")
Back to Journals » Journal of Pain Research » Volume 15
The Efficacy and Safety of Acupuncture for Depression-Related Insomnia: Protocol for a Systematic Review and Meta-Analysis
Authors Hu H , Li Z, Cheng Y, Gao H
Received 13 April 2022
Accepted for publication 2 July 2022
Published 13 July 2022 Volume 2022:15 Pages 1939—1947
DOI https://doi.org/10.2147/JPR.S370476
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Hantong Hu,1,2,* Zengtu Li,3,* Yingying Cheng,1,2,* Hong Gao1,2
1Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China; 2Department of Neurobiology and Acupuncture Research, the Third Clinical Medical College, Zhejiang Chinese Medical University, Key Laboratory of Acupuncture and Neurology of Zhejiang Province, Hangzhou City, People’s Republic of China; 3Department of Massage, the Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong Gao, Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, No. 219 Moganshan Road, Xihu District, Hangzhou City, People’s Republic of China, Email [email protected]
Background: There is a bidirectional relationship between depression and insomnia. Depression-related insomnia is common and remains a challenging medical condition. Although acupuncture might be a potential treatment option and increasing randomized controlled trials (RCTs) have emerged, currently available evidence regarding the effect and safety of acupuncture on depression-related insomnia remains inconclusive. Thus, this protocol aims to systematically synthesize the evidence about the efficacy and safety of acupuncture for depression-related insomnia.
Methods and Analysis: Eligible RCTs will be searched in nine representative databases and pooled in meta-analyses using RevMan 5.3. The methodological quality of included studies will be rated by Cochrane’s risk of bias 2.0 tool. The quality of evidence will be appraised using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach. Subgroup analysis, sensitivity analyses, and publication bias will also be conducted.
Discussion: This protocol outlines the planned scope and methodology for an upcoming systematic review meta-analysis, which will critically synthesize the evidence about the efficacy and safety of acupuncture on depression-related insomnia. Findings will shed light on fulfilling evidence gaps and influence evidence-based treatment decisions for clinicians in the treatment of depression-related insomnia.
Keywords: acupuncture, depression-related insomnia, systematic review, meta-analysis
Introduction
Rationale
Insomnia is featured with reduced sleep quality or quantity, difficulty falling asleep, frequent nighttime awakenings, and/or early morning awakenings. It is widely accepted that there is a close relationship between depression and insomnia. Specially, abnormal changes in the normal sleep–wake cycle are frequently reported in patients with depression, and in many cases, sleep disturbance is the major complaint of depression.1 Given that depression can significantly affect the normal sleep structure, persistent insomnia is one of the most prominent symptoms in depressive patients.2 It is reported that approximately 60–80% of the depressive patients suffer from persistent insomnia.3 What is worse, reduced sleep quality and quantity may persist even if depressive symptoms have been adequately relieved.
In recent years, the bidirectional association between depression and insomnia has been further investigated. Insomnia can increase the risk of depression, which in turn raises the risk of developing and worsening insomnia. The emerging new perspective regards that insomnia is not only an epiphenomenon of depression but also a prodromal symptom with significant predictive value.4 Therefore, it is now considered that persistent insomnia is an independent diagnostic entity that may precipitate the onset and development of depressive disorders.4 Relieving insomnia improves clinical outcomes of depression.5 In such situations, increasing attention has been paid to the sleep-specific treatment needs for patients with depression.
