")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
The Health Diary Telemonitoring and Hospital-Based Home Care Improve Quality of Life Among Elderly Multimorbid COPD and Chronic Heart Failure Subjects
Authors Persson HL , Lyth J , Lind L
Received 26 October 2019
Accepted for publication 24 January 2020
Published 9 March 2020 Volume 2020:15 Pages 527—541
DOI https://doi.org/10.2147/COPD.S236192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Hans Lennart Persson,1,2 Johan Lyth,3,4 Leili Lind5,6
1Department of Respiratory Medicine in Linköping, Linköping University, Linköping SE-581 85, Sweden; 2Department of Biomedical and Clinical Sciences, Linköping University, Linköping SE-581 85, Sweden; 3Research and Development Unit in Region Östergötland, Linköping University, Linköping SE-581 85, Sweden; 4Department of Health, Medicine and Caring Sciences, Linköping University, Linköping SE-581 85, Sweden; 5Department of Biomedical Engineering/Health Informatics, Linköping University, Linköping SE-581 85, Sweden; 6Digital Systems Division, Department of Industrial Systems, RISE Research Institutes of Sweden, Linköping University, Linköping, S-581 83, Sweden
Correspondence: Hans Lennart Persson
Department of Respiratory Medicine in Linköping, Linköping University, Linköping SE-581 85, Sweden
Tel +46 13 10 1033621
Email [email protected]
Background: Elderly, multimorbid patients with advanced chronic obstructive pulmonary disease (COPD) and/or chronic heart failure (CHF) exhibit poor health-related quality of life (HRQoL). Telemonitoring, based on digital pen technology, supported by hospital-based home care (HBHC) significantly reduces the number of hospitalizations. We hypothesized that the same intervention would prevent the deterioration of HRQoL that follows upon disease progression.
Methods: Elderly computer-illiterate subjects with ≥ 2 hospitalizations the previous year were included. HRQoL was assessed at inclusion (baseline) and at 1, 6 and 12 months employing EuroQol-5 Dimensions (EQ-5D) and RAND-36 for general HRQoL, and Minnesota Living with Heart Failure Questionnaire (MLHFQ) and St. Georges Respiratory Questionnaire (SGRQ) for disease-specific HRQoL. Healthcare contacts, hospitalizations, as-needed medications, prescription changes and healthcare costs were registered.
Results: Ninety-four patients were enrolled of which 53 subjects completed the 12-month study period. Compared to baseline, most domains of RAND-36 were improved significantly at 1 time-point or more. Only among COPD subjects, the disease-specific HRQoL was worsened at the 12 month evaluation. Measures of healthcare dependency were associated with poor HRQoL.
Conclusion: The Health Diary system and HBHC together improve general HRQoL, and measures of healthcare dependency are associated with HRQoL variables.
Keywords: digital pen, exacerbation, home care services, hospital-based, hospitalization, multimorbidity, telemedicine, QoL
Introduction
Both chronic obstructive pulmonary disease (COPD) and chronic heart failure (CHF) are progressive diseases characterized by organ failure and frequent hospitalizations at end-stage diseases.1,2 As both diseases are associated with significant co-morbidity,3 they also commonly co-exist.4 Symptom distress due to COPD or CHF is associated with poor health-related quality of life (HRQoL).5,6 Deterioration of HRQoL occurs over time as the diseases progress.7,8 At end-stage diseases, subjects with COPD and CHF typically experience impaired functioning and impaired HRQoL.9,10 Janssen et al compared subjects with advanced COPD or CHF in a 12-month longitudinal study.11 Impaired HRQoL correlated with physical and psychological symptoms, care dependency and number of drugs, while age, gender, disease severity and co-morbidities did not.11
The effects of telemonitoring on HRQoL have been evaluated among subjects with COPD and CHF with varying success.12,13 One meta-analysis reports inconsistent findings on the positive impact of telehealthcare on HRQoL measures among CHF subjects.13 Indeed, a recent study by Cichosz et al demonstrated that only the short form (SF)-36 questionnaire Mental Component Summary score was significantly higher among CHF subjects in the telehealthcare group compared to the control group during the 12-month follow-up.14 In that study, the Kansas City Cardiomyopathy Questionnaire (KCCQ) was used to assess the disease-specific HRQoL, which did not differ between the two groups of CHF subjects.14 As for subjects with COPD, Lilholt et al recently reported no statistically significant differences in general HRQoL, assessed by Short Form 36-Item Health Survey, between telehealthcare and usual practice.15 The review and meta-analysis by McLean et al indicated a possible impact of telehealthcare on the HRQoL of COPD subjects.16 Moreover, a review by Cruz et al indicated inconsistency in HRQoL findings, but most of the studies reported no significant changes in HRQoL.17 Possibly, the inconsistent results reported were due to the different HRQoL instruments employed.16,17
We have recently reported on the eHealth Diary study, which is a 12-month longitudinal telemonitoring study.18,19 Elderly, multimorbid subjects, the majority computer illiterate with advanced stages of CHF and COPD, were included.18,19 Clinical features, such as disease severity, as well as number of hospitalizations, healthcare contacts and ensuing healthcare costs were registered during an intervention of telemonitoring, employing digital pen technology, combined with healthcare provided by a hospital-based home-care (HBHC) unit.18,19 Subjects were very ill and death was the major cause for not finalizing the study; the death rate was 36% and 28% among COPD and CHF subjects, respectively.18 Compared to the 12-month prior inclusion, the intervention significantly reduced number of hospitalization.18 Accordingly, costs associated with hospitalizations were significantly reduced for both CHF and COPD subjects.19
The present study is an intervention non-randomized single-center clinical study compared with expected outcomes. We hypothesized that an intervention, consisting of the Health Diary telemonitoring system supported by HBHC, would at least maintain HRQoL among the elderly, multimorbid subjects included. Thus, we thought the intervention would to some extent compensate for the expected loss of HRQoL when advanced stage of disease progress into end-stage disease and ultimately death. Moreover, we also hypothesized that measures of healthcare dependency would be of great importance for the HRQoL displayed by these subjects. The primary aim was to assess HRQoL, general and disease-specific, during a 12-month intervention in the study population. Secondary aims were to evaluate the influence of measures of healthcare dependency on HRQoL or vice versa. Measures of healthcare dependency were the registered use of as-needed (pro re nata; P.R.N.) medications, the number of changes of prescribed medications, alarms and all healthcare contacts and related costs during the study period. For hospitalizations, we also included the number of those during the 1-yr prior inclusion.
Materials and Methods
Study Setting and Design
This study is part of the longitudinal study the eHealth Diary study that was performed at the HBHC unit, Linköping University Hospital. Thus, study settings and design are described in more detail elsewhere.18,19
Briefly, following written informed consent to participate in the study patients aged ≥65 years with ≥2 hospitalizations due to exacerbation for either COPD or CHF during the last 12 months were included in the study. The study lasted a 4-yr period (November 2013-December 2017) due to an inclusion period of 3 yrs and a planned study period of 12 months for each patient. Subjects participating in the eHealth Diary study received a multi-disciplinary healthcare of COPD and/or CHF provided by HBHC, but study subjects had to consult primary care or other care providers for health conditions not related to CHF or COPD or end-of-life care. Subjects reported their daily health status using a digital pen and a Health Diary paper form (green, yellow, blue), thereby providing the professional caregivers at HBHC, nurses and/or physicians supervising the system, with data signaling early signs of patients’ deterioration. CHF subjects reported their health using the green and blue Health Diary forms, and the COPD subjects used the yellow and blue forms.18 The Health Diary forms let the subjects report various symptoms, measurement values and intake of P.R.N. medication. Moreover, the subjects could write free text messages on each form if desirable. Responsible physicians decided on individual ranges for all symptoms and measurements to be reported by the subjects and adjusted these whenever needed. If the reported values were below/above the limits, the system generated alarms. Besides showing these alarms as icons in the Health Diary system, more serious alarms, generated due to low oxygen saturation or an increased breathlessness, were additionally shown as Short Message Service (SMS; cellular phone text messaging) text messages in a mobile nurse phone. SMS alarms were also generated if a patient failed to send in a report or if the care providers forgot to check and sign the patient report in time (for more details, see Reference [18]).
