")
Back to Journals » International Journal of Women's Health » Volume 13
The Effects of Fear and Knowledge of COVID-19 on Preventive Practice Among Pregnant Women Who Attend Antenatal Care in Northwest Ethiopia, 2020: Institution-Based Cross-Sectional Study
Authors W/Mariam TGM , Kassie BA , Asratie MH , Abate AT
Received 10 October 2020
Accepted for publication 30 December 2020
Published 14 January 2021 Volume 2021:13 Pages 95—100
DOI https://doi.org/10.2147/IJWH.S286088
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Everett Magann
Tesfamichael G/Mariam W/Mariam,1 Belayneh Ayanaw Kassie,2 Melaku Hunie Asratie,2 Addisu Taye Abate3
1Department of Surgical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Women’s and Family Health, School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Medical Nursing, School of Nursing, College of Medicine and Health Sciences University of Gondar, Gondar, Ethiopia
Correspondence: Tesfamichael G/Mariam W/Mariam
Department of Surgical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, P.O. Box 196, Gondar, Ethiopia
Tel +251918723043
Email [email protected]
Background: The novel coronavirus disease 2019 (COVID-19) pandemic has infected over one million individuals with almost 50,000 deaths worldwide. COVID-19 is currently a global health threat and a public health emergency. Therefore, accurate and up-to-date information regarding prevention and control methods is essential.
Objective: The aim of the study was to assess the effects of fear and knowledge of COVID-19 on preventive practices among pregnant women who attend antenatal care in northwest Ethiopia, 2020.
Methods: An institution-based cross-sectional study was conducted between July and August 2020. The systematic random sampling technique was used to select 422 participants. Data collected by a face to face interview on pretested and structured questions were entered using Epi-Info version 7 and it was analyzed using SPSS version 22 software. The bivariate and multivariable logistic regression model was used to assess factors associated with COVID-19 preventive practices. Adjusted odds ratio (OR) with a 95% confidence interval (CI) was used to determine the association between covariates and the outcome variable. The p-value less than 0.05 was considered statically significant.
Results: According to this study, good preventive practice of COVID-19 among pregnant women was found to be (47.4%). Fear of COVID-19 was (50.9%). The majority (55.0%) of the respondents had good knowledge. Fear [AOR: 2.485, 95% CI: (1.664– 3.711)] and having good knowledge [AOR: 2.308, 95% CI: (1.541– 3.457)] were significantly associated with good prevention practices among the women.
Conclusion and Recommendation: Only half of the pregnant women had good preventive practice. The findings suggest that healthcare bodies should consider these findings to develop strategies for preventive practice against COVID-19.
Keywords: COVID-19, pregnant women, fear, knowledge, northwest Ethiopia
Introduction
The novel coronavirus disease (COVID-19) pandemic has infected over one million individuals with almost 50,000 deaths worldwide as of December 18, 2020.1 COVID-19 disease is a global health threat and public health emergency of international concern.2 Accurate and up-to-date information regarding prevention and control methods is essential.3 Urgent questions that need to be answered timelyinclude whether pregnant women are highly compromised by the policies and strategies for COVID-19 preventive practices, and whether they are highly affected by the fear of acquiring the disease.4 The preventive practices and public health actions such as social distancing, staying at home, and restriction of mobility make people feel lonely and isolated, increasing stress and anxiety.5 In Taiwan, a total of 52.1% of respondents reported moderate-to-severe levels of anxiety.6
For many women, pregnancy by itself increases vulnerability to psychiatric conditions and stress may be aggravated by the fear of COVID-19 and cause serious health problems, like increased blood pressure, which is often the direct cause of maternal mortality in Ethiopia.7,8 Problems, therefore, require great attention for the sake of the wellbeing of both the mother and the neonate.7,9
Pregnancy needs regular appointments and appropriate scans to see what is there. For instance, pregnant women need a minimum of eight contacts with health care providers to reduce perinatal mortality and improve the experience of care.10 But currently, there are difficulties to pursue schedules as usual due to the pandemic. For instance, appointments made online are most challenging in the context of our country Ethiopia, and in some situations, the schedules might be cancelled unless they are emergency cases.11,12