Notably, depressive patients who suffer from clinically significant insomnia tend to present more severe symptoms and treatment difficulties,6 making them a particularly challenging group to treat.7 At present, the treatment of depression-related insomnia is mainly based on pharmacological treatment, complemented with cognitive behavioral therapy (CBT) and other treatments.8–10 Although pharmacological treatment, represented by antidepressants and sedative-hypnotics, can improve the efficacy and prognosis in the treatment, the application of drugs is often limited by inevitable side effects, such as nausea, addiction, tolerance, and excessive sedation.11,12 Some kinds of antidepressants can cause daytime sleepiness or even worsen insomnia,13 and high hypnotic dosages for insomnia are closely related to worse outcomes for depression.14 Additionally, CBT can be a beneficial option for depression-related insomnia, but a high proportion of patients, especially in developing countries, have no access to them due to cultural barriers, unaffordable expenses, and lack of qualified psychotherapists.15 Taken together, the currently available therapies for depression-related insomnia remain unsatisfactory. In such a scenario, an increasing number of patients diagnosed with insomnia seek complementary and alternative medicine (CAM) to treat their condition.16
As an important component of CAM, acupuncture has been widely utilized to ameliorate both depressive moods and sleep disturbance, which includes multiple modalities of acupuncture, such as manual acupuncture, electroacupuncture, and auricular acupuncture. For example, evidence based on a previous systematic review and meta-analysis revealed a positive effect of auricular acupuncture for insomnia.17 An RCT study revealed that auricular acupuncture could effectively reduce the dosage of antidepressants, reduce the incidence of withdrawal syndromes of antidepressants, and reduce the long-term recurrence rate in patients with depression.18 Nevertheless, the vast majority of previous studies focused on either acupuncture for treating insomnia or that for treating depression,19 the therapeutic effect of acupuncture on depression-related insomnia remains uncertain. Therefore, a growing number of randomized controlled trials (RCTs)20–24 have been conducted to verify whether acupuncture is effective and safe for depression-related insomnia. However, their results are conflicting. Some studies yield favorable results, revealing that acupuncture is beneficial for depression-related insomnia.20–22 For example, a recently published RCT20 in 2020 suggested that the efficacy of acupuncture on depression-related insomnia was superior to two sham acupuncture groups after 8-weeks of treatment. But other trials demonstrate that the efficacy of acupuncture was only mild and similar to that of minimal acupuncture and placebo acupuncture for treating insomnia associated with major depressive disorder.23,24 Furthermore, some RCTs19,25 with sound methodology in this field are still ongoing and their future results are worth looking forward to. For example, an ongoing RCT conducted by Yin et al19 aims to investigate the therapeutic effect of electroacupuncture in treating depression-related insomnia, and it is strictly schemed with a blinded and multicentre design, long intervention and follow-up period, large sample sizes, and objective outcome measures for insomnia.
Taken together, it is urgent to critically synthesize the evidence regarding the efficacy and safety of acupuncture for depression-related insomnia.
Objectives
The current protocol outlines the planned scope and methods for an upcoming systematic review meta-analysis. The objective of this protocol is to critically assess the evidence about the efficacy and safety of acupuncture for depression-related insomnia. It is expected to influence evidence-based treatment decisions and guide new studies to fulfill the current evidence gap in the management of this challenging disease.
Methods and Analysis
This protocol for a systematic review and meta-analysis has been rigorously designed following guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P),26 as displayed in the PRISMA-P checklist (Supplementary Table 1). To improve transparency, we have also registered this protocol in the International Prospective Register of Systematic Reviews (PROSPERO) with the identification number CRD42022309955.
Eligibility Criteria
The eligibility criteria for the included trials will be in accordance with the following PICOS elements.
Participants
Participants with a definitive diagnosis of depression-related insomnia will be eligible regardless of age, gender, and country. The standard diagnostic criteria of insomnia should be provided in the original RCT, such as the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition (DSM-IV),27 or Fifth Edition (DSM-5)28), the Third version of the International Classification of Sleep Disorders (ICSD-3),29 the Chinese Classification of Mental Disorders (CCMD),30 etc. In addition, insomnia is related to depression by providing the diagnostic criteria of depression in the original RCT, such as the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition (DSM-IV),27 Fifth Edition (DSM-5)28), the International Statistical Classification of Diseases and Related Health Problems (ICD),31 the Chinese Classification of Mental Disorders (CCMD),30 etc.
Interventions
Acupuncture therapy should be adopted in the experimental group. Acupuncture can be either used alone in the experimental group or combined with other active therapies that are the same as the control group. Notably, in order to reduce heterogeneity among included trials from the clinical perspective, in this study acupuncture therapy is defined as those acupuncture techniques involving the insertion of needles, including electroacupuncture, manual acupuncture, auricular acupuncture, warming-needle moxibustion, intradermal needling, and so on. Therefore, acupuncture techniques that do not puncture the skin are excluded, such as acupressure, laser acupuncture, and transcutaneous electrical acupoint stimulation.
Comparators
- Active therapies that are recommended by clinical guidelines,32–34 such as pharmacological treatment (eg, antidepressants and sedative-hypnotics), CBT, sleep hygiene, music therapy, light therapy, physical activity, and relaxation techniques.
- Placebo controls: sham acupuncture, placebo drugs.
- No treatment or waiting list.
Outcomes
We refer to similar studies10,35 to determine outcomes of interest. Thus, eligible trials should report at least one of the following outcomes.
Primary Outcome
Sleep quality measured by validated self-reported questionnaires such as Pittsburgh Sleep Quality Index (PSQI) and Insomnia Severity Index (ISI), and/or device-recorded objective sleep parameters, such as total sleep time, sleep efficiency (ie, the percentage of sleep time relative to the time spent in bed), sleep onset latency, and wake after sleep onset.
Secondary Outcomes
- Depression measured by standardized questionnaires with established validity, such as Beck Depression Inventory (BDI) and Hamilton Depression Scale (HAMD).
