")
Back to Journals » Patient Preference and Adherence » Volume 11
The effects of patient and physician characteristics on early outpatient satisfaction with substance dependence care: results of the SUBUSQOL study
Authors Bourion-Bédès S , Schwan R, Di Patrizio P, Vlamynck G, Viennet S, Schvartz M, Gaunard A, Bédès A, Clerc-Urmès I, Baumann C
Received 10 February 2017
Accepted for publication 11 April 2017
Published 8 May 2017 Volume 2017:11 Pages 887—896
DOI https://doi.org/10.2147/PPA.S134242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Stéphanie Bourion-Bédès,1–3 Raymund Schwan,2 Paolo Di Patrizio,2 Guillaume Vlamynck,2 Sarah Viennet,2 Maxime Schvartz,2 Anne Gaunard,2 Alex Bédès,4 Isabelle Clerc-Urmès,5 Cédric Baumann3,5
1Regional Medical and Psychological Service (SMPR), 2CSAPA (Healthcare Center of Accompaniment and Prevention in Addictology), University Hospital of Nancy, 3EA4360 APEMAC, University of Lorraine, Nancy, 4ANPAA 15-CSAPA (Healthcare Center of Accompaniment and Prevention in Addictology), Saint-Flour, Cantal, 5Platform of Clinical Research Facility PARC, Unit MDS, University Hospital of Nancy, Nancy, France
Background: Although patient perceptions of health care have increasingly been explored in the literature, little is known about care satisfaction among individuals with substance dependence. This exploratory study assessed the relationships between patient and physician characteristics and early outpatient satisfaction with care for alcohol and opioid dependence.
Methods: Satisfaction was assessed using a multidimensional, self-administered and validated questionnaire during the early care process among a prospective outpatient cohort. In addition to measuring satisfaction and obtaining sociodemographic and clinical data, this study collected data on the self-reported health status and physician characteristics at inclusion. Cross-sectional analysis with multiple linear regression was performed to identify the variables associated with satisfaction level.
Results: A total of 249 outpatients were included, and 63.8% completed the satisfaction questionnaire. Patients without a history of previous care for substance dependence were more satisfied with the appointment-making process (β=7.2; P=0.029) and with the doctor consultation (β=10.3; P=0.003) than those who had received care previously. Neither sociodemographic characteristics nor self-reported health status was associated with outpatient satisfaction.
Conclusion: The factors that affect patients’ ratings of early satisfaction with the care that they receive should be studied further because increased understanding of the factors that negatively affect these ratings might enable caregivers and outpatient management facilities to improve the patient experience during the early stages of care, which might in turn improve treatment adherence, continuity of care, and other health-related outcomes.
Keywords: satisfaction, determinants, outpatient, substance dependence
Introduction
Improving quality of care is a priority and a persistent challenge for health care departments from the perspectives of both clinicians and health care managers.1 Patient satisfaction with health care is a current and important indicator of health care quality that gives the patient a central role in this measurement.2,3 In both mental health and addiction populations, studies have recognized patient satisfaction as a key target.4 Researchers have conducted numerous studies of patient satisfaction to assess a broad range of service factors, ranging from the availability of medical visits, social workers and therapy to professional behavior and trust in physicians, the information that they provide, and other aspects of the patient–physician relationship. Studies have also demonstrated that satisfied patients are more likely to cooperate with treatment and maintain a continuing relationship with a practitioner; such patients enjoy better medical prognoses.5,6 The general use of validated satisfaction questionnaires in surgical or medical care, such as care provided for diabetes, arthritis, or cancer,7–9 has enabled the identification of determinants of satisfaction. The primary factors that influence satisfaction are the type of health care setting and caregiver characteristics, such as their experience, age, and gender.2,10 Certain patient characteristics also influence satisfaction with care: better self-reported health status, older age, less education, and good health have commonly been reported as traits associated with greater satisfaction.2,11,12
Prior to the 1990s, limited attention had been devoted to satisfaction in research on substance use disorders; since then, however, the field has grown due to the chronic, relapsing nature of substance use and the negative consequences for the various life domains affected by substance use.13,14 In addition to hospitalization, ambulatory care was increasingly a focus by researchers aiming to explore satisfaction for patients with substance use disorders. However, follow-up studies have been limited by patient attrition.15,16 Within substance use disorders research, it is important to improve patient satisfaction by enhancing the understanding regarding patient satisfaction and its determinants because this understanding might improve treatment adherence, continuity of care, follow-up results, and other health-related outcomes as known in the case of ambulatory care.3 Although assessments of patient satisfaction have increased in the psychiatric care literature, the timing of when satisfaction with care assessments are administered varies across studies for both in inpatient care and in outpatient care.17,18 Because dissatisfaction during the early care process can lead patients to stop treatment or consult elsewhere,19 understanding patient satisfaction early in the care process is a topic of interest. No previously published study has focused on early satisfaction in addiction care. Following prior works in general health care,2 we hypothesize that patient sociodemographic data and health status and physician characteristics are associated with early satisfaction in addiction care.
Thus, this exploratory study sought to determine whether and to what extent patient health status and other patient and physician characteristics are associated with early satisfaction among outpatients who are starting care for alcohol or opioid dependence.
Methods
Participants and design
This study is a cross-sectional analysis from the SUBstance Users Satisfaction and Quality Of Life (SUBUSQOL) study, a prospective cohort study of outpatients who met the Diagnostic and Statistical Manual, fourth edition (DSM-IV) criteria for alcohol dependence, opioid dependence, or both (ClinicalTrials.gov ID: NCT02894476).
