")
Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 13
The Identification of a Novel Thiopurine S-Methyltransferase Allele, TPMT*45, in Korean Patient with Crohn’s Disease
Authors Ha C , Kim ES, Kwon Y , Choe YH, Kim MJ , Lee SY
Received 29 August 2020
Accepted for publication 11 November 2020
Published 26 November 2020 Volume 2020:13 Pages 665—671
DOI https://doi.org/10.2147/PGPM.S279446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin Bluth
Changhee Ha,1 Eun Sil Kim,2 Yiyoung Kwon,2 Yon Ho Choe,2 Mi Jin Kim,2 Soo-Youn Lee1,3
1Department of Laboratory Medicine and Genetics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea; 2Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea; 3Department of Clinical Pharmacology and Therapeutics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Correspondence: Mi Jin Kim
Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea
Tel +82 2 3410 0951
Fax +82 2 3410 0043
Email [email protected]
Soo-Youn Lee
Department of Laboratory Medicine and Genetics, Department of Clinical Pharmacology and Therapeutics, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea
Tel +82 2 3410 1834
Fax +82 2 3410 2719
Email [email protected]
Abstract: Pediatric Crohn’s disease (CD) carries a higher genetic susceptibility and an increased risk of a more aggressive disease course than adult CD. Treatment of CD is based on immunomodulatory drugs, such as thiopurines. The enzyme mainly involved in drug metabolism is thiopurine S-methyltransferase (TPMT). An increased concentration of drug metabolites can cause adverse drug effects, such as myelosuppression and hepatotoxicity; therefore, assessing the activity of TPMT is essential both before and during treatment. TPMT genotyping result is not affected by previous thiopurine dose and currently is the primary component of TPMT activity and disease monitoring. Until now, more than 40 allelic variants of the TPMT gene have been reported, with most of them having an uncertain or no enzyme function. In this article, we report the first case of a novel TPMT allele, TPMT*45, that was identified in a Korean girl with CD whose findings suggested decreased TPMT activity. This newly observed variant is caused by a single nucleotide polymorphism resulting in nonsense mutation (c.676C>T, p.R226*) and the partial loss of amino acids in the TPMT protein. Initially, the patient began azathioprine at a standard dosage (1.5 mg/kg/day), and her laboratory results, including red blood cell (RBC) TPMT activity (6-methylmercaptopurine 2.68 nmol/mL/h and 6-methylmercaptopurine riboside 4.82 nmol/mL/h) along with thiopurine metabolite levels (6-thioguanine nucleotides 479.3 pmol/8× 108 RBC), suggested an enzyme deficiency. The thiopurine dose was reduced to half (0.7 mg/kg/day), and the follow-up metabolite results as well as the associated inflammatory markers were continuously within reference ranges. Along with an improvement in the patient’s subjective reports and clinical symptoms, the patient demonstrated a good treatment response to the adjusted dose. The results of our report illustrate the importance of TPMT genotyping and pharmacogenetic-based thiopurine dose adjustment. Further research should focus on the functional characterization and impact on this novel allele’s treatment effect.
