalence of COVID-19 and patient profile in France: a registry study. Lancet Public Health. 2020;5(10):e536–e542. doi:10.1016/S2468-2667(20)30188-2
25. Marijon E, Karam N, Jost D, et al. Out-of-hospital cardiac arrest during the COVID-19 pandemic in Paris, France: a population-based, observational study. Lancet Public Health. 2020;5(8):e437–e443. doi:10.1016/S2468-2667(20)30117-1
26. Baldi E, Sechi GM, Mare C, et al. Out-of-hospital cardiac arrest during the covid-19 outbreak in Italy. N Engl J Med. 2020;383(5):496–498. doi:10.1056/NEJMC2010418
27. Campo G, Fortuna D, Berti E, et al. In- and out-of-hospital mortality for myocardial infarction during the first wave of the COVID-19 pandemic in Emilia-Romagna, Italy: a population-based observational study. Lancet Reg Health Eur. 2021;3:100055. doi:10.1016/j.lanepe.2021.100055
28. Thygesen K, Joseph Alpert DS, Allan Jaffe US, et al. Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol. 2018;72(18):2231–2264. doi:10.1016/J.JACC.2018.08.1038
29. Aajal A, El Boussaadani B, Hara L, et al. The consequences of the lockdown on cardiovascular diseases. Ann Cardiol Angeiol. 2021;70(2):94–101. French. doi:10.1016/J.ANCARD.2021.01.006
30. Cransac-Miet A, Zeller M, Chagué F, et al. Impact of COVID-19 lockdown on lifestyle adherence in stay-at-home patients with chronic coronary syndromes: towards a time bomb. Int J Cardiol. 2021;323:285–287. doi:10.1016/j.ijcard.2020.08.094
31. Grave C, Gabet A, Puymirat E, et al. Myocardial infarction throughout 1 year of the COVID-19 pandemic: French nationwide study of hospitalization rates, prognosis and 90-day mortality rates. Arch Cardiovasc Dis. 2021;114(12):768–780. doi:10.1016/j.acvd.2021.10.008
32. Lavie G, Battat E, Saliba W, Flugelman MY. Change in hospitalizations and 30-day mortality of patients with acute myocardial infarction during the first COVID-19 lockdown - A pure social isolation effect? Cardiovasc Revasc Med. 2021;38:38–42. doi:10.1016/J.CARREV.2021.08.025
33. Fioranelli M, Bottaccioli AG, Bottaccioli F, Bianchi M, Rovesti M, Roccia MG. Stress and inflammation in coronary artery disease: a review psychoneuroendocrineimmunology-based. Front Immunol. 2018;9(SEP):2031. doi:10.3389/fimmu.2018.02031
34. Violant-Holz V, Gallego-Jiménez MG, González-González CS, et al. Psychological health and physical activity levels during the covid-19 pandemic: a systematic review. Int J Environ Res Public Health. 2020;17(24):1–19. doi:10.3390/ijerph17249419
35. Hammoudeh AJ, Madanat E, Tabbalat R, et al. Acute cardiovascular events triggered by the COVID-19 pandemic-related stress in non-infected individuals. The Jordan COVID-19 Acute Cardiovascular Events (JoCORE) study. Rev Cardiovasc Med. 2021;22(4):1677–1683. doi:10.31083/j.rcm2204175
36. Yildirim H, Işik K, Aylaz R. The effect of anxiety levels of elderly people in quarantine on depression during covid-19 pandemic. Soc Work Public Health. 2021;36(2):194–204. doi:10.1080/19371918.2020.1868372
37. Eberle C, Stichling S. Impact of COVID-19 lockdown on glycemic control in patients with type 1 and type 2 diabetes mellitus: a systematic review. Diabetol Metab Syndr. 2021;13(1). doi:10.1186/s13098-021-00705-9
38. Butt JH, Fosbøl EL, Gerds TA, et al. All-cause mortality and location of death in patients with established cardiovascular disease before, during, and after the COVID-19 lockdown: a Danish nationwide cohort study. Eur Heart J. 2021;42(15):1516–1523. doi:10.1093/EURHEARTJ/EHAB028
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.