")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
The Effects of 24-Week, High-Concentration Hydrogen-Rich Water on Body Composition, Blood Lipid Profiles and Inflammation Biomarkers in Men and Women with Metabolic Syndrome: A Randomized Controlled Trial
Authors LeBaron TW , Singh RB, Fatima G, Kartikey K, Sharma JP, Ostojic SM, Gvozdjakova A, Kura B, Noda M , Mojto V, Niaz MA , Slezak J
Received 26 November 2019
Accepted for publication 3 March 2020
Published 24 March 2020 Volume 2020:13 Pages 889—896
DOI https://doi.org/10.2147/DMSO.S240122
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Tyler W LeBaron,1,2 Ram B Singh,3 Ghizal Fatima,4 Kumar Kartikey,3 Jagdish P Sharma,3 Sergej M Ostojic,5,6 Anna Gvozdjakova,7 Branislav Kura,2 Mami Noda,8 Viliam Mojto,9 Mohammad Arif Niaz,10 Jan Slezak1
1Centre of Experimental Medicine, Institute for Heart Research, Slovak Academy of Sciences, Bratislava, Slovak Republic; 2Molecular Hydrogen Institute, Enoch, UT, USA; 3Hospital and Research Institute, Moradabad, India; 4Era Medical College, Lucknow, India; 5Applied Bioenergetics Lab, Faculty of Sport and PE, University of Novi Sad, Novi Sad, Serbia; 6Faculty of Health Sciences, University of Pécs, Pécs, Hungary; 7Medical Faculty, Pharmacobiochemical Laboratory of 3rd Medical Department, Comenius University Bratislava, Bratislava, Slovakia; 8Laboratory of Pathophysiology, Graduate School of Pharmaceutical Sciences, Kyushu University, Fukuoka, Japan; 9Third Internal Clinic, Faculty of Medicine, Comenius University, Bratislava, Slovakia; 10Center of Nutrition Research, International College of Nutrition, Moradabad, India
Correspondence: Jan Slezak
Centre of Experimental Medicine, Institute for Heart Research, Slovak Academy of Sciences, Dúbravská Cesta 9, Bratislava 841 04, Slovak Republic
Tel +421 903 620 181
Email [email protected]
Purpose: Metabolic syndrome is associated with several medical risk factors including dyslipidemia, hyperglycemia, and obesity, which has become a worldwide pandemic. The sequelae of this condition increase the risk of cardiovascular and neurological disease and increased mortality. Its pathophysiology is associated with redox dysregulation, excessive inflammation, and perturbation of cellular homeostasis. Molecular hydrogen (H2) may attenuate oxidative stress, improve cellular function, and reduce chronic inflammation. Pre-clinical and clinical studies have shown promising effects of H2-rich water (HRW) on specific features of metabolic syndrome, yet the effects of long-term, high-concentration HRW in this prevalent condition remain poorly addressed.
Methods: We conducted a randomized, double-blinded, placebo-controlled trial in 60 subjects (30 men and 30 women) with metabolic syndrome. An initial observation period of one week was used to acquire baseline clinical data followed by randomization to either placebo or high-concentration HRW (> 5.5 millimoles of H2 per day) for 24 weeks.
Results: Supplementation with high-concentration HRW significantly reduced blood cholesterol and glucose levels, attenuated serum hemoglobin A1c, and improved biomarkers of inflammation and redox homeostasis as compared to placebo (P < 0.05). Furthermore, H2 tended to promote a mild reduction in body mass index and waist-to-hip ratio.
Conclusion: Our results give further credence that high-concentration HRW might have promising effects as a therapeutic modality for attenuating risk factors of metabolic syndrome.
Keywords: metabolism, fasting blood glucose, cholesterol, inflammation, oxidative stress, hydrogen water
Introduction
The prevalence of metabolic syndrome is considered a growing epidemic in countries worldwide, and is characterized by various medical conditions including visceral obesity, hyperglycemia, insulin resistance, hypertension, and dyslipidemia.1 The sequelae of this condition increase the risk of cardiovascular and neurological disease and increased mortality. Its pathophysiology is associated with redox dysregulation, excessive inflammation, and perturbation of cellular homeostasis.2 There is no approved drug to prevent or treat metabolic syndrome. Modifications to diet and lifestyle including caloric restriction and exercise are currently recommended and if implemented can be effective.3 However, stresses of daily life, lack of time, and sufficient motivation are often cited as reasons that prevent people from making sufficient modifications until after they develop symptoms. Nevertheless, even after symptoms emerge, many still do not make the needed changes, and, as a corollary, develop the associated diseases that otherwise could have been prevented.4
Molecular hydrogen (H2 gas) has been demonstrated to attenuate oxidative stress, improve cellular function, and reduce chronic inflammation,5 many of which are associated with the pathology and etiology of metabolic syndrome and its associated diseases.1 Molecular hydrogen modulates signal transduction, protein phosphorylation cascades, gene expression, autophagy, miRNA expression, as well as has important metabolic effects.5,6 H2 can induce the Keap1/Nrf2 signaling pathway,7 promote mitochondrial biogenesis,8 and the cytoprotective mitochondrial unfolded protein response.9 H2 has been proposed to act as an exercise mimetic and redox adaptogen via activating hormetic pathways.10