Co-morbidities were documented at baseline and scored accordingly using the Charlson Co-morbidity index (CCI).
Assessment of General and Disease-Specific Health-Related Quality of Life
All study subjects were asked to complete validated questionnaires reflecting general and disease-specific HRQoL at the time of inclusion (hereafter called “baseline”) and at 1, 6 and 12 months of the study period. The minimal clinically important difference (MCID) is defined as the cut-off for clinically meaningful changes.
For assessment of general HRQoL, two questionnaires were employed; EuroQol-5 Dimensions (EQ-5D)20 and the RAND-36, the latter developed by the RAND company.21 EQ-5D consists of five questions assessing mobility (EQ-5D1), self-care (EQ-5D2), usual activity (EQ-5D3), pain/discomfort (EQ-5D4) and anxiety/depression (EQ-5D5). For every question, the subject can choose either “no problems”, “some problems” or “extreme problems”. An index score is created; −0.59 is the worst and 1.0 is the best. Subjects are also requested to score their current health using a visual analogue scale (VAS), which ranges from 0 to 100 (0 = worst possible health; 100 = best possible health). The RAND-36 questionnaire is validated in previous studies.22 It consists of 36 items, which are divided into eight domains assessing physical functioning (PF), role-physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role-emotional (RE) and mental health (MH). For each domain, scores range from 0, which is the worst, to 100 points, which is the best.
For assessment of disease-specific HRQoL among COPD and CHF subjects, the St. Georges Respiratory Questionnaire (SGRQ)23 and the Minnesota Living with Heart Failure Questionnaire (MLHFQ)24 were employed, respectively. SGRQ consists of three domains (symptoms, activities, and impact), which together give a total score, ranging from 0 points, which is the best, to 100 points, which is the worst. MLHFQ consists of two domains [physical, which ranges from 0 points (the best) to 40 points (the worst), and emotional, which ranges from 0 points (the best) to 25 points (the worst)], which together give a total score, which ranges from 0 points, which is the best, to 105 points, which is the worst.
Collection of Data on Healthcare Dependency
Every use of P.R.N. medication and every change of prescription were registered. Common P.R.N. medication, often used by COPD and/or CHF patients, was listed on the Health Diary forms for the subject to put a mark on, if taken. The listed P.R.N. medications were: “Extra inhalation”, “Cortisone”, “Antibiotics”, “Extra anxiolytics”, “Diuretics”, “Nitroglycerines” and “Other as needed medication”. For example, if a COPD subject was prescribed extra inhalation and anxiolytics for shortness of breath, he/she could decide to take these P.R.N. medications and report this via the Health Diary. For every study subject, data on healthcare contacts (hospitalization and outpatient) and direct healthcare costs were collected for one yr or to date of death or earlier exclusion. For hospitalizations, the number during the 1-yr period prior the study inclusion was also recorded. All uses of healthcare resources and costs were registered since COPD and CHF are systemic disorders, which may cause hospitalization for various reasons. By employing the unique 10-digit Swedish personal identity number, patient data were then linked to the Care Data Warehouse in Östergötland (CDW) and the Cost Per Patient database (CPP). The CDW registers all healthcare contacts (hospitalization, outpatient, and primary care) including both private care and public care, while CPP records costs for all contacts within the public care only. Types of healthcare contacts were hospitalization, physician visit, district nurse visit, registered nurse visit, and visit to nurse assistant. Less than 1% of contacts with missing costs were related to inpatient care. The contacts with health services were then divided into hospitalization, emergency care, primary care, other outpatient care, and care provided by the multi-disciplinary team of the HBHC unit.19
Ethics
The study was approved by the Regional Ethical Review Board in Linköping, Sweden (no. 213/309-31) and was registered at ISRCTN (ISRCTN34252610). The study was conducted in accordance with the Declaration of Helsinki, the guidelines of the International Conference on Harmonization of Good Clinical Practice (ICH-GCP), and the applicable Swedish laws. It was required that study subjects gave informed written consent before participation.
Statistical Analysis
Subject’s baseline characteristics and HRQoL are presented as means ± 1 S.D. (range) for continuous variables and percentage for categorical variables. The Student’s t-test was used on continuous variables and the Chi-square test was used on categorical variables when comparing CHF and COPD subjects. Fisher’s exact test was used on EQ-5D dimensions because of few numbers in each category. Because of repeated measures per subject (baseline, +1, +6 and +12 months), the Generalized Estimating Equations (GEE) method was used to assess HRQoL over time with baseline as reference. In all models, a normal distribution with an identity link was used and correlations were handled by an unstructured correlation matrix. Estimated marginal means for all time points were extracted from the GEE method and values for +1, +6 and +12 months were compared to baseline. Correlations between healthcare dependency variables and mean HRQoL values were calculated with Pearson’s correlation coefficient (r). Healthcare dependency variables as well as baseline characteristics were further investigated against HRQoL using a backward elimination linear regression. The level of significance was 0.05 and all p-values were two-tailed. All analyses except for the Fisher’s exact test were undertaken using SPSS version 25.0 (IBM Corp., Armonk, NY). Fisher’s exact test was undertaken using R version 3.5.2 (R Core Team, Vienna, Austria).
Results
Health-Related QoL at Baseline
Compared to elderly multimorbid subjects with CHF as a major cause of hospitalizations, subjects with COPD as a major cause of hospitalizations were significantly younger and thinner and had significantly more pack-yrs tobacco and co-morbidities (Table 1). Subjects with COPD also exhibited significantly reduced lung function, reflected by lower FEV1 as % of predicted and lower blood oxygenation (Table 1). Some COPD subjects even depended on LTOT (Table 1). Both diseases presented with advanced stages, reflected by NYHA stage 3–4 and GOLD stage C-D (Table 1).
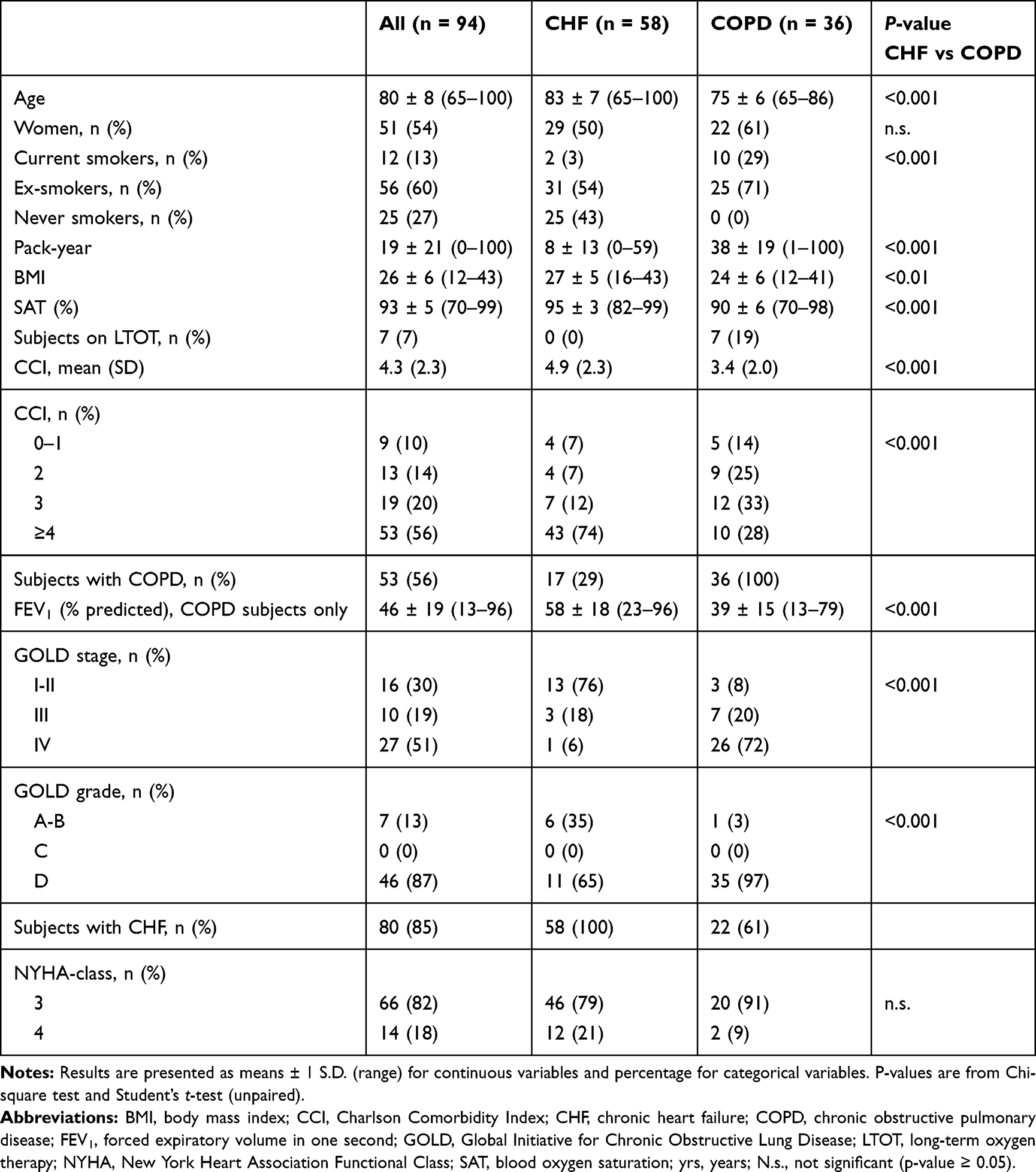 |
Table 1 Subject Characteristics |
The major reason to stop study participation was death; 28% in the CHF group and 36% in the COPD group. Other reasons for not finalizing the study period were physical or cognitive deterioration or change of residency, mostly by moving to a nursing home.
