")
Back to Journals » OncoTargets and Therapy » Volume 9
The EGFR tyrosine kinase inhibitors as second-line therapy for EGFR wild-type non-small-cell lung cancer: a real-world study in People's Republic of China
Authors Xu J, Ding G, Zhang X, Jin B, Lou Y , Zhang Y, Wang H, Wu D, Han B
Received 9 August 2016
Accepted for publication 31 August 2016
Published 20 October 2016 Volume 2016:9 Pages 6479—6484
DOI https://doi.org/10.2147/OTT.S119341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yao Dai
Jianlin Xu,1,* Guozheng Ding,2,* Xueyan Zhang,1 Bo Jin,1 Yuqing Lou,1 Yanwei Zhang,1 Huiming Wang,1 Dan Wu,3 Baohui Han1
1Department of Pulmonary, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Department of Pulmonary, Anqing Municipal Hospital, Anhui, People’s Republic of China; 3Central laboratory, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Introduction: Clinical evidence comparing chemotherapy and tyrosine kinase inhibitors (TKIs) as second-line therapy for epidermal growth factor receptor (EGFR) wild-type non-small-cell lung cancer (NSCLC) are conflicting.
Methods: We retrospectively reviewed stage IV EGFR wild-type NSCLC patients who relapsed on first-line chemotherapy at the Shanghai Chest Hospital to compare the efficacy of TKIs and chemotherapy as second-line therapy among different clinical subgroups.
Results: The progression-free survival (PFS) and overall survival for patients receiving chemotherapy as second-line therapy for NSCLC were longer than patients who received TKIs. The hazard ratios (HRs) were 0.40 (P<0.001) and 0.50 (P<0.001), respectively. Subgroup analyses showed that second-line TKI therapy resulted in inferior PFS among smokers (HR =0.24, P<0.001), males (HR =0.33, P<0.001), females (HR =0.54, P=0.004), and patients with adenocarcinoma (HR =0.48, P<0.001) and nonadenocarcinoma histology (HR =0.20, P<0.001). Among never-smokers, the PFS in cohorts receiving second-line chemotherapy or TKIs was not significantly different (HR =0.70, P=0.08).
Conclusion: These results suggest that EGFR TKI therapy was inferior compared to chemotherapy in EGFR wild-type NSCLC patients who relapsed from first-line chemotherapy; however, among never-smokers, these two treatment strategies were comparable.
Keywords: TKI, wild-type, NSCLC
Introduction
Lung cancer is the most frequently diagnosed cancer worldwide. Non-small-cell lung cancer (NSCLC) accounts for 85%–90% of all lung cancers.1,2 Most lung cancer patients are diagnosed at an advanced stage; thus, only a minority of patients are surgical candidates.3–5 In the last decade, the discovery of epidermal growth factor receptor (EGFR) as a driving gene in NSCLC and the subsequent discovery of the superior efficacy of tyrosine kinase inhibitors (TKIs) in patients with EGFR mutations have changed treatment patterns and outcomes.6–8 According to previous reports, the benefit of TKIs does not appear to be limited to patients with activating mutations of EGFR, and data from randomized trials suggest that some of these wild-type patients will derive a modest benefit from these agents.9 Current guidelines suggest that EGFR TKIs are an option upon progression to first-line treatment;10 however, the role of EGFR TKIs in treatment of EGFR wild-type NSCLC is debatable. In the present study, we collected clinical data at Shanghai Chest Hospital to analyze the efficacy of TKI therapy among different clinical subgroups.