Inhalation of H2 gas suppressed brain damage induced by middle-cerebral artery occlusion in rats,11 and improved cognitive scores and reduced brain injury in patients with acute cerebral infarction.12 Additionally, H2 gas dissolved in water to make H2-rich water (HRW) has also been shown to have therapeutic and ergogenic effects in pre-clinical and clinical studies10,13 such as, mild cognitive impairments,14 metabolic syndrome,15 and submaximal exercises.10,16,17 Furthermore, as has been reviewed recently,5 molecular hydrogen may be a novel approach for the treatment of cardiovascular diseases. For example, as illustrated in the recent review,5 H2 attenuates radiation-induced heart disease and myocardial ischemia-reperfusion injury in rats by decreasing inflammation, apoptosis, sarcoplasmic and oxidative stress, and by regulating microRNAs and autophagy.5 In APOE knockout mice, ingestion of HRW prevented the development of atherosclerosis,18 and H2 also protected against drug-induced cardiac hypertrophy and dysfunction.19
However, most studies with HRW have been conducted using relatively low concentrations of H2.20 For example, an early study in a mouse model of Parkinson’s disease21 suggested that a low H2 concentration (≈40 μM) may be as effective as a higher H2 concentration (≈800 μM). However, even this higher H2 concentration was not high enough to result in detectable increases in brain H2 concentration.22 It was subsequently determined that H2-induced secretion of neuroprotective gastric ghrelin, which, as a 2nd messenger, mediated the neuroprotective effects of HRW.22 However, the mechanism appears more complicated since the protective effects of HRW were still observed in a ghrelin-KO mice model of Parkinson’s disease.23 Nevertheless, it appears that a higher concentration of H2 is at least as effective as, and often more effective than, a lower H2 concentration. For example, it has been demonstrated that high-concentration hydrogen produced via magnesium was more effective than low-concentration H2 contained in alkaline ionized water in attenuating non-alcoholic fatty liver disease (NAFLD) in mice fed a high-fat diet.24 Similarly, in a randomized controlled pilot study in patients with NAFLD, we found that high-concentration HRW significantly decreased liver fat as measured by dual-echo magnetic resonance imaging.25 In addition, supplementation with high-concentration HRW in middle-aged overweight women significantly reduced body fat percentage and decreased fasting insulin levels.26 In addition to the H2 concentration being important, the duration of use is also an important consideration. Although HRW has been studied in subjects with potential metabolic syndrome for up to 10 weeks, no study has determined the effect long-term (24-week), high-concentration HRW in this population. Despite hydrogen’s ability to ostensibly induce hormesis, and therefore potentially elicit adverse effects, there are no studies either in cells, animals, or humans, even at very high doses, where clear adverse effects have been reported.10 We therefore evaluated the effects of 24-week intervention with high-concentration HRW on body composition, blood lipid profiles and inflammation biomarkers in men and women with metabolic syndrome.
Methods and Subjects
Sixty subjects of Indian ethnicity (30 men and 30 women; age 43.2 ± 10.0 years) with metabolic syndrome were recruited to participate in this double-blinded, placebo-controlled interventional trial. Subjects participated in this study if they met at least three of the five inclusion criteria including prehypertension/hypertension (systolic blood pressure [BP] > 130 mmHg and/or diastolic BP > 85 mmHg), prediabetes/diabetes (fasting glucose > 110 mg/dL), central obesity (waist circumference [WC] > 90 cm for men, and WC > 80 cm for women), and dyslipidemia (high-density lipoprotein [HDL] < 40 mg/dL for men and < 50 mg/dL for women; triglycerides [TG] > 200 mg/dL). Exclusion criteria included cancer, chronic dysentery, human immunodeficiency virus infection, stroke, myocardial infarction, pregnancy or use of contraceptives, and other chronic diseases. The study was conducted in Moradabad India, and all participants were recruited by pamphlet distribution, local newspapers, and announcements on hospital notice boards. Ethical clearance was obtained from the Hallberg Hospital and Research Institute ethic committee (Moradabad), with the trial registered within the Drug Controller of India (Clinical Trial Registration #2018/03/012487). Written informed consent was obtained from all participants, and the trial was conducted in accordance with the Declaration of Helsinki, and this statement was added to the methods.
An initial observation period of one week was used to acquire baseline clinical metrics and biochemical data (Table 1), with no differences found between the HRW and the placebo group. Subjects were then randomized in a double-blind fashion to either intervention (HRW) or placebo group by computer-generated random numbers. All subjects were asked to maintain the same lifestyle throughout the study. Moreover, data on food, tobacco, and alcohol intake and physical activity were obtained by dietary diaries and assessed by a dietitian. The data was collected again after 24 weeks of the intervention. High-concentration HRW was prepared via hydrogen-producing tablets (HRW Natural Health Products Inc., New Westminster BC, Canada) while the placebo was prepared as described previously16,25 with the final placebo drink similar in taste, dissolution, and appearance to HRW. The participants consumed 1 tablet 3 x daily in 250 mL of 12-18°C water. They were advised to drink the product in one gulp as soon as the tablet finished dissolving on an empty stomach/morning. This method of H2 administration would provide >5.5 millimoles H2/day. The concentration of molecular hydrogen produced via these tablets was determined by H2 Analytics (Las Vegas, USA) via gas chromatography (SRI 8610C; California USA).