Patients were recruited from the French specialized addiction treatment centers where they began care. Treatment combined individual therapy with individual sessions focused on listening and support, which aimed to investigate interpersonal difficulties and patients’ social environment and to change these addictive behaviors. In addition to individual therapy, patients might benefit from medication. The clinician assigned the patients who sought care to either alcoholic or opioid groups based on their main type of dependence using axis I of the DSM-IV. Clinicians certified in addiction pathologies who were trained on use of the DSM-IV20 made the diagnoses.
Data collection
The sociodemographic data and clinical characteristics were collected through medical interview and clinical testing. Satisfaction and health status measures were assessed with the French versions of the self-administered questionnaires during the early care process.
Outpatient satisfaction
Satisfaction was measured using the quality of care satisfaction questionnaire in outpatient consultation (Quality of Care Scale in outpatient consultation [EQS-C]) to assess early outpatient satisfaction 15 days after study inclusion (ie, their first consultation in the department). The EQS-C is a 27-item self-report instrument that is composed of four dimensions that explore the technical and interpersonal aspects of care and satisfaction with staff and treatment. These dimensions are contact/appointments (6 items), reception facilities (5 items), waiting time (3 items), and consultation with the doctor (13 items). The last dimension is related to the medical intervention that explores the warmth of the doctor, whether the doctor explained his or her decisions, whether the doctor took the patient’s opinion into account, whether the patient received the information that he or she wanted, and whether the doctor warned the patient about possible side effects of treatment. The other three dimensions are related to organizational/nonmedical aspects of care. Each item was scored from 0 to 4, where 4 indicated the greatest level of satisfaction. A “does not apply” category was provided for 13 items related to situations that are not universally relevant. The nonresponse and “does not apply” categories were considered as missing data. Scores were computed when at least half of the items in a dimension were completed. The scores for each dimension were based on the sum of the items and were standardized to range from 0 (low satisfaction) to 100 (high satisfaction). The instrument also included one additional item pertaining to behavioral intent (“I think I will continue attending this department”) that was not included in the scoring, as well as sociodemographic data, overall life satisfaction, and an open-ended comment field at the end of the questionnaire. Responses to the open-ended question (“What part of our service do you think could be improved?”) were classified as negative comments, positive comments, mixed comments, or no comments.
The validity and reliability of the questionnaire have been previously established.3 Because completing the questionnaire at home was preferable to completing it immediately after consultation, participants returned their data via the mail.3 The questionnaire was mailed 10 days after the first visit (to be received for an early measure at 15 days) to be completed at home. Participants were asked to complete and return the questionnaire by mail in a prepaid envelope.
Self-perceived quality of life
Self-perceived quality of life was assessed using the Short-Form 12 questionnaire (SF-12) and the Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form (Q-LES-Q-SF). These questionnaires were completed as part of the routine care received at the time of study inclusion. The SF-12 is a well-known generic instrument that measures self-reported health status and includes a subset of 12 items from the SF-36.21 Information from all 12 items is used to calculate the physical component summary (PCS) and the mental health component summary (MCS). All scores are transformed into a standardized score ranging from 0 to 100. Higher scores indicate better self-reported health status. The Q-LES-Q-SF is a self-report instrument composed of 16 items derived from the general activities scale of the original 93-item form.22 The French version of the Q-LES-Q-SF yields valid and reliable clinical assessment of self-reported health status.23,24 This version consists of 14 items assessing patient satisfaction with his or her physical health, social relationships, ability to function in daily life, physical mobility, mood, family relationships, sexual drive and interest, ability to engage in work, leisure activities, economic status, household activities, living/housing situation, vision, and overall sense of well-being. Each of the 14 items is rated on a 5-point scale that indicates the degree of enjoyment or satisfaction experienced over the past week. The total score for items 1 to 14 is computed (ranging from 14 to 70) and expressed as a percentage (1–100) of the maximum total score. Higher scores on the Q-LES-Q-SF indicate greater contentment or satisfaction. The instrument also includes two additional items measuring satisfaction with medication and overall life satisfaction; these items were not included in the scoring.
Anxiety and depression
The Hospital Anxiety and Depression Scale (HADS), a 14-item self-report questionnaire, was used to assess the levels of depression (7 items) and anxiety (7 items).25 Each of the 14 items is rated on a 4-point Likert scale. Consistent with previous research, a cutoff of 8 was used for each HADS subscale to differentiate normal distress from mild and severe distress.26 The French version of the HADS was used in this study because it has yielded valid and reliable clinical assessments of depression and anxiety in previous research.27
Patient sociodemographic and clinical data and physician characteristics
The collected data included factors that had been previously identified as associated with satisfaction. At the time of inclusion, data on participants’ age, gender, educational level, marital status, occupational status, type of substance dependence, duration of illness, history of previous care for substance dependence, therapeutic strategy, and the presence of medical and/or psychiatric comorbidities were obtained. The origin of the care request and the care setting were also noted. Data concerning the physicians’ genders, academic qualifications (senior vs junior), and years of clinical practice were also collected.
Statistical analyses
Descriptive and comparative analyses
The mean (±standard deviation) or median, as appropriate, was used for the continuous variables, whereas the number or percentage was used for the categorical variables. The qualitative data were compared using Pearson’s chi-square test or Fisher’s exact test, whereas the quantitative variables were compared using Student’s t-test.
