")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 13
The Impact of AC and AC-T Chemotherapy’s Toxicities on Quality of Life Among Women with Breast Cancer in Ethiopia: A Prospective Patient-Reported Outcomes Study
Authors Gadisa DA , Wang SH, Yimer G
Received 4 November 2020
Accepted for publication 22 January 2021
Published 24 February 2021 Volume 2021:13 Pages 107—132
DOI https://doi.org/10.2147/BCTT.S289014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Diriba Alemayehu Gadisa,1 Shu-Hua Wang,2,3 Getnet Yimer4
1Pharmacy Department, College of Medicine and Health Sciences, Ambo University, Ambo, Ethiopia; 2Division of Infectious Diseases, Department of Internal Medicine, The Ohio State University, Columbus, OH, USA; 3Ben Franklin TB Control Program, Columbus, OH, USA; 4Ohio State Global One Health Initiative, Office of International Affairs, The Ohio State University, Addis Ababa, Ethiopia
Correspondence: Diriba Alemayehu Gadisa 19 Tel +251915958190
Email [email protected]
Purpose: The study aimed to evaluate the quality of life patterns and the effects of AC and AC-T chemotherapy’s toxicities on QoL among Ethiopian women with breast cancer.
Methods: QoL was measured at baseline and at every end of two cycles, for the median of 8 cycles among 146 breast cancer women on AC and AC-T chemotherapy, using EORTC QLQ-C30 and BR23 instruments. The effect of QoL score, socio-demographic, and clinical variables at baseline were adjusted for the effect of chemotherapy’s toxicities on QoL.
Results: Overall QoL, all functional scales (except cognitive functioning, body image, future perspectives, and sexual functioning) and symptom scales (except dyspnea, insomnia, pain score, arm, and breast symptoms) of EORTC QLQ-C30 and BR23 deteriorated significantly both clinically and statistically, in particular, during the first two cycles of chemotherapy. After the end of cycle 2 or 4, except for cognitive, social functioning, and financial difficulties of the patients, almost all other QoL dimensions were improved towards pretreatment score by the end of cycle 8. In addition to age, educational status, and tumor stage, the Global Health Status (− 10.55≤B≤− 7.71, P≤ 0.013), and the functional scales (− 25.320≤B≤− 6.351, P≤ 0.033) of EORTC QLQ-C30 and BR23 were significantly affected at least by one of the AC and AC-T chemotherapy’s toxicity such as grade≥ 2 fatigue, dysgeusia, constipation, dry mouth, vomiting, oral mucositis, skin hyperpigmentation and/or peripheral neuropathy than their lower grade. Grade≥ 2 fatigue, dysgeusia, oral mucositis, constipation, peripheral neuropathy, anemia arthralgia/myalgia, dry mouth, diarrhea, constipation, and/or skin hyperpigmentation were positively predicted for the deterioration of symptoms scale of EORTC QLQ-C30 and BR23 (4.819≤B≤ 26.451, P≤ 0.043).
Conclusion: Quality of life among Ethiopian breast cancer patients on AC and AC-T regimens significantly deteriorated particularly during the first two cycles of chemotherapy. In addition to the age, tumor stage and educational status of the patients, grade≥ 2 fatigue, dysgeusia, constipation, oral mucositis, dry mouth, peripheral neuropathy, and skin hyperpigmentation due to AC and AC-T chemotherapy were frequently associated with deterioration of different scales/items QoL. Hence, devising different strategies to improve the deteriorated QoL due to chemotherapy’s toxicities particularly during the first two cycles has paramount importance.
Keywords: quality of life, deterioration, chemotherapy, toxicity, breast cancer, Ethiopia
Introduction
In the era of an increasing number of breast cancer patients worldwide and the longer survival due to early detection programs and advancement in medical technology, accurately assessing the quality of life (QoL) of breast cancer patients is becoming crucial.1,2 As such, there is a need to understand the impact of breast cancer treatment on quality of life (QoL) to help breast cancer patients cope with cancer and its treatment.3 It is due to the quality of life is frequently deteriorated during and after cancer chemotherapy, though the expected treatment outcome in chronic diseases like cancer is the improvement of quality of life.4,5
Patient-reported outcomes measures (PROMs), especially QoL instruments, have increasingly been collected in randomized controlled trials (RCTs) to inform patient-centered care, clinical decision-making, and health policy or reimbursement decisions.6,7 QoL is increasingly being recognized as a valuable endpoint of cancer care for its prognostic value in clinical trials8,9 to serve as an endpoint, complementing traditional assessment measures, eg tumor response, freedom from relapse, survival, and the physician’s opinion concerning patient status.10–13
Breast cancer is probably the most feared by women, especially by the negative stigma and psychological distress brought by its diagnosis and treatments which eventually led them to reduced QoL.14 In addition to the disease itself, other socio-demographic characteristics like age, residence, educational level, employment status, and TNM stage were among the significant predictors for deterioration of QoL.8
Breast cancer chemotherapy has been known to cause deterioration of quality of life (QoL)15–17 as the greater treatment-related burden was associated with poorer QoL.18 That is why the impact of chemotherapy’s toxicities on quality of life and patients’ preferences gain particular relevance.10,19
QoL assessment in women with breast cancer on therapy should address physical symptoms such as nausea, vomiting, fatigue (tiredness and pain), hair loss, functional ability, sexuality (intimacy and body perception), emotional symptoms such as worry (anxiety, depression, and insecurity); social function, work-life, family situation, hope for the future, future planning, spiritual aspects, and total QoL assessment, ie general life satisfaction.11
More attention should be paid to improve patients’ QoL through dealing with the particular impaired function or symptom.8 Unfortunately, evaluation of the impact of treatment modalities on QoL in patients with cancer is very limited.20 In general, the AC and/or AC-T breast cancer chemotherapy poses physical, emotional, and financial burdens on the patients and families.21 Henceforth, it affects almost all domains of quality of life to a greater or lesser degree.22 Hence, the present study aims to evaluate the quality of life patterns and the effects of AC and AC-T chemotherapy’s toxicities on different domains of QoL among Ethiopian women with breast cancer.
Methods and Patients
The institutional-based longitudinal study was conducted from January 1 to February 30, 2017 GC at the only nationwide oncology center, Tikur Anbessa Specialized Hospital (TASH), Addis Ababa, Ethiopia. We enrolled all the146 patients who visited the facility, with no missing quality of life data. A sample size of 100 patients is considered to have enough power to evaluate the quality of life study for each specific cancer site.14 Women age above 18 years with proven newly diagnosed breast cancer from stage I to IV and scheduled to receive the most commonly used neo/adjuvant or palliative first-line chemotherapy (ie, Adriamycin-Cyclophosphamide [AC] and Adriamycin-Cyclophosphamide followed by Paclitaxel [AC-T] regimen) were included.
We excluded patients who had a previous history of breast cancer treatment (ie currently on the second line for recurrent breast cancer). Patients with psychiatric disorders, other severe medical illnesses, and incomplete quality of life data were also excluded from the analysis. Overall, since this data was the part of the study previously described by Gadisa et al,23–25 the study participants in this finding share similarities with previously published articles of the same study project.
Treatment Modalities
The details of treatment modalities were also previously described by Gadisa et al.23–25 Moreover, seventy-one (71) women breast cancer patients on AC regimen received Doxorubicin (A) 60 mg/m2 and Cyclophosphamide (C) 600 mg/m2 as intravenous infusion repeated every 21 days for four or six cycles while 75 study participants on AC-T regimen received Doxorubicin (A) 60 mg/m2 and Cyclophosphamide (C) 600 mg/m2 for four cycles and followed by Paclitaxel (T) 175 mg/m2 intravenous infusion repeated every 21 days for 4 cycles.
Besides, for every cycle of treatment, premedication with ondansetron 8 mg, dexamethasone 16 mg, cimetidine 400 mg, and metoclopramide 10 mg was given by intravenous infusion before the commencement of chemotherapy.
Study Outcomes
The primary endpoints of the study were patterns of QoL among women with breast cancer on chemotherapy. Secondary endpoints were toxicities of breast cancer chemotherapy that cause significant deterioration of QoL.
Assessment for Safety End-Point
Adverse events were graded using the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAEs), Patient-Reported Outcome (PRO) version 4.03.26 Each adverse event is graded as grade 1 (mild), grade 2 (moderate), grade 3 (severe), grade 4 (life-threatening), or grade 5 (death) according to an internationally agreed standard (Common Terminology Criteria for Adverse Events).27 Accordingly, grade≥2 leucopenia (white blood cells count <3000/mm3), grade ≥2 anemia (hemoglobin level <10.0 g/dl), grade≥2 thrombocytopenia (platelets count <75,000/mm3), grade ≥2 neutropenia (absolute neutrophil count <1500/mm3); grade≥1 alanine/aspartate aminotransferase increment (> normal upper limit, U/L); grade≥1 alkaline phosphatase (ALP) increment (> normal upper limit, U/L); grade ≥1 serum creatinine increment (> normal upper limit, mg/dL). The patients were personally interviewed for subjective toxicities such as nausea, vomiting, and the like and their toxicity grades were assessed based on the diary maintained during their revisits. The highest toxicity during any cycle was considered as the toxicity grade for that patient. We presented the detail of each adverse event used in our study, which was abstracted from NCI CTCAEs (version 4.03), in the supplementary material 1. And, the detail of those toxicities experienced by our study participants was previously published25 and/or available at http://DOI.org/10.1177/1078155220907658.
Assessment for Quality of Life Endpoints
Quality of life was assessed with the validated Amharic version of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (QLQ-C30, version 3.0) and the breast–cancer-specific QLQ-BR23 (version 1.0).23 The QLQ-C30 includes nine multiple-item scales of symptoms (nausea and vomiting, diarrhea, constipation, appetite loss, pain, fatigue, insomnia, dyspnea, and financial problems), five to function [physical (PF), role (RF), emotional (EF), cognitive (CF) and social (CF)], and one to overall health—the global health status (GHS) and quality-of-life scale. It also includes six single-item scales. The QLQ-BR23 includes 23 questions regarding disease symptoms, treatment-related side effects, body image, sexuality, and future perspective.28 Patients were asked to complete both questionnaires at baseline and every two cycles of treatment.
For each of the multi-item scales, no item occurs in more than one scale. All of the scales and single-item measures range in score from 0 to 100. A high scale score represents a higher response level. Thus, a high score for a functional scale represents a high/healthy level of functioning, a high score for the global health status/QoL represents a high QoL, but a high score for a symptom scale/item represents a high level of symptomatology/problems. And the scoring was fixed according to the procedures stated on the scoring manual of EORTC QLQ-C30 and BR23.29 QoL deterioration was considered clinically meaningful using previously established thresholds for minimally important differences (MID) in QoL; for EORTC QLQ-C30 and BR23, the threshold for MID was a change of 10 points from baseline.30
Statistical Analysis
The Statistical Package for Social Sciences v.25.0 (SPSS 25.0) software was used for analysis. Descriptive parameters were expressed as percentages and frequencies, continuous variables expressed as mean, standard deviation (SD). Repeated measure general linear model (GLM) and linear mixed model were used to determine the changes in quality of life score in terms of estimated marginal means from baseline and/or between cycles. Unstructured covariance structure was used and Bonferroni was also used for adjustment for multiple comparisons in linear mixed models.
The stepwise linear regression model was used to determine the effect of breast cancer chemotherapy’s toxicities and sociodemographic variables or clinical variables on different domains of QoL. The linear regression model for different QoL domains’ deterioration due to chemotherapy toxicities was corrected/adjusted for baseline QoL score, the statistically significant socio-demographic and clinical variables. The Probability of the variables to be entered into stepwise linear regression was ≤0.050 while the probability of the variable to be removed was ≥0.100. All significance tests were 2-sided with a type I error of 5%. For identifying any outliers we used the outlier with ≥3 SD throughout the analysis. For the detail of variables entered into stepwise linear regression model for the effect of sociodemographic and clinical variables on QoL see supplementary material 2, and for the effect, each chemotherapy toxicity on QoL see supplementary material 3.
Ethical Approval
The study was approved by the Institutional Review Board (IRB) of the school of pharmacy, College of Health Sciences, Addis Ababa University (Ref No: ERB/SOP/09/2016). Addis Ababa University approved the study since our site of data collection was Tikur Anbessa Specialized Hospital (the only oncology center at the national level) which was the part of College of Health sciences of Addis Ababa University.
Informed consent was obtained from all individual participants prior to participation in the study. Moreover, this study was conducted in accordance with the Declaration of Helsinki.31
Results
Socio-Demographic and Clinical Characteristics of Study Participants
The study participants had 42.2 years and 1.6 m2 mean age and body surface area, respectively. The majority of the study participants had stage III 64 (43.8%) and ECOG performance I 135 (92.5%). The mean of all laboratory values was within the normal range. Averagely, study participants received 6.4 cycles or a median of 8 cycles of chemotherapy (Table 1). Since this data were part of the study previously described by Gadisa et al,23–25 the study participants in this finding share similarities with previously published articles of the same study project (see Table 1).
