")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 12
The efficacy of extrafine beclomethasone dipropionate–formoterol fumarate in COPD patients who are not "frequent exacerbators": a post hoc analysis of the FORWARD study
Authors Singh D, Vezzoli S, Petruzzelli S, Papi A
Received 9 May 2017
Accepted for publication 4 October 2017
Published 3 November 2017 Volume 2017:12 Pages 3263—3271
DOI https://doi.org/10.2147/COPD.S141416
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Dave Singh,1 Stefano Vezzoli,2 Stefano Petruzzelli,2 Alberto Papi3
1Medicines Evaluation Unit, University of Manchester, Manchester, UK; 2Chiesi Farmaceutici SpA, Parma, 3Section of Respiratory Diseases, University of Ferrara, Ferrara, Italy
Abstract: The GOLD 2017 strategy document recommends that the pharmacological management of COPD patients be based on the risk of future exacerbations and the severity of symptoms. A threshold of two moderate exacerbations or one hospitalization is used to define high-risk patients. The FORWARD study was a randomized, double-blind, parallel-group trial that compared 48 weeks’ treatment with extrafine beclomethasone dipropionate plus formoterol fumarate (BDP-FF) versus FF in severe COPD patients with a history of one or more exacerbations in the previous year. The new GOLD 2017 recommendations mean that many patients in the FORWARD study are now reclassified as GOLD B. We conducted a post hoc analysis of the FORWARD study, in order to investigate the effects of extrafine BDP/FF in patients with one exacerbation in the previous year, focusing on those categorized as group B using the GOLD 2017 definition. The analysis showed a 35% reduction in exacerbation rate with an inhaled corticosteroid (ICS) + long-acting β-agonist (LABA) versus LABA. We propose that ICS-LABA treatment is a therapeutic option for COPD patients with one exacerbation in the previous year.
Keywords: COPD, GOLD B, GOLD 2017, exacerbations, corticosteroid
Introduction
The GOLD 2017 strategy document recommends that the pharmacological management of COPD patients be based on the risk of future exacerbations and the severity of symptoms.1 Forced expiratory volume in 1 second (FEV1) has been removed as a criterion for identifying patients at high risk of exacerbation for pharmacological treatment decisions. A threshold of two exacerbations requiring antibiotics and/or corticosteroids or one hospitalization in the previous year is used as the sole criterion to identify patients at high risk of future exacerbations.
The ECLIPSE study showed that COPD patients with a history of one compared to zero exacerbations in the previous year were at increased risk of future exacerbations (OR 2.24, P<0.001).2 Other COPD cohorts have confirmed the increase in risk in patients with a history of one exacerbation in the previous year,3 supporting the case for treatment strategies to reduce future exacerbation risk in this subgroup of patients. However, GOLD has used two or more exacerbations, “frequent exacerbators”, as a threshold for preventive treatment, due to a greater level of risk (OR 5.72, P<0.001 in the ECLIPSE study).2
In line with the previous 2011 version, GOLD 2017 still recommends inhaled corticosteroid (ICS)–long acting β-agonist (LABA) combination inhalers for high-risk patients, ie, groups C and D,1 but not for patients at lower risk (groups A and B). However, clinical trials investigating the effects of ICS-LABA combinations on exacerbation prevention have often used inclusion criteria of FEV1 <50% predicted and one or more exacerbations in the previous year.4–6 Under the GOLD 2011 recommendations, most enrolled in these studies were high-risk patients because of low FEV1, as only a minority had had two or more exacerbations in the previous year. However, the removal of FEV1 from the risk assessment means that the patients enrolled in previous ICS/LABA clinical trials are a mixture of high- and low-risk patients using the GOLD 2017 definition.
