")
Back to Journals » Patient Preference and Adherence » Volume 16
The Health-Related Quality of Life of Patients with Type 2 Diabetes in Saudi Arabia
Authors AbuAlhommos AK , Alturaifi AH, Al-Bin Hamdhah AM, Al-Ramadhan HH, Al Ali ZA, Al Nasser HJ
Received 11 December 2021
Accepted for publication 26 April 2022
Published 11 May 2022 Volume 2022:16 Pages 1233—1245
DOI https://doi.org/10.2147/PPA.S353525
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Amal Khaleel AbuAlhommos, Amjad Heji Alturaifi, Amnah Mohammed Al-Bin Hamdhah, Hawra Hassan Al-Ramadhan, Zahra Abdullah Al Ali, Hawra Jumah Al Nasser
Pharmacy Practice Department, Clinical Pharmacy College, King Faisal University, Alhasa, Saudi Arabia
Correspondence: Amal Khaleel AbuAlhommos, Pharmacy Practice Department, Clinical Pharmacy College, King Faisal University, Alhasa, Saudi Arabia, Tel +966596150032, Email [email protected]
Objective: Diabetes mellitus (DM) is one of the most common chronic diseases in the world. Diabetes mellitus has a major effect on patients’ quality of life, especially when the patient has other comorbidities. Therefore, this study aims to assess the quality of life of type 2 diabetic patients in the Al-Ahsa region of Saudi Arabia.
Methods: This was a cross-sectional study, which was conducted from September 2020 to May 2021 on patients with type 2 diabetes mellitus in the Al-Ahsa region of Saudi Arabia. Inclusion criteria were patients diagnosed with T2DM and aged 18 years and older. The EQ-5D-5L tool was used in this study to measure the quality of life.
Results: A total of 321 patients with T2DM participated in the study. Only 8.4% of the study participants reported that their disease did not let them do their daily activities at all. The most commonly reported problems related to diabetes mellitus and its effect on patients’ quality of life were pain/discomfort (around 68.0% of the patients reported some sort of problems in this dimension), followed by mobility, and depression and anxiety. There was a significant difference between males and females in terms of their quality of life, specifically self-care, pain and discomfort, and depression and anxiety (p< 0.05). Patients from different marital statuses, education levels, employment status, and duration of the disease showed a significant difference in quality of life, except for depression and anxiety (p> 0.05).
Conclusion: Pain/discomfort, mobility, and depression/anxiety are the main problems that are affecting diabetic patients’ quality of life. Future studies are recommended to explore the effectiveness of patient tailored interventions to decrease the negative impact of these dimensions on patients’ quality of life.
Keywords: patients, quality of life, Saudi Arabia, type 2 diabetes mellitus
Introduction
Diabetes mellitus (DM) is one of the most common chronic diseases in the world.1 It is characterised by an abnormal and prolonged (long-lasting) high level of glucose in the blood and is considered a metabolic syndrome. Type 2 diabetes mellitus is a non-insulin-dependent diabetes mellitus characterised by insulin resistance, hyperglycaemia, and relative insulin deficiency.2 The aetiology of type 2 DM results from a complex interaction between multiple risk factors, such as environmental, genetic, and behavioural risk factors. The common risk factors are obesity, physical inactivity, cigarette smoking, a sedentary lifestyle, heavy consumption of alcohol, family history, especially first degree relatives, being 45 years old or older, and an unhealthy diet. Many medical conditions could induce type 2 DM, such as hypertension, hyperlipidemia, polycystic ovarian syndrome, and endocrine disorders such as Cushing syndrome.2,3
Patients with type 2 DM are often asymptomatic or may experience symptoms that include polydipsia, polyuria, polyphagia, lethargy, nocturia, and overweight. There are criteria to diagnose DM patients based on laboratory measurements that include fasting blood glucose levels equal to 126 mg/dl or 7 mmol/l or more in two or more sessions, in which the patient must fast for at least eight hours, HbA1C equal to 6.5% or more and the patient does not need to fast, an oral glucose tolerance test (OGTT) equal to 200 mg/dl or more after drinking 75g anhydrous glucose dissolved in water, and random blood glucose levels equal to 200 mg/dl or more with symptoms of diabetes.2
The goals of treating patients with diabetes are generally to control blood glucose levels, to relieve signs and symptoms associated with hyperglycaemia, to prevent short-term acute complications such as diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic non-ketotic syndrome (HHNK), to prevent long-term chronic macrovascular and microvascular complications, and eventually to maintain or improve patients’ quality of life (QoL) and reduce mortality.1,4 Previous studies in the Middle East regions explored different aspects related to diabetes mellitus, including hypoglycemic events and intensive antidiabetic therapy.5,6 However, there are limited studies exploring patients’ QoL, specifically in Saudi Arabia. Diabetes mellitus has a major effect on patients’ QoL, not only because of the health problems caused by this disease but also it can cause familial, financial, and social issues, especially when the patient has other comorbidities.7 Frequent hospitalisation that could lead to financial loss, job loss, diminished interaction with family, psychological effects, and other issues is an example of the effects of DM on QoL.8 However, DM is not the only factor that can affect the QoL of a diabetic patient. According to the World Health Organization (WHO), QoL is defined as “an individual’s perceptions of their position in life in the context of the culture and value systems in which they live, and in relation to their goals, expectations, standards, and concerns. It is a broad-ranging concept affected in a complex way by the person’s physical health, psychological state, level of independence, social relationships, and their relationship to salient features of their environment”.9
A number of questionnaires have been developed by the WHO to measure QoL, including WHOQOL-100 and WHOQOL-BREF. The latter measures four domains: psychological health, physical health, the environment, and social relationships.9 In Birjand, Iran, investigators assessed the QoL of type 2 diabetic patients in a cross-sectional study by using EQ-5D-5 L, which was introduced in 2009 by the EuroQol Group. EQ-5D-5L is a short, clear questionnaire with the advantage of being easy to complete by the patients in a short period of time. The results of this study showed that 12% of the patients had moderate to severe problems in the anxiety/depression dimensions; 13.7% experienced pain or discomfort, and 13.6% of the patients had mobility problems in. They concluded that the QoL of patients is affected by many factors, such as sex, the duration of the disease, occupation, and the occurrence of diabetic complications.10
Another prospective descriptive study was conducted in southern India for the same reason. In this instance, the measurement tool was a modified diabetes quality of life (MDQOL)-17 questionnaire, which consists of 17 questions that cover seven domains. The researchers found that the presence of comorbidities and complications is inversely related to patients’ QoL. Moreover, several factors such as, age, type and number of complications, and duration of diabetes, were significantly correlated to QoL.11 Thus, in the management of chronic diseases, assessing patients’ QoL is considered an important measure of outcomes. To that end, this study aims to assess the quality of life of type 2 diabetic patients in the Al-Ahsa region of Saudi Arabia.