Keywords: TPMT*45, Crohn’s disease, thioupurine, single nucleotide polymorphism, TPMT activity, drug metabolism
Introduction
Crohn’s disease (CD) is a chronic relapsing and remitting inflammatory bowel disease (IBD), and its incidence is increasing worldwide.1,2 Approximately 20–25% of patients are pediatric, and children have greater genetic susceptibility and typically a more aggressive disease course than adult CD patients.3,4 The treatment of pediatric CD includes immunomodulatory agents, such as thiopurines and methotrexate,1,3 and disease monitoring markers include pediatric Crohn’s disease activity index (PCDAI), C-reactive protein (CRP) and fecal calprotectin.4,5
Thiopurine drugs, such as azathioprine, 6-mercaptopurine, and thioguanine, are widely used to treat IBD, as well as leukemia, rheumatic diseases, and solid organ transplant rejection.6,7 Thiopurines are S-methylated by the enzyme thiopurine S-methyltransferase (TPMT) and are thereby converted to metabolites, including thioguanine nucleotides (TGNs) and methylated mercaptopurine (MMPN).7,8 TGNs are involved in the inhibition of de-novo purine synthesis in hematopoietic stem cells,8–10 while MMPN is associated with hepatotoxicity.9 In patients being treated with thiopurines, measuring these metabolites in washed red blood cells (RBCs) can be used for drug monitoring in association with TPMT activity.11,12
The activity of TPMT is largely affected by the TPMT gene polymorphism, which is inherited as a monogenic, autosomal codominant trait.8,13,14 To date, more than 40 allelic variants of the TPMT gene have been reported to the TPMT nomenclature committee and assigned allele names (http://www.imh.liu.se/tpmtalleles).10 Most of these alleles have a single nucleotide polymorphism that causes amino acid changes that reduce TPMT activity.7 According to the Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines, patients with TPMT variants demonstrate moderate to severe myelosuppression; therefore, 30–70% of the standard dose is recommended for heterozygous TPMT-deficient patients (ie, TPMT intermediate metabolizer phenotype), while 10% of the standard dose is typically prescribed for homozygous TPMT deficient patients (ie, TPMT poor metabolizer phenotype).13 Previous studies have shown that three TPMT alleles (TPMT*2, TPMT*3A, and TPMT*3C) contribute to approximately 95% of TPMT deficiencies.8,10,15 Ethnic variability in the alleles exists, with TPMT*3A being most commonly deficient in Caucasians and Southwest Asians, whereas TPMT*3C is most likely to be deficient in Africans and Southeast Asians.6,7,15 Among the Korean population, TPMT*3C and TPMT*6 are the two most common variant alleles;15–17 the allele frequencies of TPMT*1 (wild-type), *3C, and *6 are 98.1%, 1.4%, and 0.2%, respectively.15
Since pediatric CD involves a genetic susceptibility, pharmacogenetic tests carried out both before and during treatment can contribute to personalized therapy through dose adjustments and attempts to reduce adverse effects. In this article, we report the first case of a novel TPMT allele, TPMT*45, found in a Korean girl with CD whose findings suggested TPMT deficiency. This study was reviewed and approved by the Institutional Review Board of Samsung Medical Center in Seoul, Korea (approval number: 2012–04-106-020). Parental informed consent including the case details and images published was obtained since the patient was under the age of 19. The research was carried out in accordance with the World Medical Association Declaration of Helsinki.
Case Report
A 17-year-old girl was referred to our hospital in April 2020 with a 4-month history of abdominal pain, diarrhea, hematochezia, and weight loss >10% of her baseline body weight. One month ago, she was admitted to another hospital. At that time, laboratory tests showed a white blood cell count of 4.74 x109/L, an absolute neutrophil count of 3.81×109/L, an absolute lymphocyte count of 0.74×109/L, a hemoglobin of 90 g/L, a hematocrit of 25.4%, a platelet count of 397 x109/L, an erythrocyte sedimentation rate (ESR) of 77 mm/h, a CRP of 41.2 mg/L, and albumin level of 35 g/L; other laboratory tests were unremarkable. The stool occult blood test was positive and the fecal calprotectin level was >1000 μg/g. Ileocolonoscopy revealed multiple deep ulcers from the terminal ileum to the rectum. The upper gastrointestinal endoscopy findings were unremarkable. Magnetic resonance enterography revealed enhanced wall thickening in the entire colon and ileum without evidence of stricturing or penetrating complications. Pelvic magnetic resonance imaging showed perianal inflammation at the 5-o’clock direction. The patient was diagnosed with CD of an A2, L3, B1p, G0 phenotype according to the Paris classification.18 The patient’s PCDAI was 60, indicating severe CD, and the simple endoscopic score for CD was 32. Right after diagnosis, the patient was prescribed azathioprine (50 mg once daily, 1.4 mg/kg/day), mesalazine (1000 mg twice daily, 56.0 mg/kg/day), prednisolone (20 mg twice daily, 1.1 mg/kg/day), and exclusive enteral nutrition for CD treatment. After three weeks of azathioprine treatment, the patient was referred to our hospital.
According to our clinic’s protocol, every patient with IBD is routinely performing TPMT genotyping. Briefly, TPMT genotyping was performed according to the following procedures. Peripheral blood from the patient was collected in a vacuum tube containing ethylenediaminetetraacetic acid as a preservative. Total genomic deoxyribonucleic acid (DNA) was extracted using a Wizard Genomic DNA Purification Kit (Promega, Madison, Wisconsin, USA) according to the manufacturer’s instructions. All coding exons with their intron-exon boundaries of the TPMT gene (NCBI reference sequence: NM_000367.2) were amplified by polymerase chain reaction (PCR). PCR was performed using a GeneAmp PCR system 9700 thermal cycler (Applied Biosystems, Foster City, California, USA). Cycle sequencing was carried out using BigDye Terminator Cycle Sequencing Ready Reaction Kits (Applied Biosystems) and an ABI 3130xl genetic analyzer (Applied Biosystems).