The FORWARD study was a randomized, double-blind, parallel-group trial that compared 48 weeks’ treatment with extrafine beclomethasone dipropionate (BDP) 100 μg plus formoterol fumarate (FF) 6 μg with pressurized metered-dose inhaler (two inhalations twice daily) versus FF 12 μg with pressurized metered-dose inhaler (one inhalation twice daily).4 Severe COPD patients (FEV1 <50% predicted) with one or more exacerbations in the previous year were recruited. An important element of the design was that patients who had previously been taking the long-acting muscarinic antagonist (LAMA) tiotropium before screening were allowed to continue this treatment during the run-in period and after randomization to either BDP-FF or FF. This study demonstrated a significant and clinically relevant7 reduction in the rate of moderate–severe exacerbations (31% reduction using negative binomial model) and lung function improvement with BDP-FF compared to FF treatment. Moderate exacerbations were defined as events requiring treatment with oral CSs and/or antibiotics, while severe events required hospitalization.
The majority of patients in the FORWARD study did not meet the GOLD 2017 criteria for high exacerbation risk, as they had had one exacerbation in the previous year. While ICS-LABA treatments are not recommended by GOLD 2017 for such patients, the known increase in exacerbation risk in these patients indicates that treatments designed to prevent exacerbations should be considered. We conducted a post hoc analysis of the effects of extrafine BDP-FF in patients with one exacerbation in the previous year in the FORWARD study. We focused on patients with a higher level of symptoms who would be classified as GOLD B patients.
Materials and methods
The full design and results of the study have been published (registered at ClinicalTrials.gov, NCT00929851).4 The study was approved by the ethics committee or institutional review board at each site (Tables S1–S3) and was done in accordance with the Declaration of Helsinki, International Conference on Harmonisation Good Clinical Practice (ICH/CPMP/135/95), and applicable local regulations. All patients provided written informed consent before any study-related procedure.
The COPD assessment test (CAT) and modified Medical Research Council (mMRC) scores were not collected at screening. We used the St George’s Respiratory Questionnaire (SGRQ) to identify patients with greater symptoms using a threshold of ≥25 as previously described.8 This was called analysis 1. To provide confirmation of these results, we performed analysis 2, using items regarding breathlessness within the SGRQ that identify patients with dyspnea corresponding to mMRC scores ≥2. The SGRQ questions were those about “what activities usually make subjects feel breathless” and those about “how activities may be affected by their breathing”. Answers indicating greater dyspnea than others of the same age or dyspnea while walking on level ground/needing to rest were used to identify dyspnea corresponding to mMRC scores ≥2.
Information on the number of exacerbations (requiring oral CSs and/or antibiotics) in the last year was available for each patient, but the specific number of these events resulting in hospitalization was not registered. A threshold of two exacerbations was used to define high-risk patients (GOLD C or D). Using the GOLD 2017 classification, 716 patients in analysis 1 (60.4% of 1,186 patients included in the intention-to-treat population) were categorized as GOLD B, with 87 (7.3%), 25 (2.1%), and 313 (26.4%) categorized as GOLD A, C, and D, respectively, while for 45 patients the category could not be assessed. There were similar proportions for analysis 2: 662 patients (55.8%) were GOLD B, with 160 (13.5%), 44 (3.7%), and 301 (25.4%) categorized as GOLD A, C, and D, respectively, while for 19 patients the category could not be assessed. In each GOLD group, the same approach for statistical analysis as originally used in the overall population was followed. The number of COPD exacerbations and predose morning FEV1 were analyzed using a negative binomial model and a mixed model for repeated measures, respectively.4 Stratified analyses according to the concomitant use of tiotropium were additionally performed.
Results
For analysis 1, in GOLD B patients, adjusted exacerbation rates were 0.67 and 1.04 events/patient/year with BDP-FF and FF, respectively (Figure 1), with an adjusted RR of 0.65 (P<0.001) in favor of BDP-FF (Table 1). Similar results were obtained for patients using tiotropium or no tiotropium (adjusted RR 0.54 and 0.76, respectively), although the latter was not statistically significant (P=0.119). Analysis 2 in GOLD B patients gave similar results: adjusted exacerbation rates were 0.71 and 1.09 events/patient/year with BDP-FF and FF, respectively (Figure 2), with an adjusted RR of 0.65 (P<0.001) in favor of BDP-FF. Effects of tiotropium versus no tiotropium use gave adjusted RRs of 0.58 and 0.7, respectively, with the latter again not reaching statistical significance (P=0.054).