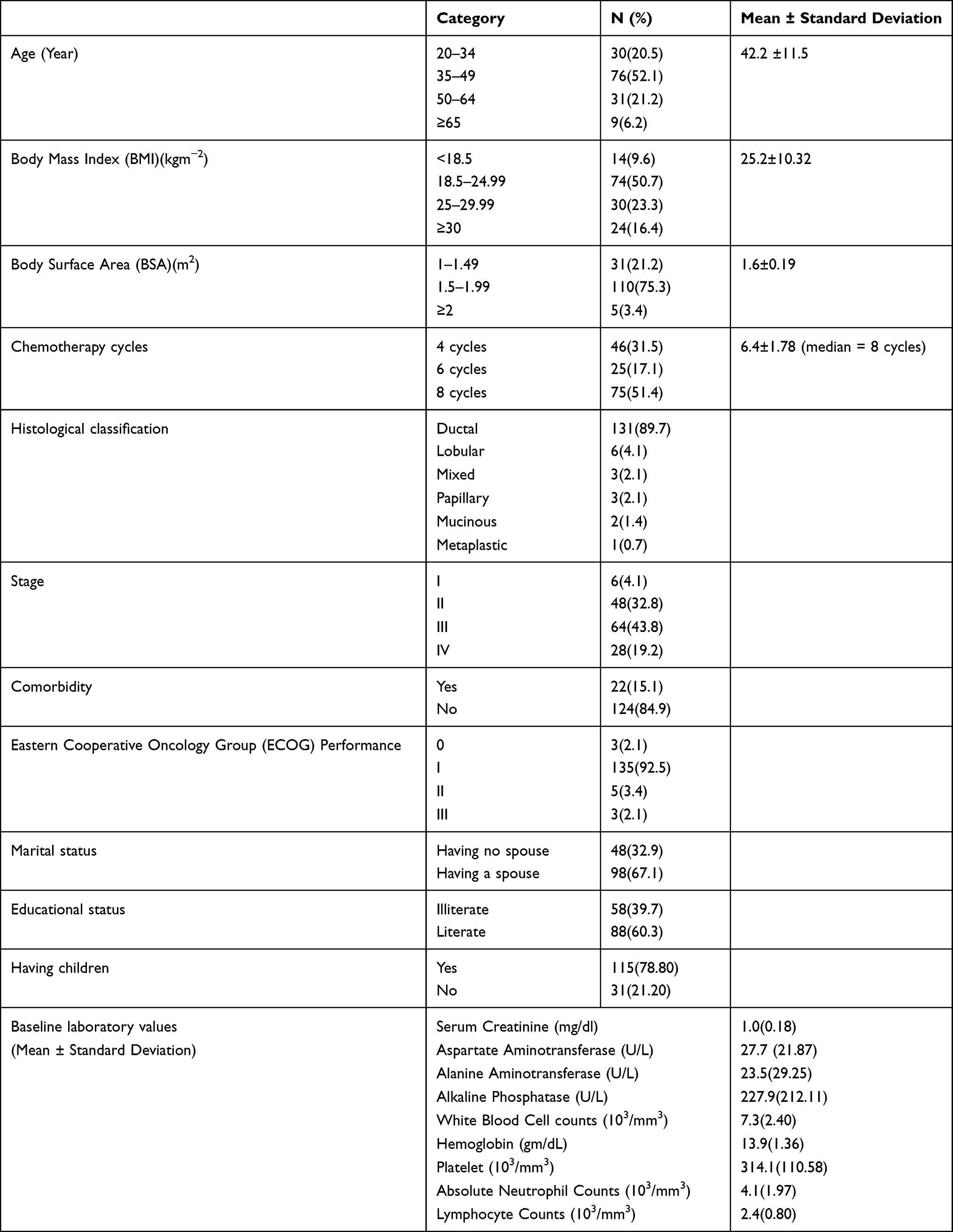 |
Table 1 Socio-Demographic and Clinical Characteristics of Women with Breast Cancer on AC and AC-T Chemotherapy at TASH, N=146 |
Quality of Life Pattern Among Breast Cancer Patients on AC and AC-T Regimen
The Pattern of Quality of Life (EORTC QLQ-C30 Scales) Scores Among Breast Cancer Patients on Chemotherapy
The results from GLM repeated measures in Figure 1 and a linear mixed model in Table 2 depicted, global health status was declined by 15.78 points from baseline to the end of cycle 2. Likewise, cognitive functioning, emotional functioning, social functioning, role functioning, and physical functioning of the patients were significantly (P≤0.001) decreased by 9.02, 12.21, 16.67, 17.63, and 28.99 points from baseline/pretreatment score to the end of cycle 2 score respectively. After the end of cycle 2, GHS increased slowly to 6.85 (P=0.02) above baseline score at the end of the chemotherapy course whereas emotional functioning was also increased to 4.44 points (P=0.155) below the pretreatment score by the end of cycle 8. Moreover, role functioning (28.99 to 22.67 points below the baseline score) and physical functioning (17.63 to 18.58 points below the baseline score) subscales showed a kind stable pattern between cycle 2 and cycle 6, though they increased steeply (ie recovered) towards 11.39 (P=0.000) and 8.11 (P=0.039) points below pretreatment level by the end of cycle 8, respectively. However, the cognitive functioning of the patients was showed a decreasing pattern from baseline to the end of cycle 8 (ie, 17.24 points below baseline score, P=0.000) though social functioning started to recover from its lowest score (32.70 points below pretreatment score, P=0.000) at the end of cycle 6 to 22.80 points below pretreatment score (P=0.000) at the end of cycle 8 (see Figure 1 and Table 2).
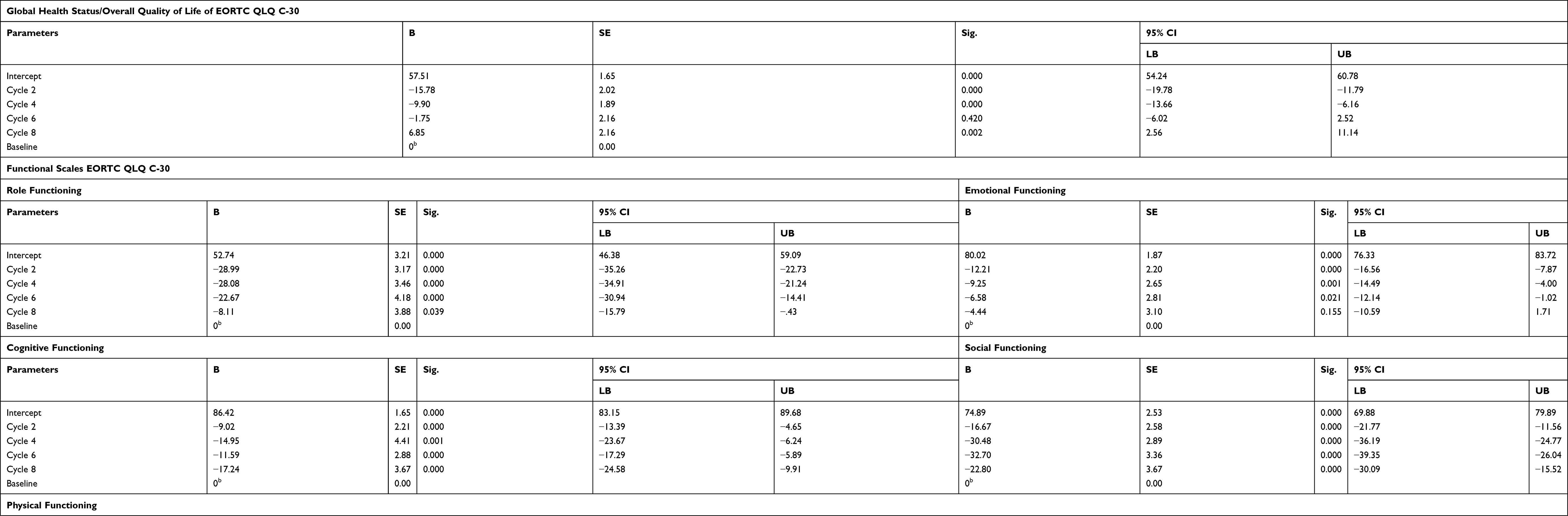 |
Table 2 EORTC QLQ-C30 Global Health Status and Functional Scales Score Over Time Among Breast Cancer Patients on AC and AC-T Chemotherapy, from January 1 to September 30, 2017 GC (Using a Linear Mixed Model) |
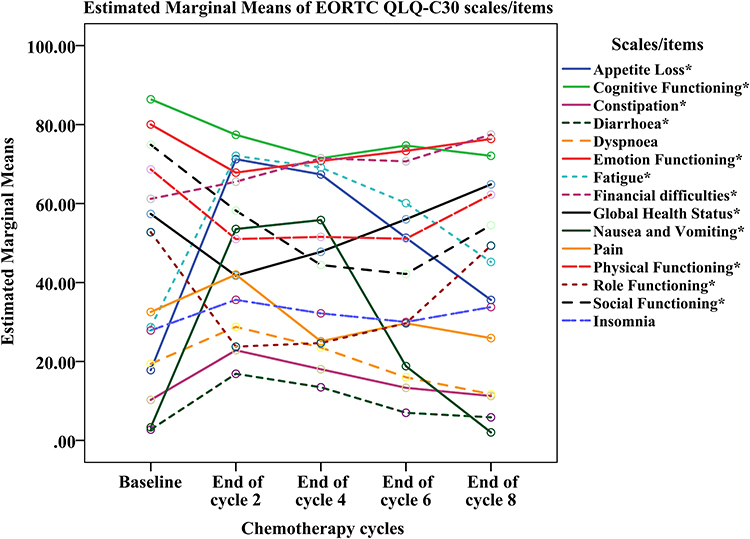 |
Figure 1 Patterns of quality of life (EORTC QLQ C-30 scales) score over time among women with breast cancer on chemotherapy, from January 1 to September 30, 2017 GC, N=146 (using GLM repeated measures). *Those quality of life domains score with both statistically and clinically significant deterioration at least once from baseline score. |
The symptom scales/items of EORTC QLQ-C30 such as constipation, diarrhea, fatigue, nausea and vomiting, and appetite loss scores were increased by 12.56, 14.16, 43.38, 50.23, and 53.42 points from baseline score to the end cycle 2 score, respectively (see Table 3). However, after a steep increment from baseline to the end of cycle 2, nausea and vomiting, fatigue, and appetite loss were started declining to 1.27 points (P=0.295) below pretreatment score, 18.09 (P=0.000) and 19.57 (P=0.000) points above pretreatment score, respectively, after the end cycle 4. Moreover, constipation, diarrhea, and dyspnea scores were started to decrease flatly from their higher score at cycle 2 to the end of chemotherapy cycles (ie, cycle 8) on contrary to insomnia which started to deteriorate again after cycle 6 (ie, from 2.43 to 4.70points above pretreatment score). However, the financial difficulties of the patients were increased from baseline to the end of cycle 8 (17.13 points above pretreatment score, P=0.000) (for more please see Figure 1 and Table 3).
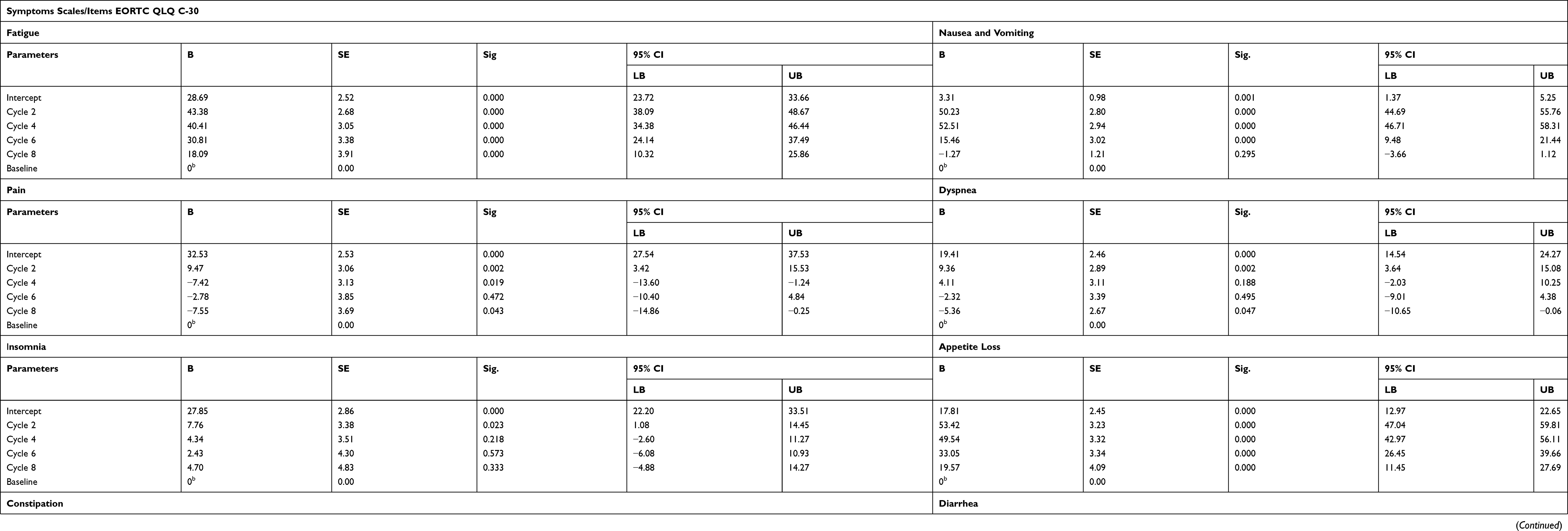 |
Table 3 EORTC QLQ C-30 Items/Symptom Scales Score Over Time Among Breast Cancer Patients on AC and AC-T Chemotherapy, from January 1 to September 30, 2017 GC (Using a Linear Mixed Model) |
In general, during the first two cycles of chemotherapy, the GHS and majority of functional scales and symptom scales/items of EORTC QLQ-C30 showed a steep decreasing and increasing pattern, respectively. Overall QoL, all functional scales (except cognitive functioning) and symptom scales/items (except dyspnea, insomnia, and pain score) of EORTC QLQ-C30 deteriorated significantly both clinically (ie change at least by 10 points from the baseline) and statistically (ie P≤0.05) at least during the first two cycles of chemotherapy (Figure 1, and Tables 2 and 3).
