")
Back to Journals » International Journal of Women's Health » Volume 12
The Extent of Maternal Nutritional Knowledge and Practice During Lactation in Kombolcha Town, South Wollo Zone, Ethiopia: A Mixed Study Design
Authors Tessema DG, Girma E, Mekonnen TC , Mebratu W
Received 12 October 2019
Accepted for publication 3 January 2020
Published 26 February 2020 Volume 2020:12 Pages 79—87
DOI https://doi.org/10.2147/IJWH.S234398
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Demissie Gelaw Tessema,1,* Eshetu Girma,2,* Tefera Chane Mekonnen,3,* Wondwosen Mebratu3,*
1PathFinder of Ethiopia, Debre Birhan, Ethiopia; 2Department of Preventive Medicine, School of Public Health, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Public Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
*These authors contributed equally to this work
Correspondence: Tefera Chane Mekonnen
Wollo University, Dessie, Ethiopia
Tel +251 911587075
Email [email protected]
Objective: The study aimed to assess nutritional practice and its associated factors among lactating mothers in Kombolcha Town, South Wollo Zone, Amhara Region, Ethiopia, 2017.
Design and Setting: A community-based cross-sectional study design supplemented with qualitative research was conducted at Kombolcha Town from October 23 to November 10, 2017. A systematic sampling technique was used to select the study participants from listed households and purposive sampling was used for the qualitative inquiry.
Participants: A total of 425 lactating mothers were interviewed using a pre-tested structured questionnaire. The data were analyzed using Statistical Package for Social Sciences version 23. For the qualitative data, thematic content analysis was used. Multiple logistic regression was used to evaluate the association between nutritional practice with independent variables.
The Results: Lactating mothers who had good nutritional practice and knowledge were 28.7% (95% CI: 24.9%, 33.5%) and 52.0% (95% CI: 47.1%, 57.6%) respectively. This study revealed that government-employed mothers (AOR=6.0, 95% CI: 1.953, 18.485) and mothers with good nutritional knowledge (AOR=3.12, 95% CI: 1.832, 5.318) had statistically significant associations with nutritional practices of lactating mothers.
Conclusions and Recommendations: The nutritional practices and knowledge of lactating mothers were low in the study area. The mother’s occupation and nutritional knowledge were significantly associated with nutritional practice. Hence, the provision of maternal nutritional education regarding a healthy diet, and timely and regular dissemination of nutritional information were recommended.
Keywords: nutritional knowledge, practice, lactating mother, Kombolcha Town, Ethiopia
Background
Maternal nutrition refers to the nutritional needs of women when they are pregnant and breastfeeding and to the time before conception.1 Lactation is within the critical window and one of the most complex and nutritionally demanding phases of the human life cycle. Adequate nutrition knowledge during lactation plays a bigger role in daily practices2,3 because nutritional knowledge is a backbone for confronting malnutrition at all levels of society, and plays an important role in influencing healthy food habits that ensure that nutrient needs throughout the lifecycle are met adequately. Misconceptions about nutrition within communities negatively influence the proper practice of nutrition.4 When an individual is aware of how to meet these nutritional needs this facilitates food choices that enhance health and wellness by preventing excess or inadequate intake of nutrients that could be associated with ill health.5
Studies have suggested that lactating mothers are the most vulnerable to malnutrition due to low dietary intake and/or low meal frequency, low family income, low educational level, high unemployment status, narrow birth interval, socio-cultural barriers, work overload in the household, limited accessibility of nutritional information and nutritional knowledge, infectious diseases, and lower health-care utilization.6–11
The nutritional knowledge and practice of lactating mothers vary across different countries, e.g. 67% and 51% in Swaziland, and 84% and 65.5% in Pakistan.12
A study conducted in Honduras revealed that standardized health education for reproductive-age women was needed if iron-folic acid consumption through fortification and supplementation is to be successful and sustainable in order to prevent neural tube defects and anemia.13,14
Studies showed that Ethiopia is one of the countries with the highest levels of malnutrition burden among lactating mothers in Sub-Saharan Africa. One in every four lactating mothers in Ethiopia is undernourished.15,16
According to the Ethiopian Demographic Health Survey (EDHS), undernutrition among women dropped from 23% in 2011 to 22% in 2016. The national health promotion and strategy has identified gaps in knowledge and changes in behavior or practice at the individual level that affect all the health programs. Considering the general literacy status, there is a low level of health literacy, which adversely affects the health of the population including lactating women. This indicates that there are still significant gaps in knowledge and healthy practices in most health programs that continue to impact progress towards meeting national targets, including the improved nutritional status of lactating women.17,18
Many consumers have knowledge about certain foods, but this knowledge can be merely misconceptions about the nutritional values of foods. This limited knowledge among lactating mothers may adversely affect the nutritional status of their child and the family in general. Research-based information regarding lactating maternal nutrition improves their nutritional knowledge and practice among the community, and special attention should be given to mothers’ diet during lactation.