- Anxiety measured by standardized questionnaires with established validity, such as Hamilton Anxiety Scale (HAMA).
- Adverse events.
- Quality of life (QOL) measured by standardized questionnaires with established validity, such as the Short Form 36 (SF-36).
- Effective rate of treatment, which is often reported in Chinese acupuncture trials and is generally divided into three levels (ie, clinical cure, effectiveness, and invalid) according to different syndrome improvement degrees.
Study Designs
Only randomized control trials (RCTs) will be included (with or without blinding, including crossover design and pragmatic trials) if they aim to investigate the efficacy of acupuncture for depression-related insomnia. If crossover trials are included, only the initial results of the experimental group versus the control group before crossover will be considered for meta-analysis.36 Publication language is limited to English and Chinese. Case series, reviews, and other types of non-randomized controlled trials will be excluded.
Information Sources
We will conduct a systematic search in five English-language databases (PubMed, EMBASE, Web of Science, Physiotherapy Evidence Database (PEDro), and Cochrane Central Register of Controlled Trials) and four Chinese-language databases (Chinese National Knowledge Infrastructure, Chinese Biomedical Literature Database, VIP Database for Chinese Technical Periodicals, and Wangfang database). All databases will be searched for RCTs from the data inception to September 2022.
Search Strategy
The retrieval strategy mainly consists of three components: study designs (randomized clinical trial), participants (eg, depression-related insomnia; depression-associated insomnia, comorbid depression and insomnia, sleep disorders, insomnia, sleep disturbance, depression, depressive disorders), and interventions (eg, electroacupuncture, manual acupuncture, scalp acupuncture, and auricular acupuncture). The aforementioned English-language search terms will be used individually or combined in English databases. Corresponding Chinese-language search terms will be used in Chinese databases. To obtain the highest sensitivity, the search strategy will adopt a combination of subject terms (eg, Medical Subject Headings [MeSH] for PubMed) and free-text terms. The retrieval strategy for PubMed (as presented in Table 1) will be adjusted for other databases by replacing MeSH terms with proper subject terms (if available) and maintaining the same free-text terms.
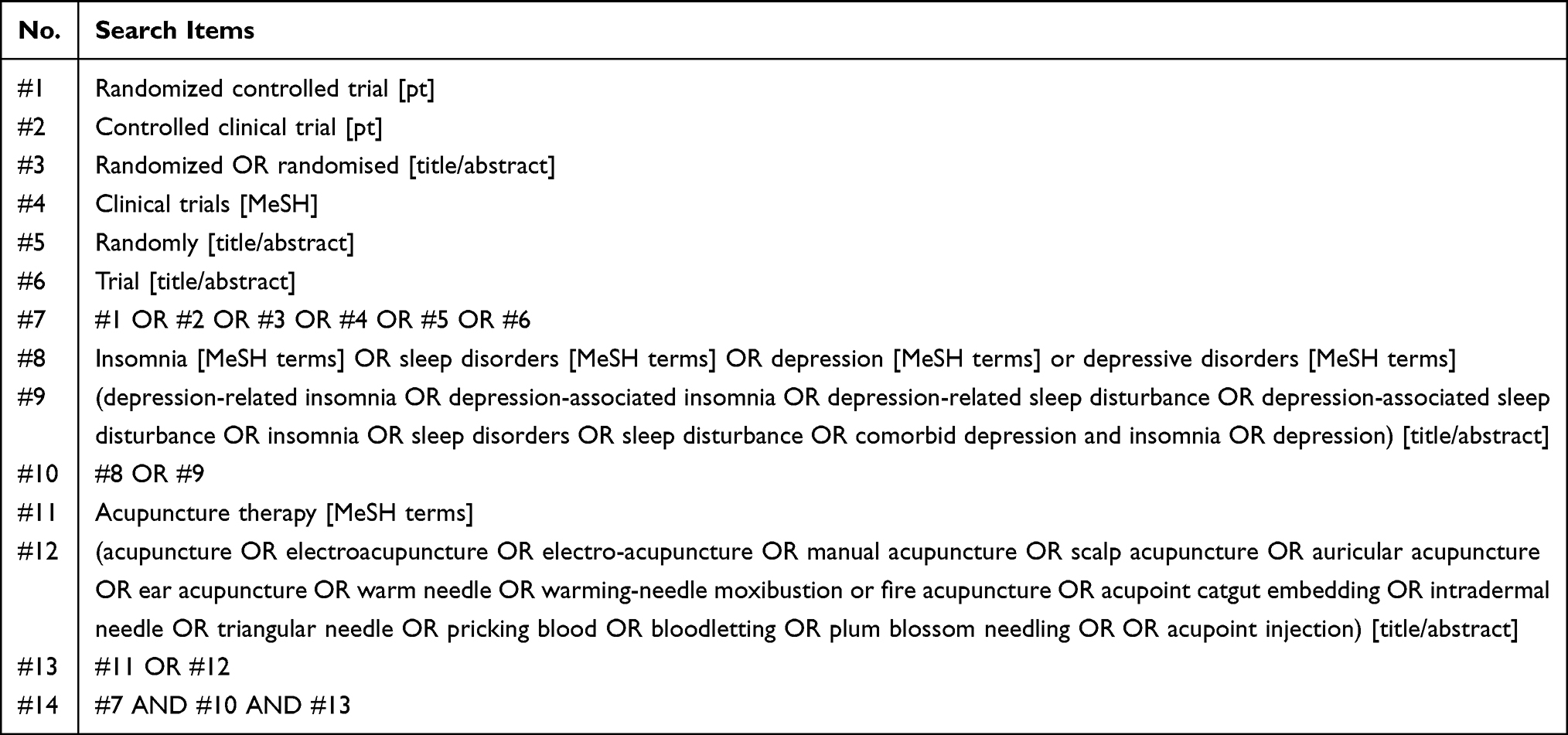 |
