")
Back to Journals » Patient Preference and Adherence » Volume 14
The Experiences of Multiple Sclerosis Patients’ Family Caregivers at the First Hospitalization of Their Patients: A Qualitative Study
Authors Tehranineshat B , Yektatalab S, Momennasab M, Bijani M , Mohammadi F
Received 10 April 2020
Accepted for publication 23 June 2020
Published 13 July 2020 Volume 2020:14 Pages 1159—1172
DOI https://doi.org/10.2147/PPA.S257746
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Banafsheh Tehranineshat,1 Shahrzad Yektatalab,2 Marzieh Momennasab,1 Mostafa Bijani,3 Fateme Mohammadi4
1Community-Based Psychiatric Care Research Center, Department of Nursing, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran; 2Community-Based Psychiatric Care Research Center, Department of Mental Health and Psychiatric Nursing, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran; 3Department of Medical Surgical Nursing, Fasa University of Medical Sciences, Fasa, Iran; 4Chronic Diseases (Home Care) Research Center, Autism Spectrum Disorders Research Center, School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran
Correspondence: Shahrzad Yektatalab
Community-Based Psychiatric Care Research Center,Department of Mental Health and Psychiatric Nursing,School of Nursing and Midwifery, Shiraz University of Medical Sciences, Zand St., Nemazee Sq.,7193613119, Shiraz, Iran
Email [email protected]
Background and Aim: Being diagnosed with multiple sclerosis is usually accompanied by emotional trauma for patients and their families. The chronic, progressive, and unpredictable nature of the disease spells the patients’ long-term need for care from their families. As soon as a diagnosis is made, family caregivers are faced with many challenges. The present study aims to identify family caregivers’ experiences at the first hospitalization of their patients.
Materials and Methods: The present study is a work of qualitative research and uses the conventional content analysis approach. It lasted from July 2019 to March 2020. The subjects were selected via purposeful sampling. To collect data, the researchers conducted in-depth, semi-structured interviews with 18 family caregivers of patients with multiple sclerosis. The collected data were analyzed using MAXQDA 2007.
Results: Analysis of the data yielded three themes: peaceful environment, need for continuing full support, and religion-based coping strategies.
Conclusion: The findings of the present study can be used to develop support programs that address family caregivers’ problems and needs to assist them in accepting and coping with the conditions of their patients, thereby increasing the quality of care provided to patients with multiple sclerosis.
Keywords: family caregivers, hospitalization, multiple sclerosis, patients
Introduction
Multiple sclerosis (MS) is a prevalent chronic neuron-damaging disease that often affects young adults and is the most common cause of non-traumatic disablement in this age group.1 Currently, over 1 million people aged between 17 and 65 years are suffering from the disease worldwide. Nearly 400,000 people in the US and 60,000 people in Iran have multiple sclerosis. In most cases, being diagnosed with MS is accompanied by emotional trauma, which leads to the denial of the disease.4 The complex nature of MS and various psychological, emotional, physical, familial, and social issues complicate the acceptance of the disease for patients and, thus, lengthen the adaptation period.5
Fear is the most important feeling created by the knowledge of having the disease and can, eventually, have a negative impact on the quality of life patients and their family members.4 The fact that MS is a chronic, progressive, and unpredictable disease means that the patients need long-term care.1 Most patients and their families have their first realization of the terrifying aspect of this chronic disease at hospitalization as it does not seem that hospital care is part of the treatment plan for patients with chronic diseases.6,7
As soon as an individual is diagnosed with a chronic disease, he/she is potentially subject to stigmatization due to concern over the negative attitude of the society. The cognitive and temperamental disorders and physical disabilities that are associated with MS can lead to stigmatization.8 Perception of stigmatization in patients with a chronic disease may undermine their self-esteem, diminish their understanding of social support, damage their self-efficacy, increase the risk of depression and anxiety, and create feelings of social conflict and psychological distress.9,10 These stressful factors can, in turn, weaken the patients’ immunity system and discourage them from performing positive self-care behaviors, including seeing a doctor on a regular basis and accepting treatment.9
The family caregivers of MS patients also are subject to varying degrees of social pressure and stigmatization. Feelings of shame, fear of being despised by others, fear of being ostracized by the other members of their families, and trying to hide their patients’ condition in order to avoid stigmatization have been reported as examples of the experiences of family caregivers. Public stigmatization has an impact on the identity of patients’ family members as, despite being healthy, they experience varying degrees of social discrimination, ostracization, and negligence depending on the severity of the condition of their MS patients. Thus, the family caregivers of MS patients are not willing to reveal the condition of their patients.10 As long as the symptoms of MS may not be perceptible to others, especially in the early stages of relapsing remitting MS, the patients and their family caregivers try to hide the existence of the disease. Such efforts may avert discrimination, but they are stressful and have adverse effects on the physical and psychological health of the patients and their family caregivers and limit their chances of receiving social support.9
MS patients need the support of their families to cope with the crisis following their diagnosis. The illness of one family member can influence the life of the whole family and make them worry about the other members. Families are expected to be in the front line of support for patients;11 however, in the hospital environment, most family caregivers feel abandoned in the process of providing care to their patients and their prolonged involvement in care can result in the dissatisfaction of the patients and their families with hospital care.12
In addition, family caregivers expect the medical personnel to prepare them for caring for their patients after discharge.13 Yet, many family caregivers report that they lack the needed knowledge and skill for providing care to their patients. Family caregivers’ lack of confidence and preparation presents them with a variety of challenges.14 It is a responsibility of the healthcare system to support family caregivers and satisfy their needs with regard to caring for their patients. In critical conditions, healthcare stresses caring for patients, while the needs of their family caregivers should be considered too.15,16
Evidence shows that providing care to MS patients affects the physical, mental, social, and financial status and, in general, the quality of life of their non-professional caregivers.17,18 The extent of perceived care burden depends on the severity of the patients’ symptoms and the length of their disease. Extended caring hours per day, the limited ability of the caregivers to perform their daily activities, increased anxiety, and low salary can increase the care burden of care providers.19 Demographic characteristics also can determine the care burden. Younger caregivers, male caregivers, and married caregivers experience heavier care burden.19,20 In addition, the cultural structure of a society has an impact on care burden. In some societies, though male MS patients receive care from their wives, men whose wives have MS are not willing to accept the responsibility of caring for their spouses and the fear that their wives cannot have babies or perform household tasks make them divorce their wives, which aggravates the care burden of female patients and their families.20,21 Social support of the family caregivers of MS patients can reduce their care burden and improve their living standards, thus the need for providing these caregivers with emotional, physical, and financial support.21,22
Studies show that the support of family caregivers and attention to their needs have been neglected.23 Family caregivers suffer from restricted social interactions, financial issues, and uncertainty about the future.24 In the context of Iranian healthcare, family members are an important source of support in caring for inpatients: they attend to their patients’ personal hygiene and nutrition, obtain their medication, and take their specimens to laboratories outside the hospital.25 Although it is vital that family caregivers be supported, they have inadequate interactions with healthcare team members and are not provided with the information they need for their safety and welfare.23,26
Emphasis on identifying the clinical challenges of caring for MS patients has resulted in a change from patient-centered care to a combination of patient-centered care and family caregiver-centered care in recognition of the significant role of family caregivers in caring for MS patients.14 In Iran, nurses provide care to MS patients in hospitals only and there are not any social centers which provide services to the patients and their families. For a final diagnosis and to receive specialized care, all MS patients in Iran (even after having been to private doctors’ offices or clinics) are hospitalized in state hospitals. Due to lack of space, equipment, and workforce in some of these hospitals, MS patients’ family caregivers experience additional stress upon the first hospitalization of their patients. Thus, it is essential that any care-related issues be identified and addressed at the first time of hospitalization and diagnosis. High-quality care cannot happen unless healthcare providers consider the rich experiences of family caregivers at the time of the first hospitalization of their patients. Without an understanding of family caregivers’ feelings and challenges when their patients are hospitalized, it is not possible to establish an effective relationship with them and give their patients comprehensive care. Accordingly, the present study relies on a qualitative approach for an in-depth description of the family-caregivers’ experiences. An understanding of the experiences of MS patients’ family caregivers at the first hospitalization of their patients can lead to a better comprehension of the caregivers’ needs and, consequently, an improvement in the quality of care and higher satisfaction of the patients and their family caregivers. Thus, the present study aims to determine the experiences of MS patients’ family caregivers the first time their patients are hospitalized.