Bivariate and multivariate analyses
Each dimension of the EQS-C (contact/appointments, reception facilities, waiting time, and consultation with the doctor) was considered as a separate dependent variable. A preliminary analysis consisted of calculating Cronbach’s alpha for each dimension of EQS-C and the global score to verify the internal consistency in the current sample.
Linear regression models were used to determine which variables were associated with satisfaction scores among the outpatient substance users starting care. The influence of physician characteristics on both the “waiting time” and “consultation with the doctor” dimensions was investigated. Variables were identified as relevant if they were significant in bivariate analyses at the 20% threshold; however, age, gender, and type of dependence remained in each of the models for adjustment. A multivariate linear regression was used to retain significant factors at the 5% threshold. The correlations between the variables retained in the models were also tested. Positive and significant β coefficients reflected positive effects on the satisfaction scores. SAS 9.4 (SAS Inst., Cary, NC, USA) was used for the data analyses.
Ethics approval and consent to participate
Ethical approval for the data collection was granted by the Institutional Review Board (Comité National Informatique et Liberté DR-2013-156) and ensured the confidentiality of the information collected. Potential participants were informed of the research’s purpose and aims. They received guidance about how they could withdraw consent at any point. All participants had the capacity to consent and gave informed consent for participation in the research and for their data to be used. Consent forms were signed in the presence of a researcher and kept in the main study site file.
Results
Patient and physician characteristics
Of the 249 patients included in the SUBUSQOL cohort, 159 answered the EQS-C, which was sent 11.5 days (SD =3.6 days) after study inclusion on average. Nine questionnaires were returned because of incorrect addresses, and the 159 EQS-C forms were returned in a mean time of 17.1 days (13.7 days). The sociodemographic and clinical characteristics of the patients are presented in Table 1 for the entire sample and separately based on whether the EQS-C was answered. Most patients were male (76.1%) with a mean age of 39.5 years old (SD =11.1). More than one-third of these patients were married (37%), and a minority reported a high-school or university-level education (17.7%). Of the 159 respondents, 71 (44.7%) sought care for alcohol dependence and 88 (55.3%) for opioid dependence according to the DSM-IV criteria. The mean duration of substance dependence was 14.6 (SD =11.1) years. Nineteen patients required care while undergoing a legally mandated addiction treatment. Patients who responded to the satisfaction questionnaire were older than those who did not respond (P=0.03); otherwise, the EQS-C nonresponders did not differ from the EQS-C responders in terms of their sociodemographic or clinical characteristics.
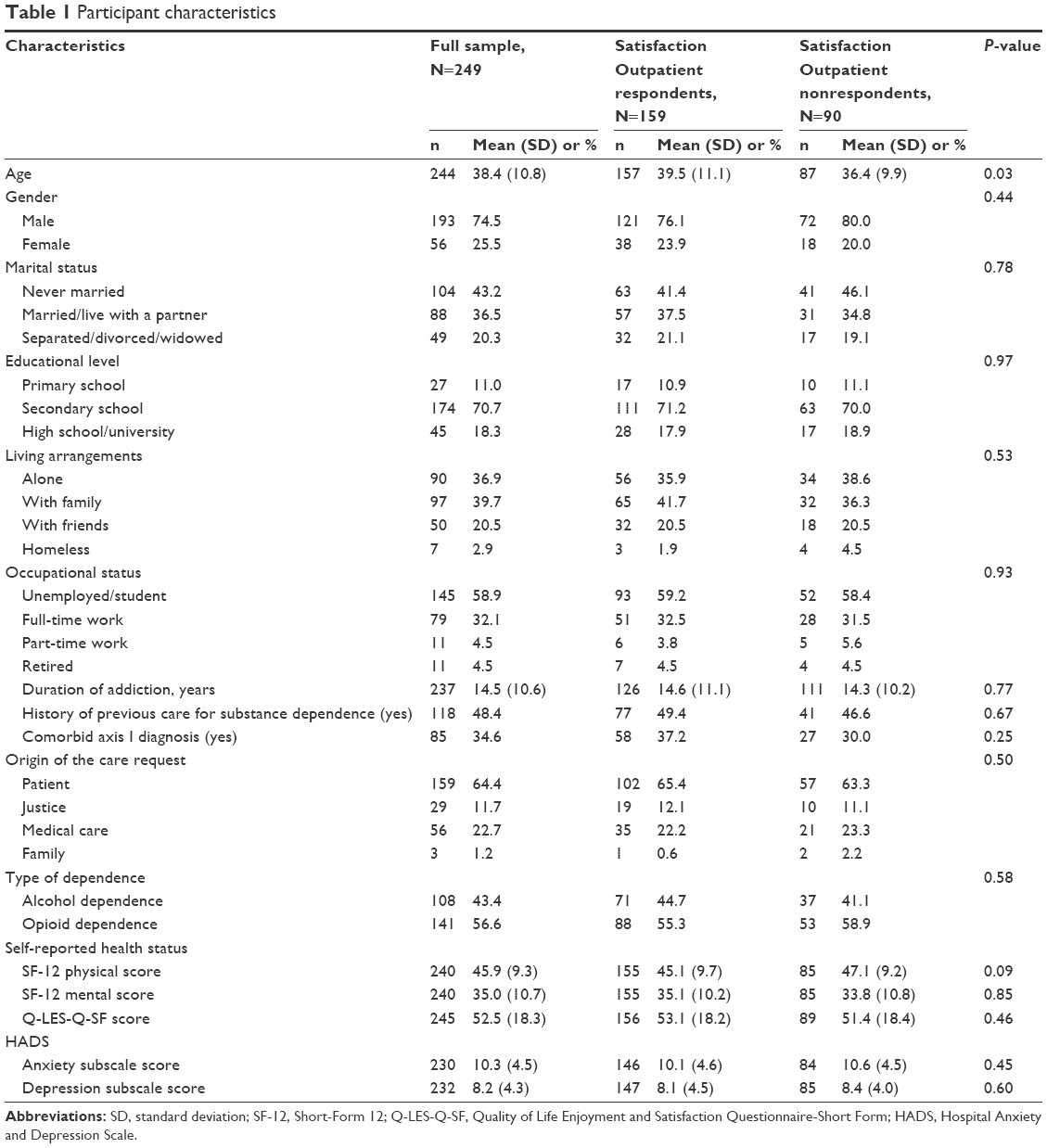 | Table 1 Participant characteristics |
All of the physicians were currently working with patients with substance dependence. Slightly fewer than half of the physicians (46.7%) were men, and both senior and junior physicians were represented. Of the 159 respondents, 54 were screened by a senior physician (34.4%), whereas 103 were evaluated by a junior physician (65.5%). In 49.1% of all cases, the patient and physician were of the same gender. Responders and nonresponders did not differ in terms of their physicians’ genders, academic qualifications, or experience.
