")
Back to Journals » International Journal of General Medicine » Volume 14
The Feasibility of Anterior Occipital Condyle Screw for the Reconstruction of Craniovertebral Junction: A Digital Anatomical and Cadaveric Study of a Novel Technique
Authors Xu D , Peng Y, Li H, Wang Y, Ma W
Received 31 July 2021
Accepted for publication 26 August 2021
Published 8 September 2021 Volume 2021:14 Pages 5405—5413
DOI https://doi.org/10.2147/IJGM.S332071
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dingli Xu, 1 Yujie Peng, 2 Haojie Li, 2 Yang Wang, 2 Weihu Ma 2
1Department of Orthopedics, The Affiliated Hospital of Medical School, Ningbo University, Ningbo, Zhejiang, People’s Republic of China; 2Department of Spine, Ningbo No.6 Hospital, Ningbo, Zhejiang, People’s Republic of China
Correspondence: Weihu Ma
Department of Spine, Ningbo No.6 Hospital, Ningbo, Zhejiang, People’s Republic of China
Email [email protected]
Background: Anterior occipital condyle screw (AOCS) could be a feasible alternative technique for occipitocervical fusion for reconstruction of craniovertebral junction. This study aimed to analyze the feasibility of AOCS.
Methods: The craniovertebral junction computed tomography (CT) scans of 40 adults were enrolled and imported into Mimics software. Then, the three-dimensional reconstruction digital model of craniovertebral junction was established to determine entry point, insertion angle, and screw’s trajectory. After AOCS insertion into ten human cadaver spine specimens, CT scans were performed to verify the location between screws and important structures.
Results: The optimal entry point was located caudally and medial to the ventral of occipital condyle. The optimal trajectory was in inclination angle (5.9°± 3.4°) in the sagittal plane and divergence angle (26.7°± 6.0°) in the axial plane with the screw length around 21.6± 1.2mm. None of the screws invaded the hypoglossal canal and vertebral artery in any of the specimens.
Conclusion: AOCS fixation is a feasible, novel technique for anterior craniovertebral junction reconstruction, and it could be an effective alternative operation for anterior reconstruction with titanium mesh cage.
Keywords: anterior occipital condyle screw, craniovertebral reconstruction, optimal trajectory, cadaveric study
Background
The craniovertebral junction (CVJ) which connects the spine and skull base is a pivotal structure, because it is a complex combination — osseous and ligamentous, with two functions both supporting a large degree of motion, and allowing biomechanical stability.1 However, there are some disorders that lead to death and disability in CVJ, such as rheumatoid arthritis, tuberculosis, deformity, trauma, infection, congenital malformation and tumors. These diseases result in cranial nerve dysfunction, limb paralysis, myelopathy and even death.2
Occipitocervical fixation and reconstruction should be performed when CVJ is rendered unstable or if there is spinal cord compression caused by those dangerous diseases.3 Usually, rod/wires, rod/screw and plate/screw fixation are widely used in posterior occipitocervical fusion, such as Luque rod with wires fixation,4 occipital squama plate fixation.5 Visocchi et al reported that out of 9 adult patients with craniovertebral junction instability treated with posterior occipitocervical fusion, 8 patients had neurological improvement without complication,6 and similar articles reported that posterior occipitocervical fusion can achieve satisfaction and high bone fusion rate.7,8 Whereas, adverse events of posterior occipitocervical fusion were also reported including vascular injury, cerebrospinal fluid leakage, tectorial membrane injury even fixation failure.9,10
As for the anterior approach treatments of occipitocervical fusion, the total en bloc spondylectomy using a combined approach11 and reconstruction using a clival plate with titanium mesh cage have been reported.12 Although these two methods can guarantee immediate immobility and achieve satisfactory bone fusion, lots of complications were reported including new neurologic deficit, implant failure, cerebrospinal fluid leakage and cervical nerve root injury.13,14 And clival plate with titanium mesh cage invaded the skull without long learning time and abundant exercises.15 So, optimal internal fixation which permits stronger support and safe insertion is needed.
As a result, the occipital condyle is a hot point and regarded as a feasible anchor point in craniovertebral junction reconstruction. Zhou et al reported a CT-based method for morphometric analysis of 27 fresh-frozen human cadaveric, and they concluded that the occipital condyle can safely hold a 3.5 mm diameter screw.16 Tong et al reported that they used occipital condyle-C1 complex screw in 8 patients with basilar invagination, and the screw was not misplaced or poorly positioned on the CT-scan and no neurovascular complications were detected during follow-up.17 Those studies indicated occipital condyle could be a feasible anatomical structure for occipitocervical fusion. Although posterior occipital condylar screw fixation is regarded as a feasible technique for occipitocervical fusion, it is not available in cases of high-riding vertebral artery, narrow pedicle and previous cervical fusion.18 Transoral anterior occipital condylar screw fixation (AOCS) can be safely used in these situations. Moreover, AOCS can be combined with posterior occipitocervical fusion in order to permit strong support and maintain alignment.
