")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
The effects of Maras powder use on patients with migraine
Authors İnanç Y, Orhan FÖ , İnanç Y
Received 7 February 2018
Accepted for publication 13 March 2018
Published 7 May 2018 Volume 2018:14 Pages 1143—1148
DOI https://doi.org/10.2147/NDT.S164818
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Yılmaz İnanç,1 Fatma Özlem Orhan,2 Yusuf İnanç3
1Department of Neurology, Kahramanmaraş Sütçüimam University School of Medicine, Kahramanmaraş, Turkey; 2Department of Psychiatry, Kahramanmaraş Sütçüimam University School of Medicine, Kahramanmaraş, Turkey; 3Department of Neurology, Gaziantep University School of Medicine, Kahramanmaraş, Turkey
Background: It is accepted that smoking often triggers migraine. However, studies evaluating the relationship between the use of smokeless tobacco and migraine are limited, and there is no clear consensus on the subject. In this study, it was aimed to evaluate the relationship between migraine and Maras powder, which is the most common smokeless tobacco in Turkey.
Subjects and methods: The study included a total of 600 subjects, consisting of 300 patients (aged >18 years) diagnosed with a migraine according to the International Headache Society (IHS-ICHD-3 Beta) criteria after presenting at Sütçü Imam University Medical Faculty Neurology Policlinic with the complaint of headache between July 2016 and December 2016 and a control group of 300 individuals with similar features of age, gender, and educational level. A questionnaire was administered to each patient to record the status of smoking or using Maras powder.
Results: In the migraine patient group, 16.4% smoked and 9.7% used Maras powder. In the control group, the rate of smoking was 8.5% and the rate of Maras powder use was 11.86%. In males diagnosed with a migraine, the use of Maras powder was found to be at a higher rate than smoking (p<0.001). The Visual Pain Score and the headache frequency values were higher in those who smoked or used Maras powder than in non-users (p<0.001). The Fagerström Test for Nicotine Dependence Smokeless Tobacco results of the patients diagnosed with migraine and who used Maras powder were found to be higher than of those who smoked (Fagerström Test for Nicotine Dependence; p<0.001). When patients were evaluated according to the Migraine Disability Assessment Scale, the majority of migraine patients were seen to be at stages 1 and 2, and one in every three patients who used Maras powder cigarette and one in every two patients who smoked had headaches of a severity which affected their daily activities (p<0.001).
Conclusion: Smoking or the use of Maras powder increases the frequency and severity of migraines in a similar way. Therefore, Maras powder must be included in the scope of the fight against tobacco and people should be warned about this issue.
Keywords: cigarette, Maras powder, migraine, smokeless tobacco
Background
Migraine is a primary and episodic headache, which is known to be associated with various forms of neurological, gastrointestinal, and autonomic changes over the course of many years.1 Migraine affects one in every seven people in the general population, although it varies between countries and regions.2 It is often seen in working-age groups and females, and to a lesser degree in children and elderly people. Migraine seriously affects the quality of life and daily life of a patient and causes serious labor loss.3,4 Although controversial results have been obtained in studies about the effect of smoking on migraine, the general view is that cigarette smoke, together with nicotine and other chemical derivatives contained in the cigarette, has a serious effect on the frequency and triggering of a migraine. There are smokeless tobacco products under various names and specifications in the world, especially in Southeast Asia, India (gutka), Bangladesh (bidi), and Turkey (Maras powder). More than 300 million people in >70 countries worldwide are estimated to smoke smokeless tobacco.5 Maras powder, an important example of a smokeless cigarette, is frequently used in Turkey’s Eastern Mediterranean region.6–8 It is used by being put into the mouth, under the lip. It is widely accepted that cigarette smoke triggers migraine, and there is a limited number of studies on the effect of smokeless cigarettes on migraine.9,10
In this study, it was aimed to investigate the relationship between the use of Maras powder by migraine patients and the migraine attack severity and frequency.