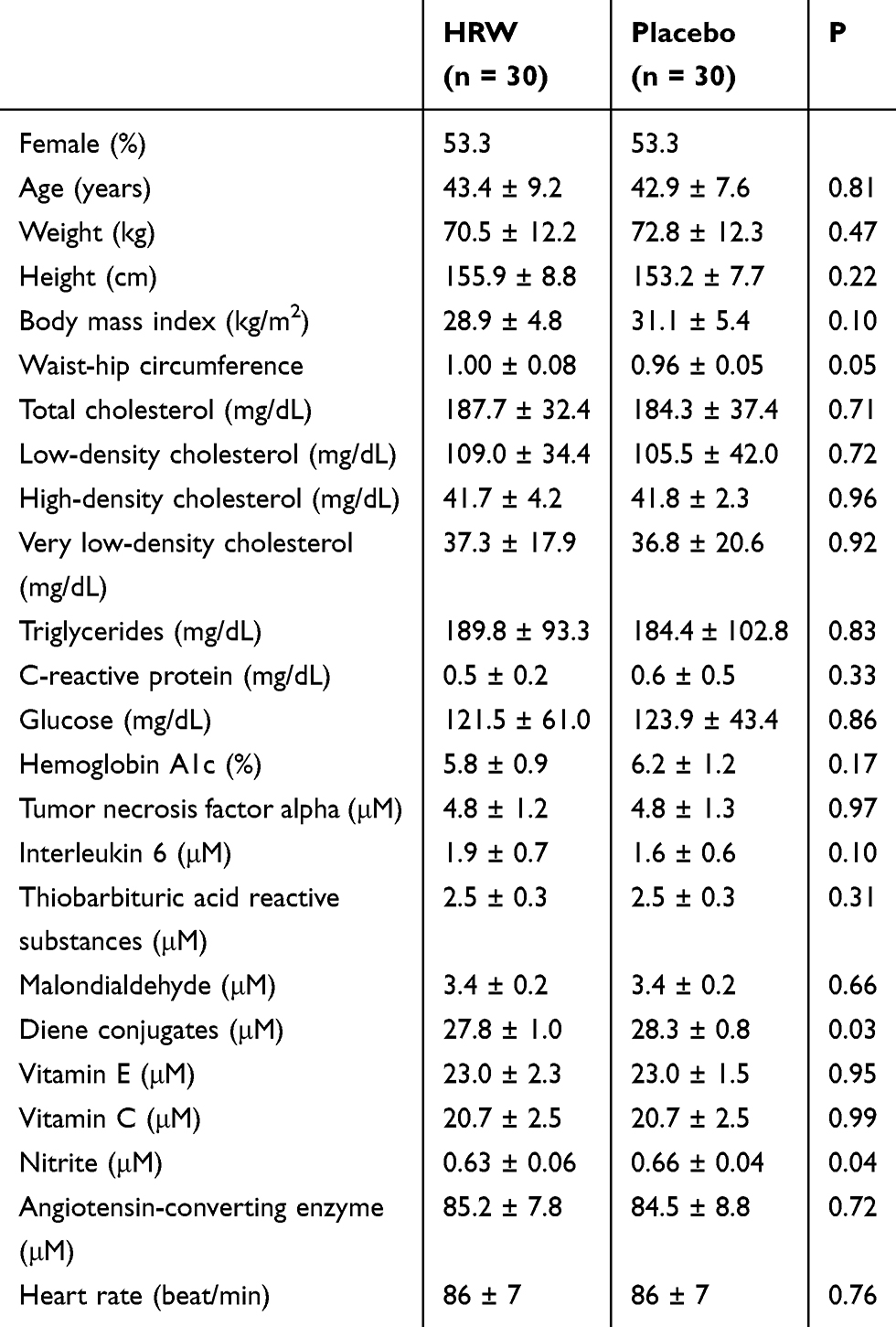 |
Table 1 Baseline Characteristics of the Study Participants of Indian Ethnicity. Values are Mean ± SD |
The laboratory data were obtained following an overnight fast (10–12 hrs) at 08:00 to 09:00 am. Height was measured using a measuring stand after removing shoes. Body weight was measured in underclothes after removing shoes. Waist circumference was measured with anthropometric tape as the largest horizontal circumference between iliac crest and costal margin. The hip girth was measured at the greatest circumference at the level of greater trochanters. Heart rate was measured by auscultation for 5 mins at rest at the supine position. Fasting blood glucose was measured after an overnight fast. Thiobarbituric acid reactive substances (TBARS), malondialdehyde (MDA), diene conjugate, vitamin E and C, nitrate, and angiotensin-converting enzyme were measured by colorimetric methods using a UV–VIS Spectrophotometer (Electronics Corporation of India, Ltd). Glycosylated hemoglobin (HbA1c) was assayed by HPLC using DIO machine (Bio-Rad Laboratories, Inc, Hercules, CA). Fasting blood sugar, lipid profiles, and C-reactive protein (CRP) were determined by Pictus 500 Diatron kits (Medicon Hellas S.A., Gerakas, Greece). Tumor necrosis factor-alpha (TNF-α) and interleukin 6 (IL-6) were analyzed with an enzyme-linked fluorescent assay on Vidas machines (Vidas Biomerieux, Marcy I’Étoile, France). The inter-and intra assay coefficients of variation of these markers are shown in Table 2.
