")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
The Feasibility of TACE Combined with TKIs Plus PD-1 Antibody for Advanced HCC
Authors Sun T , Ren Y, Sun B, Chen L , Zhu L, Zhang L , Zheng C
Received 17 December 2022
Accepted for publication 23 February 2023
Published 16 March 2023 Volume 2023:10 Pages 447—457
DOI https://doi.org/10.2147/JHC.S400948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmed Kaseb
Tao Sun,1,2,* Yanqiao Ren,1,2,* Bo Sun,1,2,* Lei Chen,1,2 Licheng Zhu,1,2 Lijie Zhang,1– 3 Chuansheng Zheng1,2
1Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 2Hubei Province Key Laboratory of Molecular Imaging, Wuhan, Hubei, People’s Republic of China; 3Department of Interventional Radiology, The Fifth Medical Center of Chinese, PLA General Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chuansheng Zheng, Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China, Tel +86-13329702158, Email [email protected] Lijie Zhang, Department of Interventional Radiology, The Fifth Medical Center of Chinese, PLA General Hospital, Beijing, People’s Republic of China, Email [email protected]
Objective: To evaluate the efficacy and safety of transarterial chemoembolization (TACE) combined with tyrosine kinase inhibitors (TKIs: sorafenib, lenvatinib, and apatinib) plus camrelizumab (TACE-TKIs-C) vs TACE combined with TKIs (TACE-TKIs) for advanced hepatocellular carcinoma (HCC).
Methods: In this two-center retrospective study, patients with advanced HCC treated with TACE-TKIs-C or TACE-TKIs were enrolled between January 1, 2018, to October 1, 2020. A total of 260 eligible patients received TACE-TKIs-C (N=70) or TACE-TKIs (N=190). The differences in overall survival (OS), progression-free survival (PFS) and tumor response were compared between two groups. Propensity score matching (PSM) analysis was applied to reduce patient selection bias. The risk factors affecting OS or PFS were analyzed.
Results: Fifty-three pairs of patients were matched after PSM analysis. Before PSM analysis, the median OS and PFS of TACE-TKIs-C were significantly longer than those of the TACE-TKIs (OS: not reached vs 12.0 months, P< 0.0001; PFS: 10.0 months vs 6.0 months, P< 0.0001). After PSM analysis, the median OS and PFS of TACE-TKIs-C were significantly longer than those of the TACE-TKIs (OS: Not reached vs 13.0 months, P< 0.0001; PFS: 9.0 months vs 6.0 months, P< 0.0001); the uni- and multivariate analysis revealed that TACE-TKIs-C treatment was a protective factor of OS and PFS. Grade 3 or 4 hypertension occurred in 14.3% of patients in the TACE-TKIs-C group and other high-grade toxic effects were infrequent.
Conclusion: In patients with advanced HCC, TACE-TKIs-C may improve overall and progression-free survival outcomes over TACE-TKIs with manageable safety profile.
Keywords: hepatocellular carcinoma, transarterial chemoembolization, tyrosine kinase inhibitors, camrelizumab, propensity score matching
Introduction
Hepatocellular carcinoma (HCC) is the leading cause of cancer-related death worldwide with high morbidity.1 Despite advances in treatments such as resection, liver transplantation, ablation, tyrosine kinase inhibitors (TKIs), or immunotherapy, the prognosis of most HCC patients remains poor.2
The multikinase inhibitors sorafenib and lenvatinib are recommended as the first-line treatment of advanced HCC but with modest efficacy.3 In this setting, transarterial chemoembolization (TACE) is recommended to provide local disease control for advanced HCC with preserved liver function and exhibited encouraging survival outcomes.4,5 Due to upregulation of vascular endothelial growth factor (VEGF) concentration in residual tumor, the combination of TACE with antiangiogenic therapy, like sorafenib, lenvatinib, and apatinib may improve clinical outcomes. A randomised, multicenter prospective trial (RCT) by Kudo et al reported that this combination improved progression-free survival (PFS) significantly.6 However, other RCTs focusing on the combination of TACE with TKIs, such as sorafenib, brivanib, and olantinib, failed to improve clinical outcomes compared with TACE alone.7–9
In addition to TKIs, TACE has also shown the potential to combine with immunotherapy. As a locoregional therapy, TACE was expected to release neoantigens, which could enhance immunotherapy by activating relevant immune system.10 According to Phase I/II clinical trials (CheckMate040, KEYNOTE-224), immune checkpoint inhibitors (ICIs) targeting programmed death 1 (PD-1) have shown significant clinical activity as second-line treatment for hepatocellular carcinoma.10–12 However, in Phase III studies of single-agent treatment, nivolumab and pembrolizumab failed to improve overall survival significantly.13,14 To improve the efficacy of immunotherapy, combination immunotherapy has become an urgent need in HCC therapy research. Combination strategies include two types of immune checkpoint inhibitors (anti-PD-1/PD-L1 and anti-CTLA-4 antibodies), anti-PD-1/PD-L1 antibody with TKIs, and anti-PD-1/PD-L1 or -CTLA-4 antibody with locoregional therapies.10 Among these, the combination of ICIs with TKIs reached a remarkable outcome which has been recognized as first-line treatment by the National Comprehensive Cancer Network (NCCN) based on IMbrave150.15
The hypoxia response induced by TACE could not only upregulate VEGF but also stimulate system immune, which indicates that TACE, ICIs and TKIs may have the potential to combined with each other. It is reported that TACE+ICIs+Sorafenib is better than TACE-Sorafenib in the treatment of advanced TACE-refractory HCC.12 Therefore, it is valuable to study whether ICIs+TKIs are beneficial compared with TKIs in TACE-initial HCC.
Sorafenib, lenvatinib, and apatinib are the most commonly used TKIs in China and have been approved for first-line or second-line treatment of advanced HCC in China. Camrelizumab, an anti-PD-1 monoclonal antibody with high affinity to PD-1 and a different binding epitope from nivolumab and pembrolizumab, was recently approved in China as a second-line treatment for advanced HCC. During the past three years, a subset of HCC patients undergoing TACE were treated with sorafenib, lenvatinib, or apatinib monotherapy or combination of sorafenib, lenvatinib, or apatinib with camrelizumab. Therefore, we conducted this comparative study to elevate the efficacy and side effects of TACE combined with TKIs (sorafenib, lenvatinib, or apatinib) + camrelizumab in the treatment of advanced HCC.