SF-12, Q-LES-Q-SF, and HADS scores
The results of SF-12, Q-LES-Q-SF, and HADS are presented in Table 1. The mean SF-12 scores were 45.1 (SD =9.7) and 35.1 (SD =10.2) for the PCS and MCS domains, respectively. The mean Q-LES-Q-SF score was 53.1 (SD =18.2). The mean and median HADS scores for the depression subscale were 8.1 (SD =4.5) and 8, respectively, and the mean and median HADS scores for the anxiety subscales were 10.1 (SD =4.6) and 10, respectively. The results did not reveal a significant difference between EQS-C respondents and nonrespondents.
Satisfaction scores
Cronbach’s alpha of the EQS-C dimensions varied from 0.80 to 0.93 and 0.95 for the global score in the current sample. The overall satisfaction results with regard to each dimension are presented in Table 2. The mean satisfaction scores were 80 (SD =18.3) for “consultation with the doctor”, 71.7 (SD =26) for “waiting time”, 79 (18.9) for “contact/appointments”, and 77.5 (SD =16.8) for “reception facilities”. A total of 64 patients (40.2%) made several comments in the open-ended comment field of the EQS-C; in particular, these comments were often negative and pertained to waiting and reception. Of the 159 patients, 111 (69.7%) intended to consult with their doctor again after the initial consultation.
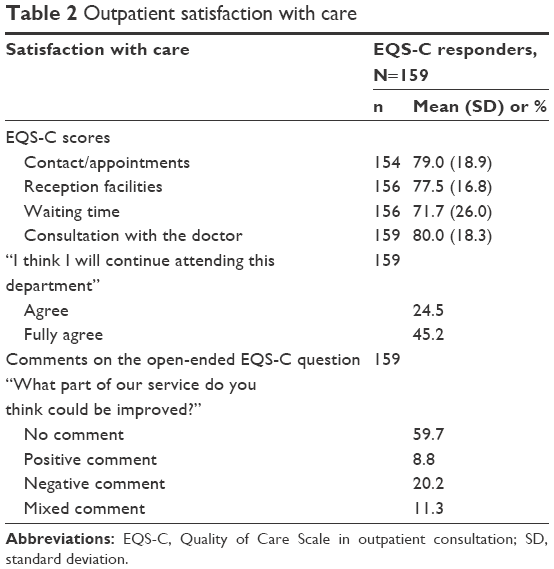 | Table 2 Outpatient satisfaction with care |
Factors associated with early outpatient satisfaction with care
The results of bivariate and multivariate analyses are reported in Tables 3 and 4. The multivariate analysis included the significant variables from the bivariate analyses with a bivariate P-value <0.2 and adjusted for age, gender, and type of dependence. One variable was associated with the level of patient satisfaction. Patients with no history of previous care for substance dependence were more satisfied with the appointment-making process (β=7.2; P=0.029) and with the doctor consultation (β=10.3; P=0.003) than those who received care previously. The proportion of variance explained (ie, R2) ranged from 0.06 (reception dimension) to 0.20 (consultation with the doctor dimension).
