")
Back to Journals » Journal of Asthma and Allergy » Volume 7
The effects of concomitant GERD, dyspepsia, and rhinosinusitis on asthma symptoms and FeNO in asthmatic patients taking controller medications
Authors Ishizuka T , Hisada T, Kamide Y, Aoki H, Seki K, Honjo C, Sakai H, Kadowaki M, Umeda Y, Morikawa M, Anzai M, Ameshima S, Ishizaki T, Dobashi K, Yamada M, Kusano M
Received 30 April 2014
Accepted for publication 30 June 2014
Published 5 September 2014 Volume 2014:7 Pages 131—139
DOI https://doi.org/10.2147/JAA.S67062
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Tamotsu Ishizuka,1,2 Takeshi Hisada,2 Yosuke Kamide,2 Haruka Aoki,2 Kaori Seki,2 Chisato Honjo,1 Hiroyuki Sakai,1 Maiko Kadowaki,1 Yukihiro Umeda,1 Miwa Morikawa,1 Masaki Anzai,1 Shingo Ameshima,1 Takeshi Ishizaki,1 Kunio Dobashi,2 Masanobu Yamada,2 Motoyasu Kusano3
1Third Department of Internal Medicine, Faculty of Medical Sciences, University of Fukui, Fukui, 2Department of Medicine and Molecular Science, Gunma University Graduate School of Medicine, 3Department of Endoscopy and Endoscopic Surgery, Gunma University Hospital, Maebashi, Japan
Background: Losing the sense of smell, which suggests eosinophilic rhinosinusitis, is a subjective symptom, sometimes reported in asthmatic patients taking controller medication. Upper abdominal symptoms, suggesting gastroesophageal reflux disease (GERD) or functional dyspepsia, occur also in these patients. However, the relationship between these symptoms, concomitant with asthma, and the intensity of eosinophilic airway inflammation remains obscure.
Objective: To assess the symptoms of asthma and rhinosinusitis, and to examine the relationship between the symptoms and bronchial inflammation, a new questionnaire, the G scale, was developed. To investigate the effects of GERD, dyspepsia, and rhinosinusitis on asthma symptoms and bronchial inflammation, the symptoms of asthma and rhinosinusitis obtained by the G scale, upper abdominal symptoms obtained by the modified F scale, a questionnaire for GERD and dyspepsia, and fractional exhaled nitric oxide (FeNO) were analyzed.
Methods: A prospective, observational study was performed in four hospitals in Gunma prefecture, and a retrospective analysis was done using data obtained from five hospitals in Gunma prefecture and Fukui prefecture, Japan. A total of 252 patients diagnosed as having asthma participated in the prospective study.
Results: The frequency of daytime phlegm or losing the sense of smell had a positive correlation with FeNO levels in asthmatic patients taking controller medication. Upper abdominal symptoms, as well as symptoms suggesting rhinitis, were well correlated with asthma symptoms. However, neither upper abdominal symptoms nor rhinitis symptoms increased FeNO levels, which reflect eosinophilic airway inflammation during treatment for asthma. On the other hand, the degree of upper abdominal symptoms or dyspepsia symptoms had a weak but significant negative correlation with FeNO levels.
Conclusion: Daytime phlegm and losing the sense of smell suggest that eosinophilic airway inflammation persists, despite anti-inflammatory therapy, in patients with asthma. Although rhinitis and GERD made the subjective symptoms of asthma worse, they did not seem to enhance eosinophilic airway inflammation.
Keywords: asthma symptoms, FeNO, rhinosinusitis, GERD, dyspepsia
Introduction
Pharmacological treatment is the mainstay of management for most patients with asthma. Guideline-based management results in significant improvement in health-related quality of life in most patients.1 Although the goal of therapy is to control asthma by reducing impairment and risk, many patients seem to continue to have some asthma symptoms, such as cough, phlegm, or dyspnea, when asked about their symptoms on a questionnaire.2 Some important complications that occur with asthma, such as rhinitis,3 sinusitis,4,5 and gastroesophageal reflux disease (GERD),6 are known to affect asthma symptoms. These complications may make bronchial inflammation worse, because asthma symptoms are mainly caused by airway inflammation. Whether these complications directly affect the intensity of bronchial inflammation continues to be an unanswered question.