The Pattern of Quality of Life (EORTC QLQ-BR23 Scales) Scores Among Breast Cancer Patients on Chemotherapy
As it is depicted in Figure 2 (results from GLM repeated measures) and Table 5 (results generated from the linear mixed model), systemic therapy side effects were increased by 37.83 (P=0.000) points above the pretreatment score by the end of the cycle 2 score. However, starting from the end of cycle 4 (38.88 points above pretreatment score, P=0.000), systemic therapy side effects were decreased (ie, recovered) towards 25.74 points above the pretreatment score (P=0.000). Also, the highest score for an upset by hair loss was detected at the end of cycle 2 (16.28 points above score at cycle 8, P=0.000) and the lowest score at the end of cycle 6 (10.90 points below the score at cycle 8, P=0.000) but it started to deteriorate afterward (see Figure 2 and Table 5). On contrary to the systemic therapy side effects and upset by hair loss escalation during the first two cycles of chemotherapy, breast symptoms and arm symptoms were slowly decreased (ie, improved) to 14.85 (P=0.000) and 19.79 (P=0.000) points below the pretreatment score, respectively, by the end cycle 8.
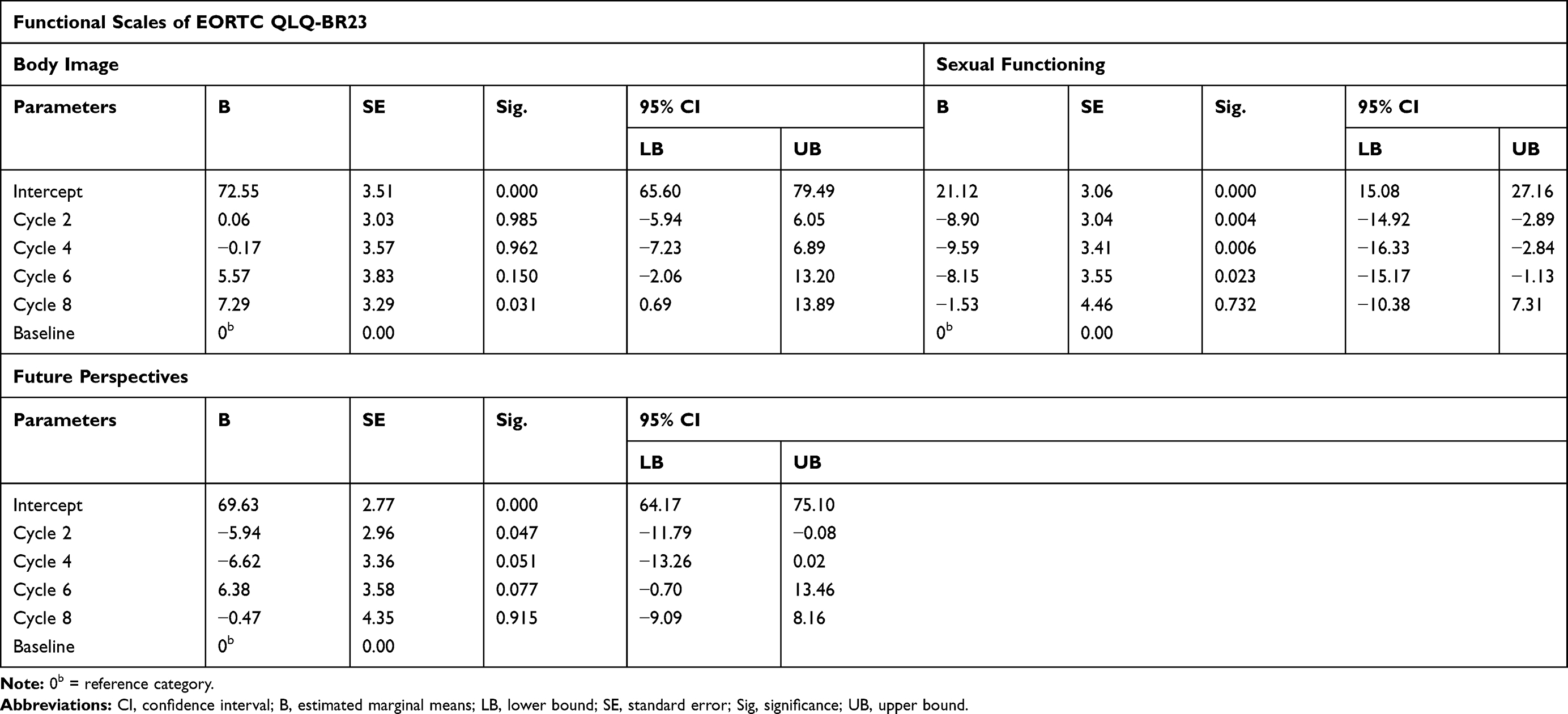 |
Table 4 EORTC QLQ-BR23 Functional Scales Score Over Time Among Breast Cancer Patients on Chemotherapy, from January 1 to September 30, 2017 GC (Using a Linear Mixed Model) |
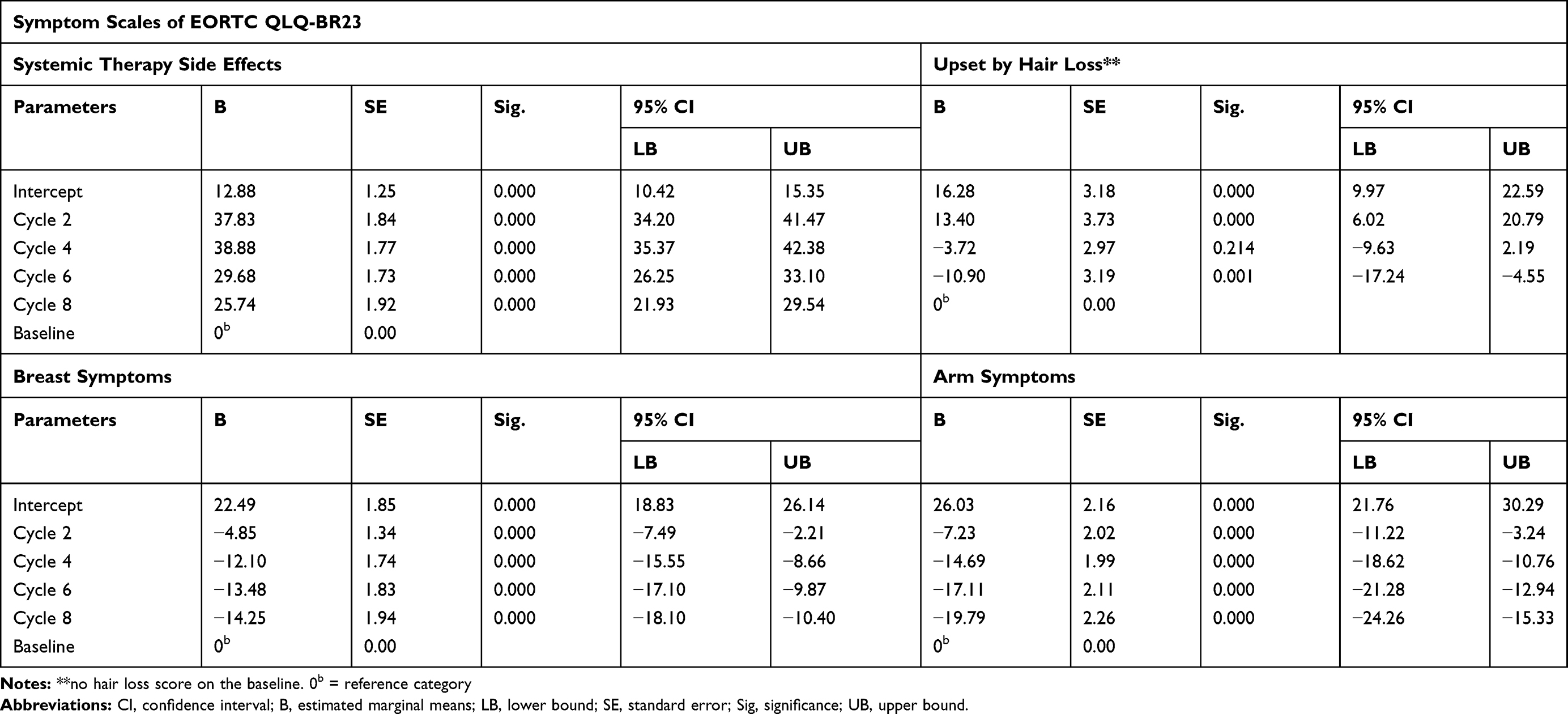 |
Table 5 EORTC QLQ-BR23 Symptom Scales Score Over Time Among Breast Cancer Patients on Chemotherapy, from January 1 to September 30, 2017 GC (Using a Linear Mixed Model) |
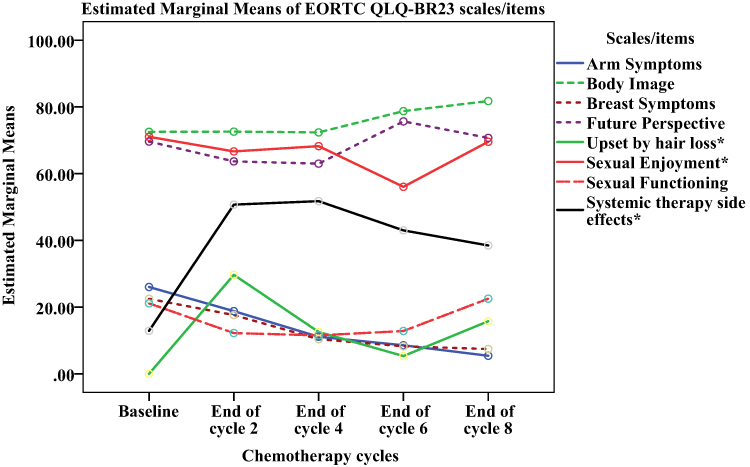 |
Figure 2 Patterns of quality of life score (EORTC QLQ-BR23 scales) over time among women with breast cancer on chemotherapy, from January 1 to September 30, 2017 GC, N=146 (using GLM repeated measures). *Those quality of life domains score with both statistically and clinically significant deterioration (ie except breast and arm symptoms) at least once from baseline score. |
Among the functional scales of EORTC QLQ-BR23, body image score was slightly increased from baseline to the end of cycle 8 (ie, 7.29 points above pretreatment score, P=0.031). However, future perspectives and sexual functioning showed a decreasing pattern from pretreatment to the end of cycle 4 (ie, 6.62 points below the pretreatment score, P= 0.051) and cycle 6 (ie, 9.59 points below the pretreatment score, P=0.006), respectively, even though they increased towards to pretreatment level afterward (for more please see Figure 2 and Table 4).
Overall, except for body image, breast symptoms, arm symptoms, future perspectives, and sexual functioning, all EORTC QLQ-BR23 dimensions were deteriorated significantly (ie, both statistically and clinically) during chemotherapy (Figure 2).
