")
Back to Journals » OncoTargets and Therapy » Volume 9
The efficiency and safety of trastuzumab and lapatinib added to neoadjuvant chemotherapy in Her2-positive breast cancer patients: a randomized meta-analysis
Authors Chen Z, Shen Y, Li S, Li C , Zhang L, Yang J, Lv M, Lin Y, Wang X, Yang J
Received 8 February 2016
Accepted for publication 8 April 2016
Published 30 May 2016 Volume 2016:9 Pages 3233—3247
DOI https://doi.org/10.2147/OTT.S106055
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Li
Zhe-Ling Chen, Yan-Wei Shen, Shu-Ting Li, Chun-Li Li, Ling-Xiao Zhang, Jiao Yang, Meng Lv, Ya-Yun Lin, Xin Wang, Jin Yang
Department of Medical Oncology, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China
Background: The addition of human epidermal growth factor receptor 2 (Her2) therapies to neoadjuvant chemotherapy (NAC) during treatment of Her2-positive breast cancer has been proposed as an effective way to improve the prognosis. However, the treatment outcomes of adding trastuzumab, lapatinib, or both to NAC were not unequivocal in randomized clinical trials. Based on these data, a meta-analysis was performed.
Objective: The main objective was to evaluate the efficiency and safety of trastuzumab and lapatinib added to NAC for treatment of Her2-positive breast cancer.
Methods: ClinicalTrials.gov and PubMed were searched for randomized clinical trials that compared trastuzumab, lapatinib, or both, added to NAC. The main endpoint was a pathologically complete response (pCR) rate, in breast only or in breast and lymph nodes. The drug safety and the influence of hormone-receptor status, comparing the clinical response and the rate of breast conservation, were evaluated.
Results: A total of eight publications were included in the primary analysis, designed as two or three subgroups. The cumulative cases were 2,349 and the analyses of all the clinical trials showed that the pCR rate was significantly higher in the group receiving trastuzumab than that in the group with lapatinib, either in breast only (P=0.001) or in breast and lymph nodes (P=0.0001). Similar results could be seen in comparisons of the combination versus trastuzumab group. Further studies of subgroups divided into hormone receptor-positive or-negative patients showed that the addition of trastuzumab or dual Her2-targeted therapy significantly improved the pCR rate in patients who were hormone-insensitive. Regarding the toxic effects, we found more grade 3 and 4 toxic effects, such as diarrhea, skin disorder, and hepatic biochemical changes in the lapatinib and combination groups. No temporally significant differences were found when the clinical response and the rate of breast conservation in the groups were analyzed.
Conclusion: The combination of trastuzumab and lapatinib was superior to single-agent treatment for improved pCR rate. However, combination treatment was not effective in improving the rate of breast conservation. Furthermore, a higher risk for toxicity was associated with combined administration.
Keywords: breast cancer, trastuzumab, lapatinib, human epidermal growth factor receptor, neoadjuvant, pathologically complete response
Introduction
The overexpression of human epidermal growth factor receptor 2 (Her2) can be found in 15%–20% of breast cancer patients, which is associated with significantly shortened disease-free and overall survival.1 The expression product of the Her2 gene is a membrane spanning oncogenic protein that is processed externally at the membrane. Because of its specific overexpression in tumor cells, Her2 can be used as a target antigen for breast cancer therapy.
The use of trastuzumab, a chimeric monoclonal antibody recognizing the extracellular region of the Her2 protein, has dramatically changed the outcome of patients with Her2-amplified breast cancer.2 Pegram et al3 reported that when given single-therapy trastuzumab as the first-line treatment in 112 Her2-positive breast cancer patients, the total responsive rate was 23%. The responsive rate in a subgroup of patients that overexpressed Her-2 was 31%. Trastuzumab has therefore been shown to be effective when used as a single agent, or when used with other chemotherapeutic drugs.
Recently, many other inhibitors such as small molecule tyrosine-kinase inhibitors, monoclonal antibodies, and antibody–drug conjugates are emerging as additional treatments.2 However, although these new drugs show promise, the most efficacious preoperative Her2 inhibitory agents are still being explored. Currently, the overexpression of the epidermal growth factor receptor and Her2 can be found in 20%–30% of the patients. Lapatinib is an orally bioavailable dual inhibitor of both the intracellular domain of the Her2 protein and the epidermal growth factor receptor. This dual inhibitor can effectively prevent the downstream signal transduction initiated by tyrosine kinase, thereby reducing the proliferation of tumor cells. Lapatinib was demonstrated to be beneficial in patients with Her2-positive locally advanced and metastatic breast cancer that had progressed after prior treatment with anthracycline, taxane, and trastuzumab. Because of their different mechanisms of drug actions, it may be useful to combine two drugs in order to provide improved clinically curative effects. Konecny et al4 found synergistic interactions between two agents in Her2-positive breast cancer models. If benefits such as decreasing the primary tumor and improving tumor response to chemotherapy5 could be achieved from neoadjuvant chemotherapy (NAC) alone, then using anti-Her2 agents together with NAC may provide a better outcome. It is therefore important to understand the efficacy and safety of a dual NAC/Her2-targeted therapy in the treatment of Her2-positive breast cancer patients. In this study, we evaluated pathologically complete response (pCR) rates when NAC was added to lapatinib, trastuzumab, or both in a meta-analysis of randomized clinical trials. We also evaluated the safety of these drugs and the influence of hormone-receptor (HR) status on treatment success. The clinical response and the rate of breast conservation were also investigated as additional parameters.
Methods
Search strategy
We carried out searches of ClinicalTrials.gov and PubMed for randomized clinical trials. The keywords used included breast cancer, trastuzumab, lapatinib, and Her2. We also used some selected studies for inclusion in the analyses.
Study criteria
The randomized Phase II or III clinical trials divided patients into groups with interventions using NAC with trastuzumab, lapatinib, or both in accordance with the inclusion criteria. Further inclusion criteria were that the patients should have Her2-positive operable breast cancer, with a primary endpoint of pCR rates. We included the chemotherapy regimen in every study and ensured homogeneity between studies.
Data extraction
After the exclusion criteria were met, eight studies met all the criteria. We extracted the following data from each eligible study: author’s name, trial phase, year of publication, number of patients enrolled, chemotherapy regimens used, treatment arms, HR status, and the endpoints.
Assessment of risk of bias between included studies
The random sequence generation, sample size, blinding procedure, loss to follow-up, dropout, and intentions to treat were used to assess the risk of bias between included studies. Jadad scoring was used to assess the quality of each study.