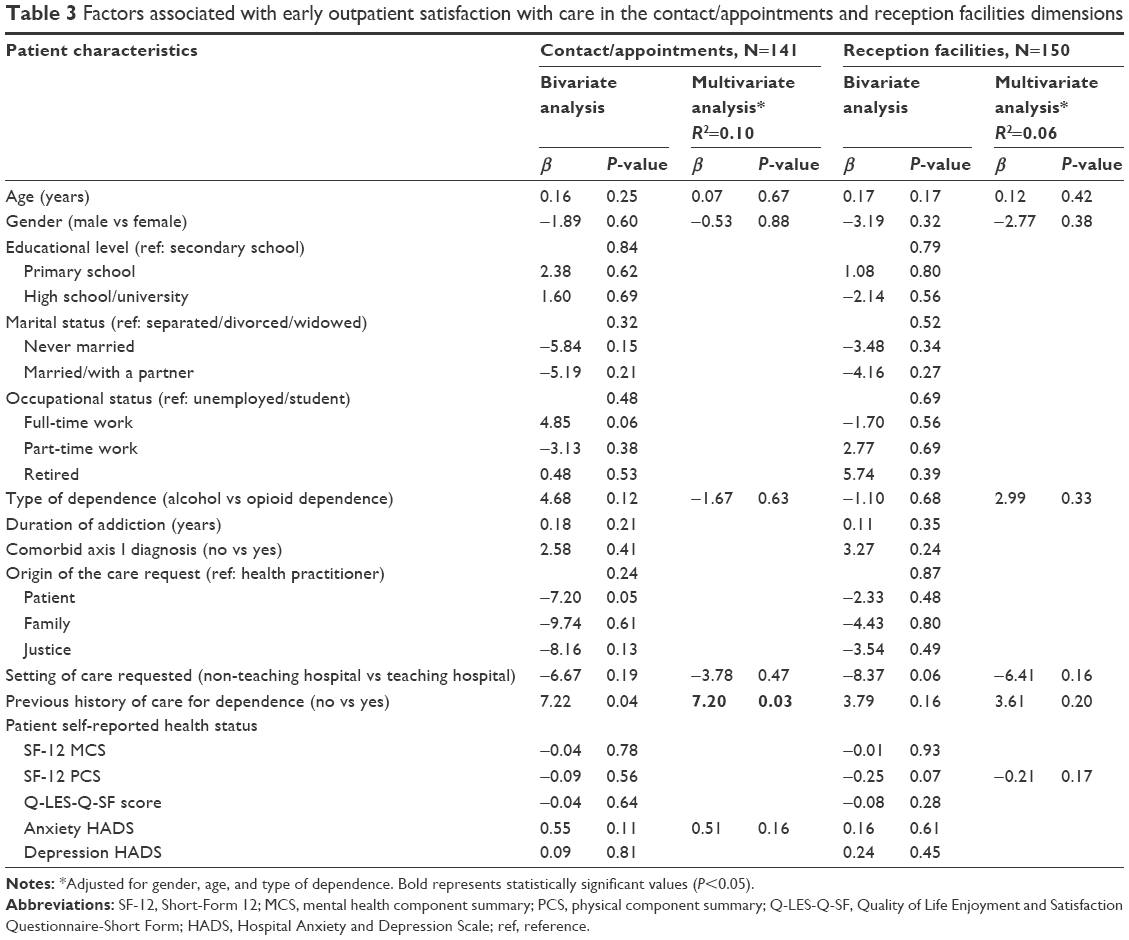 | Table 3 Factors associated with early outpatient satisfaction with care in the contact/appointments and reception facilities dimensions |
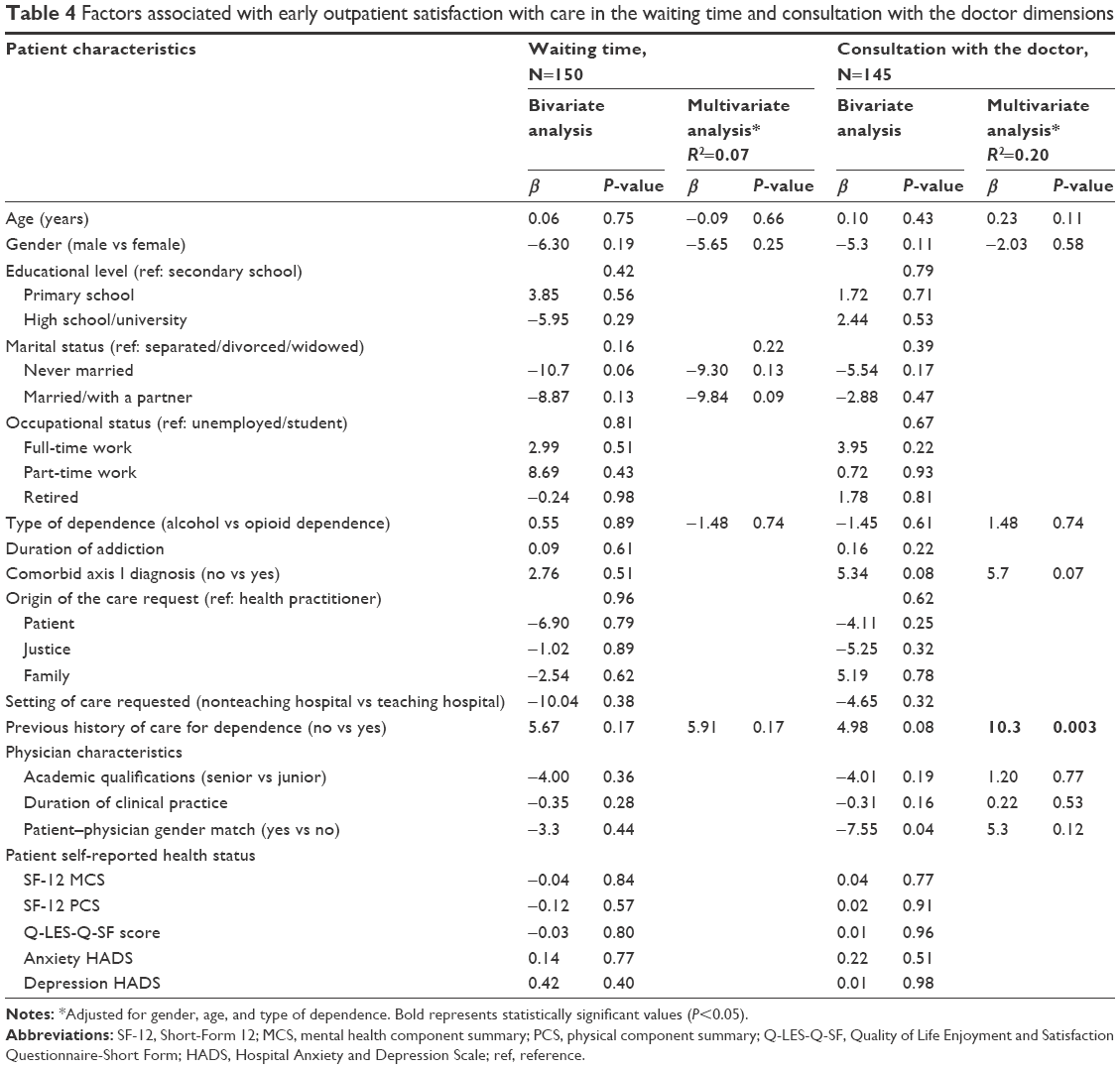 | Table 4 Factors associated with early outpatient satisfaction with care in the waiting time and consultation with the doctor dimensions |
Discussion
In our study, one characteristic was associated with early outpatient satisfaction with care among patients with alcohol or opioid dependence. Among the sociodemographic, clinical, and self-reported health status characteristics selected, patients with no previous history of care for substance dependence tended to be more satisfied with appointment making and consultation with the doctor than were those who had received care previously. These results might be useful for interventions among clinicians to make them more aware of patients with a history of previous care who are at risk of having less satisfactory experiences. Moreover, if other studies confirm our results, then measures targeted at clinicians might be created to improve satisfaction and reduce the risk of withdrawal from care. None of the sociodemographic, clinical, or self-reported health status factors were significantly associated with the other two domains of satisfaction. Although previous works investigating the satisfaction of care provided to patients with substance use disorders have shown that participants with higher psychosocial functioning and better health were more satisfied with treatment,28,29 our results showed that neither self-reported health status nor physician characteristics were associated with early ratings of satisfaction with care. If our results were not aligned with the previously described positive correlation between satisfaction with care and health-related quality of life among patients living with chronic conditions,30 certain hypotheses should be mentioned. First, the findings suggest that these two concepts represent different aspects of patients’ experiences. Alternatively, the fact that no health status aspects predicted satisfaction does not prove that health status and satisfaction with care are unrelated. The small number of patients included reduced the power; therefore, true relationships between health status and early satisfaction with care might not have been detected.
Compared with studies reporting the satisfaction scores associated with French outpatient medical and surgical departments at public teaching hospitals in Paris, the current study included a homogeneous population of outpatients with substance dependence. The results showed that the mean satisfaction scores in domains “consultation with the doctor”, “appointment making” and “reception” were well below 80, whereas the mean score for the “waiting time” dimension was more aligned with the previous results.3 Long waiting time has been identified in psychiatric outpatient settings as a primary cause of low patient satisfaction ratings, and previous studies have reported that patients who had waited for a long time were more dissatisfied with staff, with their prospects of influencing their care, and with the care that they received.31,32 In light of these findings, the results of this study indicated that practitioners working in outpatient settings must continually improve the technical and interpersonal aspects of the care that they provide because dissatisfaction with initial contact might lead patients to cease care or consult elsewhere.19
