")
Back to Journals » International Medical Case Reports Journal » Volume 16
The Effectiveness of Microdosed Psilocybin in the Treatment of Neuropsychiatric Lyme Disease: A Case Study
Authors Kinderlehrer DA
Received 29 October 2022
Accepted for publication 25 January 2023
Published 3 March 2023 Volume 2023:16 Pages 109—115
DOI https://doi.org/10.2147/IMCRJ.S395342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Daniel A Kinderlehrer
Private Practice, Denver, CO, USA
Correspondence: Daniel A Kinderlehrer, Email [email protected]
Abstract: Lyme disease can result in severe neuropsychiatric symptoms that may be resistant to treatment. The pathogenesis of neuropsychiatric Lyme disease is associated with autoimmune induced neuroinflammation. This case report describes an immunocompetent male with serologically positive neuropsychiatric Lyme disease who did not tolerate antimicrobial or psychotropic medications and whose symptoms remitted when he began psilocybin in microdosed (sub-hallucinogenic) amounts. A literature review of its therapeutic benefits reveals that psilocybin is both serotonergic and anti-inflammatory and therefore may offer significant therapeutic benefits to patients with mental illness secondary to autoimmune inflammation. The role of microdosed psilocybin in the treatment of neuropsychiatric Lyme disease and autoimmune encephalopathies warrants further study.
Keywords: Lyme, neuroinflammation, psychedelic, psilocybin, microdose, mental illness, autoimmune, encephalopathy
Introduction
Lyme borreliosis is an infection caused by Borrelia burgdorferi sensu lato (Bbsl). These bacteria are transmitted by Ixodes ticks and can generate multisystem complaints. Persistent infection, resulting in chronic neurological symptoms, is well documented.1–8 It is now appreciated that chronic infection with Bbsl can cause a host of psychiatric issues, and that neuropsychiatric complaints, particularly anxiety and depression, may dominate the clinical picture. In addition, chronic Lyme neuroborreliosis has been linked to eating disorders, addiction syndromes, violence, anhedonia, depersonalization, dissociative episodes, suicide, and illnesses that look like schizoaffective disorders and bipolar disease.9–16
The neurological manifestations of Lyme disease are often complicated by co-infections, other microbes that are additionally transmitted by Ixodes ticks and exacerbate the clinical picture. In particular, Bartonella spp. are associated with a wide range of mental health disorders including anxiety, panic disorder, depression, obsessive compulsive disorder (OCD), phobias, eating disorders, alcohol and drug abuse, psychosis and personality disorders.17–21 Other tick-borne microbes including Babesia and Mycoplasma spp. may also engender mental health issues.22–29
The pathophysiology of mental health disorders as a result of these infections may be a result of multiple mechanisms. While neuroborreliosis can be caused by infection of the central nervous system or vascular disruption, most often it is associated with neuroinflammation from infection outside the nervous system. Persistent infection with Bbsl can result in the production of anti-neuronal antibodies and autoimmunity with the production of proinflammatory cytokines, chemokines and proinflammatory lipoproteins.9,30–33
There is increasing recognition that mood disorders may be linked to persistent infections and autoimmune illnesses.34 This pathophysiology is exemplified in patients with Pediatric Acute-onset Neuropsychiatric Syndrome (PANS), in which antineuronal antibodies generated by microbial triggers cross the blood brain barrier resulting in neuroinflammation; children suffering from PANS exhibit severe mood and behavioral symptoms.35
The treatment of Microbe-induced Autoimmune Neuropsychiatric Syndromes (MANS) thus requires a trimodal approach: psychopharmacologic agents, antimicrobials, and anti-inflammatory agents. In the latter category, several interventions have exhibited some but limited success. These include nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroids, and intravenous immunoglobulin (IVIG).36
There is compelling evidence that psilocybin has potential value in the treatment of some mental health conditions. Multiple studies have documented its effectiveness in patients with depression, anxiety syndromes, end of life anxiety, and suggested benefit in OCD and addiction disorders.37–43 Psilocybin is a serotonin agonist with an affinity for several serotonin receptors.44 In addition, psilocybin extracts are capable of down-regulating pro-inflammatory mediators and have been shown to have anti-inflammatory activity.45–48 These actions suggest that psilocybin has potential benefit in treating mental health issues associated with neuroinflammation.
Methods
A case is presented of an immunocompetent 70-year-old male diagnosed with polymicrobial tick-borne infections: neuroborreliosis, babesiosis and bartonellosis. His predominant symptoms were neuropsychiatric. The patient was not responding to antimicrobial or psychotropic pharmaceuticals, but symptoms remitted when treated with low intermittent doses of psilocybin—ie, microdosing.
Informed consent was obtained from the patient to publish this history. No institutional review was required.