Subjects and methods
The study included a total of 600 subjects, consisting of 300 patients (aged >18 years) diagnosed with migraine headache according to the International Headache Society (Headache Classification Committee of the International Headache Society-The International Classification of Headache Disorders, 3rd edition)11 criteria after presenting at Kahramanmaraş Sütçü Imam University Medical Faculty Neurology Policlinic with the complaint of headache between July 2016 and December 2016 and a control group of 300 individuals with similar features of age, gender, and educational level. Approval for the study was granted by the Sütçü Imam University Medical Faculty Local Ethics Committee of the Kahramanmaraş Sütçü Imam University Medical Faculty Neurology clinic date: 15.06.2016; number: 194), and written informed consent forms were obtained from all the study participants.
Fagerström nicotine addiction test (Fagerström Test for Nicotine Dependence [FTND])
This test was developed by Karl O Fagerström to determine the level of physical addiction to smoking and was adapted to the Turkish language by Uysal et al.12 The test consists of six closed-ended questions. A score of <5 points in the test was defined as mild, 5–6 points as moderate, and ≥7 points as severe nicotine or Maras powder addiction.13 To assess smokeless tobacco addiction, the Fagerström survey (Fagerström Test for Nicotine Dependence smokeless tobacco [FTND-ST]), adapted by Mushtaq and Beebe for tobacco-free cigarettes, was used in this study.14
Migraine Disability Assessment Scale (MIDAS)
The MIDAS was administered to the patients diagnosed with migraine to determine the duration of illness, the duration of attacks, the frequency of attacks, the presence of aura, and the severity of a migraine. The patients were asked, “For how many days in the last 3 months has there been at least a 50% deterioration in your work, home, and social activities because of your migraine?15” According to the MIDAS scores, 0–5 was classified as the absence of loss–very little loss, 6–10 as slight loss, 11–20 as moderate loss, and 21+ as severe loss.
Hospital Anxiety Depression Scale
This scale was developed by Zigmond and Snaith (1983) to assess the risk in terms of anxiety and depression, and to assess the level and severity change of this risk.16 The validity and reliability study of the modified version of the scale for Turkey was performed by Aydemir et al.17 Of the total 14 questions, 7 (single numbers) measure anxiety and 7 (double numbers) measure depression. The lowest score that patients can take from both subscales is 0 and the highest score is 21.
Statistical analysis
SPSS 22.0 (IBM Corporation, Armonk, NY, USA) program was used to analyze the variables. The Mann–Whitney U-test was used together with Monte Carlo results in the comparison of two independent groups according to quantitative data. The one-way analysis of variance test, as a parametric method, was used for the comparison of independent multiple groups in respect of quantitative results, while the Kruskal–Wallis H test, as a nonparametric test, was used with the Monte Carlo simulation technique results. Dunn’s test was used for the post hoc analyses. Pearson’s chi-square and Fisher’s exact tests were used together with exact and Monte Carlo results for the comparison of categorical variables. The quantitative variables were shown as mean±SD and median range (maximum–minimum), and the categorical variables were shown as number (n) and percentage (%). Variables were analyzed at 95% CI, and a value of p<0.05 was considered statistically significant.
Results
Of the patients diagnosed with migraine, 75.67% were female; 16.4% of these patients smoked and 9.7% used Maras powder. In the control group, the smoking rate was 8.5% and the rate of Maras powder use was 11.86%. The rate of smoking in migraine patients was found to be higher than that of non-migraine patients, whereas the use of Maras powder was found to be more common in non-migraine patients (p=0.013). It was seen that 65.31% of the patients diagnosed with a migraine who smoked were female. The use of Maras powder in females was seen to be low in both groups. In males diagnosed with migraine, the use of Maras powder use was found to be higher than smoking addiction (p<0.001). It was found that the use of any tobacco product was highest in patients who lived in cities (p=0.186; Table 1).