Several methodological limitations should be discussed. First, a small number of patients were included in this study, which probably limits the statistical power. Second, our findings might not be generalizable to other groups of patients with substance dependence, nor might the sample be fully representative of patients who begin treatment for substance dependence. Third, a single measure was used to assess satisfaction with care. The results might vary with the choice of another satisfaction measurement or instrument, and this possibility cannot be explored within the current dataset. Fourth, despite the large number of determinants included in the analyses, the multivariate models explained between 6% and 20% of the explained variance; thus, other factors not accounted for by our study should be included in future research. Previous studies in psychiatric research suggested that generic instruments might not be relevant to psychiatric assessments of inpatient satisfaction, as patients with psychiatric disorders have specific and varying expectations regarding inpatient care.33,34 These observations led researchers to develop a specific self-administered and multidimensional questionnaire to assess inpatient satisfaction. The results of this study might support the development of a specific early satisfaction questionnaire for outpatients undergoing care for substance dependence, as they might have specific expectations regarding satisfaction that are not adequately captured by generic instruments. Nevertheless, despite the use of a specific questionnaire for psychiatric inpatient care, the proportion of variance explained was not higher than those estimated in our models.35
To the best of our knowledge, this study is the first to assess the effect of various demographic, psychosocial, and health-related determinants on satisfaction among individuals who are alcohol or opioid dependent and beginning outpatient care. The present study has several strong methodological merits, such as the use of a multidimensional validated outpatient satisfaction questionnaire and a study design requiring completion of the satisfaction questionnaire at home, restraining a variant of the Hawthorne effect.3,36 The 63.8% response rate for the outpatient satisfaction questionnaire in our sample should be emphasized because it is consistent with the 65% response rate obtained using the same satisfaction questionnaire applied in French medical and surgical departments and similar to the results of the studies using other instruments in outpatient psychiatric care centers.3,31,37 This response rate emphasizes the importance that patients with substance dependence attribute to evaluating their own care, and it is a positive indicator of patients’ future willingness to measure their satisfaction in substance-dependence care settings. Moreover, the demographics of our patient sample were consistent with those in the literature. One-quarter of the patients in this study were women, which is consistent with the proportion of female patients in addiction research. Moreover, the mean duration of substance dependence was consistent with the time taken to establish substance dependence.38,39 Compared with the 9% of people who were unemployed and the 30% of people living alone among the French population over 18 years of age, the high proportion of patients who were living alone and unemployed (close to 60%) reflects the social and familial causes or consequences of substance dependence.40,41 No differences between the satisfaction survey respondent and nonrespondent groups were observed in the sociodemographic and clinical variables, except for age. This observation is important because it is believed that the health status or sociodemographics of nonrespondents may differ. The results concerning poor self-reported quality of life in both the mental and physical health domains were consistent with studies using the SF-12 or SF-36 questionnaires that indicated that patients with substance dependence present impaired self-reported quality of life, particularly in the mental domain.17,42,43 The results of this study did not reveal significant differences between the respondents and nonrespondents with regard to their baseline self-reported quality of life or their anxiety-depression assessments. The respondents were older than the nonrespondents, consistent with previous studies conducted in inpatient care settings showing that sociodemographic characteristics, such as age, differ between nonresponders and responders.17 We hypothesize that older participants are more concerned about evaluating their own care.