Outcome definition
The main objective of this analysis was to determine the pCR rate after adding trastuzumab, lapatinib, or both to NAC, to estimate the efficacy of different methods in anti-Her2 therapy. Two definitions of pCR were used in the included studies, no invasive tumors in breast only, or in breast and axillary nodes. We therefore adopted both as the endpoints. Other objectives, such as evaluating the safety of the drug, the influence of HR status, comparing the clinical responses, and the rates of breast conservation were also included.
Statistical analyses
We extracted the number of patients achieving pCR and the total number in each included trial, and then estimated the odds ratio (OR) between comparable groups and the 95% confidence interval (CI). In every trial, OR was calculated to evaluate the relative advantage of a group receiving NAC plus trastuzumab, lapatinib, or both. Assuming study variations existed, we used fixed effects or random effects model to complete the data analyses.
Cochran Q (significant cutoff point: P=0.10) and I2 (I2>50%, strong heterogeneity) statistics were used to test the heterogeneity between studies.
All the analyses and graphs were obtained using RevMan 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark, https://tech.cochrane.org).
Results
Study selection and exclusion
The primary search yielded a total of 52 relevant studies: 42 randomized clinical trials from PubMed and ten studies from additional references. The strategies used for selecting eligible studies are shown in Figure 1. Among the eliminated studies, the RC0639 study took disease-free survival and overall survival as the endpoints, not the pCR rate.6 The clinical trial described by Davies et al7 had a purpose inconsistent with our study.
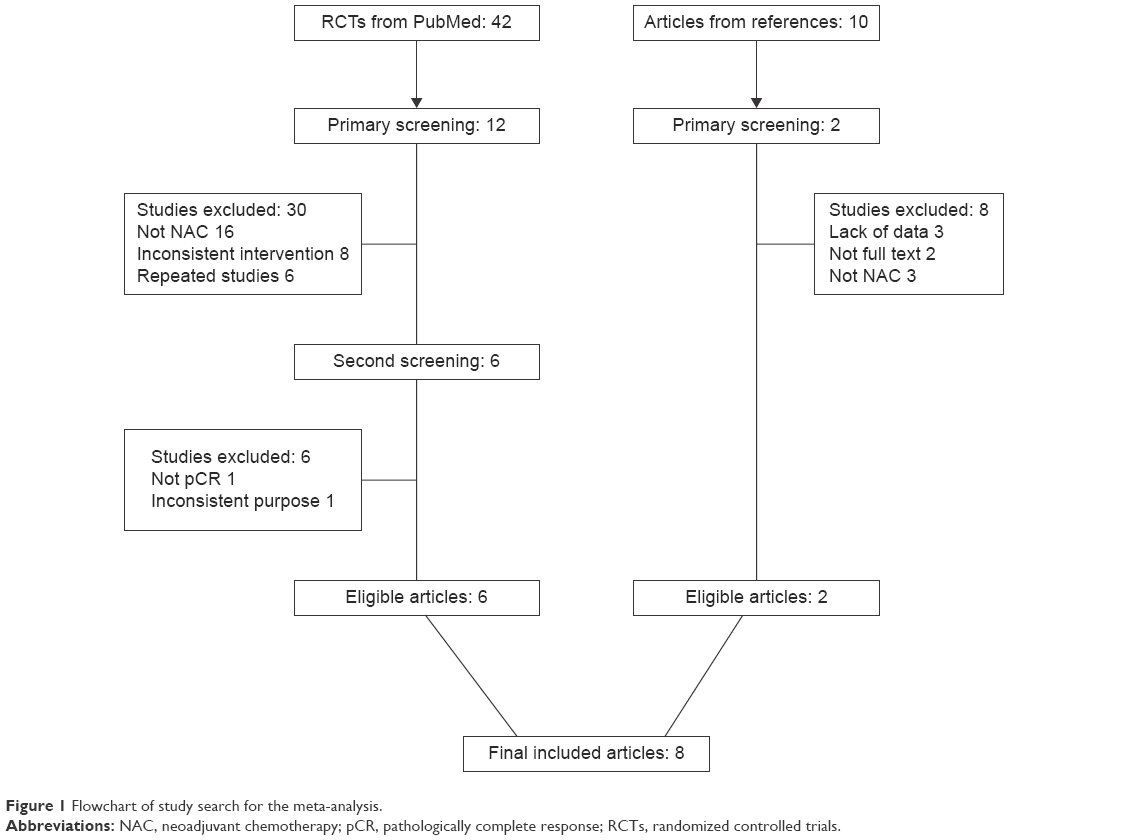 | Figure 1 Flowchart of study search for the meta-analysis. |
Study characteristics
Table 1 summarizes the baseline characteristics of the eight clinical trials that met the inclusion criteria and included 2,349 patients. The characteristics of the studies show that the eight studies were randomized control trials; the number of cases ranged from 100 to 700 cases. Six trials had three groups, which compared the addition of trastuzumab versus lapatinib versus their combination added to NAC; while the other two trials compared only trastuzumab versus lapatinib. Trastuzumab was used at a 4 mg/kg loading dose followed by 2 mg/kg in another six studies, while the other two studies used an 8 mg/kg loading dose followed by 6 mg/kg. The dose of lapatinib ranged from 1,000 to 1,500 mg given daily. Regarding the combination groups, lapatinib was administered at 1,000 mg. The Phase I safety, pharmacokinetics, and clinical activity study of lapatinib (GW572016) suggested that lapatinib was well tolerated at doses ranging from 500 to 1,600 mg given once daily, and clinical activity was observed most frequently at 900–1,200 mg.8 The clinical choice of dose was related to the tolerance to toxicities and there was no correlation between clinical response and different doses.
