")
Back to Journals » Journal of Blood Medicine » Volume 10
The Effects of Hydroxyurea Therapy on the Six-Minute Walk Distance in Patients with Adult Sickle Cell Anemia: An Echocardiographic Study
Authors Garadah T, Mandeel F , Jaradat A, Bin Thani K
Received 1 February 2019
Accepted for publication 16 October 2019
Published 27 December 2019 Volume 2019:10 Pages 443—452
DOI https://doi.org/10.2147/JBM.S203828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Taysir Garadah,1,2 Fatema Mandeel,2 Ahmed Jaradat,1 Khalid Bin Thani1,2
1Medical Department, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Kingdom of Bahrain; 2Medical Department, Cardiac Unit, Salmanyia Medical Complex, Manama, Kingdom of Bahrain
Correspondence: Taysir Garadah
Medical Department, College of Medicine and Medical Sciences, Arabian Gulf University, P.O. Box 26671, Manama, Kingdom of Bahrain
Tel +973-17239681
Fax +973-17230730
Email [email protected]
Background: The impact of hydroxyurea (HU) medication as treatment of choice has not been evaluated in adult sickle cell anemia (SCA) patients in terms of the 6-min walk distance (6 MWD).
Aim: The aim of the study was evaluating the effects of HU on the 6 MWD, serum brain natriuretic peptide (NT-pro BNP) level, and pulmonary hypertension (PH) measured by tricuspid regurgitation velocity (TRV).
Methods: In this cross-sectional, prospective study, 110 patients with homozygous SCA were studied and compared with age- and gender-matched healthy controls. Every patient was investigated via pulsed and tissue Doppler echo evaluation, 6-min walk test (6 MWT), and blood level for the level of NT-pro-BNP hormone. Data were compared in patients with (n = 59; group 1, G1) and without (n = 51; group 2, G2) HU medication. Pearson correlation analysis was applied and clinical follow-up for the frequency of acute chest syndrome (ACS). Analysis of variance (ANOVA) multivariate statistical analysis was applied between groups.
Results: In the study, 110 patients with SCA were studied and compared with 110 control patients. Patients in G1 compared with G2 had a longer 6 MWD (491 ± 64.4 m vs 428.6 ± 54.3 m, p < 0.005), higher HbF% (21 ± 2.5% vs 8 ± 1.8%, p < 0.005), and lower NT-pro-BNP level (314.1 ± 27.5 pmol/L vs 407 ± 18.9 pmol/L, p = 0.05). The mean TRV values were 2.8 ± 0.5 m/s in G1 versus 3.4 ± 0.4 m/s in G2, p < 0.005, and 1.5 ± 0.7 m/s in the control group. The high probability of PH based on a TRV > 3.4 m/s was 10.1% in G1 versus 17.6% in G2 and 3.6% in the control. There were weak positive correlations between NT-pro-BNP and TRV (r = 0.264; p = 0.005) and HbF% and 6 MWD (r = 0.452; p = 0.001). After 12 months of follow-up, frequency of acute chest syndrome (ACS) was twice as high in G2, at 32 patients, versus 16 in G1.
Conclusion: Patients with SCA on HU medication compared with no HU had significantly longer 6 MWD, lower level of NT-pro-BNP, higher HbF% level. After 1-year follow-up HU patients had less frequency of ACS. There were significant positive correlations between the level of NT-pro BNP level and TRV in m/s on echo.
Keywords: sickle cell anemia, 6-min walk test, hydroxyurea, NT-pro BNP, echocardiography, diastolic dysfunction, pulmonary hypertension
Introduction
Sickle cell anemia (SCA) is a hereditary hemolytic anemia characterized by the synthesis of abnormal hemoglobin, leading to abnormal mutant hemoglobin S (HbSS) in its homozygous form.1 Patients with SCA present with different clinical manifestations, such as vaso-occlusive crisis (VOC) and acute chest syndrome (ACS), with different degrees and frequencies of anemia. SCA also leads to long-term complications, including chronic organ dysfunction, which ultimately results in end organ failure.2
The 6-min walk test (6 MWT) is implemented in patients with SCA to evaluate the submaximal functional exercise capacity.3,4 The 6 MWT reflects the global physiological response of various systems in a situation simulating a daily life activity. It has been shown that patients with homozygous (HBSS) anemia had a shorter walking distance in comparison with SCA in heterozygous form (HbS) and thalassemic patients.5
Hydroxyurea (HU) is an antineoplastic agent that decreases sickle cell hemoglobin polymerization, vaso-occlusive events, and RBC hemolysis HU therapy in symptomatic patients with SCA is beneficial via its mediation of increased production of fetal hemoglobin (HbF; α2γ2).6 The increased production of HbF reduces RBC sickling and optimizes lifespan thus reducing hemolysis.7,8 The overall effect of HU in patients with SCA is reducing the relative concentration of hemoglobin S (HbS; α2βS2) by increasing production of HbF.
NT-pro B-type natriuretic peptide (pro-BNP) is used as a diagnostic marker of congestive cardiac failure. The level of pro-BNP has been shown to correlate with mean pulmonary arterial pressure (PAP) and pulmonary vascular resistance (PVR) in patients with pulmonary hypertension (PH).9 The serum level of NT-pro-BNP has been shown to be a useful marker in the stratification of PH in patients with SCA.10
Left ventricular (LV) diastolic filling pattern on pulsed and tissue Doppler was recently reclassified by American Society of Echocardiography (ASE).11 Accordingly, LV diastolic dysfunction is classified into the four following grades: grade I, with an E/A ratio ≤ 0.8 (where E is the early diastolic filling velocity on pulsed Doppler and A is the atrial contraction filling) and E-wave velocity ≤ 50 cm/s; grade II, with an E/A ratio between ≥0.9 and ≤1.9 and two of three supporting echo parameters of the following: a) E/e´ ratio > 14, where e´ is tissue Doppler of the E-wave, b) left atrial (LA) volume index > 34 mL/m2, and c) tricuspid regurgitation velocity (TRV) > 2.8 cm/s; grade III, with E/A ≥2 and elevated LA pressure, indicated by the pulmonary vein velocity with a systolic over diastolic (S/D) ratio < 1; and finally, undetermined grade, where E/A is between ≥0.9 and ≤1.9, but there is pulmonary vein S/D > 1 with two negative pieces of supporting echocardiogram (echo) evidence, as in grade II.