Materials and Methods
The present qualitative study uses the conventional content analysis method and lasted from July 2019 to March 2020. Qualitative research is a systematic mental process that aims to describe human concepts and experiences.27 Since the family caregivers’ perception of the first hospitalization of their patients was a mental experience, the present study used a qualitative, exploratory-descriptive design. The present study relies on purposeful sampling which is a conscious selection of subjects for study by the researcher. In this type of sampling, the researcher selects participants who have first-hand experience and rich knowledge of the phenomenon under study.27,28 The population which is especially familiar with the phenomenon under study is called the target population. Thus, in this type of research, the researcher is after subjects who can provide information about a particular topic. The logic and strength of this manner of selection lies in the fact that purposefully selected subjects can provide the most information regarding the research question.29 As the demographics table shows, a wide range of participants with varying educational levels were interviewed in the present study.28 The research environment was all the rehabilitation and neurology units of three major university hospitals affiliated with Shiraz University of Medical Sciences located in the south-east of Iran. The inclusion criteria were: being the main caregiver and aged between 18 and 60 years, being the main source of support for the patient, having the most physical and emotional connection with the patient, being able to interact properly with the patient and the healthcare team, being able to answer the interviewer’s questions clearly, and having a good command of Farsi.
To obtain a better understanding of the experiences of multiple sclerosis patients’ family caregivers at the first hospitalization of their patients, the first author consulted the supervisors at the rehabilitation and neurology units of the hospitals and selected those family caregivers who were better at interacting and could provide more information for the first few interviews. Also, the selected participants represented a wide range of caregivers in terms of age, gender, education, and social and financial status. After the well-informed family caregivers have been identified and contacted, they were provided with information about the objectives and methods of the study. After the researcher and participants have agreed on a suitable time and place (in terms of privacy and noise), the interviews were conducted and recorded. The collection of data was continued to the point of data saturation.
Data were collected through unstructured, in-depth interviews. Each interview began with the following general questions: “Can you tell us about your experience of the first time your patient was hospitalized?” and “What did you do on the first day of your patient’s hospitalization?”. And gradually more specific questions were raised, including “What were your feelings the first time your patient was hospitalized?”. The interviewer (first author) used exploratory questions, eg, “Can you explain further?” to collect more in-depth data. At the end of each interview, the participants were asked to talk about anything else that was important to them but not touched upon in the course of the interview. Each interview lasted from 40 to 120 minutes.
The present study uses qualitative content analysis which is a research method for mental interpretation of the content of textual data through systematic categorizing, coding, and theme making or designing known paradigms.30,31 According to Hsieh and Shannon, in this method, researchers should avoid all preconceptions and try to describe the phenomenon under study based on the collected data.30,32 As data were being collected, they were analyzed using the approach to conventional content analysis recommended by Graneheim and Lundman (2004): transcribing every interview as soon as it is finished, reading the transcripts to achieve a general understanding of the content, determining the semantic units and initial codes, classifying initial codes into broader categories based on their similarities and differences, and identifying the implicit content of the data.33
In order to accurately describe the participants’ viewpoints, the researchers tried to ignore their own knowledge, beliefs, values, and experiences. In other words, the participants’ responses were not prejudged and were considered as they were. While collecting and analyzing the data, the researchers applied bracketing. Bracketing is a method commonly used in qualitative research to mitigate the potentially harmful effects of preconceptions that may cause bias in research.33 All the interviews were conducted and recorded by the first author. Immediately after each interview, the first author transcribed it and determined the semantic units and codes. Then, the second author reviewed the transcripts and verified the semantic units and open codes. All possible inconsistencies were discussed and resolved in a meeting attended by all the members of the research team. Also, the themes were extracted in several joint meetings after deep contemplation and comparison of the categories. The trustworthiness of the data was tested using Guba and Lincoln’s criteria.34 Credibility was achieved through prolonged engagement, member checking, peer debriefing, maximum variation sampling, and negative case analysis. To test the dependability and confirmability of the data, the researchers had a panel of experts to examine the accuracy of the process of transcription and verify the transcripts and the extracted themes and categories. Transferability was achieved through thorough and accurate descriptions of the subject under study and the participants’ characteristics.