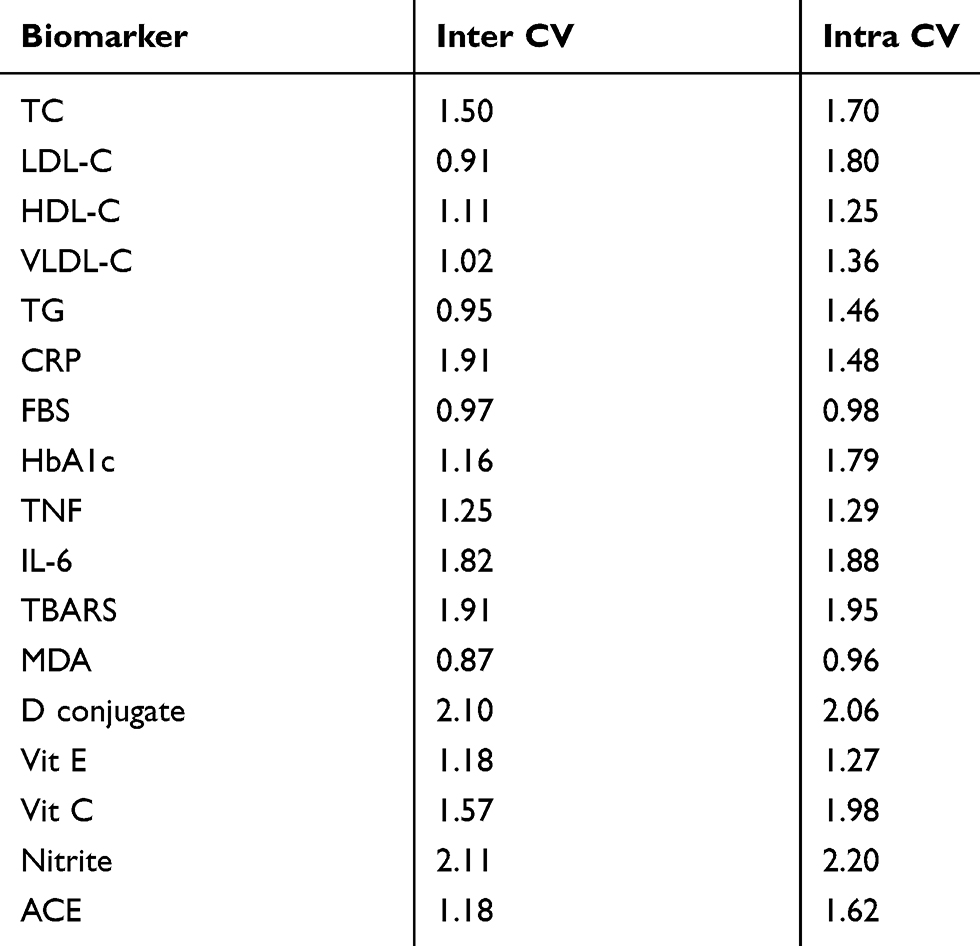 |
Table 2 Inter- and Intra-Assay Coefficients of Variation for the Measured Biomarkers (CV) |
The number of participants recruited was in accordance with a minimal sample size (n = 48) calculated by power analysis (G*Power 3.1, Heinrich Heine University, Düsseldorf, Germany), with effects size set at 0.30, alpha error probability 0.05, power 0.80 for two groups and two measurements of study outcomes. Subject baseline data were analyzed using a two-tailed two-sample t-test. Two-way mixed model ANOVA with repeated measures (treatment vs time interaction) adjusted for age and gender was used to establish if any significant differences existed between patients’ responses over time of intervention. The statistical significance was set at P ≤ 0.05. All values are reported as mean ± SD. Data were analyzed using the SPSS program (version 21.0) (SPSS Inc., Chicago, IL, USA).
Results
All subjects completed the study and both interventions were well tolerated with no ill-reported effects. HRW favorably affected all outcomes at 24-week follow-up as compared to placebo (P < 0.05), except for TBARS, a marker of lipid peroxidation (P = 0.309) (Table 3). Other markers of oxidation (MDA, D-conjugate) decreased while vitamins E and C increased in the HRW group. This was accompanied by a significant reduction in HR, BMI and WHR after HRW intervention (P < 0.05). HRW induced a significant reduction in total cholesterol by approximately 18.5 mg/dL (P < 0.05), and in triglycerides levels by ~ 47 mg/dL (P < 0.05). Fasting blood glucose also decreased after 24-week HRW intervention from 121.5 ± 61.0 mg/dL to 103.1 ± 33.0 mg/dL, with an accompanying 12% reduction in HbA1C (P < 0.05). Furthermore, HRW significantly attenuated the inflammatory markers, such as TNF-α, IL-6, and CRP (P<0.05).