The frequency scale for the symptoms of GERD (F scale) is the standard questionnaire used in Japan for the diagnosis of GERD and assessment of the response to treatment.7 Recently, the F scale was modified by adding two questions on interdigestive and postprandial epigastric pain.8 We imitated the F scale and developed a new questionnaire, the Frequency Scale for the Symptoms of Asthma and Rhinosinusitis Developed in Gunma (G scale), to assess the symptoms of asthma and rhinosinusitis in adult patients with asthma. The relationships between asthma symptoms and the symptoms that come from the complications were investigated using both the modified F scale and the G scale.
Measurement of fractional exhaled nitric oxide (FeNO), a surrogate marker of eosinophilic airway inflammation,9 is slowly becoming part of the routine clinical evaluation of asthmatic patients in Japan. In this study, whether the symptoms of rhinosinusitis or upper abdominal symptoms were related to eosinophilic airway inflammation, and which symptoms in asthmatic patients were related to eosinophilic inflammation during treatment for asthma, were also investigated.
Methods
Study design and patients
A total of 252 patients diagnosed as having asthma by medical specialists (certified by either the Japanese Respiratory Society or the Japanese Allergology Society) participated in this prospective, observational study to investigate the correlations between symptoms and eosinophilic airway inflammation. All patients with asthma were enrolled consecutively, without any selection. After giving their written, informed consent, the patients answered two kinds of questionnaire: the modified F scale and the G scale (Table 1). In developing the G scale, the intention was not to use it for the diagnosis of asthma or rhinosinusitis. The goal was to evaluate chronic rhinosinusitis; but symptoms of acute rhinosinusitis and those of chronic rhinosinusitis cannot be distinguished using the G scale. Complications associated with asthma, such as rhinosinusitis, GERD, or dyspepsia, were not diagnosed by objective findings in all patients in the present study, although some patients were diagnosed, based on the findings of endoscopy or computerized tomography (CT), as part of their routine medical care. FeNO was measured in all participants, using the NIOX MINO® (Aerocrine AB, Solna, Sweden), according to the manufacturer’s instructions.
 | Table 1 The G scale: the frequency scale for the symptoms of asthma and rhinosinusitis developed in Gunma |
Of the 252 patients, 2 were found not to have asthma, by a physician in charge, after they had provided their consent. They were excluded from the analysis. Two patients with asthma, who agreed to participate in this observational study, did not take any medicine for asthma, because their asthmatic symptoms were stable without treatment. These patients were also excluded from the analysis. Therefore, the data obtained from 248 patients who took controller medications for asthma were analyzed in this prospective, observational study. These 248 patients (97 males, 151 females; age range: 16–88 years; mean ± standard deviation (SD): 58.6±16.3 years) received sufficient treatment for asthma. Treatments for rhinorrhea, sneezing, nasal obstruction, olfactory dysfunction, or upper abdominal symptoms were prescribed at the physician’s discretion. Of the 248 patients, 246 had used inhaled corticosteroids (ICS): 92 used low-dose ICS, 106 used medium-dose ICS, and 48 used high-dose ICS. In addition, 50 patients were treated according to Treatment Step 2 of the Global Initiative for Asthma (GINA) guidelines, 47 patients were treated according to Treatment Step 3, 120 were treated according to Treatment Step 4, and 31 were treated according to Treatment Step 5. Long-acting beta-agonists (LABA) were used by 170 patients, leukotriene receptor antagonists were used by 86 patients, sustained release theophylline was used by 44 patients, and oral corticosteroids were used by 31 patients for asthma control. Proton pump inhibitors (PPIs) were used by 61 patients, and 6 patients took histamine H2 blockers. Forty-eight patients took histamine H1 blockers, and 31 patients used nasal corticosteroids.
This prospective, observational study (UMIN 000007762) was approved by the Ethics Committees of Gunma University Faculty of Medical Science (Maebashi, Japan), National Numata Hospital (Numata, Japan), Maebashi Kyoritsu Hospital (Maebashi, Japan), and Heisei Hidaka Clinic (Takasaki, Japan). This study was started on April 10, 2012 and completed on November 30, 2012.