Table 1 Search Strategy in PubMed |
In addition, reference lists of previously published systematic reviews will also be manually searched to avoid potential omissions of eligible RCTs. For future updates of this review, the following clinical trials registry platforms will also be searched to identify relevant ongoing trials, including Clinical Trials Registry (https://clinicaltrials.gov/), the World Health Organization’s International Clinical Trials Registry Platform (https://www.who.int/clinical-trials-registry-platform), and Chinese Clinical Trial Registry (http://www.chictr.org.cn).
Study Selection Process
All search records generated by databases will be imported into Mendeley Reference Manager (Mendeley, Elsevier, the Netherlands) to delete duplicate records. During study selection, two independent reviewers (Z.L and L.W) will firstly scan publication titles and abstracts to determine potentially qualified RCTs based on the aforementioned inclusion/exclusion criteria. For potentially qualified studies, a full copy of publications will be downloaded to further confirm eligibility. Should any between-reviewer disagreement for study inclusion arise, it will be settled through discussion with another senior reviewer (H.G). The flow diagram of the study selection is summarized in Figure 1.
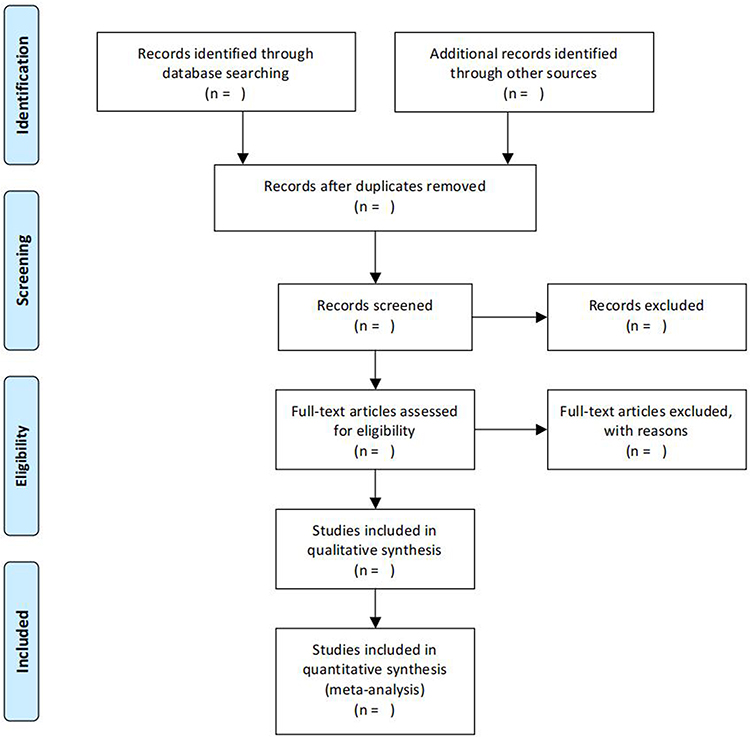 |
Figure 1 Flow diagram of study selection. |
Data Extraction and Data Items
After all eligible RCTs are included, two independent reviewers (H.H and Y.C) will adopt a pre-defined electronic form to extract relevant information in terms of author names, publication year, study designs, study population characteristics, sample sizes, interventions, control types, treatment durations, the total number of treatment sessions, outcomes, etc (as shown in Supplementary Table 2). Regarding continuous outcomes, means and standard deviations (SDs) will be extracted. In cases where continuous outcomes are shown in other forms (eg, median [interquartile range], mean [95% CI]), they will be converted to means (SDs) based on the method recommended by the Cochrane Handbook for Systematic Reviews of Interventions.37 Regarding dichotomous outcomes, the number of responders and the total number of subjects in each study group will be obtained. If corresponding data are unavailable in original publications, reviewers will contact the corresponding authors for missing data by sending emails. Any between-reviewer disagreements will be resolved by consulting another senior reviewer (H.G).