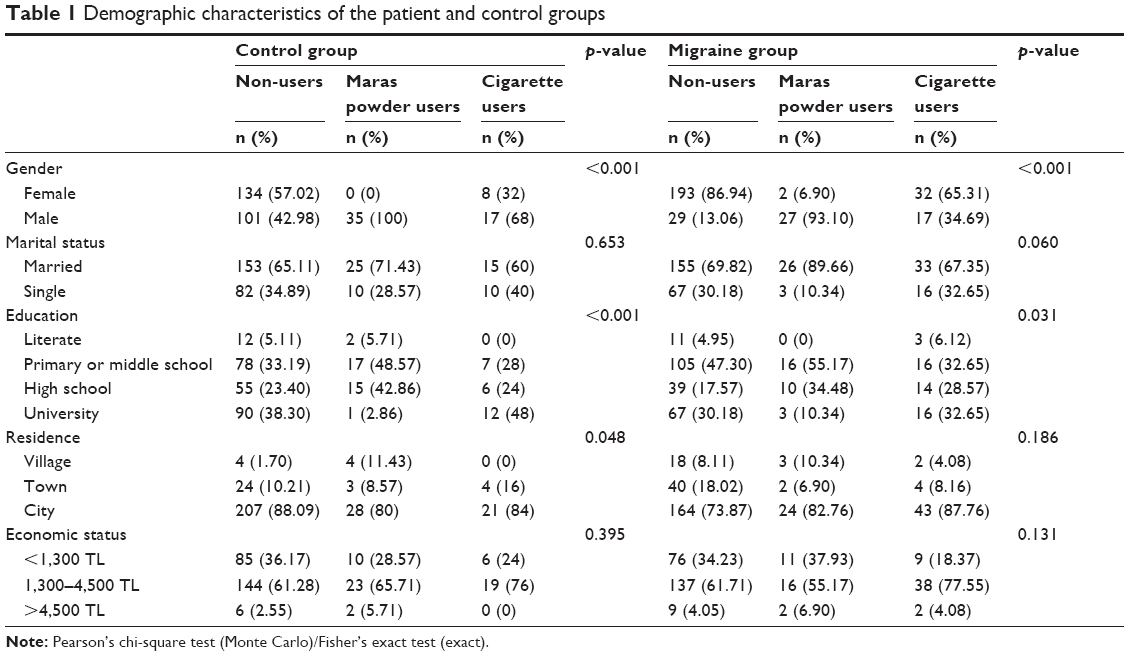 | Table 1 Demographic characteristics of the patient and control groups |
There was no significant difference between the groups in terms of smoking addiction (p=0.006 and p=0.093, respectively; Table 2), although it was observed that the migraine patient group was composed of younger patients. The Hospital Anxiety Score (HAS) anxiety depression scores of patients diagnosed with migraine were found to be higher than of those without a migraine diagnosis (p<0.001; Table 2).
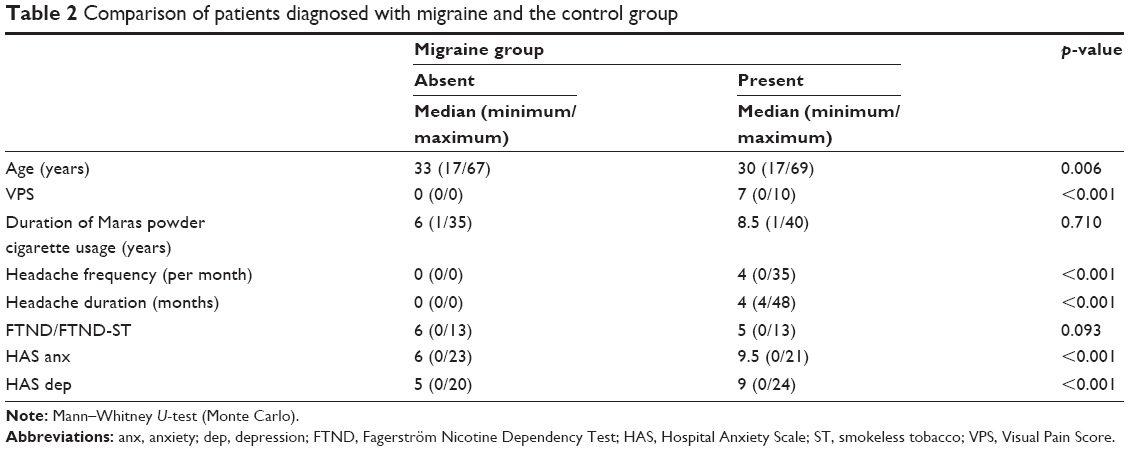 | Table 2 Comparison of patients diagnosed with migraine and the control group |
The mean age of migraine patients using Maras powder was higher than that of those who did not use tobacco products and smokers (p=0.007). The visual analog scale score and headache frequency were higher in smokers or Maras powder users than in those who did not use either product (p<0.001). The FTND-ST scores of patients using Maras powder were higher than those of smokers (p<0.001). The headache frequency in migraine patients using tobacco products (cigarettes or Maras powder) was significantly increased (p=0.016 and p=0.021, respectively) compared to those who did not use such products. No significant difference was found with respect to headache duration and frequency between those who used Maras powder and smokers (p>0.05). The Hospital Anxiety Score and depression scores were similar in all three groups (p>0.05; Table 3).