Materials and Methods
Study Design
This cross-sectional study, which was conducted from September 2020 to May 2021, aims to assess the quality of life of type 2 diabetes mellitus patients (T2DM). Patients with type 2 diabetes mellitus were approached in the Diabetic Centre at King Fahad Hospital andPrince Saud Bin Jalawy in the Al-Ahsa region of Saudi Arabia. Inclusion criteria were patients diagnosed with T2DM and aged 18 years and above with no obvious cognitive deficit. Patients who did not match the inclusion criteria or who did not give their consent to participate in the study were not involved in the study.
Participants Recruitment
Patients who met the inclusion criteria and agreed to participate were recruited using a convenience sampling technique. After explaining the study’s goal and objectives to type 2 diabetes mellitus patients attending the participating diabetes centers at King Fahad Hospital and Prince Saud Bin Jalawy, they were invited to participate. Participants were informed that their agreement to participate in the study qualifies them as having given informed consent.
Quality of Life Assessment Tool
The EQ-5D-5 L tool, which was introduced in 2009 by the EuroQol Group was used in this study to measure the QoL. This tool comprises five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each dimension has 5 levels: no problems, slight problems, moderate problems, severe problems and extreme problems.12 The EQ-5D questionnaire was administered in Arabic.13,14 The participants were interviewed in Arabic and their sociodemographic and clinical data (medications use history, diseases history, and diabetes-related information) were collected. Individuals completed the questionnaire and were given any support they required.
Statistical Analysis
Descriptive statistics were used to describe participants’ demographic characteristics. Continuous data were reported as mean ± SD for normally distributed variables. Categorical data were reported as percentages (frequencies). The Chi-square test was used to explore whether there is a significant difference in the five dimensions of quality of life (mobility, self-care, usual activities, pain/discomfort and anxiety/depression) between different demographic groups. EQ-5D-5L utilize five-point Likert scale, a score of 1 indicates no problems at all and 5 indicates worse health for that dimension. Binary logistic regression analysis was conducted to explore the association between participants demographic and diabetes related status and participants’ quality of life. For each dimension we used the mean score as a cut-off point to define the dummy variable of having good quality of life, were patients with a score higher than the median score (as the quality of life score was not normally distributed) of the study sample defined as having good quality of life compared to others (mobility mean score: 2.1 (SD: 1.2), self-care mean score: 1.6 (SD: 1.2), usual activities mean score: 2.0 (SD: 1.3), pain and discomfort mean score: 2.2 (SD: 1.1), and anxiety and depression mean score: 1.9 (SD: 1.0)). A confidence interval of 95% (p0<0.05) was applied to represent the statistical significance of the results. A two-sided p0≤0.05 was considered statistically significant. The statistical analyses were carried out using SPSS (version 27).
Ethical Approval and Consent to Participate
Ethical approval was obtained for this study from the Research Ethics Committee of Pharmacy Practice at the Clinical Pharmacy College at King Faisal University. All participants gave written informed consent. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments.
Results
Participants’ Baseline Characteristics
A total of 321 patients with T2DM participated in the study. Around half of them (49.5%) were aged 26–40 years. More than half of them (62.9%) were females. A total of 66.0% were married and 64.5% had primary education. 62.3% of the participants reported that they were without a job or were housewives. Around one-third of the study participants were covered by health insurance. The majority of them (72.9%) reported that they had been diagnosed with T2DM more than five years before. Similarly, the majority of them (76.3%) reported that they have a family history of T2DM. The BMI for the vast majority of the participants (86.3%) was within the normal range (18–24.9 kg/m2). Only 13.1% of the participants reported a smoking history. Around one-third of the study participants reported that they exercise on daily basis. The most commonly reported comorbidities were hypertension and cardiovascular diseases.
Around half of the study participants (51.1%) reported that they are on lifestyle modification and oral antidiabetic medications to manage their disease, with 43.0% using antidiabetic monotherapy. The vast majority (87.5%) reported that they take their medication regularly as prescribed by their doctor. One-third of the study participants reported that they have retinopathy as a complication due to their disease. A similar percentage of the participants reported that they have been admitted to hospital due to complications from diabetes at least once. For further details on the study participants, please refer to Table 1.