The retrospective analysis for the relationship between the asthma control test (ACT) and the G scale was performed as follows. Both the ACT and the G scale had been used at the same time in the daily medical treatment of outpatients with asthma since October 2012. The data on the ACT and the G scale obtained from 128 patients (42 males, 86 females; age range: 22–88 years; mean ± SD: 60.3±16.9 years) who had been treated by controller medications for asthma from October 2012 to December 2013 (in Gunma University Hospital, Heisei Hidaka Clinic, Maebashi Kyoritsu Hospital, University of Fukui Hospital, and Fukui Sogo Clinic), were analyzed retrospectively. Of these 128 patients, 125 had used ICS (53 patients had used low-dose ICS, 37 had used medium-dose ICS, and 35 had used high-dose ICS). Three other patients were treated by a leukotriene receptor antagonist alone. LABAs were used by 104 patients, leukotriene receptor antagonists by 40 patients, sustained release theophylline by 22 patients, and oral corticosteroids by 24 patients, for asthma control. In addition, 20 patients were treated according to Treatment Step 2 in the GINA guidelines, 31 according to Treatment Step 3, 53 according to Treatment Step 4, and 24 according to Treatment Step 5. PPIs were used by 30 patients, and 1 patient took a histamine H2 blocker. Thirty-one patients took histamine H1 blockers, and nasal corticosteroids were used by 22 patients. When data were repeatedly obtained from the same patient, the latest data were used in the analysis.
Statistical analysis
The data were analyzed using SPSS software (IBM Japan, Tokyo, Japan). FeNO was analyzed as a continuous variable. Answers to the questionnaire were dealt with as discrete variables. The differences between the mean FeNO values of two categorical independent groups were determined using an unpaired t-test (Student’s t-test or Welch’s t-test), after the equality of variances was assessed by Levene’s test. Correlations of two variables were calculated using Spearman’s rank correlation coefficient, because the variables did not show a normal distribution and some of them were discrete. Multiple regression analysis was performed to determine the multiple regression function, and the standardized partial regression coefficients were calculated to compare the strengths of two factors that affected a third factor.
Results
The relationship between the asthma symptoms score in the G scale and ACT sum score
The data on the ACT and the G scale obtained from 128 asthmatic patients who received controller medication continuously were analyzed. The asthma symptoms score was calculated as the sum of the first eight questions on asthma symptoms of the G scale. The ACT sum score was calculated as the sum of five questions. The asthma symptoms score was strongly but negatively correlated with the ACT sum score (Figure 1A). ACT sum scores of ≥20 and ≤19 are useful for identifying patients with controlled and uncontrolled asthma, respectively. When an ACT cut-off point of 19 was established to screen for uncontrolled asthma, a cut-off point of 6 for the asthma symptoms score was suitable for identifying uncontrolled asthma. The sensitivity and specificity for identifying uncontrolled asthma using this cut-off value were 89.3% and 84.0%, respectively (Figure 1B). Asthma was considered uncontrolled in 41 (32%) of the 128 patients because their asthma symptoms scores were 6 or greater.
 | Figure 1 The relationship between asthma symptoms scores calculated by the G scale and ACT sum score. |
G scale score in asthmatic patients continuously treated by controller medications
The data on the G scale obtained from the 248 patients with asthma who participated were analyzed. The percentages of respondents who answered sometimes, often, or always for each question of the G scale were 28% (G1), 27% (G2), 25% (G3), 28% (G4), 15% (G5), 15% (G6), 13% (G7), 16% (G8), 31% (G9), 31% (G10), 29% (G11), and 25% (G12). The frequencies of cough and phlegm were higher than those of wheeze and difficulty breathing. G3 and G4 did not refer to the features of phlegm, although it was important to explore the cause of phlegm. The frequencies of symptoms of rhinosinusitis (G9–G12) were relatively higher than those of symptoms of asthma (G1–G8). The question to which patients most often answered “always” (14%) was the question on losing the sense of smell (G12).
A diagnosis of allergic rhinitis or sinusitis cannot be made using the G scale. Although post nasal drip was also one of the important findings in patients with sinusitis, there was no question that referred directly to post nasal drip, because the G scale consisted of patients’ subjective symptoms.