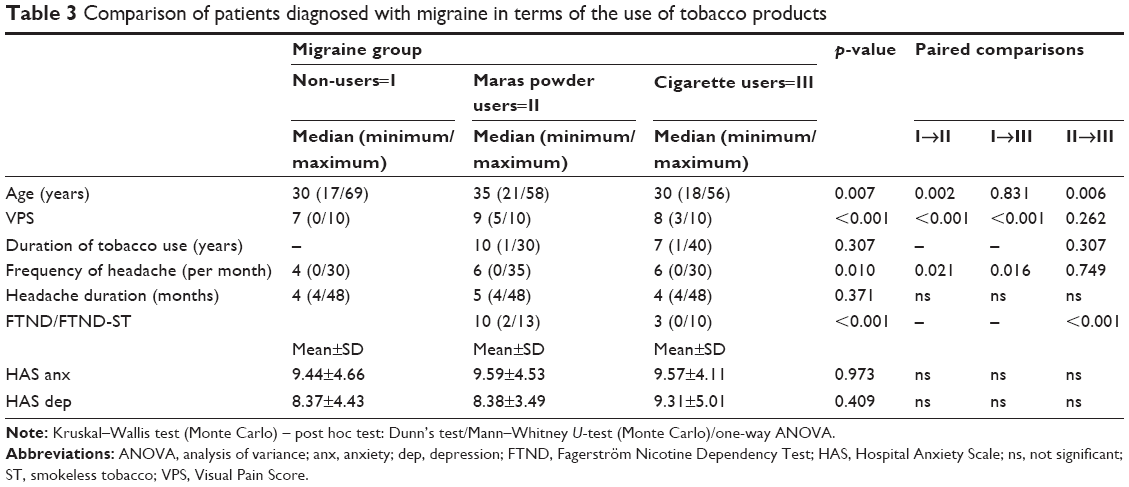 | Table 3 Comparison of patients diagnosed with migraine in terms of the use of tobacco products |
The incidence of migraine aura was determined to be higher in patients using Maras powder (p=0.012). When the patients were compared in terms of triggering factors, there was no significant difference between the patients using and not using tobacco products (p>0.05). Migraine patients who did not use tobacco products were frequently found to have MIDAS scores at stages 1 and 2, and one in every three patients who used Maras powder and one in every two patients who smoked had headache of a severity which affected their daily activities (p<0.001; Table 4).
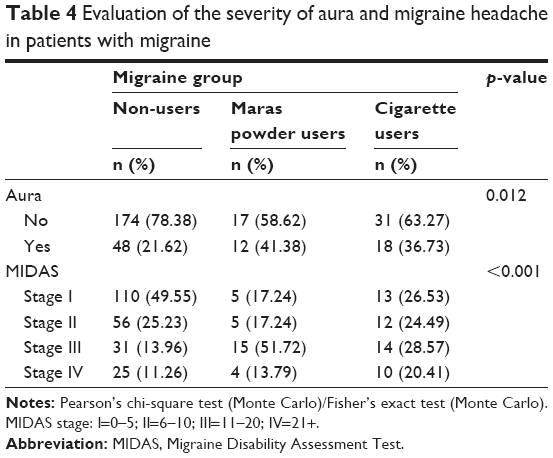 | Table 4 Evaluation of the severity of aura and migraine headache in patients with migraine |
Discussion
A migraine is a chronic and episodic type of headache that has a significant effect on quality of life. In this study, it was found that the use of Maras powder increased migraine frequency, duration, and severity in a manner similar to smoking. These results are highly consistent with the literature reports.18,19 There are studies in literature that have different conclusions regarding the relationship between smoking and migraine.2,20 The results of the present study are largely consistent with the literature, where it is reported that smoking and the use of Maras powder, a smokeless tobacco product, are important triggers for migraine.19,21,22
The use of smokeless tobacco is particularly prevalent in South Asian countries. It is reported to be used at higher rates by younger adults, lower income groups, and less educated people.23 This is explained by the fact that smokeless cigarettes are cheap, easily accessible, and can be used in closed areas, and therefore, women and children can use them easily in society. However, there is a misconception that it is less harmful than smoking because it is smokeless.9 Although the damage is not fully known, there has been no significant decrease in the use of smokeless cigarettes over the past 20 years.