The aforementioned preventive practices of COVID-19 might compromise the quality of maternal health care services given by healthcare providers from diagnosis to counselling as a prescription of medications.13 There are shreds of evidence that show a reduction in the contact rate of a pregnant woman with a health care provider significantly associated with perinatal death.1,14 Another evidence shows that the majority of the complications of pregnancy can be averted due to counselling based on schedules of antenatal care.15 Overall, 41.3% of the visitors had high knowledge. Frequent hand washing (77.3%) and avoidance of shaking hands (53.8%) were the dominant good practices.16
Despite these facts, there are plenty of evidence as every pregnant woman is at risk and their follow-up should not be compromised as to end the course of pregnancy with the health of the mother and the neonate. But, currently, excessive worry/fear of pregnant women of COVID-19 and shift of government’s attention towards preventive practices may lead to increased maternal, neonatal, and child mortality indirectly from the progression of fear to advanced psychological disorders. However, there is limited evidence that shows the current status of fear and knowledge of COVID-19 on the preventive practices of pregnant women.
Therefore, this study aimed to assess fear and knowledge of COVID-19 on the preventive practices of pregnant women attending antenatal care in Gondar town, northwest Ethiopia.
Methods
Study Design, Setting and Period
An institution-based cross-sectional study was conducted to assess the effect of fear and knowledge of COVID-19 on the preventive practices of pregnant women in northwest Ethiopia from July 01 to 30, 2020.
Source of Population: All pregnant women attending antenatal care services in the public health facilities of Gondar town.
Study Population: All pregnant women attending antenatal care services in the public health facilities of Gondar town during the data collection period.
Inclusion Criteria: All pregnant women who were attending antenatal care service in selected public health facilities of Gondar town during the study period were included in the study.
Exclusion Criteria: Pregnant women who were seriously ill and unable to communicate throughout the study period were excluded.
Sample Size Determination and Procedure
The single population proportion formula was used with the assumption of a 95% confidence interval, 5% margin of error, 50% proportion, and as there was no similar study in the area, a 10% non-response rate was taken to determine the final sample size of 422. Finally, participants were proportionally allocated to the six health facilities in the town based on the number of pregnant women who visited each health facility (Maraki clinic= 30, Gabriel clinic= 20, Loza clinic=60, Azezo clinic=40, Poly clinic=80, University of Gondar referral hospital=192) respectively. During the preceding 3 months before data collection. Then, the study participants were selected through a systematic random sampling technique. The K interval/fraction was calculated by K = N/n = where N=total number of pregnant women attending antenatal care per month from a single public health facility in Gondar town and n=the required sample that should be taken per health facility. Then, to start the interview, we used the lottery method from the first pregnant woman attending antenatal care to the value of k antenatal care attendee per a given health facility. Then, the interview started with the selected antenatal care attendee and continued by recruiting every k value of pregnant woman antenatal care attendee and based on their sequence of exit after check-up up to the required 422 participants.
Data Collection Method and Instrument
Data were collected by using pre-tested face-to-face interview questions with a minimum of one-meter distance between interviewers and interviewees. The questions first prepared in English were translated to Amharic, and back to English for consistency. The questions included: socio-demographic characteristics, and fear-related factor (7 questions), knowledge assessment questions (24 questions); and practice assessment (14 questions). Four BSc degree graduates and two MSc holding midwives collected the data and supervised the process, respectively. Both data collectors and supervisors got a one-day training before the actual work about the aim of the study, procedures, necessary precautions, ways of collecting and ensuring the confidentiality of information gained from respondents.16,17
Operational Definitions
Good knowledgeable of COVID-19: Participants who scored the mean (13.93) and above the mean on knowledge questions.