The relationship between FeNO and symptoms
The correlation between the frequency of each symptom and FeNO was investigated. The frequency of daytime phlegm was significantly correlated with FeNO (Figure 2A). FeNO was significantly higher in patients who answered “occasionally”, “sometimes”, “often”, or “always” for G3, the question on daytime phlegm (47.0±36.6 parts per billion [ppb], n=104), than in patients who answered “never” (38.1±31.3 ppb, n=144) (Figure 2B). The frequency of losing the sense of smell was also significantly correlated with FeNO (Figure 2C). FeNO was significantly higher in patients who answered “occasionally”, “sometimes”, “often”, or “always” for G12, the question on losing the sense of smell (50.8±40.1 ppb, n=84), than in patients who answered “never” (37.3±29.2 ppb, n=164) (Figure 2D). Although the frequency of losing the sense of smell was well correlated with FeNO, the frequencies of runny nose, sneezing, and nasal congestion were not (data not shown). In contrast, the scores for runny nose, sneezing, or nasal congestion, but not that for losing the sense of smell, were significantly correlated with the asthma symptoms score (Figure 3A–D).
 | Figure 2 The relationship between FeNO and symptoms evaluated by the G scale. |
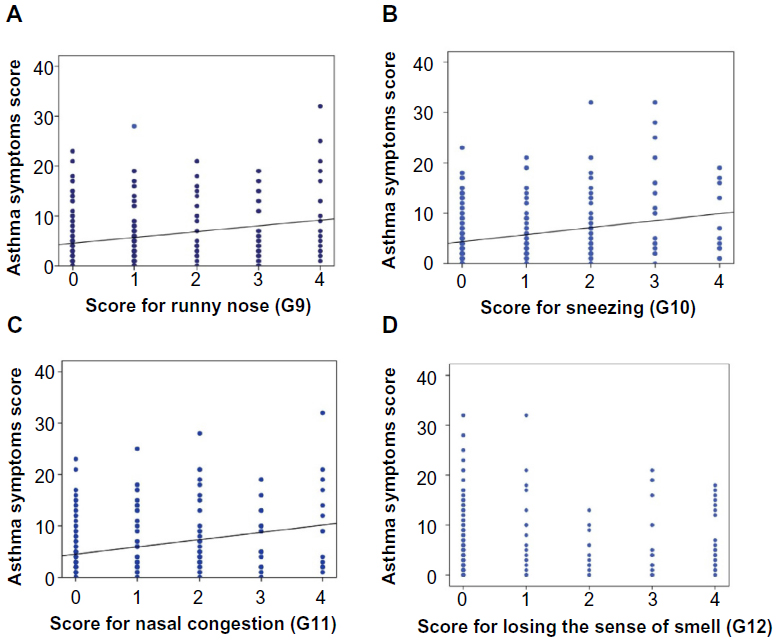 | Figure 3 The relationship between asthma symptoms and rhinosinusitis symptoms. |
The relationships between upper abdominal symptoms, GERD symptoms, dyspepsia symptoms, and asthma symptoms
The sum scores for upper abdominal symptoms (upper abdominal score), GERD symptoms (GERD score), and dyspepsia symptoms (dyspepsia score) were calculated using the modified F scale.8 Specifically, the upper abdominal score was calculated as the sum of 14 questions of the modified F scale. The GERD score or dyspepsia score was calculated as the sum of seven questions, each on GERD symptoms or dyspepsia symptoms. The upper abdominal score, GERD score, and dyspepsia score were well correlated with the asthma symptoms score (Figure 4A–C). Although symptoms of both GERD and dyspepsia seemed to affect asthma symptoms, GERD symptoms had a greater contribution to asthma symptoms than dyspepsia symptoms. The multiple regression function was as follows:

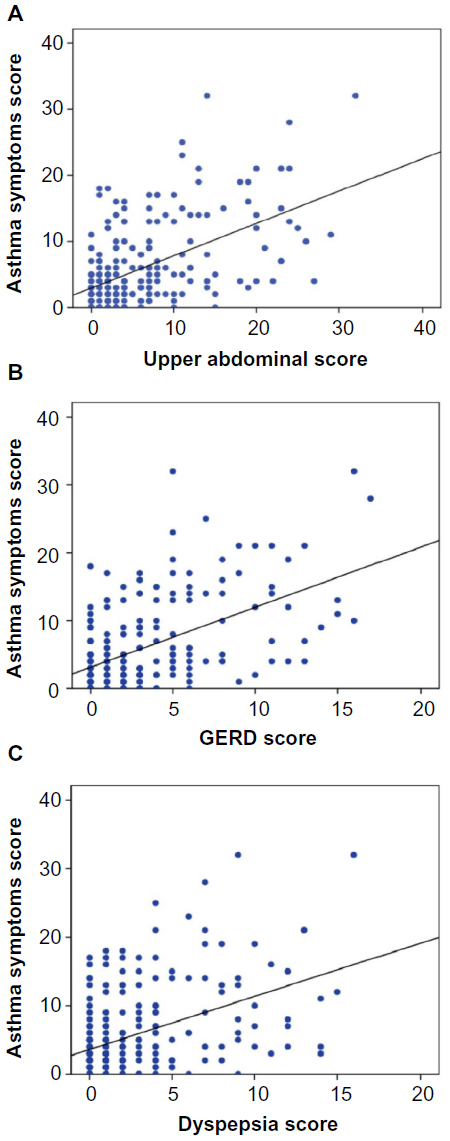 | Figure 4 The relationship between upper abdominal symptoms and asthma symptoms. |
The standardized partial regression coefficients were 0.419 for GERD symptoms and 0.148 for dyspepsia symptoms.