The sequencing results showed that the patient had a single nucleotide polymorphism (SNP) of 676C>T (Figure 1), resulting in a premature stop codon (Arg226*) in exon 10. In silico analysis using MutationTaster19 (Genome Reference Consortium Human Build 37_ensembl 69) was performed and predicted this SNP as deleterious. This SNP fulfilled the inclusion criteria for the TPMT Nomenclature Committee for novel alleles10 and was named TPMT*45 (exon 10, c.676C>T, p.R226*rs761990479). Another variant was not observed, which confirmed the patient’s TPMT genotype as TPMT*1/*45.
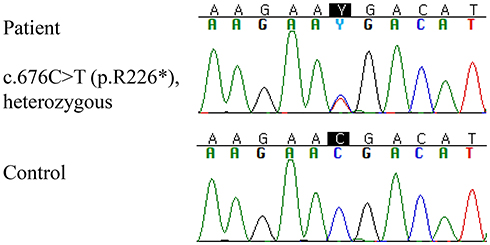 |
Figure 1 Sequence analysis result of the TPMT gene. |
A thiopurine metabolite analysis was performed using an API4000 tandem mass spectrometer (Applied Biosystems, Foster City, California, USA) equipped with an Agilent Technologies Series 1200 high-performance liquid chromatography system (Agilent Technologies, Santa Clara, California, USA) and an electrospray ionization source that was operated in positive-ion detection mode.20 Intra- and inter-assay coefficients of variation for the thiopurine metabolite measurements were <10%.20 The lower limits of quantification were 0.1 mol/L for 6-TGN and 0.5 mol/L for 6-MMPN. The concentration of the 6-TGN was 479.3 pmol/8×108 RBC, indicating a high risk of leukopenia, while the concentration of 6-MMPN was 609.5 pmol/8×108 RBC, which suggested a lower risk of hepatotoxicity (<5700 pmol/8×108 RBC).
To evaluate the RBC TPMT activity profile, mesalazine was withheld from the patient for 48 hours prior to blood sampling. The specimen obtained from the patient was sent to the Mayo Clinic Laboratories (Rochester, Minnesota, USA) for testing. Using three different substrates and a liquid chromatography-tandem mass spectrometry method, RBC TPMT activity was shown to be low in two of the three substrates: 2.68 of 6-MMPN (reference range: 3.00–6.66), 4.82 of 6-MMPN riboside (reference range: 5.04–9.57) and 4.19 of 6-methylthioguanine riboside (reference range: 2.70–5.84), with all units in nmol/mL/h.
Collectively, laboratory results of this patient suggest TPMT deficiency.9 The dosage of azathioprine was reduced to 25 mg once daily (0.7 mg/kg/day), and prednisolone was tapered since the patient was a non-responder to steroids. She maintained exclusive enteral nutrition for eight weeks and was treated with infliximab. The patient’s clinical symptoms improved, even with the azathioprine reduction and steroid tapering. The patient’s PCDAI score decreased to zero, and all follow-up laboratory test results (including complete blood cell counts, ESR, CRP, and albumin) were all within normal limits. The concentration of 6-TGN decreased to 364.0 pmol/8×108 RBC, which was within the therapeutic range (235.0–450.0 pmol/8×108 RBC).
The patient is on maintenance therapy and regularly visits the outpatient department for a PCDAI check and routine laboratory follow-up. After three months on a decreased dose, the patient’s PCDAI was still zero, and follow-up laboratory tests were all within normal limits, which indicated that there was no evidence of severe leukopenia or hepatotoxicity. Follow-up level of stool calprotectin was 5.5 μg/g, while the blood thiopurine metabolite levels of 6-TGN and 6-MMPN were 415.3 pmol/8×108 RBC and 159.3 pmol/8×108 RBC, respectively. The patient’s treatment course along with her major laboratory findings are shown in Figure 2, and clinical laboratory results are listed in Table 1.