Conclusion
The results of this exploratory study have both practical and theoretical implications because they offer a starting point for measuring the early satisfaction of outpatients with substance dependence. From a practical perspective, the early satisfaction scores of patients with substance dependence should be improved, and no sociodemographic or health-related factors appear to be associated with early satisfaction with outpatient care. From a theoretical perspective, the factors that affect patients’ ratings of satisfaction with early care must be better understood because additional information regarding the factors that negatively affect such ratings might enable caregivers and outpatient management facilities to improve the patient experience early in the care process and limit the number of early drop-outs. Thus, future studies should identify the factors that influence the early satisfaction of outpatients. Future qualitative and in-depth interviews might help to provide more information regarding how individuals with substance dependence perceive satisfaction and to determine which factors affect their early satisfaction with outpatient care. Moreover, longitudinal studies might reveal additional information about patient satisfaction with substance dependence care, especially in terms of the effect of early satisfaction on health-related outcomes and how early dissatisfaction might predict the withdrawal of care among these patients.
Acknowledgments
The authors gratefully acknowledge the study team and all the care workers who provided care for these patients. We are also grateful to SETHS for supporting this work and to CIC-EC-Inserm CIC1433, particularly to Ms Pierrez’s for her assistance.
Author contributions
SB-B, RS, and CB designed the study protocol. SV, PDP, AB, MS, AG, and GV collected the data used in the current manuscript. SB-B and IC-U performed the statistical analysis. RS and CB oversaw the writing of the manuscript. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Beattie M, Lauder W, Atherton I, Murphy DJ. Instruments to measure patient experience of health care quality in hospitals: a systematic review protocol. Syst Rev. 2014;3(1):4. | ||
Fan VS, Burman M, McDonell MB, Fihn SD. Continuity of care and other determinants of patient satisfaction with primary care. J Gen Intern Med. 2005;20(3):226–233. | ||
Gasquet I, Villeminot S, Estaquio C, Durieux P, Ravaud P, Falissard B. Construction of a questionnaire measuring outpatients’ opinion of quality of hospital consultation departments. Health Qual Life Outcomes. 2004;2:43. | ||
Schulte SJ, Meier PS, Stirling J. Dual diagnosis clients’ treatment satisfaction – a systematic review. BMC Psychiatry. 2011;11(1):64. | ||
Deyo RA, Inui TS. Dropouts and broken appointments. A literature review and agenda for future research. Med Care. 1980;18(11):1146–1157. | ||
Williams B. Patient satisfaction: a valid concept? Soc Sci Med. 1994;38(4):509–516. | ||
Sampson MJ, Singh H, Dhatariya KK, Jones C, Walden E, Bradley C. Education and psychological aspects psychometric validation and use of novel diabetes in-patient treatment satisfaction questionnaire. Diabet Med. 2009;26(7):729–735. | ||
Baumann C, Rat AC, Mainard D, Cuny C, Guillemin F. Importance of patient satisfaction with care in predicting osteoarthritis-specific health-related quality of life one year after total joint arthroplasty. Qual Life Res. 2011;20(10):1581–1588. | ||
Nguyen TV, Bosset JF, Monnier A, et al. Determinants of patient satisfaction in ambulatory oncology: a cross sectional study based on the OUT-PATSAT35 questionnaire. BMC Cancer. 2011;11(1):526. | ||
Hall JA, Blanch-Hartigan D, Roter DL. Patients’ satisfaction with male versus female physicians: a meta-analysis. Med Care. 2011;49(7): 611–617. | ||
Bidaut-Russell M, Gabriel SE, Scott CG, Zinsmeister AR, Luthra HS, Yawn B. Determinants of patient satisfaction in chronic illness. Arthritis Rheum. 2002;47(5):494–500. | ||
Nguyen Thi PL, Briançon S, Empereur F, Guillemin F. Factors determining inpatient satisfaction with care. Soc Sci Med. 2002;54(4):493–504. | ||
de Maeyer J, Vanderplasschen W, Broekaert E. Quality of life among opiate-dependent individuals: a review of the literature. Int J Drug Policy. 2010;21(5):364–380. | ||
Rudolf H, Watts J. Quality of life in substance abuse and dependency. Int Rev Psychiatry. 2002;14(3):190–197. | ||
Digiusto E, Panjari M, Gibson A, Rea F; NEPOD Research Group. Follow-up difficulty: correlates and relationship with outcome in heroin dependence treatment in the NEPOD study. Addict Behav. 2006;31(7):1201–1210. | ||
Nemes S, Wish E, Wraight B, Messina N. Correlates of treatment follow-up difficulty. Subst Use Misuse. 2002;37(1):19–45. | ||