Despite the described differences of clinical features, CHF and COPD subjects exhibited great similarity regarding their general HRQoL at baseline. Results are summarized in Table 2. Indeed, only the domain GH of the RAND-36 differed significantly (Table 2). Consequently, for further analysis of general HRQoL changes over time the two groups were analyzed as a single group.
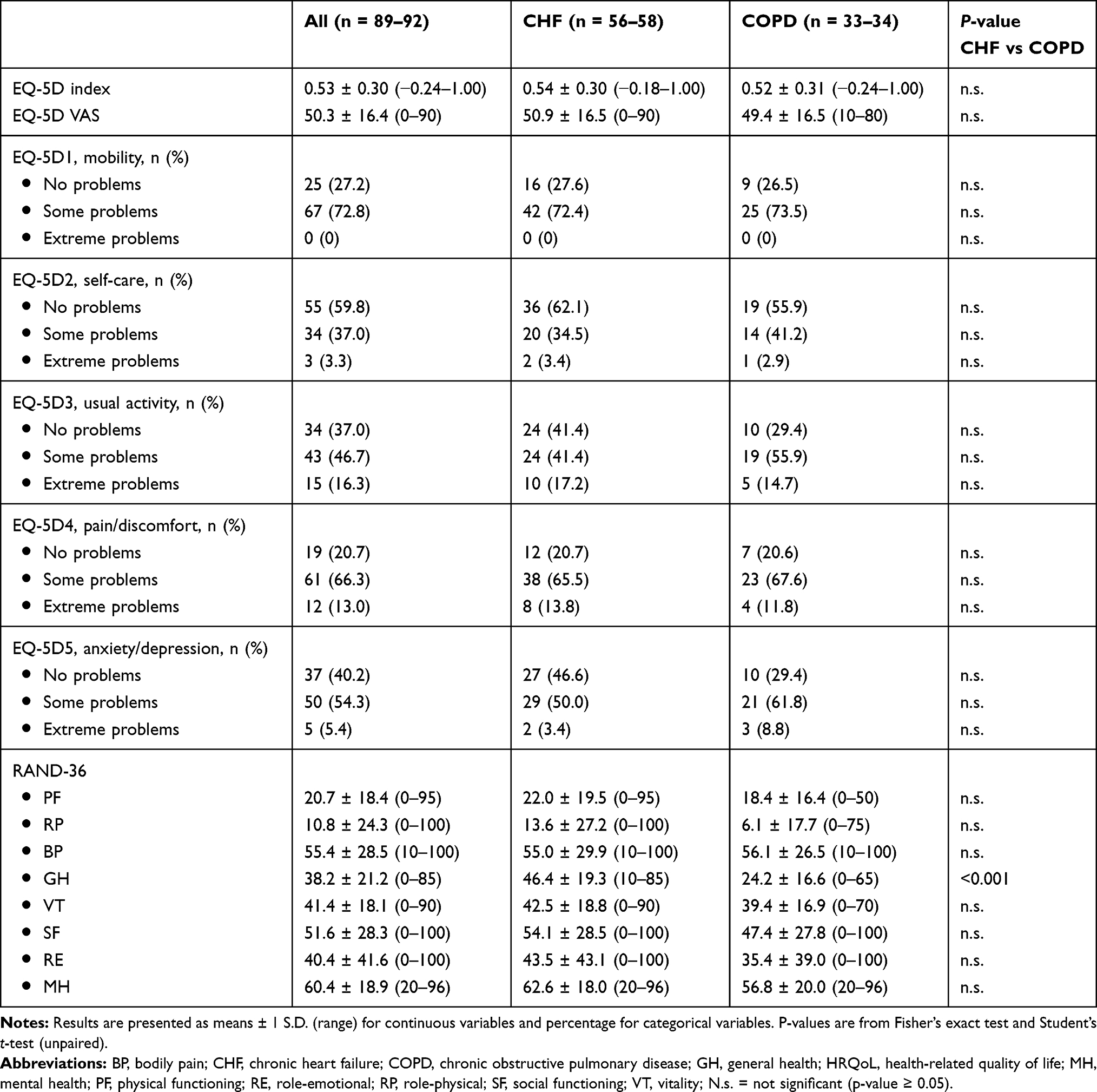 |
Table 2 General HRQoL Assessed with EQ-5D and RAND-36 at Inclusion (Baseline) |
General and Disease-Specific Health-Related QoL Over Time
Compared to baseline, general HRQoL assessed for all subjects at +1, +6 and +12 months using EQ-5D and RAND-36 demonstrated a significant improvement of almost all variables at ≥1 time point (Table 3). Exceptions were the EQ-5D index and the RAND-36 domain PF, which did not deviate from baseline significantly at any time-point (Table 3). Although significant, the improvement of EQ-5D VAS did not reach the specified MCID, which is set to 8 points.25 In contrast, all significant improvements of the RAND-36 domains were above the 3–5 points specified as the MCID of RAND-36.26
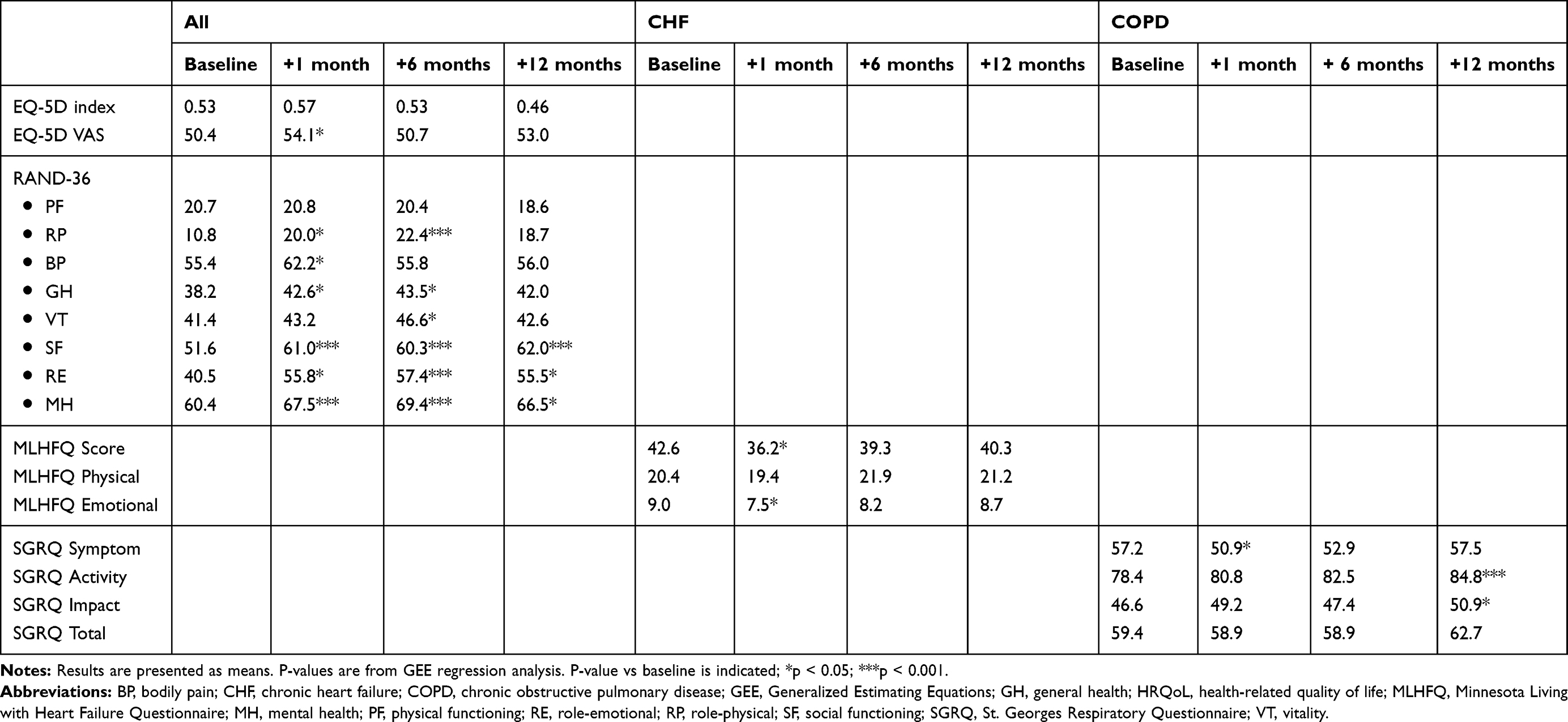 |
Table 3 General and Disease-Specific HRQoL – Changes Over Time |
Disease-specific HRQoL among CHF subjects, assessed as the change of the MLHFQ score and emotional domain from baseline, was significantly improved at +1 month, and disease-specific HRQoL among COPD subjects, assessed as the change of the symptom domain of SGRQ from baseline, was also significantly improved at +1 month (Table 3). However, by time disease-specific HRQoL became worsened among the COPD subjects as reflected by significant deviations from baseline of the SGRQ domain activity and impact, which appeared at +12 months (Table 3). Although significant, the improvement of the MLHFQ score at +1 month did not reach the specified MCID, considered as 8.2027 and neither did the significant improvement of the SGRQ symptom domain noted at +1 month (Table 3). In contrast, the worsening of the SGRQ domain activity and impact noted at +12 months did exceed the MCID limit set at 4 points (Table 3).28
Healthcare Dependency