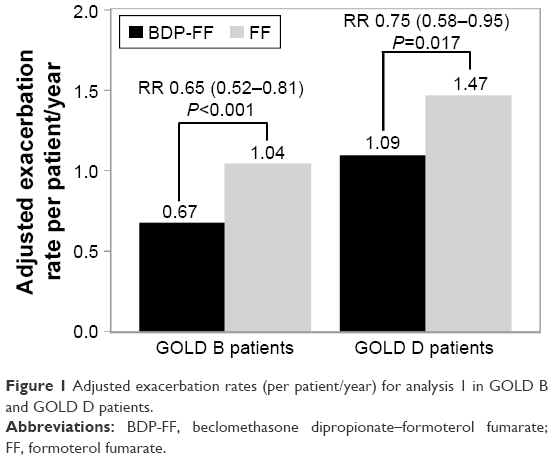 | Figure 1 Adjusted exacerbation rates (per patient/year) for analysis 1 in GOLD B and GOLD D patients. |
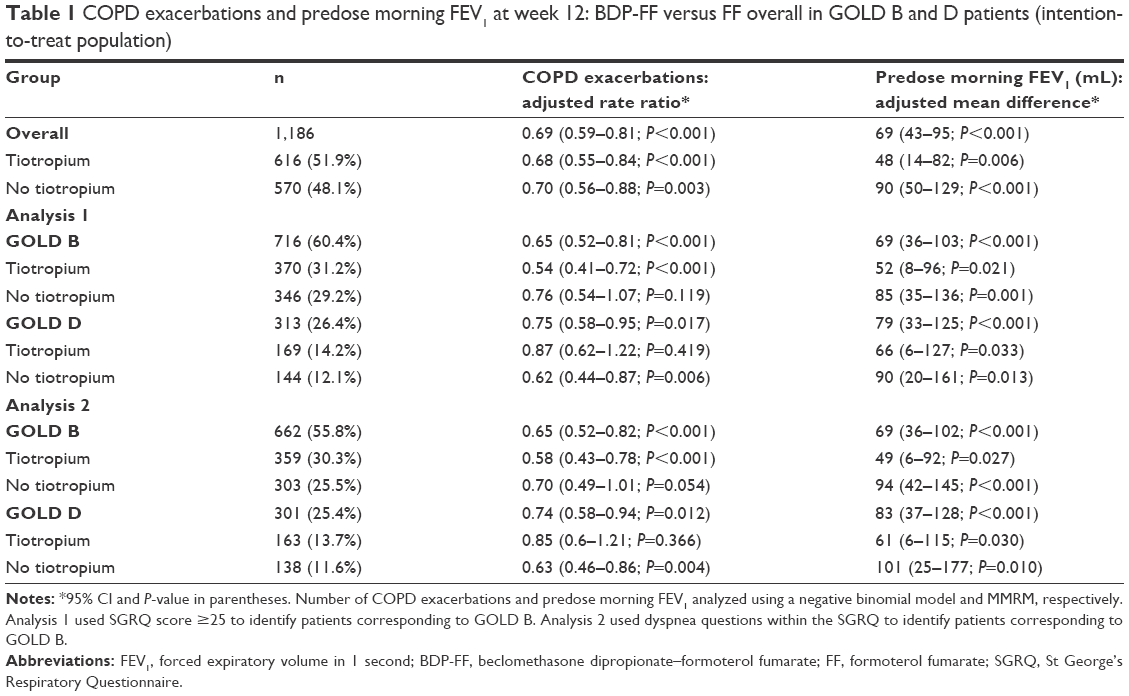 | Table 1 COPD exacerbations and predose morning FEV1 at week 12: BDP-FF versus FF overall in GOLD B and D patients (intention-to-treat population) |
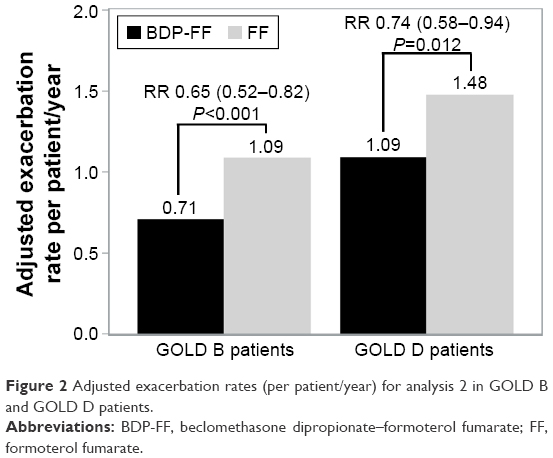 | Figure 2 Adjusted exacerbation rates (per patient/year) for analysis 2 in GOLD B and GOLD D patients. |
For analyses 1 and 2, in GOLD B patients the adjusted mean difference in predose FEV1 at week 12 was 69 mL (P<0.001) in favor of BDP-FF compared to FF. This significant difference between treatments was present in both analyses, irrespective of tiotropium use. Analyses for the overall population and GOLD D patients are shown in Table 1 and Figures 1 and 2. The number of exacerbations/patient/year was higher in GOLD D compared to GOLD B patients, but treatment effects were similar in these two groups for both FEV1 changes and exacerbation rate reduction.
Discussion
This post hoc analysis focused on COPD patients with one exacerbation in the previous year and a high burden of symptoms. There was a 35% reduction in exacerbation rate with ICS-LABA compared to LABA. GOLD B consists of patients with no or one exacerbation in the previous year. The future exacerbation risk is higher in the subgroup with one event in the previous year,3,4 and we provide evidence for the efficacy of ICS-LABA over LABA alone in these patients.