Methods
Study design and patients
The study was approved by the Institutional Review Board of the Shanghai Chest Hospital. All subjects or their family members provided written informed consent. All of the patients were diagnosed with advanced NSCLC (stage IV) at the Shanghai Chest Hospital between January 2012 and December 2014. The inclusion criteria were as follows: 1) patients with stage IV NSCLC (NSCLC staging was performed according to the 7th edition of the TNM classification)11 and 2) patients with the EGFR wild-type mutation status. Untreated patients and patients with missing survival details were excluded from this analysis. The baseline clinical characteristics included age at diagnosis, tumor histology, smoking history, sex, and treatment-free interval. Treatment-free interval was defined as the time that elapsed from the completion of first-line treatment to progression.12
Testing method for EGFR mutations
DNA was extracted from five serial slices of a 5-μm paraffin section using the DNA FFPE Tissue Kit (Qiagen, Hilden, Germany). A highly sensitive method (Amplification Refractory Mutation System) was used to detect mutations in the EGFR gene according to the manufacturer’s protocol provided with the ADx EGFR mutation test kit (Amoy Diagnostics Co., Ltd., Xiamen, People’s Republic of China).13 The kit allows the detection of 29 known recurrent mutations in EGFR exons 18–21, which include G719X in exon 18; 19 deletions in exon 19; S768I, T790M, and three insertions in exon 20; and L858R and L861Q in exon 21.14 Real-time PCR was carried out using the cycling conditions described in Table S1. The assay was performed using a LightCycler480 (Hoffman-La Roche Ltd., Basel, Switzerland) machine according to the manufacturer’s instructions. If the sample FAM Ct value was greater than or equal to the critical negative value shown in the “Negative” row in manufacturer’s protocol of the ADx EGFR mutation test kit, the sample was classified as negative.
Clinical assessments
Clinical follow-up included a physical examination, an imaging examination, and routine laboratory tests, which were performed every 4 weeks. The PFS was determined from the date of initiating second-line therapy until the date of the first documented progression or the last follow-up visit. The OS was measured from the date of second-line therapy until the date of death or the last follow-up visit, whichever occurred first.
Statistical methods
For descriptive purposes, demographic and clinical data were summarized as the median with a range of continuous variables; categorical variables were expressed and summarized as the mean of absolute numbers and percentages. The survival results were summarized as median values, and two-sided 95% confidence intervals (CIs) were analyzed using the Kaplan–Meier method. Statistical significance was defined as a P<0.05. SPSS software (version 22; IBM Corporation, Armonk, NY) was used for all statistical analyses.
Results
A total of 364 EGFR wild-type NSCLC patients who received second-line therapy were included in this analysis, of whom 108 received EGFR TKIs as second-line therapy, whereas 256 received chemotherapy as second-line therapy. Patient demographic data are shown in Table 1.
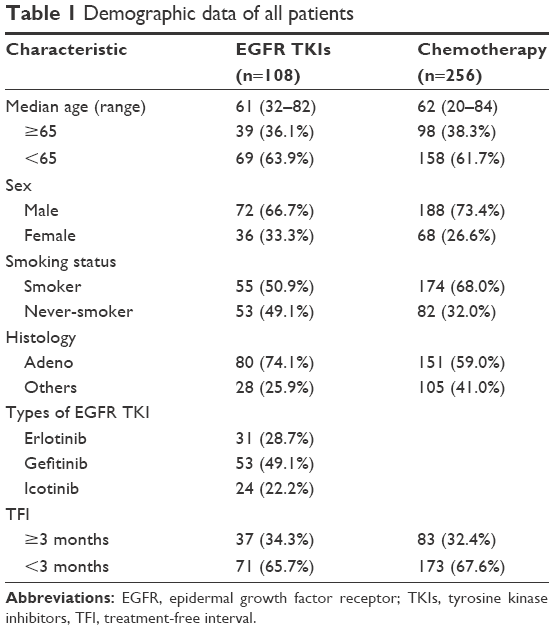 | Table 1 Demographic data of all patients |
The PFS for patients receiving chemotherapy (3.8 months; 95% CI, 3.3–4.2) as second-line therapy was significantly longer than patients who received TKIs (2.0 months; 95% CI, 1.8–2.3 and hazard ratio [HR], 0.40; 95% CI, 0.30–0.52; P<0.001; Figure 1). The OS of the chemotherapy and TKI cohorts was 8.0 months (95% CI, 7.2–8.8) and 7.0 months (95% CI, 6.1–7.8), respectively. The HR was 0.50 (95% CI, 0.38–0.66; P<0.001; Figure 2).