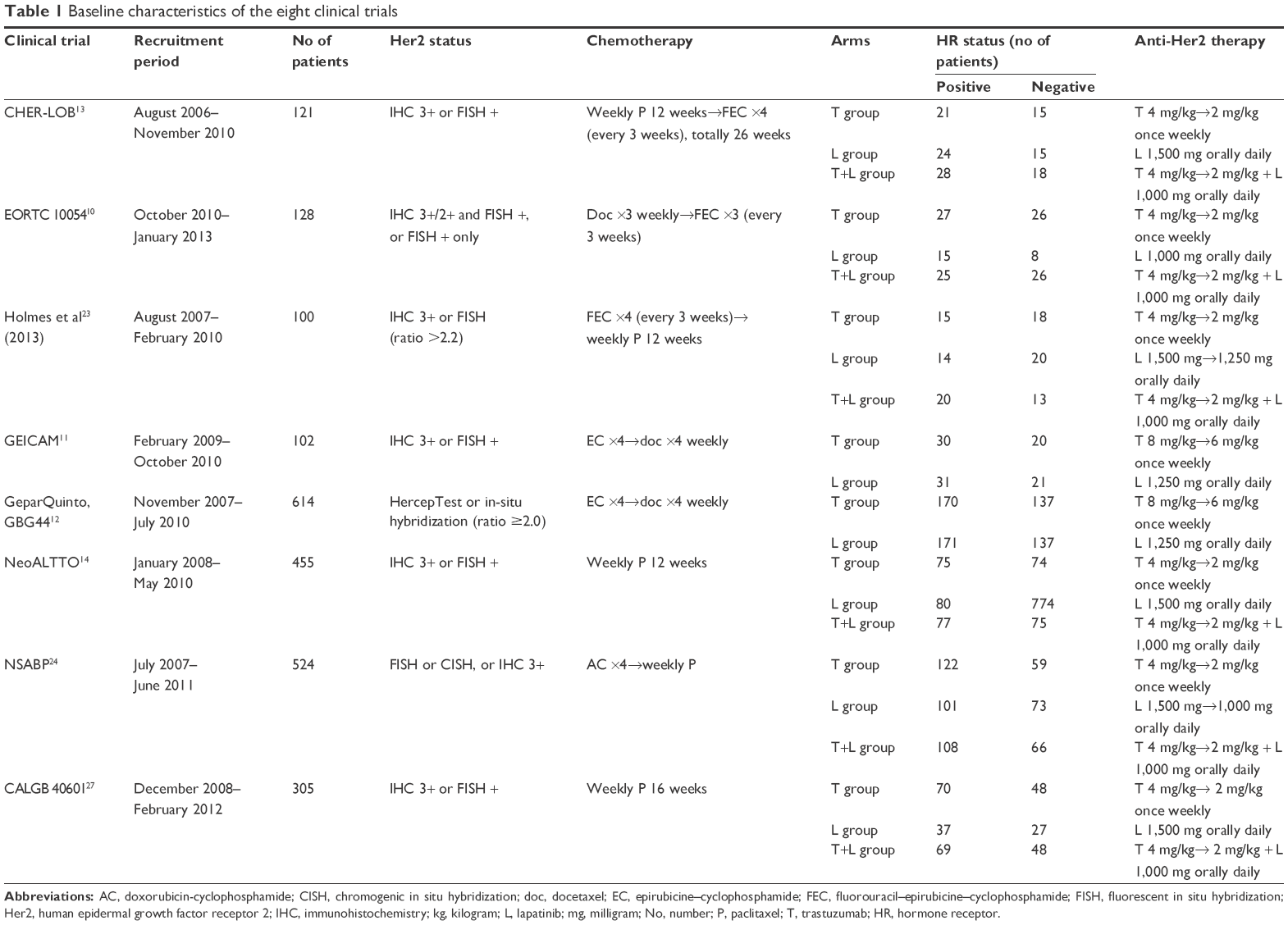 | Table 1 Baseline characteristics of the eight clinical trials |
Assessment of the methodological quality
All trials had definitely established inclusion and exclusion criteria. All patients with Her2-positive breast cancer were randomized to receive different anti-Her2 therapy, including trastuzumab, lapatinib, or their combination. The anti-HER2 therapy was carried out simultaneously with NAC, and included fluorouracil–epirubicine–cyclophosphamide, epirubicine–cyclophosphamide, and doxorubicin-cyclophosphamide. HER2 amplification was confirmed by immunohistochemistry or fluorescent in situ hybridization, and HR status was recorded for every trial. Study quality was assessed using the five-item Jadad score (seven points), with a score range of 4–7 (Table 2).
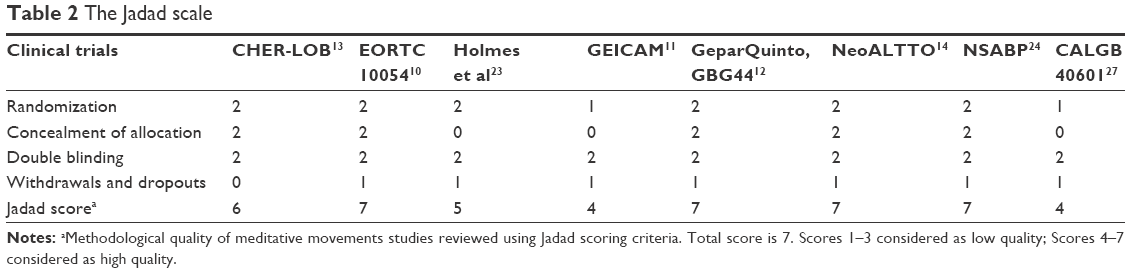 | Table 2 The Jadad scale |
The pCR rate of trastuzumab versus lapatinib
Seven trials, including 1,694 patients (n=887 in the trastuzumab group and n=807 in the lapatinib group), were analyzed for the pCR rate after addition of trastuzumab versus lapatinib compared to NAC in breast only. The absolute pCR rate was estimated to be 41% in the trastuzumab group compared to 33% in the lapatinib group. The pCR rate tended to be higher in the trastuzumab group versus the lapatinib group (OR, 1.41, 95% CI 1.14–1.73, P=0.001) (Figure 2A).