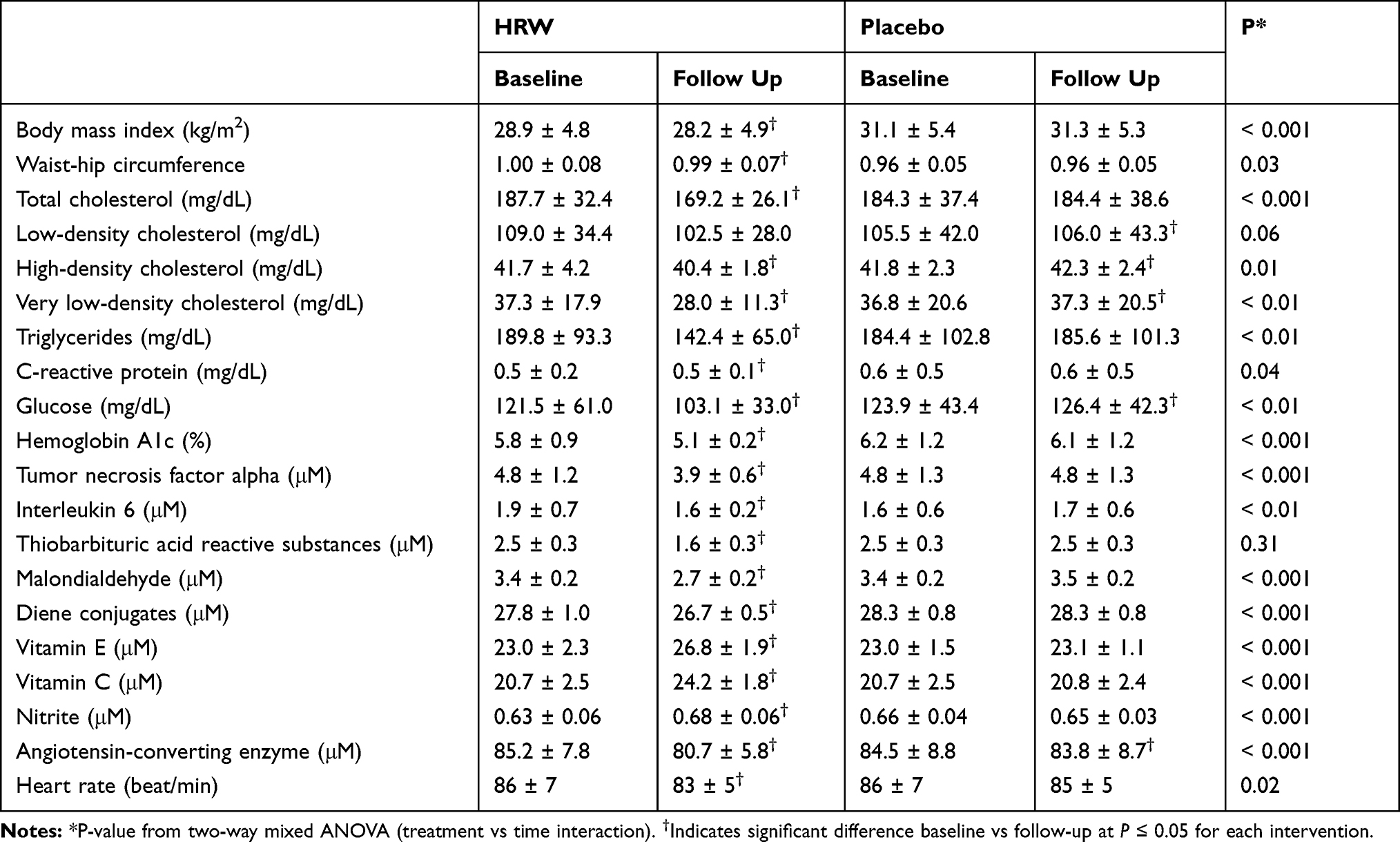 |
Table 3 Changes in Body Composition and Biochemical Variables from Baseline to 24 Weeks. Values are Mean ± SD |
Discussion
Uncontrolled metabolic syndrome increases the risk of cardiovascular disease. For example, the risk factors that are associated with metabolic syndrome play causative roles in the development of atherosclerosis, which further leads to coronary artery disease, stroke, and myocardial infarction.27 Atherosclerosis develops when LDL cholesterol infiltrates the subendothelial space and gets oxidized, which promotes inflammation and subsequent migration and transformation of vascular smooth muscle cells.28 This process is further exacerbated in the presence of hyperglycemia due to the increased formation of advanced-glycated end products (AGEs), which is when the reducing end of glucose molecules reacts and combines with proteins and creates protein cross-linking. AGEs further promote inflammation, oxidation, and cellular damage contributing to cardiovascular disease.28 Accordingly, in our study we determined if high concentration HRW would improve the various biomarkers of metabolic syndrome that are casually involved in the development of cardiovascular disease namely dyslipidemia (HDL, LDL, VLDL, TG), inflammation (TNF-α, IL-6, CRP), oxidative stress, (MDA, TBARS, diene conjugates, vitamins E and C,) and hyperglycemia (glucose, HbA1c).
In this study, we found that a 24-week intervention with high-concentration HRW improved several biomarkers of cardiometabolic health in mid-age men and women with metabolic syndrome, including BMI, WHR, resting HR, blood lipids and glucose, inflammation and redox homeostasis. The favorable changes in blood cholesterol need to be cautiously interpreted since the absolute change was relatively low, and HDL decreased by ~ 1.3 mg/dL. HDL cholesterol is considered to be beneficial due to its role in reverse cholesterol transport.29 However, the ratios of total cholesterol or triglycerides to HDL are better predictors of cardiovascular disease than total cholesterol, with lower ratios correlating with a lower risk for heart disease.30 Since we found that HRW significantly lowered total cholesterol (by ~ 18.5 mg/dL), the ratio of total cholesterol to HDL favorably decreased by ~ 7.2%, whereas it stayed the same in the placebo group. Similarly, the risk ratio of triglycerides to HDL auspiciously decreased by 22.9% in the HRW group, yet stayed about the same in the placebo group. Our data also show that HRW essentially lowered the mean glucose level from the upper range to the lower range of the prediabetic criteria, which was also accompanied by a 12% reduction of HbA1C.