Materials and Methods
Study Design and Participants
From January 1, 2018, to October 1, 2020, consecutive HCC patients treated with TACE at our centers were reviewed. Among these patients, those who received camrelizumab in combination with sorafenib, lenvatinib, or apatinib were assigned to the TACE-TKIs-C arm. The patients who treated with sorafenib, lenvatinib or apatinib were classified into TACE-TKIs arm. All patients were pathologically or clinically diagnosed with HCC based on the standard of AASLD. This retrospective study has been approved by ethics committee of Union Hospital, Tongji Medical college, Huazhong University of Science and Technology (UHCT-IEC-SOP-016-03-01). Nonidentified information was used to protect patient confidentiality. The data in this article are anonymous, and the requirement for informed consent was therefore waived.
Inclusion criteria included (A) age of 18 years or older; (B) radiological diagnosed with advanced HCC; (C) Child-Pugh class A, B; (D) measurable tumor lesions on computed tomography (CT) or magnetic resonance imaging (MRI); (E) Eastern Cooperative Oncology Group performance score (ECOG PS) of 0 or 1.
Exclusion criteria included: (A) metastatic liver malignant; (B) Child-Pugh class C; (C) portal vein invasion with Vp4;19 (D) any contraindication for therapy with TACE.
TACE Procedure
All patients in both groups received TACE once at least. TACE was conducted by specialists with 10 years` experiences. Under the guidance of digital subtraction angiography (DSA), a 5-F catheter (Cook, Bloomington, Indiana, USA) was placed into the hepatic artery and a 2.7-F microcatheter (Progreat, Terumo, Tokyo, Japan) was inserted selectively into tumor feeding arteries. About 2–20 mL lipiodol and 20–60 mg epirubicin were prepared to make emulsion. Then, the emulsion was administrated into the tumor feeding arteries through the microcatheter. Gelatin sponge particles (350–710 μm, Alicon, Hangzhou, China) were used to embolize completely the tumor feeding arteries. Finally, hepatic artery angiography was performed to validate the complete embolism of the feeding arteries. If the residual lesions were confirmed by enhanced CT, the repeated TACE would be recommended.
Camrelizumab and TKIs Administration
Camrelizumab and TKIs were administrated within seven days after TACE therapy. Camrelizumab was recommended at a dose of 200mg every 3 weeks and administrated intravenously. If patients developed serve adverse events (AEs), camrelizumab was interrupted or discontinued and symptomatic treatment such as glucocorticoids or immune-suppressant agents were administered, depending on the severity and the affected organs. Sorafenib was orally administrated at a dose of 400mg twice a day. Lenvatinib was recommended at a dose of 12 mg (≥60 kg) or 8 mg (<60 kg) once daily based on body weight. Apatinib was orally administered at a dose of 200 mg once daily for 28 days as a treatment cycle. When the tolerable AEs grade 1–2 occurred, the TKIs administration were continued. Once serve AEs occur, TKIs administration were discontinued according to drug directions.
Follow Up and Assessment
The first follow-up was conducted within 6 weeks after TACE procedure, and the next clinical follow-up was recommended every 2 or 3 months. The tumor response was evaluated by contrasted MRI or CT according to the mRECIST. The coprimary end points included overall survival (OS, defined as the time from first TACE procedure to death from any cause) and progression-free survival (PFS, defined as the time from first TACE procedure to disease progression according to mRECIST). Secondary endpoints were disease control rate (DCR, the percentage of patients with a complete or partial response, or stable disease) and objective response rate (ORR, the percentage of patients with a complete or partial response). The incidence and severity of AEs were recorded and assessed using vital signs and clinical laboratory test results according to the General Adverse Event Terminology Criteria Version 5.0.
Propensity Score Matching (PSM) Analysis
PSM analysis was conducted to reduce bias in patient selection to compare the difference between the TACE-TKIs-C group and TACE-TKIs group. The variables showing significant differences or associations with patient selection, including ECOG performance, ALT, PT, tumor size, tumor number, TKIs type, were matched in our model. One-to-one matching without replacement was applied, and the value of the caliper was 0.05.
Statistical Analysis
The statistical analyses were performed using the SPSS 24.0 software (IBM, Armonk, NY, USA). Continuous variables are presented as the mean ± standard deviation (SD) and calculated using the student’s t-test. Categorical variables are reported by frequency with percentages and calculated using Chi-squared test. The survival curve of OS and PFS was analyzed using Kaplan–Meier analysis and log rank test. Variables with the value of P < 0.10 at univariate analysis were entered into multi-univariate Cox proportional hazards regression model analysis, which was used to identify risk factors affecting OS and PFS. P-value <0.05 (two-tailed) was considered statistically significant.
Results
Baseline Characteristics of the Study Population
From January 1, 2018, to October 1, 2020, a total of 260 patients (70 TACE-TKIs-C, 190 TACE-TKIs) were included. After PSM analysis, 53 pairs of patients were matched. The detailed baseline characteristics are listed in Table 1. The TKIs was adopted as sorafenib, lenvatinib, apatinib in 17 (24.3%), 24 (38.6%), and 26 (37.1%) patients, respectively, in the TACE-TKIs-C group, and 52 (27.3%), 52 (27.3%), and 86 (45.3%) patients, respectively, in the TACE-TKIs group. There was no significant difference in the TKIs composition between the two groups before (P=0.214) and after PSM analysis (P=0.970). Besides, the other baseline characteristics between two groups were not significantly different after PSM analysis.