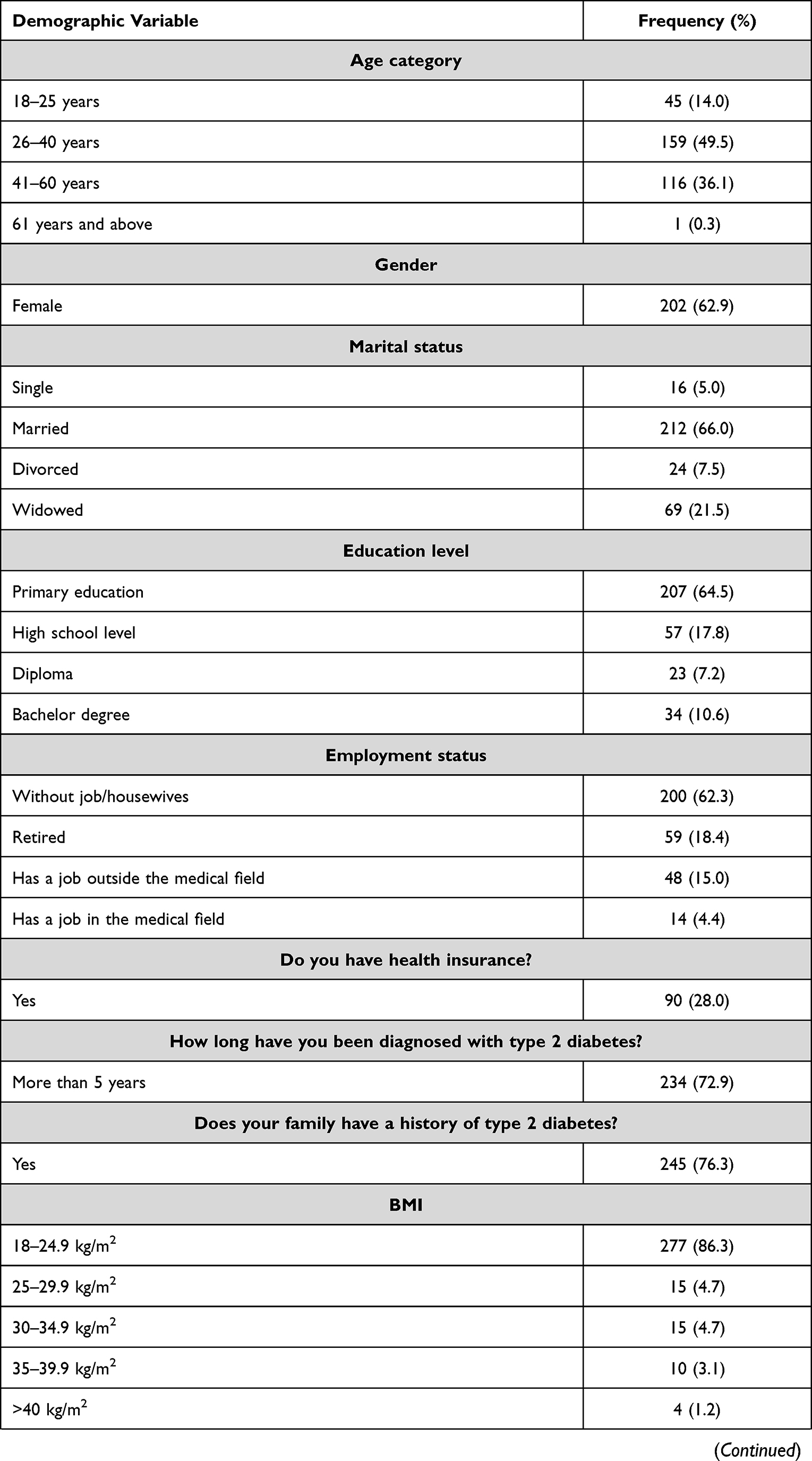 | 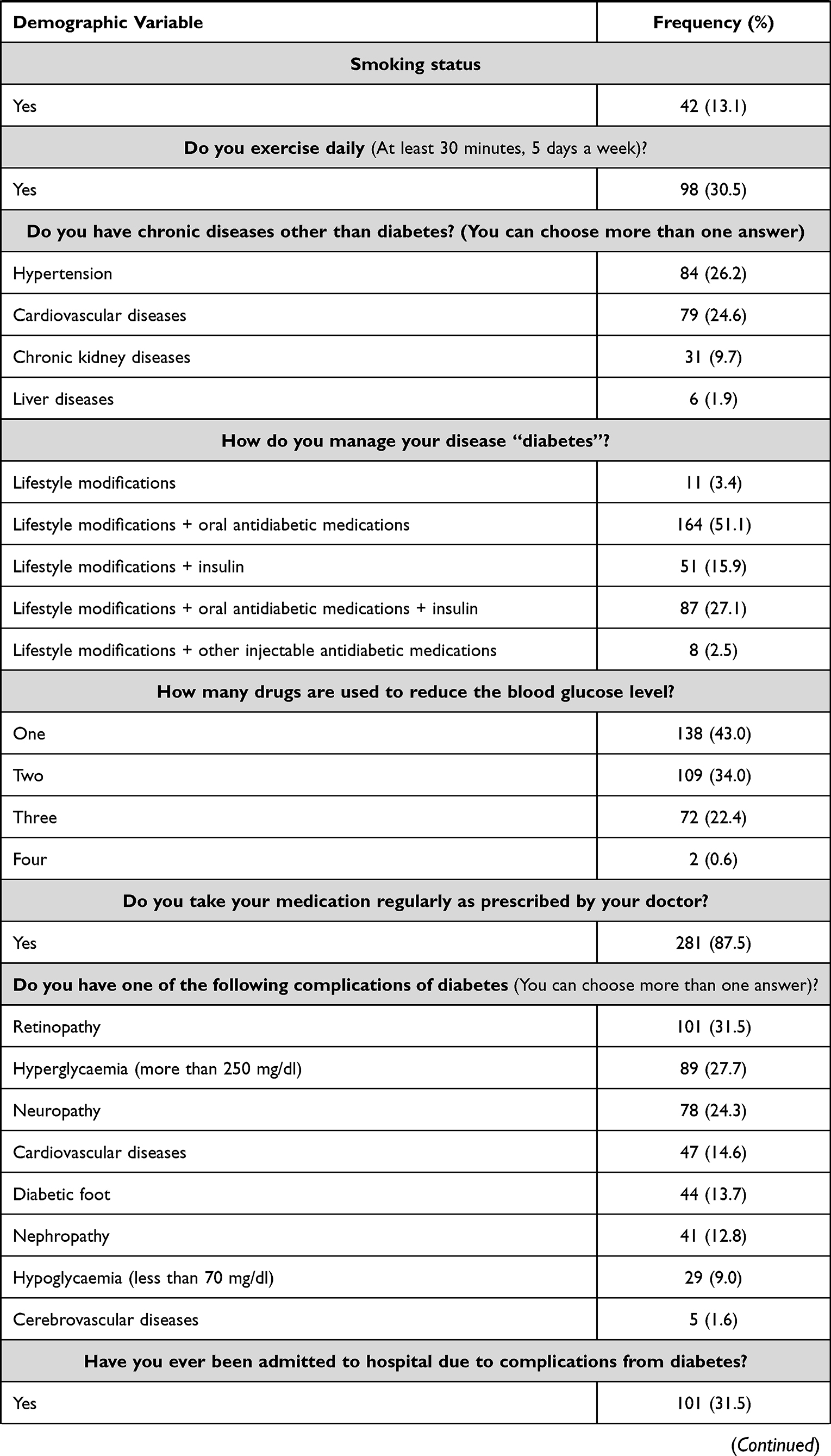 | 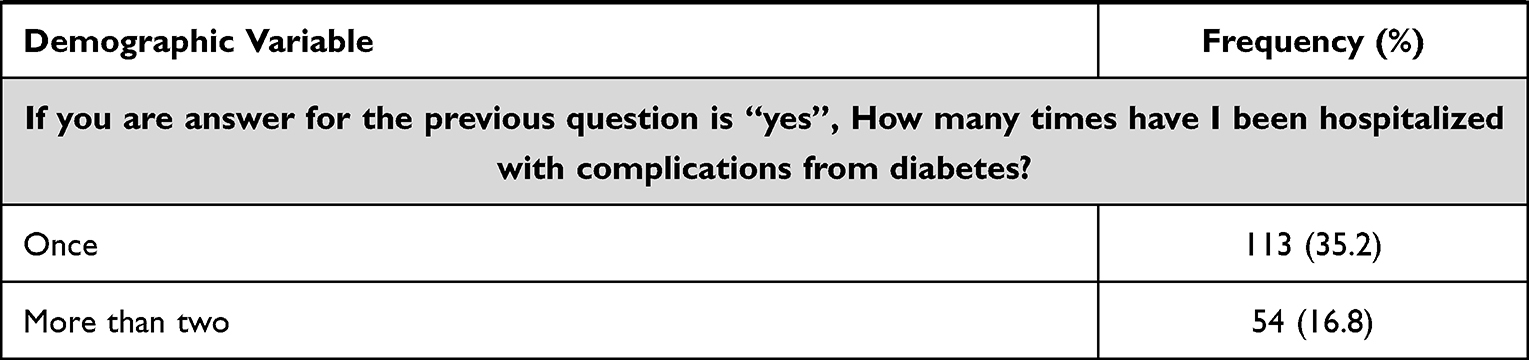 |
Table 1 Participants’ Demographic Characteristics |
Diabetes Mellitus Related Measures
Around 40.5% of the participants reported that their average blood sugar level (after eight hours of fasting) is between 80 and 130 mg/dl. One-third of the study participants reported that their average blood sugar level two hours after a meal is <180 mg/dl. A similar percentage of the participants reported that their last measured HbA1c level is between 7–8%. A total of 34.6% of the study participants reported that they measure their HbA1c level regularly. 47.7% of the study participants reported that they follow a diet that is low in carbohydrates, low in fat, rich in vegetables, low in salt, and limited to some fruits. For further details on patient-related diabetes measures, please refer to Table 2.