In this study, we aimed to analyze the anatomical parameters and evaluate the optimal screw trajectory of AOCS with commercial 3D reconstruction software package and design a plate based on these parameters. Then, by using human cadaveric specimens, we tested the feasibility and accuracy of AOCS.
Methods
40 healthy adults had CT scans (Philips Medical Systems, Eindhoven, the Netherlands) of the craniovertebral junction from July 2017 to November 2018 which were enrolled in this study. Exclusion criteria were as follows: 1) patients less than 25 years of age or older than 65 years of age, 2) surgical history of craniovertebral junction, 3) abnormalities including Klippel-Feil syndrome, atlas assimilation and basilar invagination, 4) patients with trauma, tumor, rheumatic arthritis. Then, their craniovertebral junction 3D models were generated based on CT data and the parameters of virtue screws inserted in the models were measured.
Then a plate for anterior occipital condyle screw fixation was designed, which was used to verify the feasibility and accuracy of specimen simulation. The flow diagram of this study was shown in Figure 1. All patients provided written informed consent to participate in our study. This study was approved by the Ethics Committee of The Affiliated Hospital of Medical School, Ningbo University. All patients provided informed consent, and this study was conducted in accordance with the Declaration of Helsinki.
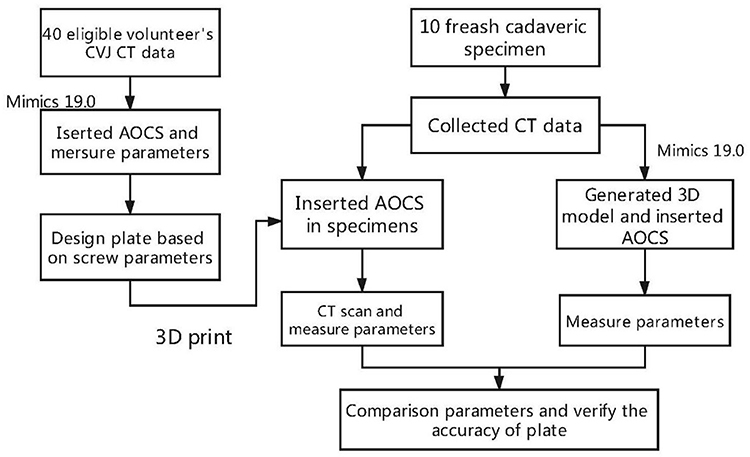 |
Figure 1 This picture shos the flow of this study. |
Digital Measurement of AOCS in Volunteers’ 3D Models
A total of 40 suitable patients met the criteria after our analysis, with average age 35.4±7.6 years (22 males, 18 females). Then all patients’ CT scans were converted to DICOM 3.0 format, and imported into commercial 3D reconstruction software package Mimics 19.0 (Materialise, Leuven, Belgium). The 3D reconstruction model of skull base, occipital and atlas was generated (Figure 2).
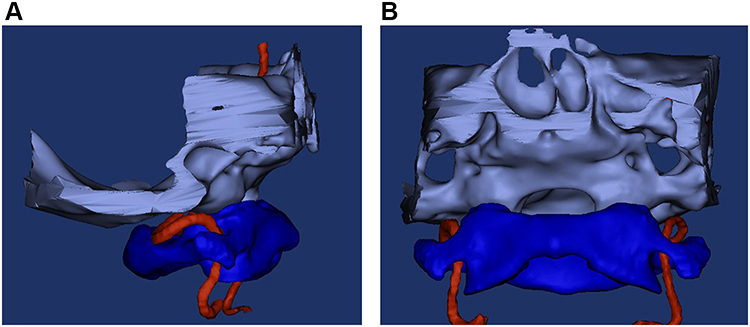 |
Figure 2 (A) Sagittal and (B) frontal views of 3D reconstruction model of skull base, atlas and vertebral artery. |
After generating the 3D model, we inserted the anterior occipital condyle screw in these models. The optimal trajectory should have the longest screw length of bicortical purchase and not invade the hypoglossal canal or vertebral artery. The insertion point was at the medial and caudal on the anterior occipital condyle, then one screw was inserted at this insertion point and the screw direction was pointed to transfigure site of occipital condyle and skull base (Figure 3). Then we imported the 3D model and screws into 3-matic (Materialise, Leuven, Belgium), and built horizontal plane (P1) and vertical plane (P2) of foramen magnum and the long axis of screws by Analyze Tool. The angle between screw and P1, P2 was inclination angle, and divergence angle respectively (Figure 4).