Methods and Materials
Study Design and Area
A community-based cross-sectional study design supplemented with qualitative research was conducted in Kombolcha Town from October 23 to November 10, 2017. The town is one of the 22 districts in the South Wollo Zone of Amhara Region, Northeast Ethiopia. The town has 12 kebeles (lowest administrative unit) with a total population of 143,637, of whom 71,103 were men and 72,534 women. The town is found at a latitude and longitude of 11°5′N 39°44′E/11.083°N 39.733°E with an elevation between 1,842 and 1,915 meters above sea level (Kombolcha Town Health Office, South Wollo Zone Health Department, Amhara Regonal Health Beruea, Ethiopia: Annual Plan, 2017) and it is situated 325 km from Addis Ababa and 25 km from Dessie. The town has four health centers and twelve health posts/kebeles, with 6,176 households in total (Kombolcha Town Health Office, South Wollo Zone Health Department, Amhara Regonal Health Beruea, Ethiopia: Annual Plan, 2017).
The study population was randomly selected lactating mothers who were breastfeeding during data collection and were permanent residents in randomly selected kebeles. The study units for qualitative research were lactating mothers who were purposefully selected from the corresponding randomly selected kebeles.
Sample Size Determination and Sampling Technique
The sample size was determined using EPI-Info statistical software version 7.2 by assuming 56.9% of nutrition knowledge, power of 80%, 95% confidence level, the odds ratio of 1.84 and 0.5 ratio of unexposed to exposed of maternal occupation.19 Finally, 438 was the total sample size for this study.
Primarily, there are twelve kebeles in the study area, of which four were randomly selected. The sample size was allocated for each selected kebele proportional to their population. A list of households with lactating mothers was identified from the Kebele Health Extension Workers and eligible mothers were recorded and numbered with their house number, which served as the sampling frame. Lactating mothers were selected using a systematic sampling technique at a regular interval, i.e. after the first household as a random start point, from every three lactating mothers from the list of households, two were selected for an interview by using the lottery method. In addition, if there was more than one lactating mother in a household, one was selected using the lottery method.
For the qualitative study, three focus group discussions were conducted at three sites parallel to the quantitative data collection period using a semi-structured interview guide. Each of the groups consisted of six lactating women that were grouped based on their similar characteristics, such as mothers who have formal and non-formal education groups from the community, health workers’ group from health centers to be a total eighteen lactating women and women’s development army group. The selection was done using a purposive sampling technique and participants were selected on the criterion that they did not participate in the quantitative study.
Data Collection and Measurements
Data were collected through structured questionnaires (social, demographic and economic, source of nutrition information, health service and obstetric history, and practice) and semi-structured questionnaires for focus group discussions as a guideline for interview. The tool was developed and adapted from standard sources, such as FAO guidelines and by reviewing different literature20–23 to address the research objectives.
The focus group discussion sessions were used to understand and explain the meaning, beliefs, and cultures that influence feelings and behaviors or practices of individuals with their nutritional knowledge and practice during lactation, and to triangulate with the quantitative data. The investigator led the discussion using a focus group guide to direct the discussions and it was stopped after reaching a point of redundancy of information. There were two assistants with the investigator who took notes and observations during the discussion. In addition, a tape recorder was used to record the discussion to support the notes. The discussion was ceased when it reached saturation point.
Data were collected on socio-demographic and economic characteristics (such as age, religion, ethnicity, marital status, maternal education, occupational status, husband’s education, husband’s occupation, monthly income, family size), socio-cultural features (types of food culturally allowed/forbidden, food taboos, activities expected/forbidden), health service and obstetric history, nutritional knowledge, practices, and access to nutrition information.
The composite variables knowledge and practices of nutrition during lactation were measured from 14 and 10 items, respectively. Knowledge was categorized into “good knowledge” if respondents scored more than or equal to 20 out of 28 points and “poor knowledge” if respondents scored less than 20 out of 28 points. Similarly, the nutritional practices of lactating mothers were dichotomized as having “good practices” if they scored ≥7 out of 10 points and “poor practices” if they scored less than 7 out of 10 points.19,20
To assure the data quality, the data collection tool was pre-tested, and data collectors and supervisors were trained for two days. The questionnaire was pretested before the actual data collection days on 22 lactating mothers to check its clarity, reliability, consistency and to make the necessary modifications. Moreover, during data collection supervisors were responsible to check in the field how the data collectors were doing their task. The principal investigator also closely supervising the field activity on a daily basis.