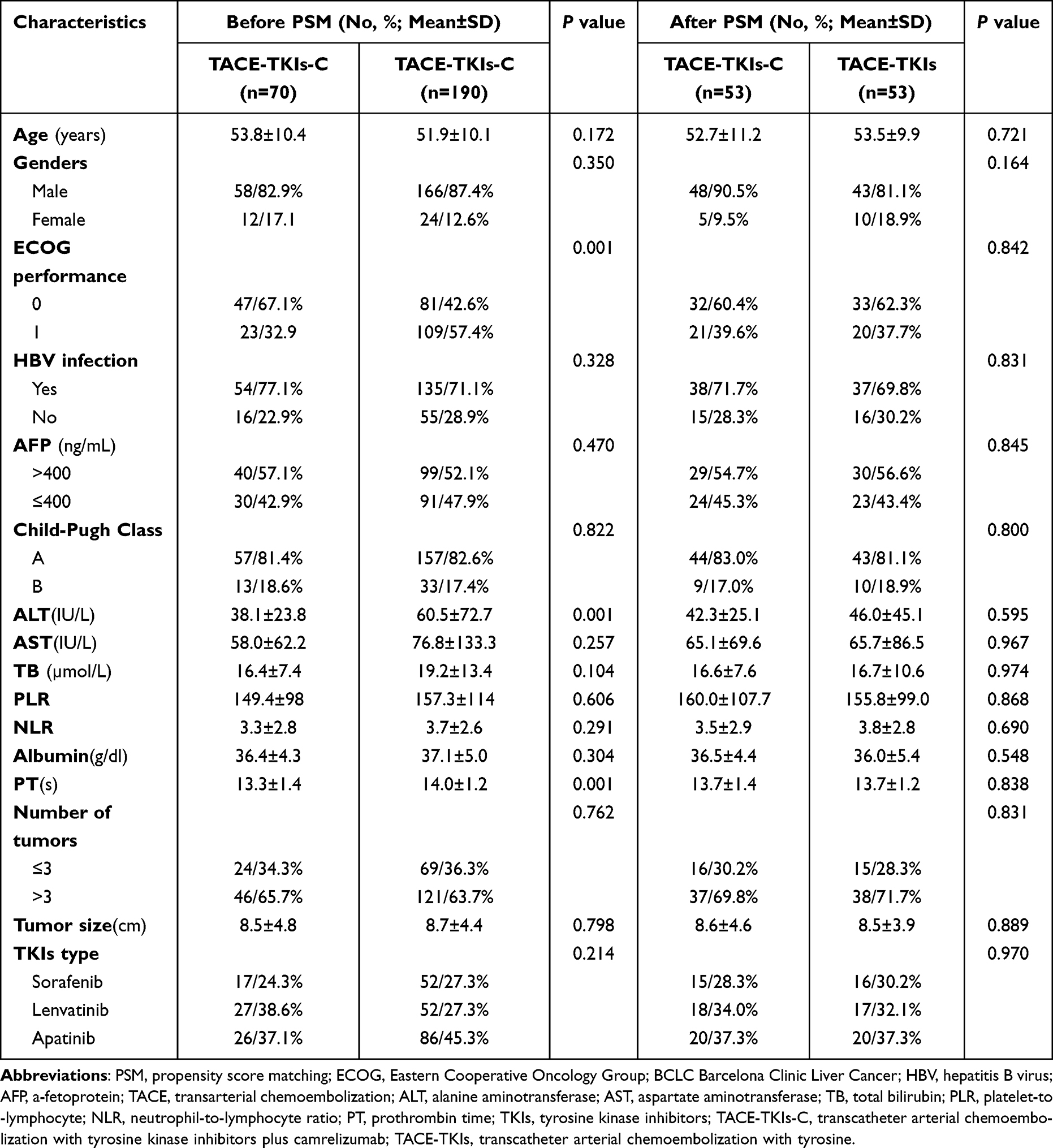 |
Table 1 Baseline Characteristics of Patients Between the Two Groups Before and After PSM Analysis |
Tumor Response Evaluation
To evaluate the tumor response, ORR and DCR were both tested (Table 2). Before PSM analysis, the ORR was significantly higher with TACE-TKIs-C group (27.1% vs 10.0%, P=0.001). After PSM analysis, the ORR of tumor response was 26.4% in the TACE-TKIs-C group, which was significantly higher than 9.4% in the group of TACE-TKIs group (P = 0.023). The confirmed DCRs were 77.1% with TACE-TKIs-C and 64.7% with TACE-TKIs (P=0.057) before PSM analysis, 73.6% with TACE-TKIs-C and 67.9% with TACE-TKIs (P=0.522) after PSM analysis, respectively.
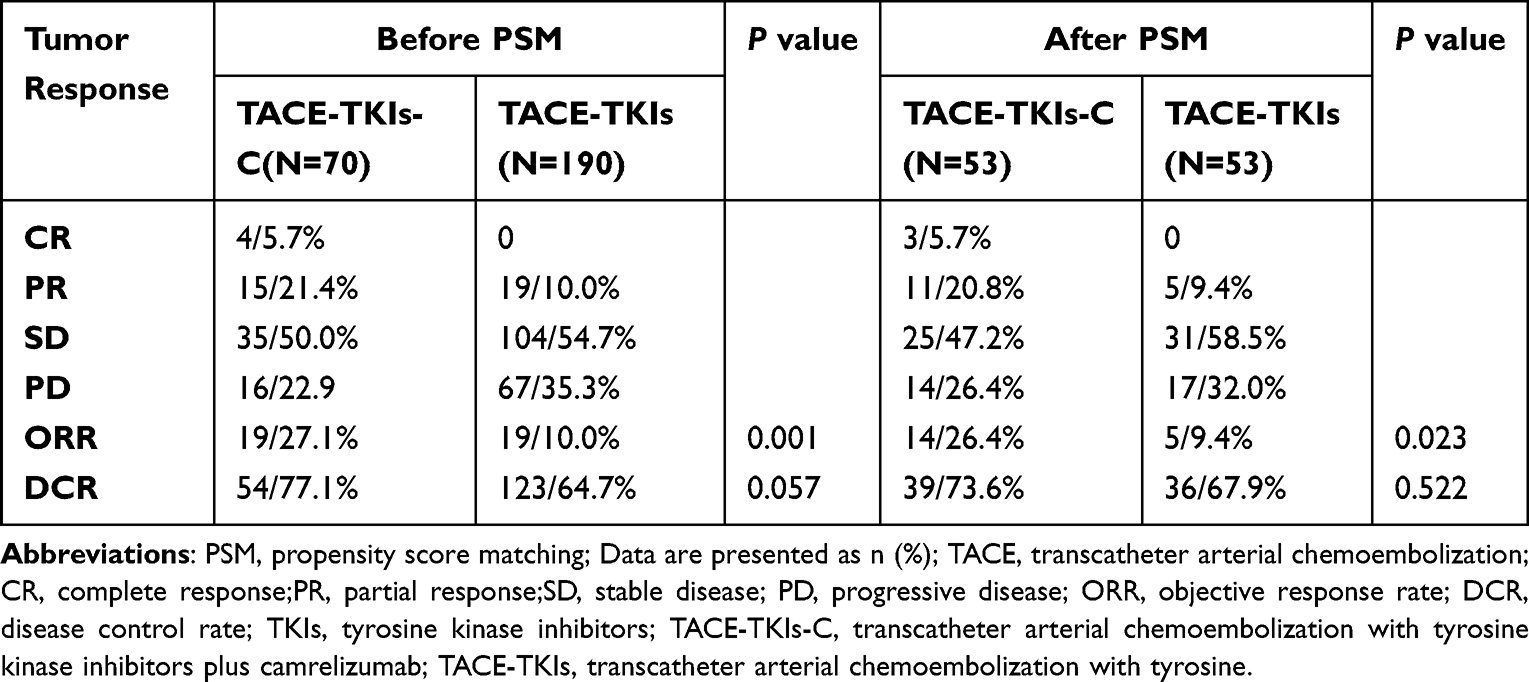 |
Table 2 Tumor Response in Both Groups |
Efficacy
The median follow-up time was 9.8 months (range, 2.0–24.0 months). At clinical cut-off date, a total of 24 patients (34.3%) in the TACE-TKIs-C group and 147 patients (77.4%) in the TACE-TKIs group had died. Before PSM analysis, the median OS of TACE-TKIs-C group was not reached and the median OS of TACE-TKIs was 12.0 months (95% CI, 11.8–14.2 months). However, OS was significantly longer with TACE-TKIs-C (P<0.0001) (Figure 1A). After PSM analysis, the median OS in the TACE-TKIs-C group was not reached and in the TACE-TKIs group were 13.0 months (95% CI, 11.3–15.9 months) respectively, and the difference between the two groups was significantly different (P<0.0001) (Figure 1C). Before PSM analysis, the median PFS was significantly longer with TACE-TKIs-C than TACE-TKIs (median, 10.0 months [95% CI, 8.9–11.0 months] vs 6.0 months [95% CI, 5.4–6.6 months], P<0.0001) (Figure 1B). After PSM analysis, the median PFS was significantly longer with TACE-TKIs-C than TACE-TKIs (median, 9.0 months [95% CI, 7.5–10.4 months] vs 5.0 months [95% CI, 4.3–5.9 months], P<0.0001) (Figure 1D).