Case Presentation
This patient was well until the age of 46 when he experienced the acute onset of fever, rigors, drenching sweats and myalgias. These symptoms lasted three days then recurred weekly for the next two weeks. Physical examination was significant for splenomegaly, and laboratory tests were positive for acute Lyme disease (see Table 1). He was not aware of a tick attachment or a rash; he lived in eastern Massachusetts.
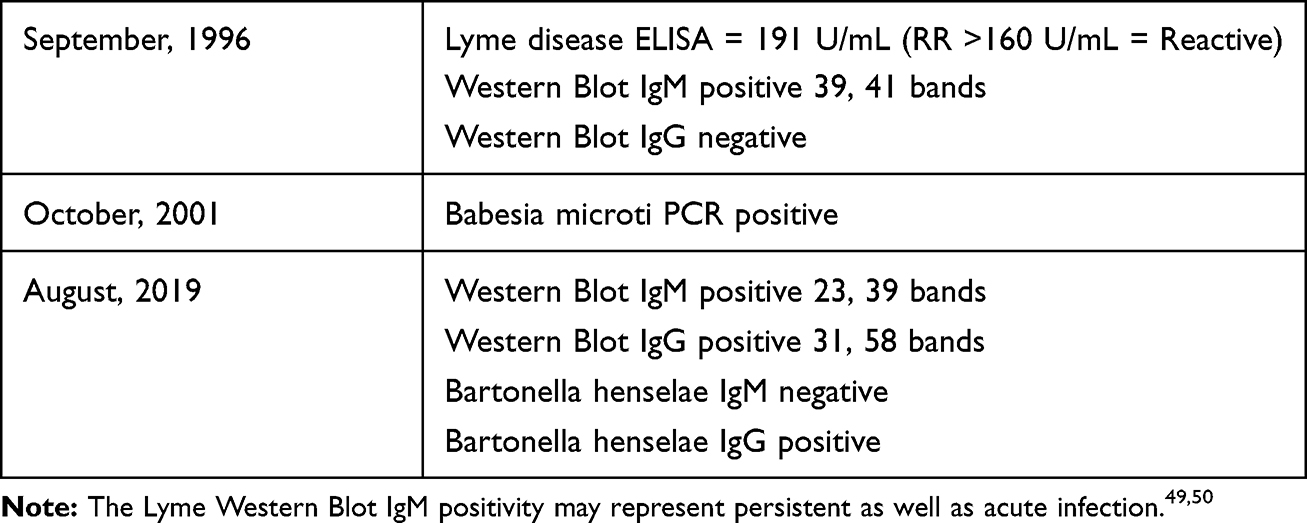 |
Table 1 Results of Testing for Tick-Borne Infections |
Treatment was begun with oral doxycycline, and the recurrent febrile episodes remitted, but he subsequently developed severe insomnia and anxiety. Over the next ten months he was on continuous antibiotics with oral doxycycline, clarithromycin or cefuroxime, either alone or in combination. In addition to insomnia and anxiety he complained of myalgias, neck pain and drenching night sweats. He stopped antibiotics because there was no apparent benefit in his mood or physical symptoms. The subject did not have a family history of psychiatric illness, had no prior history of mood disorder, and had not experienced a stressful event that might precipitate mood issues.
Five years after the onset of his illness he was diagnosed with babesiosis with PCR positivity (see Table 1). He took three weeks of azithromycin and atovaquone resulting in a Herxheimer reaction with panic attacks. At the end of three weeks his symptoms had lessened.
Over the next two decades the patient continued to have partial remissions and relapses. The relapses manifested in anxiety, panic attacks, depression, cognitive dysfunction and insomnia, and were accompanied by fatigue, neck pain, myalgias and night sweats. The relapses typically lasted about two years. Antidepressants including sertraline and mirtazapine were somewhat helpful but over time were not tolerated. At some point the patient was clinically diagnosed with bartonellosis, and was maintained on sulfamethoxazole-trimethoprim (SMZ-TMP) with some benefit. Laboratory tests subsequently demonstrated positive serologies to both Borrelia burgdorferi and Bartonella henselae (see Table 1).
At 70 years old, the patient suffered a relapse when his antimicrobial regimen was changed. He again experienced severe depression, anxiety, and sleep difficulties, as well as a return of his physical symptoms. He could no longer tolerate any antimicrobials without making his symptoms worse. He was prescribed benzodiazepines for sleep and anxiety but they made the depression worse. Sertraline afforded no benefit. After suffering for three months, he began microdosing psilocybin (desiccated whole mushrooms) 100 mg orally three times a week, increasing the dose to 125 mg after two weeks. Within two days there was a noticeable improvement in mood. Within two weeks he was feeling consistently well again. He has continued this regimen and two years later his depression and anxiety continue to be in remission.
When the subject began this treatment regimen, he was led to expect that it would take two weeks to have any benefit, if at all. He stated that he believed it had a 50% chance of helping him. He was genuinely surprised that he experienced benefits so quickly after starting the regimen.