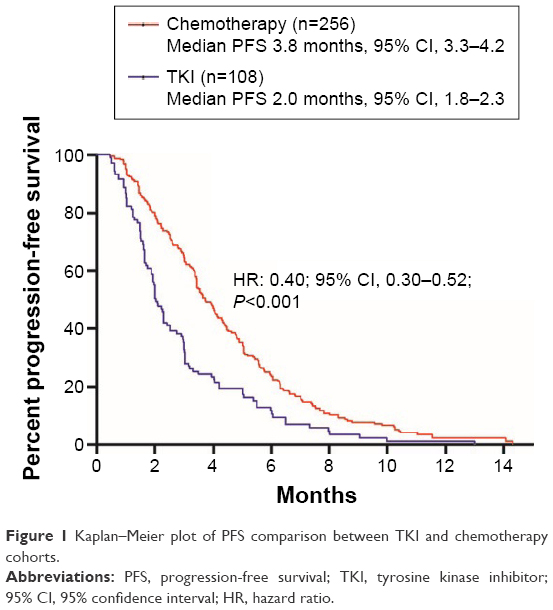 | Figure 1 Kaplan–Meier plot of PFS comparison between TKI and chemotherapy cohorts. |
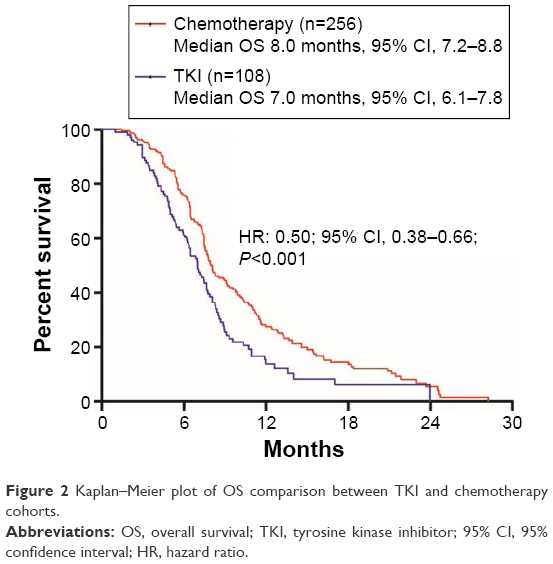 | Figure 2 Kaplan–Meier plot of OS comparison between TKI and chemotherapy cohorts. |
Subgroup analyses showed that second-line TKI therapy resulted in inferior PFS compared to chemotherapy among smokers (HR, 0.24; 95% CI, 0.17–0.34; P<0.001); males (HR, 0.33; 95% CI, 0.23–0.46; P<0.001), females (HR, 0.54; 95% CI, 0.35–0.82; P=0.004), patients with adenocarcinoma (HR, 0.48; 95% CI, 0.35–0.66; P<0.001) and nonadenocarcinoma histology (HR, 0.20; 95% CI, 0.12–0.33; P<0.001), age ≥65 years (HR, 0.36; 95% CI, 0.23–0.55; P<0.001), and age <65 years (HR, 0.42; 95% CI, 0.30–0.60; P<0.001). Among never-smokers, the PFS in cohorts receiving second-line chemotherapy or TKIs was not significantly different (HR, 0.70; 95% CI, 0.47–1.04; P=0.08) (Figure 3).