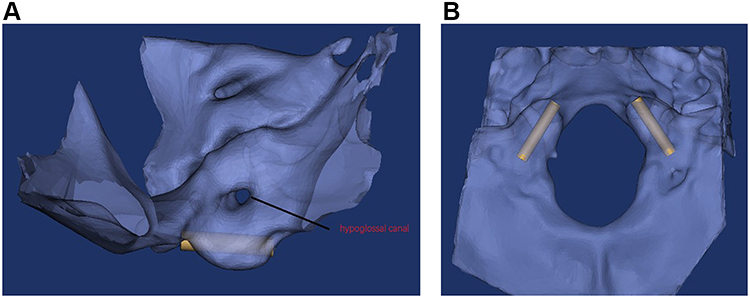 |
Figure 3 The sagittal (A) and axial (B) views of anterior occipital condyle screw fixation, and hypoglossal canal which was not injured by screw. |
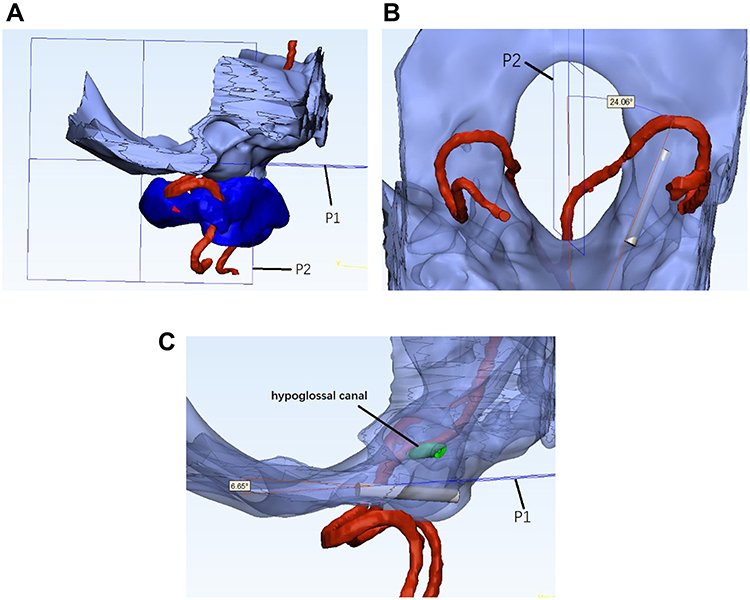 |
Figure 4 (A) The 3D model of skull base, occipital condyle, AOCS, vertebral artery and atlas in 3-matic 19.0, (B) the measurement of divergence angle between AOCS and vertical plane (P2) of foramen magnum, (C) the measurement of inclination angle between AOCS and horizontal plane (P1) of foramen magnum, and there was no injury to hypoglossal canal or vertebral artery. |
Cadaveric Specimen Verification of AOCS
The plate was designed based on the parameters of anterior occipital condyle screw and craniovertebral junction (Figure 5). Ten human cadaveric specimens were collected from our hospital. The age and cause of death were unknown. The specimens were confirmed by CT scans as normal craniovertebral junction to exclude the existence of any deformities, trauma, tuberculosis, tumors, and rheumatoid arthritis.
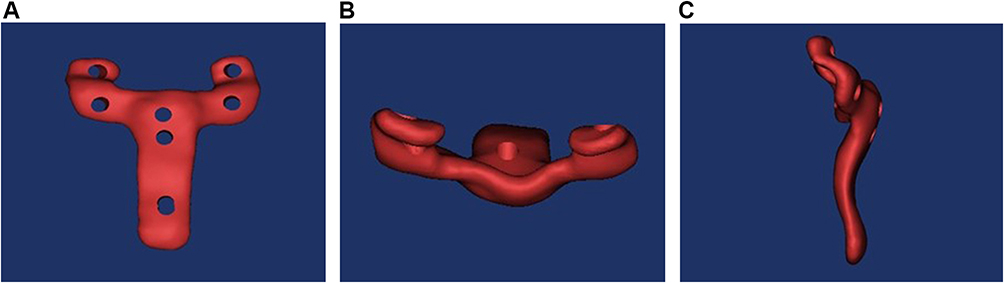 |
Figure 5 The front (A), top (B) and lateral (C) views of 3D reconstruction model of plate. |
Measuring Parameters of AOCS in 3D Model of Specimens
Firstly, we generated 3D models of 10 specimens in Mimics 19.0 based on CT scans, and placed plate model to the anterior of occipital and atlas. Secondly, screws were inserted according to the plate model. Finally, we imported 3D models into 3-matic 19.0 and measured parameters of AOCS.
Measuring Parameters of AOCS in Specimens
After exposing the anterior occipital condyle and atlas, we firstly put-up plate to the craniovertebral junction and inserted screws assisted by plate. Secondly, we performed CT scans on those specimens to clarify whether there was any hypoglossal canal or vertebral artery injury. Finally, the parameters of AOCS in specimens and 3D models were measured and compared (Figure 6).