Results
In the present study, 18 multiple sclerosis patients’ family caregivers—13 females and 5 males—with the average age of 43±10.19 were interviewed. Table 1 shows the participants’ demographics. Analyses of the caregivers’ experiences at the first hospitalization of their patients yielded three main themes and ten categories (Table 2).
 |
Table 1 The Demographic Characteristics of the Participants |
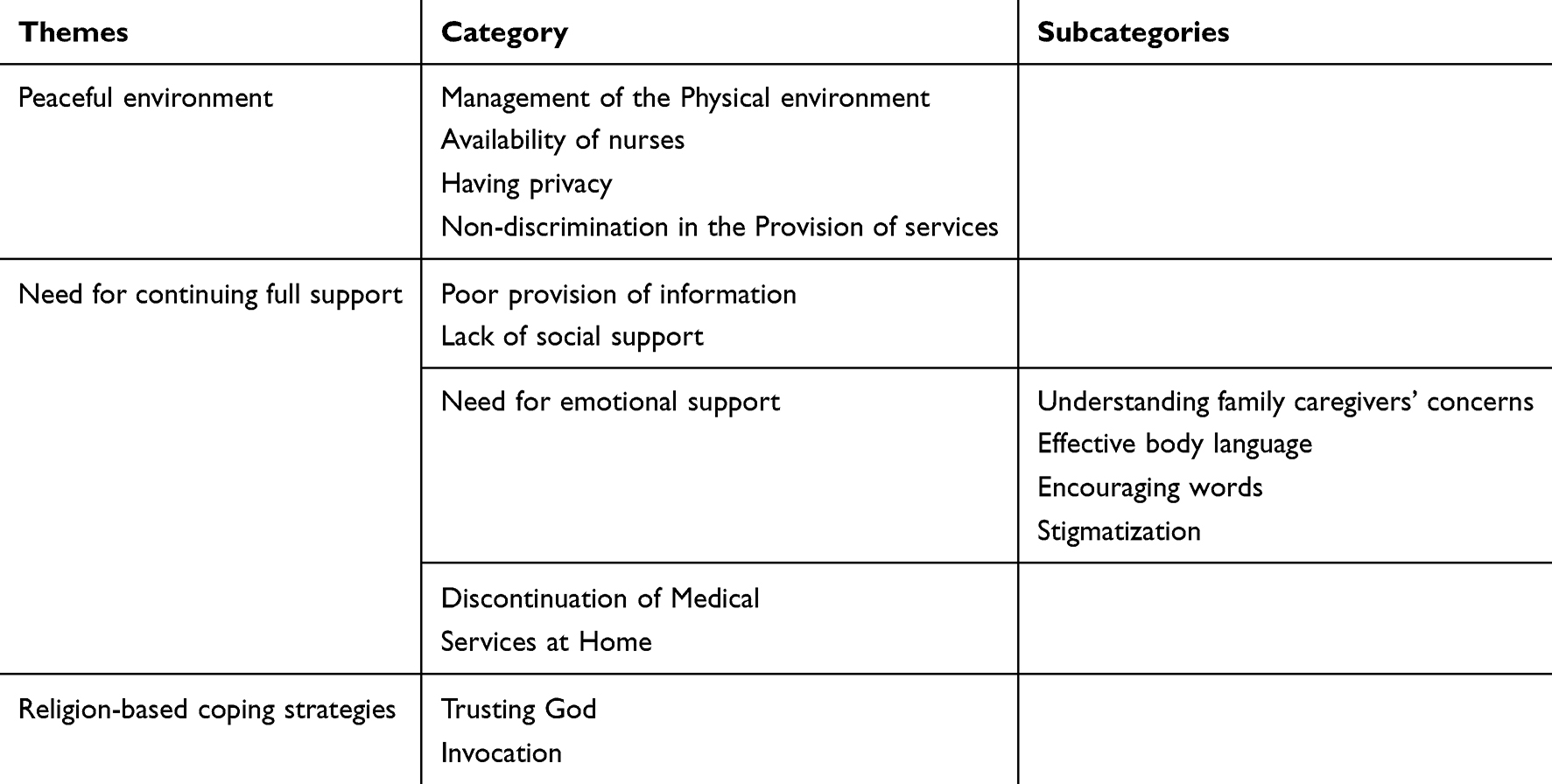 |
Table 2 The Themes, Categories and Sub-Categories of This Study |
Peaceful Environment
This theme is comprised of the secondary themes of management of the physical environment, having privacy, availability of nurses, and non-discrimination in the provision of services. From the perspective of the family caregivers, a comfortable and safe environment in the hospital is vital to their having peace and, in the absence of such an environment for any reason, they will experience more distress and anxiety.
Management of the Physical Environment
Some of the participants referred to loud noise as a stressful environmental factor that interferes with their peace and comfort. Lack of bathrooms for family caregivers was another issue that bothered the patients’ companions. A peaceful, clean, and quiet hospital environment is influential in reducing the anxiety and fear which family caregivers experience upon the first hospitalization of their patients. According to one of the participants:
It’s really important for the family caregivers of MS patients to be in a quiet and clean environment. Especially at night, they should have access to a comfortable place for rest so they can refresh and be ready to attend to their patients’ needs again … P3.
Availability of Nurses
The participants’ experiences show that family caregivers constantly need nurses to be present when they are caring for their patients—in other words, they demand the supervision of professional caregivers to be assured that they are doing things right.
Whenever I called them [the nurses], they responded; whenever I called them, they did what my child needed … P5.
The experiences of some other of the participants showed that some nurses were not cooperative, did not attend to the patients’ needs, eg, connecting drips and administering medicine, on a timely basis, and ignored the family caregivers’ requests for the timely performance of a task:
I had to ask them ten times before they finally came and replaced a drip, like it is not their job … P2.
Another family caregiver stated that:
A patient who is on corticosteroids must have his blood pressure checked regularly. I had to keep reminding the nurse that she should check his blood pressure …. P11.
Having Privacy
Having privacy was one of the factors that the family caregivers felt very strongly about. The participants’ experiences showed that a variety of factors could disrupt their privacy in the hospital environment, including the entrance of strangers into their patients’ rooms, people entering their patients’ rooms without knocking, and the opposite-gender companions of other patients. In the present study, privacy refers to visual and audio privacy and confidentiality. Many of the family caregivers expressed discontent at having had to see disturbing scenes, having been forced to witness certain events, having seen the performance of medical procedures, and hearing other patient companions’ speaking loudly.
Early in the morning, the nurse suddenly opens the door without knocking and opens the curtains—this shocks me and my daughter …. P9.
According to another family caregiver,
Loud noises, the sound of other patients’ moaning, the clamor in the unit, seeing the defibrillation of a patient next to me, all these added to the mental stress I was suffering from already for the sickness of my child—I needed a quiet and private place at that time …. P15.
The participants’ experiences showed that the healthcare teams treated the information of their patients as confidential:
My daughter’s in-laws went to her doctor to ask what was wrong with my daughter, why she was in the hospital, and if she could have a baby or not, but her doctor refused to give them any information … P10.
Non-Discrimination in the Provision of Services
Family caregivers should be treated impartially, free of any ethnic or racial prejudices. Favoritism on the part of healthcare teams in the provision of hospital facilities is an example of injustice which disrupts family caregivers’ peace:
In this room, there was a patient who knew one of the staff members. She wasn’t happy with the air conditioning of the room and they immediately changed her room. Whatever she wanted, she got it. I’ve told them repeatedly that this room is too cold and they should take my daughter to a different room or fix the air conditioner, but nothing has been done for us … P16.