PH is defined as a resting mean pulmonary artery pressure (mPAP) ≥ 25 mm Hg. It occurs in 6–11% of patients with sickle cell disease.12 Echocardiography helps identify SCA patients at risk for PH, but definitive diagnosis requires right-heart catheterization.13 As per the guideline of the European Society of Cardiology (ESC),14 the probability of PH is high if the TRV is >3.4 m/s, but if TRV < 3.4 m/s, the probability of PH is assessed in conjunction with two of the following three markers: 1) inferior vena cava diameter > 21 mm with decreased inspiratory collapse < 50% with a sniff; 2) right ventricular outflow Doppler acceleration time < 105 ms; and 3) right ventricle (RV)/LV basal diameter ratio > 1.0). If the TRV is ≥2.8 but ≤3.4 m/s and two of the other three echo markers are positive, the probability is high. In contrast, if two are negative, then the probability is intermediate. Finally, if the TRV is <2.8 m/s with two negative markers, then the probability is low. One study utilizing right heart catheterization defined the prevalence of PH in sickle cell disease using a definition of mean pulmonary artery pressure > 25 mmHg to be between 6% and 10.5%.15
Currently, most of cross-sectional studies included pediatric SCA patients aged less than 12 years, but with few prospective randomized clinical trials on adult SCA patients in the literature.
Therefore, in this study of adult patients with SCA aged >14 years, we aim to accomplish the following: 1) Evaluate the outcomes of performing submaximal exercise capacity (6 MWT) in adult patients with SCA with and without HU treatment; 2) Assess the effects of HU therapy on the frequency of developing ACS and VOC; 3) Correlate the NT-pro BNP level with the degree of TRV assessed by echo Doppler; 4) Determine the correlation between HbF% and 6-min walk distance (6 MWD).
Materials and Methods
For this study, 110 adult patients with homozygous SCA (HbSS) aged ≥14 years were recruited between December 2011 and December 2012. The patients were selected from the Hematology Clinic at Salmanyia Medical Complex (SMC). SMC is the main public hospital in the country, with a population of 950,000 in the catchment area.
Patients were recruited prospectively and on a consecutive basis. A control group of patients with no SCA, matching for age and gender (n = 110), were recruited; the controls were attending the same clinic for hematological symptoms but with no evidence of SCA or any other blood disorders.
The diagnosis of SCA was based on hemoglobin electrophoresis and a solubility screening test. The study was approved by the local institutional ethics committee in SMC. An informed consent approved by the ethics committee was signed by every participants and parents or legal guardian provided the consent for participants under the age of 18 years, in accordance with the declaration of Helsinki.
The inclusion criteria were as follows: Each SCA patient had to exhibit a homozygous form and be in a steady state, with regular follow-up in the clinic for at least 1 year prior to recruitment. (A steady state in an SCA patient is defined as no hospitalization or emergency visits for pain crisis, ACS, stroke, splenic sequestration or other SCA crisis in the last month, and no blood transfusion (BT) in the last 3 months). In addition, every patient had to agree to perform the 6 MWT and an echocardiographic test. The exclusion criteria were the presence of severe motor, locomotor, or cognitive disability at the time of inclusion prohibiting individuals’ participation in the test.
The 6 MWT was performed according to the guidelines of the American Thoracic Society (ATS).16 The age-standardized predicted distance of the 6 MWD was established by Geiger et al3 and the 6 MWT was considered normal if the 6 MWD achieved was more than 80% of the age-standardized predicted distance, moderately decreased if the 6 MWD was 60–80% of the predicted distance, and severe if achieved <60% compared with the distances predicted based on the published reference equations by Geiger et al, where the predicted distance was calculated as follows: 6 MWD (m) = 196.72 + 39.81 × age (years) − 1.36 × age2 (years) + 138.28 × height (m). For each patient in the study, biometric data were collected for height, weight, body surface area, heart rate, and mean blood pressure. The history and frequency of the following clinical parameters were documented for all patients: the frequency of VOCs and hospital admissions, frequency of ACS, need for BT, the development of leg ulcers, stroke, and requirement for the treatment of HU over the past 12 months.
Patients were classified into two groups. Group 1 (G1) comprised adult SCA patients on active HU treatment for more than 12 months (n = 59), while group 2 (G2) included patients with no concurrent HU medication (n = 51). The dose of HU was given at 15–35 mg/kg per day in the form of a 500-mg capsule administered at night for at least 12 months. Laboratory data for the blood samples were obtained from all the patients by venipuncture in a fasting state. A complete blood count was performed on an automated hematology analyzer for the total white blood test, reticulocyte count percent, adult hemoglobin (Hbs), HbF and RBC indices of the mean cell volume (MCV) and mean cell hemoglobin concentration (MCHC). In addition, the serum levels of NT-pro-BNP, lactate dehydrogenase (LDH), and ferritin were determined. The data in the study represent an average of three laboratory results during the study period and both tests of echo and 6MWT were accomplished within 1-month period.
Transthoracic echocardiography was performed for every participant in the study. Two-dimensional (2D) and M mode echo sectors in addition to tissue and pulsed Doppler velocities were obtained using an E30 ultrasound machine (Philips Healthcare). Echocardiograph data were obtained by an echo specialist and read by a cardiologist. The M mode dimensions were measured according to the ASE criteria.17 Heart chamber dimensions, LV mass index, and the ventricular systolic ejection fraction percentage (LVEF%) were obtained using the single ellipse formula.18 Abnormal flow across the mitral and tricuspid valves was recorded as previously described;19 the TRV was assessed via the parasternal right ventricular inflow, parasternal short-axis, and apical four-chamber views. Continuous-wave Doppler sampling of the peak TRV was used to estimate the RV-to-right-atrial (RA) systolic pressure gradient with the modified Bernoulli equation. Inferior vena cava diameter measured in subcostal view and pulmonary vein velocity in apical four chambers. For the analysis purpose, PH was defined as high probability if TRV > 3.4 m/s, intermediate if >2.8 but <3.4 with two positive markers, and low probability if it was <2.8 m/s with two negative echo markers per the ESC guideline.20
The 6 MWT was performed indoors, along a flat, straight, enclosed corridor with a hard surface. The walking course was 30 m in length, the total distance walked was calculated and compared with that predicted based on height, weight, and age. The transcutaneous arterial oxygen saturation was determined by pulse oximetry in the same setting for pre- and post-test readings of SaO2%.