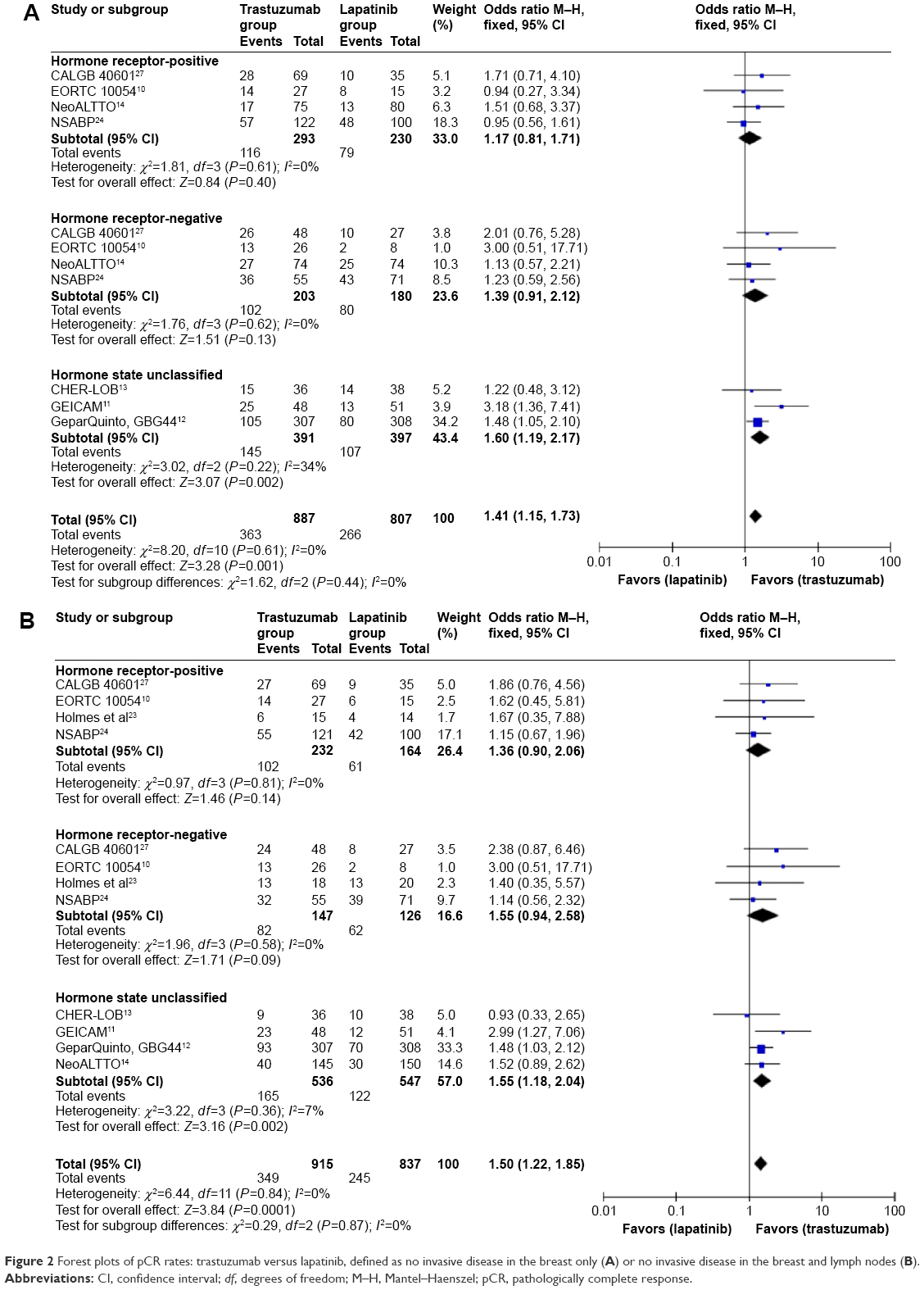 | Figure 2 Forest plots of pCR rates: trastuzumab versus lapatinib, defined as no invasive disease in the breast only (A) or no invasive disease in the breast and lymph nodes (B). |
Eight trials including 1,752 patients (n=915 in trastuzumab group and n=837 in the lapatinib group) were compared for the pCR rates in breast and lymph nodes. The absolute pCR rate was estimated to be 38% in the trastuzumab group and 29% in the lapatinib group. There were significant differences between the two groups, and the probability to achieve pCR was higher for the trastuzumab group versus the lapatinib group (OR, 1.50, 95% CI 1.22–1.85, P=0.0001) (Figure 2B).
The pCR rate of the combination treatment versus trastuzumab alone
For this comparison, data were available from five trials, providing the endpoints of the rates of pCR in breast alone. Overall, 1,057 patients enrolled (n=535 in the combination group and n=522 in the trastuzumab group), and the pCR rate was significantly higher in the combination group than that in the trastuzumab group (57.6% versus 44.6%, OR, 1.70, 95% CI 1.33–2.19, P<0.0001) (Figure 3A).
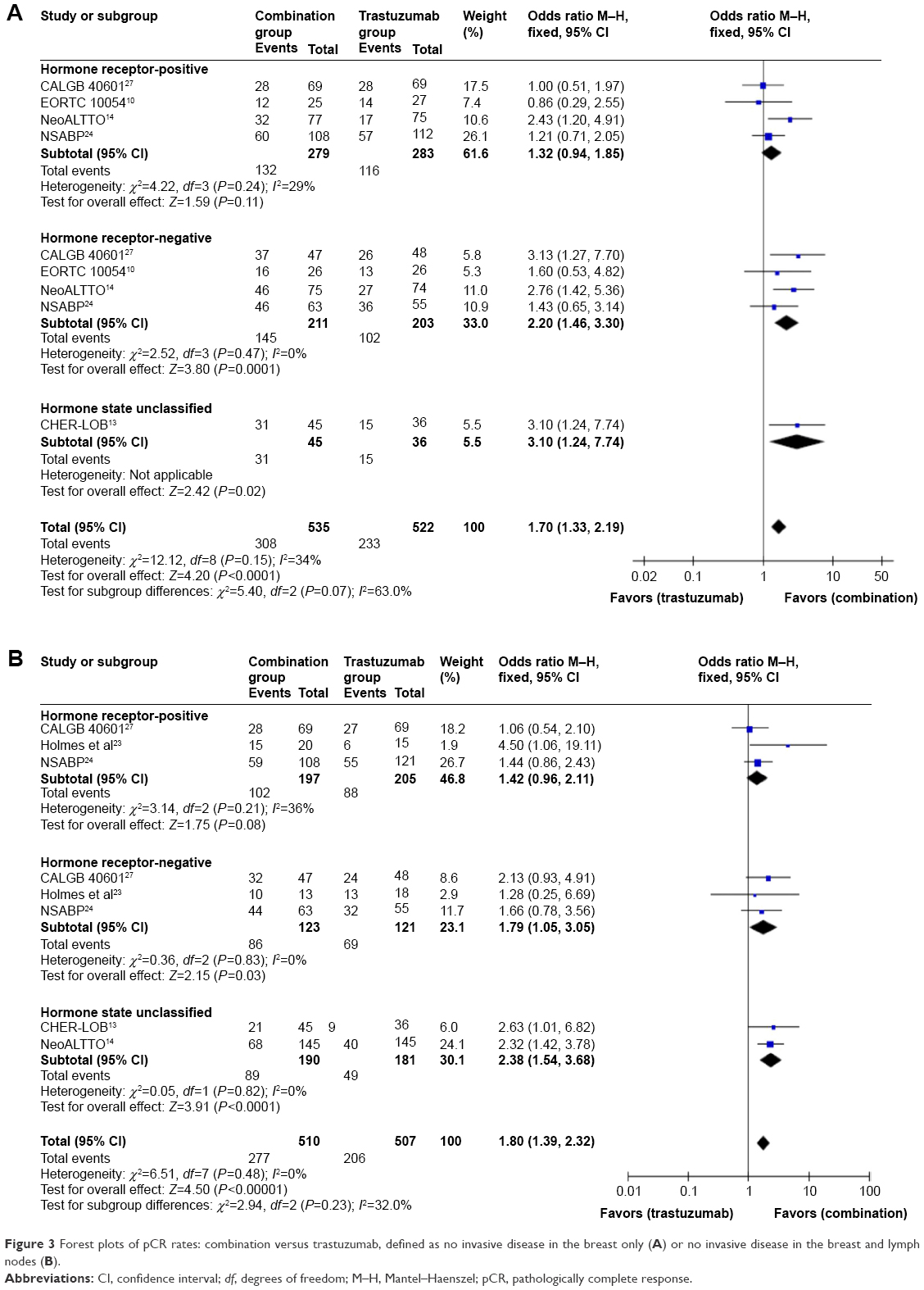 | Figure 3 Forest plots of pCR rates: combination versus trastuzumab, defined as no invasive disease in the breast only (A) or no invasive disease in the breast and lymph nodes (B). |
The pCR rate in breast and lymph nodes could be obtained from five trials (1,017 patients; 510 patients treated with lapatinib plus trastuzumab and 507 patients treated with trastuzumab alone). It is noteworthy that the dual HER2-targeted combination treatment achieved the higher rate of pCR in breast and lymph nodes (54% versus 41%, OR, 1.80, 95% CI 1.39–2.32, P<0.00001) (Figure 3B).
Subgroup analysis: the influence of HR status