Poor knowledgeable of COVID-19: Participants who scored below the mean (13.93) on knowledge questions.
Have fear towards COVID-19: Participants who scored the mean (23.68) and above on fear questions.
Have no fear towards COVID-19: Participants who scored below the mean (23.68) on fear questions.
Good preventative of COVID-19: Participants who scored the mean (7.69) and above on practice items.
Poor preventative practice towards COVID-19: Participants who scored below the mean (7.69) on practice items.
Statistical Analysis
All the data were checked visually, and then it was coded and entered into Epi Info version 7, and it was finally exported to Statistical Package for Social Sciences (SPSS) version 22 for analysis. Frequencies, percentages, summary statistics like mean and standard deviation were examined to describe the data. Binary logistic regression was run to see the crude significant relations of each independent variable with the total preventive practice score. Then, variables with P-value <0.2 in bi-variable logistic regression were again entered into multivariable logistic regressions. Finally, significant factors were identified based on adjusted odds ratio (AOR) which included a 95% confidence level at P-value <0.05.
Results
Socio-Demographic Characteristics
A total of 422 pregnant women with a response rate of 100% participated in the study. More than half (55.9%) of the respondents were aged 26–35 years with a mean age of (27.56 ± 5.031) years. The majority of the respondents (73.7%) were Orthodox Christians, 9.2% were single, 91.0% were urban residents, 89.8% were from the Amhara, 15.9% and 10.4% of the mother were unable to read and write. Out of those who could read and write, 16.1%, 10.4% and 24.6% had primary, secondary, diploma and above of education, respectively. 11.1% of the participants were housewives, 22.7% government employee, 64.2% daily labourer, and 1.9% market trade vender. Out of the husband occupational status, 39.6%, 8.5%, 29.1%, and 22.7% were government employee, farmers, daily labourer, and market trade vender. The average family income is =<2500ETB accounting 87.0% of the participants (Table 1).
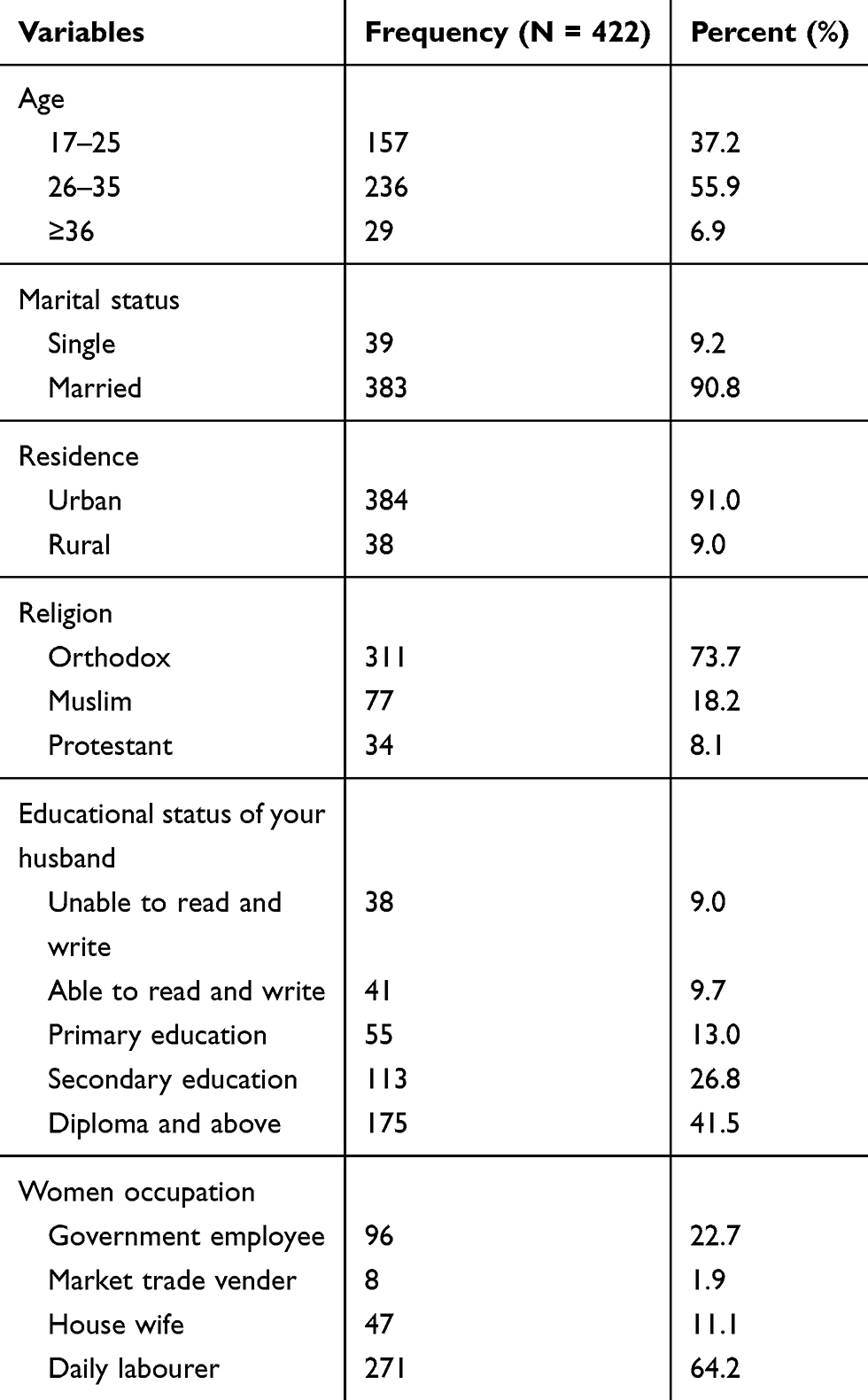 |
Table 1 Socio-Demographic Characteristics of Participants in Gondar Town, Northwest Ethiopia, 2020 (N = 422) |
Obstetric Characteristics of Respondents
Most of the participants, (35.1%) and (32.9%), were Gravida I, II, while only 21.3% and 10% were Gravida III and IV, respectively. In term parity, 37.0% were para zero, 32.5% I, 20.6% II, 8.3% III, and 1.7% >III para. Of the entire participants, 23.0%, 27.7%, 23.7%, and 25.5% had 1st, 2nd, 3rd and ≥4th ANC visits, respectively (Table 2).