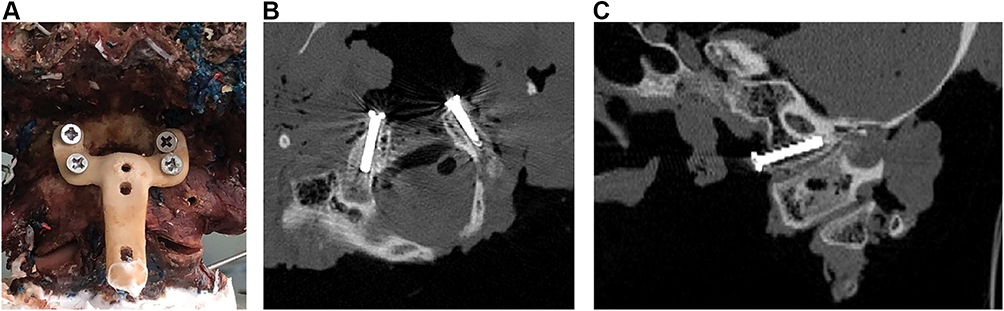 |
Figure 6 (A) This picture shows anterior occipital condyle screw and plate fixation in cadaveric specimen. Axial (B) and sagittal (C) views of the CT scan of anterior occipital condyle screw fixation in cadaveric specimen, and the hypoglossal canal was not injured by screw. |
Statistical Analysis
All results were presented as Mean±Standard deviation. The left and right occipital condyle’s inclination angle, divergence angle and screw length of volunteers’ 3D models were analyzed by compared t-test in SPSS version 21.0 (Chicago, IL). And the comparison of occipital condyle’s inclination angle, divergence angle and screw length between specimen’s model and specimens was conducted by compared t-test. P<0.05 was set as statistically significant in this study.
Result
The Parameters of AOCS Measured in Volunteers’ 3D Models
All 3D models had screws successfully inserted without hypoglossal canal or vertebral artery injury, and the parameters of anterior occipital condyle screw were shown in Table 1. There was no significant difference between left and right site in the parameters of anterior occipital condyle screw (P>0.05). The total inclination angle was 5.9°±3.4° (0.6°~11.9°) and divergence angle was 26.7°±6.0° (17.1°~37.7°), the screw length in all models was 21.6±1.2mm (19.1~25.0mm).
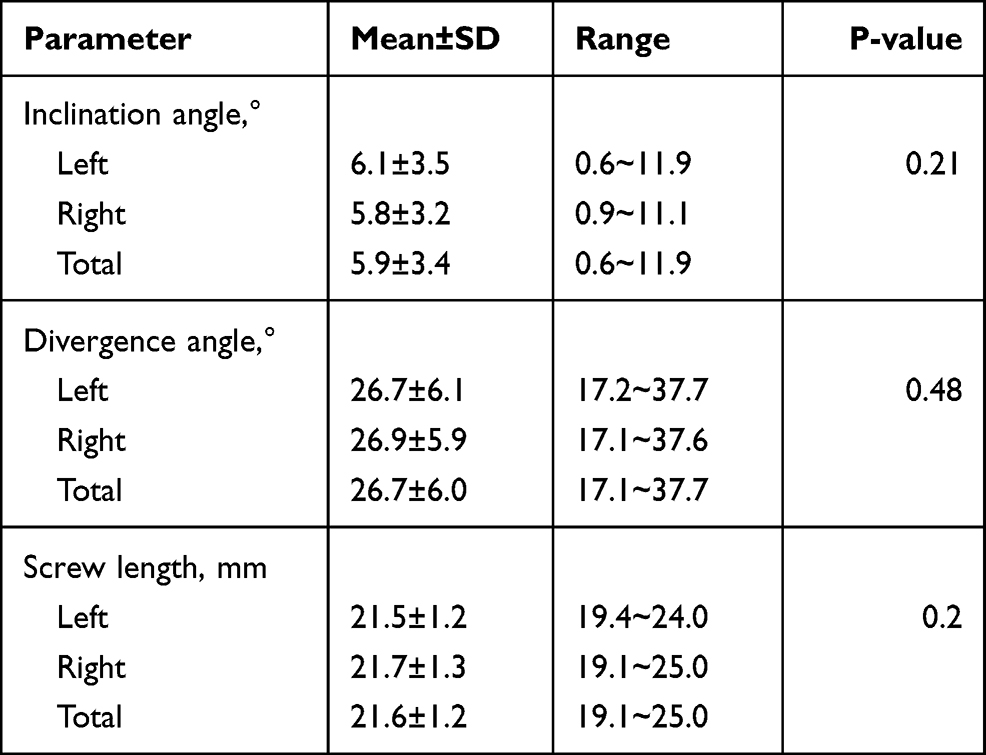 |
Table 1 The Parameters of Anterior Occipital Condyle Screw on the Volunteer’s 3D Model |
The Parameters Measured in Specimens’ Models and Specimens
Before inserting anterior occipital condyle screws in these ten cadaveric specimens, we performed CT scans and imported the data into Mimics 19.0 for 3D model generation. Then we inserted anterior occipital condyle screws in specimens’ 3D models and measured the parameters including inclination angle, divergence angle, and screw length. Next, anterior occipital condyle screws were inserted assisted by plate. The parameters of models and specimens were shown in Table 2. There was no significant difference in inclination angle between specimen’s model (5.8°±0.5°) and specimen (5.7°±0.5°) (P=0.42). Similarly, there was no statistically significant difference in divergence angle and screw length between specimen’s model and specimens (26.7°±5.4°, 21.6mm±0.7mm VS 21.7°±1.0°, 20.3mm±6.0mm. P>0.05).