Factors Affecting the Quality of Life of Study Participants
Socio-Demographic and Clinical-Pathological Factors
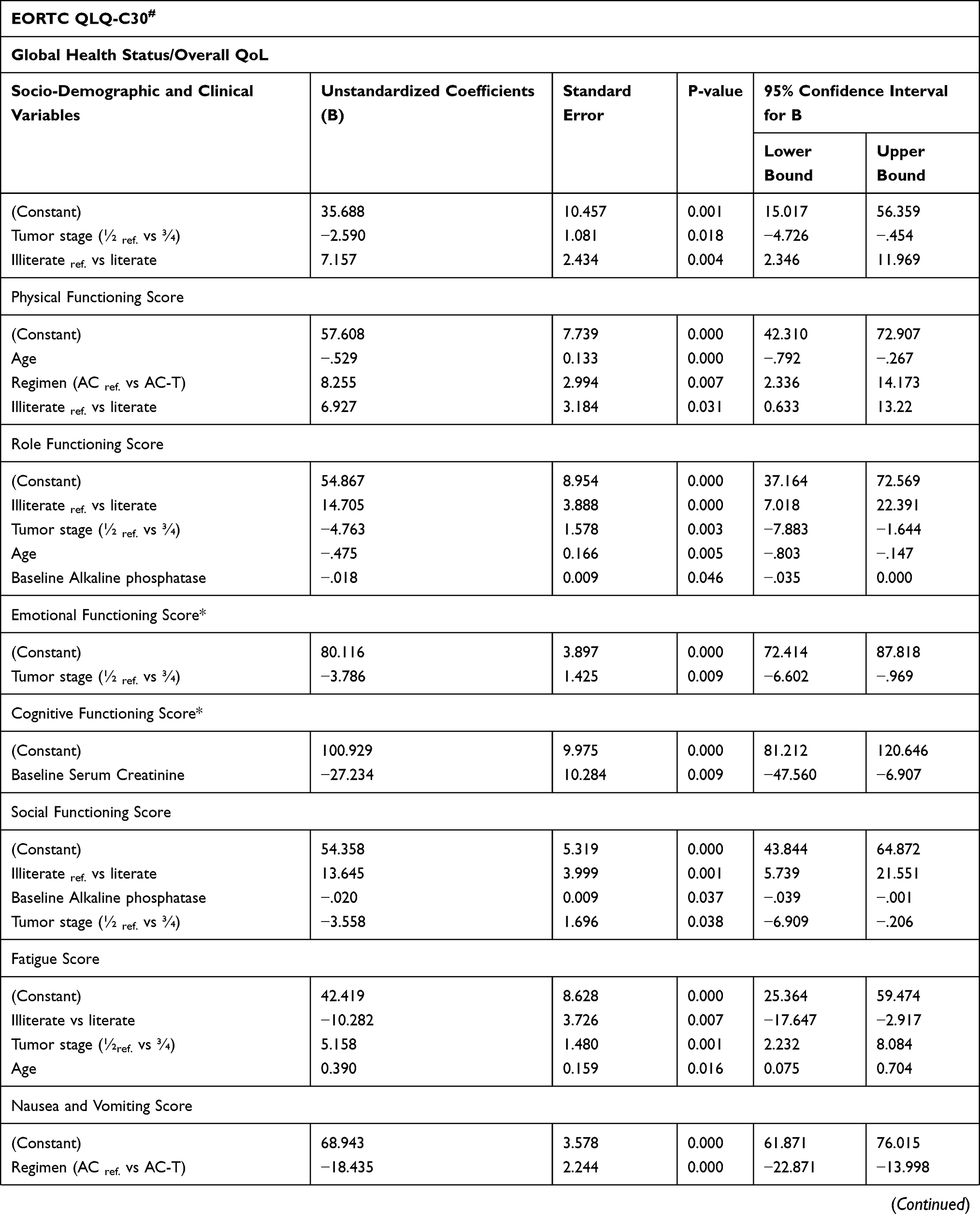
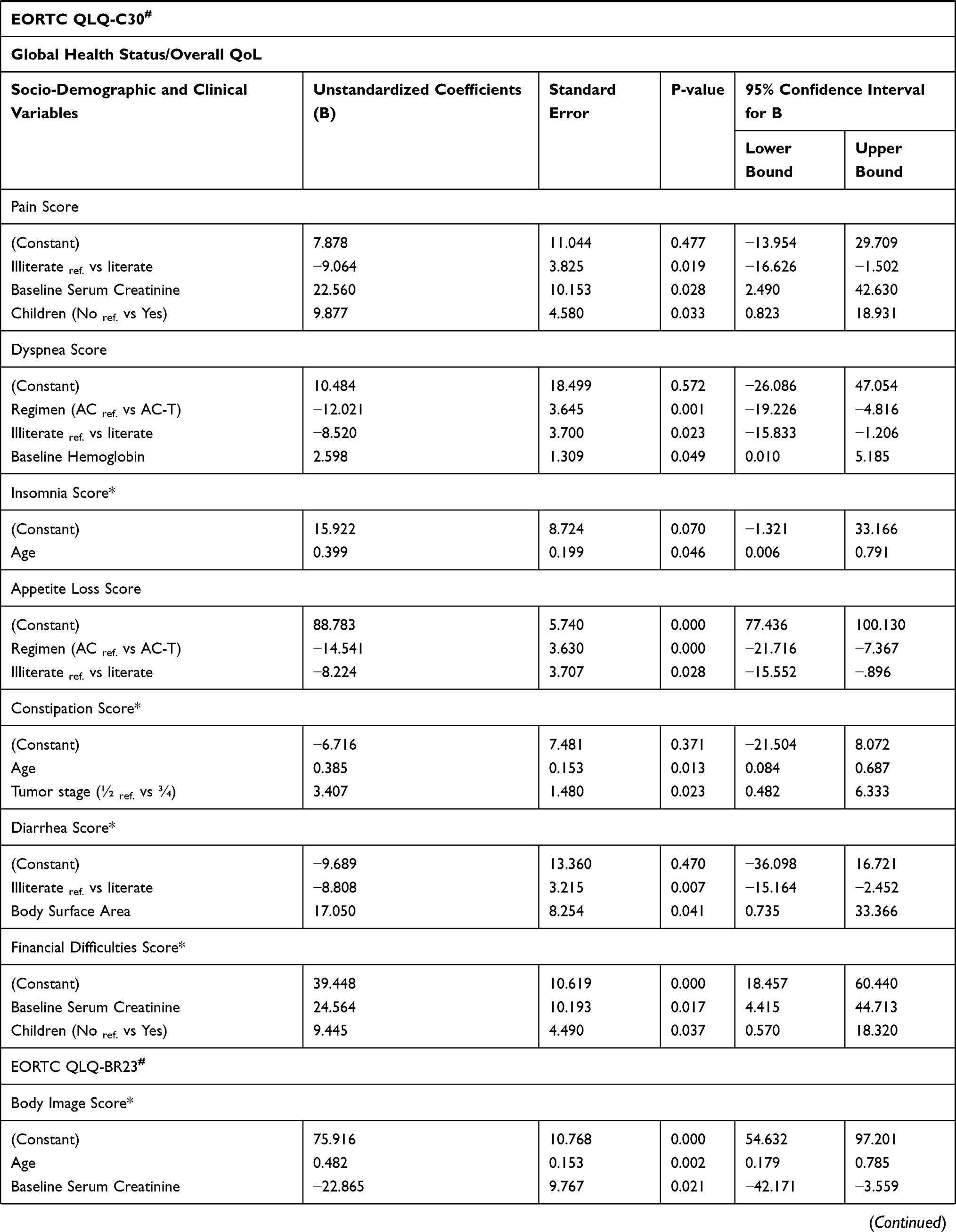
Literate patients had higher Global Health Status, physical, role, social functioning and sexual functioning scores (6.927≤B≤14.705, P≤0.043) than illiterate ones. Moreover, literate patients had lower fatigue, pain, dyspnea, appetite loss, diarrhea, and systemic therapy side effects scores (−10.282≤B≤−5.318, P≤0.028) than their counterparts. Tumor stage ¾ significantly impairs GHS, role, emotional, social functioning, sexual functioning, and future perspectives score (−4.763≤B≤−2.590, P≤0.038) of the patients than patients with tumor stage ½. Besides, it also causes deterioration (1.977≤B≤5.158, P≤0.023) of fatigue, constipation, and breast symptoms score.
Increasing age was also associated with increment (0.385≤B≤0.567, P≤0.033) in-body image, future perspectives, fatigue, insomnia, and constipation scores on contrary to its association with decrement (−0.529≤B≤-0.366, P≤0.033) in physical functioning, role functioning, and upset by hair loss score (Table 6).
 |
 |
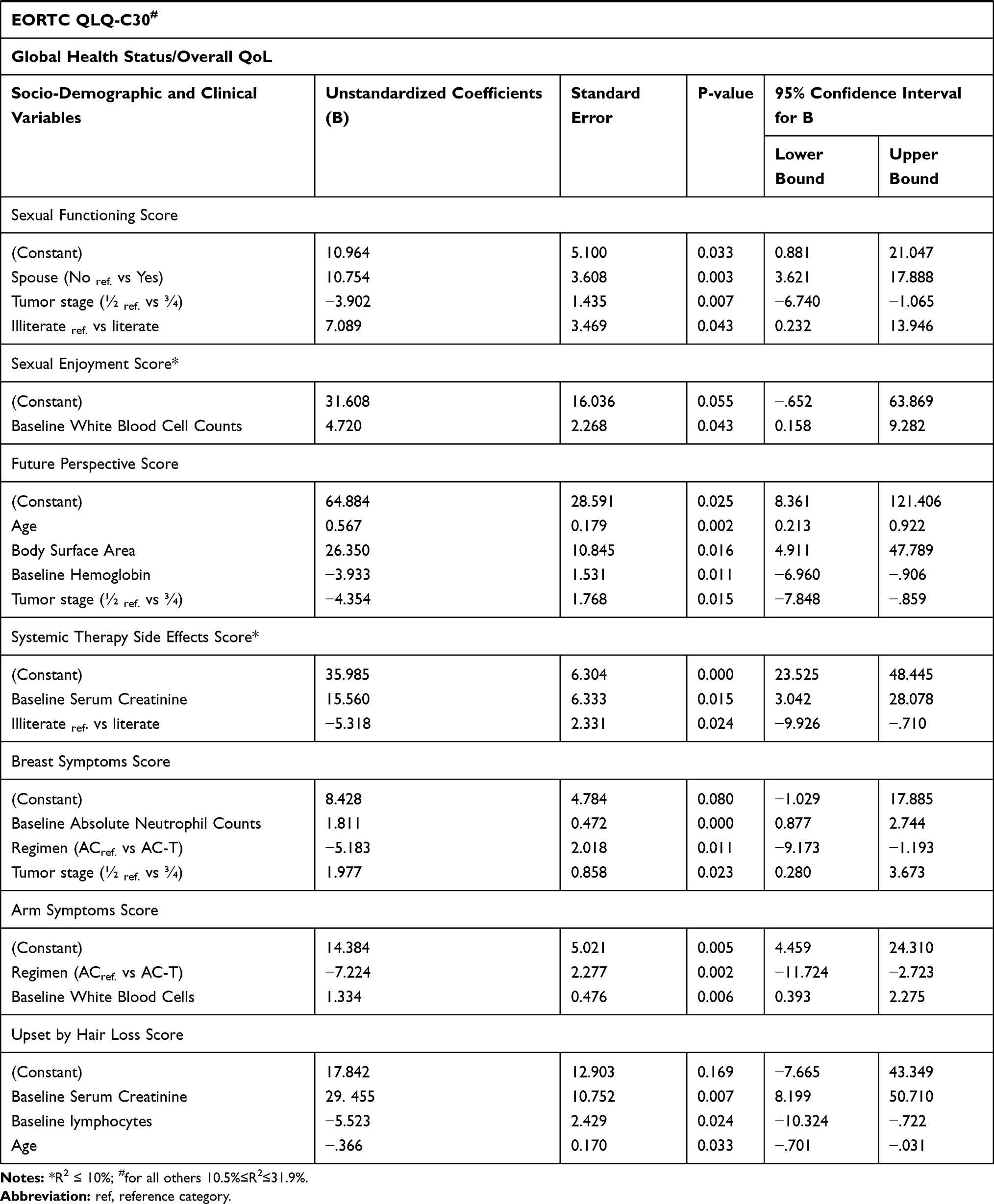 |
Table 6 Socio-Demographic and Clinical Factors Associated with Deterioration of Quality of Life on Stepwise Linear Regression, from January 1 to September 30, 2017 GC |
Patients who received the AC-T regimen had lower (−18.46≤B≤−12.02, P≤0.001) nausea and vomiting, dyspnea, and appetite loss than those who received the AC regimen. Having children was among the contributing factor for having higher (9.45≤B≤9.87, P≤0.037) pain and financial problems score than those who had no children.
Moreover, baseline serum creatinine was a positive predictor (15.560≤B≤29.455, P≤0.007) for symptom scales such as pain, financial difficulties, systemic therapy side effects, and upset by hair loss scores on contrary to cognitive functioning (B=−27.234, P=0.009). Baseline alkaline phosphatase is also negatively associated (−0.018≤B≤-0.020, P≤0.046) with the role and social functioning scores. Having had higher baseline absolute neutrophil counts (B=1.81, P=0.000) and white blood cell counts (B=1.334, P=0.006) was associated with higher breast symptoms and arm symptoms score, respectively (see Table 6).