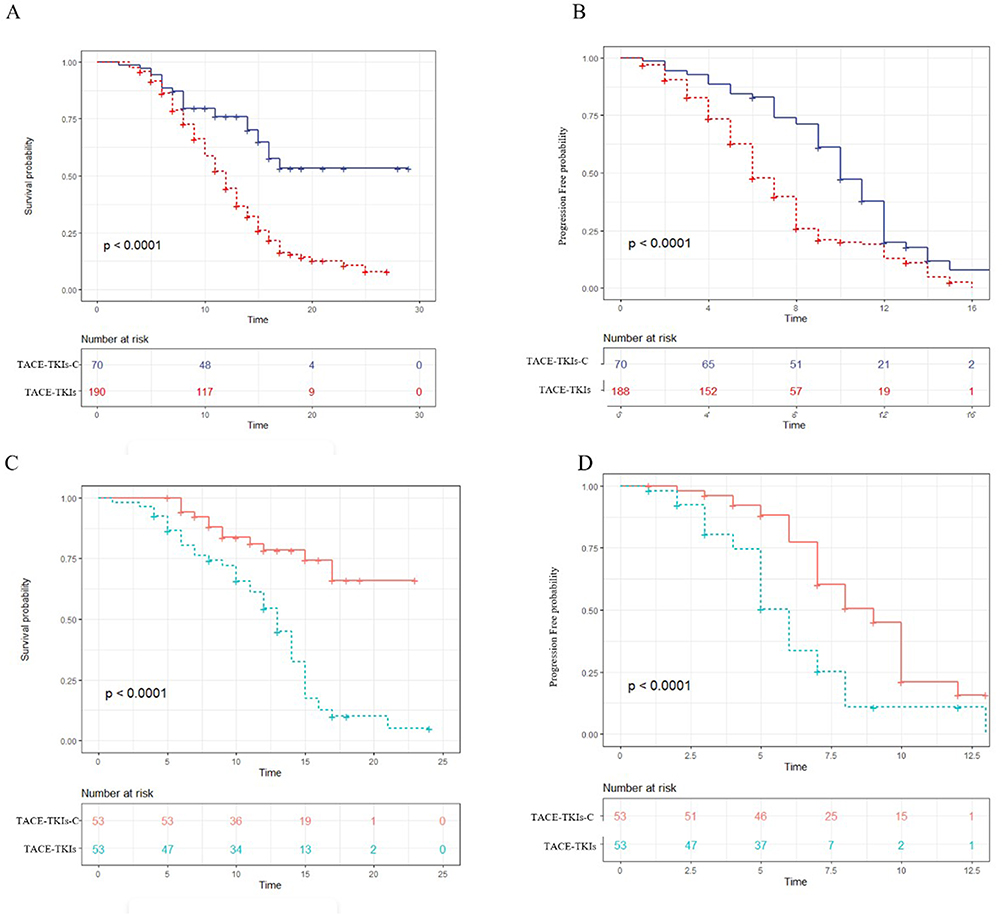 |
Figure 1 The Kaplan–Meier (KM) curves for patients with advanced hepatocellular carcinoma who received the treatment of transcatheter arterial chemoembolization with tyrosine kinase inhibitors plus camrelizumab (TACE-TKIs-C) or transcatheter arterial chemoembolization with tyrosine kinase inhibitors (TACE-TKIs): (A) the KM curves of overall survival time before PSM analysis; (B) the KM curves of time to progression before PSM analysis; (C) the KM curves of overall survival time after PSM analysis; (D) the KM curves of time to progression after PSM analysis. |
Prognostic Factors Affecting OS and PFS
Before PSM analysis, univariate analysis indicated that ECOG, number of tumors, tumor size, and treatment were significantly associated with OS. Multivariate Cox analysis showed that ECOG, number of tumors, tumor size and treatment were significantly predictive factors for OS of the patients in the two groups (HR=1.057, 95% CI, 1.020–1.096, P=0.005; HR=3.342, 95% CI: 2.033–5.495, P<0.001, respectively). Moreover, univariate analysis showed that ECOG, Tumor size, PLR, AST, and treatment were associated with PFS. Multivariate Cox analysis indicated AST, and treatment were significantly predictive factors (HR=0.537, 95% CI, 0.393–0.732, P<0.001). After PSM analysis, multivariate Cox analysis confirmed that TACE-TKIs-C was the protective factor of OS and PFS (Table 3 and Table 4).