Notably, before full-scale data extraction for all included studies, inter-rater agreements on data extraction will be assessed via kappa coefficients by extracting data for 10 randomly selected studies. Once inadequate inter-rater consistency and accuracy have arisen, additional training on data extraction will be executed.
Methodological Quality Assessment
Two independent reviewers (H.H and Y.C) will appraise the methodological quality of each included RCT in accordance with the Cochrane’s risk of bias 2.0 (RoB 2.0) tool.38 The ROB of each included study will be rated in terms of five key domains, namely (1) randomization process; (2) deviations from intended interventions; (3) missing outcome data; (4) measurement of the outcome; and (5) selection of the reported result. Each domain will be classified as “low”, “high”, or ‘some concerns’. Besides, reviewers will also rate the overall ROB for individual trials as “low” (ie, ROB is low for all domains), ‘some concerns’ (ie, some concerns in at least one domain), or “high” (ie, high ROB for at least one domain or some concerns for multiple domains). All between-reviewer discrepancies will be resolved by negotiations with the third senior reviewer (HG).
Data Synthesis and Statistical Analysis
Meta-analysis of pooled studies with available data will be conducted by calculating the effect size and 95% CI using the RevMan software program (Version 5.30, Cochran Collaboration, London, England). Given the expected heterogeneity among different acupuncture protocols for the included studies, the random effects model will be adopted for meta-analyses. Heterogeneity across all the included trials will be identified by the χ2 test and reported as I2 statistic value, in which an I2 value greater than 50% is considered to be substantially heterogeneous. Pooled effects will be measured and a two-sided P value less than 0.05 is regarded as statistical significance. In addition, sensitivity analyses will be undertaken to evaluate the robustness of the meta-analysis results of the primary outcome using the leave-one-out approach.
Subgroup Analysis
If it is available and possible, we will conduct subgroup analyses in terms of the following factors.
- Types of acupuncture (eg, manual acupuncture, electro-acupuncture).
- Types of control arms (eg, active controls, sham controls).
- Measuring time points of primary outcomes.
Assessment for the Quality of Evidence
The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach will be used to evaluate the quality of evidence for primary outcomes included in meta-analyses. The quality of evidence will be summarized by an overall “certainty of evidence” grading, which is divided into four grades, namely (1) high; (2) moderate; (3) low; and (4) very low).39
Publication Bias
If at least 10 trials are included, publication bias will be examined by the Egger test and funnel plots for asymmetry.
Ethical Consideration
Given that a systematic review and meta-analysis will not involve the private information of individuals, ethical approval is not required for this study.
Discussion
It has been increasingly accepted that there is a bidirectional relationship between depression and insomnia.4 Despite conventional treatment approaches, depression-related insomnia remains a challenging medical condition. Previous studies indicate that acupuncture is a potential therapeutic strategy for depression-related insomnia.10,40 Although the mechanisms underlying acupuncture for treating depression-related insomnia are not fully elucidated, as a key component of traditional Chinese medicine, acupuncture is likely to work through multi-level and multi-target pathways, and the therapeutic effect of acupuncture on depression-related insomnia is possibly mediated through a variety of actions and mechanisms, such as modulating neurotransmitter, oxidative stress, signaling pathways, hypothalamic-pituitary-adrenal axis, and other cellular events.40 For instance, experimental studies reveal that the antidepressant-like effect of acupuncture can be mediated by inhibition of inflammatory mediators via modulation of NF-κB in the prefrontal cortex and hippocampus.41 The present study has several advantages to be addressed as follows.
First, irrespective of previously published relevant systematic reviews and meta-analysis in the acupuncture field, the vast majority of them only focused on insomnia regardless of their psychiatric disorders42,43 or only primary insomnia.44 In addition, previous systematic reviews and meta-analyses45,46 only concentrated on the efficacy of acupuncture on depression regardless of its common comorbidity such as insomnia. Given that depression and insomnia are bidirectionally associated in patients,4 depression-related insomnia is a common medical condition that is difficult to treat. To the best of our knowledge, only one previous study10 assessed the evidence regarding the therapeutic effect of acupuncture for depression-related insomnia, but this systematic review and meta-analysis only included RCTs published before 2016. As warranted by new RCTs in recent years, previous evidence gained from this study calls for an urgent update. Moreover, although more and more RCTs20–24 have emerged in this field, results between different studies are sometimes conflicting, thereby resulting a lack of definitive conclusions about the efficacy and safety of acupuncture for depression-related insomnia. In such a scenario, we conduct this protocol for a systematic review and meta-analysis to systematically synthesize the evidence regarding the efficacy and safety of acupuncture for depression-related insomnia. To a certain degree, our study will contribute to evidence-based treatment decisions and help fulfill the current evidence gap in the management of this challenging disease.