Discussion
Within three weeks of the acute onset of symptoms, this patient was diagnosed with Lyme disease, but despite antibiotics he continued to be symptomatic. It was only after being diagnosed with babesiosis that it became clear that he did not respond to the initial antimicrobials because of the presence of co-infections. In fact, the acute onset of high fevers, rigors and diaphoresis with splenomegaly is consistent with babesiosis and not with Lyme borreliosis. But since he continued to suffer from neuropsychiatric symptoms, he was subsequently also diagnosed with bartonellosis. This diagnosis was supported by his response to SMZ-TMP as well as subsequent serologic testing. The presence of co-infections in patients with persistent Lyme disease is more the rule than the exception.51–58
It is clear that the etiology of this subject’s neuropsychiatric symptoms is the presence of tick-borne infections. The neuropsychiatric symptoms began within a month of the acute infection; the subject had no prior history of mood disorders; relapses in his mood issues were accompanied by physical symptoms consistent with the infections; Herxheimer reactions caused an exacerbation in neuropsychiatric symptoms; there was no family history of psychiatric disorders and no stressful event to account for a mood disorder.
As noted previously, these tick-borne infections often result in significant neuropsychiatric symptoms. Patients with neuropsychiatric Lyme disease are often intolerant of psychotropic medication or resistant to their benefits.9,32 The underlying pathophysiology of autoimmune neuroinflammation suggests the need for additional pharmaceutical approaches.
After a 40-year prohibition in the US of lysergic acid diethylamide (LSD) and psilocybin, there has been renewed interest in their potential for therapeutic benefit. The preponderance of research in the past two decades has been in controlled clinical settings in which subjects are administered a single high dose of a hallucinogen while under the supervision of a therapist/guide. In 2018 the US Food and Drug Administration categorized psilocybin as “a breakthrough therapy” in the treatment of depression, a designation the agency applies to drugs that in early trials demonstrate substantial improvement over existing treatments.59
Microdosing is the practice of consuming very low, sub-hallucinogenic doses of a psychedelic substance on a regular basis. The intention of microdosing is to offer similar benefits to full dose psychedelic therapy, but without perceptual distortions, the need for clinical oversight, or the risk of a “bad trip”.60
Microdosing has become increasingly popular. In one online microdosing forum that was begun in 2013, the number of subscribers rose to 40,000 in 2018 and 219,000 in October 2022.61 LSD and psilocybin continue to be listed as schedule I controlled substances, meaning legally they have no accepted therapeutic value. Nevertheless, possession of psilocybin has been decriminalized in many US cities and is on the ballot of many states to be legalized in clinical therapeutic settings; Oregon and Colorado have already done so.62
Typical full dose psilocybin psychotherapy ranges from 3.0 to 5.0 gm of dried mushroom as a single dose. The doses of psilocybin used in clinical studies refers to a synthetic version of the active purified derivative, O-phosphoryl-4-hydroxy-N,N-dimethyltryptamine, a.k.a. psilocin, and averages 25 mg. for a single dose. Microdoses of psilocybin are commonly taken two to three times a week at doses of 0.1 to 0.3 gm of dried mushroom. While the concentration of the active substance varies among mushrooms, 25 mg of psilocin is roughly equivalent to 5 gm of dried mushroom. Therefore, a macrodose is anywhere from ten to fifty times more potent than a microdose.
There are numerous reports in the medical literature regarding the therapeutic benefits of microdosed psilocybin in which recipients report reductions in stress, anxiety and depression as well as improvements in cognition and creativity.61,63–67 The majority of these reports have significant shortcomings: most are anecdotal or open-label research utilizing self-reported surveys; investigators generally included users of both microdosed LSD and psilocybin; and the positive outcomes could not consistently be distinguished from preexisting expectations or placebo effect.68–71 Clearly it would be preferable to perform prospective, controlled and blinded studies, and to do so on psilocybin and LSD separately.
Cavanna et al performed a double-blind placebo-controlled study of psilocybin with 0.5 gm of ground dried mushroom administered two separate days for one week and a placebo of the same weight administered two separate days on a different week.72 There were 34 participants, and the sequence was randomized by a third party. The investigators documented subjective changes in the participants while on the active leg of the study, characterized only by the participants’ capacity to distinguish the active vs placebo intervention. There were EEG changes (reduced activity in the theta band) in the active leg but the only other difference between the active and placebo arms was a slight impairment in cognition when taking the psilocybin. The authors concluded that alleged benefits of microdosing psilocybin are a placebo effect.
The Cavanna study suffers from obvious shortcomings: the dose of 0.5 gm is over twice the average microdose; one week with two doses was an exceedingly short trial; there were only 34 participants; and the study design excluded subjects with a history of anxiety or depression.
It is clear that studies based on self-reporting of subjective symptoms suffer from validation issues. In none of the studies described above are populations matched in the active vs placebo arms of the trials in terms of mental health issues. Indeed, it is difficult to quantify these subjective symptoms; outcomes are assessed by self-reporting that could suffer from expectations or inaccurate memories.