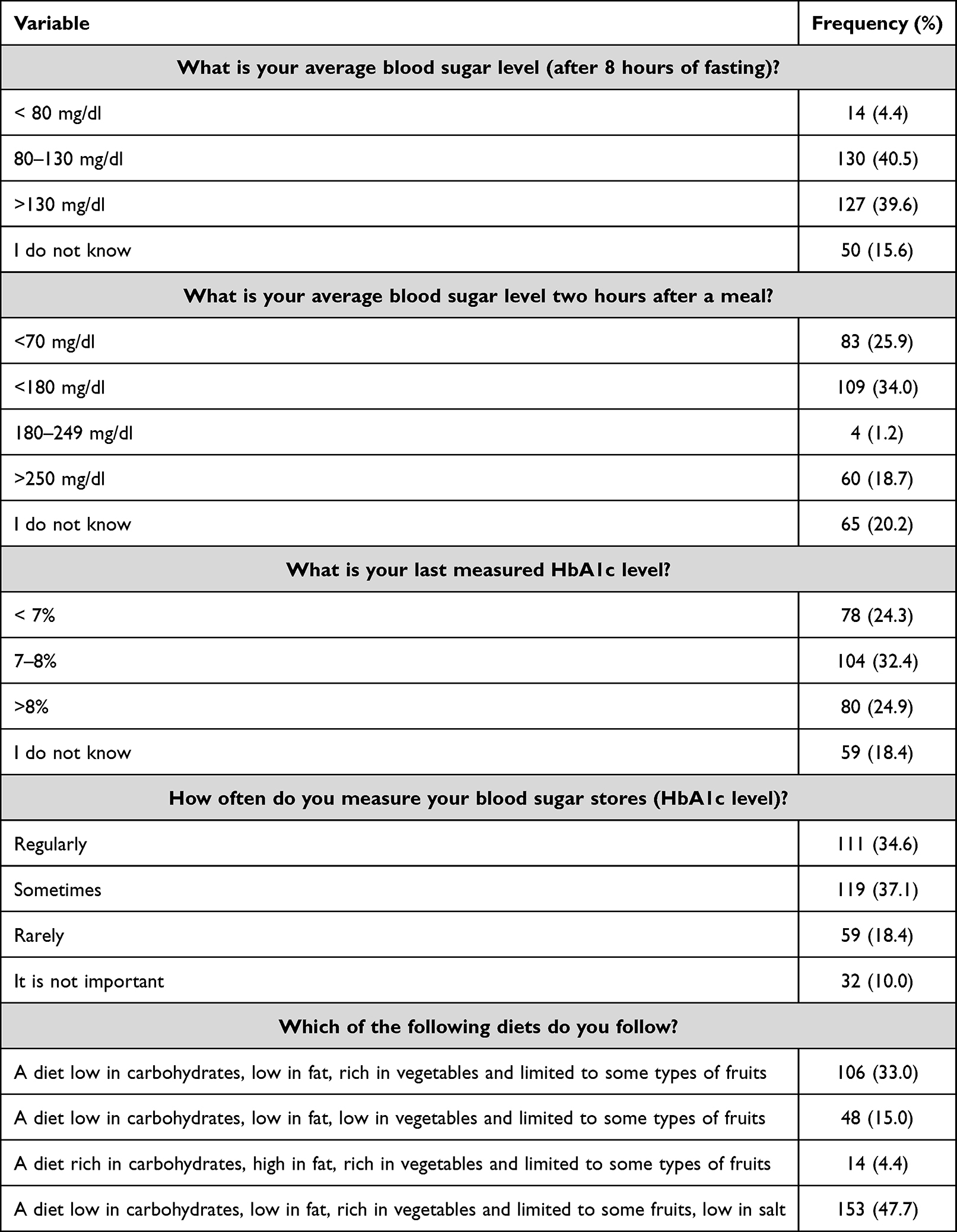 |
Table 2 Participants’ Knowledge About DM |
Patients’ Quality of Life
Most of the study participants reported that their disease did not affect their quality of life to an extent that restricted their ability to live their life normally. Only 8.4% of the study participants reported that their disease did not let them practise their daily activities at all. The most commonly reported problems related to diabetes mellitus and its effect on patients’ quality of life were pain/discomfort (around 68.0% of the patients reported some sort of problems in this dimension), followed by mobility, and depression/anxiety. For further details on participants’ quality of life, please refer to Figure 1.