Data Processing and Analysis
The data were checked, cleaned, and entered using Epi-info statistical software version 7.2 and exported to SPSS version 23 for analysis. The nutritional knowledge and practice questions were tested for using reliability analysis, the test comprised fourteen-item questions on nutrition knowledge and ten-item questions on nutritional practice which were found to be Cronbach’s alpha of 0.91 and 0.76, respectively; indicating good reliability.
The data initially were analyzed using bivariate analysis between the dependent variable (the nutritional practice of lactating mothers) and each of the factors potentially associated with the nutritional practice of mothers. All variables having p-value <0.3 in the bivariable analysis were further entered into the multivariable logistic regression model. Hence, the odds ratio with a 95% confidence level and the corresponding p-value was used to evaluate the association between independent variables with the outcome variables.
Qualitative data were analyzed manually using thematic content analysis where familiarization, coding, interpretation of the findings, and summarizing major themes from findings were done. In familiarization, a full-recorded audio transcription of each of the group discussions was done. The audio transcriptions were then supplemented with recorded notes taken during the interview as well as a summary of the events as they were observed. The main themes in the data were selected by writing short phrases, ideas, and concepts in the margin of the text. Themes were achieved by reading the transcripts in their entirety several times and grouping responses according to the questions they answered. Coding schemes were developed by a list of all themes, the main and sub-themes, then coded all themes and applies these codes to the whole set of data by written codes on the margin of transcripts. Interpretation of findings was done through data analyzed by data reduction, which was achieved by comparing and contrasting data and cutting and pasting similar quotes together, and the individual quotes, the relationship between the quotes, and the links between the data as a whole were seen. Finally, the results were triangulated with quantitative findings for discussion.
Results
Socio-Demographic Characteristics
A total of 425 lactating mothers, with a response rate of 97.0%, were included in the study. The age of the respondents ranged from 18 to 41 years with a mean age (±SD) of 28.92 ± 4.56 years. Among the respondents, 302 (71.1%) were in the age range of 25–34 years. Regarding ethnicity, a higher proportion of respondents were Amhara (384 (90.4%)) followed by Tigre (30 (7.1%)). About half of the respondents, 222 (52.2%) were housewives and again half of the respondents’ husbands, 216 (50.8%) were employed (Table 1).
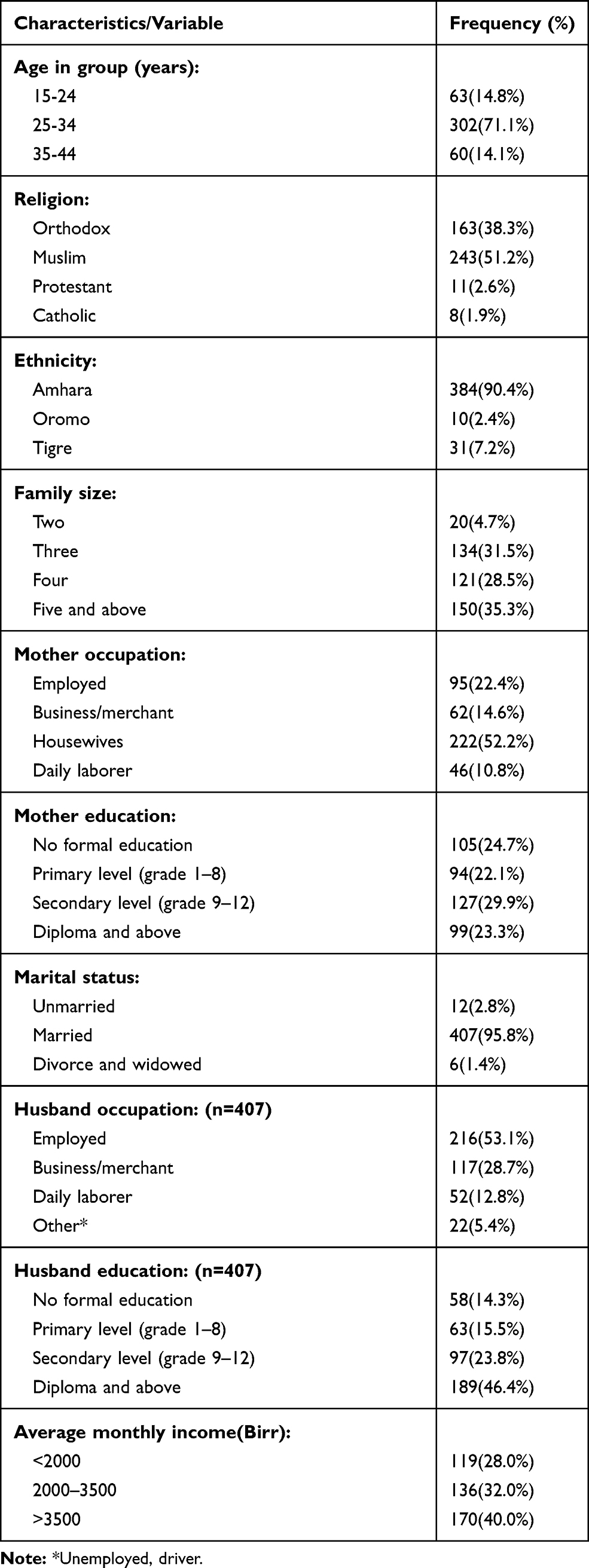 |
Table 1 Socio-Demographic Characteristics of Lactating Mothers, in Kombolcha Town, South Wollo Zone, Amhara Region, Ethiopia, December 2017 |
Health Service and Obstetric History
Regarding the last pregnancy, all 425 of the mothers reported that they had attended antenatal care; about three-quarters of them (310 (73.2%)) had four and above antenatal care visits. Among all respondents, 293 (68.9%) had one to two children and 26.8% of respondents had three to four children, respectively.