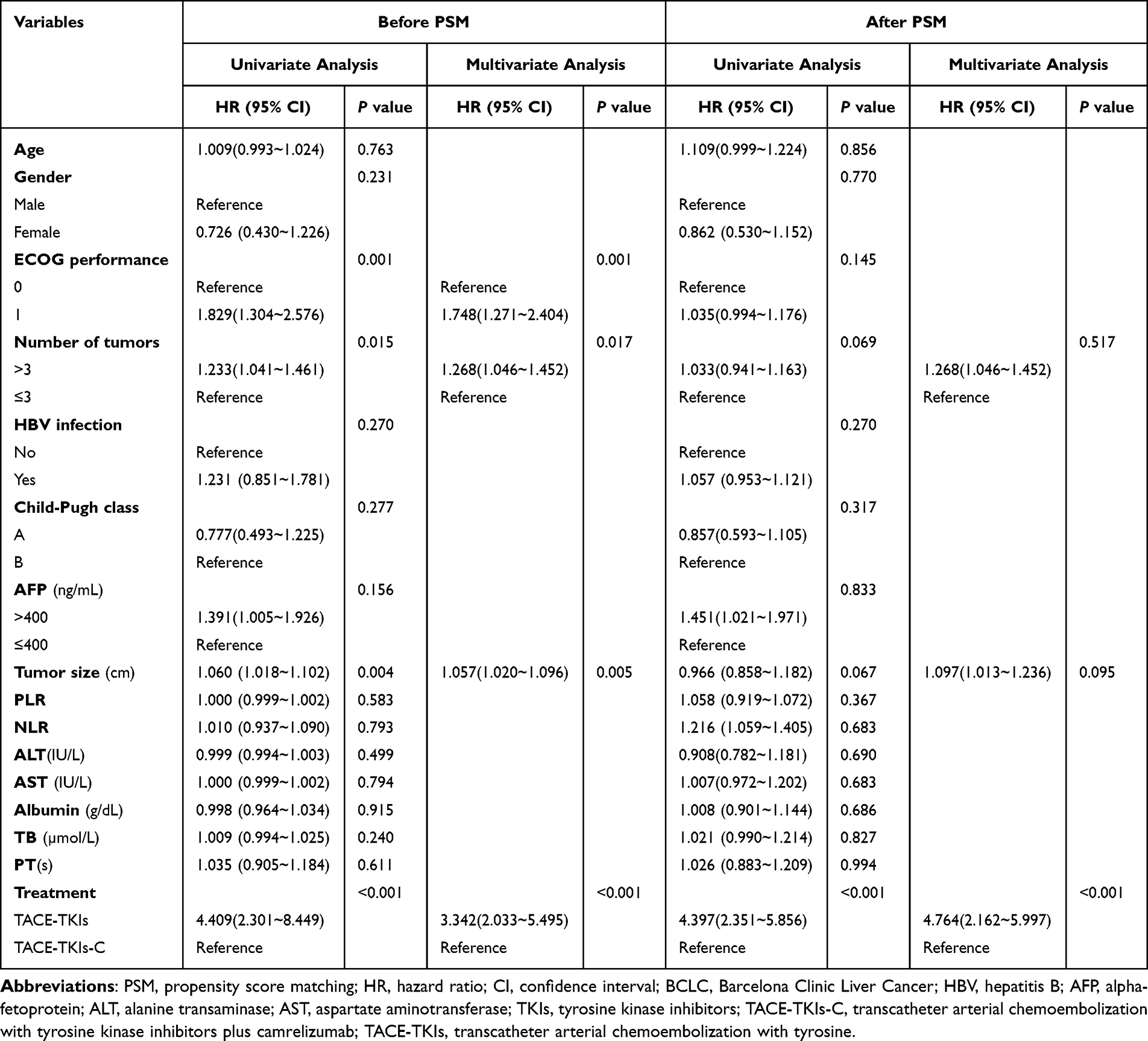 |
Table 3 Univariate and Multivariate Analysis of Prognostic Factors for OS Before and After PSM Analysis |
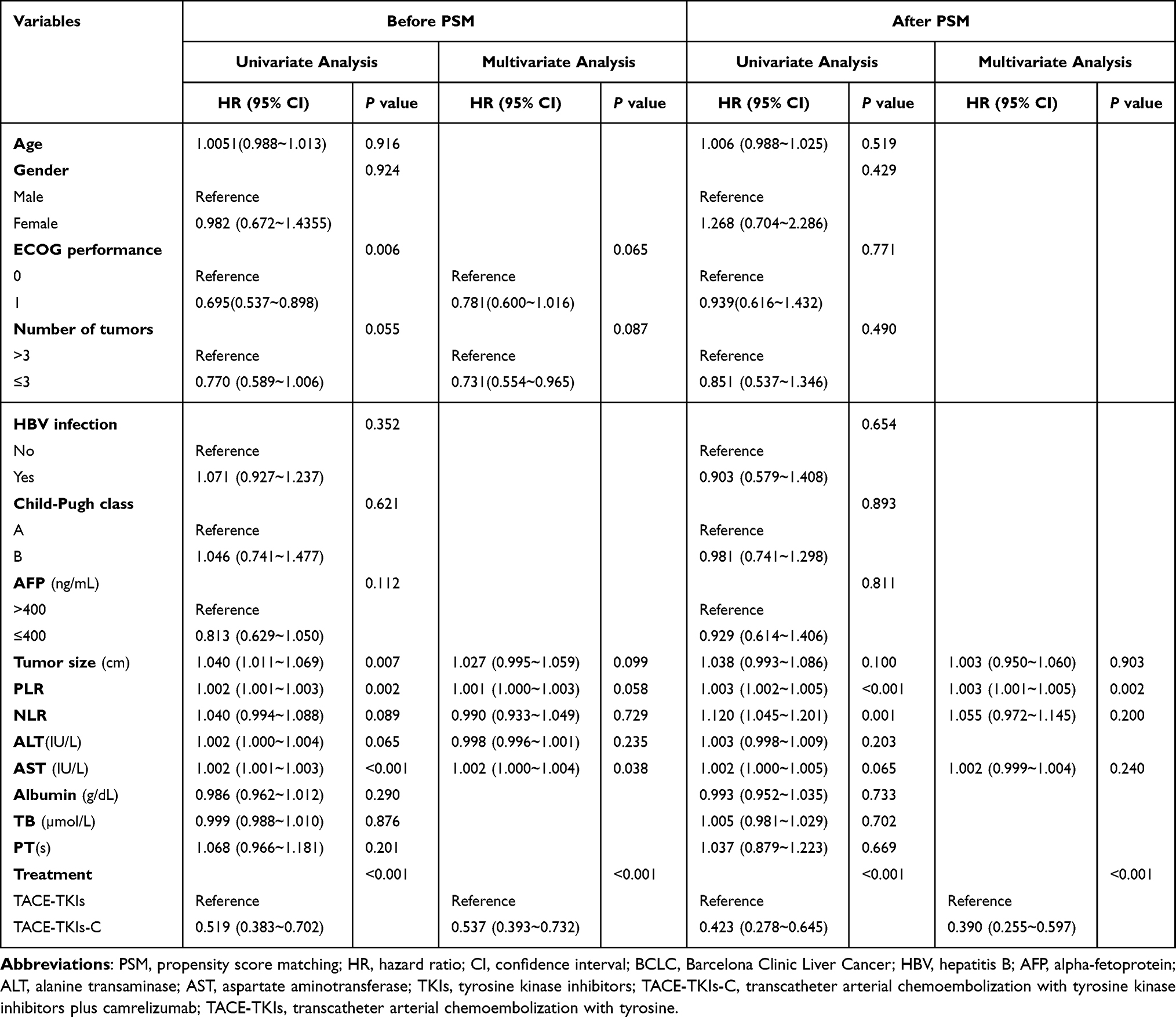 |
Table 4 Univariate and Multivariate Analysis of Prognostic Factors for PFS Before and After PSM Analysis |
OS and PFS Subgroup Analysis by the TKIs Type of TACE-TKIs-C Group Before PSM Analysis
In the subgroup analysis, median OS of TACE-Apatinib-C was 15.0 months (95% CI, 12.173–17.827 months) and the median OS of TACE-Sorafenib-C group and TACE-Lenvatinib-C groups were not reached. The median PFS of TACE-Sorafenib-C, TACE-Lenvatinib-C, and TACE-Apatinib-C was 6 months (95% CI, 5.073–6.927 months), 7 months (95% CI, 6.4–7.6 months), and 5 months (95% CI, 3.749–6.251 months), respectively. There were significant differences in OS and PFS between different TKIs types of TACE-TKIs-C group (P=0.012, P=0.0027) (Figure 2A and B).