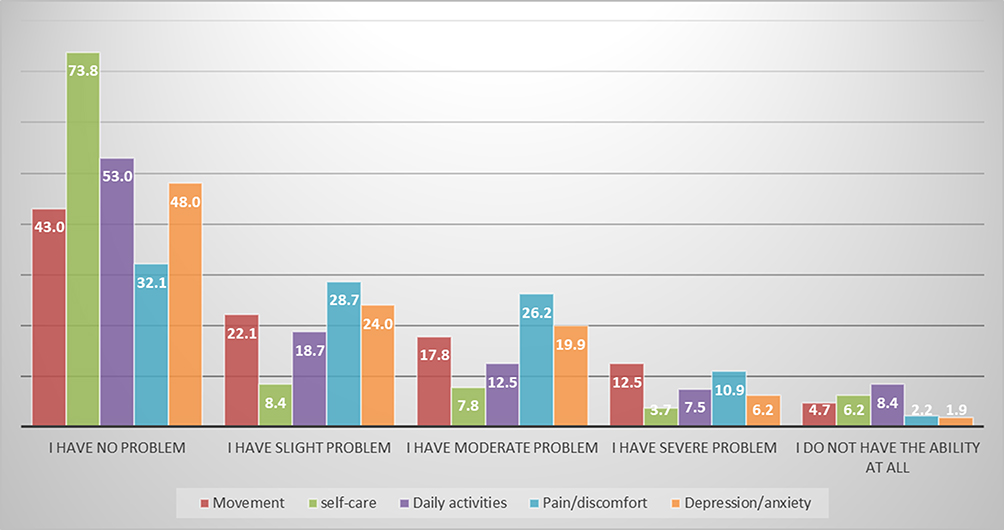 |
Figure 1 Participants quality of life classified as per EQ-5D measures. |
All dimensions of patients’ quality of life significantly differed between different demographic groups based on age (p<0.001). There was a significant difference between males and females in terms of their quality of life, specifically self-care (p=0.001), pain and discomfort (p=0.017), and depression and anxiety (p=0.039). Patients from different marital statuses, education levels, employment status, and duration of the disease showed a significant difference in quality of life, except for depression and anxiety (p>0.05).
The mean score for each of the five quality of life dimensions was quite similar among the participants. The mean mobility score was 2.1 (SD: 1.2), the mean self-care score was 1.6 (SD: 1.2), the mean normal activities score was 2.0 (SD: 1.3), the mean pain and discomfort score was 2.2 (SD: 1.1), and the mean anxiety and depression score was 1.9. (SD: 1.0).
Factors Affecting Quality of Life
Binary logistic regression analysis identified that young age (26–40 years), being married, having a higher level of education, working outside the medical field, having insurance, having a family history of type 2 diabetes mellitus, exercising regularly, and adhering to prescribed medications were all important factors that positively influenced participants’ quality of life, Table 3.
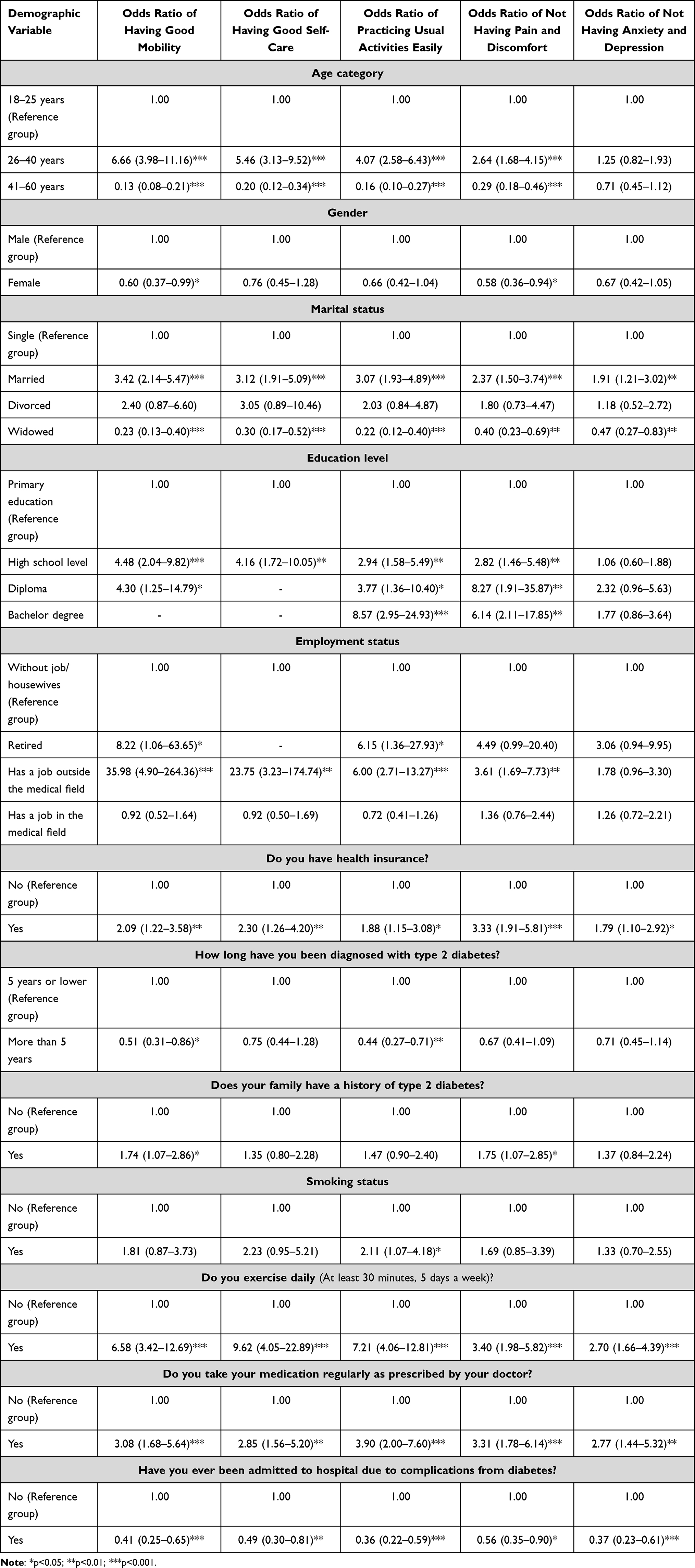 |
Table 3 Binary Logistic Regression Analysis |
Discussion
In this cross-sectional study, we investigated the quality of life for type 2 diabetes mellitus patients in the Al-Ahsa region of Saudi Arabia. The key findings of this study are: a) Approximately 40.5% and 34.0% of participants reported that their average blood sugar level (after eight hours of fasting) is between 80 and 130 mg/dl, respectively, and that their average blood sugar level two hours after a meal is 180 mg/dl.b) only 34.6% of study participants reported measuring their blood sugar levels (HbA1c level) on a regular basis, c) 47.7% of study participants reported eating a healthy diet, d) 8.4% of study participants reported that their disease prevented them from doing their daily activities at all, e) The most commonly reported problems related to diabetes mellitus and its effect on patients’ quality of life were pain/discomfort, followed by mobility, and depression/anxiety, f) patients’ quality of life significantly differed between different demographic groups based on age, gender, marital status, education level, employment status, and duration of the disease, and g) young age (26–40 years), being married, having a higher level of education, working outside the medical field, having insurance, having a family history of type 2 diabetes mellitus, exercising regularly, and adhering to prescribed medications were all important factors that positively influenced participants’ quality of life.
In our study, diabetes mellitus affected the QoL of the patients to varying degrees. A total of 8.4% of our study sample reported that their disease affected their lives completely and that they did not practice their daily activities at all. In our study, the most common QoL problems were pain and discomfort, followed by movement, depression, and anxiety, and the impact on daily activities and self-care. Previous studies that explored the impact of diabetes mellitus on patients’ QoL reported consistent findings that the disease has a negative impact on their lives due to its adverse effects.11,19,20 Moreover, the negative impact on QoL would be if the diabetic patients showed complications.21–23 This is mainly caused by increasing physical discomfort, decreasing activity, and reducing their physical state.24