Second, this protocol of a systematic review and meta-analysis is rigorously designed following the PRISMA-P recommendations.26 For example, our study will conduct a comprehensive search to identify eligible trials, which covers a total of 9 representative English and Chinese databases. The quality of evidence will be appraised using the GRADE approach recommended by the Cochrane Collaboration. When available, subgroup analysis, sensitivity analyses, and publication bias will also be conducted.
Third, Cochrane guidelines strongly recommend authors publish corresponding protocols before the accomplishment of a systematic review and meta-analysis.37 Additionally, we have registered this protocol in the online platform authoritative registry platform PROSPERO to avoid performance bias in the future. These measures will significantly contribute to the transparency of the subsequent systematic review process, thereby promoting the quality and validity of the complete systematic review and meta-analysis in the future. Similar studies have been published in the acupuncture field47,48 and other research fields,49,50 so we think this is a favorable approach to follow.
Nevertheless, our study has some limitations to be addressed. First, the majority of the included RCTs are likely to be conducted in China. It is regarded that publication bias is notable for acupuncture-related trials conducted in China, where the proportion of RCTs with positive conclusions conducted in China is much higher than those conducted in Western countries.51 Thus, publication bias will probably appear in our subsequent systematic review and meta-analysis, which will potentially weaken the validity of future findings. Second, the publication language for literature is limited to English and Chinese in our study, and only nine representative English and Chinese databases will be retrieved for potentially eligible trials, the possibility of literature omissions cannot be totally eliminated.
Conclusions
This protocol outlines the planned scope and methods for an upcoming systematic review meta-analysis, which aims to critically assess the evidence regarding the efficacy and safety of acupuncture for depression-related insomnia. Findings are expected to provide the evidence base for clinicians, healthcare managers, and policymakers, and guide new studies to fulfill the current evidence gap.
Ethical Statement
Given that a systematic review and meta-analysis will not involve private information of individuals, ethical approval is not required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was supported by the 2021 Special Project for Modernization of Chinese Medicine in Zhejiang Province (NO.2021ZX010) and Zhejiang Provincial Famous Traditional Chinese Medicine Experts Inheritance Studio Construction Project (grant no.GZS2021027).
Disclosure
The authors declare that they have no competing interests.
References
1. Armitage R. Sleep and circadian rhythms in mood disorders. Acta Psychiatr Scand Suppl. 2007;115(433):104–115. doi:10.1111/j.1600-0447.2007.00968.x
2. Ohayon MM, Roth T. Place of chronic insomnia in the course of depressive and anxiety disorders. J Psychiatr Res. 2003;37(1):9–15. doi:10.1016/S0022-3956(02)00052-3
3. Winokur A, Gary KA, Rodner S, Rae-Red C, Fernando AT, Szuba MP. Depression, sleep physiology, and antidepressant drugs. Depress Anxiety. 2001;14(1):19–28. doi:10.1002/da.1043
4. Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23(4):2324–2332. doi:10.1111/jcmm.14170
5. Mccall WV, Blocker JN, D’Agostino R, Kimball J, Rosenquist PB. Treatment of insomnia in depressed insomniacs: effects on health-related quality of life, objective and self-reported sleep, and depression. J Clin Sleep Med. 2010;6(4):322–329. doi:10.5664/jcsm.27872
6. Kim H, Moritz S, Botzenhardt J, et al. Changes in cortisol secretion during antidepressive treatment and cognitive improvement in patients with major depression: a longitudinal study. Psychoneuroendocrinology. 2012;37(5):685–692. doi:10.1016/j.psyneuen.2011.08.012
7. Carney CE, Edinger JD, Kuchibhatla M, et al. Cognitive behavioral insomnia therapy for those with insomnia and depression: a randomized controlled clinical trial. Sleep. 2017;40(4):zsx019. doi:10.1093/sleep/zsx019
8. Asarnow LD, Manber R. Cognitive behavioral therapy for insomnia in depression. Sleep Med Clin. 2019;14(2):177–184. doi:10.1016/j.jsmc.2019.01.009