Advanced stage of the disease, and in many cases even end-stage disease resulting in death during the study period, was described in measures of healthcare dependency. Measures used to assess healthcare dependency and the results of these are presented for all subjects and the sub-groups CHF and COPD subjects in Table 4. Compared to CHF subjects, COPD subjects had significantly more prescription changes, home visits by a physician and total home care contacts executed by HBHC and more contacts with primary care (Table 4). During the 4 yr eHealth Diary study, the subjects together reported a total of 74,923 assessed symptoms and measured physiological parameters. The number of reported symptoms and measurements that generated the more serious SMS alarms, due to certain values outside predetermined limits, was significantly higher among COPD subjects, as were all SMS alarms, including SMS alarms due to subjects missing their daily reports and care providers missing to sign incoming reports (Table 4). Moreover, COPD subjects demonstrated significantly greater costs regarding HBHC, primary care, other outpatient care and subsequently total costs as well (Table 4).
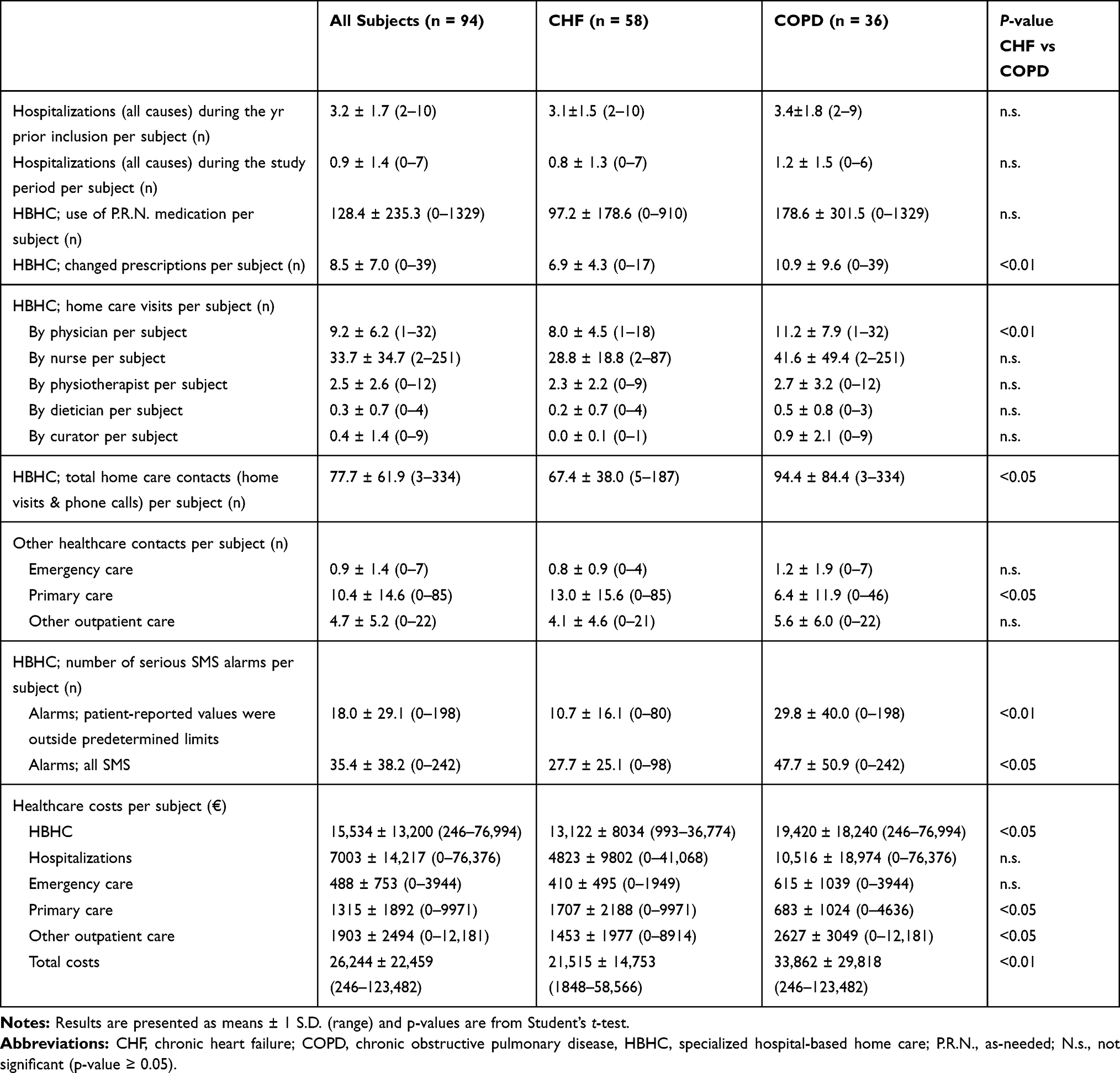 |
Table 4 Measures of Healthcare Dependency |
Extensive Healthcare Dependency Is Associated with Poor HRQoL
Next, we assessed correlations between measures of healthcare dependency and HRQoL variables (Table 5). Among all subjects, number of P.R.N medications per subject negatively correlated with the EQ-5D index. Likewise, number of HBHC home visits by physician and number of HBHC phone calls by curator per subject negatively correlated with the RAND-36 domains VT and MH, respectively. Among CHF subjects, number of HBHC phone calls by nurse and number of HBHC phone calls by physician correlated positively with MLHFQ score and the emotional domain of MLHFQ, respectively. Among COPD subjects, number of HBHC home visits by physiotherapist correlated positively with SGRQ total score. All these correlations were significant when tested in a multivariable regression analysis (for details see below). Regarding all SMS alarms, Pearson’s correlation coefficients were significant for the GH and RE domains of RAND-36, but these correlations were not significant when tested in the multivariable regression model.