Need for Continuing Full Support
This theme is comprised of the following categories: poor provision of information, lack of social support, need for emotional support, and discontinuation of medical services at home.
Poor Provision of Information
Nurses and doctors can support family caregivers by giving them information about nearby drugstores, laboratories, and accommodations (for the family caregivers of patients from other towns), in addition to necessary information about the nature of the illness, treatment plans, the side effects of medication, and how to care for a patient with multiple sclerosis. By providing MS patients’ family caregivers with information, doctors and nurses enable them to understand their patients’ conditions better and experience less tension.
Many of the participants admitted that, because they were not familiar with the nature of multiple sclerosis at the time of diagnosis, they had a wrong perception of the disorder which originated in the general negative understanding of MS. The participants also stated that since most of the doctors and nurses did not give them enough information about the nature of the illness, how it developed, the efficacy of the existing treatments, and the results of diagnostic tests, they had to rely on unofficial online sources to increase their knowledge of multiple sclerosis.
In the beginning, I didn’t have a realistic understanding of this disorder—like many others, I thought my daughter would stay blind forever, or would become paralyzed and die in a few months … P15.
Lack of Social Support
One of the issues referred to by many of the participants is the financial burden of treatment which most of them had experienced after their patients had been diagnosed with MS. The majority of the participants declared that the cost of medical treatment was high, and since they did not have full-coverage health insurance, they usually had to buy Iranian medication rather than its more expensive western counterpart though they believed that the latter was more effective. In addition, occasionally, due to lack of medication in their own towns, some of the family caregivers had to buy their patients’ medication from another town or city. They stated that the costs of laboratory tests were high and before taking certain medicines, their patients had to have some specialized laboratory tests which were costly.
You know, the foreign Rituxan costs 4 million tomans, so I had to buy its Iranian version which is 400 thousand tomans and is partly covered by insurance, and even that wasn’t easy to find …. P6.
They were also found to be under financial pressure from the collateral costs of treatment, including the purchase of dietary supplements, costs of hospitalization, and purchase of nutritious foods—the participants from lower social classes were visibly under more pressure.
“I can’t meet my son’s needs entirely, but my husband and I are skimping on our nutrition and recreation so we can take better care of our son.” P13.
The interviewed family caregivers also expressed discontent over inadequate support from the Iranian MS Association and lack of rehabilitation centers for MS patients.
The physiotherapy center for MS patients is very far from our home and the trip back and forth tires my child very much. What’s more, there are many visitors there and you have to wait a long time for your turn and they don’t have enough equipment, like pads and elastic bands … P12.
Need for Emotional Support
Most of the participants declared that the appearance of their patients’ symptoms had been sudden and they were shocked to learn that their patients had MS Some of the caregivers referred to the first hospitalization of their patients as a horrifying time. This is the time when family caregivers need the emotional support of healthcare teams and their relatives the most. From the family caregivers’ perspective, emotional support is provided through others’ understanding of their family concerns, effective body language, encouraging words, and Stigmatization.
Many of the participants mentioned that the psychological pressure which they experienced at the first hospitalization of their patients was too much and that they needed attention, sympathy, and empathy from the healthcare team. They were willing to talk with a person about their concerns and have a chance to alleviate their emotional stress.
I was so worried about the condition of my child. At that time, I needed them to understand my problems and concern, be kind to me, and try to imagine how I felt … P13.
Among the major concerns of family, caregivers are not having a clear picture of their role and responsibilities and being preoccupied with what will happen in the future. The participants were found to be psychologically and emotionally disturbed by these concerns. Some of the participants mentioned that they were worried about the occupation, education, and marriage of their children in the future and expected the professional caregivers to attend to their concerns over these matters. What follows exemplifies this apprehension:
“I’m constantly wondering how this will turn out: will she get better or not? Can she get married or not? … P17.
The recurring nature of MS and lack of a definite cure for it subject the patients’ family caregivers to feelings of instability and uncertainty about the future.
“I’m always wondering if my daughter will get well or if her kids will lose her. Is she going to be cured or not? … P5.
According to the participants, non-verbal communication is an integral part of treatment and care and conveys the feelings and attitudes of healthcare teams toward patients. Examples of supportive behaviors that the participants expected from doctors and nurses were: behaving kindly, listening well, making eye contact, speaking clearly, and showing respect. They believed that healthcare teams’ respectful behavior paves the way for building trust and facilitates the recovery process.
Some of these nurses don’t look at you when you ask them a question—they don’t make any eye contact … P7.
Another participant remarked that:
When the medical personnel enter the room with a smile and address us politely and softly, we can communicate with them more easily … P10.
Family caregivers are in a stressful situation; especially when their patients are hospitalized for the first time, they experience high levels of anxiety which can adversely affect the process of providing care to their patients. Patients’ families hope to hear encouraging words from healthcare teams. Healthcare teams’ attempts at raising the spirits of patients’ families can effectively reduce their anxiety when their patients are hospitalized.
When I was trying to give hope to my child, my relatives, and the healthcare team would give examples of people with a similar disorder who had recovered to make me feel better … P16.
Some of the participants stated that multiple sclerosis severely harms the functioning of the patients and their family members and affects their social relations. Therefore, their relatives and healthcare teams should avoid pitying behaviors and Stigmatization.
Unfortunately, some friends and relatives didn’t help us; they only kept saying poor thing … P6.
The participants were also dissatisfied with the inappropriate behaviors of the society towards MS patients, which stem from their unfamiliarity with the disease, and the poor awareness-raising campaigns of the media. According to one of the participants:
The name of this disease is still mysterious to many people. They are afraid of its very name. They think it’s contagious; they avoid the patients who have it and say that someone they knew had this disease and died from it. People’s unawareness about MS makes them think it is contagious and that they should steer clear of the patients and avoid interacting with them … P18.
According to another participant:
“People treat us differently. They mistake MS with AIDS. They keep us and our patients at bay. Some people even avoid talking to us for a few minutes … P8.
Another participant mentioned that:
Some people have a negative view of MS. They don’t know what it is. Some say it’s contagious, or incurable, or is fatal … P12.
Many of the family caregivers who were interviewed in the present study stated that the process of providing care to their patients lacked consistency. They mentioned that professional care was given exclusively in the hospital and the caregivers’ follow-up measures and instructions for the family caregivers to follow were inadequate. According to them, after their patients’ discharge, all the burden of providing care lies with family caregivers who do not have professional competency; thus, professional caregivers must consider family caregivers’ needs and continue guiding them in the performance of their caregiving tasks at home. Family caregivers’ lack of preparation will cause them to give care on a trial and error, rather than a scientific, basis, which can have consequences for their patients.