These favorable changes in cholesterol and glucose are corroborated with a few discrepancies in several previous clinical trials. For example, Song et al reported that HRW, supplying 0.5 millimoles H2/day, for 10 weeks in patients with potential metabolic syndrome decreased total serum cholesterol and LDL-C levels, improved HDL function and redox status (eg increased serum superoxide dismutase [SOD] and decreased MDA), and reduced inflammation (eg serum TNF-α).31 However, whereas our study showed significant improvements in BMI, WHR, and fasting glucose, their study only reported a potential, albeit non-significant, downward trend in these parameters. Similarly, an earlier randomized, placebo-controlled, crossover study in patients with type 2 diabetes or impaired glucose tolerance demonstrated that ingestion of HRW (~ 0.6 millimoles/day) slightly improved cholesterol, significantly decreased markers of oxidative stress (eg urinary 8-isoprostanes) and increased serum SOD.32 However, in contrast to our study, there were no statistically significant changes in either BMI, CRP, HbA1c, or fasting blood glucose. Perhaps the higher dose of H2 and longer duration of our study compared to those studies could account for the differences. Additionally, the subjects in our study had significantly higher baseline glucose levels (~ 122 mg/dL vs 108 mg/dL). Lastly, although not tested in our study, the previous study32 reported that in 4 of 6 subjects with impaired glucose tolerance, HRW normalized the oral glucose tolerance test, and that 1 hr plasma insulin levels were significantly increased compared to baseline.32
An open-label 8-week study on 20 subjects with potential metabolic syndrome demonstrated that HRW (~ 1 millimole H2/day) increased SOD level by 39% and decreased TBARs by 43%.15 Although a decrease in TBARS was not detected in our study, we found a decrease in the more specific marker of lipid peroxidation MDA, as well as increased levels of vitamins C and E, which collectively suggest that HRW favorably modulates oxidative processes. Similar to our study, the open-label trial revealed that HRW decreased the total cholesterol to HDL ratio by 13%. However, in our study, the primary change was a decrease in total cholesterol, whereas in the open-label study, it was an increase in HDL cholesterol. Additionally, in contrast to our findings, HRW did not decrease BMI, triglycerides or fasting blood glucose. However, the triglyceride and fasting glucose level was significantly higher in the subjects in our study compared to those in the open-label study (~ 143 mg/dL vs 190 mg/dL; 88 mg/dL vs 122 mg/dL, respectively). Again, it may be due to our study condition with a higher dose of H2 and the longer time duration.
The underlying molecular mechanisms that mediate these effects induced by HRW need further study. However, H2 appears to influence metabolism and bioenergetics.33 For example, we previously demonstrated that HRW treatment increased mitochondrial coenzyme Q9 concentration, which enhanced mitochondrial respiratory chain function (ie complex I and complex II) and subsequent increase in ATP production rat myocardium.34,35 In another study in mice lacking the leptin receptor, and in normal mice fed a high-fat diet, HRW reduced oxidative stress, reduced fatty liver deposits, and decreased plasma glucose, insulin, and triglyceride levels. This effect was comparable to a 20% caloric restriction.36 HRW increased energy expenditure as measured by oxygen consumption and induced the hepatic hormone, fibroblast growth factor 21 (FGF-21), which stimulates fatty acid and glucose expenditure.36 In streptozotocin-induced type 1 diabetic mice, H2 induced translocation of glucose transporter-4 via activation of phosphatidylinositol-3-OH kinase (PI3K), protein kinase C (PKC), and AMP-activated protein kinase (AMPK).37
This study demonstrated that HRW induced significant improvements in clinically relevant metrics of blood biomarkers and biometric data in subjects with metabolic syndrome. Compared to previous studies, it may also indicate that high doses of H2 are more effective than lower doses at least in metabolic syndrome. However, more dose-dependent studies in this area are needed. Moreover, several limitations should be considered when interpreting our study. We only performed analysis during the final 24 weeks instead of at 4-week follow-ups, which prevented us from finding important temporal changes in the various parameters. We also did not investigate gender- or age-dependent effects, which may be important since metabolic parameters are influenced by both sex and age.38 Additionally, although subjects were instructed to consume HRW on an empty stomach, we could not ensure that this occurred. There may be differences in the biological effects of H2 if HRW is ingested with or without food intake since following ingestion of normal fibers from the diet, bacterial production of H2 gas significantly increases.39 Lastly, we did not measure the temporal changes or pharmacokinetics of H2 in the blood and breath of the subjects. Therefore, the suggested molecular mechanisms as demonstrated in vitro or in animal studies may be different than those in our study since the cellular H2 concentration may be significantly different. Future research should investigate if there are sexually dimorphic responses to H2 therapy, the molecular mechanisms of H2 at physiologically relevant H2 concentrations, and also the comparison of the effects of different doses, durations, and methods of administration (eg drinking vs inhaling).