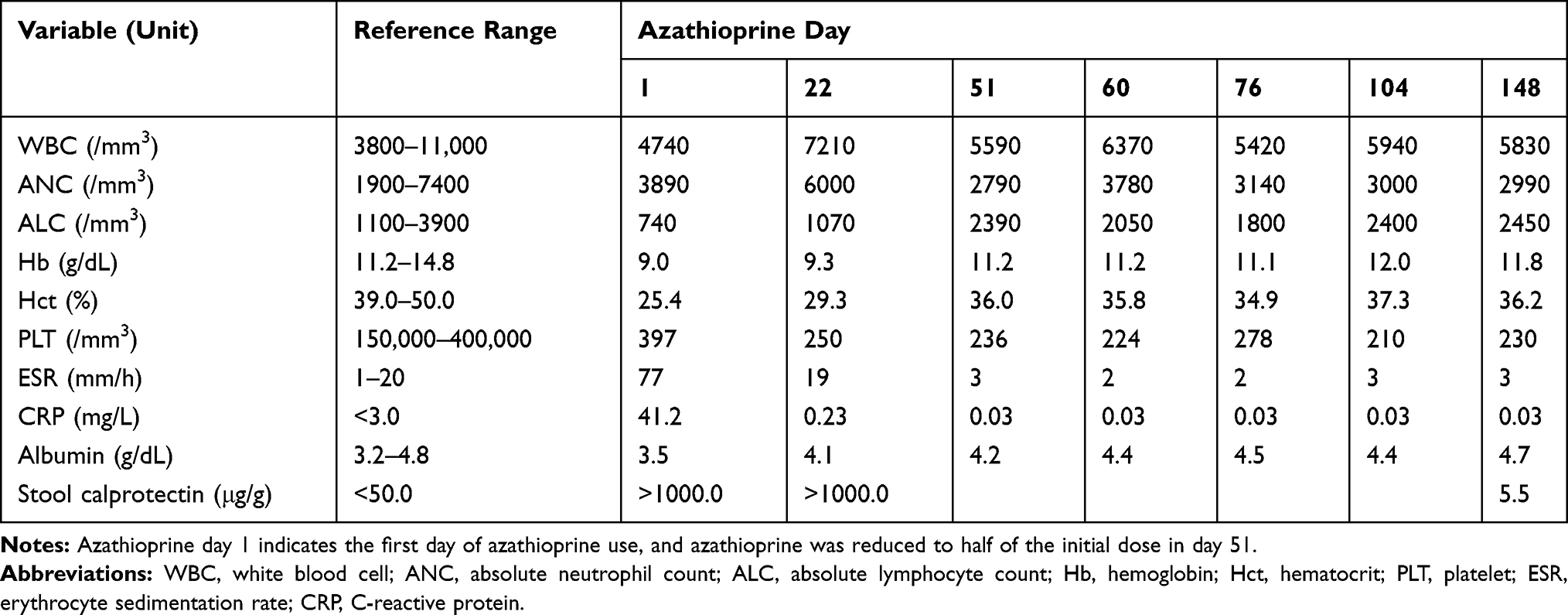 |
Table 1 Clinical Laboratory Results |
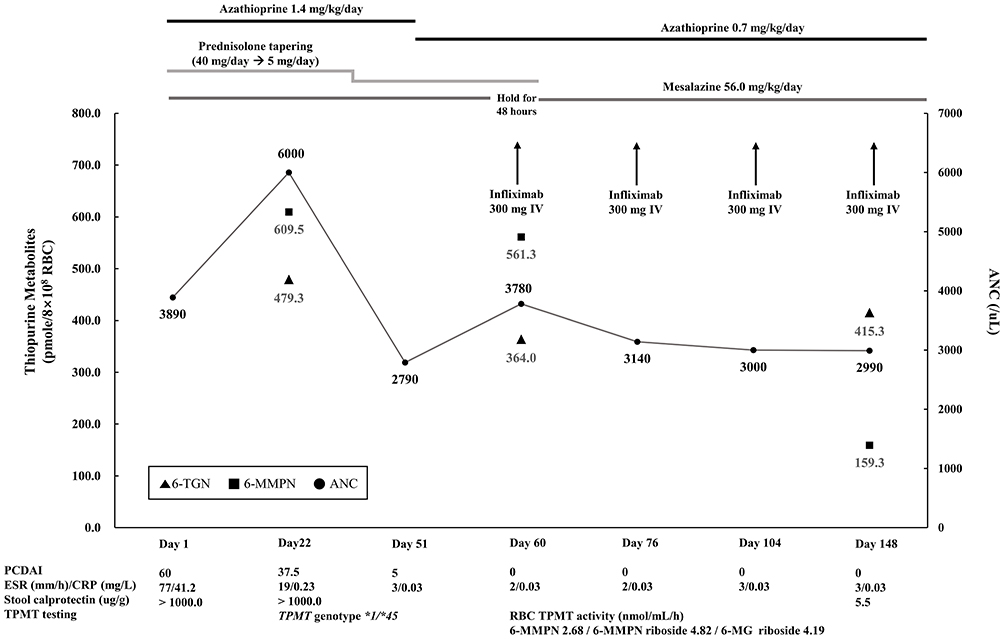 |
Figure 2 Treatment course of the patient. |
Discussion
This is the first report of a patient with TPMT*45, which is only the third nonsense mutation (c.676C>T; p.Arg226*) to be identified among TPMT alleles after TPMT*3D and TPMT*37.10,21 Since nonsense mutations result in a premature stop codon, the synthesized messenger ribonucleic acid (mRNA) may undergo degradation to prevent production of a truncated protein.22 It is possible that a decreased amount of protein production may contribute to thiopurine metabolism. The increased initial concentration of the thiopurine metabolite (6-TGN) in this patient also supports this assumption, showing correlation with the RBC TPMT activity profile results.
Pediatric CD is more aggressive than adult CD, with a stronger impact of genetic determinants.1,3 Many pediatric CD patients begin thiopurine therapy at a standard dosage (eg, 1.0–2.0 mg/kg/day) and when available, testing of the TPMT activity (genotype or phenotype) is also suggested before initiating treatment.3,23 In most clinical settings, including our patient’s, thiopurine treatment had already been established and was ongoing prior to assessing the TPMT activity results. According to the 2018 updated CPIC guidelines, the recommended dose for heterozygous TPMT deficient patients should be 30–70% of the standard dose.13 However, many of the TPMT alleles have an uncertain functional status, resulting in an indeterminate phenotype.24 In the case of unknown phenotypes, dose adjustments should be made only after reaching a steady state based on disease-specific guidelines, with evaluation of RBC TPMT activity and close monitoring.25 In pediatric CD patients whose enzyme activity is affected, a dose reduction by a half is recommended.3 After adjusting our patient’s azathioprine amount to 50% of the starting dose, PCDAI and laboratory results were normalized and persistently within the reference ranges, indicating a good treatment response.