Source of Information and Socio-Cultural Characteristics
Regarding nutrition information, 391 (92.0%) of the mothers had got lactating related nutritional information from different sources, among those sources nearly two-thirds of mothers got the information from health workers (63.6%), health workers and mass media (8.9%) followed by from all sources (8.1%).
Mothers were asked if they had received family member encouragement or support on frequently taking foods and who had offered the encouragement. The majority of mothers (339 (79.8%)) received family encouragement and support, among those 118 (34%), 68 (20%) and 89 (26.2%) from husband, mother, and all family members, respectively. Mothers were asked if there were cultural-specific foods or fluids that a lactating mother should eat in their community. The majority of mothers (298 (70.1%)) reported that there were culture-specific foods in the community and among those respondents 204 (68.4%) mentioned that porridge and cereal soup is a specific and cultural food for mothers during lactation.
Out of the total respondents, two in every three mothers (297 (69.9%)) did not know the type of foods or fluids that are culturally forbidden. Nearly one-third of lactating mothers (128 (30.1)) listed that any alcohol-related drinks, raw vegetable and meat, and “Khat” are culturally forbidden (Table 2).
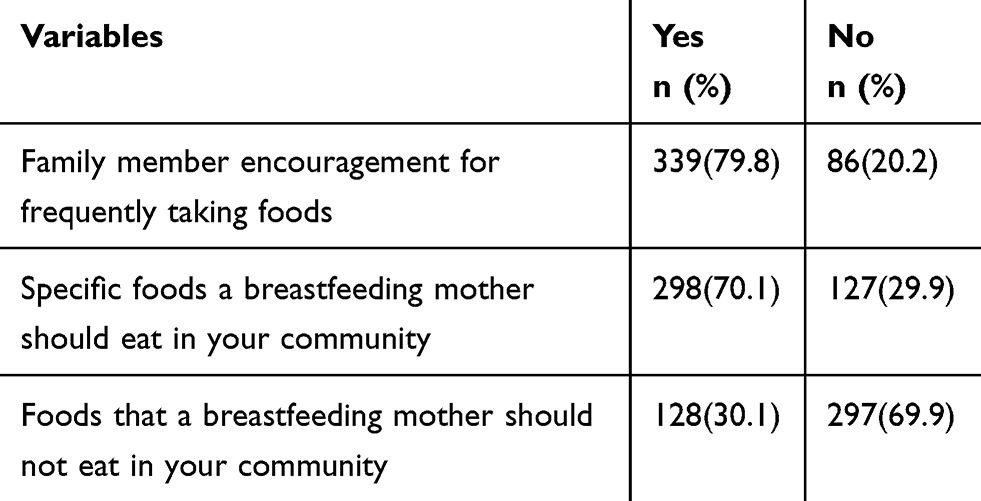 |
Table 2 Cultural Characteristics of Lactating Mothers, in Kombolcha Town, South Wollo Zone, Amhara Region, Ethiopia, December 2017 |
Nutritional Knowledge of Lactating Mothers
More than half of the respondents had a complete and correct answer to what food is (249 (58.6%)), a balanced diet is (243 (57.2%)), and components of a balanced diet are (215 (50.6%)). On the other hand, 150 (35%), 126 (29.6%), 116 (27.0%), and 267 (62.8%) did not know the importance of protein, carbohydrates, vitamins, and minerals for lactating mothers, respectively. Regarding sources of nutrients, 193 (45.4%), 213 (50.1%), 211 (49.6%), and 64 (15.1%) of mothers had complete correct answers to the sources of protein, carbohydrates, vitamins, and minerals, respectively. From the analysis of the nutrition knowledge questionnaire, responses to the questions about the sources and uses of minerals revealed a lack of knowledge about the nutrition concepts by more than half of the study group (259 (60.9%) and 267 (62.8%), respectively). Generally, the finding showed that 52.0% with 95% CI (47.1%, 57.6%) of the respondents were knowledgeable.