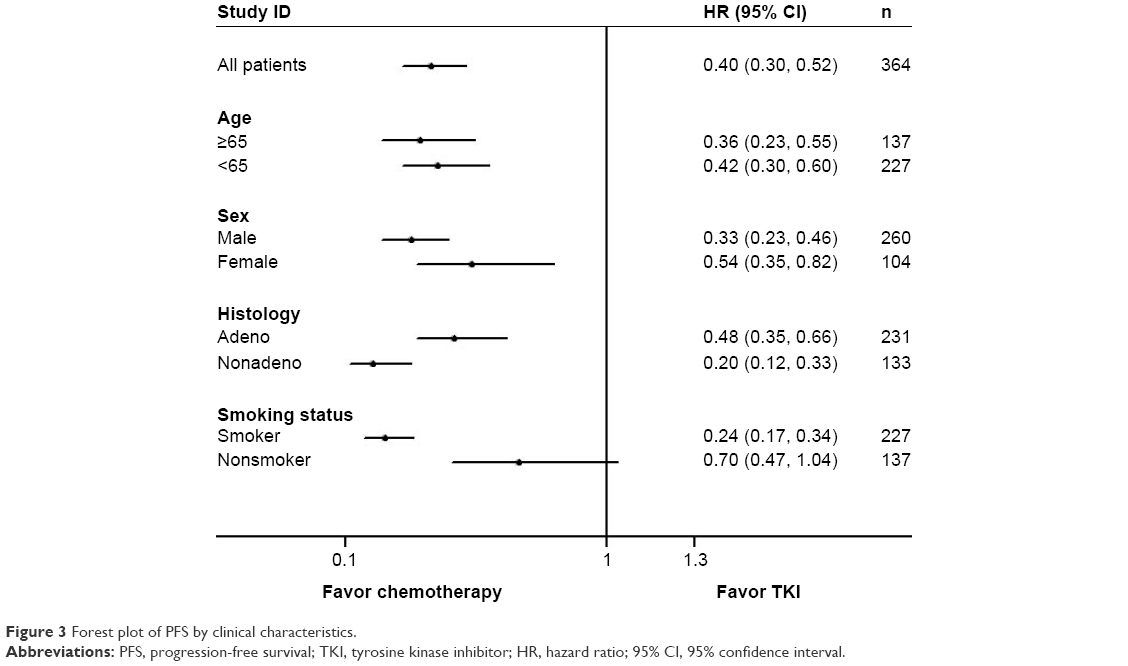 | Figure 3 Forest plot of PFS by clinical characteristics. |
Of the 108 patients who received TKI therapy, ten responded. Among the 53 never-smokers who received TKI therapy, nine responded. Among the 55 smokers, only one responded to TKI therapy.
Discussion
The present study directly compared TKIs with chemotherapy as second-line treatment for advanced NSCLC in patients with EGFR wild-type mutation status, and the results suggested that EGFR TKI therapy was inferior to chemotherapy. Subgroup analyses demonstrated a comparable PFS between the two treatment strategies among never-smokers.
Subgroup analysis of the Iressa Pan-Asia Study trial demonstrated that chemotherapy is superior to TKI as first-line therapy in patients with EGFR wild-type NSCLC.7 While TKIs also achieve modest efficacy in EGFR wild-type patients, they are recommended as an option when chemotherapeutic reagents have failed, and this is based on the results of longer survival in comparison with best supportive care.9 Clinical evidence involving a comparison of chemotherapy and TKIs as second-line therapy for EGFR wild-type NSCLC are controversial. The CTONG 0806 study compared pemetrexed with gefitinib in EGFR wild-type patients, and the overall results favored pemetrexed, with a PFS of 5.6 versus 1.7 months.15 Similarly, the TAILOR and DELTA trials also demonstrated a significant improvement in PFS with second-line chemotherapy compared with TKIs in patients with wild-type EGFR tumors.16,17 However, the INTEREST and TITAN trials demonstrated noninferiority of gefitinib as second-line therapy for patients with wild-type EGFR tumors in comparison with chemotherapy.18,19 According to a previous meta-analysis, the different EGFR mutation detection methods in those trials might explain some of the discrepancy in results. Trials using direct sequencing as the method of EGFR mutation detection showed a lack of significant difference in PFS between TKI and chemotherapy groups. In trials using a more sensitive method for detection of EGFR mutations, the PFS was significantly different between the TKIs and chemotherapy groups.20 The method of EGFR mutation detection in the present study involved Amplification Refractory Mutation System, which has a sensitivity of 99%, compared to the 70% sensitivity of direct sequencing.21,22 The overall results demonstrated a longer PFS in the chemotherapy cohort over the TKI cohort.
In the present study, among the 53 never-smokers who received TKI therapy, nine patients responded. Among the 55 smokers, only one patient responded to TKI therapy. This result suggests that smoking status is predictive of benefit from TKI therapy in EGFR wild-type patients as well as lung adenocarcinoma patients with activating EGFR mutations.23,24 It has been reported that lung cancer in smokers has multiple genetic alterations that are associated with smoking, such as activation of the AKT and ERK signaling pathways,25 and these alterations mediate resistance to EGFR TKIs.26 Moreover, cigarette smoking can result in increased clearance and decreased plasma concentrations and area under the curve of erlotinib in current smokers.27,28 Previously, in an effort to identify patients with EGFR wild-type NSCLC who would benefit most from TKI treatment, mass spectrometry analysis of serum samples was used to categorize candidates likely to have good or poor survival.29 Previous research has tried to use KRAS mutations status to as a predictor of response to EGFR TKIs.30 However, to date, no consensus has been translated into clinical practice.