We hypothesized that patients on HU therapy would walk a longer distance and have less frequency of events like ACS, VOC, and requirement for blood transfusion. All data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 25.0. Data are presented as the mean ± standard deviation (SD). The Student’s t-test was used for continuous data and Chi-square for determining the frequency of non-continuous data. The differences of the mean of M mode data, septal wall thickness of the LV, RV cavity, and the LV mass index were calculated in all groups.
Pearson correlation coefficient analysis was used for assessing the associations between the serum level of pro-BNP and tricuspid valve velocity and the HbF% and 6 MWD. One-way analysis of variance (ANOVA) and post hoc analysis were used to determine the significance of mean difference in G1 and G2 versus control and then between G1 and G2. All the reported p-values were two-tailed, and a p-value < 0.05 was regarded as significant.
Results
The mean age of patients with SCA and HU therapy (G1) was 27.5 ± 9.1 years (range: 14–42 years), and there were 39 males (66.1%). In G2, in which the SCA patients had no HU, the mean age was 29.3 ± 8.7 years, and there were 34 males (66.6%), while in the control group, the mean age was 28.7 ± 8.7years (range: 14–42 years) and there were 73 males (66.3%).
On arbitrary division for age categories of 14–18 years as adolescence and 18–40 years as adult, it was disclosed that number of adolescents in G1, G2, and control was of 16, 14, and 25, respectively. Table 1 shows the clinical characteristics of patients with SCA in G1 (n = 59), G2 (n = 51), and the control group (n = 110).
 |
Table 1 Clinical Characteristics of the Patients with SCA and Control Group. Data Presented as Mean ± SD |
The data comparison was carried out using the ANOVA test between the three groups. There was no significant difference between the three groups in terms of heart rate or mean blood pressure. Hemoglobin was lowest in G1 compared with G2 and control, with significant statistical differences between each of them. The platelet and WBC counts were significantly lower in G1 and G2 compared with the normal population.
The HbF% was higher in G1 (21.7%) than G2 (8.18 %), p < 0.001 and the control group (1.7%). Hematocrit was lowest in G1 (24.7) versus G2 (28.8) and the control group (44.8), and the difference was statistically significant between all the groups.
The pro-BNP level was significantly lower in G1 versus G2, but both levels were higher than that of the control group. The leucocyte count was significantly lower in G1 versus G2 (p < 0.05), and both counts were statistically significantly lower than that of controls. The body mass index was significantly lower in G1 versus G2 (p < 0.05), and both results were statistically significantly lower than that of controls. The reticulocyte count and LDH were significantly higher compared with the normal population; however, both parameters were significantly lower in G1 versus G2, at p-values of 0.005 and 0.007, respectively.
Table 2 shows the echocardiographic data of patients with SCA with and without treatment with HU and the control group. Patients with SCA in G1 and G2 had significant right ventricle dilation compared with normal but no significant difference compared with each other. The LV mass index was higher in G2 compared with G1, and both were higher than the control, with a significant difference between the three groups. The LV systolic function presented as LVEF% was significantly lower in G1 and G2 compared with controls, but there was no significant difference between the two groups. The LA area was highest in G2, with significant differences between G1 and G2 and between both groups and the control. G1 and G2 showed signification dilation in the RV compared with the control, but they did not exhibit a difference from each other in this regard. The TAPSE as a marker of RV function was significantly low in G2 compared with G1, and both were significantly lower compared with the control. The mean tricuspid valve velocity was highest in G2 (3.4 ± 0.4 cm/s), and this was significantly higher than that of G1 (2.9 ± 0.5 cm/s; p < 0.005); both groups showed significantly higher results than that of the control (1.5 ± 0.7 cm/s).