Nutritional Practice of Lactating Mothers
Regarding nutrition-related practices, only 56 (13.2%) of the lactating mothers followed a specific dietary regimen, a majority of mothers 358 (84.20%) used iodized salt properly at the end or after a cooked meal, 295 (69.40%) had the habit of taking fresh fruits like orange, lemon, mango, and juice.
Just less than two-thirds of respondents (260 (61.2%)) had a meal frequency of four and above per day. The rest (165 (38.8%)) of the respondents had two to three servings per day. More than two-thirds of mothers (295 (69.4%) and 299 (70.4%)) had the habits of eating snacks and more carbohydrates between meals, respectively. Even if the majority of mothers (410 (96.5%)) had a habit of drinking coffee or tea, only (61 (14.4%)) had the good practice of drinking two hours or more before or after a meal (Table 3).
 |
Table 3 Nutritional Related Practice of Lactating Mothers, in Kombolcha Town, South Wollo Zone, Amhara Region, Ethiopia, December 2017 |
In general, this study finding revealed that 122 (28.7%) with 95% CI (24.9%, 33.5%) of the respondents had good nutritional practice.
Factors Associated with Nutritional Practices of Lactating Mothers
Variables that showed statistical significance at bivariate logistic regression were mother’s education, mother’s occupation, husband’s education, husband’s occupation, number of children, culturally forbidden foods, nutritional knowledge, family size, nutrition information, income, and culturally specific foods.
In multiple logistic regression analyses, the mother’s occupation and nutritional knowledge of lactating mothers were found to have a significant association with the nutritional practices of lactating mothers. Concerning the mother’s occupation, employed lactating mothers were 6 times more likely to have good nutritional practice during lactating (AOR=6.0, 95% CI: 1.953, 18.485). Mothers with good nutritional knowledge were 3.1 times more likely to have good nutritional practice during lactation (AOR=3.12, 95% CI: 1.832, 5.318) (Table 4).
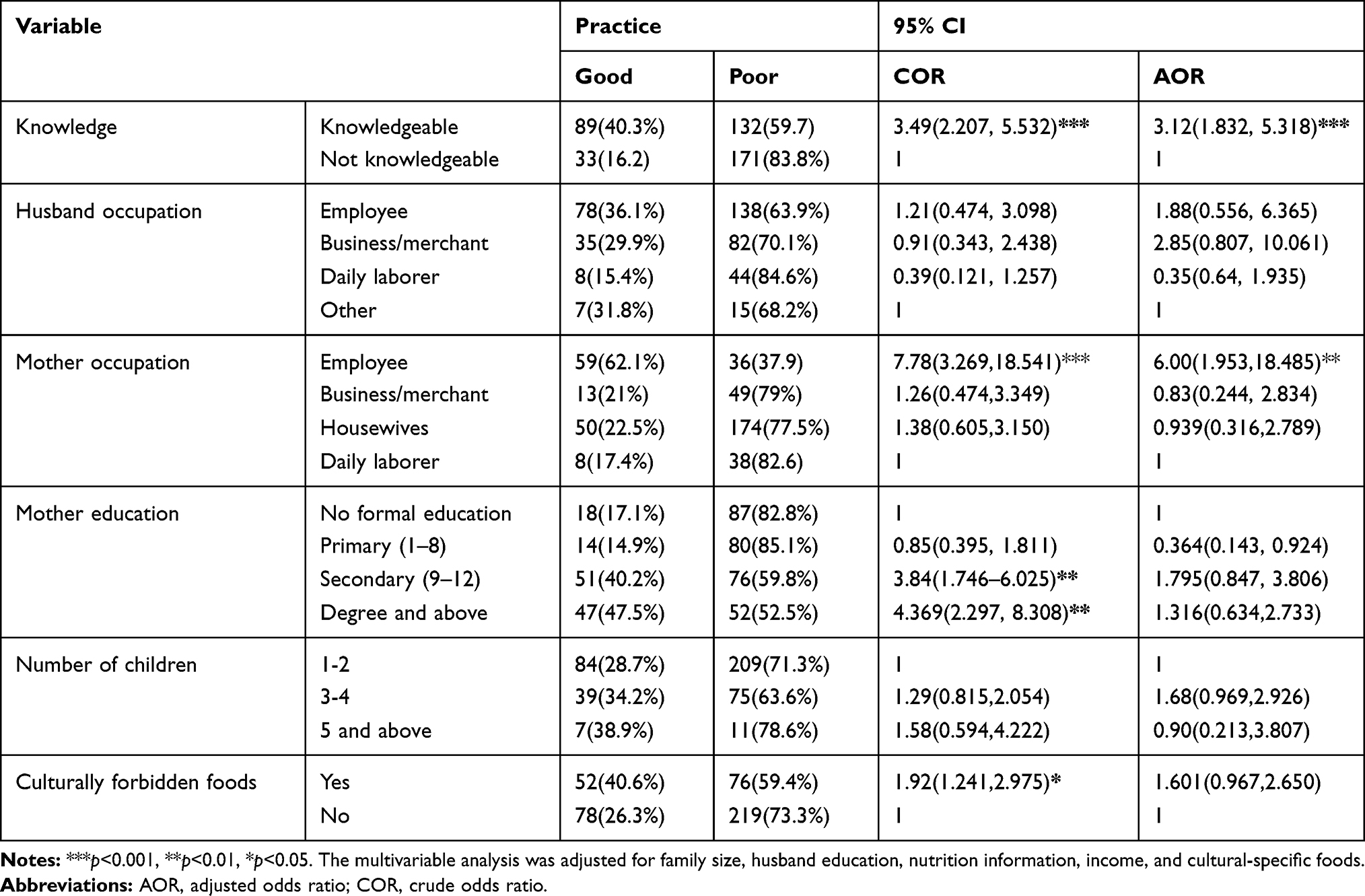 |
Table 4 Multivariable Logistic Regression of Nutritional Practice of Lactating Mothers, in Kombolcha Town, South Wollo Zone, Amhara Region, December 2017 |
Discussions
This study showed that the percentage of lactating mothers who had a good nutritional practice was 28.7%. This is lower than studies conducted in Swaziland (51%), Pakistan (65.5%) and Addis Ababa (34.5%).12,19,24 The findings of this study also showed that a higher proportion of lactating mothers (369 (86.8%)) do not follow a specific dietary regimen while 30.6% had poor practices on the intake of fresh fruits. This finding was relatively similar to reports from Baringo country, 75% and 16.4%, respectively.21 Regarding meal frequency of lactating mothers, 61.2% of them fed four and above times per day, which was consistent with the study conducted in Addis Ababa, Ethiopia which was 65%.19 The focus group discussants reported that the majority of mothers from all three groups agreed that they took meals three times a day. In contrast to the above, two of the mothers from the health workers’ group mentioned that there should be five meals in a day for lactating mothers, three main meals and two snacks. These additional meals are due to mothers' lost blood during delivery and they breastfeed their child.