It has been shown that some GOLD B patients are at high risk of rapid disease progression.9 The factors known to be associated with a greater decline in lung function include current smoking, emphysema, and exacerbations.10 GOLD B is clearly a heterogeneous patient group, and the data presented here support the use of ICS-LABA in a subset of GOLD B.
We used the SGRQ to identify patients with a higher symptom burden and categorized these patients as GOLD B. The SGRQ threshold of 25 has been used previously for this purpose.8 We realize that this methodology does not strictly match the GOLD B definition based on CAT or mMRC scores, but it is a recognized way to identify patients with a greater level of symptoms. We performed an analysis using specific questions within the SGRQ to identify patients with greater breathlessness. The two different analyses provided very similar results.
Although we knew how many overall exacerbations occurred in the previous year, the number of these that required hospitalization was not known. It is thus likely that some patients categorized as GOLD B here were really GOLD D patients. These were likely to be only a small proportion of individuals, as hospitalizations occur in a minority of exacerbations. We suggest that this reclassification would not have altered the results, as the results in GOLD B and D were similar.
This post hoc analysis has limitations in terms of the definition of GOLD B patients. Furthermore, the smaller sample sizes of the subgroups analyzed results in a decrease in statistical power. Caution must thus be applied to the interpretation of these data. Nevertheless, these results provide a level of evidence to debate the place of ICS-LABA treatment for patients with a history of one exacerbation.