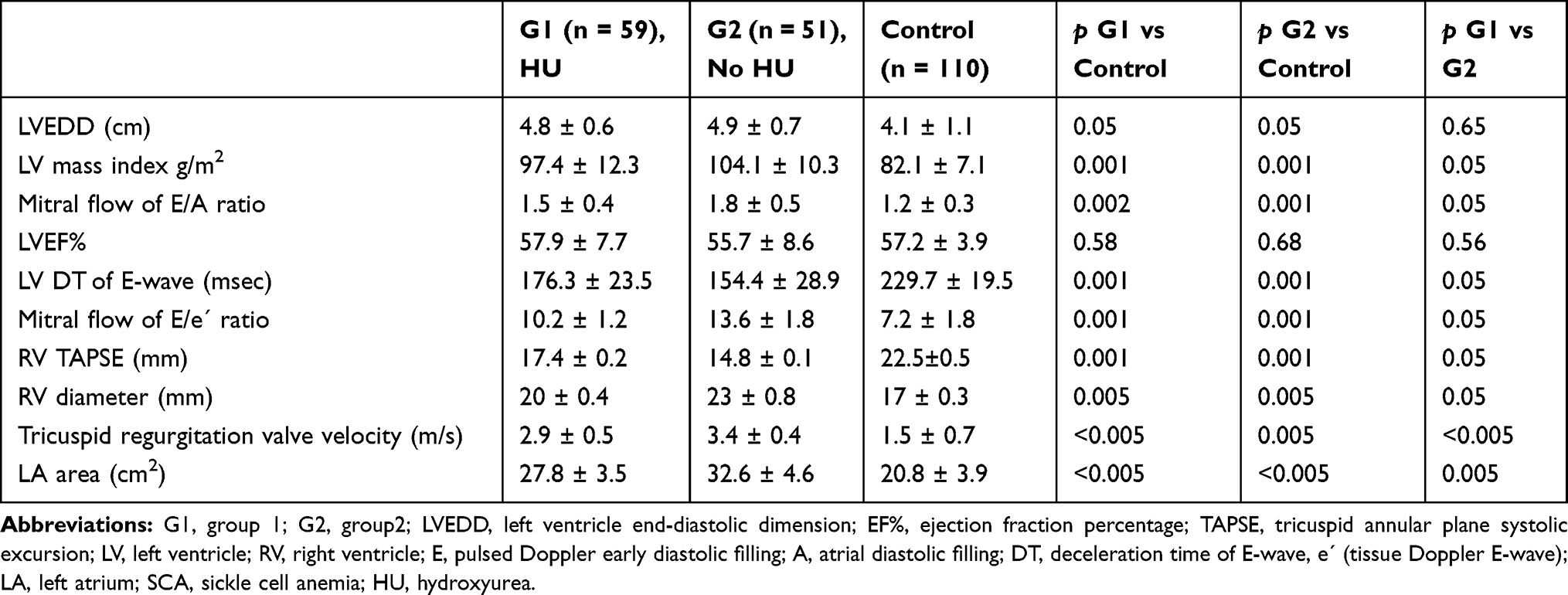 |
Table 2 Echocardiographic M Mode and 2D, Pulse, and Tissue Doppler Echocardiographic Data in the Patients with SCA and Control Data are Presented as Mean Value ± SD |
The pulse Doppler mean of E/A ratio was highest in G2 of 1.8 ± 0.5, that is significantly higher than G1 of 1.5 ± 0.4 and both were higher than that of the control of (1.2 ± 0.3). There was a statistically significant difference between each group and the control. The ratio of the E-wave of the pulse Doppler to E wave on the tissue Doppler was highest in G2 (13.6 ± 1.8), and it was significantly higher than that of G2 (10.2 ± 1.2); both values were significantly higher than that of the control group (7.2 ± 1.8). In G1, type 1 diastolic dysfunction was observed in 22 (37.5%), type 2 in 8 (13.5%), type 3 in 21 (35.5%), and undetermined type in 8 patients (13.5%). In G2, there were 11 patients (21.6%) with type 1, 6 (11.7%) with type 2, 30 (58.8%) with type 3, and 4 (7.9%) of undetermined type. Finally, in the control group, the results were 15 (13.6%), 8 (7.2%), 22 (2.0%), and 65 patients (59%) with types 1, 2, 3, and undetermined, respectively.
In G1, the tricuspid velocity on continuous wave Doppler was <2.8 m/s in 42 patients (71.1%; low probability, ≥2.5 but ≤3.4 m/s in 11 patients (18.6%; intermediate probability), and >3.4 m/s in 6 patients (10.1%; high probability). In G2, there were 30 patients (58.8%) in the low probability category, 12 (23.5%) with intermediate probability, and 9 (17.6%) with high probability. In the control group, there 90 patients (81.8%) with low probability, 20 (18.2%) with intermediate probability, and 4 (3.6%) with high probability. The correlation between the serum level of BNP in p mol/L and the velocity of tricuspid valve regurgitation in cm/s was r = 0.264, p = 0.005, showing positive weak correlation. Likewise, in patients with SCA, the correlation between the HbF% and the 6 MWD was positive, with r = 0.452, p = 0.001).
Table 3 shows the hemodynamic data of the patients with SCA and controls. It was found that the resting oxygen saturation was significantly lower in G2 compared with G1, and both were lower the control level; there were significant differences of So2% between resting and after 6MWT in G2 only with mean of 0.9±0.1, P<0.05, but the mean difference in G1 and control was 0.3±0.2 and 0.1±0.1 with no significant difference. The heart rate increments in the three groups after the 6 MWD were not significant, and the mild increment of the mean BP after the 6 MWD was not significant. The distance walked in the groups was higher in G2 by >50 m, and the control was higher than G1 by >50 m. The difference of the mean distance walked in the three groups was significant.
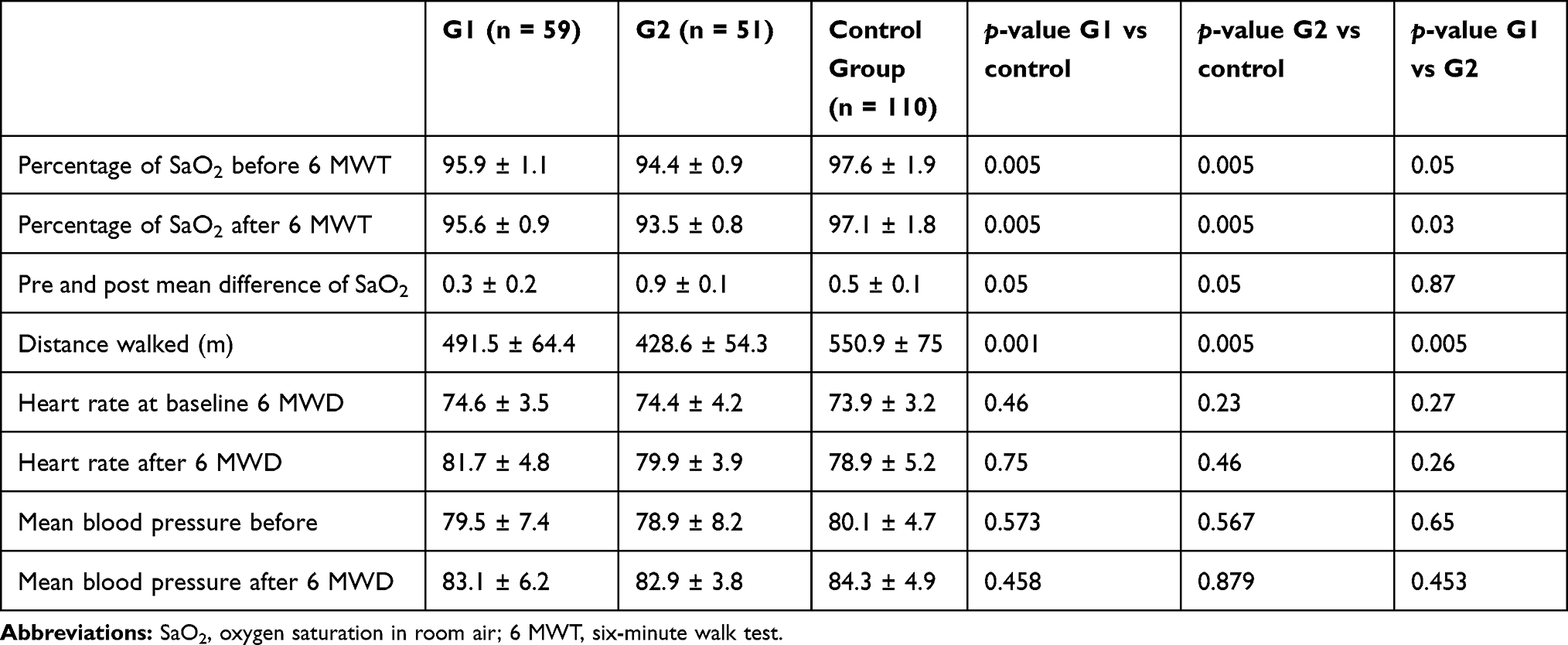 |
Table 3 Findings of 6 MWT in the SCA Patient Group 1 (G1) on HU and Group 2 (G2) with No HU Compared with the Control Group. Data Presented as Mean ± SD |