According to this study, employed mothers were found to have a significant association with nutritional practice. The finding of the studies done in Belgium and Australia revealed that women’s being employed in a high-level type of occupation was the most important determinant to exhibit better dietary behavior/practice,9,10 which was similar to the current finding. The probable reason for this may be that employed mothers had a greater chance of getting nutritional information from mass media, school, partners, newspapers, and posters, which may lead them to have good food choices and practice as usual. Mothers’ employment increases household income, with consequent benefit to household nutrition in general and the woman’s nutritional knowledge in particular. Employment may increase women’s status and power and may bolster a woman’s preference to spend her earnings on health and nutrition practice. This study finding also stated that individuals with a higher nutritional knowledge of employed women in the study may be explained by more access to books and magazines as a source of information in the work area.25 The focus group discussion also supported this finding that all mothers from the health workers’ group who were employed had good knowledge about basic nutrients and adequate well-balanced diet, usually resulting in positive dietary practices. As reported from focus group discussions among the health workers’ group, all mothers mentioned all balanced diet components and sources of vitamin, protein, carbohydrate, mineral, fat, and fluids properly. A 37-year-old mother of the health workers’ group said that “there are also other sources of minerals and vitamins from supplements that are given during pregnancy and after delivery like iron, vitamin-A, and a multivitamin.”
In the present study, nutritional knowledge of mothers was statistically associated with nutritional practices. Mothers who were knowledgeable about nutrition were almost three times more likely to have good nutritional practices than mothers who were not knowledgeable. Similar studies done in Belgium and Addis Ababa showed that knowledge was a significantly associated factor in practice.9,19 This result was supported by the fact that good knowledge about basic nutrients and an adequate, well-balanced diet usually result in positive dietary practices, which are important determinants of optimum health from conception until death.25 Nutrition knowledge has been shown to play an important role in influencing healthy food habits/practices that ensure nutrient needs throughout the lifecycle.5,7
It might be due to mothers might know foods and fluids that culturally allowed for lactating mothers which had the nutritional value of scientific facts. Findings from focus group discussions revealed that culturally allowed foods and fluids were prepared and used during lactation were mentioned, which seemed, had scientific value for lactating mothers as follows, which supported this study found. Consumption of some foods was believed to have a positive effect on the health of lactating mothers.