Boyer L, Baumstarck-Barrau K, Cano N, et al. Assessment of psychiatric inpatient satisfaction: a systematic review of self-reported instruments. Eur Psychiatry. 2009;24(8):540–549. | ||
Zhiwei Z, Gerstein DR, Friedmann PD. Patient satisfaction and sustained outcomes of drug abuse treatment. J Health Psychol. 2008;13(3):388–400. | ||
Ware JE, Davis AR. Behavioral consequences of consumer dissatisfaction with medical care. Eval Program Plann. 1983;6(3):291–297. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 2000. | ||
Gandek B, Ware JE, Aaronson NK, et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: results from the IQOLA Project. International quality of life assessment. J Clin Epidemiol. 1998;51(11):1171–1178. | ||
Endicott J, Nee J, Harrison W, Blumenthal R. Quality of life enjoyment and satisfaction questionnaire: a new measure. Psychopharmacol Bull. 1993;29(2):321–326. | ||
Bourion-Bédès S, Schwan R, Epstein J, et al. Combination of classical test theory (CTT) and item response theory (IRT) analysis to study the psychometric properties of the French version of the quality of life enjoyment and satisfaction questionnaire-short form (Q-LES-Q-SF). Qual Life Res. 2015;24(2):287–293. | ||
Bourion-Bédès S, Schwan R, Laprevote V, Bédès A, Bonnet J-L, Baumann C. Differential item functioning (DIF) of SF-12 and Q-LES-Q-SF items among french substance users. Health Qual Life Outcomes. 2015;13(1):172. | ||
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. | ||
Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res. 2002;52(2):69–77. | ||
Lépine JP. L’échelle HAD [hospital anxiety and depression scale]. In: Guelfi JD, editor. L’évaluation Clinique Standardisée en Psychiatrie. Tome 1 [Standardized Clinical Psychiatric Assessment, Vol. 1]. Boulogne: Éditions Médicales Pierre Fabre; 1996:367–374. | ||
Trujols J, Garijo I, Siñol N, del Pozo J, Portella MJ, Pérez de los Cobos J. Patient satisfaction with methadone maintenance treatment: the relevance of participation in treatment and social functioning. Drug Alcohol Depend. 2012;123(1–3):41–47. | ||
Marchand K, Palis H, Peng D, et al. The role of gender in factors associated with addiction treatment satisfaction among long-term opioid users. J Addict Med. 2015;9(5):391–398. | ||
Bamm EL, Rosenbaum P, Wilkins S. Is health related quality of life of people living with chronic conditions related to patient satisfaction with care? Disabil Rehabil. 2013;35(9):766–774. | ||
Lundqvist LO, Ahlstrom G, Wilde-Larsson B, Schröder A. The patient’s view of quality in psychiatric outpatient care. J Psychiatr Ment Health Nurs. 2012;19(7):629–637. | ||
Siponen U, Valimaki M. Patients’ satisfaction with outpatient psychiatric care. J Psychiatr Ment Health Nurs. 2003;10(2):129–135. | ||
Bjørngaard JH, Ruud T, Friis S. The impact of mental illness on patient satisfaction with the therapeutic relationship: a multilevel analysis. Soc Psychiatry Psychiatr Epidemiol. 2007;42(10):803–809. | ||
Zendjidjian XY, Baumstarck K, Auquier P, Loundou A, Lançon C, Boyer L. Satisfaction of hospitalized psychiatry patients: why should clinicians care? Patient Prefer Adherence. 2014;8:575–583. | ||
Zendjidjian XY, Auquier P, Lançon C, et al. Determinants of patient satisfaction with hospital health care in psychiatry: results based on the SATISPSY-22 questionnaire. Patient Prefer Adherence. 2014;8:1457–1464. | ||
Trujols J, Iraurgi I, Oviedo-Joekes E, Guàrdia-Olmos J. A critical analysis of user satisfaction surveys in addiction services: opioid maintenance treatment as a representative case study. Patient Prefer Adherence. 2014;8:107–117. | ||
Perreault M, Leichner P, Sabourin S, Gendreau P. Patient satisfaction with outpatient psychiatric services. Eval Program Plann. 1993;16(2):109–118. | ||
Malet L, Llorca PM, Beringuier B, Lehert P, Falissard B. AlQoL 9 for measuring quality of life in alcohol dependence. Alcohol Alcohol. 2006;41(2):181–187. | ||
Ponizovsky AM, Grinshpoon A. Quality of life among heroin users on buprenorphine versus methadone maintenance. Am J Drug Alcohol Abuse. 2007;33(5):631–642. | ||
Aerts AT, Bigot JF. National Survey about Employment in 2002. National Institute of Statistics and Economical Studies; Paris: 2002. INSEE Première, No 857. | ||
Chaleix M. 7.4 Millions Adults Live Alone in 1999. National Institute of Statistics and Economical Studies; Paris: 2001. INSEE Première, No 788. | ||
Astals M, Domingo-Salvany A, Buenaventura CC, et al. Impact of substance dependence and dual diagnosis on the quality of life of heroin users seeking treatment. Subst Use Misuse. 2008;43(5):612–632. | ||
March JC, Oviedo-Joekes E, Perea-Milla E, Carrasco F, PEPSA Team. Controlled trial of prescribed heroin in the treatment of opioid addiction. J Subst Abuse Treat. 2006;31(2):203–211. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.