Genetic evaluation in CD patients had different views among studies and guidelines. The European Crohn’s and Colitis Organisation (ECCO) guidelines did not recommend routine genetic study for diagnosis and classification of CD.26,27 In one study of IBD patients, performing TPMT genotyping before treatment was not beneficial in predicting adverse reactions to azathioprine.28 On the other hand, updated ECCO guideline for pediatric CD suggested pre-treatment TPMT genotyping for optimized thiopurine treatment since up-front thiopurine dose reduction showed decreased risk of hematological adverse drug reactions.29
Previous studies have emphasized the importance of measuring biomarkers (such as TGNs) to predict a patient’s response to thiopurines and to minimize any adverse reactions.9,23,30 These tests are also helpful in assessing the TPMT phenotype; however, the concentrations of TGNs rely on prior thiopurine dosing. Measurement of the RBC TPMT activity also aids in evaluating patients’ TPMT phenotype; however, it can be increased after thiopurine administration; therefore, cautious interpretation is required.13 Since TPMT activity is measured using RBCs, other conditions that may affect the RBC turnover rate or any history of blood transfusions can interfere with the results.13,23,31 In our patient’s case, she had not received a transfusion but had begun taking azathioprine three weeks prior to our hospital visit.
Compared to biomarkers, TPMT genotype has the advantage of unchanging during treatment. In many medical centers, patients undergo TPMT testing before they start thiopurines. This method is faster, more cost-effective, and less labor-intensive than the phenotyping method.7 Genotyping can be a representative method, with previous study results have shown a high concordance of 94.5%7 and 98.4%32 between TPMT genotype and phenotype. Another meta-analysis revealed that TPMT genotype is the primary component of TPMT activity,33 so it is important to perform genetic testing in routine practice to determine the best individual dose.