When my sister was first hospitalized, I had no idea what to do for a patient who is paralyzed in her legs … as long as my sister was in the hospital, things were fine, but at home, the doctor or nurses didn’t come to give her follow-up care and we didn’t know much about her illness, so my sister’s condition got worse … P4.
From the participants’ perspective, consistency is the most import part of the treatment for MS patients. Continuing quality care is possible only through easy access to professional care at any time of the day, even on holidays. Access to an information source that answers the questions of the patients and their families is essential to continuation of care at home.
Patients and their family members should be provided with a phone number so that there is always someone to answer their questions to avoid possible complications … P18.
Religion-Based Coping Strategies
The participants declared that in the hard times of having their patients hospitalized for the first time, their religious beliefs became more important to them than ever before and helped them accept the situation and tolerate the difficulties. This theme is comprised of the categories of trusting God and invocation.
Trusting God
Having belief in God and His wisdom and will in everything which happens in the universe enables family caregivers to place their trust in God and adapt themselves to their patients’ conditions more easily:
In that situation, I trusted God’s will and thought maybe God wanted to test me through my son … P3.
Invocation
Patients’ families and relatives invoke God and the imams for the healing of their patients and the power to bear the hardship.
When my daughter was first hospitalized, I was always holding a rosary … I prayed nonstop and asked my relatives too to pray for my child … P10.
Discussion
The findings of the present study show that, when their patients are hospitalized for the first time, MS patients’ family caregivers consider a peaceful environment, continuing full support, and religion to be their priorities. A clean and well-equipped environment in the hospital, respect for the privacy of patients and their family caregivers, and impartial giving of care and other services can relax family caregivers in the hospital environment. Absence of the above-mentioned conditions will add to the stress and anxiety of family caregivers.
The results of a study show that a stressful hospital environment and continuous distress have a negative impact on the competency of MS patients’ family caregivers and cause them internal tension.23 Some of the interviewed family caregivers in another study mentioned that the psychological pressure of caring for an MS patient was very much and that they expected a more relaxing hospital environment.3,35 Patients expect that their family caregivers and other companions to be at ease and have access to the equipment and facilities which they need for their comfort. In Iran, family caregivers play an important role in medical centers as they are the ones who provide the medication and equipment which are not available in hospitals and are responsible for the every-day care of their patients.25 According to another study, though patients’ companions attend to patients’ basic needs, their comfort is often neglected in hospitals.25 According to one study, the parents of children with cancer experience discomfort during their children’s hospital stay due to lack of accommodations and facilities. Though these caregivers were dissatisfied with the conditions in state hospitals, they selected them over private hospitals due to the high costs of medical care, chemotherapy, and specialized cancer care.37 Disrespect for the privacy of patients and their family caregivers will undermine their self-esteem.25 The results of a study show that patients’ access to healthcare is not equitable.38 Many studies report that showing respect for the privacy of patients and their families, providing care without contempt,39 and avoiding discrimination are indicative of healthcare teams’ respect for human dignity.40 Family caregivers care about their comfort and psychological security as well as their patients in clinical environments and expect healthcare teams to deal with any events which disrupt their comfort and privacy during their stay.
In the present study, another theme extracted from the data is family caregivers’ need for continuing full support. The participants’ responses showed that they had experienced a need for information, lack of social support, and need for emotional support at the first hospitalization of their patients. They were also dissatisfied with the discontinuation of healthcare when their patients were discharged. Similarly, a study reports that, due to a lack of information and the society’s negative perception of MS, family caregivers have a wrong understanding of the illness. Moreover, to avoid being pitied, they hide their patients’ condition and care for them on a trial and error basis in the absence of any practical instructions from a professional caregiver. They are also displeased with the inconsistency in the provision of healthcare and inadequate follow-up and instructions after their patients’ discharge.5
Preparing MS patients’ family caregivers by giving them information about their patients’ disorder and teaching them coping and problem-solving strategies can significantly improve their quality of life.24 Nurses’ regular contact with patients and their family caregivers gives them a good chance to identify their educational needs and provide information and instructions accordingly.41 A study reports family caregivers’ discontent at healthcare teams’ insufficient education for them about medication and the right ways of giving care. They are also unhappy with the high costs of treatment, inadequate social and state support, and lack of easy access to physiotherapy and rehabilitation centers. Family caregivers expect to receive sympathy, compassion, hope and reassurance. They also expect that medical personnel listen to them and make eye contact with them out of respect.35 One of the experiences of the caregivers of patients with cardiac diseases is uncertainty about their patients’ conditions which originates in their lack of knowledge about the disorders and medications, lack of access to reliable sources of information, healthcare teams’ failure to guide them, the unpredictable nature of the diseases, and stress in providing care.42 Another study reports that the family caregivers of patients with cardiac diseases experience feeling of loneliness and abandonment and concern over their patients’ insurance.43
During the hospital stay and intensive care of their patients, the family caregivers of stroke patients experience shock and denial, stress, confusion, fear, and lack of control. In this period when the focus of care and treatment is on the patients’ survival, the caregivers want to know everything about what a stroke patient needs.44 The families of patients hospitalized in semi-ICU experience uncertainty about their patients’ conditions which leads to feelings of loneliness, fear, insecurity, anger, and instability in the family. Having their patients hospitalized in semi-ICU makes the patients’ families emotionally vulnerable, so they need social and spiritual sources of support to cope with the illness and hospitalization of their patients to maintain stability in the family.45 Through effective educational interventions, nurses and other professional caregivers can decrease uncertainty and fear in these patients and their family caregivers, thereby increasing the efficacy of their care and reducing the side effects of treatment.
Studies show that the psychological and financial burden of caring for their patients and lack of support from the healthcare system and the government have an adverse effect on family caregivers’ interactions with the other members of their families.14,16 Raising public awareness about MS can help improve family relationships. The physical, psychological, emotional, social, and financial challenges which MS patients’ family caregivers experience can depress them and reduce the quality of their lives.3 Other studies show that the stress of realizing that their patients have the illness can cause MS patients’ families emotional harm as well as anger and depression.46,47 The high cost of medication, the unavailability of some medication, the fear that their patients may lose their jobs, and lack of support from the government increase the stress which MS patients’ families experience and make them search for other sources of support.48 The participants were concerned about the possible progression of the disease in the future and the possible impact of atrophy caused by the disease on their lives; thus, their need for emotional support to cope with their crisis. Social support, especially from their friends and relatives, also can help them cope with their situation.49
In Asian cultures, collectivism prevails, meaning that individuals prefer to have their emotional needs met by their families in order to achieve a sense of unity, belonging, and identity. Collectivist cultures stress family relations and responsibilities and regard them as more important than other responsibilities and roles. However, in European and North American cultures, individualism is dominant.50 Individualism emphasizes self-sufficiency, independence, personal achievements, voluntary family relations, and equality.51 In collectivist societies, involving patient’s families in clinical decision-making is important. Thus, though patients are at the center of counseling and receiving information about their conditions to make decisions, their families are involved in the making of those decisions too according to the patients’ priorities and preferences.52
In the collectivist culture of China, families decide the amount and type of information which is provided to cancer patients—at the request of patients’ families, doctors are required to keep the patients uninformed about their status. So, professional caregivers must consider the culture of patients and their families.53 In the Iranian culture, too, the family is the main source of emotional support for patients: the presence of family members by the side of patients and visits from friends and relatives are a regular part of care for patients and a manifestation of their social and religious values. In such a culture, holistic healthcare would demand that professional caregivers respect the needs of patients and their family members in the clinical environment.