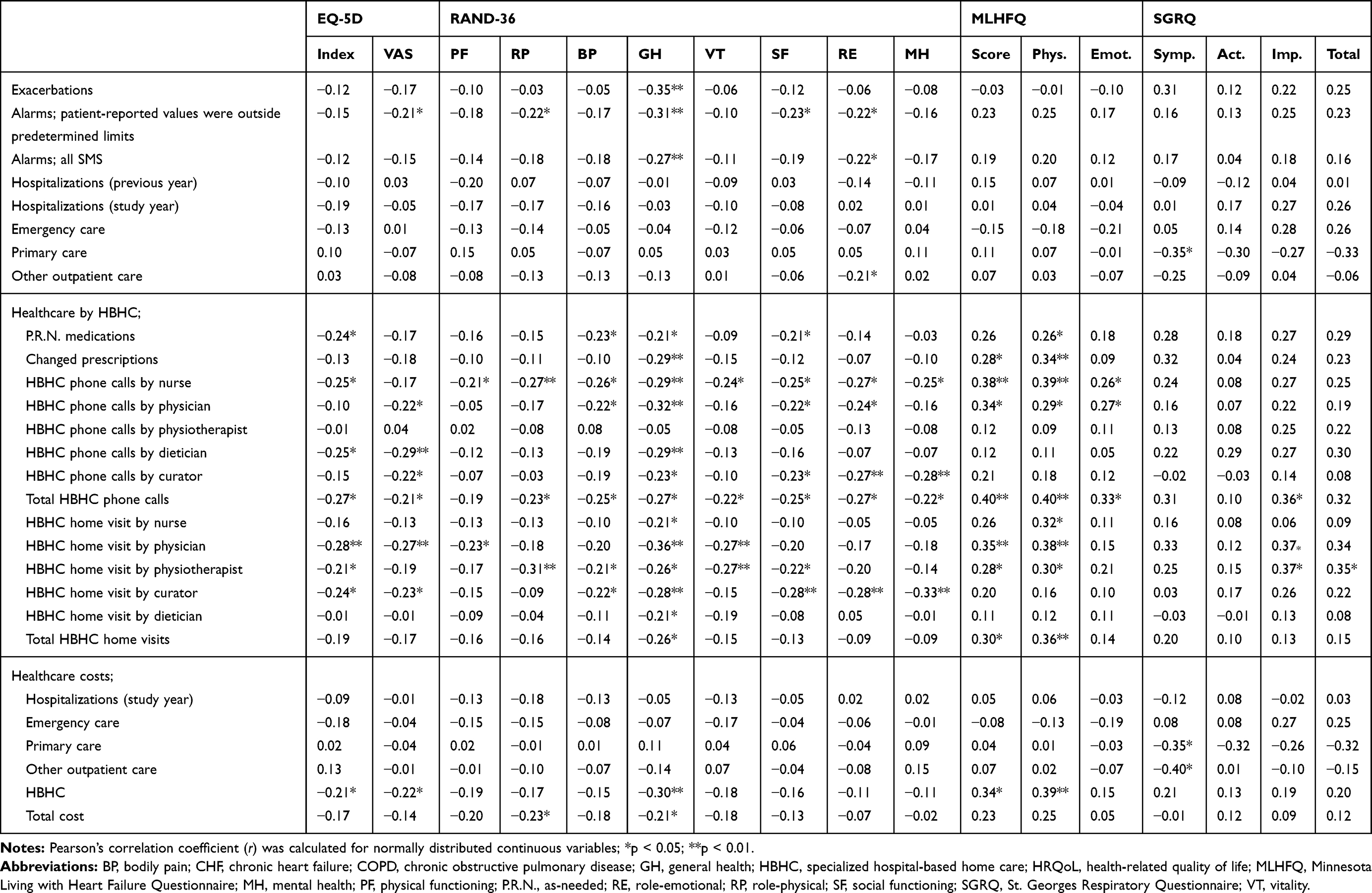 |
Table 5 Significant Correlations of Measures of Healthcare Dependency and HRQoL Variables |
Using a multivariable linear regression analysis (backward elimination method) the correlations stated in Table 5 were all significant. Results are summarized in Table 6. Additional significant correlations were: use of P.R.N. medications was positively associated with the symptom domain of SGRQ among COPD subjects; the number of HBHC phone calls by nurse was negatively associated with GH, RE and MH domains of RAND-36 among all subjects and positively associated with the physical domain of MLHFQ among CHF subjects; the number of HBHC phone calls by physician was positively associated with the impact domain of SGRQ among COPD subjects; the number of HBHC home visits by physiotherapist was negatively associated with the RP and BP domains of RAND-36 among all subjects; the number of HBHC total home visits was negatively associated with the EQ-5D index and the PF and SF domains of RAND-36 among all subjects; healthcare costs for hospitalizations during the study period were positively associated with the impact domain of SGRQ among COPD subjects; healthcare costs for HBHC were negatively associated with index and VAS of EQ-5D and the PF and SF domains of RAND-36. Collectively, these correlations indicate that the dependence of healthcare is to a great extent associated with poor HRQoL. Indeed, healthcare dependence before study participation, here represented by frequent hospitalizations the yr prior study inclusion, correlated significantly to poor general HRQoL as demonstrated by the PF domain of the RAND-36 (Table 6).