The benefit of macrodosed psilocybin for some mental health disorders is well documented. However, thus far the evidence for similar benefits of microdosed psilocybin remains anecdotal. Clearly more research on the effectiveness of microdosing is warranted.
The subject of this report maintains that he was not expecting any response to the microdose intervention, if any, for at least two weeks. Unexpectedly, he experienced a significant decrease in anxiety and depression within two days. In his case, this would appear to exclude a placebo effect.
Most reports on psilocybin attribute its mental health benefits to its role as a serotonin agonist. Psilocybin has a high affinity for the serotonin receptor 5-HT2A, and milder affinity for serotonin receptors 5-HT1A and 5-HT2C, as well as other serotonin and non-serotonin receptors.44,73,74 While pretreatment with ketanserin, a 5-HT2A antagonist, can block the psychomimetic effects of psilocybin,75 one animal study found that ketanserin did not appear to block its antidepressant action.74 In addition, stimulation of both the 5-HT1A and 5-HT2A receptors could be linked to striatal dopamine release, suggesting that psilocybin-induced psychotropic effects could be both dopaminergic and serotonergic.73,76
Less attention has been paid to the anti-inflammatory action of psilocybin, which could yield significant therapeutic benefit when mental health issues are associated with neuroinflammation. Serotonin is a known immune modulator as well as a neurotransmitter, suppressing the production of cytokines by human macrophages.47 Extracts of psilocybin containing mushrooms significantly inhibit the lipopolysaccharide production of tumor necrosis factor (TNF)-α and interleukin (IL)-1β, and lowered IL-6 and cyclooxygenase-2 concentrations in human macrophage cells.46–48 In a review of the immunomodulatory effects of psychedelics, Thompson and Szabo have proposed that these agents hold the potential to “attenuate or even resolve autoimmunity”.77 In the case presentation under discussion, the rapidity of the clinical response to microdosed psilocybin is consistent with the anti-inflammatory actions of this agent.
Concerning safety issues, Studerus et al reviewed eight studies consisting of 110 human subjects, each of whom received one to four macrodoses of psilocybin.78 The only adverse reactions were short-term dysphoria and/or anxiety; these reactions were associated with the highest doses of psilocybin. The subjects were followed for eight to 16 months post psilocybin administration, and did not report any long-term side effects. The participants in those studies received ten to fifty times the amount of an average microdose. In studies of individuals who microdose, the only adverse reactions reported have been short-term physical discomfort, impaired cognition and anxiety.79
Conclusion
Neuropsychiatric Lyme disease is associated with autoimmune neuroinflammation triggered by microbial infection. While antibiotics and psychopharmacologic agents are important arms of treatment, agents that can modulate the inflammatory response without immune suppression have therapeutic potential. In the present case presentation, an immunocompetent male with well documented neuropsychiatric Lyme disease experienced significant improvement soon after taking microdoses of psilocybin three times weekly.
The therapeutic benefit of a single high dose of psilocybin in some mental health disorders administered while under the supervision of a therapist/guide has been well documented. While the evidence for therapeutic benefit in those who microdose has not been well authenticated, the anti-inflammatory action of psilocybin may be valuable in the treatment of autoimmune conditions in general and autoimmune neuroinflammation in particular. The present case history is the first to document the successful application of microdosed psilocybin in the treatment of mental health issues secondary to microbe induced autoimmune neuroinflammation.
Clearly more research is warranted into the therapeutic potential of microdosing psilocybin in patients with mental health issues and autoimmunity. Ideally, studies will employ double blinded placebo-controlled investigations in which matched subjects include those with anxiety and depression. Similar research in patients suffering from neuropsychiatric Lyme and other autoimmune encephalopathies could yield effective therapeutic options in this difficult to treat population.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Lawrence C, Lipton RB, Lowy FD, Coyle PK. Seronegative chronic relapsing neuroborreliosis. Eur Neurol. 1995;35:113–117. doi:10.1159/000117104
2. Logigian EL, Kaplan RF, Steere AC. Chronic neurologic manifestations of Lyme disease. N Engl J Med. 1990;323:1438–1444. doi:10.1056/NEJM199011223232102
3. Shadick NA, Phillips CB, Logigian EL, et al. The long-term clinical outcomes of Lyme disease. A population-based retrospective cohort study. Ann Intern Med. 1994;121:560–567. doi:10.7326/0003-4819-121-8-199410150-00002
4. Liegner KB, Rosenkilde C, Campbell G, et al. Culture confirmed treatment failure of cefotaxime and minocycline in a case of Lyme meningoencephalomyelitis in the United States.