The FORWARD study was conducted in severe COPD patients being followed up, with approximately half taking tiotropium. A subanalysis of GOLD B patients according to concurrent tiotropium use showed efficacy for additional ICS therapy on exacerbations and lung function in both patients using a LABA alone and those using a LABA plus LAMA. Exacerbation rate reductions of 24% and 30% (analyses 1 and 2, respectively) due to ICS in patients not using tiotropium were not statistically significant (P=0.119 and P=0.054), and we suggest this was due to a relatively small sample size in a subgroup. Nevertheless, the overall pattern of results on exacerbations and FEV1 in GOLD B patients with one exacerbation in the previous year support the addition of an ICS to either LABA monotherapy or LABA plus LAMA treatment. Indeed, the significant exacerbation reduction in both analyses for patients taking triple therapy (BDP-FF plus tiotropium) versus LABA-LAMA treatment (FF plus tiotropium) indicates the potential effectiveness of triple therapy in a subset of GOLD B patients.
GOLD recognizes that some of its recommendations lack evidence and may require refinement or alteration as new evidence becomes available.1,11 We provide some evidence to debate the current use of inhaled medicines in patients with a history of one exacerbation, particularly those corresponding to the definition of GOLD B. We propose ICS-LABA treatment is a therapeutic option in the subset of GOLD B patients with one exacerbation in the previous year.