Duration of disease was one of the main factors that significantly affected patients’ QoL in our study. Previous research found a conflicting relationship between diabetes duration and QoL.25 According to a previous systematic review by Jing et al, the longer the duration, the worse the QoL.24 Another study by Glasgow et al reported that longer duration of diabetes was associated with reduced QoL in T2DM patients.26 This could be due to the fact that glycaemic control tended to be worse with longer duration due to a decline in beta cell function, and a decline in patients’ attitude, adherence, and response to treatment regimen.27
The vast majority of the patients (85.6%) in our study sample were in the age group between 40–60 years of age. A global study on the prevalence of diabetes in developing countries reported that the majority of diabetic patients are in the same age range (45–65 years).28 This was also confirmed by multiple studies, which concluded that age is negatively associated with the patients’ QoL due to the longer duration of the disease.26,29
Around 86.0% of the patients in our study sample had a BMI that ranged from 18–24.9 kg/m2. This could explain why a small proportion of the patients reported problems in terms of pain and discomfort, movement, self-care, daily activities, and depression and anxiety (ranging from 1.9% to 8.4%). Previous studies that explored the association between BMI and QoL reported that high BMI (for obese patients) significantly impairs the QoL of the patients.11,30,31
In our study, 24.3% of the patients reported that their HbA1c level was below 7%, which is a good indicator for diabetes control (the lower the better). Previous literature has confirmed the fact that a lower HbA1c level is associated with better QoL and, as this level increases, QoL deteriorates.32 Previous literature reported that disease control among diabetic patients was one of the most important determinants of QoL.33–35 Furthermore, checking glucose levels on a regular basis may be beneficial for glycemic control and may be a preventive factor for QoL.24,27
The most common diabetes complications in our study were retinopathy, hyperglycaemia, and neuropathy. These are the most troublesome health problems among diabetic patients that interfere with their lives and daily activities. Diabetes complications are associated with impaired QoL; the higher the number of complications, the worse the patients’ QoL becomes.36
In our study, all dimensions of patients’ quality of life were significantly affected by demographic factors such as age, gender, marital status, education level, employment status, and duration of the disease. These factors showed a significant difference in all patients’ quality of life. This was confirmed by a previous study by Olukotun et al that documented that demographic factors affect the QoL of diabetic patients differently.37 Based on this fact, tailored healthcare interventions that take individual variations into consideration should be developed to improve the QoL of patients with T2DM.