The Effect of AC and AC-T Chemotherapy’s Toxicities on Quality of Life Among Women with Breast Cancer in Ethiopia
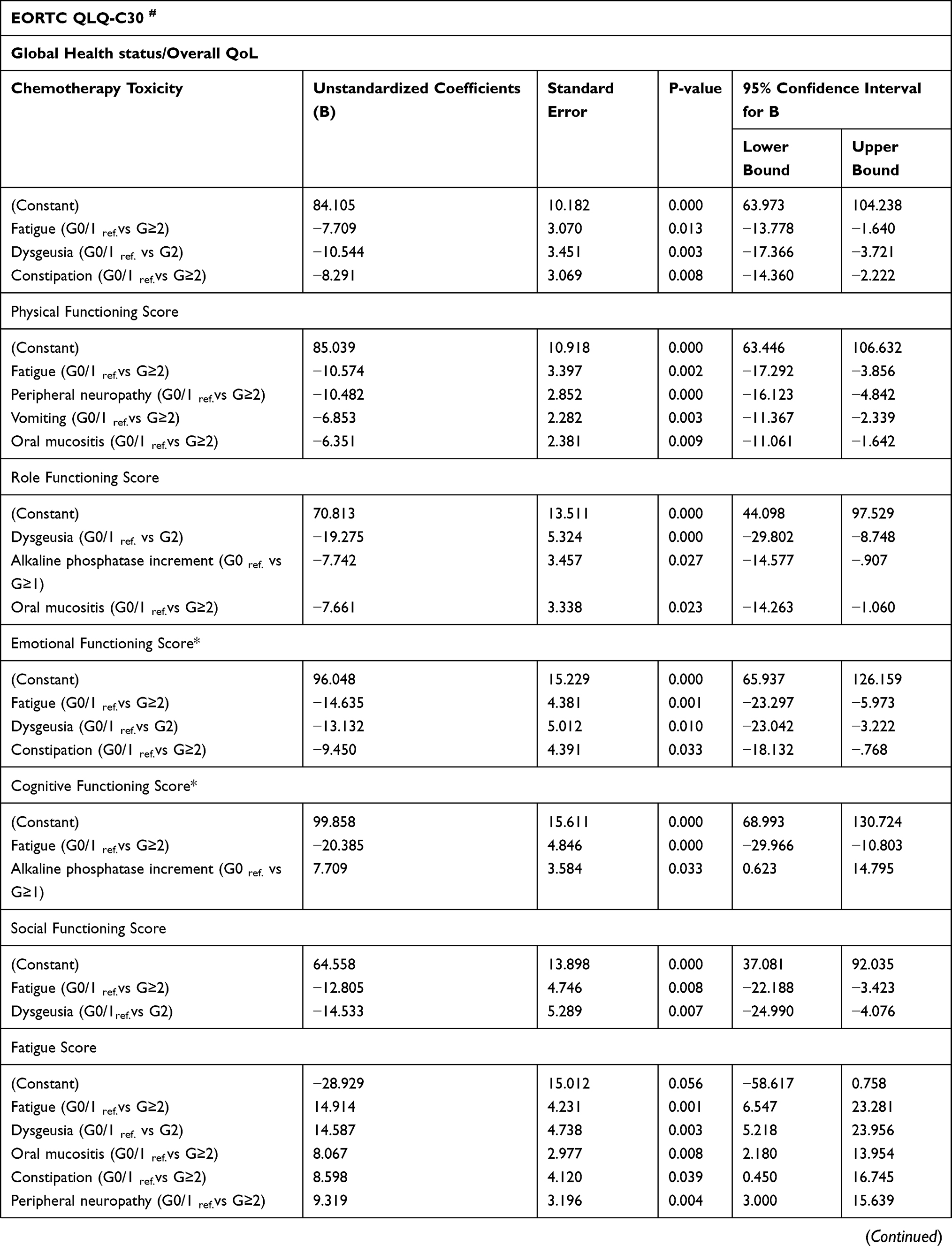
Upon adjusting for baseline quality of life score, significant socio-demographic and clinical cofounding factors, grade 2 and above fatigue (−25.320≤B≤−7.709, P≤0.013) was significantly associated with deterioration of Global health status, physical functioning, emotional functioning, cognitive functioning, social functioning, sexual functioning and sexual enjoyment of the patients than those with lower grade fatigue. It is also significantly associated with the deterioration (9.620≤B≤14.914, P≤0.043) of symptom scales such as fatigue, insomnia, appetite loss, and financial difficulties (Table 7).
Grade 2 dysgeusia causes a significant impairment (−19.275≤B≤−10.544, P≤0.025) in global health status, role functioning, emotional functioning, social functioning, body image, future perspectives of the patients than grade 0/1 dysgeusia. It is also frequently associated with deterioration (13.352≤B≤22.962, P≤0.003) of symptom scales such as fatigue, pain, dyspnea, insomnia, appetite loss, systemic therapy side effects, and upset by hair loss scores.
Furthermore, grade 2 and above constipation (8.355≤B≤26.451, P≤0.039) was frequently associated with the deterioration of symptom scales like fatigue, pain, dyspnea, constipation, diarrhea, and systemic therapy side effects than its counterparts. Besides, it is also negatively (−9.450≤B≤−8.291, P≤0.033) associated with the global health status and emotional functioning of the patients.
Grade 2 and above peripheral neuropathy was also the other non-hematological toxicity of AC and AC-T chemotherapy that causes the significant deterioration of physical functioning (B=−10.482, P=0.000) and symptom scales (4.819≤B≤9.557, P≤0.014) such as fatigue, dyspnea, and systemic therapy side effect. Also, grade 2 and above oral mucositis was associated with significant impairment of physical and role functioning (−7.661≤B≤−6.351, P≤0.023), and fatigue and financial difficulties of the patients (7.963≤B≤8.067, P≤0.010).
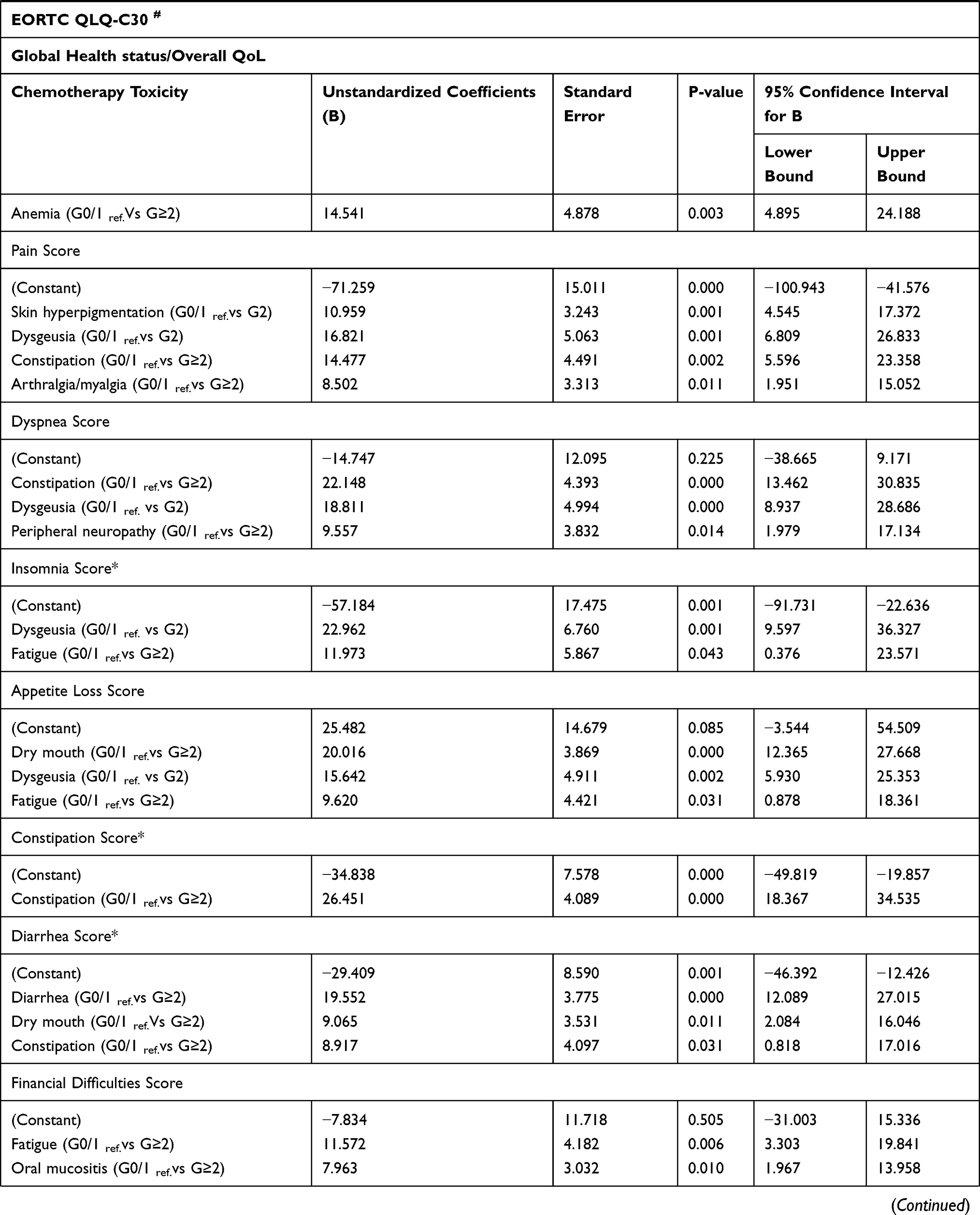
Some quality of life deteriorations were mirror images of their chemotherapy’s toxicity. For examples, those suffering from grade≥2 dry mouth and dysgeusia had significantly higher appetite loss score (15.64≤B≤20.12, P≤0.002); grade≥2 constipation for higher constipation score (B= 26.45, P≤0.001), grade≥2 diarrhea for higher diarrheal score (B=19.55, P≤0.001) and grade≥2 myalgia and arthralgia for higher pain score (B=8.50, P=0.011), grade≥2 skin hyperpigmentation for a higher upset by hair loss score (B= 7.715, P=0.033) and lower body image (B=−6.189, P=0.05). Moreover, some laboratory result based toxicities like grade 2 and above lymphopenia was associated with lower arm symptoms (B=−6.607, P=0.009), grade≥2 anemia associated with higher fatigue score (B=14.541, P=0.003), and grade≥1 alkaline phosphatase increment was also associated with lower role functioning score (B=−7.742, P=0.027) than their lower-grade toxicities. For more effect of AC and AC-T regimen’s toxicities on quality of life please see Table 7.