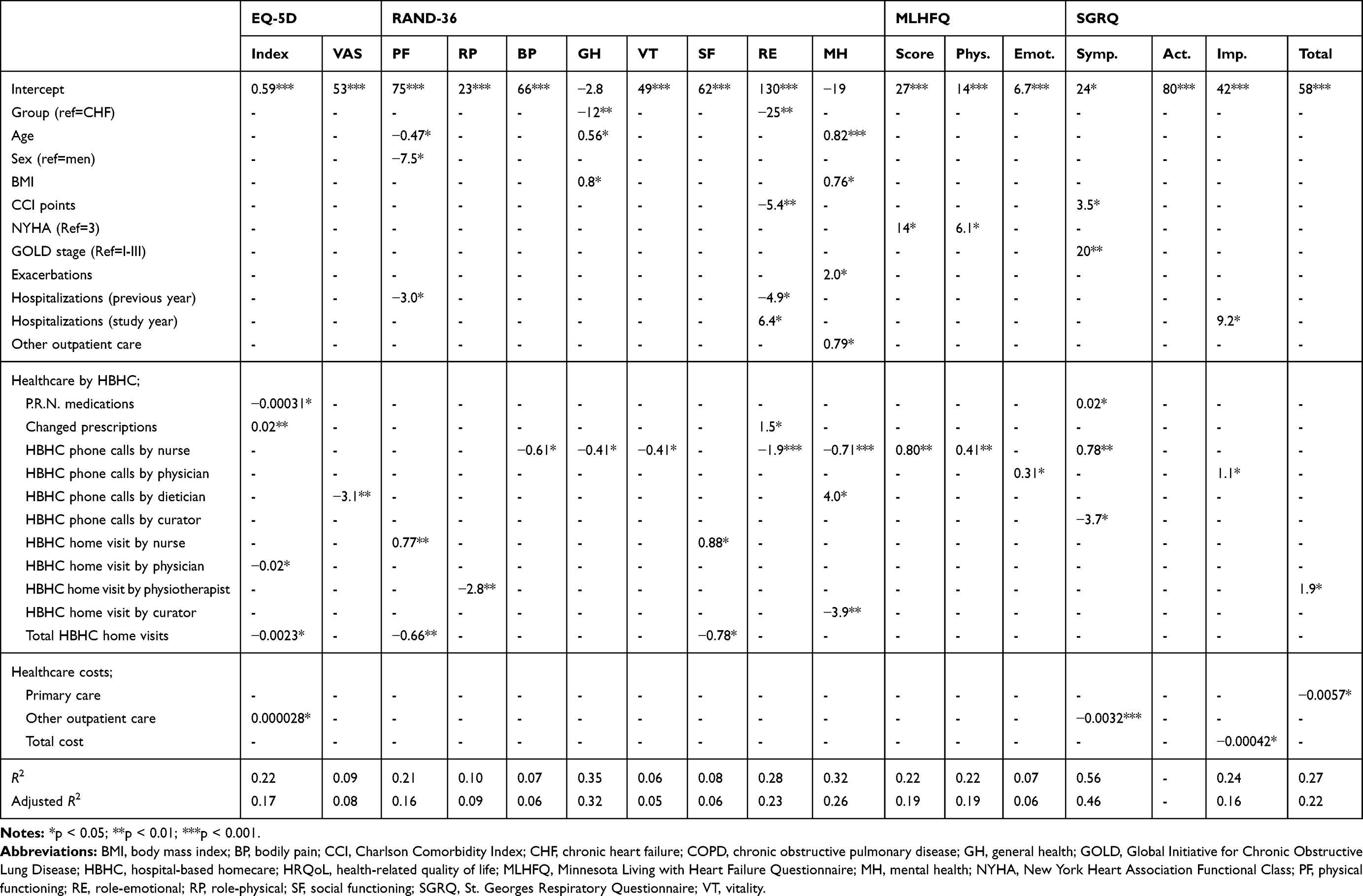 |
Table 6 Results of a Multivariable Linear Regression Analysis (Backward Elimination) |
In addition, advanced stages of CHF and COPD, reflected by the NYHA and the GOLD state, were significantly associated with poor disease-specific HRQoL, reflected by MLHFQ and SGRQ (Table 6).
Discussion
To the best of our knowledge, the present study is the first study to show that HRQoL is possible to maintain, and, indeed, even to improve by very simple telemonitoring technology; as in the present study, executed daily by subjects using a digital pen and Health Diary forms. In Sweden 2018, approximately 500,000 individuals, corresponding to approximately 5% of the total population, the majority being ≥75 yrs, never use the internet.29 Barriers to telecommunication technologies may be impaired functioning of sensory and motor organs due to high age in many cases,30,31 but the most common reasons given are “no interest” and “complicated technology”.29,32 Considering this, it becomes crucial to use telemonitoring technologies suitable to this group of elderly, multimorbid patients.
Present knowledge, summarized in a review by Gregersen et al from 2016, suggests that the positive effect of telehealth interventions on HRQoL in COPD subjects is limited.33 This is in contrast to an earlier review by Kamei et al, which concluded that telehealth intervention improved HRQoL in severe and very severe COPD patients receiving the intervention for more than 6 months.34 Very recently a study by Talboom-Kamp et al analyzed the impact of usage of a COPD self-management Web-based platform on disease-specific HRQoL of COPD subjects.35 The authors concluded that subscales of the clinical COPD questionnaire (CCQ), reflecting the mental state and the symptoms, improved significantly before and after the introduction of the program.35 In contrast, a large Danish 12-month study published 2017 found no statistical HRQoL differences among COPD subjects randomized to the telemonitoring group, compared to the control group offered conventional healthcare.15 In this study, the SF-36-Item Health Survey, Version 2, was used to assess general HRQoL.15 Moreover, an RCT by Rixon et al found no reductions in COPD patients’ HRQoL in the longer term by a telehealth intervention, observed through disease-specific measures.36 In a recent paper by Tupper et al, a 6-month telehealth intervention significantly improved HRQoL, assessed by a health-related QoL questionnaire (15D©) and the COPD Assessment Test (CAT), compared to the control group.37 Notably, subjects included presented with advanced COPD; indeed, 86% of the subjects were stage 3 or 4 and the subjects were considered at high risk of exacerbations.37
Likewise, the possible positive impact of telehealthcare on HRQoL measures of CHF subjects should be cautiously interpreted as well, due to inconsistent findings as shown by two systematic reviews.38,39 However, due to a larger amount of studies, there is much more evidence on the effect on HRQoL of telehealthcare to patients with CHF than for COPD. In a recently published Danish RCT, the mental component of SF-36, used to evaluate general HRQoL, was significantly improved in the telehealth intervention group compared to the control group.14 The telehealth intervention focused on self-empowerment achieved by engaging the patients in their own illness through self-monitoring.14 Notably, patients were excluded if they lacked a landline phone, a mobile phone or GSM (Global System for Mobile communications) coverage.14 The disease-specific questionnaire employed, the KCCQ12 score, did not demonstrate any significant change due to intervention nor did the physical component of SF-36.14 The CHF subjects addressed in this study displayed median NYHA score 2.14 Thus, these CHF subjects were much less ill compared to the CHF subjects included in the present study. Notably, a recent paper by Nouryan et al report significant beneficial effects on CHF subjects, NYHA 1–2, by a telehealth intervention (weekly video-televisits with daily vital sign monitoring) on all-cause emergency department utilization, length of stay and HRQoL, assessed by MLHFQ, compared to comprehensive outpatient management (weekly contacts by telephone).40
Few previous studies have made a longitudinal telemonitoring comparison of general and disease-specific HRQoL among both CHF and COPD subjects as in the present study. In a recent paper by Bernocchi et al the authors evaluated the effects of a combination of medical/nursing telesurveillance and telerehabilitation on disease-specific HRQoL.41 Disease-specific HRQoL were assessed among CHF subjects by MLHFQ and among COPD subjects by the CAT.41 Following a 4-month intervention, not only physical parameters but also the disease-specific HRQoL were improved in the telehealth intervention group compared to the control group.41 Unlike the present study, the study by Bernocchi et al was an RCT and the telemonitoring applied was used for surveillance as well as home training purpose.41 Study subjects were elderly and multimorbid, but stages of CHF and COPD were less advanced; thus, compared to the present study, subjects were better suited for physical training at home.41 Clearly, as demonstrated in the present study, improvement of general HRQoL among much sicker subjects than those in the study by Bernocchi et al is possible to achieve by telesurveillance only. This is because of the possibility offered by telesurveillance, to start treatment of exacerbations early, as previously reported by us.18 In contrast to the present study, a telehealth intervention (the Whole Systems Demonstrator telehealth trial), executed by the general practice, did not improve HRQoL, assessed by SF-12 and EQ-5D, for patients with COPD, diabetes, or CHF compared to usual healthcare over 12 months.42
Whether a telehealth intervention turns out beneficial on the HRQoL of the included subjects or not very much depends on the study settings applied and the subjects chosen to study. It might be that CHF subjects benefit more by telehealth interventions than COPD subjects do, and, it might be that subjects presenting with more advanced stages of these diseases exhibit greater benefit than subjects with less advanced diseases do. In this context, the telemonitoring study by Gellis et at is particularly interesting.43 The inclusion criteria and the outcomes of intervention were very much like the present study.43 Similar to the present study, homebound medically ill older adults diagnosed with CHF or COPD were randomized to either a multifaceted telehealth intervention for 12 months, but a parallel group offered usual care was also studied.43 CHF subjects dominated over COPD subjects with an inclusion ratio of 3–4:1;43 the corresponding ratio for the present study was 1.6:1. At follow-up, employing the questionnaire SF-36, the telehealth intervention group reported significantly greater improvement on GH and SF; findings in line with the present study.43 Gellis et al used the Honeywell “HomMed” Health Monitoring System, which consisted of a small, tabletop in-home monitor and a Central Station located at the home healthcare agency.43 Notably, among excluded patients were those who were unable to learn how to use the “HomMed” telehealth device.43 Importantly, in the present study, we did not have to exclude any patients due to difficulties in handling the digital pen and Health Diary forms.