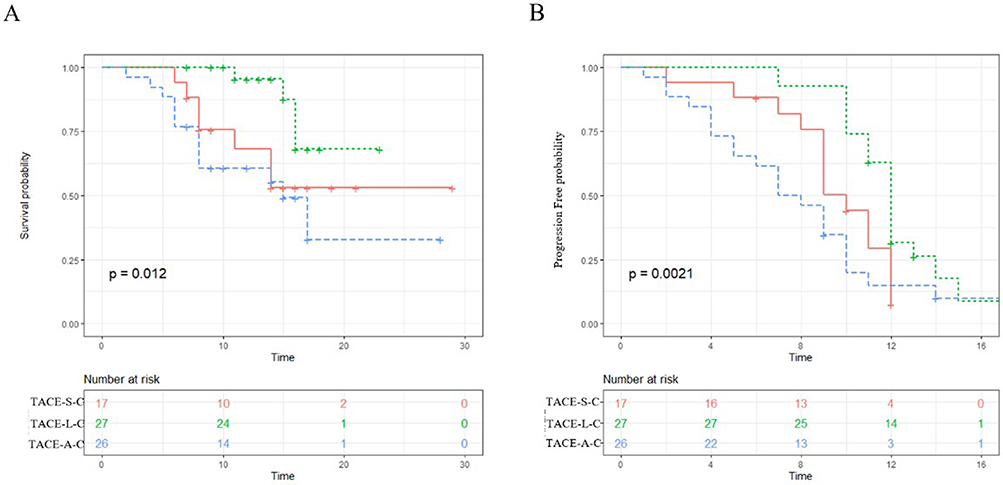 |
Figure 2 The Kaplan–Meier (KM) curves for patients with advanced hepatocellular carcinoma who received the treatment of transcatheter arterial chemoembolization with tyrosine kinase inhibitors plus camrelizumab (TACE-TKIs-C): (A) the KM curves of overall survival time for TACE-S-C, TACE-L-C, and TACE-A-C; (B) the KM curves of progression-free time TACE-S-C, TACE-L-C, and TACE-A-C. TACE-S-C TACE with sorafenib plus camrelizumab; TACE-L-C TACE with lenvatinib plus camrelizumab; TACE-A-C TACE with apatinib plus camrelizumab. |
Safety
Any grade AEs from any cause were reported by 63 patients (90.0%) who received TACE-TKIs-C and by 175 (92.1%) who received TACE-TKIs. The common AEs included hypertension, hand-foot skin reaction, elevated TB, and fatigue in the TACE-TKIs-C group, as consistent with TACE-TKIs group (Table 5). Grade 3–4 AEs occurred in 28 patients (40.0%) with TACE-TKIs-C and in 48 patients (25.3%) with TACE-TKIs, and it occurred more common in patients who received TACE-TKIs-C when compared with TACE-TKIs (P=0.02). Grade 5 AEs did not occur among all patients. Furthermore, there was no significant difference between the TACE-TKIs-C group and the TACE+TKIs group in embolization-related syndrome.
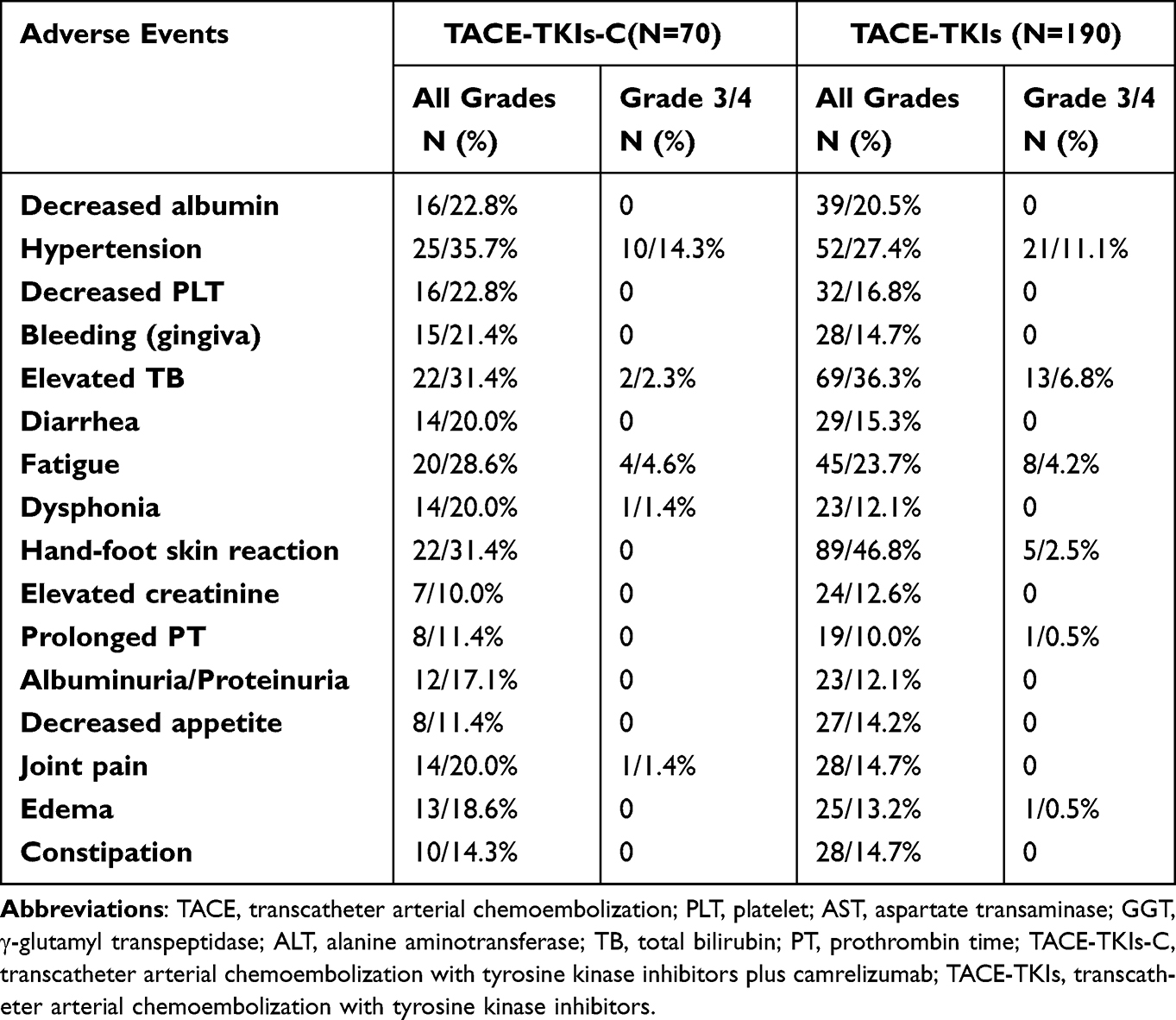 |
Table 5 Adverse Events (>10%) from Any Cause Before PSM |
Discussion
In recent years, the application of ICIs against immune checkpoints, especially PD-1 antibody, is a major breakthrough in the treatment of HCC.11,14 The Check Mate-040 and the KEYNOTE-224 trial showed that advanced HCC could benefit from nivolumab or pembrolizumab, respectively.10,11 However, these treatments were characterized with low ORR, 20% for nivolumab and 16.9% for pembrolizumab. Hence, investigators proposed to combine TKIs with ICIs due to the additional immunomodulatory effects of TKIs.16 Based on the remarkable results of the ORR of 27.3% in the IMbrave150 study, atezolizumab combined with bevacizumab has been approved by the US FDA for the first-line treatment of patients with advanced HCC.15 Thus, the combination of ICIs with TKIs may be the optimal treatment strategy. TACE, as a locoregional therapy, plays a pivotal role in the treatment of advanced HCC.17 In addition to destroying primary tumors, TACE promotes the release of VEGF and promotes antitumor immunity by releasing tumor antigens from dead tumor cells.18,19 The treatment of TACE combined with TKIs plus ICIs may obtain a better clinical effect for advanced HCC.
TKIs including sorafenib, lenvatinib, and apatinib could prolong the OS of advanced HCC, which were recommended as first-line or second-line treatment for advanced HCC patients by China Diagnosis, management, and treatment of hepatocellular carcinoma (V2019). Previous studies about TACE plus TKIs have not yielded the desired results.7–9 TACTICS trial reported that TACE plus sorafenib achieved better PFS compared with TACE alone but without survival benefits in the later data.6 In this two-center retrospective study, the results showed that the TACE-TKIs-c group had significantly better OS and PFS results than the TACE-TKIs group (median OS: NE vs 12.0 months, P<0.0001; median PFS 10.0 months vs 6.0 months, P<0.0001), likely reflecting