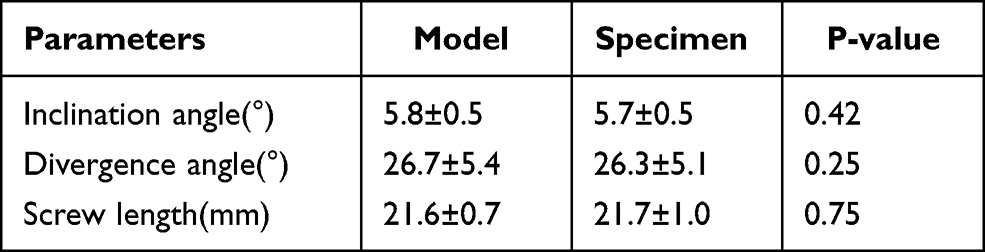 |
Table 2 The Comparison of Screw Parameters Between Specimen’s Model and Specimen |
Discussion
In recent years, there has been an increase in the incidence rate of tumor, tuberculosis, and trauma in craniovertebral junction, many scholars have reported the risk of danger and challenge of these diseases.19,20 Posterior occipital cervical fusion is now widely used for craniovertebral junction reconstruction because of satisfactory clinical outcome. Whereas posterior occipitocervical fusion may have some complications including nonunion and screw loosening, dural tears, infection, and failure to reduce neurological pain.21 What is more, posterior occipital squama screw and plate fixation cannot be performed when inner occipital crest is located off the suboccipital midline ridge and abnormal.22 Although posterior occipital condyle screw is an alternative technique when skull base is abnormal or in case of previous skull base operation,23 many important anatomical structures such as vertebral artery, C2 nerve root and posterior cervical muscle will be damaged during exposure in posterior approach, which may result in neck pain.24,25 And posterior pedicle screws may be infeasible in some patients with anatomic variations such as narrow C2 isthmus and absence of bone structure.26,27 As for anterior occipitocervical fusion, en bloc resection is one method for upper cervical reconstruction which has been reported to have achieved desired clinical efficacy.14,28,29 Similarly, clival screw and plate fixation was also reported as a feasible technique for craniovertebral reconstruction in anatomy.30 However, both these surgical methods have some disadvantages. There are some complications and risks of aforementioned methods including 1) the inner structure of clivus was the epencephalon and foramen magnum which contains medulla oblongata and it may be injured when inserting the clival screw. Invasion into cranial cavity is a fatal risk, 2) during the posterior approach exposure, the vertebral venous sinus and plexus around the upper cervical spine which may cause bleeding once injured.31
As a consequence, our group intended to design an alternative operation method, which can prevent the aforementioned difficulties and complications. Bosco et al reported a morphometric evaluation and anatomical parameters of occipital condyle, and showed that average occipital condyle length, width, anterior height and posterior height were 18.8±2.3 mm, 10.3±1.5 mm, 13.2±2.2 mm and 8.5±1.6 mm, respectively. Moreover, the occipital condyle can safely hold a screw without hypoglossal canal being invaded.32 Similarly, our group reported the same outcome in a CTA based study.33 As for cadaveric specimen evaluation, Yu et al reported that a total of 40 4-mm posterior occipital condyle screws were successfully inserted into twenty (40 occipital condyles) cadaveric specimens, and no screw invaded the hypoglossal canal as verified by postoperative CT scan.34 According to these studies, occipital condyle could be a feasible bone structure for craniovertebral junction reconstruction in anterior approach, and AOCS has been shown to be a feasible and safe technique which can be used in narrow C2 isthmus and high-riding vertebral artery. However, vital surrounding structures need to be taken into account. The cephalad and medially of occipital condyle is hypoglossal canal which contains hypoglossal nerve and foramen magnum.35 So, in the sagittal plane, if the anterior occipital condyle screw is placed with a large inclination angle, it may invade the hypoglossal canal and damage hypoglossal nerve, on the contrary, if the screw is inserted too caudally or medially, it may violate vertebral artery or foramen magnum which may cause injury to spinal cord and medulla oblongata.36,37
In this study, we enrolled 40 healthy adults’ craniovertebral junction CT data and generated 3D models using Mimics 19.0 software. This digital anatomy and cadaveric study of craniovertebral junction confirmed the anatomical feasibility of anterior occipital condyle screw and plate fixation and primarily verified the entry point and optimal trajectory of AOCS. According to our result, the optimal trajectory for AOCS insertion is an inclination angle of 5.9°±3.4° on sagittal plane and divergence angle of 26.7°±6.0° on axial plane, and the average screw length was 21.6±1.2 mm. Researchers reported that screw length longer than 18 mm can have enough pull-out strength.38 As for simulation in cadaveric specimens, all AOCS were inserted assisted with plate successfully without hypoglossal canal injury or broken cortex. Then CT scans were performed and 3D models generated using Mimics 19.0 software. After that, parameters of anterior occipital condyle screw were measured and compared between specimen’s models and specimens. There was no significant difference in inclination angle, divergence angle, and screw length between the two groups (P>0.05). This showed that the anterior occipital condyle screw can be safely placed assisted with plate, and using plate can enhance the accuracy and decrease the risk of vital surrounding anatomical structure damage.