5. Embers ME, Barthold SW, Borda JT, et al. Persistence of Borrelia burgdorferi in rhesus macaques following antibiotic treatment of disseminated infection. PLoS One. 2012;7(1):e29914. PMID: 22253822; PMCID: PMC3256191. doi:10.1371/journal.pone.0029914
6. Embers ME, Hasenkampf NR, Jacobs MB, et al. Variable manifestations, diverse seroreactivity and post-treatment persistence in non-human primates exposed to Borrelia burgdorferi by tick feeding. PLoS One. 2017;12(12):e0189071. PMID: 29236732; PMCID: PMC5728523. doi:10.1371/journal.pone.0189071
7. Hodzic E, Imai D, Feng S, Barthold SW. Resurgence of persisting non-cultivable Borrelia burgdorferi following antibiotic treatment in mice. PLoS One. 2014;9(1):e86907. PMID: 24466286; PMCID: PMC3900665. doi:10.1371/journal.pone.0086907
8. Oksi J, Kalimo H, Marttila RJ, et al. Inflammatory brain changes in Lyme borreliosis. A report on three patients and review of the literature. Brain. 1996;119:2143–2154. PMID: 9010017. doi:10.1093/brain/119.6.2143
9. Bransfield RC. Neuropsychiatric Lyme borreliosis: an overview with a focus on a specialty psychiatrist’s clinical practice. Healthcare. 2018;6(3):104. PMID: 30149626; PMCID: PMC6165408. doi:10.3390/healthcare6030104
10. Bransfield RC. Lyme Disease, comorbid tick-borne diseases, and neuropsychiatric disorders. Psychiatr Times. 2007;24(14):59–61.
11. Fallon BA, Nields JA, Burrascano JJ, et al. The neuropsychiatric manifestations of Lyme borreliosis. Psychiatr Q. 1992;63(1):95–117. doi:10.1007/BF01064684
12. Fallon BA, Nields JA. Lyme disease: a neuropsychiatric illness. Am J Psychiatry. 1994;151(11):1571–1583. PMID: 1438607. doi:10.1007/BF01064684
13. Fallon BA, Kochevar JM, Gaito A, Nields JA. The underdiagnosis of neuropsychiatric Lyme disease in children and adults. Psychiatr Clin N Am. 1998;21(3):693–703. doi:10.1016/s0193-953x(05)70032-0
14. Bransfield RC. Aggressiveness, violence, homicidality, homicide, and Lyme disease. Neuropsychiatr Dis Treat. 2018;14:693–713. PMID: 29576731; PMCID: PMC5851570. doi:10.2147/NDT.S155143
15. Mattingley DW, Koola MM. Association of Lyme disease and schizoaffective disorder, bipolar type: is it inflammation mediated? Indian J Psychol Med. 2015;37(2):243–246. PMID: 25969618; PMCID: PMC4418265. doi:10.4103/0253-7176.155660
16. Greenberg R. Tick-borne infections and pediatric bipolar disorder. Neurol Psychiatry Brain Res. 2015;22:11. doi:10.1016/j.npbr.2015.12.025
17. Breitschwerdt EB, Sontakke S, Hopkins S. Neurological manifestations of bartonellosis in immunocompetent patients: a composite of reports from 2005–2012. J Neuroparasitol. 2012;3:1–15. doi:10.4303/jnp/235640
18. Flegr J, Preiss M, Balátová P. Depressiveness and neuroticism in bartonella seropositive and seronegative subjects-preregistered case-controls study. Front Psychiatry. 2018;9:314. PMID: 30061846; PMCID: PMC6055045. doi:10.3389/fpsyt.2018.00314
19. Breitschwerdt EB, Greenberg R, Maggi RG, et al. Bartonella henselae bloodstream infection in a boy with pediatric acute-onset neuropsychiatric syndrome. J Cent Nerv Syst Dis. 2019;11:1179573519832014. PMID: 30911227; PMCID: PMC6423671. doi:10.1177/1179573519832014
20. Breitschwerdt EB, Bradley JM, Maggi RG, et al. Bartonella associated cutaneous lesions (BACL) in people with neuropsychiatric symptoms. Pathogens. 2020;9(12):1023. PMID: 33291688; PMCID: PMC7761945. doi:10.3390/pathogens9121023
21. Greenberg R. Infections and childhood psychiatric disorders: tick-borne illness and bipolar disorder in youth. Bipolar Disord. 2017;3:113. doi:10.4172/2472-1077.10001
22. Sherr VT. Human babesiosis--an unrecorded reality. Absence of formal registry undermines its detection, diagnosis and treatment, suggesting need for immediate mandatory reporting. Med Hypotheses. 2004;63(4):609–615. PMID: 15325004. doi:10.1016/j.mehy.2004.04.006
23. Banerjee B, Petersen K. Psychosis following mycoplasma pneumonia. Mil Med. 2009;174(9):1001–1004. PMID: 19780379. doi:10.7205/milmed-d-00-8209