 |
 |
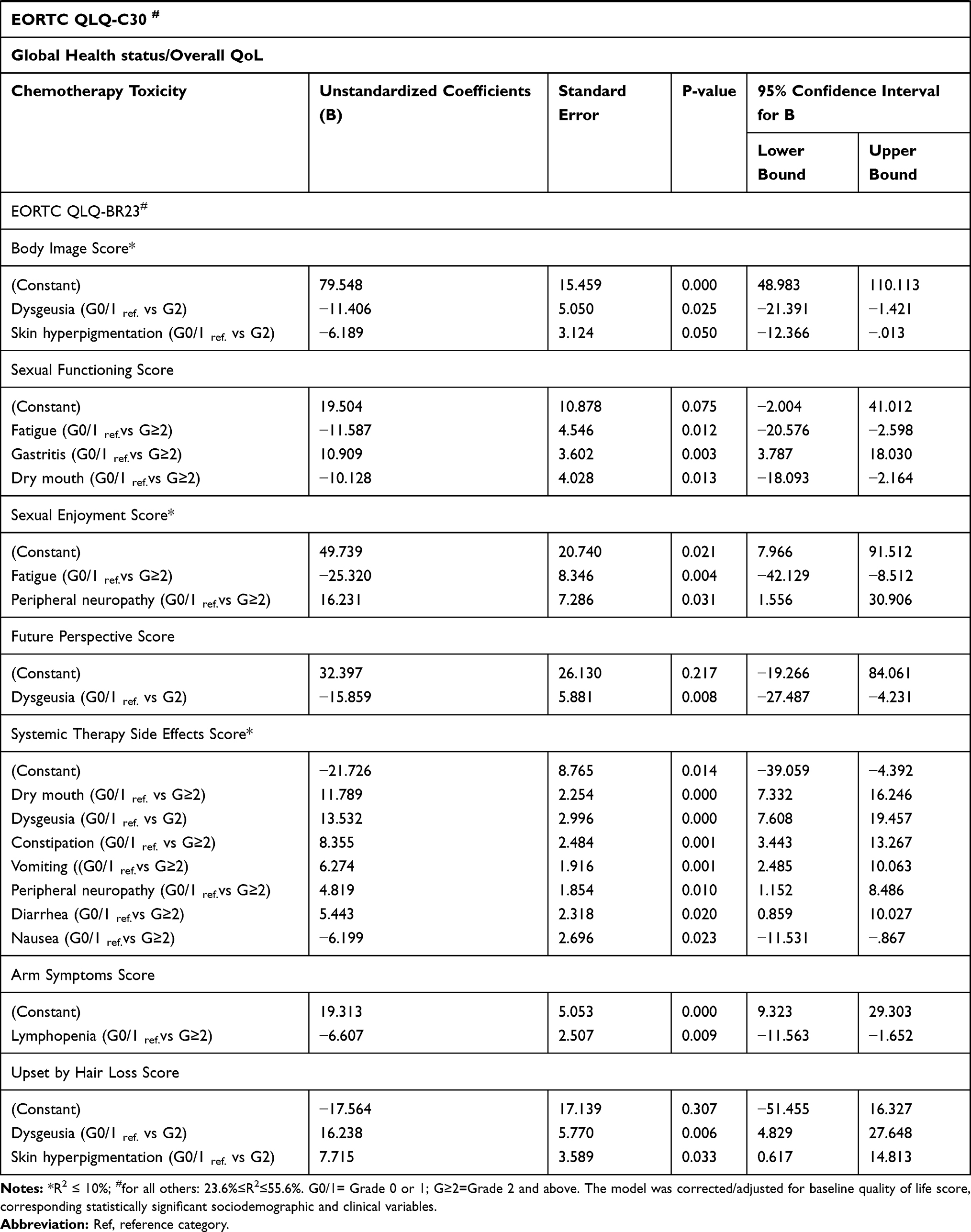 |
Table 7 The Effect of AC and AC-T Regimen’s Toxicities on Quality of Life Among Women with Breast Cancer in Ethiopia, from January 1 to September 30, 2017 GC |
Discussion
Breast cancer chemotherapies harm the quality of life17,32 even though it increases overall survival (OS) and disease-free survival (DFS).33–36 As a result, understanding the effect of breast cancer treatment on patients’ quality of life has been the central clinical and research question.37 The trial of Hall and his coworker38 showed that overall QoL/GHS and systemic therapy side effects significantly deteriorated clinically from baseline to throughout therapy. A minimum clinically meaningful difference/deterioration is considered to be 10 points, using an established method of interpretation for the EORTC QLQ-C30 scores.39
Our study found that the global health status score, physical functioning, role functioning, and emotional functioning scores of the study participants were decreasing steeply from baseline to the end of cycle 2 by more than 12 points and increasing slowly after the end of cycle 2 to the end of cycle 8. Different cross-sectional studies also revealed that different functional dimensions of QoL and GHS score were low among breast cancer patients chemotherapy.40–42 Despite the global health status was increased to 6.85 points above the pretreatment score by the end of cycle 8 (P=0.020), physical, role, and emotional functioning of the patients persisted below the pretreatment score by 11.39 (P=0.000), 8.11 (P=0.039) and 4.44 (P=0.155), respectively, by the end of cycle 8. Conversely, a study also reported that women who received chemotherapy will have worse QOL even at a 5-month follow-up.43 However, the social and cognitive functioning of the patients were shown a persistent worsening pattern from baseline to the end of cycle 8. The psychological distress,44 worsening of physical well-being43 and social domain45 were frequent among patients with breast cancer on chemotherapy. Cross-sectional studies in Ethiopia also indicated that social and psychological domains and social support were found to be poor in women with breast cancer.42,45 Therefore, implementing appropriate psychosocial support and social networks might improve the functional dimensions of QoL.42,46
Even though different cross-sectional studies reported that the quality of life of breast cancer patients under chemotherapy treatment is poor,45,47 our prospective study found that the deterioration of quality of life among women with breast cancer depends on the domain/scales of quality of life and the cycle of chemotherapy. Likely, on contrary to the GHS and functional scales of scores, body image scores of the patients were slightly increased from baseline to the end of cycle 8 (ie, 7.29 points above pretreatment score, P=0.031). However, future perspectives and sexual functioning showed a decreasing pattern from pretreatment to the end of cycle 4 (ie, 6.62 points below the pretreatment score, P=0.051) and cycle 6 (ie, 9.59 points below the pretreatment score, P=0.006), respectively, even though they increased towards to pretreatment level afterward. The study by Horwitz et al.43 supports our finding that chemotherapy harmed women’s sexual functioning (P=0.01) and their physical well-being (P=0.09).
In addition to the functional scales, the symptom scales/items of the quality of life of the patients with cancer got worse (as shown by an increase in scores) during chemotherapy.45,47,48 Conversely, fatigue, appetite loss, and nausea and vomiting scores were increased (ie, deteriorated) from baseline to end of cycle 2 by more than 40 points while they started to decrease slowly from the end of cycle 2 to cycle 8. Nausea and vomiting score at the end of cycle 8 was 1.27 points below the pretreatment score (P=0.295), whereas fatigue and appetite loss were decreased to 18.09 (P=0.000) and 19.57 (P=0.000) points above the pretreatment score. Therefore, these results indicated that there is a significant clinical and statistical worsening as compared to baseline for fatigue and appetite loss dimensions even by the end of all chemotherapy courses.
Shortness of breath/dyspnea, pain, and insomnia were also among the dimensions of quality of life that were impaired among breast cancer women who received chemotherapy.43,49 On contrary to fatigue, appetite loss, and nausea and vomiting subscale, maximum score difference observed for dyspnea, pain, and insomnia from baseline scores were 9.47 points which were less than 10 points to reach significant clinical deterioration despite their statistically significant impairment (P≤0.023) during the first two cycles of chemotherapy.
Except from financial difficulties in which its worsening were persistently increased from baseline to end of cycle 8 (P=0.000), pain, dyspnea, insomnia, constipation, and diarrhea scores among the study participants were recovered to scores that had no statistical and clinical significant worsening from baseline score by the end of cycle 8. Different cross-sectional studies in Ethiopia also indicated that financial difficulties were frequently reported, in addition to other dimensions, among patients with cancer.45,48,50
The other dimensions of quality of life frequently affected during breast cancer chemotherapy were systemic therapy side effects.38,42,51 Our current finding also indicated that the systemic therapy side effects and upset by hair loss scores were increased steeply from baseline to the end of cycle 2 at least by 30 points. However, starting from the end of cycle 4, systemic therapy side effects were decreased (ie, recovered) towards 25.74 (P=0.000) points above the pretreatment score. This indicates that despite its significant decrements from the end of cycle 4, systemic therapy side effects remained statistically and clinically meaningful worsening even by the end of cycle 8. Moreover, the upset by hair loss score was started to worsening after it reached the pretreatment level in cycle 6. On contrary to the other symptom scales, breast symptoms and arm symptoms were decreasing (i.e, improved) at least by 14 points from baseline to the end of cycle 8.
As it was demonstrated in our finding, different cross-sectional studies reported that the majority of the quality of life dimensions were deteriorated significantly (ie, clinically and/or statistically) in the first two/three cycles of chemotherapy than higher cycles,9,39,47 and it improves once chemotherapy is completed or near to the end.52,53 Overall, our finding indicated that overall QoL/global health status and functional scales (ie physical, role, emotional, social, and sexual enjoyment), except for cognitive function significantly decreased both clinically (decreased at least by ten and more points) and statistically (P≤0.05) in particular from baseline score to the end of cycle 2. Except for cognitive and social functioning which persistently declined from baseline to the end of cycle 8, others were started to recover (ie, increased) after the end of cycle 2 and approached pre-treatment scores by the end of all treatment courses. However, despite their statistically significant deterioration (P≤0.05) from baseline, the other functional scales such as sexual functioning, body image, and future perspectives of the patients did not reach clinically meaningful deterioration during any course of chemotherapy.
On contrary to the functional scales above, the symptom scales such as nausea and vomiting, fatigue, appetite loss, constipation, diarrhea, systemic therapy side effects, and upset by hair loss of the patients were significantly deteriorated (ie, increased) both clinically and statistically from baseline score to the end of cycle 2, though they showed declining pattern afterward. However, dyspnea, insomnia, and pain did not reach clinically meaningful worsening even though their deterioration was statistically significant (P≤0.05) in particular during the first two cycles of chemotherapy. Fortunately, on opposite to all other symptom scales/items, breast symptoms, and arm symptoms of the patients were decreased even during the first two cycles to the end of cycle 8. As it was learned from our finding, the majority of the quality of life dimensions that were deteriorated during the first two cycles of chemotherapy were started to improve after the end of cycle 2 or cycle 4. This might be happened due to the so-called “response shift” characterized by an internal reframing of the patient concerning their perception of health.54
Decreasing quality of life implicates that an increased dependence of the patients on family members or caregivers, and it might also cause an increased state of immunosuppression (ie, increased risk of infectious complications) and which ultimately affects the psychology of the cancer patient.55
The deterioration of different dimensions of quality of life during chemotherapy and its improvements near and/or after the end of chemotherapy indicates that it is obviously due to adverse events associated with chemotherapy.56–58 Unfortunately, on top of that, due to sociodemographic, clinical, and treatment-related factors, as well as behavioral and psychosocial factors,59 the quality of life of Ethiopians with cancer was found below.50
Multidimensional QoL assessment showed that breast cancer chemotherapy’s toxicities mainly affect physical functioning and global quality of life.18,32,60 Likewise, among the AC and AC-T chemotherapy toxicities observed in our study,25 grade 2 and above fatigue, dysgeusia, and constipation negatively affect the overall quality of life/Global Health Status of the patients (−10.544≤B≤−7.709, P≤0.013). Furthermore, the functional subscales such as physical functioning, role functioning, social functioning, emotional functioning, cognitive functioning, sexual functioning, sexual enjoyment, body image, and future perspectives were also negatively affected (−25.320≤B≤−6.351, P≤0.033) at least by one or more grade≥2 AC and AC-T chemotherapy toxicities like fatigue, dysgeusia, constipation, vomiting, oral mucositis, and peripheral neuropathy. Conversely, a cross-sectional study in Spain found that nausea, dysgeusia, peripheral neuropathy, loss of appetite, myalgia, and peripheral edema due to cancer chemotherapy harmed the quality of life of those who did not experience these toxicities.55
Studies elucidated that breast cancer chemotherapy impairs cognitive functions61 such as problems with memory, attention, processing speed, and executive functioning.3 And fatigue (B=−20.385, P≤0.001) was the only non-hematological toxicity that negatively associated with impairment of cognitive functioning among our study participants. As it was explained above, the social functioning of our study participants persistently decreased from baseline to the end of the chemotherapy course. Managing fatigue and dysgeusia in these patients could be a solution since grade≥2 fatigue (P=0.008) and dysgeusia (P=0.007) were negatively associated with decrements in social functioning among our study participants. Our study also revealed that illiterate and patients with higher alkaline phosphatase and tumor stage ¾ had a lower social functioning status than their counterparts. Hence, they might need some fatigue and dysgeusia coping-up mechanisms in particular among illiterate and with tumor stage ¾ to overcome their social functioning problem.
The symptom scales were also frequently deteriorated due to breast cancer chemotherapy’s toxicities in our study participants. For example, the fatigue score was significantly increased (8.067≤B≤14.914, P≤0.039) due to grade≥2 fatigue, dysgeusia, constipation, oral mucositis, and peripheral neuropathy. The systemic therapy side effects score was also significantly increased (4.819≤B≤13.532, P≤0.020) due to grade 2 to above dry mouth, dysgeusia, constipation, diarrhea, vomiting, and peripheral neuropathy.
As it was elucidated in our finding, different studies indicated that fatigue is the symptom that had, by far, the largest impact (ie, strong predictor) on limiting function and on overall QoL in breast cancer patients, unlike other toxicities.62–65 Conversely, in our study, in addition to its impact on GHS and functional scales, grade 2 and above fatigue was significantly associated with the worsening of different symptom scales/items of QoL. For example, it was associated with increased fatigue (B=14.914, P=0.001), appetite loss (B=9.620, P=0.031), insomnia (B=11.973, P=0.043) and financial problems (B=11.572, P=0.006) scores. Different studies in Ethiopia and elsewhere also indicated that cancer and treatment-related fatigue is common among cancer patients who have received chemotherapy and results in substantial adverse physical, psychosocial, and economic consequences for patients that significantly worsened QoL.44,47,66
Henceforth, as the grade≥2 fatigue was frequently associated with deterioration of multidimensional quality of life (ie, GHS, functional scales, and symptoms scales/items) of the patients with breast cancer on AC or AC-T chemotherapy, devising fatigue coping mechanism like yoga type physical exercise among the breast cancer patients have paramount importance for the improvement of overall quality of life.67–69
Like that of fatigue, grade 2 dysgeusia was also frequently associated with impairment of multidimensional QoL among breast cancer patients who received AC or AC-T chemotherapy. Conversely, it was associated with the worsening of GHS (P=0.003), role functioning (P=0.000), emotional functioning (P=0.010), social functioning (P=0.007), body image (P=0.025), future perspectives (P=0.008), fatigue (P=0.003), pain (P=0.001), dyspnea (P=0.000), insomnia (P=0.001), appetite loss (P=0.002), systemic therapy side effects (P=0.000) and upset by hair loss (P=0.006). In line with our study, Ponticelli et al and other authors found that patients with dysgeusia have a higher probability of having a worse QoL.70,71
Prieto-callejero et al.55 reported that peripheral neuropathy as the toxicity of chemotherapy affects diverse aspects of quality of life in those patients who received taxane-containing regimen. Also, constipation is has a highly significant effect on a patient’s well-being.72 Likely, in our case, grade≥2 peripheral neuropathy and constipation (4.819≤B≤26.451, P≤0.039) were also the other toxicities of AC and AC-T breast cancer chemotherapy that frequently associated with deterioration of symptom scales/items like fatigue, pain, dyspnea, constipation, diarrhea and/or systemic therapy side effects than their lower-grade counterparts. One preliminary finding reported that regional cooling of hands and feet might have good effectiveness and tolerability, in reducing the symptoms of chemotherapy-induced peripheral neuropathy, hence improving the different dimensions of quality of life affected by it.73
The above finding of our study supported the evidence that all chemotherapy’s toxicities do not equally deteriorate the quality of life.74,75 On the other hand, patients’ self-reports quality of life domains mirrored those of their chemotherapy side effects.38 For instance, in grade 2 and above, dry mouth and dysgeusia were associated with deterioration of appetite loss (15.642≤B≤20.016, P≤0.031). Likewise, grade 2 and above constipation (B=26.451, P≤0.001) and diarrhea (B=19.52, P≤0.001) were the positive predictor for constipation and diarrheal score, respectively. Grade ≥2 myalgia and arthralgia were also predicted for higher pain score (B=8.50, P=0.011), grade 2 skin hyperpigmentation was associated with lower body image (B=−6.189, P=0.05) and higher upset for hair loss score (B= 7.715, P=0.033).