The major limitation of the present study is its retrospective nature. Furthermore, one of the limitations of current study is that only a single EGFR detection method was used. It is known that currently available EGFR detection methods have different specificities and sensitivities.31
Conclusion
Our findings lead us to surmise that EGFR wild-type NSCLC patients who relapse from first-line chemotherapy should be given priority for second-line chemotherapy. For never-smokers, however, TKIs might be an option.
Acknowledgments
The authors acknowledge support from the Department of Pathology of Shanghai Chest Hospital. We also thank Liyan Jiang, Hua Zhong, Chunlei Shi, Aiqing Gu, Liwen Xiong, and Yizhuo Zhao for their provision of study materials or patients for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global Cancer Statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. | ||
Chen W, Zheng R, Zeng H, Zhang S, He J. Annual report on status of cancer in China, 2011. Chin J Cancer Res. 2015;27(1):2–12. | ||
Aberle DR, Abtin F, Brown K. Computed tomography screening for lung cancer: has it finally arrived? Implications of the national lung screening trial. J Clin Oncol. 2013;31(8):1002–1008. | ||
Nelson C, Elmendorf S, Mead P. Neoplasms misdiagnosed as “chronic lyme disease”. JAMA Intern Med. 2015;175(1):132–133. | ||
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30. | ||
Lynch TJ, Bell DW, Sordella R, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small cell lung cancer to gefitinib. N Engl J Med. 2014;350(21):2129–2139. | ||
Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361(10):947–957. | ||
Li MJ, He Q, Li M, Luo F, Guan YS. Role of gefitinib in the targeted treatment of non-small-cell lung cancer in Chinese patients. Onco Targets Ther. 2016;9:1291–1302. | ||
Osarogiagbon RU, Cappuzzo F, Ciuleanu T, Leon L, Klughammer B. Erlotinib therapy after initial platinum doublet therapy in patients with EGFR wild type non-small cell lung cancer: results of a combined patient-level analysis of the NCIC CTG BR.21 and SATURN trials. Transl Lung Cancer Res. 2015;4(4):465–474. | ||
Reck M, Popat S, Reinmuth N, De Ruysscher D, Kerr KM, Peters S. Metastatic non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25:iii27–iii39. | ||
Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. | ||
Roengvoraphoj M, Tsongalis GJ, Dragnev KH, Rigas JR. Epidermal growth factor receptor tyrosine kinase inhibitors as initial therapy for non-small cell lung cancer: focus on epidermal growth factor receptor mutation testing and mutation-positive patients. Cancer Treat Rev. 2013;39(8):839–850. | ||
Zhang Q, Zhu L, Zhang J. Epidermal growth factor receptor gene mutation status in pure squamous-cell lung cancer in Chinese patients. BMC Cancer. 2015;15:88. | ||
Tang Y, Wang WY, Zheng K, et al. EGFR mutations in non-small cell lung cancer: an audit from West China Hospital. Expert Rev Mol Diagn. 2016;16(8):915–919. | ||
Zhou Q, Cheng Y, Yang JJ, et al. Pemetrexed versus gefitinib as a second-line treatment in advanced nonsquamous nonsmall-cell lung cancer patients harboring wild-type EGFR (CTONG0806): a multicenter randomized trial. Ann Oncol. 2014;25(12):2385–2391. | ||
Garassino MC, Martelli O, Broggini M, et al. Erlotinib versus docetaxel as second-line treatment of patients with advanced non-small-cell lung cancer and wild-type EGFR tumours (TAILOR): a randomised controlled trial. Lancet Oncol. 2013;14(10):981–988. | ||