In our study, participants with health insurance were more likely to have a better quality of life in all dimensions. This confirms the findings of the previous study that was conducted in India.11 Having an insurance plan is associated with regular checkups, as well as improved coverage for prescription medications, which is associated with higher medication adherence as the likelihood of cost-related nonadherence decreases.11,38
In comparison to others, younger participants (26–40 years old) were more likely to have a greater QoL score. Diabetic patients who are older are more likely to develop problems with their sexual function, musculoskeletal system, and psychological well-being.39–41 Besides, a previous meta-analysis reported that having complications leads to worse QoL in term of physical functioning, bodily pain, social functioning, and general health perception.21–24
Previous research has found a negative relationship between age and physical activity.15 Besides, marital status, employment status, and practicing daily activities were important factors that influenced diabetic patients’ QoL.15,16 Education is an important predictive factor of socioeconomic status, which is related to QOL in diabetes.17,18 A previous meta-analysis reported that practicing physical exercise is associated with better QoL.24 Practicing regular exercise improved participants’ vitality, social functioning, emotional status, and general health perception.21,24 Additionally, practicing regular exercise is correlated with better diabetes control.42,43
One interesting finding from our study was that patients with a family history of diabetes had a higher QoL score than those without. This could be linked to the fact that having a good understanding of the disease’s natural history helped people establish a positive attitude towards type 2 diabetes.27
Strengths and Limitations
This study is among the few studies that have explored the QoL of T2DM patients in Saudi Arabia. At the same time, this study has limitations. First, the cross-sectional design of the study restricted our ability to explore causal associations between the demographic variables and QoL of patients with T2DM. Second, we used a self-reported questionnaire to collect the data for this study, which could be a potential source of bias. Third, the participants in this study were recruited from the Al-Ahsa region, which could limit the generalisability of our findings to other regions in Saudi Arabia. Patients as young as 18 years old and as old as 60 years old have different disease progressions. This could have had an impact on the patients’ quality of life. We were unable to determine the response rate for our study, which may have resulted in nonresponse bias because we were unable to demonstrate how well the sample was selected from the target population. As a result, our findings should be interpreted carefully.
Conclusions
Diabetes mellitus affects the QoL for patients with T2DM at different levels. Pain/discomfort, mobility, and depression/anxiety are the main problems that are affecting the QoL of diabetic patients. Future studies are recommended to explore the effectiveness of patient tailored interventions to decrease the negative impact of these dimensions on patients’ QoL.
Ethical Approval
Ethical approval was obtained for this study from the Research Ethics Committee at King Faisal University, Alhasa, Saudi Arabia (No.66350).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Deanship of Scientific Research (DSR, Grant no. 262), King Faisal University, AlAhsa, Saudi Arabia.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Solli O, Stavem K, Kristiansen I. Health-related quality of life in diabetes: the associations of complications with EQ-5D scores. Health Qual Life Outcomes. 2010;8(1):1–8. doi:10.1186/1477-7525-8-18
2. Ookoba A, Obateru O, Olokoba L. Type 2 diabetes mellitus: a review of current trends. Oman Med J. 2012;27(4):269–273. doi:10.5001/omj.2012.68
3. Skyler JS, Bakris GL, Bonifacio E, et al. Differentiation of diabetes by pathophysiology, natural history, and prognosis. Diabetes. 2017;66(2):241–255. doi:10.2337/db16-0806
4. Naser AY, Wong ICK, Whittlesea C, et al. Use of multiple antidiabetic medications in patients with diabetes and its association with hypoglycaemic events: a case-crossover study in Jordan. BMJ Open. 2018;8(11):e024909. doi:10.1136/bmjopen-2018-024909
5. Naser AY, Wong ICK, Whittlesea C, et al. Attitudes and perceptions towards hypoglycaemia in patients with diabetes mellitus: a multinational cross-sectional study. PLoS One. 2019;14(10):e0222275. doi:10.1371/journal.pone.0222275
6. Naser AY, Alsairafi Z, Alwafi H, et al. The perspectives of physicians regarding antidiabetic therapy de-intensification and factors affecting their treatment choices-A cross-sectional study. Int J Clin Pract. 2021;75(1):e13662. doi:10.1111/ijcp.13662
7. Chung J, Cho D, Chung D, Chung M. Assessment of factors associated with the quality of life in Korean type 2 diabetic patients. Intern Med. 2013;52(2):179–185. doi:10.2169/internalmedicine.52.7513
8. Naser AY, Alwafi H, Alsairafi Z. Cost of hospitalisation and length of stay due to hypoglycaemia in patients with diabetes mellitus: a cross-sectional study. Pharm Pract. 2020;18(2):1847.
9. World Health Organization. WHOQOL: measuring quality of life; 2021. Available from: https://www.who.int/tools/whoqol.
10. Abedini M, Bijari B, Miri Z, Shakhs EF, Abbasi A. The quality of life of the patients with diabetes type 2 using EQ-5D-5 L in Birjand. Health Qual Life Outcomes. 2020;19(1):1–9.
11. Prajapati VB, Blake R, Acharya LD, Seshadri S. Assessment of quality of life in type II diabetic patients using the modified diabetes quality of life (MDQoL)-17 questionnaire. Braz J Pharma Sci. 2018;53(4). doi:10.1590/s2175-97902017000417144
12. EuroQoL. EQ-5D-5L | About; 2017. Available from: https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/.
13. Aburuz S, Bulatova N, Twalbeh M, Gazawi M. The validity and reliability of the Arabic version of the EQ-5D: a study from Jordan. Ann Saudi Med. 2009;29(4):304–308. doi:10.4103/0256-4947.55313
14. Bekairy A, Bustami R, Almotairi M, et al. Validity and reliability of the Arabic version of the the EuroQOL (EQ-5D). A study from Saudi Arabia. Int J Health Sci. 2018;12(2):16–20.