Maras powder is a smokeless tobacco product, which is sucked and chewed on the inner surface of the lips, similar to other smokeless tobacco products. The present study was conducted in the city of Kahramanmaraş in the Eastern Mediterranean region of Turkey, the place after which Maras powder is named and where smokeless tobacco habits are common. In studies conducted in this region, it has been reported that up to 16% of people used Maras powder.24 In the present study, it was determined that 16.4% of migraine patients were smokers and 9.6% used Maras powder. It is thought that the current increase in the rate of living in cities, the decrease in social pressure, and easier access to cigarettes have created this situation. These findings are also important with regard to the use of Maras powder in Turkey, which are similar to the results of previous studies and indicate that is still used in significant quantities.
Stimulants (noise, light, smell) before the beginning of pain are questioned during the determination of migraine triggers. However, the effects of other stimulants (such as smells, cigarettes) during the early period of pain are often ignored. According to the results of a study by Lima et al conducted in 96 male patients, it was found that smell, especially perfume, cigarette smoke, and cleaning products (48%) were the second most frequent migraine trigger after stress (59%).25,26 It is known that a stressful working life, sleeping problems, air change, skipping meals, bright light environments, and some nutrients are the major triggering factors of a migraine. Some migraine patients say that the onset of headache attacks does not depend on any specific cause. In addition, hormonal changes have an important role in migraine pathogenesis. This may explain the frequent occurrence of migraine attacks in females during the menstruation period.27 In this study, the incidence of migraine in females and urban residents was determined to be higher, which was seen to be consistent with literature.22,28 It was also observed that stressful and noisy city life facilitated the occurrence of migraine cases. While there is no full consensus on the effects of smoking on migraine, many studies have shown that smoking is a direct trigger for migraine and that stopping smoking can reduce the frequency and severity of migraine attacks.18,20,29–31 It has also been shown that smoking improves myofascial pain, which causes a deterioration in sleeping pattern and quality.32 The high smoking rate in patients with back pain, headache, and fibromyalgia makes the situation even more difficult by creating a vicious circle.33 In a case–control study conducted by Abul et al in 276 patients, smoking and use of smokeless tobacco (bidi) were shown to be closely associated with migraine.19 In the present study, it was determined that Maras powder significantly increased the severity and frequency of migraine and affected the quality of life, and these effects were similar to those of smoking. Some social studies have shown that smokeless tobacco products can be used to stop smoking. However, it does not seem to be a good method of stopping smoking as it is difficult to control smokeless cigarettes and they have higher nicotine content. In a study conducted in the USA, 3,996 young males using smokeless tobacco products between the ages of 11 and 19 were followed during a 4-year period. Based on the results of the study, it was emphasized that the use of smokeless tobacco is a beginning for smoking.34 The most commonly used test for assessing smoking addiction is the Fagerström nicotine dependence test (FTND).13 The present study used FTND to determine the degree of addiction of smokers and the FTND-ST scale, which was adapted to smokeless tobacco products by Mushtaq and Beebe to determine the degree of addiction of Maras powder users. It was observed that the physical nicotine addiction of migraine patients using Maras powder was significantly higher than that of smokers. This result showed that Maras powder was a serious stimulus to start smoking rather than being a step toward stopping smoking. It can be predicted that the use of smokeless tobacco, especially in young people, will cause major health problems in the future. Considering the risks of secondhand smoking, it is important to include Maras powder in tobacco control programs.