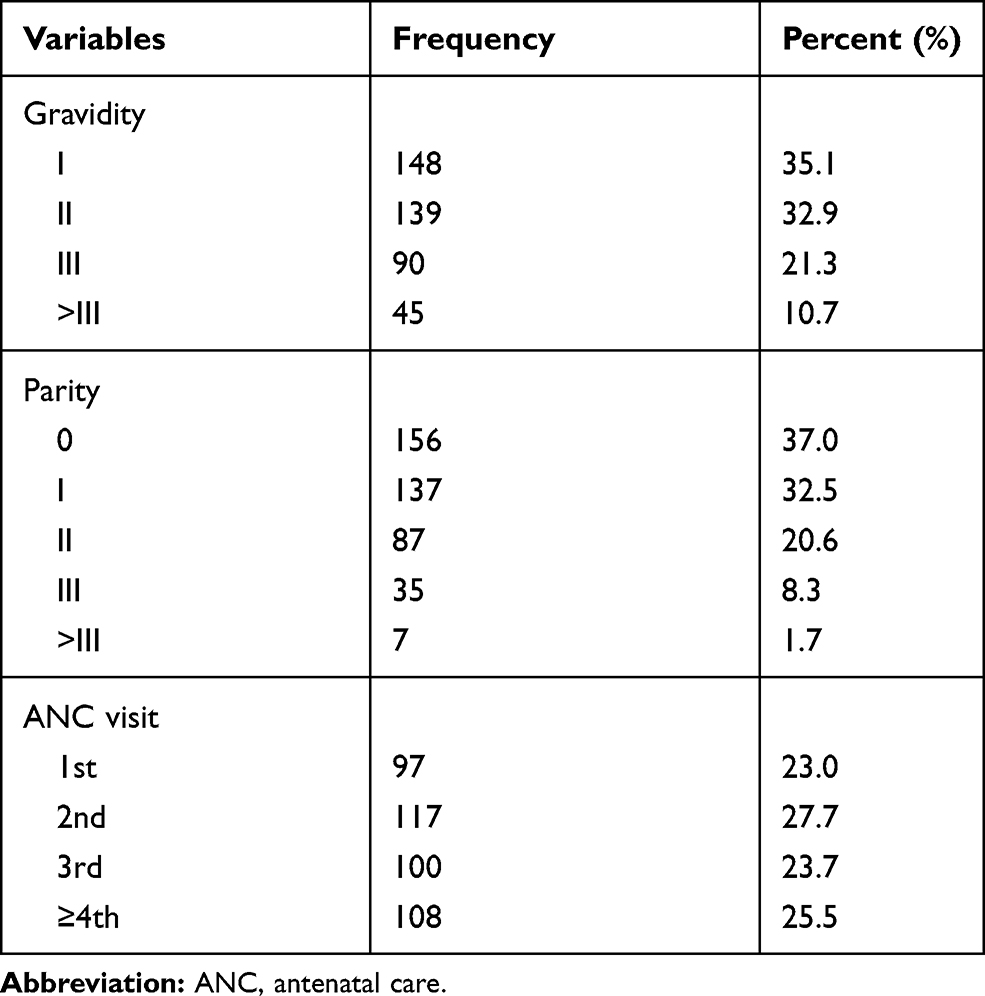 |
Table 2 Obstetric Characteristics of Participants in Gondar Town, Northwest Ethiopia, 2020 (N = 422) |
Fear, Knowledge and Preventive Practice-Related Characteristics of the Respondents
Half (50.9%) of the respondents have fear for the Preventive practices of COVID-19, 55% had good knowledge of the preventive and 47.4% of them have good preventive practice towards COVID-19 (Table 3).
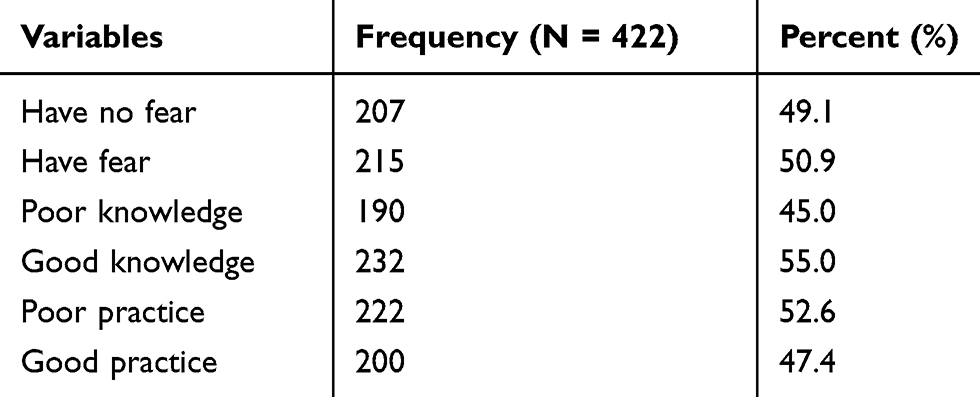 |
Table 3 Fear, Knowledge and Preventive Practice-Related Characteristics of Respondents in Gondar Town, Northwest Ethiopia, 2020 (N = 422) |
Factors Associated with Preventive Practices of COVID-19
Variables that were significantly associated in the bivariate analysis were further examined in multivariate logistic regression of the variables included in the multivariate logistic regression model based on their P value in the bivariate analysis, respondent’s knowledge and fear were significantly associated in the multivariate logistic regression. Those who had good knowledge were 2.3 times [AOR: 2.308, 95% CI: (1.541–3.457)] more likely to have good prevention practice than their counterparts. Respondents who had fear were about 2.5 times [AOR: 2.485, 95% CI: (1.664–3.711)] more likely to have good prevention practices than their counterparts (Table 4).