Considering that the evaluation of biomarkers is highly recommended for the best management and therapeutic decision of breast cancer patient treatment, we divided patients into subgroups according to HR status in two comparisons, although the differences were small. The result showed that HR status contributed to the efficacy of different anti-Her2 therapies. In patients with HR-negative tumors, the pCR rate for the trastuzumab group, in breast only or in breast and lymph nodes, was significantly higher than for the lapatinib group. However, there was no significant difference in patients with HR-positive tumors (Figure 2). Similar outcomes were obtained with the comparison between the combination group and the trastuzumab group (Figure 3).
The clinical response
There were six trials providing comparison data of clinical response status between patients in the trastuzumab group and the lapatinib group. Four trials provided results comparing patients treated with trastuzumab plus lapatinib versus those treated using trastuzumab only. The percentage of patients who achieved a clinically complete response was similar in patients treated with trastuzumab or lapatinib (82.8% versus 82.4%, OR, 0.99, 95% CI 0.75–1.32, P=0.95) (Figure 4A). A similar result was observed for patients who were given dual Her2 block treatment or trastuzumab only (85.4% versus 82.2%, OR, 1.34, 95% CI 0.91–1.98, P=0.14) (Figure 4B).
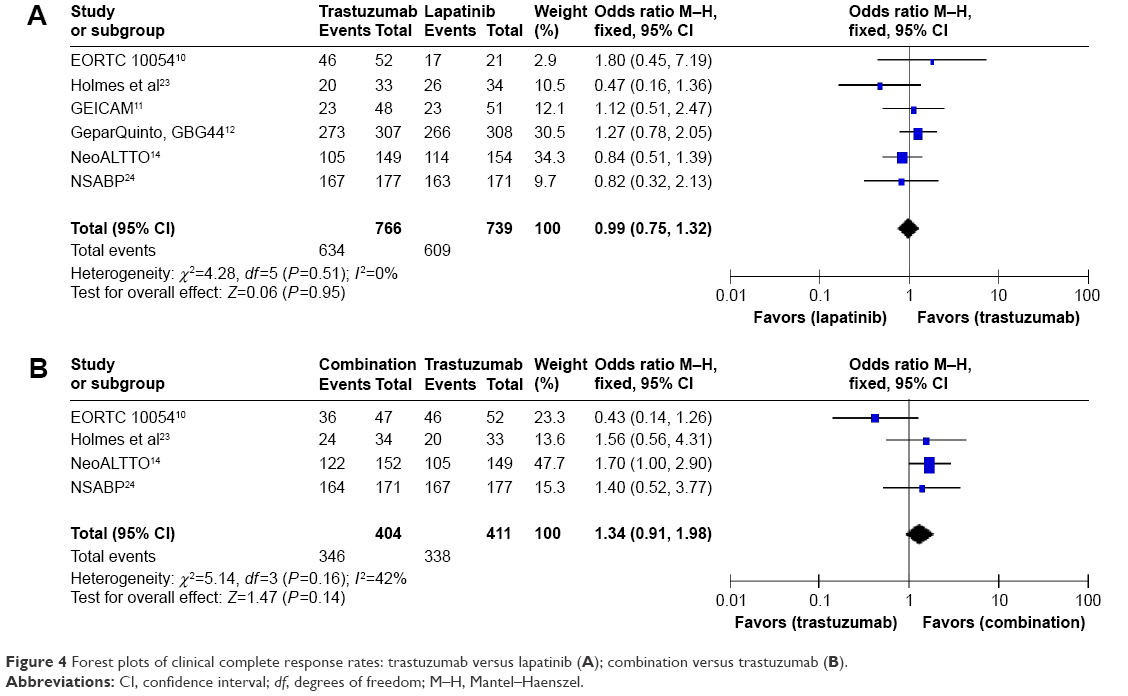 | Figure 4 Forest plots of clinical complete response rates: trastuzumab versus lapatinib (A); combination versus trastuzumab (B). |
The rate of breast conservation
Surgery was planned after the last chemotherapy administration and the candidates underwent breast conservation, or alternately, total mastectomy. The choice of surgery depended on the results obtained after chemical drug treatments. The rate of breast conservation between the groups showed no significant difference, either in the comparison groups of trastuzumab and lapatinib (50.5% versus 47.5%, OR, 1.812, 95% CI 0.91–1.38, P=0.27) (Figure 5A) or in that of the combination group and trastuzumab-alone group (45.7% versus 44.3%, OR, 1.05, 95% CI 0.79–1.40, P=0.73) (Figure 5B).