SNP occurred in our patient resulted in a nonsense mutation (c.676C>T; p.Arg226*). In a study that investigated the TPMT structure of murine, six amino acid residues were found to interact directly with 6-MPN, and they were conserved across mammalian species. Among them, Arg147 and Arg221 (Arg152 and Arg226 in human TPMT) were the only polar amino acids near 6-MPN that could be a candidate for substrate deprotonation and substitution of Arg147 influences the enzyme’s kinetics more significantly than Arg221.34 These findings could suggest that the position of our patient’s SNP is involved in some part of the TPMT enzyme’s reaction.
In our novel allele (TPMT*45), the nucleotide change occurred near the 3`-end of the DNA sequence. Despite the existence of premature stop codon, this variant may avoid mRNA degradation through an escape pathway,35 which is variable among species.36 Since this variant is predicted to generate a protein missing the last 20 amino acids near the C-terminus, it, therefore, produces a relatively less defected enzyme than the other alleles. This relatively less defected protein may explain the patient’s initial thiopurine metabolite level (6-TGN) being close to the upper limit, and two substrates’ RBC TPMT activity (6-MMPN and 6-MMPN riboside) being close to the lower limit of the reference values.
Nonetheless, most clinically relevant results are obtained from the TPMT enzyme activity measurements since they determine the actual metabolic status of patients.7 Other blood inflammatory biomarkers also allow follow-up assessment, especially during maintenance therapy.3 Combining the PCDAI score, CRP level, and fecal calprotectin drop has great utility in predicting disease activity before and after induction therapy.4 Fecal calprotectin is particularly useful in pediatric CD due to its role as a non-invasive marker of mucosal recovery.3
Collectively, compared to the adult CD patients genetic evaluation as well as biomarker levels are important in the monitoring and risk assessment of pediatric CD patients.3,29 In this case, a novel TPMT variant was identified, and this nonsense mutation is assumed to affect the activity of the TPMT enzyme. Our prediction was supported by the patient’s clinical manifestations and laboratory findings obtained after adjusting the dose of azathioprine.
Conclusion
To the best of our knowledge, this is the first report of the novel allele, TPMT*45. This nonsense mutation is related to the partial amino acid loss of the TPMT enzyme. The thiopurine metabolite concentrations and RBC TPMT activity results implied a deficiency of the enzyme in this patient. The patient’s daily thiopurine amount was reduced to half of the initial daily drug dose, and currently showing a good response to this patient-specific treatment. The results of our report illustrate the importance of TPMT genotyping and pharmacogenetic-based thiopurine dose adjustment. Nevertheless, there has been no functional study, and clinical evidence including TPMT enzyme activity of TPMT*45 is insufficient as data has been obtained only from a single case. Further research should focus on the functional characterization and impact on its treatment effect.
Abbreviations
CD, Crohn’s disease; IBD, inflammatory bowel disease; PCDAI, Pediatric Crohn’s Disease Activity Index; CRP, C-reactive protein; TPMT, thiopurine S-methyltransferase; TGN, thioguanine nucleotide; MMPN, methylated mercaptopurine; RBC, red blood cell; CPIC, Clinical Pharmacogenetics Implementation Consortium; ESR, erythrocyte sedimentation rate; DNA, deoxyribonucleic acid; PCR, polymerase chain reaction; SNP, single nucleotide polymorphism; mRNA, messenger ribonucleic acid; ECCO, European Crohn’s and Colitis Organisation.
Data Sharing Statement
The data are available upon reasonable request to the corresponding author, Soo-Youn Lee.
Ethics Statement
This study was reviewed and approved by the Institutional Review Board of Samsung Medical Center in Seoul, Korea (approval number 2012-04-106-020). The research was carried out in accordance with the World Medical Association Declaration of Helsinki, and the parents provided written informed consent since the patient was under age 19.
Acknowledgments
We thank the patient and her parents for their collaboration with respect to this report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from the Korean Foundation for Cancer Research 351 (KFCR-2017-D-1).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lahad A, Weiss B. Current therapy of pediatric Crohn’s disease. World J Gastrointest Pathophysiol. 2015;6(2):33–42. doi:10.4291/wjgp.v6.i2.33
2. Sýkora J, Pomahačová R, Kreslová M, Cvalínová D, Štych P, Schwarz J. Current global trends in the incidence of pediatric-onset inflammatory bowel disease. World J Gastroenterol. 2018;24(25):2741–2763. doi:10.3748/wjg.v24.i25.2741
3. Ruemmele FM, Veres G, Kolho KL, et al. Consensus guidelines of ECCO/ESPGHAN on the medical management of pediatric Crohn’s disease. J Crohns Colitis. 2014;8(10):1179–1207.