In all the groups, all mothers mentioned foods like barley porridge, soup (called “Muk” or “Atmit” in Amharic), honey, butter, and meat that are specifically prepared ahead of time for lactating mothers. Two of the mothers from one focus group discussion reported that ale (locally named “bukri” or “keribo” in Amharic; unfermented fluid with low alcoholic nature) was one of the specific fluids prepared for lactating mothers.
Mothers from all the groups reported that prepared culturally specific foods were important as they had positive effects on the health of lactating mothers. Mothers in all groups mentioned that culturally prepared specific foods were used to increase blood production and to replace the blood loss during childbirth, to restore the body, to improve strength, to protect the child from diseases, and to help in maintaining the mother’s health and increase the quantity of breast milk production for the child.
Some limitations of this study include the social desirability bias and the lack of similar studies with this specific target population to make comparative discussion.
In addition, a qualitative study was carried out to supplement the findings of the quantitative data.
Conclusions and Recommendations
Lactating mothers had a low level of nutritional practice and knowledge. Furthermore, the most significant factors that affect the nutritional practice of lactating mothers were the mother’s occupation being employed and nutritional knowledge. Therefore, nutritional knowledge does influence the nutritional practices of lactating mothers in the study area.
Adequate nutrition education and counseling about proper and balanced maternal nutrition should be provided at the community and facility level. Nutrition education should be provided to the community in different kebeles, health centers, health posts, and women’s organizations, particularly for lactating mothers concerning nutrition during breastfeeding in the study area.
One-to-one counseling/consultation approaches should be applied at the facility level to correct the nutritional knowledge and practices of lactating mothers, especially on the use of locally available low-cost alternative foods and to avoid undue food restrictions. Women's nutrition services should be included in maternal and child health quality improvement tools at the health institution level.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; EDHS, Ethiopia demographic and health survey; FAO, Food and Agriculture Organization; MCH, maternal and child health; NGO, non-governmental organization; PPS, population proportion size; SPSS, statistical package for social sciences; UNICEF, United Nations Children’s Fund; UNU, United Nation University; WHO, World Health Organization.
Ethical Standards Disclosure
Ethical clearance was obtained from the Ethical and Research Review Committee of the College of Medicine and Health Sciences of Wollo University, it was conducted following the Declaration of Helsinki. Written informed consent was obtained from the study subjects and confidentially of the information was also guaranteed.
Acknowledgment
We would like to thank Wollo University, College of Medicine and Health Science, Department of Public Health for giving us a chance to study and conduct this thesis.
We would like to acknowledge Kombolcha Town Health Office, the Health Institutions for their cooperation. Our special appreciation goes to data collectors, study participants, and supervisors. We are grateful to all our teachers and friends who helped us a lot throughout this research work. We also extend our special thanks to Mr. Sisay Eshetie for his valuable support on manuscript revision and edition.
Author Contributions
DG: contributed to the conception, design, data collection, analysis, interpretation of data, drafting the manuscript, give final approval of the version to be published and agreed to be accountable for all aspects of the work. EG: contributed to the design, data collection, analysis, interpretation of data, revising the manuscript, give final approval of the version to be published and agreed to be accountable for all aspects of the work. TC: contributed to the conception, design, data collection, analysis, interpretation of data, drafting the manuscript, give final approval of the version to be published and agreed to be accountable for all aspects of the work. WM: contributed to the design, data collection, analysis, interpretation of data, revising the manuscript, give final approval of the version to be published and agreed to be accountable for all aspects of the work. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
Self-sponsored research.
Disclosure
The authors declared that they have no conflict of interest.
References
1. Nutrition & Integrated Programming. Maternal Nutrition & Maternal and Child Health. Available from: https://www.care.org/sites/default/files/documents/MH-2013-Maternal-Nutrition-Maternal-and-Child-Health.pdf. Accessed February 17, 2020.
2. National Academy of Sciences/Institute of Medicine and Food and Nutrition Board. A Report of the Subcommittee on Nutrition During Lactation on Nutritional Status During Pregnancy and Lactation; 1996.
3. N, Durham H, Sherry C. Nutrient Intakes from Food of Lactating Women Do Not Meet Many Dietary Recommendations Important for Infant Development and Maternal Health. Food and Nutrition Sciences. 2014;5:1644-1651.
4. Ministry of Public Health and Sanitation-Republic of Kenya . National Nutrition Action Plan 2012-2017. Available from: https://scalingupnutrition.org/wp-content/uploads/2013/10/Kenya-National-Nutrition-Action-Plan-2012-2017-final.pdf. Accessed February 17, 2020.