We should pay attention to the hypoglossal canal during anterior occipital condyle screw fixation, because the hypoglossal canal which contains hypoglossal nerve and venous plexus passes from intracranial to the anteromedial upper part of occipital condyle, its location determines the safe area of screw placement. Usually, the hypoglossal canal is located in the anterior medial of occipital but some patients’ hypoglossal canal is located posterior and medial to occipital condyle. Therefore, we should analyze the CT scan of every single patient and justify the inclination angle when hypoglossal canal is located posterior and medial to occipital condyle.39 Moreover, intraoperative monitoring of hypoglossal nerve function can help anatomical localization of the hypoglossal triangle, and reflect whether there has been hypoglossal nerve injury during operation.40,41 Therefore, correct preoperative diagnosis and radiological outcome analysis should be performed before anterior occipital condyle screw fixation.
The primary indications for AOCS fixation are as follows: 1) anterior craniovertebral junction reconstruction and combined posterior approach occipitocervical fusion; 2) upper cervical spine abnormalities such as narrow C2 isthmus; 3) occipital condyle fracture; 4) patients who suffer from failure of posterior upper cervical spine fixation who cannot undergo a second operation. However, patients with occipital condyle or vertebral artery deformity should be considered as contraindicated. The significance of AOCS fixation was as follows: 1) a new insertion point in skull base; 2) a salvage technique when other occipitocervical fusion failed or is not available.
Limitations
This study has some limitations, first, the simple size of the volunteers was not ideal, but this was a study which aimed to propose a new technique and test the feasibility. Second, as a result of limited source of specimens, only ten cadaveric specimens were simulated for anterior occipital screw fixation. Although all specimens were placed anterior occipital condyle screws safely, this technique still needs a lot of research for further proof. Finally, anterior occipital condyle screw plate fixation is feasible but whether it can achieve immediate stability and abundant support strength still needs biomechanical study and further clinical study.
Conclusion
In conclusion, AOCS fixation for craniovertebral junction reconstruction is a feasible and safe surgical technique, and it could be regarded as a salvage technique eventually. More importantly, insertion of anterior occipital condyle screw assisted with plate can improve accuracy and avoid risks.
Abbreviations
AOCS, anterior occipital condyle screw; CVJ, craniovertebral junction; 3D, three dimensional.
Data Sharing Statement
All data are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
All patients signed a written informed consent form to participate in our study. This study was approved by the Ethics Committee of The Affiliated Hospital of Medical School, Ningbo University. All patients provided informed consent, and this study was conducted in accordance with the Declaration of Helsinki. In this study, there were no identifying personal or clinical details along with any identifying images published.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Author Contributions
The contribution of each author to this paper is as follows: Dingli Xu (data collection, writing original manuscript); Yujie Peng (methodology); Yang Wang and Haojie Li (software measurements, statistical analysis); and Weihu Ma (prepared the figures, revised the manuscript). All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The role of funding which named National Nature Foundation of China (81572217) is in the design of the interpretation of data and in writing the manuscript, and Natural Science Foundation of Zhejiang Province (LY18H060002) is in the design of this study.
Disclosure
The authors declare no conflicts of interest in association with the present study.