Another important category extracted from the participants’ experiences is professional caregivers’ body language. Since through effective body language, the members of healthcare teams can demonstrate that they understand the psychological and emotional concerns of patients’ families and companions, it is important that they use this means of communication effectively as part of their interventions from the time of patients’ admission and throughout their stay in the hospital.54
To care for their patients properly, especially after discharge, MS patients’ family caregivers need to be given information and full support. The participants’ experiences show that receiving follow-up care at home is very important. The results of a review study show that family caregivers, during the transition of the palliative care of their patients from hospital to home, experience poor interaction on the part of the healthcare team and lack of coordination in the continuation of care at home, which adds to their stress and anxiety.55 In a study, the researchers use a Multiple Sclerosis at Home Access model to provide a group of patients with full support and prevent the common complications of MS in their case. The key features of their plan include monthly visits at the patients’ homes and the continuation of the caregiving process by professional caregivers. In this society-centered healthcare model, the nurses act as a link between the primary caregivers and the professional caregivers. The results show that, after one year, the family caregivers’ satisfaction increased and the indexes of their quality of life improved.56 A family-centered care program is another innovative approach to planning, providing, and checking healthcare. In this kind of program, the abilities and needs of all the members of a patient’s family are considered.57
Another category extracted from the family caregivers’ experiences is undue expressions of pity from the members of healthcare teams and relatives. The findings show that, rather than trying to alleviate the pain and suffering of patients and their family caregivers, healthcare teams and friends and relatives occasionally add to their suffering by displaying pitying behaviors. According to the participants of a study, educating the public about an illness can eliminate the possible stigma which is attached to it and encourage people to understand the conditions of patients and their families rather than pitying them.3 A new topic of interest in healthcare is compassionate care which stresses ethical and human values. Compassionate care is defined as a deep feeling of being connected to human suffering and an ethical response to the sufferings of others.40,54 It appears that many professional caregivers and patients’ friends and relatives do not comprehend compassionate care and only communicate a sense of pity to their patients. This failure to provide any practical solutions is perceived by patients and their family caregivers as pitying.
Another finding of the present study is family caregivers’ reliance on religion-based coping strategies. The results show that MS patients’ family caregivers try to cope with the stressful experience of the first hospitalization of their patients by placing their trust in God and invocation. In another study, family caregivers are reported to try to achieve peace through their trust in God and invocation.5 Similarly, another study lists chanting hymns, praying, and reciting the Quran as religious acts performed by family caregivers at their patients’ bedside. These religious behaviors are family caregivers’ attempts at coping with the stress of their patients’ illness and improving their sense of purpose.58
A study introduces spirituality as an effective factor in the coping of married couples with MS. The couples claimed that they always remembered God, saw their illness as a divine test, and that their illness could be a blessing since they experienced good events in the post-illness period of their lives.59 The benefits of religiousness and spirituality can enable an individual to cope with illness more easily and achieve internal peace, optimism, positive relations, social and emotional support, life satisfaction, and eventually the power to adapt to life with a spouse who has MS.60,61 The Iranian culture attaches great importance to religion and spirituality and people tend to seek help and protection from God in times of crisis. People’s spirituality helps them cope with the difficulties of life; in other words, spiritual well-being facilitates adjustment.
The present study explores the experiences of MS patients’ family caregivers at the first hospitalization of their patients to provide health policy-makers with a better insight into ways of improving family caregivers’ competencies. One of the limitations of the study is the possibility of social desirability bias in the family caregivers’ answers to the researchers’ questions in the interviews. Social desirability bias is respondents’ tendency to over-report their positive social behaviors and attitudes and downplay their negative ones, which can affect the reliability of the data collected by researchers.62 In the present study, the researcher tried to minimize the impact of this bias by explaining the objective of the study to the participants.
Conclusion
When their patients are hospitalized for the first time, MS patients’ family caregivers have a variety of needs which must be identified and attended to by professional caregivers to reduce the psychological stress which the patients’ family caregivers experience. The psychological and social problems of family caregivers can adversely affect their coping mechanism. In the present study, the participants were found to rely on such coping strategies as searching for full support and religion. Informing professional caregivers about the various forms of coping can enable them to help patients and their family caregivers to better cope with the disease and improve their quality of life. The findings of the present study provide a framework for developing educational programs for improving the skills of family caregivers and the quality of counseling and support plans for them based on their religious and cultural background. Follow-up care and giving them guidance at home can contribute to the empowerment of family caregivers.
Ethics Approval and Informed Consent
This study was conducted in accordance with the World Medical Association’s Declaration of Helsinki. The present study has been approved by the ethics committee of the Shiraz University of Medical Sciences, Shiraz, Iran (IR.SUMS.REC.1398.831). The study materials (interview questions and informed consent form) were approved by the ethics committee of the university. In line with the ethical principles of research, before the interviews, the participants were informed about the objectives of the study, the voluntary basis of their participation, the reason for recording the interviews, and the role of the researcher. Subsequently, the participants’ informed consent was obtained verbally and in writing. In addition, the participants were assured about the confidentiality and anonymity of their information. They were also informed that they had the right to withdraw at any point through the study and that the time and place of the interviews would be decided with their prior agreement.
Acknowledgments
The present study was extracted from a research project-number 97-01-08-17539-approved by the ethics committee of Shiraz University of Medical Sciences, Shiraz, Iran. The researchers would like to express their gratitude to the authorities of the Nursing Department and research deputy at Shiraz University of Medical Sciences. The authors’ thanks are also due to the caregivers who participated in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Smeltzer S, Bare B, Hinkle J, Cheever K. Brunner& Suddarth’s Textbook of Medical-Surgical Nursing. China: Lippinicott Williams and Wilkins; 2010:889.
2. Ghafari S, Fallahi-Khoshknab M, Norouzi K, Mohamadi E. Experiences of hospitalization in patients with multiple sclerosis: a qualitative study. Iran J Nurs Midwifery Res. 2014;19:255. doi:10.4103/1735-9066.208168
3. Abolhassani S, Yazdannik A, Taleghani F, Zamani A. Expectations of multiple sclerosis patients and their families: a qualitative study in Iran. Iran Red Crescent Med J. 2015;17. doi:10.5812/ircmj.18293.