Figure 1 shows the percentage of patients who achieved >80% of the predicted distance, those who reached 60–80% of the predicted distance, and those who walked <60% of the distance. In G1, 26 patients reached >80%, 27 reached 60–80%, and 6 walked <60%; in G2, 8, 27, and 16 patients, and in the control group, 98, 18, and 4 patients reached these distances.
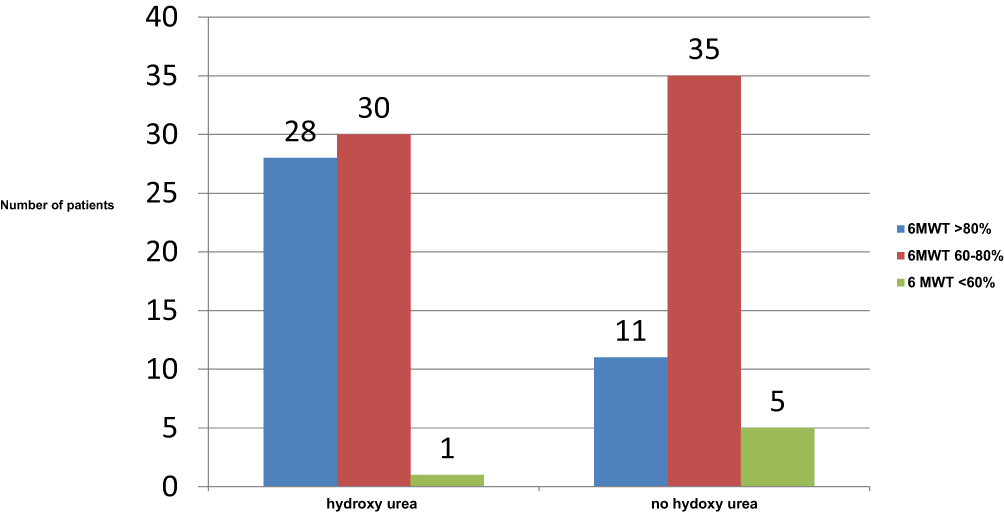 |
Figure 1 The rate of maximum predicted distance achieved on 6MWT in patients with sickle cell anemia, with hydroxyurea medication, n=59 and no hydroxyurea, n =51. |
At the 12-month follow-up, among patients in G1 (SCA on HU), there were 4 who required BT, 16 with ACS, and 15 with VOC. In group 2, there were 8, 32, and 20 patients, and in the control group, there were 4, 3, and 5 with BT, ACS, and VOC, respectively. The frequency of ACS was twice higher in G2 compared with G1.
Table 3 shows the results of the 6 MWT in patients with SCA on HU medication (n = 59) compared with no HU medication (n = 51). Patients on HU had higher total hemoglobin and HbF% values and longer walking distance compared with those without HU medication. The mean heart rate and blood pressure showed no significant difference in the two groups and the control. In subgroup analysis hemoglobin HbF% in the study, there were 30 (50.8%) patients with HbF ≥15%, 17 (28.8%) with HbF % between 10% and 15%, and 12 (20.3%) with ≤10% in G1 while in G2, there were 5 (9.8%) patients with HbF ≥ 15%, 11 (21.6%) between 10% and 15%, and 35 (68.6%) with ≤10%.
Figure 1 shows the outcomes of patients for the 6-min walk in terms of the percentage of achieving the maximum predicted walking distance. In the HU medication group, 30 patients (50.8%) reached >80% of the predicted 6 MWD, 28 (47.4%) reached 60–80% of the predicted 6 MWD, and only 1 patient reached <60% of the predicted 6 MWD. In patients with no HU medication, the results were 11 (21.5%), 35 (68.6%), and 5 (9.8%) for these categories. Over 1 year of follow-up, 20 G1 patients (33%) had ACS, 14 (23.7%) had VOC, and 6 (10.1%) had BT. In contrast, 26 (50.9%), 22 (43.1%), and 12 G2 patients (23.5%) and 3, 5, and 4 controls exhibited the same complications, respectively.
Discussion
This study is designed to compare the results in adult patients with SCA taking HU medication (G1) with those who were not taking HU (G2) in terms of the 6 MWD and Doppler echo findings, in addition to serum level of NT-pro-BNP hormone. Type 1, diastolic filling pattern (abnormal relaxation) was observed in 37.2% in G1 patients, which was higher than the rate of 21.6% in G2. Type 3 (restrictive) was found in 35.5% of patients in G1 that is lower compared with 58.8% in G2 and type 3 patterns. The LA area was also significantly lower in G1 of 27.8 cm2 compared with G2 of 32.6 cm2, p < 0.005.