References
1. Lopez AJ, Scheer JK, Leibl KE, Smith ZA, Dlouhy BJ, Dahdaleh NS. Anatomy and biomechanics of the craniovertebral junction. Neurosurg Focus. 2015;38(4):E2. doi:10.3171/2015.1.FOCUS14807
2. Ji W, Xu X, Liu Q, et al. Anterior atlantooccipital transarticular screw fixation. Spine. 2019;44(17):E1010–E1017. doi:10.1097/BRS.0000000000003056
3. Joaquim AF, Osorio JA, Riew KD. Occipitocervical fixation: general considerations and surgical technique. Global spine j. 2020;10(5):647–656. doi:10.1177/2192568219877878
4. Klimo P, Astur N, Gabrick K, Warner WC, Muhlbauer MS. Occipitocervical fusion using a contoured rod and wire construct in children: a reappraisal of a vintage technique. J Neurosurg Pediatr. 2013;11(2):160–169. doi:10.3171/2012.9.PEDS12214
5. Yanai Y, Tsuji R, Ohmori S, Kubota S, Nagashima C. Foramen magnum syndrome caused by a dolichoodontoid process. Surg Neurol. 1985;24(1):95–100. doi:10.1016/0090-3019(85)90073-4
6. Visocchi M, Di Rocco F, Meglio M. Craniocervical junction instability: instrumentation and fusion with titanium rods and sublaminar wires. Effectiveness and failures in personal experience. Acta neurochirurgica. 2003;145(4):265–272. doi:10.1007/s00701-002-1067-6
7. Matsunaga S, Ijiri K, Koga H. Results of a longer than 10-year follow-Up of patients with rheumatoid arthritis treated by occipitocervical fusion. Spine. 2000;25(14):1749–1753. doi:10.1097/00007632-200007150-00002
8. Singh SK, Rickards L, Apfelbaum RI, Hurlbert RJ, Maiman D, Fehlings MG. Occipitocervical reconstruction with the ohio medical instruments loop: results of a multicenter evaluation in 30 cases. J Neurosurg. 2003;98(3 Suppl):239–246.
9. Fiester P, Rao D, Soule E, Jenson M, Patel J. Tectorial Membrane injury, frequently identified in adult trauma patients who undergo occipital-cervical fusion for craniocervical instability. Cureus. 2021;13(4):e14254.
10. Salunke P, Sahoo SK, Sood S, Mukherjee KK, Gupta SK. Focusing on the delayed complications of fusing occipital squama to cervical spine for stabilization of congenital atlantoaxial dislocation and basilar invagination. Clin Neurol Neurosurg. 2016;145:19–27. doi:10.1016/j.clineuro.2016.04.001
11. Wei F, Liu Z, Liu X, et al. An approach to primary tumors of the upper cervical spine with spondylectomy using a combined approach: our experience with 19 cases. Spine. 2018;43(2):81–88. doi:10.1097/BRS.0000000000001007
12. Lin J, Kong G, Xu X, et al. Clival screw and plate fixation by the transoral approach for the craniovertebral junction: a CT-based feasibility study. Eur spine j. 2019;28(10):2342–2351. doi:10.1007/s00586-019-06039-5
13. Wu W, Li F, Fang Z, et al. Total spondylectomy of C2 and circumferential reconstruction via combined anterior and posterior approach to cervical spine for axis tumor surgery. J Huazhong Univ Sci Technolog Med Sci. 2013;33(1):126–132. doi:10.1007/s11596-013-1084-0
14. Wang X, Eichbaum E, Jian F, Chou D. Two-stage en bloc resection of multilevel cervical chordomas with vertebral artery preservation: operative technique. Operative Neurosurgery. 2018;14(5):538–545. doi:10.1093/ons/opx178
15. Ji W, Tong J, Huang Z, et al. A clivus plate fixation for reconstruction of ventral defect of the craniovertebral junction: a novel fixation device for craniovertebral instability. Eur Spine j. 2015;24(8):1658–1665. doi:10.1007/s00586-015-4025-8
16. Zhou J, Espinoza Orias AA, Kang X, et al. CT-based morphometric analysis of the occipital condyle: focus on occipital condyle screw insertion. J Neurosurg Spine. 2016;25(5):572–579. doi:10.3171/2016.4.SPINE151431
17. Tong H, Li L, Yu XG, Zhang Y, Peng W. Occipital Condyle-C1 complex screw for fixation of basilar invagination patients with atlas assimilation. Turk Neurosurg. 2016;26(5):758–762.