4. Dennison L, Moss-Morris R, Silber E, Galea I, Chalder T. Cognitive and behavioural correlates of different domains of psychological adjustment in early-stage multiple sclerosis. J Psychosom Res. 2010;69:353–361. doi:10.1016/j.jpsychores.2010.04.009
5. Fallahi-Khoshknab M, Ghafari S, Nourozi K, Mohammadi E. Confronting the diagnosis of multiple sclerosis: a qualitative study of patient experiences. J Nurs Res. 2014;22:275–282. doi:10.1097/jnr.0000000000000058
6. Ekdahl AW, Andersson L, Friedrichsen M. “They do what they think is the best for me.” Frail elderly patients’ preferences for participation in their care during hospitalization. Patient Educ Couns. 2010;80:233–240. doi:10.1016/j.pec.2009.10.026.
7. Andenæs R, Kalfoss MH, Wahl AK. Coping and psychological distress in hospitalized patients with chronic obstructive pulmonary disease. Heart Lung. 2006;35:46–57. doi:10.1016/j.hrtlng.2005.09.009
8. Cadden MH, Arnett PA, Tyry TM, Cook JE. Judgment hurts: the psychological consequences of experiencing stigma in multiple sclerosis. Soc Sci Med. 2018;208:158–164. doi:10.1016/j.socscimed.2018.01.015
9. Cook JE, Germano AL, Stadler G. An exploratory investigation of social stigma and concealment in patients with multiple sclerosis. Int J MS Care. 2016;18(2):78–84. doi:10.7224/1537-2073.2015-021
10. Masoudi R, Khayeri F, Rabiei L, Zarea K. A study of stigma among Iranian family caregivers of patients with multiple sclerosis: a descriptive explorative qualitative study. Appl Nurs Res. 2017;34:1–6. doi:10.1016/j.apnr.2016.11.012.
11. Ebrahimi H, Hasankhani H, Namdar H, Khodadadi E, Fooladi M. Dealing with chronic illness: experiences of Iranian families of persons with multiple sclerosis—A qualitative study. Mult Scler Int. 2017;2017:9243161. doi:10.1155/2017/9243161.
12. Reader TW, Gillespie A. Patient neglect in healthcare institutions: a systematic review and conceptual model. BMC Health Serv Res. 2013;13:156. doi:10.1186/1472-6963-13-156
13. Plank A, Mazzoni V, Cavada L. Becoming a caregiver: new family carers’ experience during the transition from hospital to home. J Clin Nurs. 2012;21:2072–2082. doi:10.1111/j.1365-2702.2011.04025.x
14. Benito-León J, Rivera-Navarro J, Guerrero AL, et al. The CAREQOL-MS was a useful instrument to measure caregiver quality of life in multiple sclerosis. J Clin Epidemiol. 2011;64:675–686. doi:10.1016/j.jclinepi.2010.08.003
15. Richard Schulz SR, Beach EM, Friedman GR, Martsolf JR, Everette James III. Changing structures and processes to support family caregivers of seriously ill patients. J Palliat Med. 2018;
16. Buchanan RJ, Radin D, Huang C, Zhu L. Caregiver perceptions associated with risk of nursing home admission for people with multiple sclerosis. Disabil Health J. 2010;3:117–124. doi:10.1016/j.dhjo.2009.08.003
17. Gupta S, Goren A, Phillips AL, Stewart M. Self-reported burden among caregivers of patients with multiple sclerosis. Int J MS Care. 2012;14(4):179–187. doi:10.7224/1537-2073-14.4.179
18. van der Hiele K, van Gorp D, Heerings M, et al. Caregiver strain among life partners of persons with mild disability due to relapsing-remitting multiple sclerosis. Mult Scler Relat Disord. 2019;31:5–11. doi:10.1016/j.msard.2019.03.005
19. Buchanan RJ, Radin D, Huang C. Caregiver burden among informal caregivers assisting people with multiple sclerosis. Int J MS Care. 2011;13(2):76–83. doi:10.7224/1537-2073-13.2.76
20. Özmen S, Yurttaş A. Determination of care burden of caregivers of patients with multiple sclerosis in Turkey. Behav Neurol. 2018;2018. doi:10.1155/2018/7205046
21. Dayapoğlu N, Tan M. The care burden and social support levels of caregivers of patients with multiple sclerosis. Kontakt. 2017;19(1):e17–e23. doi:10.1016/j.kontakt.2016.12.001
22. Reinhard SC, Given B, Petlick NH, Bemis A. Supporting family caregivers in providing care. In: Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Agency for Healthcare Research and Quality (US). 2008.
23. Masoudi R, Abedi HA, Abedi P, Mohammadianinejad SE. Iranian family caregivers’ challenges and issues in caring of multiple sclerosis patients: a descriptive explorative qualitative study. Iran J Nurs Midwifery Res. 2014;19:416.
24. Martindale-Adams J, Zuber J, Levin M, Burns R, Graney M, Nichols LO. Integrating caregiver support into multiple sclerosis care. Mult Scler Int. 2020;2020:1–8. doi:10.1155/2020/3436726
25. Ebrahimi H, Torabizadeh C, Mohammadi E, Valizadeh S. Patients’ perception of dignity in Iranian healthcare settings: a qualitative content analysis. J Med Ethics. 2012;38:723–728. doi:10.1136/medethics-2011-100396
26. Lorefice L, Gioiaura G, Coni G, et al. What do multiple sclerosis patients and their caregivers perceive as unmet needs? BMC Neurol. 2013;13:177. doi:10.1186/1471-2377-13-177
27. Burns N, Grove SK. Understanding Nursing Research: Building an Evidence-Based Practice.
28. Polit DF, Beck CT. Essentials of Nursing Research: Appraising Evidence for Nursing Practice. Lippincott Williams & Wilkins; 2013.
29. Holloway I, Wheeler S. Qualitative Research in Nursing and Healthcare. John Wiley & Sons; 2013.
30. Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277–1288. doi:10.1177/1049732305276687
31. Mohammadi F, Rakhshan M, Molazem Z, Zareh N, Gillespie M. Parents’ perspectives on family violence against children with autism. Arch Iran Med. 2019; 22:505–510.
32. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107–115. doi:10.1111/j.1365-2648.2007.04569.x
33. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24:105–112. doi:10.1016/j.nedt.2003.10.001
34. Lincoln YS, Guba EG. Naturalistic Inquiry. Vol. 75. CA: Sage Thousand Oaks; 1985.
35. Gafari S, Khoshknab MF, Nourozi K, Mohamadi E. Informal caregivers’ experiences of caring of multiple sclerosis patients: a qualitative study. Iran J Nurs Midwifery Res. 2017;22:243. doi:10.4103/1735-9066.208168.