9. Gebara MA, Siripong N, DiNapoli EA, et al. Effect of insomnia treatments on depression: a systematic review and meta-analysis. Depress Anxiety. 2018;35(8):717–731. doi:10.1002/da.22776
10. Dong B, Chen Z, Yin X, et al. The efficacy of acupuncture for treating depression-related insomnia compared with a control group: a systematic review and meta-analysis. Biomed Res Int. 2017;2017:9614810. doi:10.1155/2017/9614810
11. Chung KH, Li CY, Kuo SY, Sithole T, Liu WW, Chung MH. Risk of psychiatric disorders in patients with chronic insomnia and sedative-hypnotic prescription: a nationwide population-based follow-up study. J Clin Sleep Med. 2015;11(5):543–551. doi:10.5664/jcsm.4700
12. Wilson K, Mottram P. A comparison of side effects of selective serotonin reuptake inhibitors and tricyclic antidepressants in older depressed patients: a meta-analysis. Int J Geriatr Psychiatry. 2004;19(8):754–762. doi:10.1002/gps.1156
13. Santos Moraes WA, Burke PR, Coutinho PL, et al. Sedative antidepressants and insomnia. Braz J Psychiatry. 2011;33(1):91–95. doi:10.1590/S1516-44462011000100017
14. Li CT, Bai YM, Lee YC, et al. High dosage of hypnotics predicts subsequent sleep-related breathing disorders and is associated with worse outcomes for depression. Sleep. 2014;37(4):803–809. doi:10.5665/sleep.3594
15. Lovato N, Lack L, Wright H, Kennaway DJ. Evaluation of a brief treatment program of cognitive behavior therapy for insomnia in older adults. Sleep. 2014;37(1):117–126. doi:10.5665/sleep.3320
16. Ng JY, Parakh ND. A systematic review and quality assessment of complementary and alternative medicine recommendations in insomnia clinical practice guidelines. BMC Complement Med Ther. 2021;21(1):54. doi:10.1186/s12906-021-03223-3
17. Lan Y, Wu X, Tan HJ, et al. Auricular acupuncture with seed or pellet attachments for primary insomnia: a systematic review and meta-analysis. BMC Complement Altern Med. 2015;15:103. doi:10.1186/s12906-015-0606-7
18. Cai HQ, Su SY, Zhang X, Dai Q, Huang M, Lin A. Effect of auricular acupuncture on reduction of sertraline hydrochloride in patients with depression: a randomized controlled trial. Chin Acupunct Moxibustion. 2021;41(9):1005–1009. doi:10.13703/j.0255-2930.20200721-k0002
19. Yin X, Dong B, Liang T, et al. Efficacy and safety of electroacupuncture on treating depression-related insomnia: a study protocol for a multicentre randomised controlled trial. BMJ Open. 2019;9(4):e021484. doi:10.1136/bmjopen-2018-021484
20. Yin X, Li W, Wu H, et al. Efficacy of electroacupuncture on treating depression-related insomnia: a randomized controlled trial. Nat Sci Sleep. 2020;12:497–508. doi:10.2147/NSS.S253320
21. Luo W, Zhang Q, Lai X. Observation on the efficacy of relieving gloomy and regulating mind acupuncture on comorbid depression and insomnia. Chin Acupunct Moxibustion. 2010;30(11):899–903.
22. Tang XQ, Xia H, Wu Y. Clinical study of acupuncture combined with paroxetine hydrochloride in the treatment of comorbid mild to moderate depression and insomnia. Tradit Chin Med. 2021;53(16):139–142.
23. Chung KF, Yeung WF, Yu YM, et al. Acupuncture for residual insomnia associated with major depressive disorder: a placebo- and sham-controlled, subject- and assessor-blind, randomized trial. J Clin Psychiatry. 2015;76(6):e752–e760. doi:10.4088/JCP.14m09124
24. Yeung WF, Chung KF, Tso KC, Zhang SP, Zhang ZJ, Ho LM. Electroacupuncture for residual insomnia associated with major depressive disorder: a randomized controlled trial. Sleep. 2011;34(6):807–815. doi:10.5665/SLEEP.1056
25. Yin X, Xu J, Dong B, et al. Efficacy and safety of electroacupuncture on treating depression related sleep disorders: study protocol of a randomized controlled trial. Evid-Based Complementary Altern Med. 2016;2016:1069597. doi:10.1155/2016/1069597
26. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi:10.1186/2046-4053-4-1
27. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV).
28. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
29. American Association of Sleep Medicine. ICSD-3 (International Classification of Sleep ICSD-3 Disorders). Dartmouth, Illinois: American Association of Sleep Medicine; 2014.
30. Chinese Psychiatric Society. The Chinese Classification of Mental Disorders (CCMD-3).
31. World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders. Diagnostic Criteria for Research. Geneva, Switzerland: World Health Organization; 1993.