Nonetheless, diverse scales of both EORTC QLQ-C30 and EORTC QLQ-BR23 were deteriorated due to non-hematological AC and AC-T breast cancer chemotherapy’s toxicities, its hematological toxicity like anemia was associated with worsening of QoL (ie fatigue dimension). On top of that, patients with lymphopenia experienced less deterioration of arm symptoms than those who did not report lymphopenia. Besides, alkaline phosphatase increment due to chemotherapy was among the contributing factors for deterioration of role functioning (B=−7.742, P=0.027) subscales. However, we did not find any association between neutropenia or leukopenia and deterioration of QoL. Likely, the study indicated that asymptomatic toxicities like granulocytopenia and leukopenia do not necessarily mean a decline in QoL unlike with symptomatic toxicities.32,52 Consequently, establishing supportive and peer groups such as psychiatrists, psychologists, physical therapists, and social workers,34,76 and providing educational sessions on the disease, and its treatment distressing toxicities can improve the QoL58,77 of patients of this group.
In general, besides grade ≥2 fatigue, dysgeusia, constipation, dry mouth, oral mucositis, peripheral neuropathy, and skin hyperpigmentation that frequently associated with deterioration QoL; anemia, lymphopenia, and ALP increment were non-subjective toxicities that predict fatigue, arm symptoms, and role functioning score, respectively.
In addition to the toxicities of the chemotherapy, the socio-demographic and clinical characteristics of the patients also contribute to the deteriorations of different quality of life domains. Conversely, educational status (literate vs illiterate), tumor stage (½ vs ¾), age (continuous), regimen (AC vs AC-T), having at least one child, marital status (having spouse vs having no spouse), body surface area and some baseline laboratory values such as hemoglobin, white blood cells, neutrophils, alkaline phosphatase, and serum creatinine affect diverse aspects of QoL among our study participants.
There was conflicting finding regarding the effect of sociodemographic and clinical characteristics on QoL among patients who received chemotherapy.63,64,78,79 However, in line with the studies conducted by Wondie et al and others,48,50 we found that the educational status (ie, illiteracy) and/or stage of the tumor (ie, stage ¾) were the most frequent sociodemographic factors associated with the deterioration of different subscales of EORTC QLQ-C30 and BR23. A possible explanation for this finding is the ability of educated women to understand the nature of the disease and to comply with the therapeutic recommendations better than the less educated.59 Moreover, different studies identified sociodemographic predictors such as age, residence, marital status, educational level, employment status, and tumor stage for deterioration of QoL.8,47,79
A holistic approach like combined diet, physical exercise, and psychosocial intervention during chemotherapy in patients with breast cancer led to positive changes in a range of psychological, physiological, and behavioral outcomes at the end of the intervention,61,69,80 that ultimately improve the overall quality of life of women on breast cancer chemotherapy.81,82
Strength and Limitation of the Study
Even though the majority of studies conducted on QoL among patients with breast cancer so far were cross-section in nature, we reported the pattern of QoL prospectively among women with breast cancer particularly on AC or AC-T chemotherapy. Moreover, still, the majority of QoL studies were reported from clinical trials, but importantly we reported this prospective patient-reported outcome study from the actual clinical practice (ie, real-world patients). To our knowledge, the current study is the first in design to answer the pattern QoL on a course of AC and AC-T chemotherapy cycles and in determining the impact of AC and AC-T chemotherapies’ toxicities on QoL among women with breast cancer in Ethiopia. However, since we followed our cohorts only for the median of 8 cycles (ie, 6 months), we could not report the pattern of QoL and the factors that affect it long after the end of chemotherapy courses.
Conclusion
The majority of the quality of life dimensions among Ethiopian breast cancer patients on AC and AC-T chemotherapy were significantly deteriorated clinically and statistically particularly during the first two cycles of chemotherapy despite its improvements afterward. In addition to age, tumor stage and educational status of the patients, grade 2 and above AC and AC-T chemotherapy’s toxicities such as fatigue, dysgeusia, constipation, oral mucositis, dry mouth, peripheral neuropathy, and skin hyperpigmentation were frequently associated with deterioration of different dimensions of quality of life. Devising different strategies to improve the deteriorated QoL due to chemotherapy’s toxicities particularly during the first two cycles has paramount importance.
Data Sharing Statement
Please contact the corresponding author for data requests.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The author (s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Addis Ababa University. However, the funding body has no role in designing the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Yusuf A, Sairi I, Hadi A, Mahamood Z, Ahmad Z. Quality of life in malay and chinese women newly diagnosed with breast cancer in kelantan, Malaysia. Asian Pacific J Cancer Prev. 2013;14(1):435–440. doi:10.7314/APJCP.2013.14.1.435
2. Lee CK, Stockler MR, Coates AS, Gebski V, Lord SJ, Simes RJ. Self-reported health-related quality of life is an independent predictor of chemotherapy treatment benefit and toxicity in women with advanced breast cancer. Br J Cancer. 2010;102(9):1341–1347. doi:10.1038/sj.bjc.6605649
3. Park J, Jung YS, Jung Y, Bae SH. The role of depression in the relationship between cognitive decline and quality of life among breast cancer patients. Support Care Cancer. 2018.
4. Tröger W, Jezdić S, Ždrale Z, Tišma N, Hamre HJ. Quality of life and neutropenia in patients with early stage breast cancer: a randomized pilot study comparing additional treatment with mistletoe extract to chemotherapy alone. Breast Cancer Basic Clin Res. 2009;3:35–45. doi:10.4137/BCBCR.S2905
5. Ferreira AR, Di MA, Pistilli B, et al. Differential impact of endocrine therapy and chemotherapy on quality of life of breast cancer survivors: a prospective patient-reported outcomes analysis. Ann Oncol. 2019:1–12. doi: 10.1093/annonc/mdz298.
6. Lipscomb J, Reeve BB, Clauser SB, et al. Patient-reported outcomes assessment in cancer trials: taking stock, moving forward. J Clin Oncol. 2007;25(32):5133–5140. doi:10.1200/JCO.2007.12.4644
7. Calvert M, Blazeby J, Altman DG, Revicki DA, Moher D, Brundage MD. Reporting of patient-reported outcomes in randomized trials: the CONSORT PRO extension. JAMA. 2013;309(8):814–822. doi:10.1001/jama.2013.879
8. Chen Q, Li S, Wang M, Liu L. Health-related quality of life among women breast cancer patients in Eastern China. Biomed Res Int. 2018. doi:10.1155/2018/1452635.
9. Cortes J, Hudgens S, Twelves C, et al. Health-related quality of life in patients with locally advanced or metastatic breast cancer treated with eribulin mesylate or capecitabine in an open-label randomized Phase 3 trial. Breast Cancer Res Treat. 2015;154:509–520. doi:10.1007/s10549-015-3633-7
10. Cardoso F, Di LA, Lohrisch C, et al. Second and subsequent lines of chemotherapy for metastatic breast cancer: what did we learn in the last two decades ? Ann Oncol. 2002;13:197–207. doi:10.1093/annonc/mdf101
11. Gunnars B, Nygren P, Glimelius B, Gunnars B, Nygren P, Glimelius B. Assessment of quality of life during chemotherapy. Acta Oncol. 2001;40(2–3):175–184. doi:10.1080/02841860121325
12. Alzabaidey FJ. Quality of life assessment for patients with breast cancer receiving adjuvant therapy. J Cancer Sci Ther. 2012;4(3):51–55. doi:10.4172/1948-5956.1000110
13. El FS, Abda N, Bendahhou K, et al. The european organization for research and treatment of cancer quality of life questionnaire-BR 23 breast cancer-specific quality of life questionnaire: psychometric properties in a Moroccan sample of breast cancer patients. BMC Res Notes. 2014;7:53. doi:10.1186/1756-0500-7-53
14. Lôbo SA, Fernandes AF. Quality of life in women with breast cancer undergoing chemotherapy. Acta Paul Enferm. 2014;27(6):554–559. doi:10.1590/1982-0194201400090
15. Knobf MT. The influence of endocrine effects of adjuvant therapy on quality of life outcomes in younger breast cancer survivors. Oncologist. 2006;11(2):96–110. doi:10.1634/theoncologist.11-2-96
16. Quinten C, Kenis C, Hamaker M, et al. The effect of adjuvant chemotherapy on symptom burden and quality of life over time; a preliminary prospective observational study using individual data of patients aged ≥ 70 with early stage invasive breast cancer. J Geriatr Oncol. 2018;9(2):152–162. doi:10.1016/j.jgo.2017.10.001
17. Prieto-callejero B, Rivera F. Influence of the sense of coherence, the doctor – patient relationship, optimism and non-haematological adverse reactions on health-related quality of life in patients with breast cancer. J Clin Med. 2019;8:2043. doi:10.3390/jcm8122043
18. Wagner LI, Zhao F, Goss PE, et al. Patient-reported predictors of early treatment discontinuation: treatment-related symptoms and health-related quality of life among postmenopausal women with primary breast cancer randomized to anastrozole or exemestane on NCIC Clinical Trials Group (CCTG) MA.27 (E1Z03). Breast Cancer Res Treat. 2018;169(3):537–548. doi:10.1007/s10549-018-4713-2
19. Mir R, Singh VP. Breast cancer in young women and its impact on reproductive function. Apollo Med. 2009;6(3):200–208. doi:10.1016/S0976-0016(11)60528-0
20. Verma S, Shaughnessy JO, Burris HA, et al. Health ‑ related quality of life of postmenopausal women with hormone receptor ‑ positive, human epidermal growth factor receptor 2 - negative advanced breast cancer treated with ribociclib + letrozole: results from Monaleesa - 2. Breast Cancer Res Treat. 2018;170:535–545. doi:10.1007/s10549-018-4769-z
21. Friese CR, Harrison JM, Janz NK, Jagsi R. Treatment-associated toxicities reported by patients with early-stage invasive breast cancer. Cancer. 2017;123:1925–1934. doi:10.1002/cncr.30547
22. Groenvold M. Health-related quality of life in early breast cancer. Dan Med Bull. 2010;57:B4184.
23. Gadisa DA, Gebremariam ET, Ali GY. Reliability and validity of Amharic version of EORTC QLQ-C30 and QLQ-BR23 modules for assessing health-related quality of life among breast cancer patients in Ethiopia. Health Qual Life Outcomes. 2019;17(182):1–8. doi:10.1186/s12955-019-1257-z
24. Gadisa DA, Assefa M, Tefera GM, Yimer G. Patterns of anthracycline-based chemotherapy-induced adverse drug reactions and their impact on relative dose intensity among women with breast cancer in ethiopia: a prospective observational study. J Oncol. 2020;2020:1–12. doi:10.1155/2020/2636514
25. Gadisa DA, Assefa M, Wang S, Yimer G. Toxicity profile of doxorubicin- cyclophosphamide and doxorubicin- cyclophosphamide followed by paclitaxel regimen and its associated factors among women with breast cancer in ethiopia: a prospective cohort study. J Oncol Pharm Pract. 2020;26(8):1912–1920. doi:10.1177/1078155220907658
26. U.S. Department of health and human services. common terminology criteria for adverse events v4.0 (CTCAE); 2010 v4.03:1–194. Available from: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf.