 |
Table 4 Bivariate and Multivariate Analysis of Factors Associated with Prevention Practice in Gondar Town, Northwest Ethiopia, 2020 (N = 422) |
Discussion
This institution-based cross-sectional study attempted to assess the effects of fear and knowledge of COVID-19 on preventive practice among pregnant women who attend antenatal care in Gondar town, northwest Ethiopia.
In this study, out of the total 422 participants, 47.4% had good preventive practice for COVID-19. This finding goes with a study done in Jimma and.16 It is higher than those of studies done in Thailand (13.6%),3 Iran (16.7%),18 and China who had better preventive practice.19 The preventive practice of COVID-19 in this study is, however, much lower when compared to studies done in Iran & china in which 89% of the participants practiced the prevention of COVID-19.18,19 The underlying reason for these differences could be the period and the place in which the studies were conducted.
The majority of the respondents (55%) had good knowledge of the preventive practices of COVID-19. This finding is in line with a study done on educated Ethiopians in which 52.2% had good knowledge.17 The results of the current study regarding respondents’ knowledge are also lower (26.6%) compared with that of a study done in Thailand.3
The results of this study are also higher compared with a study done in Jimma (41.3%).16 This could be due to differences in the level of information regarding COVID-19.
In the current study, respondent’s knowledge and fear were significantly associated with the preventive practice of COVID-19. Those who have good knowledge were 2.3 times more likely to have good prevention practice of COVID-19 as compared with their counterparts. This finding is consistent with studies done among educated Ethiopians.17
The study also showed that pregnant women who had fear for COVID-19 were about 2.5 times more likely to have good prevention practices than those counterparts. The finding agrees with those of studies done in Iran20 and Taiwan.6 This could be due to people who fear to acquire and transmit the disease could take care of themselves, and better comply with preventive practice recommendations.
Limitation
As in any cross-sectional study, cause and effect relationship was not possible to establish for the factors dealt with in the study. In addition, a shortage of similar studies carried out in Ethiopia has limited the comparison and discussion of results.
Conclusion and Recommendation
Only half of the pregnant women had good preventive practice. The findings suggest that healthcare bodies should consider these findings to develop strategies for preventive practice against COVID-19.
Abbreviations
ANC, Antenatal care; AOR, adjusted odds ratio; CI, confidence interval; COVID-19, novel coronavirus disease 2019; ERC, Ethical Review Committee; ETB, Ethiopian Birr; SPSS, Statistical Package for Social Science; UoG, University of Gondar; WHO, World Health organization.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethical Considerations and Consent to Participate
Ethical clearance was obtained from the Ethical Review Committee (ERC) of the School of Nursing on behalf of the Institutional Review Board of the University of Gondar. All participants were informed about the purpose of the study conducted in accordance with the Declaration of Helsinki. Written consent was obtained from all participants after informing them about the purpose, benefits, risks, the confidentiality of information, and the voluntary nature of participation in the study. The respondents were notified that they had the right to refuse or stop at any point of the data collection. Additionally, informed consent was obtained from a parent on behalf of any participants under the age of 18. Personal identifiers were not included in the written questionnaires to ensure participants’ confidentiality (identities).
Acknowledgments
The authors thank all the staff members of Gondar town health facility for their contribution during data collection and the University of Gondar for giving ethical clearance. The authors would like to thank also the study participants for giving their consent to participate in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No financial support was gained to conduct the study.
Disclosure
The authors declare there is no competing interest.