The relationships between upper abdominal symptoms, GERD symptoms, dyspepsia symptoms, and FeNO
The upper abdominal score and the dyspepsia score were negatively correlated with FeNO (Figure 5A and C). The GERD score also tended to be negatively correlated with FeNO, though this correlation was not significant (P=0.097) (Figure 5B).
 | Figure 5 The relationship between upper abdominal symptoms and FeNO. |
Discussion
Asthma control is assessed by daytime symptoms, limitation of activities, nocturnal symptoms/awakening, need for reliever/rescue treatment, and lung function. Several composite control measures, such as ACT10 and the Asthma Control Questionnaire,11 have been developed and are being validated. We have developed a new questionnaire, the G scale, to evaluate the symptoms of rhinosinusitis, as well as the symptoms of asthma, in asthmatic patients. Unexpectedly, asthma symptoms were not well controlled in about one-third of patients, despite taking controller medications. This result suggests that asthma symptoms might be underestimated by doctors in patients treated continuously. Evaluation of asthma control and rhinosinusitis symptoms using the G scale was considered not always superior to a combination of ACT with the SACRA questionnaire, which was designed to reflect asthma control and the condition of allergic rhinitis. However, the G scale might be convenient for screening the concomitant sinusitis, because it contains a question on olfactory dysfunction, which suggests the presence of sinusitis. Certainly, imaging with CT or magnetic resonance imaging (MRI) is much more useful for an accurate and objective diagnosis of sinusitis.
It is known that the prevalence of allergic rhinitis as a complication of asthma is 67.3%, and the percentage of patients whose asthma is well controlled is lower in those with allergic rhinitis than those without allergic rhinitis, suggesting that allergic rhinitis may negatively affect asthma control or asthma symptoms.3 The results of the present study, based on patients’ reports of symptom frequencies, support this theory, because the symptoms of rhinitis, such as runny nose, sneezing, and nasal congestion were well correlated with asthma symptoms, such as cough, phlegm, wheeze, and difficulty breathing.
The presence of sinusitis, as well as rhinitis, in adult asthmatic patients is a very serious problem, because rhinosinusitis, in many cases of adult asthma, is expected to be eosinophilic chronic rhinosinusitis, which is characterized by bilateral nasal polyps, ethmoidal antrum-dominant lesions, and losing the sense of smell.12 This type of rhinosinusitis, which occurs mainly in adults, is resistant to macrolide therapy, and is sometimes accompanied by sinus and peripheral blood eosinophilia.13,14 According to the retrospective data on FeNO measured in Gunma University Hospital, by the American Thoracic Society/European Respiratory Society-recommended online method, FeNO levels in 12 patients, who complained of olfactory dysfunction and who showed abnormal shadows in bilateral ethmoid sinuses on CT or MRI, were higher than those of asthmatic patients who had not complained of olfactory dysfunction, although both groups had been treated by controller medications for asthma (74.5±35.4 ppb versus 37.3±24.9 ppb; n=12 versus n=58). This observation motivated us to develop the G scale containing the question on olfactory dysfunction. As expected, FeNO was significantly more elevated in asthmatic patients with olfactory dysfunction than in other asthmatic patients, even if their asthma had been treated adequately by standard therapy. Because the diagnosis of rhinosinusitis was not made by CT, MRI imaging, or rhinoscopy in the present study, one can only conclude that olfactory dysfunction, as one of the subjective symptoms, was related to FeNO levels. Although olfactory dysfunction is a representative symptom of eosinophilic sinusitis or nasal polyps, this symptom is not specific for eosinophilic sinusitis or nasal polyps.