32. Edinger JD, Arnedt JT, Bertisch SM, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2021;17(2):255–262. doi:10.5664/jcsm.8986
33. Riemann D, Baglioni C, Bassetti C, Bjorvatn B. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26(6):675–700. doi:10.1111/jsr.12594
34. Davidson JR. Major depressive disorder treatment guidelines in America and Europe. J Clin Psychiatry. 2010;71(Suppl E1):e04. doi:10.4088/JCP.9058se1c.04gry
35. Banno M, Harada Y, Taniguchi M, et al. Exercise can improve sleep quality: a systematic review and meta-analysis. Peer J. 2018;6:e5172. doi:10.7717/peerj.5172
36. Lee CJ, Iyer G, Liu Y, et al. The effect of vitamin D supplementation on glucose metabolism in type 2 diabetes mellitus: a systematic review and meta-analysis of intervention studies. J Diabetes Complications. 2017;31(7):1115–1126. doi:10.1016/j.jdiacomp.2017.04.019
37. Higgins J, Green SR; Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions. Chichester, England; 2011.
38. Flemyng E, Dwan K, Moore TH, Page MJ, Higgins JP. Risk of bias 2 in Cochrane reviews: a phased approach for the introduction of new methodology. Cochrane Database Syst Rev. 2020;10:Ed000148. doi:10.1002/14651858.ED000148
39. Brozek JL, Akl EA, Alonso-Coello P, et al. EGrading quality of evidence and strength of recommendations in clinical practice guidelines. Part 1 of 3. An overview of the GRADE approach and grading quality of evidence about interventions. Allergy. 2009;64(5):669–677. doi:10.1111/j.1398-9995.2009.01973.x
40. Zhao FY, Fu QQ. Acupuncture: a promising approach for comorbid depression and insomnia in perimenopause. Nat Sci Sleep. 2021;13:1823–1863. doi:10.2147/NSS.S332474
41. Lu J, Shao RH, Jin SY, Hu L, Tu Y, Guo JY. Acupuncture ameliorates inflammatory response in a chronic unpredictable stress rat model of depression. Brain Res Bull. 2017;128:106–112. doi:10.1016/j.brainresbull.2016.11.010
42. Cheuk DK, Yeung WF, Chung KF, Wong V. Acupuncture for insomnia. Cochrane Database Syst Rev. 2007;3:Cd005472. doi:10.1002/14651858.CD005472.pub2
43. Kim SA, Lee SH, Kim JH, et al. Efficacy of acupuncture for insomnia: a systematic review and meta-analysis. Am J Chin Med. 2021;49(5):1135–1150. doi:10.1142/S0192415X21500543
44. Zhao FY, Fu QQ, Kennedy GA, et al. Can acupuncture improve objective sleep indices in patients with primary insomnia? A systematic review and meta-analysis. Sleep Med. 2021;80:244–259. doi:10.1016/j.sleep.2021.01.053
45. Armour M, Smith CA, Wang LQ, et al. Acupuncture for depression: a systematic review and meta-analysis. J Clin Med. 2019;8(8):1140. doi:10.3390/jcm8081140
46. Smith CA, Armour M, Lee MS, Wang LQ, Hay PJ. Acupuncture for depression. Cochrane Database Syst Rev. 2018;3(3):Cd004046. doi:10.1002/14651858.CD004046.pub4
47. Li Y, Liu Y. Acupuncture for pain and function in patients with nonspecific low back pain: study protocol for an up-to-date systematic review and meta-analysis. J Pain Res. 2022;15:1379–1387. doi:10.2147/JPR.S362980
48. Kim JY, Seo BK. Thread embedded acupuncture for non-specific posterior neck pain: a PRISMA-compliant protocol for systematic review and meta-analysis. J Pain Res. 2021;14:2327–2334. doi:10.2147/JPR.S310846
49. McCutcheon R, Pillinger T, Welby G, et al. Magnitude and variability of structural brain abnormalities in neuropsychiatric disease: protocol for a network meta-analysis of MRI studies. Evid Based Ment Health. 2021;24(3):111–114. doi:10.1136/ebmental-2020-300229
50. Aceituno D, Pennington M, Iruretagoyena B, Prina MA, McCrone P. Health state utility values in schizophrenia: protocol for a systematic review and meta-analysis. Evid Based Ment Health. 2019;22(4):142–144. doi:10.1136/ebmental-2019-300089
51. Gang WJ, Gong CZ, Jing XH. Acupuncture randomized controlled trials: comparing China-based vs Western-based studies. Chin Acupunct Moxibustion. 2022;42(1):3–7. doi:10.13703/j.0255-2930.20201224-k0001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.