a higher ORR achieved in patients receiving TACE-TKI-C rather than TACE-TKI. Multivariate analysis also confirmed that the TACE-TKI-based combination of camrelizumab was a significant protective factor for OS and PFS. Similar results were obtained after PSM analysis. As reported by IMbrave150 trial, the median PFS of atezolizumab–bevacizumab group was 6.8 months, which was lower than that of patients with TACE-TKIs-C group in our study. The benefits of OS and PFS in our study over IMbrave150 trial may be due to the role of TACE. Although the PFS of TACE plus sorafenib reported by TACTICS trial was up to 25.2 months, which was much higher over that of TACE-TKIs-C group in our study, the new intrahepatic lesions were not regarded as PD in the TACTICS trial.6 These results indicated that the triple combination treatment of TACE-TKIs-C might be a superior treatment option in advanced HCC patients.
There were several trials which reported combinations of TKIs and ICIs including apatinib plus camrelizumab, lenvatinib plus camrelizumab and sorafenib plus camrelizumab, but with totally different OS.20–22 Thus, different types of TKIs may have different influence on efficacy when combined with camrelizumab. In the present study, three different TKIs were used for the treatment of patients in TACE-TKIs-C group. To determine the impact of TKIs types on efficacy of TACE-TKIs-C group, we evaluated the OS and PFS of TACE-sorafenib-camrelizumab, TACE-lenvatinib-camrelizumab, and TACE-apatinib-camrelizumab by Kaplan–Meier analysis and log rank test. TACE-lenvatinib-camrelizumab group had longer median OS and median PFS, which indicated that different TKIs may affect efficacy and exploring different combinations of TACE-TKIs-camrelizumab is promising. In our study, the dosage and cycle of TKIs were different, which may affect treatment efficacy. However, it still remains meaningful in clinical practice because TKIs were given as the drug directions in our study.
Similar to other studies, the most common AEs were hypertension, hand-foot skin reaction, elevated TB, and fatigue in the TACE-TKIs-C group, which were easily to be controlled.11–15 Although the incidence of Grade 3–4 AEs of TACE-TKIs-C was much higher than that of TACE-TKIs, these AEs including hypertension, fatigue, and elevated TB were significantly improved after symptomatic treatment. No grade 5 AEs were observed in both groups. Thus, these results indicated that the treatment of TACE with TKIs plus camrelizumab for advanced HCC was effective and safe.
The two-centre retrospective study has several limitations. First, due to the nature of the retrospective study, the patient’s background may influence the choice of treatment. Second, due to the short follow-up time, the median OS was not reached in the TACE-TKIs-C group. Third, although this study included data from two centers, the sample size was too small. More convincing prospective, large-scale randomized controlled trials are needed to confirm the efficacy of TACE combined with TKIs plus camrelizumab.
Conclusions
In patients with advanced HCC, TACE-TKIs-C may improve overall and progression-free survival outcomes over TACE-TKIs with manageable safety profile and different types of TKIs may influence the efficacy.