27. Basch E, Reeve BB, Mitchell SA, et al. Development of the national cancer institute ’ s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). J Natl Cancer Inst. 2014;106(9):dju244. doi:10.1093/jnci/dju244
28. Aaronson N, Ahmedzai S, Bergman B, et al. The European organisation for research and treatment of cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85:365–376. doi:10.1093/jnci/85.5.365
29. Fayers P, Aaronson N, Bjordal K, Groenvold M, Curran D, Bottomley A On Behalf of the EORTC Quality of Life Group. The EORTC QLQ-C30 Scoring Manual (
30. Park YH, Jung KH, Im SA, et al. Quality of life (QoL) in metastatic breast cancer patients with maintenance paclitaxel plus gemcitabine (PG) chemotherapy: results from Phase III, multicenter, randomized trial of maintenance chemotherapy versus observation (KCSG-BR07-02). Breast Cancer Res Treat. 2015;152(1):77–85. doi:10.1007/s10549-015-3450-z
31. World Medical Association. Declaration of helsinki: ethical principles for medical research involving human subjects. 2008; 1–5. doi:10.1093/acprof:oso/9780199241323.003.0025
32. Osoba D, Slamon DJ, Burchmore M, Murphy M. Effects on quality of life of combined trastuzumab and chemotherapy in women with metastatic breast cancer. J Clin Oncol. 2002;20:3106–3113. doi:10.1200/JCO.2002.03.090
33. Browall M, Ahlberg K, Karlsson P, Danielson E, Persson L, Gaston-johansson F. Health-related quality of life during adjuvant treatment for breast cancer among postmenopausal women. Eur J Oncol Nurs. 2008;12:180–189. doi:10.1016/j.ejon.2008.01.005
34. Hatam N, Ahmadloo N, Daliri AAK, Bastani P, Askarian M. Quality of life and toxicity in breast cancer patients using adjuvant TAC (docetaxel, doxorubicin, cyclophosphamide), in comparison with FAC (doxorubicin, cyclophosphamide). Arch Gynecol Obs. 2011;284:215–220. doi:10.1007/s00404-010-1609-8
35. Perroud HA, Alasino CM, Rico MJ, et al. Quality of life in patients with metastatic breast cancer treated with metronomic chemotherapy. Futur Oncol. 2016;12:1233–1242. doi:10.2217/fon-2016-0075
36. Chagani P, Parpio Y, Gul R, Jabbar AA. Quality of life and its determinants in adult cancer patients undergoing chemotherapy treatment in Pakistan. Asia Pac J Oncol Nurs. 2017;4(2):140–146. doi:10.4103/2347-5625.204499
37. Perry S, Kowalski TL, Chang C. Quality of life assessment in women with breast cancer: benefits, acceptability and utilization. Health Qual Life Outcomes. 2007;5:24. doi:10.1186/1477-7525-5-24
38. Hall E, Cameron D, Waters R, Barrett-lee P, Ellis P, Russell S. Comparison of patient reported quality of life and impact of treatment side effects experienced with a taxane-containing regimen and standard anthracycline based chemotherapy for early breast cancer: 6 year results from the UK TACT trial (CRUK/01/00. Eur J Cancer. 2014;50(14):2375–2389. doi:10.1016/j.ejca.2014.06.007
39. Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16(1):139–144. doi:10.1200/JCO.1998.16.1.139
40. Dzingirai B, Wariva RN, Manyau P, Matyanga C. Health related quality of life among breast cancer patients undergoing adjuvant chemotherapy at a tertiary health facility: a cross sectional study. Value Heal. 2020;23(May):S28. doi:10.1016/j.jval.2020.04.1539
41. Lima EDNS, Ferreira IB, Lajolo PP, Paiva CE, Maia YCDP, Pena GDG. Health-related quality of life became worse in short-term during treatment in head and neck cancer patients: a prospective study. Health Qual Life Outcomes. 2020;18(307).
42. Aberaraw R, Boka A, Teshome R, Yeshambel A. Social networks and quality of life among female breast cancer patients at Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia 2019. BMC Womens Health. 2020;20:50. doi:10.1186/s12905-020-00908-8
43. Horwitz EM, Hanlon AL, Pinover WH, Anderson PR, Hanks GE. Impact of surgery and chemotherapy on the quality of life of younger women with breast carcinoma: A prospective study. Cancer. 2001;92:1288–1298. doi:10.1002/1097-0142(20010901)92:5<1288::AID-CNCR1450>3.0.CO;2-E
44. Cho O. Changes in fatigue, psychological distress, and quality of life after chemotherapy in women with breast cancer. Cancer Nurs. 2020;43(1):54–60. doi:10.1097/NCC.0000000000000689
45. Koboto DD, Deribe B, Gebretsadik A, et al. Quality of life among breast cancer patients attending Hawassa University comprehensive specialized hospital cancer treatment center. Breast Cancer Targets Ther. 2020;12:87–95. doi:10.2147/BCTT.S252030
46. Ho PJ, Gernaat SAM, Hartman M, Verkooijen HM. Health-related quality of life in Asian patients with breast cancer: A systematic review. BMJ Open. 2018;8:4. doi:10.1136/bmjopen-2017-020512
47. Hassen AM, Taye G, Gizaw M, Hussien FM. Quality of life and associated factors among patients with breast cancer under chemotherapy at Tikur Anbessa specialized. PLoS One. 2019;1–13. doi:10.1371/journal.pone.0222629
48. Wondie Y, Hinz A. Quality of life among Ethiopian cancer patients. Support Care Cancer. 2020;28(11):5469–5478. doi:10.1007/s00520-020-05398-w
49. Silva C, Machado P. Prevalence of symptoms and quality of life of cancer patients. Rev Bras Enferm. 2020;73(2):e20180287. doi:10.1590/0034-7167-2018-0287
50. Abegaz TM, Ayele AA, Gebresillassie BM. Health related quality of life of cancer patients in Ethiopia. J Oncol. 2018;2018:1–8. doi:10.1155/2018/1467595
51. Fetaini M, Hawari A, Kaki F, Ujaimi R. Impact of breast cancer treatments on body image and quality of life in survivors. Int J Med Dev Ctries. 2020;4(3):635–644.
52. Land SR, Kopec JA, Yothers G, et al. Health-related quality of life in axillary node-negative, estrogen receptor- negative breast cancer patients undergoing AC versus CMF chemotherapy: findings from the national surgical adjuvant breast and bowel project B-23 *. Breast Cancer Res Treat. 2004;86(2):153–164. doi:10.1023/B:BREA.0000032983.87966.4e
53. Mohsin S, Rehman MU, Azam N, Mashhadi SF. Comparison of quality of life of cancer patients undergoing chemotherapy in a tertiary care hospital, Rawalpindi. Pak Armed Forces Med J. 2016;66(1):83–87.
54. Megari K. Quality of life in chronic disease patients. Heal Psychol Res. 2013;1:17–20. doi:10.1016/j.jpainsymman.2020.11.029
55. Prieto-callejero B, Rivera F, Fagundo-rivera J, Romero A, Ruiz-frutos C. Relationship between chemotherapy-induced adverse reactions and health-related quality of life in patients with breast cancer. Medicine. 2020;99:
56. Martın M, Lluch A, Seguı´ MA, et al. Toxicity and health-related quality of life in breast cancer patients receiving adjuvant docetaxel, adding primary prophylactic granulocyte-colony stimulating factor to the TAC regimen. Ann Oncol. 2006;17:1205–1212. doi:10.1093/annonc/mdl135
57. Farthmann J, Veit J, Rautenberg B, Stickeler E. The impact of chemotherapy for breast cancer on sexual function and health-related quality of life female sexual function index questionnaire. Support Care Cancer. 2016;24:2603–2609. doi:10.1007/s00520-015-3073-2
58. Tiezzi MFBDM, Andrade JMD, Roma APMS, et al. Quality of life in women with breast cancer treated with or without chemotherapy. Cancer Nurs. 2017;40(2):108–116. doi:10.1097/NCC.0000000000000370
59. El HR, Abbas LA, Nerich V, Anota A. Factors associated with health-related quality of life in women with breast cancer in the middle east: A systematic review. Cancers. 2020;12:696. doi:10.3390/cancers12030696
60. Macquart-Moulin GV, Viens P, Genre D, et al. Concomitant chemoradiotherapy for patients with. Cancer. 1999;85:2190–2199. doi:10.1002/(SICI)1097-0142(19990515)85:10<2190::AID-CNCR13>3.0.CO;2-P
61. Witlox L, Schagen SB, De RMB, et al. Effect of physical exercise on cognitive function and brain measures after chemotherapy in patients with breast cancer (PAM study): protocol of a randomised controlled trial. BMJ Open. 2019;9:e028117. doi:10.1136/bmjopen-2018-028117
62. De JN, Candel MJJM, Schouten HC, Abu-saad HH, Courtens AM. Prevalence and course of fatigue in breast cancer patients receiving adjuvant chemotherapy. Ann Oncol. 2004;15:896–905. doi:10.1093/annonc/mdh229
63. Arndt V, Stegmaier C, Ziegler H, Brenner H. A population-based study of the impact of specific symptoms on quality of life in women with breast cancer 1 year after diagnosis. Cancer. 2006;107:2496–2503. doi:10.1002/cncr.22274
64. Janz NK, Mujahid M, Chung LK, et al. Symptom experience and quality of life of women following breast cancer treatment. J Women’s Heal. 2007;16(9):1348–1361. doi:10.1089/jwh.2006.0255
65. Hovan AJ, Williams PM, Stevenson-moore P, et al. A systematic review of dysgeusia induced by cancer therapies. Support Care Cancer. 2010;18:1081–1087. doi:10.1007/s00520-010-0902-1
66. Curt GA, Breitbart W, Cella D, et al. Impact of cancer-related fatigue on the lives of patients: new findings from the fatigue coalition. Oncologist. 2000;5:353–360. doi:10.1634/theoncologist.5-5-353
67. Álvarez-bustos A, Cantos B, Maximiano C, Hidalgo F, Valenzuela PL. Concurrent exercise interventions in breast cancer survivors with cancer-related fatigue authors. Int J Sport Med. 2020. doi:10.1055/a-1147-1513
68. Ehlers DK, Dubois K, Salerno EA. The effects of exercise on cancer-related fatigue in breast cancer patients during primary treatment: a meta-analysis and systematic review. Expert Rev Anticancer Ther. 2020;20:865–877. doi:10.1080/14737140.2020.1813028
69. Mokhatri-Hesari P, Montazeri A. Health-related quality of life in breast cancer patients: review of reviews from 2008 to 2018. Health Qual Life Outcomes. 2020;18:338. doi:10.1186/s12955-020-01591-x
70. Ponticelli RE, Clari RM, Frigerio S, et al. Dysgeusia and health-related quality of life of cancer patients receiving chemotherapy: A cross- - sectional study. Eur J Cancer Care. 2016:1–7. doi: 10.1111/ecc.12633.
71. Denda Y, Niikura N, Satoh S, Kozue K, Mayako Y, Toru T. Taste alterations in patients with breast cancer following chemotherapy: a cohort study. Breast Cancer. 2020;27:954–962. doi:10.1007/s12282-020-01089-w
72. Ki H, Umberger W, Aktas A, et al. The effect of constipation and pain on the psychoneurological symptoms and performance in advanced breast cancer women. Prensa Med Argent. 2020;106(3):206. doi:10.47275/0032-745X-206
73. Oneda E, Meriggi F, Zanotti L, et al. Innovative approach for the prevention of chemotherapy-induced peripheral neuropathy in cancer patients: a pilot study with the hilotherm device, the poliambulanza hospital experience. Integr Cancer Ther. 2020;19:1–11. doi:10.1177/1534735420943287
74. Cameron D, Morden JP, Canney P, et al. Accelerated versus standard epirubicin followed by cyclophosphamide, methotrexate, and fluorouracil or capecitabine as adjuvant therapy for breast cancer in the randomised UK TACT2 trial (CRUK/05/19): a multicentre, phase 3, open-label. Lancet Oncol. 2017;18:1–17. doi:10.1016/S1470-2045(17)30404-7
75. Al-Batran SE, Hozaeel W, Tauchert FK, et al. The impact of docetaxel-related toxicities on health-related quality of life in patients with metastatic cancer (QoliTax). Ann Oncol. 2015;26:1244–1248. doi:10.1093/annonc/mdv129
76. Zanville NR, Nudelman KNH, Smith DJ, et al. Evaluating the impact of chemotherapy-induced peripheral neuropathy symptoms (CIPN-sx) on perceived ability to work in breast cancer survivors during the first year post-treatment. Support Care Cancer. 2016;24:4779–4789. doi:10.1007/s00520-016-3329-5
77. Wagland R, Richardson A, Ewings S, et al. Prevalence of cancer chemotherapy-related problems, their relation to health-related quality of life and associated supportive care: a cross-sectional survey. Support Care Cancer. 2016;24:4901–4911. doi:10.1007/s00520-016-3346-4
78. Leinert E, Singer S, Janni W, et al. The impact of age on quality of life in breast cancer patients receiving adjuvant chemotherapy: a comparative analysis from the prospective. Clin Breast Cancer. 2017;17(2):100–106. doi:10.1016/j.clbc.2016.10.008
79. Lavdaniti M, Owens DA, Liamopoulou P, Marmara K. Factors influencing quality of life in breast cancer patients six months after the completion of chemotherapy. Diseases. 2019;7(26):1–16. doi:10.3390/diseases7010026
80. Carayol M, Ninot G, Senesse P, et al. Short- and long-term impact of adapted physical activity and diet counseling during adjuvant breast cancer therapy: the “ APAD1 ” randomized controlled trial. BMC Cancer. 2019;19:737. doi:10.1186/s12885-019-5896-6
81. Gebruers N, Camberlin M, Theunissen F, et al. The effect of training interventions on physical performance, quality of life, and fatigue in patients receiving breast cancer treatment: a systematic review. Support Care Cancer. 2018;27:109–122. doi:10.1007/s00520-018-4490-9
82. Ruiz-vozmediano J, Löhnchen S, Jurado L, et al. Influence of a multidisciplinary program of diet, exercise, and mindfulness on the quality of life of stage IIA-IIB breast cancer survivors. Integr Cancer Ther. 2020;19:1–11. doi:10.1177/1534735420924757
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.