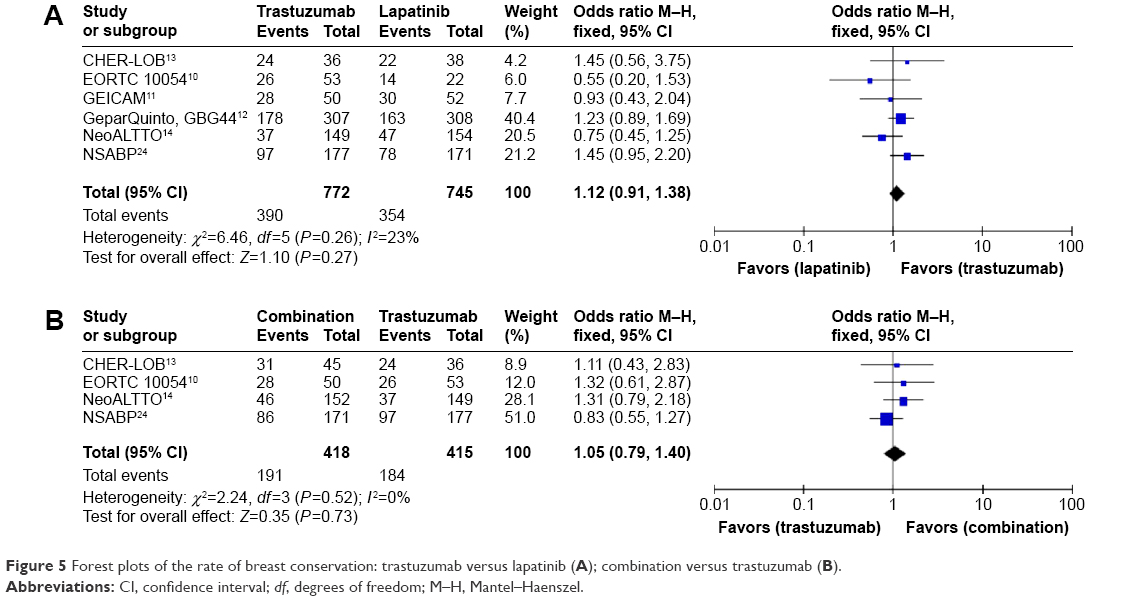 | Figure 5 Forest plots of the rate of breast conservation: trastuzumab versus lapatinib (A); combination versus trastuzumab (B). |
Toxicity studies
The main grade 3 and 4 toxic effects are summarized in Tables 3 and 4, and in Figure 6. After statistical analyses, the results showed that patients treated with lapatinib had more diarrhea, skin disorders, hepatic biochemical changes, infections, and inflammation (P<0.05) (Table 3, Figure 6). For the combination group, diarrhea, other digestive tract symptoms, hepatic biochemical changes, and skin disorders occurred much more than in patients treated with trastuzumab alone (Tables 3 and 4, Figure 6).
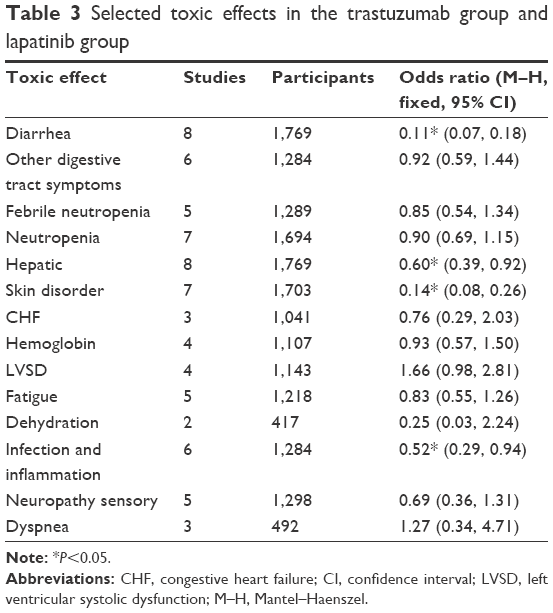 | Table 3 Selected toxic effects in the trastuzumab group and lapatinib group |
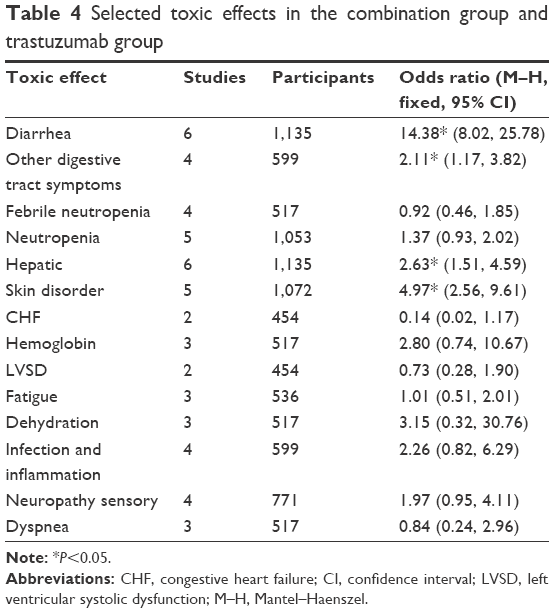 | Table 4 Selected toxic effects in the combination group and trastuzumab group |
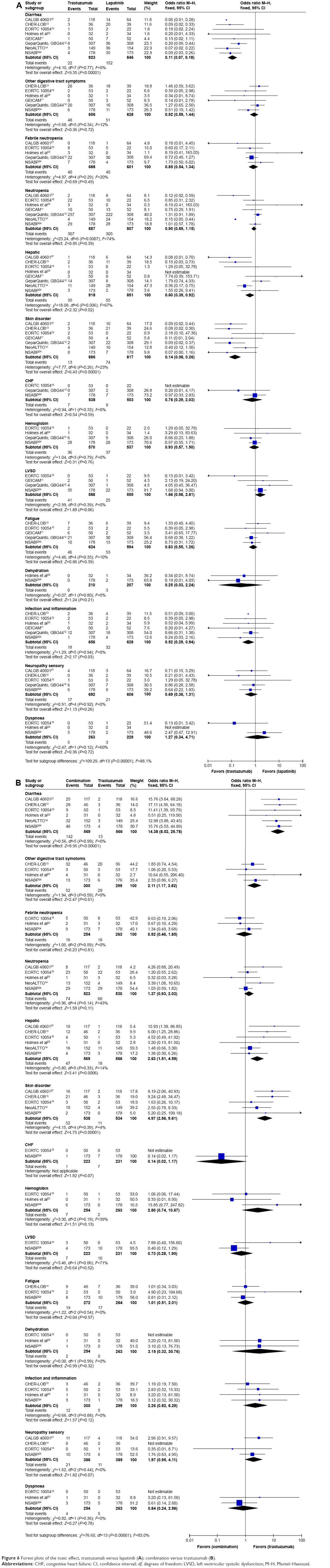 | Figure 6 Forest plots of the toxic effect, trastuzumab versus lapatinib (A); combination versus trastuzumab (B). |
Discussion
This study provides an analysis of the efficacy and safety of adding trastuzumab, lapatinib, or both to NAC in Her2-positive breast cancer patient treatments. Previous meta-analyses performed by Hicks et al9 showed an improvement in the pCR rate when lapatinib was combined with trastuzumab in patients receiving NAC. However, further analyses of the subgroups based on different HR status have not been performed. Furthermore, the toxic effects and breast conversation rates were not reported. In this study, we have updated the analysis by adding studies10–12 including the GEICAM/2006-14 trial, the GeparQuinto, GBG44 trial, and the EORTC 10054 study. In addition to including the pCR rates, we included the clinical responses, toxic effects, and the rates of breast conservation in the comparison analyses.