Abbreviations
HCC, Hepatocellular carcinoma; AFP, Alpha-fetoprotein; BCLC, Barcelona Clinic Liver Cancer; CR, Complete response; CT, Computed tomography; EASL, European Association for the Study of the Liver; MR, Magnetic resonance; mRECIST, modified Response Evaluation Criteria in Solid Tumors; OS, Overall survival; PFS, Progression-free survival; PR, Partial response; SD, Stable disease; PD, Progressive disease; PD-1, Programmed death-1; CTLA-4, Cytotoxic T-lymphocyte-associated protein-4; TACE, Transarterial chemoembolization; AEs, Adverse events.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author Chuansheng Zheng ([email protected]) upon reasonable requests.
Ethics Approval and Consent to Participate
The study was approved by institutional review board of the Union Hospital, Tongji Medical college, Huazhong University of Science and Technology (UHCT-IEC-SOP-016-03-01). The study is being conducted in accordance with standards of Good Clinical Practice and the Declaration of Helsinki. Written informed consent was waived by institutional review board of the Union Hospital, Tongji Medical College, Huazhong University of Science and Technology because of the nature of the retrospective study.
Data Deposition and Data Sharing
The data used in the study were available from the corresponding author on reasonable request.
Author Contributions
Tao Sun, Chuansheng Zheng, and Lijie Zhang, and conceived and designed the study. Tao Sun contributed significantly to manuscript preparation. Yanqiao Ren and Bo Sun performed acquisition and analysis of data. Lei Chen and Licheng Zhu helped to critically review the article. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by a grant from the National Natural Science Foundation of China (No. 81873919).
Disclosure
The authors declare that there was no potential conflict of interest.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. doi:10.3322/caac.21492
2. Llovet JM, Zucman-Rossi J, Pikarsky E, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2016;2:16018. doi:10.1038/nrdp.2016.18
3. Benson AB, D’Angelica MI, Abbott DE, et al. Hepatobiliary cancers, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19(5):541–565. doi:10.6004/jnccn.2021.0022
4. Sieghart W, Hucke F, Peck-Radosavljevic M. Transarterial chemoembolization: modalities, indication, and patient selection. J Hepatol. 2015;62:1187–1195. doi:10.1016/j.jhep.2015.02.010
5. Zhou J, Sun HC, Wang Z, et al. Guidelines for diagnosis and treatment of primary liver cancer in China (2017 Edition). Liver Cancer. 2018;7:235–260. doi:10.1159/000488035
6. Kudo M, Ueshima K, Ikeda M, et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut. 2020;69(8):1492–1501. doi:10.1136/gutjnl-2019-318934
7. Meyer T, Fox R, Ma YT, et al. Sorafenib in combination with transarterial chemoembolisation in patients with advanced hepatocellular carcinoma (TACE 2): a randomised placebo-controlled, double-blind, Phase 3 trial. Lancet Gastroenterol Hepatol. 2017;2:565–575. doi:10.1016/S2468-1253(17)30156-5
8. Kudo M, Han G, Finn RS, et al. Brivanib as adjuvant therapy to transarterial chemoembolization in patients with hepatocellular carcinoma: a randomized phase III trial. Hepatology. 2014;60:1697–1707. doi:10.1002/hep.27290
9. Kudo M, Cheng A-L, Park J-W, et al. Orantinib versus placebo combined with transcatheter arterial chemoembolisation in patients with advanced hepatocellular carcinoma (Oriental): a randomised, double-blind, placebo-controlled, multicentre, phase 3 study. Lancet Gastroenterol Hepatol. 2018;3:37–46. doi:10.1016/S2468-1253(17)30290-X
10. Kudo M. Combination cancer immunotherapy in hepatocellular carcinoma. Liver Cancer. 2018;7(1):20–2711. doi:10.1159/000486487
11. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a nonrandomised, open-label Phase 2 trial. Lancet Oncol. 2018;19:940–952. doi:10.1016/S1470-2045(18)30351-6
12. Yang XG, Sun YY, Wang HQ, et al. Efficacy and safety of transarterial chemoembolization combining sorafenib with or without immune checkpoint inhibitors in previously treated patients with advanced hepatocellular carcinoma: a propensity score matching analysis. Front Oncol. 2022;13(12):914385. doi:10.3389/fonc.2022.914385
13. Finn RS, Ryoo B-Y, Merle P, et al. Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, phase III trial. J Clin Oncol. 2020;38:193–202. doi:10.1200/JCO.19.01307
14. Yau T, Park JW, Finn RS, et al. CheckMate 459: a randomized, multi-center phase 3 study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (pts) with advanced hepatocellular carcinoma (aHCC). Ann Oncol. 2019;30(5):v874–v875. doi:10.1093/annonc/mdz394.029
15. Galle PR, Finn RS, Qin S, et al. Patient-reported outcomes with atezolizumab plus bevacizumab versus sorafenib in patients with advanced hepatocellular carcinoma (IMbrave150): an open-label, randomised, phase 3 trial. Lancet Oncol. 2021;22(7):991–1001. doi:10.1016/S1470-2045(21)00151-0
16. Ribas A, Wolchok JD. Cancer immunotherapy using checkpoint blockade. Science. 2018;359(6382):1350–1355. doi:10.1126/science.aar4060
17. Jiang JF, Lao YC, Yuan BH, et al. Treatment of hepatocellular carcinoma with portal vein tumor thrombus: advances and challenges. Oncotarget. 2017;8:33911–33921. doi:10.18632/oncotarget.15411
18. Rizzo A, Ricci AD, Brandi G. Immune-based combinations for advanced hepatocellular carcinoma: shaping the direction of first-line therapy. Future Oncol. 2021;17(7):755–757. doi:10.2217/fon-2020-0986
19. Esagian SM, Kakos CD, Giorgakis E, Burdine L, Barreto JC, Mavros MN. Adjuvant transarterial chemoembolization following curative-intent hepatectomy versus hepatectomy alone for hepatocellular carcinoma: a systematic review and meta-analysis of randomized controlled trials. Cancers. 2021;13(12):2984. doi:10.3390/cancers13122984
20. Xu J, Shen J, Gu S, et al. Camrelizumab in combination with apatinib in patients with advanced hepatocellular carcinoma (rescue): a nonrandomized, open-label, phase II trial. Clin Cancer Res. 2021;27(4):1003–1011. doi:10.1158/1078-0432.CCR-20-2571
21. Wei F, Huang Q, He J, Luo L, Zeng Y. Lenvatinib plus camrelizumab versus lenvatinib monotherapy as post-progression treatment for advanced hepatocellular carcinoma: a short-term prognostic study. Cancer Manag Res. 2021;13:4233–4240. doi:10.2147/CMAR.S304820
22. Liu Q, You N, Li J, et al. Camrelizumab plus sorafenib versus sorafenib monotherapy for advanced hepatocellular carcinoma: a retrospective analysis. Front Oncol. 2021;11:694409. doi:10.3389/fonc.2021.694409
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.