Among the symptoms of asthma, the frequency of daytime sputum was correlated with FeNO. Interleukin 13, a pleiotropic Th2 cytokine that has been shown to be central to the pathogenesis of asthma, induces goblet cell hyperplasia and increased mucus secretion.15 It also induces nitric oxide synthase in bronchial epithelium,16 resulting in increased breath NO levels. Although increased airway secretion is not a specific phenomenon for Th2-dominant or eosinophilic inflammation, persistent hypersecretion resistant to pharmacotherapy in asthmatic patients may be a key sign that suggests intense eosinophilic inflammation remaining in the lower airways.
Epidemiologic evidence suggests that 30%–90% of asthmatic patients have GERD,17,18 and respiratory symptoms associated with asthma are increased among patients with GERD.19 It is suggested that esophageal acid may produce bronchoconstriction and, therefore, exacerbate airflow obstruction in asthmatic patients.20–22 However, the impact of GERD therapy on objective outcome measures of asthma control has been variable.23–26 In patients with no evidence of organic disease, the modified F scale was useful to distinguish functional dyspepsia from nonerosive reflux disease, and to assess dyspeptic symptoms.8 Dyspepsia is defined as one or more of the following symptoms: postprandial fullness, early satiation, and epigastric pain or burning.27 Up to 75% of patients have functional dyspepsia with no underlying cause on diagnostic evaluation.28–30 Upper abdominal symptoms, including both GERD and dyspepsia, were well correlated with the degree of asthma symptoms, without enhancing the intensity of eosinophilic inflammation. On the other hand, the coexistence of upper abdominal symptoms, especially dyspepsia, may suggest decreased eosinophilic inflammation. The presence of GERD contributes more to respiratory symptoms associated with asthma than does dyspepsia, although the coexistence of GERD itself never makes eosinophilic inflammation worse.
In this study, the goal was to investigate only whether upper abdominal symptoms or rhinosinusitis symptoms affect eosinophilic inflammation of the lower respiratory tract in asthmatic patients sufficiently treated by standard asthma therapy. The present results do not necessarily suggest that some factors of the G scale, which do not affect FeNO levels, do not reflect airway inflammation of asthma. The possibility that some factors of the G scale or modified F scale may affect airway inflammation, especially noneosinophilic inflammation, under sufficient treatment for asthma, was not ruled out.
Conclusion
The presence of rhinitis and GERD may affect asthma control independent of eosinophilic inflammation, and loss of smell or persistent daytime sputum may suggest persistent eosinophilic inflammation in asthmatic patients taking guideline-recommended therapy.
Acknowledgments
The authors would like to thank Dr Yasuhiko Koga, Dr Akihiro Ono, and Prof Masatomo Mori of Gunma University Graduate School of Medicine for their helpful discussion of this research.
Disclosure
The authors have no conflicts of interest to disclose.
References
Bateman ED, Bousquet J, Keech ML, Busse WW, Clark TJ, Pedersen SE. The correlation between asthma control and health status: the GOAL study. Eur Respir J. 2007;29(1):56–62. | |
Hasegawa T, Koya T, Sakagami T, et al. Asthma control and management changes in Japan: questionnaire survey. Intern Med. 2012;51(6):567–574. | |
Ohta K, Bousquet PJ, Aizawa H, et al. Prevalence and impact of rhinitis in asthma. SACRA, a cross-sectional nation-wide study in Japan. Allergy. 2011;66(10):1287–1295. | |
Nakamura H, Kawasaki M, Higuchi Y, Takahashi S. Effects of sinus surgery on asthma in aspirin triad patients. Acta Otolaryngol. 1999;119(5):592–598. | |
Senior BA, Kennedy DW. Management of sinusitis in the asthmatic patient. Ann Allergy Asthma Immunol. 1996;77(1):6–15; quiz 15–19. | |
Cheung TK, Lam B, Lam KF, et al. Gastroesophageal reflux disease is associated with poor asthma control, quality of life, and psychological status in Chinese asthma patients. Chest. 2009;135(5):1181–1185. | |