24. Moor S, Skrine H. Psychosis in mycoplasma infection. Postgrad Med J. 1989;65(760):96–97. doi:10.1136/pgmj.65.760.96
25. Ercan TE, Ercan G, Severge B, et al. Mycoplasma pneumoniae infection and obsessive-compulsive disease: a case report. J Child Neurol. 2008;23(3):338–340. PMID: 18079308. doi:10.1177/0883073807308714
26. Becker MA, Cannon J, Certa K. A case of mycoplasma pneumoniae encephalopathy presenting as mania. J Acad Consult Liaison Psychiatry. 2021;62(1):150–154. doi:10.1016/j.psym.2020.02.004
27. Toufexis MD, Hommer R, Gerardi DM, et al. Disordered eating and food restrictions in children with PANDAS/PANS. J Child Adolesc Psychopharmacol. 2015;25(1):48–56. PMID: 25329522; PMCID: PMC4340640. doi:10.1089/cap.2014.0063
28. Piras C, Pintus R, Pruna D, et al. pediatric acute-onset neuropsychiatric syndrome and Mycoplasma Pneumoniae infection: a case report analysis with a metabolomics approach. Curr Pediatr Rev. 2020;16(3):183–193. PMID: 31642785; PMCID: PMC8193809. doi:10.2174/1573396315666191022102925
29. Frankovich J, Thienemann M, Rana S, Chang K. Five youth with pediatric acute-onset neuropsychiatric syndrome of differing etiologies. J Child Adolesc Psychopharmacol. 2015;25(1):31–37. PMID: 25695942; PMCID: PMC4442568. doi:10.1089/cap.2014.0056
30. Miklossy J. Chronic or late Lyme neuroborreliosis: analysis of evidence compared to chronic or late neurosyphilis. Open Neurol J. 2012;6:146–157. doi:10.2174/1874205X01206010146
31. Back T, Grünig S, Winter Y, et al. Neuroborreliosis-associated cerebral vasculitis: long-term outcome and health-related quality of life. J Neurol. 2013;260:1569–1575. doi:10.1007/s00415-013-6831-4
32. Bransfield RC. The psychoimmunology of Lyme/Tick-Borne diseases and its association with neuropsychiatric symptoms. Open Neurol J. 2012;688–693. doi:10.2174/1874205X01206010088
33. Fallon BA, Levin ES, Schweitzer PJ, Hardesty D. Inflammation and central nervous system Lyme disease. Neurobiol Dis. 2010;37(3):534–541. PMID: 19944760. doi:10.1016/j.nbd.2009.11.016
34. Benros ME, Waltoft BL, Nordentoft M, et al. Autoimmune diseases and severe infections as risk factors for mood disorders: a nationwide study. JAMA Psychiatry. 2013;70(8):812–820. doi:10.1001/jamapsychiatry.2013.1111
35. Chang K, Frankovich J, Cooperstock M, et al. PANS Collaborative Consortium. Clinical evaluation of youth with pediatric acute-onset neuropsychiatric syndrome (PANS): recommendations from the 2013 PANS Consensus Conference. J Child Adolesc Psychopharmacol. 2015;25(1):3–13. PMID: 25325534; PMCID: PMC4340805. doi:10.1089/cap.2014.0084
36. Calaprice D, Tona J, Murphy TK. Treatment of pediatric acute-onset neuropsychiatric disorder in a large survey population. J Child Adolesc Psychopharmacol. 2018;28(2):92–103. PMID: 28832181; PMCID: PMC5826468. doi:10.1089/cap.2017.0101
37. Davis AK, Barrett FS, May DG, et al. Effects of psilocybin-assisted therapy on major depressive disorder: a randomized clinical trial. JAMA Psychiatry. 2021;78(5):481–489. PMID: 33146667; PMCID: PMC7643046. doi:10.1001/jamapsychiatry.2020.3285
38. Moreno FA, Wiegand CB, Taitano EK, Delgado PL. Safety, tolerability, and efficacy of psilocybin in 9 patients with obsessive-compulsive disorder. J Clin Psychiatry. 2006;67(11):1735–1740. PMID: 17196053. doi:10.4088/jcp.v67n1110
39. Khan AJ, Bradley E, O’Donovan A, Woolley J. Psilocybin for trauma-related disorders. Curr Top Behav Neurosci. 2022;56:319–332. PMID: 35711024. doi:10.1007/7854_2022_366
40. Bogadi M, Kaštelan S. A potential effect of psilocybin on anxiety in neurotic personality structures in adolescents. Croat Med J. 2021;62(5):528–530. PMID: 34730895; PMCID: PMC8596485. doi:10.3325/cmj.2021.62.528
41. Yu CL, Yang FC, Yang SN, et al. Psilocybin for end-of-life anxiety symptoms: a systematic review and meta-analysis. Psychiatry Investig. 2021;18(10):958–967. PMID: 34619818; PMCID: PMC8542741. doi:10.30773/pi.2021.0209