References
1. Gupta R. Frequency and timing of antenatal care visits and its impact on neonatal mortality in EAG States of India. J Neonatal Biol. 2017;6(03). doi:10.4172/2167-0897.1000257
2. Wang C, Horby PW, Hayden FG, et al. A novel coronavirus outbreak of global health concern. Lancet. 2020;395(10223):470–473. doi:10.1016/S0140-6736(20)30185-9
3. Srichan P, Apidechkul T, Tamornpark R et al. Knowledge, attitude and preparedness to respond to the 2019 novel Coronavirus (COVID-19) among the bordered population of Northern Thailand in the early period of the outbreak. Available SSRN 3546046; 2020
4. Francesco-R, Oiuwatoyin FM, Marcela D et at. Global impact of COVID-19 on service Delivery and Vulnerable Populations Access to Dental care. CDA Journal. 48(10):507–516
5. Roth S, Cohen LJ. Approach, avoidance, and coping with stress. Am Psychol. 1986;41(7):813. doi:10.1037/0003-066X.41.7.813
6. Wong LP, Hung C-C. Anxiety symptoms and preventive measures during the COVID-19 outbreak in Taiwan. BMC Psychiatry. 2020;20:1–19.
7. Woods SM, Melville JL, Guo Y, Fan M-Y, Gavin A. Psychosocial stress during pregnancy. Am J Obstet Gynecol. 2010;202(1):
8. Hobel CJ, Goldstein A, Barrett ES. Psychosocial stress and pregnancy outcome. Clin Obstet Gynecol. 2008;51(2):333–348. doi:10.1097/GRF.0b013e31816f2709
9. Cantwell R, Cox JL. Psychiatric disorders in pregnancy and the puerperium. Curr Obstet Gynaecol. 2006;16(1):14–20. doi:10.1016/j.curobgyn.2005.11.001
10. Organization WH. WHO recommendation on antenatal care contact schedules; 2018
11. Rasmussen SA, Smulian JC, Lednicky JA, Wen TS. Coronavirus disease 2019 (COVID-19) and pregnancy: what obstetricians need to know. Am J Obstet Gynecol. 2020.
12. Mullins E, Evans D, Viner R, O’Brien P, Morris E. Coronavirus in pregnancy and delivery: rapid. Rev Ultrasound Obstet Gynecol. 2020;55(5):586–592. doi:10.1002/uog.22014
13. Liu D, Li L, Wu X, et al. Pregnancy and perinatal outcomes of women with coronavirus disease (COVID-19) pneumonia: a Prelim. Anal Am J Roentgenol. 2020;1–6.
14. Tekelab T, Chojenta C, Smith R, Loxton D. The impact of antenatal care on neonatal mortality in sub-Saharan Africa: a systematic review and meta-analysis. PLoS One. 2019;14(9):e0222566. doi:10.1371/journal.pone.0222566
15. Singh A, Pallikadavath S, Ram F, Alagarajan M. Do antenatal care interventions improve neonatal survival in India? Health Policy Plan. 2014;29(7):842–848. doi:10.1093/heapol/czt066
16. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma university medical center visitors, Southwest Ethiopia. PLoS One. 2020;15(5):e0233744. doi:10.1371/journal.pone.0233744
17. Dagne H, Alemu KA, Dagnew B, et al. Prevention practice and associated factors of Coronavirus disease 2019 (COVID-19) outbreak among educated Ethiopians: an online based cross-sectional survey; 2019
18. Erfani A, Shahriarirad R, Ranjbar K, Mohsen Moghadami AM. Knowledge, attitude and practice toward the novel coronavirus (COVID-19) outbreak: a population-based survey in Iran. Bull World Health Organ. 2020;30.
19. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
20. Yıldırım M, Geçer E, Akgül Ö. The impacts of vulnerability, perceived risk, and fear on preventive behaviours against COVID-19. Psychol Health Med. 2020. doi:10.1080/13548506.2020.1776891
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.