Kusano M, Shimoyama Y, Sugimoto S, et al. Development and evaluation of FSSG: frequency scale for the symptoms of GERD. J Gastroenterol. 2004;39(9):888–891. | |
Kusano M, Hosaka H, Kawada A, et al. Development and evaluation of a modified Frequency Scale for the Symptoms of Gastroesophageal Reflux Disease to distinguish functional dyspepsia from non-erosive reflux disease. J Gastroenterol Hepatol. 2012;27(7):1187–1191. | |
Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602–615. | |
Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113(1):59–65. | |
Juniper EF, O’Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and validation of a questionnaire to measure asthma control. Eur Respir J. 1999;14(4):902–907. | |
Sakuma Y, Ishitoya J, Komatsu M, et al. New clinical diagnostic criteria for eosinophilic chronic rhinosinusitis. Auris Nasus Larynx. 2011;38(5):583–588. | |
Ishitoya J, Sakuma Y, Tsukuda M. Eosinophilic chronic rhinosinusitis in Japan. Allergol Int. 2010;59(3):239–245. | |
Takeno S, Hirakawa K, Ishino T. Pathological mechanisms and clinical features of eosinophilic chronic rhinosinusitis in the Japanese population. Allergol Int. 2010;59(3):247–256. | |
Kondo M, Tamaoki J, Takeyama K, et al. Elimination of IL-13 reverses established goblet cell metaplasia into ciliated epithelia in airway epithelial cell culture. Allergol Int. 2006;55(3):329–336. | |
Chibana K, Trudeau JB, Mustovich AT, et al. IL-13 induced increases in nitrite levels are primarily driven by increases in inducible nitric oxide synthase as compared with effects on arginases in human primary bronchial epithelial cells. Clin Exp Allergy. 2008;38(6):936–946. | |
Sontag SJ, O’Connell S, Khandelwal S, et al. Most asthmatics have gastroesophageal reflux with or without bronchodilator therapy. Gastroenterology. 1990;99(3):613–620. | |
Harding SM, Richter JE, Guzzo MR, Schan CA, Alexander RW, Bradley LA. Asthma and gastroesophageal reflux: acid suppressive therapy improves asthma outcome. Am J Med. 1996;100(4):395–405. | |
Nordenstedt H, Nilsson M, Johansson S, et al. The relation between gastroesophageal reflux and respiratory symptoms in a population-based study: the Nord-Trøndelag health survey. Chest. 2006;129(4):1051–1056. | |
Jack CI, Calverley PM, Donnelly RJ, et al. Simultaneous tracheal and esophageal pH measurements in asthmatic patients with gastroesophageal reflux. Thorax. 1995;50(2):201–204. | |
Mansfield LE, Hameister HH, Spaulding HS, Smith NJ, Glab N. The role of the vague nerve in airway narrowing caused by intraesophageal hydrochloric acid provocation and esophageal distention. Ann Allergy. 1981;47(6):431–434. | |
Vincent D, Cohen-Jonathan AM, Leport J, et al. Gastro-oesophageal reflux prevalence and relationship with bronchial reactivity in asthma. Eur Respir J. 1997;10(10):2255–2259. | |
Littner MR, Leung FW, Ballard ED 2nd, et al. Effects of 24 weeks of lansoprazole therapy on asthma symptoms, exacerbations, quality of life, and pulmonary function in adult asthmatic patients with acid reflux symptoms. Chest. 2005;128(3):1128–1135. | |
Kiljander TO, Harding SM, Field SK, et al. Effects of esomeprazole 40 mg twice daily on asthma: a randomized placebo-controlled trial. Am J Respir Crit Care Med. 2006;173(10):1091–1097. | |
Kiljander TO, Junghard O, Beckman O, Lind T. Effect of esomeprazole 40 mg once or twice daily on asthma: a randomized, placebo-controlled study. Am J Respir Crit Care Med. 2010;181(10):1042–1048. | |
Mastronarde JG, Anthonisen NR, Castro M, et al. Efficacy of esomeprazole for treatment of poorly controlled asthma. N Engl J Med. 2009;360(15):1487–1499. | |
Tack J, Talley NJ, Camilleri M, et al. Functional gastroduodenal disorders. Gastroenterology. 2006;130(5):1466–1479. | |
Bytzer P, Talley NJ. Dyspepsia. Ann Intern Med. 2001;134(9 Pt 2):815–822. | |
Koch KL, Stern RM. Functional disorders of the stomach. Semin Gastrointest Dis. 1996;7(4):185–195. | |
Malagelada JR. Functional dyspepsia. Insights on mechanisms and management strategies. Gastroenterol Clin North Am. 1996;25(1):103–112. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.