42. Griffiths RR, Johnson MW, Carducci MA, et al. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: a randomized double-blind trial. J Psychopharmacol. 2016;30(12):1181–1197. PMID: 27909165; PMCID: PMC5367557. doi:10.1177/0269881116675513
43. Johnson MW, Garcia-Romeu A, Cosimano MP, Griffiths RR. Pilot study of the 5-HT2AR agonist psilocybin in the treatment of tobacco addiction. J Psychopharmacol. 2014;28(11):983–992. doi:10.1177/0269881114548296
44. Ling S, Ceban F, Lui LMW, et al. Molecular mechanisms of psilocybin and implications for the treatment of depression. CNS Drugs. 2022;36(1):17–30. PMID: 34791625. doi:10.1007/s40263-021-00877-y
45. Nkadimeng SM, Nabatanzi A, Steinmann CML, Eloff JN. Phytochemical, cytotoxicity, antioxidant and anti-inflammatory effects of psilocybe natalensis magic mushroom. Plants. 2020;9(9):1127. PMID: 32878164; PMCID: PMC7570254. doi:10.3390/plants9091127
46. Nkadimeng SM, Steinmann CML, Eloff JN. Anti-inflammatory effects of four psilocybin-containing magic mushroom water extracts in vitro on 15-lipoxygenase activity and on lipopolysaccharide-induced cyclooxygenase-2 and inflammatory cytokines in human U937 macrophage cells. J Inflamm Res. 2021;14:3729–3738. PMID: 34385833; PMCID: PMC8352634. doi:10.2147/JIR.S317182
47. Kubera M, Maes M, Kenis G, et al. Effects of serotonin and serotonergic agonists and antagonists on the production of tumor necrosis factor alpha and interleukin-6. Psychiatry Res. 2005;134(3):251–258. PMID: 15892984. doi:10.1016/j.psychres.2004.01.014
48. Flanagan TW, Nichols CD. Psychedelics as anti-inflammatory agents. Int Rev Psychiatry. 2018;30(4):363–375. PMID: 30102081. doi:10.1080/09540261.2018.1481827
49. Craft JE, Fischer DK, Shimamoto GT, Steere AC. Antigens of Borrelia burgdorferi recognized during Lyme disease. Appearance of a new immunoglobulin M response and expansion of the immunoglobulin G response late in the illness. J Clin Invest. 1986;78(4):934–939. PMID: 3531237; PMCID: PMC423723. doi:10.1172/JCI112683
50. Steere AC. Lyme arthritis: correlation of serum and cryoglobulin IgM with activity, and serum IgG with remission. Arthritis Rheum. 1979;22(5):471–483. PMID: 109097. doi:10.1002/art.1780220506
51. Owen DC. Is Lyme disease always polymicrobial?--The jigsaw hypothesis. Med Hypotheses. 2006;67(4):860–864. PMID: 16814477. doi:10.1016/j.mehy.2006.03.046
52. Garg K, Meriläinen L, Franz O, et al. Evaluating polymicrobial immune responses in patients suffering from tick-borne diseases. Sci Rep. 2018;8:15932. doi:10.1038/s41598-018-34393-9
53. Berghoff W. Chronic Lyme disease and co-infections: differential diagnosis. Open Neurol J. 2012;6:158–178. PMID: 23400696; PMCID: PMC3565243. doi:10.2174/1874205X01206010158
54. Sinco G, Bergamo S. Impact of co-infections in Lyme disease. Open Dermatol J. 2016;10:255–261. doi:10.2174/1874372201610010055
55. Moutailler S, Valiente Moro C, Vaumourin E, et al. Co-infection of ticks: the rule rather than the exception. PLoS Negl Trop Dis. 2016;10(3):e0004539. PMID: 26986203; PMCID: PMC4795628. doi:10.1371/journal.pntd.0004539
56. Adelson ME, Rao RV, Tilton RC, et al. Prevalence of Borrelia burgdorferi, Bartonella spp., Babesia microti, and Anaplasma phagocytophila in Ixodes scapularis ticks collected in Northern New Jersey. J Clin Microbiol. 2004;42(6):2799–2801. PMID: 15184475; PMCID: PMC427842. doi:10.1128/JCM.42.6.2799-2801.2004
57. Tokarz R, Tagliafierro T, Sameroff S, et al. Microbiome analysis of Ixodes scapularis ticks from New York and Connecticut. Ticks Tick Borne Dis. 2019;10(4):894–900. doi:10.1016/j.ttbdis.2019.04.011
58. Holden K, Boothby J, Kasten R, Chomel B. Co-detection of Bartonella henselae, Borrelia burgdorferi, and Anaplasma phagocytophilum in Ixodes pacificus Ticks from California, USA. Vector Borne Zoonotic Dis. 2006;6:99–102. PMID: 16584332. doi:10.1089/vbz.2006.6.99
59. Saplkoglu Y. Nov 25, 2019. FDA Calls Psychedelic Psilocybin a ‘Breakthrough Therapy’ for Severe Depression. Available from: https://www.livescience.com/psilocybin-depression-breakthrough-therapy.html.