The higher restrictive pattern with the higher LA area in G2 may be due to a stiffer myocardium in SCA patients with no HU medication. The higher percentage of a restrictive pattern in SCA in our patients is in keeping with a study by Appleton et al,21 in which the preload increment was associated with increased early filling and shortened deceleration time. In two separate studies, the diastolic pattern of LV was mainly the abnormal relaxation pattern, contrary to our finding in this study; however, the population of both was a combination of SCA and thalassemia.22,23
The LVEF% was slightly lower in patients with SCA compared with controls, but there was no significant difference between the two. However, the LVEF% was higher (>55%) in all patient groups, as it seems the diastolic function is impaired early in patients with adult SCA, while systolic function is preserved.24 Although significant dilation of the LV in SCA has been well documented,25 LV systolic dysfunction seems to be a late and uncommon complication of this disorder.
The RV was significantly dilated in both G1 and G2 compared with control, but with no significant difference between them. Furthermore, TAPSE as a marker of RV function was significantly low in G2 compared with G1, and both were significantly lower than that of the control. The mean TRV was 3.4 ± 0.4 cm/s in G2, which was significantly higher than that in G1, at 2.9 ± 0.5 cm/s, p < 0.005 and both groups exhibited significantly higher values than that of the control, at 1.5 ± 0.7 cm/s.
In the current study, patients with HU medication had a lower rate of a TRV level above 3.4 m/s, which is of high probability of PH. This rate of >3.4 cm/s was observed in 10.1% in G1patients versus 17.1% in G2. Furthermore, a TRV < 2.8 m/s, a level at which it is of low probability of PH, was found in 71.1% in G1 versus 58.8% in G2. The possible mechanism of RV dysfunction may be primarily due to lung involvement with predominantly high rates of repetitive VOC and ACS.
The higher restrictive diastolic pattern in G2 may play a role in the development of a higher rate of those patients with tricuspid valve velocity (TRV) of >3.4 m/s. In one study, Sachdev et al26 observed that diastolic dysfunction and PH with a TRV of >2.5 m/s can develop independently in patients with SCA, each contributing to increase mortality.
The salutary effect of HU on echocardiogram parameters was evident in G1 in terms of improved RV function with higher TAPSE and lower LV stiffness, evidenced by the lower E/e´ of 10.2± in G1 versus 13.6± in G2. The beneficial effect was evident with a higher frequency of patients with a TRV rate of <2.8 in G1 (71.1%) versus G2 (58.8%). The development of diastolic dysfunction and high TRV > 3.4 m/s in SCA has been suggested as of multifactorial origin, such as in the development of myocardial infarction followed by fibrosis, myocardial haemosiderosis, and microcirculatory dysfunction.27 Furthermore, sickling phenomena, VOCs, and ACS, with repetitive episodes of intravascular hemolysis result in the release of hemoglobin, which scavenges nitric oxide. This leads to acute and then chronic pulmonary vasoconstriction.
In a recent report by Niss et al,28 using cardiac magnetic resonance (CMR) imaging in patients with SCA, it was observed that diffuse myocardial fibrosis is a common feature in patients with SCA, appearing to predate the development of diastolic dysfunction. In this study, the prevalence of high TRV of more than 3.4 m/s, which is suggestive of PH, was 13.6% (15 adult SCA patients) in both groups. This is a higher number than that found in a previous report by Minniti et al,4 where it was 11%, and it is lower than our observation in previous reports of 28%, although the cut-off point was a TRV of <2.5 m/s.29
The serum level of NT-pro-BNP hormone was significantly higher in SCA patients in G2 in comparison with compared with G. The hemolysis-induced vasculopathy in SCA predisposing to RV dilation with higher TRV that invite for higher NT-pro BNP. In a previous report, a high NT-pro-BNP level was positively correlated with high LA area and diastolic dysfunction.30,31 In this study, there was a positive correlation between the serum level of NT-pro BNP and the velocity of tricuspid valve regurgitation (r = 0.264, p = 0.005). In one study, in the context of chronic precapillary PH, the serum NT-pro-BNP level was shown to determine the clinical severity of disease processes and is independently associated with long-term mortality.32
Another study showed that serum NT-pro-BNP levels were higher in patients with SCA and PH and correlated directly with TRV (r = 0.50, p < 0.001) on Doppler echo. In addition, it was observed that an NT-pro-BNP level of ≥160 pmol/L had a 78% positive predictive value for diagnosis of PH31 In this study, there was a weak positive correlation between the serum level of NT-pro-BNP and the TRV, with a correlation coefficient of r = 0.264, p = 0.005.
Hemodynamics of Walking Distance
The 6 MWD in the study groups showed a significantly higher walking distance in G1 versus G2 patients, with a mean of 62.9 m in G1 compared with G2. However, in both groups, the distance was significantly lower in comparison with the control group.
The salutary effect of HU on 6 MWD in SCA may be explained by the significantly higher HbF% of 21.7 versus 8.18% among those with no HU. This observation agreed with others, where the higher HbF% increases the physical capacity in SCA patients.33
The rate of patients with SCA who had achieved >80% of the predicted walking distance was three times higher than that in G1 versus G2 (47.4% versus 18.6%). Those who achieved a predicated distance of 60–80% were 50.8% in G1 versus 68% in G2. In the control group, 81.8% and 13.6% of the participants achieved >80% and 60–80% of the predicted walking distance, respectively.