18. Ahmadian A, Dakwar E, Vale FL, Uribe JS. Occipitocervical fusion via occipital condylar fixation: a clinical case series. J Spinal Disord Tech. 2014;27(4):232–236. doi:10.1097/BSD.0b013e31825bfeea
19. Menezes AH. Craniovertebral junction neoplasms in the pediatric population. Child’s Nervous System. 2008;24(10):1173–1186. doi:10.1007/s00381-008-0598-4
20. Zou J, Yuan C, Zhu R, Zhang Z, Jiang W, Yang H. Effect of occipitocervical fusion with screw-rod system for upper cervical spine tumor. BMC Surg. 2014;14:30. doi:10.1186/1471-2482-14-30
21. Lall R, Patel NJ, Resnick DK. A review of complications associated with craniocervical fusion surgery. Neurosurgery. 2010;67(5):1396–1402. doi:10.1227/NEU.0b013e3181f1ec73
22. Mullett JH, McCarthy P, O’Keefe D, McCabe JP. Occipital fixation: effect of inner occipital protuberance alignment on screw position. J Spinal Disord. 2001;14(6):504–506. doi:10.1097/00002517-200112000-00007
23. Uribe JS, Ramos E, Vale F. Feasibility of occipital condyle screw placement for occipitocervical fixation: a cadaveric study and description of a novel technique. J Spinal Disord Tech. 2008;21(8):540–546. doi:10.1097/BSD.0b013e31816d655e
24. Lee BJ, Park JH, Jeon SR, Roh SW, Rhim SC, Jung SK. Posterior cervical muscle-preserving interspinous process approach and decompression: more minimally invasive and modified shiraishi’s selective laminectomy. World Neurosurg. 2020;133:e412–e420. doi:10.1016/j.wneu.2019.09.041
25. Yang J, Jia Q, Peng D, et al. Surgical treatment of upper cervical spine metastases: a retrospective study of 39 cases. World J Surg Oncol. 2017;15(1):21. doi:10.1186/s12957-016-1085-0
26. Mandel IM, Kambach BJ, Petersilge CA, Johnstone B, Yoo JU. Morphologic considerations of C2 isthmus dimensions for the placement of transarticular screws. Spine. 2000;25(12):1542–1547. doi:10.1097/00007632-200006150-00014
27. Png W, Hey HW, Mohan K, Yue WM. Congenital absence of the posterior arch of the atlas with concomitant fusion to the axis: a case report. J Orthopaedic Surgery. 2015;23(3):402–404. doi:10.1177/230949901502300331
28. Meng T, Zhou W, Li B, et al. En bloc resection for treatment of tumor-induced osteomalacia: a case presentation and a systematic review. World J Surg Oncol. 2015;13:176. doi:10.1186/s12957-015-0589-3
29. Wewel JT, Nunna RS, Tan LA, Kasliwal MK, O’Toole JE. Novel reconstruction of the anterior craniocervical junction using an expandable cage with integrated fixation after total C2 spondylectomy for chordoma. J clin neurosci. 2016;30:157–160. doi:10.1016/j.jocn.2016.02.004
30. Ji W, Liu X, Huang W, et al. Clival screw placement in patient with atlas assimilation: a CT-based feasibility study. Sci Rep. 2016;6:1. doi:10.1038/srep31648
31. Magro E, Gentric JC, Talagas M, et al. Venous organization in the transverse foramen: dissection, histology, and magnetic resonance imaging. J Neurosurg. 2015;123(1):118–125. doi:10.3171/2014.10.JNS14906
32. Bosco A, Venugopal P, Shetty AP, Shanmuganathan R, Kanna RM. Morphometric Evaluation of occipital condyles: defining optimal trajectories and safe screw lengths for occipital condyle-based occipitocervical fixation in Indian population. Asian Spine J. 2018;12(2):214–223. doi:10.4184/asj.2018.12.2.214
33. Lou ZQ, Wang Y, Xu DL, et al. Safe trajectory for an occipital condyle screw: a computer simulation study. J Orthopaedic Surgery. 2019;27(3):2309499019879540.
34. Yu Z, Ma X, Jiang J, et al. Feasibility of screw placement in the occipital condyle of Chinese patients for occipitocervical arthrodesis: a cadaveric study. Turk Neurosurg. 2015;25(4):559–565.
35. La Marca F, Zubay G, Morrison T, Karahalios D. Cadaveric study for placement of occipital condyle screws: technique and effects on surrounding anatomic structures. J Neurosurg Spine. 2008;9(4):347–353. doi:10.3171/SPI.2008.9.10.347
36. Ozer MA, Celik S, Govsa F, Ulusoy MO. Anatomical determination of a safe entry point for occipital condyle screw using three-dimensional landmarks. Eur Spine j. 2011;20(9):1510–1517. doi:10.1007/s00586-011-1765-y
37. Degno S, Abrha M, Asmare Y, Muche A. Anatomical variation in morphometry and morphology of the foramen magnum and occipital condyle in dried adult skulls. J Craniofac Surg. 2019;30(1):256–259. doi:10.1097/SCS.0000000000004925
38. Lee JO, Buchowski JM, Lee KM, et al. Optimal trajectory for the occipital condylar screw. Spine. 2012;37(5):385–392. doi:10.1097/BRS.0b013e31821fcdfe
39. Ji W, Xu X, Liu Q, et al. Anterior atlantooccipital transarticular screw fixation: a cadaveric study and description of a novel technique. Spine. 2019;44(17):E1010–E1017.
40. Trentman TL, Thunberg C, Gorlin A, Koht A, Zimmerman RS, Bendok B. Insertion of intra-oral electrodes for cranial nerve monitoring using a Crowe-Davis retractor. J Clin Monit Comput. 2017;31(4):793–796. doi:10.1007/s10877-016-9904-y
41. Duque CS, Londoño AF, Penagos AM, Urquijo DP, Dueñas JP. Hypoglossal nerve monitoring, a potential application of intraoperative nerve monitoring in head and neck surgery. World J Surg Oncol. 2013;11:225. doi:10.1186/1477-7819-11-225
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.