60. Hutten NRPW, Mason NL, Dolder PC, Kuypers KPC. Motives and side-effects of microdosing with psychedelics among users. Int J Neuropsychopharmacol. 2019;22(7):426–434. PMID: 31152167; PMCID: PMC6600464. doi:10.1093/ijnp/pyz029
61. Reddit. Microdosing: sub-threshold dosing of psychedelic drugs for self-improvement, therapy or well-being. Available from: https://www.reddit.com/r/microdosing/.
62. Oilove, M. July 15, 2022. More States May Legalize Psychedelic Mushrooms. Available from: https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2022/07/15/more-states-may-legalize-psychedelic-mushrooms. Accessed February 26, 2023.
63. Rootman JM, Kryskow P, Harvey K, et al. Adults who microdose psychedelics report health related motivations and lower levels of anxiety and depression compared to non-microdosers. Sci Rep. 2021;11(1):22479. PMID: 34795334; PMCID: PMC8602275. doi:10.1038/s41598-021-01811-4
64. Lea T, Amada N, Jungaberle H. Psychedelic microdosing: a subreddit analysis. J Psychoactive Drugs. 2020;52:101–112. doi:10.1080/02791072.2019
65. Lea T, Amada N, Jungaberle H, et al. Perceived outcomes of psychedelic microdosing as self-managed therapies for mental and substance use disorders. Psychopharmacol. 2020;237:1521. doi:10.1007/s00213-020-05477-0
66. Fadiman J. The Psychedelic Explorer’s Guide: Safe, Therapeutic, and Sacred Journeys. New York: Simon and Schuster; 2021.
67. Johnstad PG. Powerful substances in tiny amounts: an interview study of psychedelic microdosing. Nordic Stud Alcohol Drugs. 2018;35(1):39–51. doi:10.1177/1455072517753339
68. Kuypers KPC. The therapeutic potential of microdosing psychedelics in depression. Ther Adv Psychopharmacol. 2020;10:2045125320950567. PMID: 32922736; PMCID: PMC7457631. doi:10.1177/2045125320950567
69. Cameron LP, Nazarian A, Olson DE. Psychedelic microdosing: prevalence and subjective effects. J Psychoactive Drugs. 2020;52:113–122. doi:10.1080/02791072.2020.1718250
70. Polito V, Stevenson RJ. A systematic study of microdosing psychedelics. PLoS One. 2019;14:e0211023. doi:10.1371/journal.pone.0211023
71. Szigeti B, Kartner L, Blemings A, et al. Self-blinding citizen science to explore psychedelic microdosing. Elife. 2021;10(e62878). PMID: 33648632; PMCID: PMC7925122. doi:10.7554/eLife.62878
72. Cavanna F, Muller S, de la Fuente LA, et al. Microdosing with psilocybin mushrooms: a double-blind placebo-controlled study. Transl Psychiatry. 2022;12(307). doi:10.1038/s41398-022-02039-0
73. Coppola M, Bevione F, Mondola R. Psilocybin for treating psychiatric disorders: a psychonaut legend or a promising therapeutic perspective? J Xenobiot. 2022;12(1):41–52. PMID: 35225956; PMCID: PMC8883979. doi:10.3390/jox12010004
74. Hesselgrave N, Troppoli TA, Wulff AB, Cole AB, Thompson SM. Harnessing psilocybin: antidepressant-like behavioral and synaptic actions of psilocybin are independent of 5-HT2R activation in mice. Proc Natl Acad Sci U S A. 2021;118(17):e2022489118. PMID: 33850049; PMCID: PMC8092378. doi:10.1073/pnas.2022489118
75. Vollenweider FX, Vollenweider-Scherpenhuysen MFI, Babler A, et al. Psilocybin induces schizophrenia-like psychosis in humans via serotonin-2 agonist action. Neuroreport. 1998;9:3897–3902. doi:10.1097/00001756-199812010-00024
76. Vollenweider FX, Vontobel P, Hell D, Leenders KL. 5-HAT modulation of dopamine release in basal ganglia in psilocybin-induced psychosis in man-a PET study with [11C] raclopride. Neuropsychopharmacol. 1999;112:424–434. doi:10.1016/S0893-133X(98)00108-0
77. Thompson C, Szabo A. Psychedelics as a novel approach to treating autoimmune conditions. Immunol Lett. 2020;228:45–54. PMID: 33035575. doi:10.1016/j.imlet.2020.10.001
78. Studerus E, Kometer M, Hasler F, Vollenweider FX. Acute, subacute and long-term subjective effects of psilocybin in healthy humans: a pooled analysis of experimental studies. J Psychopharmacol. 2011;25(11):1434–1452. PMID: 20855349. doi:10.1177/0269881110382466
79. Anderson T, Petranker R, Christopher A, et al. Psychedelic microdosing benefits and challenges: an empirical codebook. Harm Reduct J. 2019;16(1):43. PMID: 31288862; PMCID: PMC6617883. doi:10.1186/s12954-019-0308-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.