Conclusion
In conclusion, the results from our study suggest that supplementation with high-concentration HRW produced via H2-producing tablets improves body composition, favorably modulates fatty acid and glucose metabolism, and improves inflammation and redox homeostasis in subjects with metabolic syndrome. Therefore, long-term treatment with high-concentration hydrogen-rich water may be used as an adjuvant therapy to decrease the features of metabolic syndrome. However, a larger prospective clinical trial is warranted to further determine the biological effects of HRW in this subject population.
Data Sharing Statement
The data presented in this article constitutes all data that the authors plan on making publicly available.
Acknowledgments
We thank Mr. Alex Tarnava, CEO of HRW Natural Health Products Inc. for kindly donating DrinkHRW tablets for this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was partially supported by Slovak Research and Development Agency (APVV)-0241-11, APVV-15-0376; ITMS 26230120009; Scientific grant agency of the Ministry of Education of the Slovak Republic (VEGA) 2/0063/18, and by HRW Natural Health Products Inc.
Disclosure
TWL reports personal fees from medical/academic conferencesincluding travel reimbursement, honoraria, and speaking and consultancy fees from various academic and commercial entities regarding molecular hydrogen. All other authors report no conflict of interest.
References
1. O’neill S, O’driscoll L. Metabolic syndrome: a closer look at the growing epidemic and its associated pathologies. Obes Rev. 2015;16(1):1–12. doi:10.1111/obr.12229
2. Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444(7121):860–867. doi:10.1038/nature05485
3. Pitsavos C, Panagiotakos D, Weinem M, Stefanadis C. Diet, exercise and the metabolic syndrome. Rev Diabet Stud. 2006;3(3):118–126. doi:10.1900/RDS.2006.3.118
4. Chaves H, Pella D, Singh R, et al. The challenges of prevention of cardiovascular diseases. A Scientific Statement of the International College of Cardiology World Heart J. 2016;8:282–288.
5. LeBaron TW, Kura B, Kalocayova B, Tribulova N, Slezak J. A new approach for the prevention and treatment of cardiovascular disorders. molecular hydrogen significantly reduces the effects of oxidative stress. Molecules. 2019;24(11). doi:10.3390/molecules24112076
6. Mojto V, Singh R, Gvozdjakova A, Pella D, Fedacko J, Pella D. Molecular hydrogen: a new approach for the management of cardiovascular diseases. World Heart J. 2018;10:83–93.
7. Kura B, Bagchi AK, Singal PK, et al. Molecular hydrogen (H2): potential in mitigating oxidative stress-induced cardiotoxicity. Can J Physiol Pharmacol. 2018;97:287–292.
8. Kamimura N, Ichimiya H, Iuchi K, Ohta S. Molecular hydrogen stimulates the gene expression of transcriptional coactivator PGC-1 [alpha] to enhance fatty acid metabolism. NPJ Aging Mech Dis. 2016;2:16008. doi:10.1038/npjamd.2016.8
9. Sobue S, Inoue C, Hori F, Qiao S, Murate T, Ichihara M. Molecular hydrogen modulates gene expression via histone modification and induces the mitochondrial unfolded protein response. Biochem Biophys Res Commun. 2017;493(1):318–324. doi:10.1016/j.bbrc.2017.09.024
10. LeBaron TW, Laher I, Kura B, Slezak J. Hydrogen gas: from clinical medicine to an emerging ergogenic molecule for sports athletes (1). Can J Physiol Pharmacol. 2019;97(9):797–807. doi:10.1139/cjpp-2019-0067
11. Ohsawa I, Ishikawa M, Takahashi K, et al. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat Med. 2007;13(6):688–694. doi:10.1038/nm1577
12. Ono H, Nishijima Y, Ohta S, et al. Hydrogen gas inhalation treatment in acute cerebral infarction: a randomized controlled clinical study on safety and neuroprotection. J Stroke Cerebrovasc Dis. 2017;26(11):2587–2594. doi:10.1016/j.jstrokecerebrovasdis.2017.06.012
13. Ostojic SM. Molecular hydrogen: an inert gas turns clinically effective. Ann Med. 2015;47:1–4.
14. Nishimaki K, Asada T, Ohsawa I, et al. Effects of molecular hydrogen assessed by an animal model and a randomized clinical study on mild cognitive impairment. Curr Alzheimer Res. 2017;15:482–492.