Our work has some limitations. Since the patients who were referred to our hospital were selected especially for patient selection, the use of Maras powder was evaluated by questionnaires and the low literacy rate of the patients did not give optimal results in the evaluation of the tests. However, the fact that the patient groups are not similar and the gender, places of residence, and cigarette smoking rates of the control group differ from other groups seems to be an important limitation. The fact that groups with similar characteristics are not selected for the evaluation of migraine triggers can be considered as another important deficiency.
To the best of our knowledge, this is the first study to have demonstrated the association between migraine and the use of Maras powder. Based on the results of the study, it can be considered that reducing the use of Maras powder may also reduce the frequency and severity of migraine. It is also believed to be important to provide more information to the community about Maras powder, which seems to have a higher potential for physical dependence.
Conclusion
It was found that the use of Maras powder, which is the most popular smokeless tobacco product in Turkey, increases the severity of migraine attacks in a similar way to cigarette smoking and has a higher potential for nicotine addiction compared to smoking. To eliminate the belief35 that its relationship with migraine is less than smoking because of the smokeless property, there is a need to inform people about this issue and to make the necessary regulations.
Disclosure
The authors report no conflicts of interest in this work.
References
Barbanti P, Aurilia C, Egeo G, Fofi L. Migraine prophylaxis: what is new and what we need? Neurol Sci. 2011;32(Suppl 1):S111–S115. | ||
Rasmussen BK. Migraine and tension-type headache in a general population: precipitating factors, female hormones, sleep pattern and relation to lifestyle. Pain. 1993;53(1):65–72. | ||
Pradalier A, Auray J-P, El Hasnaoui A, et al. Economic impact of migraine and other episodic headaches in France: data from the GRIM2000 study. Pharmacoeconomics. 2004;22(15):985–999. | ||
Stewart WF, Wood GC, Manack A, Varon SF, Buse DC, Lipton RB. Employment and work impact of chronic migraine and episodic migraine. J Occup Environ Med. 2010;52(1):8–14. | ||
Glover ED, Glover PN. The smokeless tobacco problem: risk groups in North America. Pounds (millions).1992;3–10. | ||
Aral M, Ekerbicer HC, Celik M, Ciragil P, Gul M. Comparison of effects of smoking and smokeless tobacco “Maras powder” use on humoral immune system parameters. Mediators Inflamm. 2006;2006(3):1–4. | ||
Sucakli MH, Ozkan F, Inci MF, Celik M, Keten HS, Bozoglan O. Effects of smokeless tobacco (Maras powder) use on carotid intima media thickness. Med Sci Monit. 2013;19:859–864. | ||
Kamal SMM, Islam MA, Rahman MA. Sociopsychological correlates of smoking among male university students in Bangladesh. Asia Pac J Public Health. 2011;23(4):555–567. | ||
Mutti S, Reid JL, Gupta PC, et al. Patterns of use and perceptions of harm of smokeless tobacco in Navi Mumbai, India and Dhaka, Bangladesh. Indian J Community Med. 2016;41(4):280–287. | ||
Sarker MAB, Rahman M, Harun-Or-Rashid M, et al. Association of smoked and smokeless tobacco use with migraine: a hospital-based case-control study in Dhaka, Bangladesh. Tob Induc Dis. 2013;11(1):15. | ||
Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition (beta version). Cephalalgia. 2013;33(9):629–808. | ||
Uysal MA, Kadakal F, Karsidag C, Bayram NG, Uysal O, Yilmaz V. Fagerstrom test for nicotine dependence: reliability in a Turkish sample and factor analysis. Tuberk Toraks. 2004;52(2):115–121. | ||
Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom K. The fagerstrom test for nicotine dependence: a revision of the fagerstrom tolerance questionnaire. Br J Addict. 1991;86(9):1119–1127. | ||
Mushtaq N, Beebe L. Psychometric properties of fagerstrom test for nicotine dependence for smokeless tobacco users (FTND-ST). Nicotine Tob Res. 2017;16(9):1095–1101. | ||
Lipton RB, Stewart WF, Stone AM, Lainez MJ, Sawyer JP. Stratified care vs step care strategies for migraine: the Disability in Strategies of Care (DISC) Study: a randomized trial. JAMA. 2000;284(20):2599–2605. | ||
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. | ||
Aydemir Ö, Güvenir T, Küey LKS. Hastane anksiyete ve depresyon ölçeği Türkçe formunun geçerlilik ve güvenilirliği. Türk Psikiyatr Derg. 1997;8(4):280–287. | ||
Gormley P, Anttila V, Winsvold BS, et al. Meta-analysis of 375,000 individuals identifies 38 susceptibility loci for migraine. Nat Genet. 2016;48(8):856–866. | ||
Abul M, Sarker B, Rahman M, Hossain S, Kasuya H. Association of smoked and smokeless tobacco use with migraine: a hospital-based case – control study in Dhaka, Bangladesh. Tob Induc Dis. 2013;11(1):15. | ||
López-Mesonero L, Márquez S, Parra P, Gámez-Leyva G, Muñoz P, Pascual J. Smoking as a precipitating factor for migraine: a survey in medical students. J Headache Pain. 2009;10(2):101–103. | ||
Zwart J, Aamodt AH, Stovner LJ, Hagen K, Bra G. Headache prevalence related to smoking and alcohol use. The Head-HUNT study. Eur J Neurol. 2006;508:1233–1238. | ||
Taylor FR. Tobacco, nicotine, and headache. Headache. 2015;55(7):1028–1044. | ||
Hossain MS, Kypri K, Rahman B, Arslan I, Akter S, Milton AH. Prevalence and correlates of smokeless tobacco consumption among married women in rural Bangladesh. PLoS One. 2014;9(1):e84470. | ||
Haki M, Kahraman H, Çelik M, Hamit S. An evaluation of knowledge, attitude and behavior regarding smoking and smokeless tobacco (Maras powder) use among high school children. Gaziantep Med J. 2015;21(4):225–232. | ||
Sjostrand C, Savic I, Laudon-Meyer E, Hillert L, Lodin K, Waldenlind E. Migraine and olfactory stimuli. Curr Pain Headache Rep. 2010;14(3):244–251. | ||
Lima AM, Sapienza GB, Giraud VDO, Fragoso YD. Odors as triggering and worsening factors for migraine in men. Arq Neuropsiquiatr. 2011;69:324–327. | ||
Epstein MT, Hockaday JM, Hockaday TD. Migraine and reporoductive hormones throughout the menstrual cycle. Lancet (London, England). 1975;1(7906):543–548. | ||
Woldeamanuel YW, Cowan RP. The impact of regular lifestyle behavior in migraine: a prevalence case-referent study. J Neurol. 2016;263(4):669–676. | ||
Albers LS, Ziebarth. Modifiable risk factors for primary headache. A systematic review. Europe PMC. 2014;952–960. | ||
Fernández-de-las-Peñas C, Hernández-Barrera V, Carrasco-Garrido P, et al. Population-based study of migraine in Spanish adults: relation to socio-demographic factors, lifestyle and co-morbidity with other conditions. J Headache Pain. 2010;11(2):97–104. | ||
Guzey Aras Y, Doğan Güngen B, Kotan D, Güngen AC. Effect of Smoking on Migraine Attack Frequency in Patients with Migraines. Acibadem University Journal of Health Sciences. 2016;(7)2:75–78. | ||
Custodio L, Carlson CR, Upton B, Okeson JP, Harrison AL, de Leeuw R. The impact of cigarette smoking on sleep quality of patients with masticatory myofascial pain. J Oral Facial Pain Headache. 2015;29(1):15–23. | ||
Orhurhu VJ, Pittelkow TP, Hooten WM. Prevalence of smoking in adults with chronic pain. Tob Induc Dis. 2015;13(1):17. | ||
Tomar SL. Is use of smokeless tobacco a risk factor for cigarette smoking? The U.S. experience. Nicotine Tob Res. 2003;5(4):561–569. | ||
O’Connor RJ, Hyland A, Giovino GA, Fong GT, Cummings KM. Smoker awareness of and beliefs about supposedly less-harmful tobacco products. Am J Prev Med. 2005;29(2):85–90. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.