Okano Y, Ando M, Asami K, et al. Randomized Phase III trial of erlotinib (E) vs docetaxel (D) as second- or third-line therapy in patients with advanced non-small cell lung cancer (NSCLC) who have wild- type or mutant epidermal growth factor receptor (EGFR): Docetaxel and Erlotinib Lung Cancer Trial (DELTA). Paper presented at: 2013 ASCO Annual Meeting; 2013; Abstract 8006. | ||
Kim ES, Hirsh V, Mok T, et al. Gefitinib versus docetaxel in previously treated non-small-cell lung cancer (INTEREST): a randomised Phase III trial. Lancet. 372(9652):1809–1818. | ||
Ciuleanu T, Stelmakh L, Cicenas S, et al. Efficacy and safety of erlotinib versus chemotherapy in second-line treatment of patients with advanced, non-small-cell lung cancer with poor prognosis (TITAN): a randomised multicentre, open-label, Phase III study. Lancet Oncol. 2012;13(3):300–308. | ||
Lee JK, Hahn S, Kim DW, et al. Epidermal growth factor receptor tyrosine kinase inhibitors vs conventional chemotherapy in non-small cell lung cancer harboring wild-type epidermal growth factor receptor: a meta-analysis. JAMA. 2014;311(14):1430–1437. | ||
Liu Y, Liu B, Li XY, et al. A comparison of ARMS and direct sequencing for EGFR mutation analysis and Tyrosine Kinase Inhibitors treatment prediction in body fluid samples of Non-Small-Cell Lung Cancer patients. J Exp Clin Cancer Res. 2011;30:111. | ||
Zhou Q, Zhang XC, Chen ZH, et al. Relative abundance of EGFR mutations predicts Benet from getinib treatment for advanced non–small-cell lung cancer. J Clin Oncol. 2011;29(24):3316–3321. | ||
Zhang Y, Kang S, Fang W, et al. Impact of smoking status on EGFR-TKI efficacy for advanced non-small-cell lung cancer in EGFR mutants: a meta-analysis. Clin Lung Cancer. 2015;16(2):144–151. | ||
Kim MH, Kim HR, Cho BC, et al. Impact of cigarette smoking on response to epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitors in lung adenocarcinoma with activating EGFR mutations. Lung Cancer. 2014;84(2):196–202. | ||
Govindan R, Ding L, Griffith M, et al. Genomic landscape of non-small cell lung cancer in smokers and never-smokers. Cell. 2012;150(6):1121–1134. | ||
Hecht SS. Lung carcinogenesis by tobacco smoke. Int J Cancer. 2012;131(12):2724–2732. | ||
Hamilton M, Wolf JL, Rusk J, et al. Effects of smoking on the pharmacokinetics of erlotinib. Clin Cancer Res. 2006;12(7 Pt 1):2166–2171. | ||
Lu JF, Eppler SM, Wolf J, et al. Clinical pharmacokinetics of erlotinib in patients with solid tumors and exposure-safety relationship in patients with non-small cell lung cancer. Clin Pharmacol Ther. 2006;80(2):136–145. | ||
Gregorc V, Novello S, Lazzari C, et al. Predictive value of a proteomic signature in patients with non-small-cell lung cancer treated with second-line erlotinib or chemotherapy (prose): a biomarker-stratified, randomised Phase III trial. Lancet Oncol. 2014;15(7):713–721. | ||
Liu J, Hu J, Cheng L, et al. Biomarkers predicting resistance to epidermal growth factor receptor-targeted therapy in metastatic colorectal cancer with wild-type KRAS. Onco Targets Ther. 2016;9:557–565. | ||
Odabas H, Ulas A, Aydin K, et al. Is second-line systemic chemotherapy beneficial in patients with non-small cell lung cancer (NSCLC)? A multicenter data evaluation by the Anatolian Society of Medical Oncology. Tumour Biol. 2015;36(12):9641–9648. |
Supplementary material
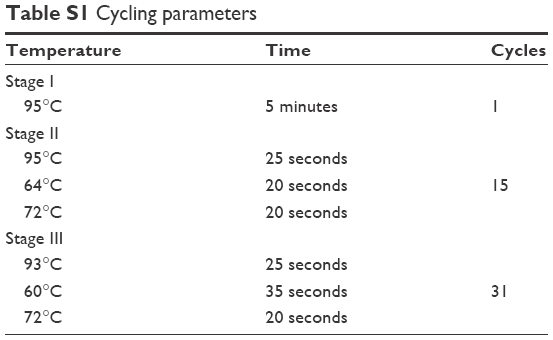 | Table S1 Cycling parameters |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.