5. Worsley A. Nutrition knowledge and food consumption: can knowledge change food behavior. Asia Pac J Clin Nutr. 2002;11:579–585. doi:10.1046/j.1440-6047.11.supp3.7.x
6. Eckhart CL, Suchindran C, Gordon-Larsen P, Adair LS. The association between diet and height in the post-infancy period changes with age and socioeconomic status in Filipino youths. J Nutr. 2005;135(9):2192–2198. doi:10.1093/jn/135.9.2192
7. Food and Nutrition Research Institute. Philippine Facts and Figures 2003. Manila, Philippines: Department of Science and Technology; 2008. Available from: http://www.fnri.dost.gov.ph/index.php?option=content&task=view&id=1130.
8. Hasan MN, Khan MNI, Sultan MZ. The pregnant and lactating mother’s KAP (knowledge, attitude and practice) and nutritional care during antenatal and postnatal period in Ukhia, Cox’s Bazar, Bangladesh. J Sci Res. 2015;8.
9. Hendrie GA, Coveney J, Cox D.Exploring nutrition knowledge and the demographic variation in knowledge levels in an Australian community sample. Public Health Nutr.2008;11:1365–1371. doi:10.1017/S1368980008003042
10. De Vriendt T, Matthys C, Verbeke W, Pynaert I, De Henauw S. Determinants of nutrition knowledge in young and middle-aged Belgian women and the association with their dietary behavior. Appetite. 2009;52:788–792.
11. Daba G, Beyene F, Garoma W, Fekadu H. Assessment of nutritional practices of pregnant mothers on maternal nutrition and associated factors in GutoGidaWoreda, East Wollega Zone, Ethiopia. Star J. 2013;2(3):105–113.
12. Mahrnood S, Atifetal MF. Assessment of nutritional beliefs and practices in pregnant and lactating mothers in an urban and rural area of Pakistan. J Pak Med Assoc. 1997;47(2):60–62.
13. Milla G, Flores A, Umaña E, Mayes I, Rosenthal J. Postpartum women in the Honduran health system: folic acid knowledge, attitudes, and practices. Pan Am J Public Health. 2007;22(5):340–347. doi:10.1590/S1020-49892007001000007
14. Idowu O, Mariana C, Dopu S. Anaemia in pregnancy: a survey of pregnant women in Abeokuta, Nigeria. Afr Health Sci. 2007;5(4):295–299.
15. Ethiopia and ORC Macro. Ethiopia demography and health survey, Addis Ababa, Ethiopia. Summary and Statistical Report of the 2007 Population and Housing Census; 2006.
16. Health Organization. 10 facts about women‘s health. Geneva: WorldHealth Organisation; 2011. Available from https://www.who.int/features/factfiles/women/en/. Accessed March 17, 2011.
17. Federal Ministry of Health-Ethiopia. National Health Promotion and Communication Strategy 2016 – 2020. Federal Ministry of Health Ethiopia; 2016.
18. Minwuyelet F, Ategbo EA. New National Nutrition Programme II envisions an Ethiopia free of malnutrition [press release]. UNICEF Ethiopia; 2016 [December 20]. Available from: https://unicefethiopia.org/2016/12/20/new-national-nutrition-programme-ii-envisions-an-ethiopia-free-of-malnutrition/. Accessed February 17, 2020.
19. Mikias A Assessment of Knowledge, Attitudes, and Practices Regarding Maternal Nutrition among Pregnant Women Attending Antenatal Care Clinics in Public Hospitals in Addis Ababa, Ethiopia [Doctoral dissertation], Addis Ababa University; 2015, 34.
20. Yvette FM, Peter G. Guidelines for Assessing Nutrition-Related Assessing Nutrition-Related Knowledge, Attitudes and Practices. Rome: FAO of United Nations; 2014.
21. HK, Kang S, Cho SH, Ju Yj, Faye D. Factors influencing nutritional practices among mothers in Dakar, Senegal. PLOS ONE. 2019;14(2):e0211787.
22. Hundera TD, Gemede HF, Wirtu D. Nutrition knowledge and determinant factors among lactating mothers, in Nekemt referral hospital and health centers, East wollega Ethiopia. Food Sci Qual Manag. 2015;38:68.
23. Anita N. Nutrient Intake and Nutrition Knowledge of Lactating Women (0-6 months postpartum) in a Low Socio-Economic Area in Nairobi, Kenya [Doctoral dissertation], University of Pretoria; December 2010.
24. Masuku SKS, Shu-Jan J. Lan nutritional knowledge, attitude, and practices among pregnant and lactating women living with HIV in the Manzini Region of Swaziland. J Health Popul Nutr. 2014;32(2):261–269.
25. Painter J, Rah J, Lee Y. Comparison of international food guide pictorial representation. J Am Diet Assoc. 2003;102:483–489. doi:10.1016/S0002-8223(02)90113-6
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.