The overall pCR rate in the dual blockade of Her2 treatment groups was above 50%, while the CALGB 4060113 and NeoALTTO14 studies reported 46.7% and 46.9%, respectively. The different definitions of the pCR rate and statistical bias might be the causes of the discrepancy in these results. In our analyses of the combination groups, the pCR rates, both in breast and in breast with lymph nodes, were 57.6% and 54% respectively, and were found to be superior to the single-agent treated groups. In addition, the pCR rate of the trastuzumab group was reported in articles that compared the effects of trastuzumab versus lapatinib. In our analyses, trastuzumab gave higher efficacy compared to lapatinib. The results suggest an advantage of adding trastuzumab to NAC as a more effective method, versus lapatinib alone, and showed elevated pCR rates either in breast or in breast and lymph nodes. These results could be explained by the lower ability of lapatinib to block the HER2 pathway, the lower drug dose of lapatinib used, and the greater ability of trastuzumab to recruit immune cells that are responsible for antibody-dependent cytotoxicity15 and inhibition of angiogenesis.16
The use of the dual blockade of Her2 is supported by biological and clinical data. Trastuzumab and lapatinib are well-known drugs that inhibit the function of Her2 by different mechanisms.17 The expression product of the Her2 gene is an oncogenic membrane-spanning protein that is processed externally at membrane sites. Because of its specific overexpression in tumor cells, it can be used as a target antigen for breast cancer therapy. Trastuzumab, a monoclonal antibody to Her2, combines with the extracellular domain of Her2,18 thereby inducing the growth arrest of cells in G1 and the decrease of cell amplification. Regarding lapatinib, it can inhibit the tyrosine-kinase activity of both the epidermal growth factor receptor and ErbB-2 (Her2). This dual inhibitory activity can effectively prevent downstream signal transduction, thus preventing the proliferation of tumor cells. Taking the different mechanisms of drug action of trastuzumab and lapatinib into consideration, we suggest that the combination of these two drugs can provide a more optimal clinical curative effect.
Whether pCR can be used as a surrogate for disease-free survival rates in HER2-positive breast carcinomas, particularly those that are HR-positive, remains to be determined. Studies have confirmed that the higher the pCR rates, the better the disease-free survival and overall survival can be achieved; but this effect may be limited to HR-negative tumors.19 However, within the same group of Her2-positive patients, when accepting the same method of anti-Her2 therapy, the outcome (pCR) could vary. The differences in results obtained in the included studies were not due to statistical errors. Untch et al12 reported that the absence of HR expression was an important predictor of pCR. Therefore, we hypothesize that a relationship between HR state and the drug effects exists. Interestingly, when we set the subgroups according to HR status, a significant difference for the pCR was found only in the HR-negative subgroups. This indicated that some relationships existed between HR and Her2, or that resistance to anti-Her2 agents existed. A previous study20 showed impaired survival in patients with estrogen receptor-negative tumors. Estrogen receptor negativity has been reported to have a negative prognostic impact in breast cancer patients with Her2-positive tumors.21,22 Further exploration of interactions between HR and Her2 will help to evaluate prognosis and to guide future treatment strategies.
Regarding toxicity of the drugs, some grade 3 and 4 toxic effects, such as diarrhea and skin disorder were more common in the lapatinib and dual-drug treated groups. This suggests both advantages and disadvantages to the patients, with some severe toxic effects from treatments.
Some trials reported additional operative procedures10–12,14,23,24 for patients after NAC with anti-Her2 therapy. Although dual Her2 inhibition provides better pCR rates, this provides no significant improvement in the rate of breast conservation. Breast conservative therapy (BCT) is reported to provide long-term survival rates equivalent to those of total mastectomy.22 Tan et al25 performed a retrospective analysis in patients with breast malignancies and found that BCT was achieved in 85% of the patients with multifocal and multicentric breast cancer without evidence of poorer local control. Benediktsson and Perbeck26 reported a series of 216 patients who underwent conservative mastectomy with a long follow-up (median 13 years). The 10-year frequency of local recurrence rate was 8.5% when patients accepted radio therapy according to international guidelines. Because BCT provides better cosmetic results and improves the quality of life, it is necessary to identify the indications for BCT. In our analyses, there was no relationship between anti-Her2 therapy and BCT. However, considering the limited studies included here, further investigations are needed.
Conclusion
In our study, we found that the combination of trastuzumab and lapatinib was superior to single-agent treatment for improved pCR rate. However, combination treatment was not effective in improving the rate of breast conservation. Furthermore, a higher risk for toxicity was associated with combined administration. There are limitations to this study. First, only English language literature was included. Second, although we chose only the randomized clinical trials, there was relative heterogeneity in the study, especially when it came to analyzing the toxicity effects. Finally, the chemotherapy regimens used in the included articles were not the same, and this could be a cause of the differences in reported pCR rates among the included groups. Based on clinical requirements, a larger study, including more evidence to verify the conclusions proposed here, is required.
Disclosure
The authors report no conflicts of interest in this work.