The mechanism of the salutary effect of HU in SCA is uncertain, but there was lowering in the blood levels of hemolysis markers (reticulocyte and LDH), with an increase in the HbF%.34 As gamma globin chain is not affected by the sickle mutation, the overall effect in patients with SCA is reducing the relative concentration of HbS. It was reported previously that patients with SCA on HU therapy had an HbF% > 20% above baseline, which was associated with 20% lower rates of hospitalization and 15% lower rates of VOC and ACS compared with an HbF% < 20%.35 Similarly, another report showed that a higher HbF in SCA patients was associated with fewer leg ulcers, less osteonecrosis, less frequent ACS and VOC, and reduced disease severity.36
In a recent retrospective study on African American adult’s patients with SCA, factors associated with exercise capacity and clinical outcomes were tested. The study disclosed that female gender, older age, higher body mass index, and lower hemoglobin were independently associated with lower exercise fitness. Furthermore, baseline exercise capacity predicted neither future ACS nor survival. However, exercise protocol was different and patients were mixture of SCA or thalassemia.37
In patients of G2, mean difference of oxygen saturation was 0.9±0.1.% between baseline and after 6MWT, while for G1 and control, the mean difference was of 0.3±0.2% and 0.1±0.1%, respectively, with no significance, and the association between hypoxemia at baseline and after the 6 MWT performance suggests that desaturation may be linked to endothelial dysfunction, with altered vasomotor function associated with reduced nitric oxide (NO) bioavailability that impairs oxygen exchanges.38 Our finding with oxygen desaturation after 6 MWT is in agreement with a recent study as observed that hydroxyurea improves the oxygen transport in SCA after 6MWT compared with those without HU as HU improves oxygen affinity and lowers the percentage of dense RBCs.39
Furthermore, after 12 months of follow-up, the requirement for BT was 50% less in G1 versus G2, and the frequency of admission with VOC was lower in G1, at 23.7%, versus 43.1% in G2 patients without HU, and there was a positive correlation between a high HbF% and 6 MWD, with a correlation coefficient of r = 0.452, p = 0.001.
Limitations
Although the number of patients recruited in the study was reasonable, it was still small as the patients were divided into two subgroups. In addition, the duration of observation may need to be longer than 12 months to conduct serial echo measurements for assessing the development of PH via TRV.
This study was conducted on adults > 14 years with no ability to evaluate the development and clinical characteristic of patients < 14 in childhood as most of current literature focused on childhood and adolescence of 6–18 years. In addition, the pulmonary hypertension probability was based on noninvasive definition using tricuspid valve velocity on echo Doppler, which may be a less sensitive method compared with invasive RV catheter-based study.
Conclusion
Patients with SCA on HU medication had significantly longer 6 MWD, lower NT-pro-BNP, higher HbF%. There was also a lower frequency of ACS, VOC episodes and BT compared with SCA with no HU medication. There were a significant but weak positive correlation between NT-pro-BNP levels and TRV on echo (r = 0.26), as well as between HbF% and 6 MWD (r = 0.45).
Acknowledgments
We are grateful to Mrs. Mona Jasem, the echo technician, for performing echocardiogram and data collection, as well as Mrs. Aziza Matouge, the head of the Cardiac Rehabilitation Unit, for performing the 6 MWD tests.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bunn HF Pathogenesis and treatment of sickle cell disease. N Engl J Med. 1997; 337(11):762–769. doi:10.1056/NEJM199709113371107
2. Platt OS, Brambilla DJ, Rosse WF, et al. Mortality in sickle cell disease. Life expectancy and risk factors for early death. N Engl J Med 1994; 330(23):1639–1644. doi:10.1056/NEJM199406093302303
3. Geiger R, Strasak A, Treml B, et al. Six-minute walk test in children and adolescents. J Pediatr. 2007; 150:
4. Minniti CP, Sable C, Campbell A, et al. Elevated tricuspid regurgitant jet velocity in children and adolescents with sickle cell disease: association with hemolysis and hemoglobin oxygen desaturation. Haematologica. 2009; 94:340–347. doi:10.3324/haematol.13812
5. Hostyn SV, de Carvalho WB, Johnston C, Braga JAP. Evaluation of functional capacity for exercise in children and adolescents with sickle cell disease through the six minute walk test. J PEDIAT BRAZIL2013. (89) 6; 588–594. doi:10.1016/j.jped.2013.04.005
6. Goldberg MA, Brugnara C, Dover GJ, Schapira L, Charache S, Bunn HF Treatment of sickle cell anemia with hydroxyurea and erythropoietin. Engl J Med. 1990; 323(6):366. doi:10.1056/NEJM199008093230602
7. Ballas SK, Dover GJ, Charache S Effect of hydroxyurea on the rheological properties of sickle erythrocytes in vivo. Am J Hematol 1989; 32(2):104–111 doi:10.1002/(ISSN)1096-8652
8. Estepp JH, Smeltzer MP, Kang G, et al. A clinically meaningful fetal hemoglobin threshold for children with sickle cell anemia during hydroxyurea therapy. Am J Hematol. 2017; 92(12): 1333–1339. doi:10.1002/ajh.v92.12
9. Yap LB, Ashrafian H, Mukerjee D, Coghlan JG, Timms PM The natriuretic peptides and their role in disorders of right heart dysfunction and pulmonary hypertension. Clin Biochem.2004; 37(10):847–856. doi:10.1016/j.clinbiochem.2004.06.002
10. Souza R, Jardim C, Julio Cesar Fernandes C, Silveira LM, Rabelo R, Humbert M. NT-pro BNP as a tool to stratify disease severity in pulmonary arterial hypertension. Respir Med 2007; 101(1):69–75. doi:10.1016/j.rmed.2006.04.014
11. Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2016; 29(4):277–314. doi:10.1016/j.echo.2016.01.011
12. De Castro LM, Jonassaint JC, Graham FL, Ashley-Koch A, Telen MJ Pulmonary hypertension associated with sickle cell disease: clinical and laboratory endpoints and disease outcomes. Am J Hematol. 2008; 83:19–25. doi:10.1002/(ISSN)1096-8652
13. Rees DC, Williams TN, Gladwin MT Sickle-cell disease. Lancet. 2010; 376(9757):2018–2031. doi:10.1016/S0140-6736(10)61029-X