15. Nakao A, Toyoda Y, Sharma P, Evans M, Guthrie N. Effectiveness of hydrogen rich water on antioxidant status of subjects with potential metabolic syndrome-an open label pilot study. J Clin Biochem Nutr. 2010;46(2):140–149. doi:10.3164/jcbn.09-100
16. LeBaron TW, Larson AJ, Ohta S, et al. Acute supplementation with molecular hydrogen benefits submaximal exercise indices. Randomized, double-blinded, placebo-controlled crossover pilot study. J Lifestyle Med. 2019;9(1):36–43. doi:10.15280/jlm.2019.9.1.36
17. Mikami T, Tano K, Lee H, et al. Drinking hydrogen water enhances endurance and relieves psychometric fatigue: a randomized, double-blind, placebo-controlled study (1). Can J Physiol Pharmacol. 2019;97(9):857–862. doi:10.1139/cjpp-2019-0059
18. Ohsawa I, Nishimaki K, Yamagata K, Ishikawa M, Ohta S. Consumption of hydrogen water prevents atherosclerosis in apolipoprotein E knockout mice. Biochem Biophys Res Commun. 2008;377(4):1195–1198. doi:10.1016/j.bbrc.2008.10.156
19. Zhang Y, Xu J, Long Z, et al. Hydrogen (H2) inhibits isoproterenol-induced cardiac hypertrophy via antioxidative pathways. Front Pharmacol. 2016;7:392. doi:10.3389/fphar.2016.00392
20. Ohno K, Ito M, Ichihara M, Ito M. Molecular hydrogen as an emerging therapeutic medical gas for neurodegenerative and other diseases. Oxid Med Cell Longev. 2012;2012:353152. doi:10.1155/2012/353152
21. Fujita K, Seike T, Yutsudo N, et al. Hydrogen in drinking water reduces dopaminergic neuronal loss in the 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine mouse model of Parkinson’s disease. PLoS One. 2009;4(9):e7247. doi:10.1371/journal.pone.0007247
22. Matsumoto A, Yamafuji M, Tachibana T, Nakabeppu Y, Noda M, Nakaya H. Oral ‘hydrogen water’ induces neuroprotective ghrelin secretion in mice. Sci Rep. 2013;3:3273. doi:10.1038/srep03273
23. Yoshii Y, Inoue T, Uemura Y, et al. Complexity of Stomach-brain interaction induced by molecular hydrogen in Parkinson’s disease model mice. Neurochem Res. 2017;42(9):2658–2665. doi:10.1007/s11064-017-2281-1
24. Jackson K, Dressler N, Ben-shushan RS, Meerson A, LeBaron TW, Tamir S. Effects of alkaline-electrolyzed and hydrogen-rich water, in a high-fat-diet nonalcoholic fatty liver disease mouse model. World J Gastroenterol. 2018;24(45):5095–5108. doi:10.3748/wjg.v24.i45.5095
25. Korovljev D, Stajer V, Ostojic J, LeBaron TW, Ostojic SM. Hydrogen-rich water reduces liver fat accumulation and improves liver enzyme profiles in patients with non-alcoholic fatty liver disease: a randomized controlled pilot trial. Clin Res Hepatol Gastroenterol. 2019;43(6):688–693. doi:10.1016/j.clinre.2019.03.008
26. Korovljev D, Trivic T, Drid P, Ostojic SM. Molecular hydrogen affects body composition, metabolic profiles, and mitochondrial function in middle-aged overweight women. Ir J Med Sci. 2017;187:85–89.
27. Tune JD, Goodwill AG, Sassoon DJ, Mather KJ. Cardiovascular consequences of metabolic syndrome. Transl Res. 2017;183:57–70. doi:10.1016/j.trsl.2017.01.001
28. Katakami N. Mechanism of development of atherosclerosis and cardiovascular disease in diabetes mellitus. J Atheroscler Thromb. 2018;25(1):27–39. doi:10.5551/jat.RV17014
29. Fisher EA, Feig JE, Hewing B, Hazen SL, Smith JD. High-density lipoprotein function, dysfunction, and reverse cholesterol transport. Arterioscler Thromb Vac Biol. 2012;32(12):2813–2820. doi:10.1161/ATVBAHA.112.300133
30. da Luz PL, Favarato D, Faria-neto JR
31. Song G, Li M, Sang H, et al. Hydrogen-rich water decreases serum LDL-cholesterol levels and improves HDL function in patients with potential metabolic syndrome. J Lipid Res. 2013;54(7):1884–1893. doi:10.1194/jlr.M036640
32. Kajiyama S, Hasegawa G, Asano M, et al. Supplementation of hydrogen-rich water improves lipid and glucose metabolism in patients with type 2 diabetes or impaired glucose tolerance. Nutr Res. 2008;28:137–143. doi:10.1016/j.nutres.2008.01.008
33. Ostojic SM. Does H2 alter mitochondrial bioenergetics via ghs-r1alpha activation? Theranostics. 2017;7(5):1330–1332. doi:10.7150/thno.18745
34. Kucharská J, Gvozdjáková A, Kura B, Rausová Z, Slezák J. Effect of molecular hydrogen on coenzyme Q in plasma, myocardial tissue and mitochondria of rats. J Nutr Heal Food Eng. 2018;8:362–364.
35. Gvozdjakova A, Kucharska J, Kura B, et al. A new insight into the molecular hydrogen effect on coenzyme Q and mitochondrial function of rats. Can J Physiol Pharmacol. 2019;98:29–34.
36. Kamimura N, Nishimaki K, Ohsawa I, Ohta S. Molecular hydrogen improves obesity and diabetes by inducing hepatic FGF21 and stimulating energy metabolism in db/db mice. Obesity (Silver Spring). 2011;19(7):1396–1403. doi:10.1038/oby.2011.6
37. Amitani H, Asakawa A, Cheng KC, et al. Hydrogen improves glycemic control in type1 diabetic animal model by promoting glucose uptake into skeletal muscle. PLoS One. 2013;8(1). doi:10.1371/annotation/ea26285b-dda3-470d-a8df-241df9fbc5ad.
38. Argente-arizon P, Ros P, Diaz F, et al. Age and sex dependent effects of early overnutrition on metabolic parameters and the role of neonatal androgens. Biol Sex Differ. 2016;7:26. doi:10.1186/s13293-016-0079-5
39. Strocchi A, Levitt MD. Maintaining intestinal H2 balance: credit the colonic bacteria. Gastroenterology. 1992;102(4 Pt 1):1424–1426. doi:10.1016/0016-5085(92)90790-6
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.