To the best of our knowledge, there is no previous study that evaluates, in a telehealth context, the association between healthcare dependence and HRQoL as extensively as the present study does. In a non-telehealth context, Janssen et al have presented data on subjects with advanced CHF and COPD.3 In that study, the results of baseline measures of general HRQoL were very similar to the data presented in the present study (Table 2).3 Indeed, as in the present study, only the GH domain of the RAND-36 demonstrated significant difference when CHF and COPD subjects were compared.3 To assess healthcare dependence, Janssen et al used the instrument The Care Dependency Scale (CDS), a questionnaire consisting of 15 items regarding basic and instrumental activities of daily living, such as personal care, household activities, social and recreational activities.3 Multiple regression analyses in that study showed that CDS and the number of drugs were correlated with impaired HRQoL in advanced COPD or CHF, while disease severity was not correlated.3 In contrast, due to a thorough analysis of healthcare consumption and costs, the present study is for the first time, in a telehealth context, able to show that poor HRQoL – general as well as disease-specific – in addition to disease severity, is associated with a variety of important healthcare dependence measures presented in Tables 5 and 6. It should be pointed though that many of the correlations of measures of healthcare dependency and HRQoL variables were rather weak.
We have previously reported on the beneficial effects of the eHealth Diary study on hospitalization frequency.18 Indeed, for both CHF and COPD subjects, numbers of hospitalizations and associated costs were significantly reduced compared to the yr prior study participation.18,19 In addition, the present study also reports significant improvement in general HRQoL. Among previous studies with the aim to reduce the number of hospitalizations as well as to improve HRQoL, the study by Ong et al deserves special attention.44 In that study, approximately 1400 CHF subjects were randomized to usual care or a telemonitoring intervention. Unlike the eHealth Diary study,18 no significant difference was observed regarding number of hospitalizations during a follow-up of 180 days, while, similar to our study, significant improvement of HRQoL was reported.44 Furthermore, we have previously reported differences between CHF and COPD subjects observed in the eHealth Diary study.18,19 In addition to much more frequent exacerbations among COPD subjects and healthcare costs, we here report significantly more serious alarms created by this group of subjects.
The present study has limitations. Major limitations are a small sample size, due to a considerable loss of enrolled patients, and a lack of a control group. Although significant, the effects of intervention found on measures of healthcare dependency and HRQoL variables were rather weak. Moreover, we did not conduct a further post-study analysis of HRQoL to determine whether the improvements were maintained after the telemonitoring period ceased.
Conclusion
The Health Diary system and HBHC together improve general HRQoL of elderly multimorbid subjects with CHF and/or COPD, and measures of healthcare dependency are associated with HRQoL variables. The simplicity of the technology applied makes this telemonitoring system very suitable for computer-illiterate subjects. As the subjects in the present study were very ill, it is very favorable that the healthcare providers responsible for monitoring and, if needed, medical actions undertaken at home, have characteristics like the HBHC unit in the present study. In future studies, we will adopt the same telemonitoring system using the primary healthcare as a responsible healthcare giver.
Abbreviations
BMI, body mass index; BP, bodily pain; CAT, COPD Assessment Test; CCI, Charlson Comorbidity Index; CCQ, clinical COPD questionnaire; CDS, Care Dependency Scale; CDW, Care Data Warehouse in Östergötland; CHF, chronic heart failure; COPD, chronic obstructive pulmonary disease; CCP, Cost Per Patient database; EQ-5D, EuroQol-5 Dimensions; FEV1(% of predicted), forced expiratory volume in one second expressed as % of predicted; GEE, Generalized Estimating Equations (GEE); GH, general health; GOLD, global initiative for chronic obstructive lung disease; GSM, Global System for Mobile communications; HBHC, specialized hospital-based home care; HRQoL, health-related quality of life; ICH-GCP, International Conference on Harmonization of Good Clinical Practice; KCCQ, Kansas City Cardiomyopathy Questionnaire; LTOT, long-term oxygen therapy; MH, mental health; MCID, minimal clinically important difference; MLHFQ, Minnesota Living with Heart Failure Questionnaire; NYHA, New York Heart Association; PF, physical functioning; P.R.N., pro re nata (as needed); RCT, randomized control study; RE, role-emotional; RP, role-physical; SAT, blood oxygen saturation; SF, social functioning; SF-36, Short Form-36; SMS, Short Message Service; SGRQ, St. Georges Respiratory Questionnaire; VAS, Visual Analogue Scale; VT, vitality; yrs, years.
Data Sharing Statement
The data upon which this analysis was based are available from the corresponding author in anonymized form, upon receipt of a reasonable request.
Acknowledgments
The authors thank all the patients in this study for their committed participation in this research and all the health professionals at the Unit of Specialized HBHC for dedicated healthcare. In particular, the authors would like to thank Dr. G. Carlgren, Dr. J. Mudra and R.N. H. Synnergren (study nurse) for collecting most of the data. This work was supported by grants from the county council of Östergötland (Region Östergötland), E-care@home: a “SIDUS – Strong Distributed Research Environment” project, funded by the Swedish Knowledge Foundation, the European Regional Development Fund through the NovaMedTech venture, and RISE Research Institutes of Sweden AB. This study was performed at the Unit of Specialized HBHC, Linköping University Hospital, Sweden.
Author Contributions
H.L.P. and L.L. designed and led the study, collected and analyzed data, and wrote the manuscript. J.L. collected and analyzed data and wrote the manuscript. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors have no financial or non-financial conflicts to disclose in relation to the present study.
References
1. Global initiative for chronic obstructive lung disease: global strategy for the diagnoses, management and prevention of chronic obstructive pulmonary disease, 2018 report. Available from: https://goldcopd.org/wp-content/uploads/2018/02/WMS-GOLD-2018-Feb-Final-to-print-v2.pdf.