36. Manookian A, Cheraghi MA, Nasrabadi AN. Factors influencing patients’ dignity: a qualitative study. Nurs Ethics. 2014;21:323–334. doi:10.1177/0969733013498526
37. Kalhor R, Azimian J, Gholami S, Darzi-Ramandi F, Moosavi S, Layeghifar M. A lump in throat: qualitative study on hospitalization-related experiences among the parents of children with cancer. Chronic Dis J. 2019;7:1–9.
38. Ferri P, Muzzalupo J, Di Lorenzo R. Patients’ perception of dignity in an Italian general hospital: a cross-sectional analysis. BMC Health Serv Res. 2015;15:41. doi:10.1186/s12913-015-0704-8
39. Skär L, Söderberg S. Complaints with encounters in healthcare–men’s experiences. Scand J Caring Sci. 2012;26:279–286. doi:10.1111/j.1471-6712.2011.00930.x
40. Tehranineshat B, Rakhshan M, Torabizadeh C, Fararouei M. Nurses’, patients’, and family caregivers’ perceptions of compassionate nursing care. Nurs Ethics. 2019;26:1707–1720. doi:10.1177/0969733018777884
41. Hagedoorn EI, Paans W, Jaarsma T, Keers JC, van der Schans C, Louise Luttik M. Aspects of family caregiving as addressed in planned discussions between nurses, patients with chronic diseases and family caregivers: a qualitative content analysis. BMC Nurs. 2017;16(1):37. doi:10.1186/s12912-017-0231-5
42. Etemadifar S, Bahrami M, Shahriari M, Farsani AK. Family caregivers’ experiences of caring for patients with heart failure: a descriptive, exploratory qualitative study. J Nurs Res. 2015;23:153–161. doi:10.1097/JNR.0000000000000076.
43. Hupcey JE, Fenstermacher K, Kitko L, Fogg J. Palliative needs of spousal caregivers of patients with heart failure followed at specialized heart failure centers. JHPN. 2011;13:142. doi:10.1097/NJH.0b013e31820ce15e
44. Lutz BJ, Ellen Young M, Cox KJ, Martz C, Rae Creasy K. The crisis of stroke: experiences of patients and their family caregivers. Top Stroke Rehabil. 2011;18:786–797. doi:10.1310/tsr1806-786
45. Neves L, Gondim AA, Soares SCMR, Coelho DP, Pinheiro JAM. The impact of the hospitalization process on the caregiver of a chronic critical patient hospitalized in a semi-intensive care unit. Esc Anna Nery. 2018;22. doi:10.1590/2177-9465-EAN-2017-0304.
46. Lee JH, Park HK, Hwang IC, et al. Factors associated with care burden among family caregivers of terminally ill cancer patients. Korean J Hosp Palliat Care. 2016;19:61–69. doi:10.14475/kjhpc.2016.19.1.61
47. Lyons JG, Cauley JA, Fredman L. The effect of transitions in caregiving status and intensity on perceived stress among 992 female caregivers and noncaregivers. J Gerontol a Biol Sci Med Sci. 2015;70:1018–1023. doi:10.1093/gerona/glv001
48. Ebrahimi H, Hasankhani H, Namdar H, Khodadadi E, Fooladi M. Impacts of chronic illness on families: experiences of Iranian family of patients with multiple sclerosis: a qualitative study. J Res Med Dent Sci. 2017;5:13–18. doi:10.1155/2017/9243161.
49. Wright AA, Zhang B, Ray A, et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA 2008;300:1665–1673. doi:10.1001/jama.300.14.1665.
50. Dai Q. Cross-cultural comparison of self-esteem among Mainland Chinese, Hong Kong Chinese, British-Born Chinese and White Scottish Children. Social Sci Asia. 2016;2:1–12. doi:10.14456/ssa.2016.3
51. Kotlaja MM. Cultural contexts of individualism vs. collectivism: exploring the relationships between family bonding, supervision and deviance. Eur J Criminol. 2018. doi:10.1177/1477370818792482
52. Lin M-L, Kan W-M, Chen C-H. Patients’ perceptions and expectations of family participation in the informed consent process of elective surgery in Taiwan. Asian Nurs Res (Korean Soc Nurs Sci). 2012;6:55–59. doi:10.1016/j.anr.2012.05.001
53. Huang Y-P, Wang S-Y, Chen S-H, Hsu W-Y, Chang M-Y. The experience of spousal caregivers of patients recently diagnosed with cancer in Taiwan. Collegian 2019;26:477–484. doi:10.1016/j.colegn.2018.12.005
54. Tehranineshat B, Rakhshan M, Torabizadeh C, Fararouei M. Compassionate care in healthcare systems: a systematic review. J Natl Med Assoc. 2019;111(5):546–554. doi:10.1016/j.jnma.2019.04.002.
55. Arias Rojas M, García-Vivar C. The transition of palliative care from the hospital to the home: a narrative review of experiences of patients and family caretakers. Invest Educ Enferm. 2015;33:482–491. doi:10.17533/udea.iee.v33n3a12
56. Rossinot H, Marquestaut O, de Stampa M. The experience of patients and family caregivers during hospital-at-home in France. BMC Health Serv Res. 2019;19:470. doi:10.1186/s12913-019-4295-7
57. Kamran A, Nasiri K, Eskandari M, et al. The comparison of nurses and families’ viewpoint of family-centered caring in Khalkhal Hospital, 2017. Int Arch Health Sci. 2017;4:58. doi:10.4103/iahs.iahs_20_17
58. Kiyancicek Z, Caydam OD. Spırıtual needs and practıces among famıly caregıvers of patıents wıth cancer. Acta Paul Enferm. 2017;30:628–634. doi:10.1590/1982-0194201700090.
59. Allahbakhshian M, Jafarpour M, Parvizi S. Spiritual well-being of patients with multiple sclerosis. Iran J Nurs Midwifery Res. 2011;16:202.
60. Yeganeh T, Shaikhmahmoodi H. Role of religious orientation in predicting marital adjustment and psychological well-being. Social Mind. 2013;3:131. doi:10.4236/sm.2013.32020
61. DeMaris A, Mahoney A, Pargament KI. Sanctification of marriage and general religiousness as buffers of the effects of marital inequity. J Fam Issues. 2010;31:1255–1278. doi:10.1177/0192513x10363888
62. Buchanan RJ, Huang C. Informal caregivers assisting people with multiple sclerosis: factors associated with the strength of the caregiver/care recipient relationship. Int J MS Care. 2011;13:177–187. doi:10.7224/1537-2073-13.4.177
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.