4. Zubin G, Peter L. Predicting endoscopic Crohn’s disease activity before and after induction therapy in children: a comprehensive assessment of PCDAI, CRP, and fecal calprotectin. Inflamm Bowel Dis. 2015;21(6):1386–1391.
5. Hyams J, Markowitz J, Otley A, et al. Evaluation of the pediatric Crohn disease activity index: a prospective multicenter experience. J Pediatr Gastroenterol Nutr. 2005;41(4):416–421. doi:10.1097/01.mpg.0000183350.46795.42
6. Sahasranaman S, Howard D, Roy S. Clinical pharmacology and pharmacogenetics of thiopurines. Eur J Clin Pharmacol. 2008;64(8):753–767. doi:10.1007/s00228-008-0478-6
7. Zimdahl Kahlin A, Helander S, Skoglund K, Söderkvist P, Mårtensson LG, Appell ML. Comprehensive study of thiopurine methyltransferase genotype, phenotype, and genotype-phenotype discrepancies in Sweden. Biochem Pharmacol. 2019;164:263–272.
8. Evans WE. Pharmacogenetics of thiopurine S-methyltransferase and thiopurine therapy. Ther Drug Monit. 2004;26(2):186–191. doi:10.1097/00007691-200404000-00018
9. Dubinsky MC, Lamothe S, Yang HY, et al. Pharmacogenomics and metabolite measurement for 6-mercaptopurine therapy in inflammatory bowel disease. Gastroenterology. 2000;118(4):705–713. doi:10.1016/S0016-5085(00)70140-5
10. Appell ML, Berg J, Duley J, et al. Nomenclature for alleles of the thiopurine methyltransferase gene. Pharmacogenet Genomics. 2013;23(4):242–248. doi:10.1097/FPC.0b013e32835f1cc0
11. Dervieux T, Meyer G, Barham R, et al. Liquid chromatography-tandem mass spectrometry analysis of erythrocyte thiopurine nucleotides and effect of thiopurine methyltransferase gene variants on these metabolites in patients receiving azathioprine/6-mercaptopurine therapy. Clin Chem. 2005;51(11):2074–2084. doi:10.1373/clinchem.2005.050831
12. Vikingsson S, Almer S, Peterson C, Carlsson B, Josefsson M. Monitoring of thiopurine metabolites – a high-performance liquid chromatography method for clinical use. J Pharm Biomed Anal. 2013;75:145–152.
13. Relling MV, Schwab M, Whirl-Carrillo M, et al. Clinical pharmacogenetics implementation consortium guideline for thiopurine dosing based on TPMT and NUDT15 genotypes: 2018 update. Clin Pharmacol Ther. 2019;105(5):1095–1105. doi:10.1002/cpt.1304
14. Liu C, Yang W, Pei D, et al. Genomewide approach validates thiopurine methyltransferase activity is a monogenic pharmacogenomic trait. Clin Pharmacol Ther. 2017;101(3):373–381. doi:10.1002/cpt.463
15. Kim HY, Lee SH, Lee MN, et al. Complete sequence-based screening of TPMT variants in the Korean population. Pharmacogenet Genomics. 2015;25(3):143–146. doi:10.1097/FPC.0000000000000117
16. Cheon JH, Kim JH, Kim BY, et al. Allele frequency of thiopurine methyltransferase and inosine triphosphate pyrophosphatase gene polymorphisms in Korean patients with inflammatory bowel diseases. Hepato-Gastroenterology. 2009;56(90):421–423.
17. Kim HY, Kim JW, Kim MJ, et al. Safe azathioprine treatment in a pediatric ulcerative colitis patient with TPMT*16 by thiopurine metabolite monitoring. Clin Chim Acta. 2014;437:101–102.