2. Ponikowski P, Voors AA, Anker SD, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;2016(18):891–975. doi:10.1002/ejhf.592
3. Janssen DJ, Spruit MA, Uszko-Lencer NH, et al. Symptoms, comorbidities, and health care in advanced chronic obstructive pulmonary disease or chronic heart failure. J Palliat Med. 2011;14:735–743. doi:10.1089/jpm.2010.0479
4. Rutten FH, Cramer M-JM, Grobbee DE, et al. Unrecognized heart failure in elderly patients with stable chronic obstructive pulmonary disease. Eur Heart J. 2005;26:1887–1894. doi:10.1093/eurheartj/ehi291
5. Blinderman CD, Homel P, Billings JA, et al. Symptom distress and quality of life in patients with advanced congestive heart failure. J Pain Symptom Manage. 2008;35:594–603. doi:10.1016/j.jpainsymman.2007.06.007
6. Blinderman CD, Homel P, Billings JA, et al. Symptom distress and quality of life in patients with advanced chronic obstructive pulmonary disease. J Pain Symptom Manage. 2009;38:115–123. doi:10.1016/j.jpainsymman.2008.07.006
7. Iqbal J, Francis L, Reid J, et al. Quality of life in patients with chronic heart failure and their carers: a 3-year follow-up study assessing hospitalization and mortality. Eur J Heart Fail. 2010;12:1002–1008. doi:10.1093/eurjhf/hfq114
8. Habraken JM, van der Wal WM, Ter Riet G, et al. Health-related quality of life and functional status in end-stage COPD: a longitudinal study. Eur Respir J. 2011;37:280–288. doi:10.1183/09031936.00149309
9. Azevedo A, Bettencourt P, Alvelos M, et al. Health-related quality of life and stages of heart failure. Int J Cardiol. 2008;129:238–244. doi:10.1016/j.ijcard.2007.07.091
10. Hajiro T, Nishimura K, Tsukino M, et al. Stages of disease severity and factors that affect the health status of patients with chronic obstructive pulmonary disease. Respir Med. 2000;94:841–846. doi:10.1053/rmed.2000.0804
11. Janssen DJ, Franssen FM, Wouters EF, et al. Impaired health status and care dependency in patients with advanced COPD or chronic heart failure. Qual Life Res. 2011;20:1679–1688. doi:10.1007/s11136-011-9892-9
12. Jayaram NM, Khariton Y, Krumholz HM, et al. Impact of telemonitoring on health status. Circ Cardiovasc Qual Outcomes. 2017;10:e004148. doi:10.1161/CIRCOUTCOMES.117.004148
13. Knox L, Rahman RJ, Beedie C. Quality of life in patients receiving telemedicine enhanced chronic heart failure disease management: a meta-analysis. J Telemed Telecare. 2017;23:639–649. doi:10.1177/1357633X16660418
14. Cichosz SL, Udsen FW, Hejlesen O. The impact of telehealth care on health-related quality of life of patients with heart failure: results from the Danish TeleCare North heart failure trial. J Telemed Telecare. 2019;1357633X19832713. doi:10.1177/1357633X19832713
15. Lilholt PH, Witt Udsen F, Ehlers L, et al. Telehealthcare for patients suffering from chronic obstructive pulmonary disease: effects on health-related quality of life: results from the Danish ‘TeleCare North’ cluster-randomised trial. BMJ Open. 2017;7:e014587. doi:10.1136/bmjopen-2016-014587
16. McLean S, Nurmatov U, Liu JL, et al. Telehealthcare for chronic obstructive pulmonary disease: cochrane review and meta-analysis. Br J Gen Pract. 2012;62:e739–e749. doi:10.3399/bjgp12X658269
17. Cruz J, Brooks D, Marques A. Home telemonitoring effectiveness in COPD: a systematic review. Int J Clin Pract. 2014;68:369–378. doi:10.1111/ijcp.12345
18. Persson HL, Lyth J, Wiréhn A-B, et al. <p>Elderly patients with COPD require more health care than elderly heart failure patients do in a hospital-based home care setting. Int J Chron Obstruct Pulmon Dis. 2019;14:1569–1581. doi:10.2147/COPD.S207621
19. Lyth J, Lind L, Persson HL, et al. Can a telemonitoring system lead to decreased hospitalization in elderly patients? J Telemed Telecare. 2019:1357633X19858178. doi:10.1177/1357633X19858178
20. Dolan P. Modeling valuations for EuroQol health states. Med Care. 1997;35:1095–1108. doi:10.1097/00005650-199711000-00002
21. Hays RD, Sherbourne CD, Mazel RM. The RAND 36-item health survey 1.0. Health Econ. 1993;2:217–227. doi:10.1002/(ISSN)1099-1050
22. Hays RD, Morales LS. The RAND-36 measure of health-related quality of life. Ann Med. 2001;33:350–357. doi:10.3109/07853890109002089
23. Jones PW, Quirk FH, Baveystock CM, et al. A self-complete measure of health status for chronic airflow limitation. The St. George’s respiratory questionnaire. Am Rev Respir Dis. 1992;145:1321–1327. doi:10.1164/ajrccm/145.6.1321
24. Riegel B, Moser DK, Glaser D, et al. The Minnesota living with heart failure questionnaire: sensitivity to differences and responsiveness to intervention intensity in a clinical population. Nurs Res. 2002;51:209–218. doi:10.1097/00006199-200207000-00001
25. Zanini A, Aiello M, Adamo D, et al. Estimation of minimal clinically important difference in EQ-5D visual analog scale score after pulmonary rehabilitation in subjects with COPD. Respir Care. 2015;60:88–95. doi:10.4187/respcare.03272
26. Samsa G, Edelman D, Rothman ML, et al. Determining clinically important differences in health status measures: a general approach with illustration to the health utilities index mark II. Pharmacoeconomics. 1999;15:141–155. doi:10.2165/00019053-199915020-00003
27. Gonzalez-saenz de Tejada M, Bilbao A, Ansola L, et al. Responsiveness and minimal clinically important difference of the Minnesota living with heart failure questionnaire. Health Qual Life Outcomes. 2019;17:36. doi:10.1186/s12955-019-1104-2
28. Jones PW. Interpreting thresholds for a clinically significant change in health status in asthma and COPD. Eur Respir J. 2002;19:398–404. doi:10.1183/09031936.02.00063702
29. Svenskarna och internet 2018. Report from Internetstiftelsen in Sweden (IIS); 2018. Available from: https://www.iis.se/docs/Svenskarna_och_internet_2018.pdf.
30. Hanson VL. Technology skill and age: what will be the same 20 years from now? Univ Access Inf Soc. 2011;10:443–452. doi:10.1007/s10209-011-0224-1
31. Foster MV, Sethares KA. Facilitators and barriers to the adoption of telehealth in older adults: an integrative review. Comput Inform Nurs. 2014;32:
32. Wildenbos GA, Peute L, Jaspers M. Aging barriers influencing mobile health usability for older adults: a literature based framework (MOLD-US). Int J Med Inform. 2018;114:66–75. doi:10.1016/j.ijmedinf.2018.03.012
33. Gregersen TL, Green A, Frausing E, et al. Do telemedical interventions improve quality of life in patients with COPD? A systematic review. Int J Chron Obstruct Pulmon Dis. 2016;11:809–822. doi:10.2147/COPD.S96079
34. Kamei T, Yamamoto Y, Kajii F, et al. Systematic review and meta-analysis of studies involving telehome monitoring-based telenursing for patients with chronic obstructive pulmonary disease. Jpn J Nurs Sci. 2013;10:180–192. doi:10.1111/j.1742-7924.2012.00228.x
35. Talboom-Kamp EPWA, Holstege MS, Chavannes NH, et al. Effects of use of an eHealth platform e-Vita for COPD patients on disease specific quality of life domains. Respir Res. 2019;20:146. doi:10.1186/s12931-019-1110-2
36. Rixon L, Hirani SP, Cartwright M, et al. A RCT of telehealth for COPD patient’s quality of life: the whole system demonstrator evaluation. Clin Respir J. 2017;11:459–469. doi:10.1111/crj.12359
37. Tupper OD, Gregersen TL, Ringbaek T, et al. Effect of tele-health care on quality of life in patients with severe COPD: a randomized clinical trial. Int J Chron Obstruct Pulmon Dis. 2018;13:2657–2662. doi:10.2147/COPD.S164121
38. Schmidt S, Schuchert A, Krieg T, et al. Home telemonitoring in patients with chronic heart failure: a chance to improve patient care? Dtsch Arztebl Int. 2010;107:131–138. doi:10.3238/arztebl.2010.0131
39. Cajita MI, Gleason KT, Han HR. A systematic review of mHealth-based heart failure interventions. J Cardiovasc Nurs. 2016;31:E10–22. doi:10.1097/JCN.0000000000000305
40. Nouryan CN, Morahan S, Pecinka K, et al. Home telemonitoring of community-dwelling heart failure patients after home care discharge. Telemed J E Health. 2019;25:447–454. doi:10.1089/tmj.2018.0099
41. Bernocchi P, Vitacca M, La Rovere MT, et al. Home-based telerehabilitation in older patients with chronic obstructive pulmonary disease and heart failure: a randomised controlled trial. Age Ageing. 2018;47:82–88. doi:10.1093/ageing/afx146
42. Cartwright M, Hirani SP, Rixon L, et al. Whole systems demonstrator evaluation team. Effect of telehealth on quality of life and psychological outcomes over 12 months (whole systems demonstrator telehealth questionnaire study): nested study of patient reported outcomes in a pragmatic, cluster randomised controlled trial. BMJ. 2013;346:f653. doi:10.1136/bmj.f653
43. Gellis ZD, Kenaley B, McGinty J, et al. Outcomes of a telehealth intervention for homebound older adults with heart or chronic respiratory failure: a randomized controlled trial. The Gerontologist. 2012;52:541–552. doi:10.1093/geront/gnr134
44. Ong MK, Romano PS, Edgington S, et al. Effectiveness of remote patient monitoring after discharge of hospitalized patients with heart failure: the better effectiveness after transition – heart failure (BEAT-HF) randomized clinical trial. JAMA Intern Med. 2016;176:310–318. doi:10.1001/jamainternmed.2015.7712
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.