References
Ross JS, Slodkowska EA, Symmans WF, Pusztai L, Ravdin PM, Hortobagyi GN. The HER-2 receptor and breast cancer: ten years of targeted anti-HER-2 therapy and personalized medicine. Oncologist. 2009;14:320–368. | ||
Olson EM. Maximizing human epidermal growth factor receptor 2 inhibition: a new oncologic paradigm in the era of targeted therapy. J Clin Oncol. 2012;30:1712–1714. | ||
Pegram MD, Finn RS, Arzoo K, Beryt M, Pietras RJ, Slamon DJ. The effect of HER-2/neu overexpression on chemotherapeutic drug sensitivity in human breast and ovarian cancer cells. Oncogene. 1997;15:537–547. | ||
Konecny GE, Venkatesan N, Yang G, et al. Activity of lapatinib a novel HER2 and EGFR dual kinase inhibitor in human endometrial cancer cells. Br J Cancer. 2008;98:1076–1084. | ||
Fisher B, Bryant J, Wolmark N, et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol. 1998;16:2672–2685. | ||
Moreno-Aspitia A, Dueck AC, Ghanem-Canete I, et al. RC0639: phase II study of paclitaxel, trastuzumab, and lapatinib as adjuvant therapy for early stage HER2-positive breast cancer. Breast Cancer Res Treat. 2013;138:427–435. | ||
Davies BR, Greenwood H, Dudley P, et al. Preclinical pharmacology of AZD5363, an inhibitor of AKT: pharmacodynamics, antitumor activity, and correlation of monotherapy activity with genetic background. Mol Cancer Ther. 2012;11:873–887. | ||
Burris HR, Hurwitz HI, Dees EC, et al. Phase I safety, pharmacokinetics, and clinical activity study of lapatinib (GW572016), a reversible dual inhibitor of epidermal growth factor receptor tyrosine kinases, in heavily pretreated patients with metastatic carcinomas. J Clin Oncol. 2005;23:5305–5313. | ||
Hicks M, Macrae ER, Abdel-Rasoul M, et al. Neoadjuvant dual HER2-targeted therapy with lapatinib and trastuzumab improves pathologic complete response in patients with early stage HER2-positive breast cancer: a meta-analysis of randomized prospective clinical trials. Oncologist. 2015;20:337–343. | ||
Bonnefoi H, Jacot W, Saghatchian M, et al. Neoadjuvant treatment with docetaxel plus lapatinib, trastuzumab, or both followed by an anthracycline-based chemotherapy in HER2-positive breast cancer: results of the randomised phase II EORTC 10054 study. Ann Oncol. 2015;26:325–332. | ||
Alba E, Albanell J, de la Haba J, et al. Trastuzumab or lapatinib with standard chemotherapy for HER2-positive breast cancer: results from the GEICAM/2006-14 trial. Br J Cancer. 2014;110:1139–1147. | ||
Untch M, Loibl S, Bischoff J, et al. Lapatinib versus trastuzumab in combination with neoadjuvant anthracycline-taxane-based chemotherapy (GeparQuinto, GBG 44): a randomised phase 3 trial. Lancet Oncol. 2012;13:135–144. | ||
Guarneri V, Frassoldati A, Bottini A, et al. Preoperative chemotherapy plus trastuzumab, lapatinib, or both in human epidermal growth factor receptor 2-positive operable breast cancer: results of the randomized phase II CHER-LOB study. J Clin Oncol. 2012;30:1989–1995. | ||
Baselga J, Bradbury I, Eidtmann H, et al. Lapatinib with trastuzumab for HER2-positive early breast cancer (NeoALTTO): a randomised, open-label, multicentre, phase 3 trial. Lancet. 2012;379:633–640. | ||
Weiner LM, Adams GP. New approaches to antibody therapy. Oncogene. 2000;19:6144–6151. | ||
Viloria-Petit A, Crombet T, Jothy S, et al. Acquired resistance to the antitumor effect of epidermal growth factor receptor-blocking antibodies in vivo: a role for altered tumor angiogenesis. Cancer Res. 2001;61:5090–5101. | ||
Konecny GE, Pegram MD, Venkatesan N, et al. Activity of the dual kinase inhibitor lapatinib (GW572016) against HER-2-overexpressing and trastuzumab-treated breast cancer cells. Cancer Res. 2006;66:1630–1639. | ||
Ahmed S, Sami A, Xiang J. HER2-directed therapy: current treatment options for HER2-positive breast cancer. Breast Cancer. 2015;22:101–116. | ||
Hamy-Petit AS, Belin L, Bonsang-Kitzis H, et al. Pathological complete response and prognosis after neoadjuvant chemotherapy for HER2-positive breast cancers before and after trastuzumab era: results from a real-life cohort. Br J Cancer. 2016;114:44–52. | ||
Duchnowska R, Wysocki PJ, Korski K, et al. Immunohistochemical prediction of lapatinib efficacy in advanced HER2-positive breast cancer patients. Oncotarget. 2016;7(1):550–564. | ||
Kennecke H, Yerushalmi R, Woods R, et al. Metastatic behavior of breast cancer subtypes. J Clin Oncol. 2010;28:3271–3277. | ||
Clarke M, Collins R, Darby S, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;366:2087–2106. | ||
Holmes FA, Espina V, Liotta LA, et al. Pathologic complete response after preoperative anti-HER2 therapy correlates with alterations in PTEN, FOXO, phosphorylated Stat5, and autophagy protein signaling. BMC Res Notes. 2013;6:507. | ||
Robidoux A, Tang G, Rastogi P, et al. Lapatinib as a component of neoadjuvant therapy for HER2-positive operable breast cancer (NSABP protocol B-41): an open-label, randomised phase 3 trial. Lancet Oncol. 2013;14:1183–1192. | ||
Tan MP, Sitoh NY, Sitoh YY. Optimising breast conservation treatment for multifocal and multicentric breast cancer: a worthwhile endeavour? World J Surg. 2016;40:315–322. | ||
Benediktsson KP, Perbeck L. Survival in breast cancer after nipple-sparing subcutaneous mastectomy and immediate reconstruction with implants: a prospective trial with 13 years median follow-up in 216 patients. Eur J Surg Oncol. 2008;34:143–148. | ||
Carey LA, Berry DA, Cirrincione CT, et al. Molecular heterogeneity and response to neoadjuvant human epidermal growth factor receptor 2 targeting in CALGB 40601, a randomized phase III trial of paclitaxel plus trastuzumab with or without lapatinib. J Clin Oncol. 2016;34(6):542–549. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.