18. Levine A, Griffiths A, Markowitz J, et al. Pediatric modification of the montreal classification for inflammatory bowel disease: the Paris classification. Inflamm Bowel Dis. 2011;17(6):1314–1321. doi:10.1002/ibd.21493
19. Schwarz JM, Cooper DN, Schuelke M, Seelow D. MutationTaster2: mutation prediction for the deep-sequencing age. Nat Methods. 2014;11(4):361–362. doi:10.1038/nmeth.2890
20. Yoo IY, Lee K, Ji OJ, Woo HI, Lee SY. Evaluation of stability of thiopurine metabolites using a validated LC-MS/MS method. Ann Lab Med. 2018;38(3):255–260. doi:10.3343/alm.2018.38.3.255
21. Roberts RL, Wallace MC, Drake JM, Stamp LK. Identification of a novel thiopurine S-methyltransferase allele (TPMT*37). Pharmacogenet Genomics. 2014;24(6):320–323. doi:10.1097/FPC.0000000000000049
22. Kurosaki T, Maquat LE. Nonsense-mediated mRNA decay in humans at a glance. J Cell Sci. 2016;129(3):461–467. doi:10.1242/jcs.181008
23. Ford LT, Berg JD. Thiopurine S-methyltransferase (TPMT) assessment prior to starting thiopurine drug treatment; a pharmacogenomic test whose time has come. J Clin Pathol. 2010;63(4):288–295. doi:10.1136/jcp.2009.069252
24. Gene-specific Information Tables for TPMT. Stanford University (U24 HG010615); 2020. Available from: https://www.pharmgkb.org/page/tpmtRefMaterials.
25. CPIC® Guideline for Thiopurines and TPMT and NUDT15. Stanford University & St. Jude Children’s Research Hospital (U24HG010135); 2020. Available from: https://cpicpgx.org/guidelines/guideline-for-thiopurines-and-tpmt/.
26. Gomollón F, Dignass A, Annese V, et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016: part 1: diagnosis and medical management. J Crohns Colitis. 2017;11(1):3–25. doi:10.1093/ecco-jcc/jjw168
27. Harbord M, Eliakim R, Bettenworth D, et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. Part 2: current management. J Crohns Colitis. 2017;11(7):769–784.
28. Ribaldone DG, Adriani A, Caviglia GP, et al. Correlation between Thiopurine S-Methyltransferase genotype and adverse events in inflammatory bowel disease patients. Medicina (Kaunas). 2019;55(8):441.
29. van Rheenen PF, Aloi M, Assa A, et al. The medical management of paediatric Crohn’s disease: an ECCO-ESPGHAN guideline update. J Crohns Colitis. 2020.
30. Roy LM, Zur RM, Uleryk E, Carew C, Ito S, Ungar WJ. Thiopurine S-methyltransferase testing for averting drug toxicity in patients receiving thiopurines: a systematic review. Pharmacogenomics. 2016;17(6):633–656. doi:10.2217/pgs.16.12
31. Lennard L, Chew TS, Lilleyman JS. Human thiopurine methyltransferase activity varies with red blood cell age. Br J Clin Pharmacol. 2001;52(5):539–546. doi:10.1046/j.0306-5251.2001.01497.x
32. Schaeffeler E, Fischer C, Brockmeier D, et al. Comprehensive analysis of thiopurine S-methyltransferase phenotype-genotype correlation in a large population of German-caucasians and identification of novel TPMT variants. Pharmacogenetics. 2004;14(7):407–417. doi:10.1097/01.fpc.0000114745.08559.db
33. Tamm R, Mägi R, Tremmel R, et al. Polymorphic variation in TPMT is the principal determinant of TPMT phenotype: a meta-analysis of three genome-wide association studies. Clin Pharmacol Ther. 2017;101(5):684–695. doi:10.1002/cpt.540
34. Peng Y, Feng Q, Wilk D, et al. Structural basis of substrate recognition in thiopurine s-methyltransferase. Biochemistry. 2008;47(23):6216–6225. doi:10.1021/bi800102x
35. Coban-Akdemir Z, White JJ, Song X, et al. Identifying genes whose mutant transcripts cause dominant disease traits by potential gain-of-function alleles. Am J Hum Genet. 2018;103(2):171–187. doi:10.1016/j.ajhg.2018.06.009
36. Conti E, Izaurralde E. Nonsense-mediated mRNA decay: molecular insights and mechanistic variations across species. Curr Opin Cell Biol. 2005;17(3):316–325. doi:10.1016/j.ceb.2005.04.005
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.