15. Ghanbari A, Yekta Z, Roushan Z, Lakeh N. Assessment of factors affecting quality of life in diabetic patients in Iran. Public Health Nurs. 2005;22(4):311–322. doi:10.1111/j.0737-1209.2005.220406.x
16. Wändell P, Brorsson B, Aberg H. Quality of life in diabetic patients registered with primary health care services in Sweden. Scand J Prim Health Care. 1997;15(2):97–102. doi:10.3109/02813439709018495
17. Eriksson L, Nordström G, Berglund T, Sandström E. The health-related quality of life in a Swedish sample of HIV-infected persons. J Adv Nurs. 2000;32(5):1213–1223. doi:10.1046/j.1365-2648.2000.01592.x
18. Rubin R, Peyrot M. Quality of life and diabetes. Diabetes Metab Res Rev. 1999;15(3):205–218. doi:10.1002/(SICI)1520-7560(199905/06)15:3<205::AID-DMRR29>3.0.CO;2-O
19. Gautam Y, Sharma A, Agarwal A, Bhatnagar M, Trehan R. A cross-sectional study of QOL of diabetic patients at Tertiary Care Hospitals in Delhi. Indian J Community Med. 2009;34(4):346–350. doi:10.4103/0970-0218.58397
20. Anumol M, Anusree TK, Aparna MA, et al. Quality of life among type 2 diabetes mellitus patients in south India: a descriptive study. Am Int J Res Human Arts Soc Sci. 2014;7(2):197–200.
21. Tang W, Wang Y, Du W, Cheng N, Chen B. Assessment of quality of life and relevant factors in elderly diabetic patients in the Shanghai community. Pharmacoepidemiol Drug Saf. 2006;15:123–130. doi:10.1002/pds.1166
22. Shiu A, Thompson D, Wong R. Quality of life and its predictors among Hong Kong Chinese patients with diabetes. J Clin Nurs. 2008;17:125–132. doi:10.1111/j.1365-2702.2007.02036.x
23. Wexler D, Grant R, Wittenberg E. Correlates of health-related quality of life in type 2 diabetes. Diabetologia. 2006;49:1489–1497. doi:10.1007/s00125-006-0249-9
24. Jing X, Chen J, Dong Y, et al. Related factors of quality of life of type 2 diabetes patients: a systematic review and meta-analysis. Health Qual Life Outcomes. 2018;16(1):189. doi:10.1186/s12955-018-1021-9
25. Al Hayek A, Robert A, Al S, Alzaid A, Al Sabaan F. Factors associated with health-related quality of life among Saudi patients with type 2 diabetes mellitus: a cross-sectional survey. Diabetes Metab J. 2014;38(3):220–229. doi:10.4093/dmj.2014.38.3.220
26. Glasgow R, Ruggiero L, Eakin E, Dryfoos J, Chobanian L. Quality of life and associated characteristics in a large national sample of adults with diabetes. Diabetes Care. 1997;20(4):562–567. doi:10.2337/diacare.20.4.562
27. Daher A, AlMashoor S, Winn T. Glycaemic control and quality of life among ethnically diverse Malaysian diabetic patients. Qual Life Res. 2015;24(4):951–958. doi:10.1007/s11136-014-0830-5
28. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27(5):1047–1053. doi:10.2337/diacare.27.5.1047
29. Gholami A, Azini M, Borji A, Shirazi F, Sharafi Z. Quality of life in patients with type 2 diabetes: application of WHOQoL-BREF scale. Shiraz E-Med J. 2013;14(3):162–171.
30. Kolotkin R, Meter K, Williams G. Quality of life and obesity. Obes Rev. 2001;2(4):219–229. doi:10.1046/j.1467-789X.2001.00040.x
31. Hlatky M, Chung S, Escobedo J, Hillegass W, Melsop K, Rogers W. The effect of obesity on quality of life in patients with diabetes and coronary artery disease. Am Heart J. 2010;159(2):292–300. doi:10.1016/j.ahj.2009.11.004
32. Stanetić K, Savić S, Račić M. The quality of life of patients with type II diabetes mellitus. Општа медицина. 2012;18(3):70–77.
33. Shim Y, Lee J, Toh M, Tang W, Ko Y. Health-related quality of life and glycaemic control in patients with type 2 diabetes mellitus in Singapore. Diabetic Med. 2012;29:e241–8. doi:10.1111/j.1464-5491.2012.03689.x
34. Weinberger M, Kirkman M, Samsa G, et al. The relationship between glycemic control and health related quality of life in patients with non-insulin-dependent diabetes mellitus. Med Care. 1994;32:1173–1181. doi:10.1097/00005650-199412000-00002
35. U.K. Prospective diabetes study group. Quality of life in type 2 diabetic patients is affected by complications but not by intensive policies to improve blood glucose or blood pressure control (UKPDS 37). Diabetes Care. 1999;22:1125–1136. doi:10.2337/diacare.22.7.1125
36. Thommasen H, Zhang W. Health-related quality of life and type 2 diabetes: a study of people living in the Bella Coola Valley. BCMJ. 2006;48(6):272–278.
37. Olukotun O, Akinboboye O, Williams JS, Ozieh M, Egede LE. Influences of demographic, social determinants, clinical, knowledge, and self-care factors on quality of life in adults with type 2 diabetes: black-white differences. J Racial Ethn Health Disparities. 2021. doi:10.1007/s40615-021-01058-9
38. Naser AY. Cost-related nonadherence for prescription medications: a cross-sectional study in Jordan. Expert Rev Pharmacoecon Outcomes Res. 2021;2001:1–7.
39. Podolsky S. Diagnosis and treatment of sexual dysfunction in the male diabetic. Med Clin North Am. 1982;66(6):1389–1396. doi:10.1016/S0025-7125(16)31371-2
40. Chew B, Vos R, Metzendorf M, Scholten R, Rutten G. Psychological interventions for diabetes-related distress in adults with type 2 diabetes mellitus. Cochrane Database Syst Rev. 2017;9(9):CD011469. doi:10.1002/14651858.CD011469.pub2
41. Verma S, Luo N, Subramaniam M, et al. Impact of depression on health related quality of life in patients with diabetes. Ann Acad Med Singap. 2010;39(12):913–917.
42. Cong J, Zhao Y, Qy X, Zhong C, Xing Q. Health-related quality of life among Tianjin Chinese patients with type 2 diabetes: a cross-sectional survey. Nurs Health Sci. 2012;14(4):528–534. doi:10.1111/j.1442-2018.2012.00734.x
43. Colberg S, Albright A, Blissmer B, et al. Exercise and type 2 diabetes: the American College of Sports Medicine and the American Diabetes Association: joint position statement. Diabetes Care. 2010;33:e147–167. doi:10.2337/dc10-9990
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.