Acknowledgments
We acknowledge Elisa Veratelli (University of Ferrara, Ferrara, Italy) for scientific editorial assistance in the preparation of the manuscript. This study received funding support from Chiesi Farmaceutici, Parma, Italy.
Disclosure
DS reports personal fees from Apellis, Cipla, and Peptinnovate; and grants and personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Glenmark, Merck, Mundipharma, Novartis, Pfizer, Pulmatrix, Teva, Theravance, Verona, Genentech, and Skyepharma. SP and SV are employees of Chiesi Farmaceutici. AP reports grants and/or personal fees from Chiesi, AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Merck Sharp and Menarini, Novartis, Zambon, Pfizer, Dohme, Takeda, Mundipharma, Teva, and Sanofi.
References
Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 report: GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. | ||
Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. | ||
Keene JD, Jacobson S, Kechris K, et al. Biomarkers predictive of exacerbations in the SPIROMICS and COPDGene Cohorts. Am J Respir Crit Care Med. 2017;195(4):473–481. | ||
Wedzicha JA, Singh D, Vestbo J, et al. Extrafine beclomethasone/formoterol in severe COPD patients with history of exacerbations. Respir Med. 2014;108(8):1153–1162. | ||
Calverley PM, Boonsawat W, Cseke Z, Zhong N, Peterson S, Olsson H. Maintenance therapy with budesonide and formoterol in chronic obstructive pulmonary disease. Eur Respir J. 2003;22(6):912–919. | ||
Sharafkhaneh A, Southard JG, Goldman M, Uryniak T, Martin UJ. Effect of budesonide/formoterol pMDI on COPD exacerbations: a double-blind, randomized study. Respir Med. 2012;106(2):257–268. | ||
Calverley PM. Minimal clinically important difference: exacerbations of COPD. COPD. 2005;2(1):143–148. | ||
Han MK, Muellerova H, Curran-Everett D, et al. GOLD 2011 disease severity classification in COPDGene: a prospective cohort study. Lancet Respir Med. 2013;1(1):43–50. | ||
Lawrence PJ, Kolsum U, Gupta V, et al. Characteristics and longitudinal progression of chronic obstructive pulmonary disease in GOLD B patients. BMC Pulm Med. 2017;17(1):42. | ||
Vestbo J, Edwards LD, Scanlon PD, et al. Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med. 2011;365(13):1184–1192. | ||
Singh D. Pharmacological treatment for COPD: GOLD 2017 changes direction. Br J Clin Pharmacol. 2017;83(5):935–937. |
Supplementary materials
 | Table S1 IECs/IRBs for recruitment wave 1 |
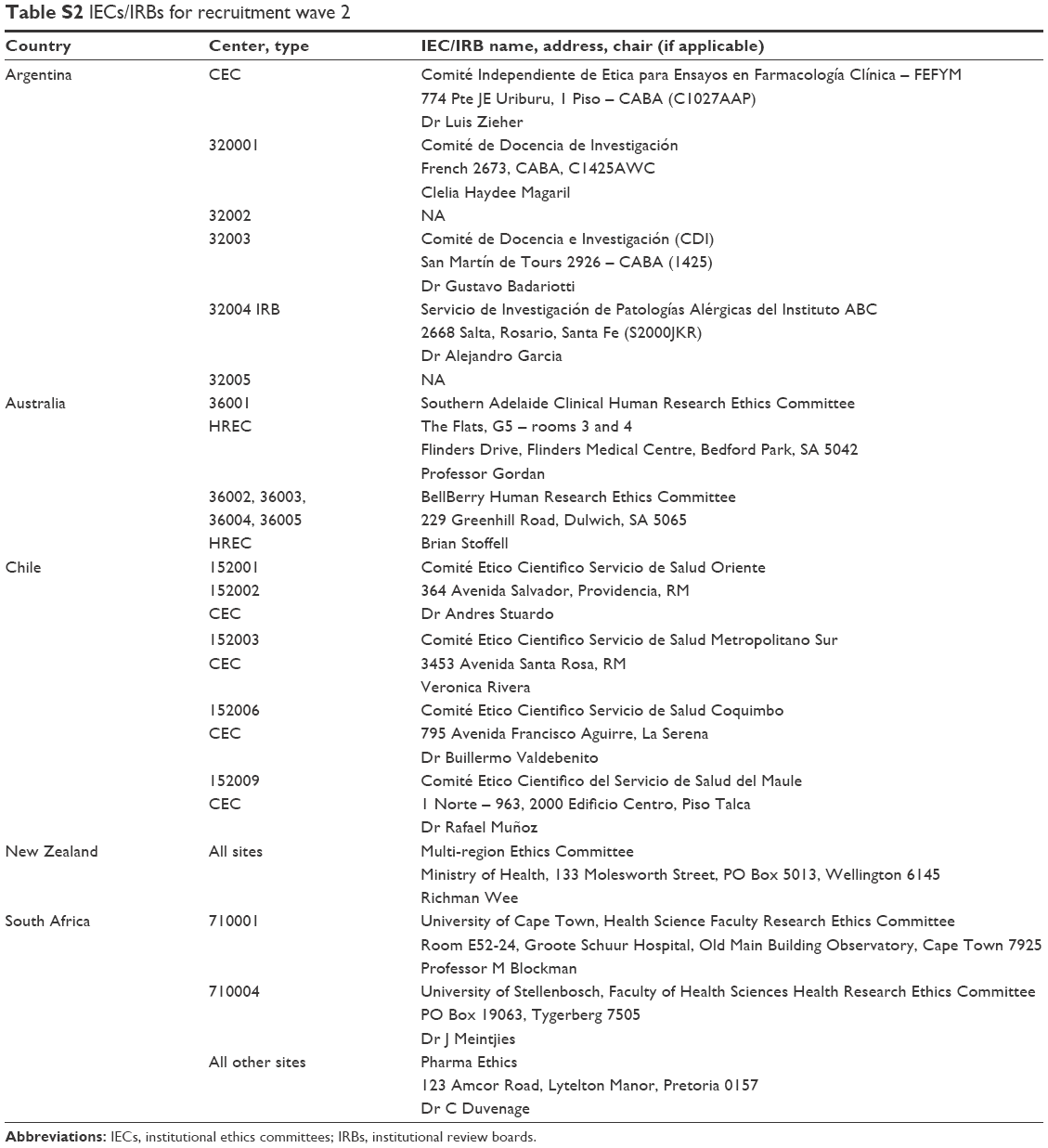 | Table S2 IECs/IRBs for recruitment wave 2 |
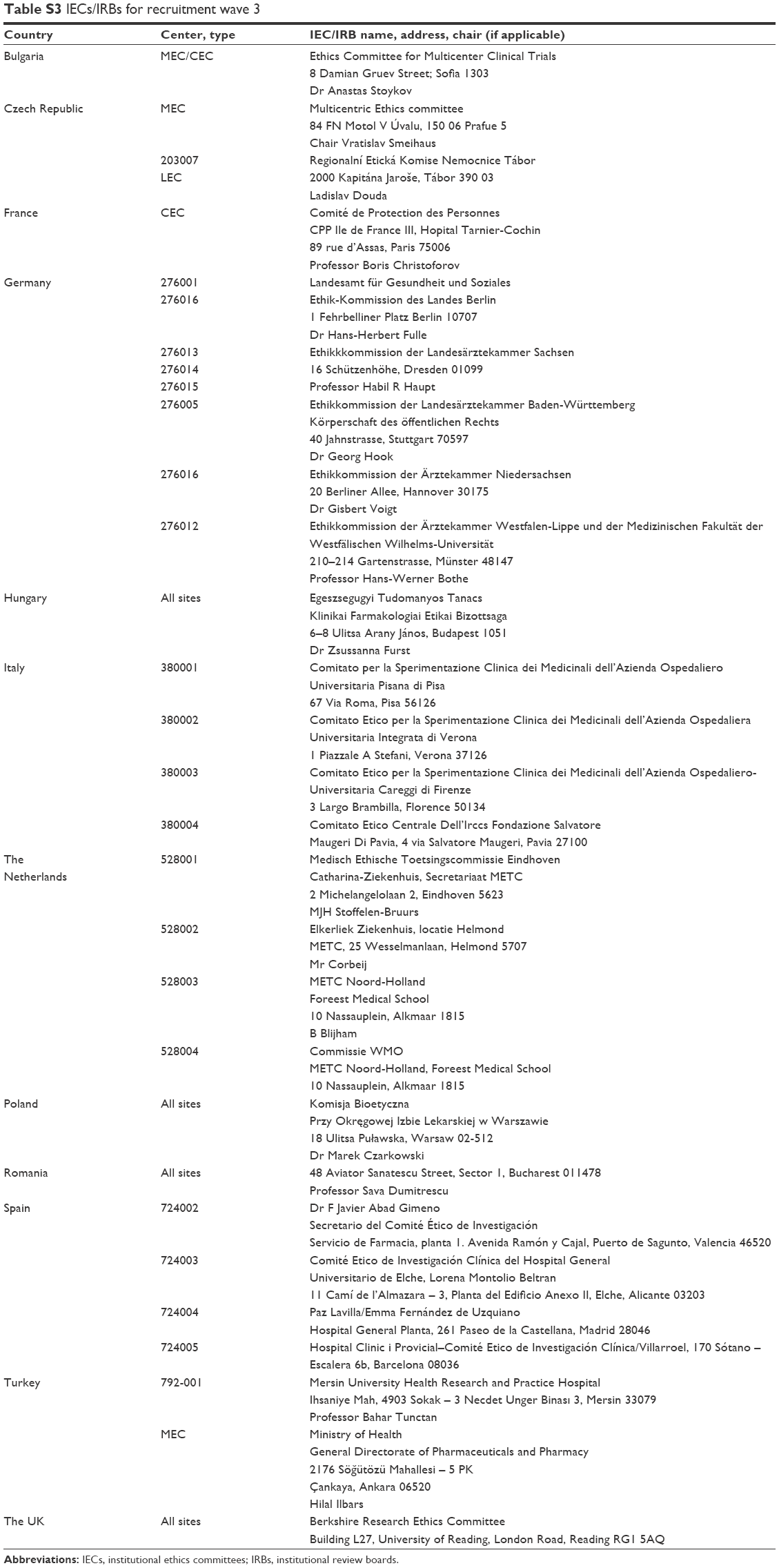 | Table S3 IECs/IRBs for recruitment wave 3 |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.