14. Galie N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016; 37:67–119.
15. Nishimura RA, Schwartz RS, Tajik AJ, Holmes DR
16. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med 2002; 166:111–117. doi:10.1164/ajrccm.166.1.at1102
17. Sahn DJ, DeMaria A, Kisslo J, Weyman A Recommendations regarding quantitation in M-mode echocardiography: results of a survey of echocardiographic measurements. Circulation. 1978; 58(6):1072–1083. doi:10.1161/01.CIR.58.6.1072
18. Otterstad JE Measuring left ventricular volume and ejection fraction with the biplane Simpson’s method. Heart. 2002; 88(6):559–560. doi:10.1136/heart.88.6.559
19. Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005; 18(12):1440–1463. doi:10.1016/j.echo.2005.10.005
20. Augustine DX, Coates-Bradshaw LD, Willis J, et al. Echocardiographic assessment of pulmonary hypertension: a guideline protocol from the British Society of Echocardiography. Echo Res Pract 2018; 5(3): G11–G24. doi:10.1530/ERP-17-0071
21. Appleton CP, Hatle LK, Popp RL. Superior vena cava and hepatic vein Doppler echocardiography in healthy adults. J Am Coll Cardiol. 1987; 10(5):1032–1039. doi:10.1016/S0735-1097(87)80343-1
22. Braden DS, Covitz W, Milner PF Cardiovascular function during rest and exercise in patients with sickle-cell anemia and coexisting alpha thalassemia-2.Am J Hematol. 1996; 52(2):96–102.
23. Moyssakis I, Tzanetea R, Tsaftaridis P, et al. Systolic and diastolic function in middle aged patients with sickle beta thalassaemia. An echocardiographic study. Postgrad Med J. 2005; 81(961):711–714. doi:10.1136/pgmj.2004.031096
24. Ommen SR, Nishimura RA, Appleton CP, et al. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: a comparative simultaneous Doppler-catheterization study. Circulation. 2000; 102(15):1788–1794. doi:10.1161/01.CIR.102.15.1788
25. Desai AA, Patel AR, Ahmad H, et al. Mechanistic insights and characterization of sickle cell disease associated cardiomyopathy. Cardiovasc Imaging. 2014; 7:430–437. doi:10.1161/CIRCIMAGING.113.001420Circulation
26. Sachdev V, Machado RF, Shizukuda Y, et al. Diastolic dysfunction is an independent risk factor for death in patients with sickle cell disease. J Am Coll Cardiol. 2007;49(4):472–479. doi:10.1016/j.jacc.2006.09.038
27. Gladwin MT Cardiovascular abnormalities in sickle cell disease. J Am Coll Cardiol. 2012;59(13):1123–33. doi: 10.1016/j.jacc.2011.10.900
28. Niss O, Fleck R, Makue F, et al. Association between diffuse myocardial fibrosis and diastolic dysfunction in sickle cell anemia. Blood. 2017; 130(2):205–213. doi:10.1182/blood-2017-02-767624
29. Garadah T, Hassan AB, Al Alawi M, Jaradat A, Sequeira R, Qureshi F Surrogates of poor prognostic signs in adult patients with homozygous sickle cell disease: an echocardiographic study. BJMMR 2014;4(26):4431–4433. doi:10.9734/BJMMR/2014/10047
30. Voskaridou E, Tsetsos G, Tsoutsias A, Spyropoulou E, Christoulas D, Terpos E Pulmonary hypertension in patients with sickle cell/beta thalassemia: incidence and correlation with serum N-terminal pro-brain natriuretic peptide concentrations. Haematologica. 2007; 92(6):738–743. doi:10.3324/haematol.11136
31. Machado RF, Anthi A, Steinberg MH, et al. N-terminal pro-brain natriuretic peptide levels and risk of death in sickle cell disease. JAMA. 2006;296(3):310–318. doi:10.1001/jama.296.3.310
32. Andreassen AK, Wergeland R, Simonsen S, Geiran O, Guevara C, Ueland T N-terminal pro-B-type natriuretic peptide as an indicator of disease severity in a heterogeneous group of patients with chronic precapillary pulmonary hypertension. Am J Cardiol. 2006;98(4):525–529. doi:10.1016/j.amjcard.2006.02.061
33. Waltz X, Romana M, Hardy-Dessources MD, et al. Hematological and hemorheological determinants of the six-minute walk test performance in children with sickle cell anemia. PLoS One. 2013; 8:e77830. doi: 10.1371/journal.pone.0077830
34. Gordeuk VR, Campbell A, Rana S, et al. Relationship of erythropoietin, fetal hemoglobin, and hydroxyurea treatment to tricuspid regurgitation velocity in children with sickle cell disease. Blood. 2009; 114:4639–4644. doi:10.1182/blood-2009-04-218040
35. Estepp JH, Smeltzer MP, Kang G, Aygun B, Ware RE, Nottage K Higher fetal hemoglobin following escalation of hydroxyurea to maximum tolerated dose provides clinical benefit to children with sickle cell anemia. Blood. 2014; 124:8. doi:10.1182/blood.V124.21.85.85
36. Rodgers GP, Steinberg MH Pharmacologic treatment of sickle cell disease and thalassemia: the augmentation of fetal hemoglobin. In: Steinberg MH, Forget BG, Higgs DR, Nagel RL, editors. Disorders of Hemoglobin: Genetics, Pathophysiology, and Clinical Management (
37. Badawy SM, Payne AB, Rodeghier MJ, Liem RI Exercise capacity and clinical outcomes in adults followed in the Cooperative Study of Sickle Cell Disease (CSSCD). Eur J Haematol. 2018; 101(4):532–541. doi:10.1111/ejh.2018.101.issue-4
38. Steinberg MH, Voskaridou E, Kutlar A, et al. Concordant fetal hemoglobin response to hydroxyurea in siblings with sickle cell disease. Am J Hematol. 2003; 72(2):121–126. doi:10.1002/(ISSN)1096-8652
39. Di Liberto G, Marden MC, Boyer L, et al. Dense red blood cell and oxygen desaturation in sickle-cell disease. Am J Hematol. 2016; 91(10):1008–1013. doi:10.1002/ajh.24467
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.