")
Back to Journals » Journal of Pain Research » Volume 12
The Effect Of The Use Of Pre-Emptive Oral Pregabalin On The Postoperative Spinal Analgesia In Patients Presented For Orthopedic Surgeries: Randomized Controlled Trial
Authors Omara AF , Ahmed SA , Abusabaa MMA
Received 17 May 2019
Accepted for publication 17 September 2019
Published 30 September 2019 Volume 2019:12 Pages 2807—2814
DOI https://doi.org/10.2147/JPR.S216184
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Amany F Omara, Sameh A Ahmed, Motaz MA Abusabaa
Department of Anesthesiology and Surgical Intensive Care, Faculty of Medicine, Tanta University, Tanta 31527, Egypt
Correspondence: Amany F Omara
Department of Anesthesiology and Surgical Intensive Care, Faculty of Medicine, Tanta University, Tanta, Egypt
Tel +20401008372249
Email [email protected]
Background: Preoperative oral pregabalin could improve postoperative analgesia and prevent chronic pain development. The aim of this study is to evaluate the effect of oral pregabalin on the duration and quality of postoperative analgesia in spinal anesthesia.
Methods: Sixty adult patients presented for internal fixation of femoral fracture under spinal anesthesia were included in the study. They were randomly distributed to a placebo group and a pregabalin group receiving 150 mg pregabalin capsules 1 hr before surgery. The onset, duration, and regression of sensory and motor block were recorded. Rescue analgesia consumption, postoperative pain score, and quality of sleep were also assessed.
Results: Oral pregabalin significantly prolonged the time to two-segment regression of sensory block, reaching 86.67±17.88 mins, the time required to regression of spinal block to L2, reaching 155.33± 34.71 mins, and the duration of motor block, reaching 138 ± 23.5 mins, with no effect on the onset of sensory or motor block (P = 0.60 and 0.62). It significantly decreased the VAS score 4 hrs, 6 hrs, and 12 hrs postoperatively, prolonged the duration of postoperative analgesia, reaching 392.00±47.23 mins, and decreased morphine consumption to 7.67±3.65 mg. It also improved the quality of sleep in the first night after surgery.
Conclusion: Preemptive oral pregabalin prolonged the time to the first request for postoperative analgesics and improved sleep in the first night after surgery.
Keywords: pregabalin, orthopedic, spinal, sensory, motor, randomized trial, postoperative analgesia
Introduction
Orthopedic surgeries are frequently associated with moderate-to-severe postoperative pain that can decrease mobility in the immediate postoperative period, interfere with postoperative rehabilitation, and delay hospital discharge. Pain may also become chronic.1
Spinal anesthesia is the most popular anesthesia technique worldwide in orthopedic lower limb surgeries.2 However, its relatively short duration of action may limit the excellent postoperative analgesic effect.3 Thus, many adjuvants had been used to improve postoperative analgesia and decrease consumption of postoperative analgesics.4
Pregabalin, the gamma amino-butyric acid analogue, is commonly used in the treatment of epilepsy and neuropathic pain. Preoperative administration of oral pregabalin was evaluated by Clarke et al and found to improve the postoperative analgesic effect and decrease postoperative opioid consumption.5 Godrat found that preemptive pregabalin in an oral dose of 150 mg offers good postoperative analgesia in lower limb orthopedic surgeries under spinal anesthesia.6 Furthermore, Reuben et al also showed that effective multi-modal analgesia prevents the development of chronic pain.7
The anti-nociceptive effect of preemptive analgesia develops by preventing the development of triggering hyperplastic changes at the surgical site in response to a noxious stimulus. It also has a central neural desensitization effect that may prevent the amplification of future impulses at the surgical site.8,9
This randomized study assumed that preemptive oral pregabalin may alter the postoperative analgesic characteristics of subarachnoid anesthesia. The aim of this clinical trial was to assess the effect of preemptive oral pregabalin (150 mg) on the duration and quality of postoperative analgesia in spinal anesthesia in patients with femoral fracture presented for an internal fixation. Time to the first request for rescue analgesia was the primary outcome.
Patients And Methods
This prospective controlled randomized double-blind study was conducted at the Orthopedic Department. It started in November 2017 and lasted for 6 months. After approval of the study by the research ethics committee (Tanta Faculty of Medicine Research Ethics Committee with approval code 31821/10/17), it was registered in the Pan African Clinical Trial Registry with registration number PACTR201711002742202. The trial was conducted in accordance with the Declaration of Helsinki.
Patients aged from 25 to 50 years of both genders, American Society of Anesthesiologists physical status I or II (ASA I: normal healthy patient, ASA II: patient with mild systemic disease), and presented for internal fixation of traumatic femoral fracture were included.
Preoperative assessment was carried out for all patients. Patient history was collected, examination was performed, and routine investigations were requested. Adequate explanation of the technique and purpose, advantage, and potential risk was delivered to all patients. They were then reassured and asked for informed written consent upon accepting to participate. All obtained data and results about participating patients were kept in private files and used for the current study only.
Patients who refused to participate; those with known or suspected coagulopathy, body mass index (BMI) above 30 kg/m2 or less than 18 kg/m2, local skin infection, history of hypersensitivity to pregabalin, or long-term opioid use; and those receiving regular doses of non-steroidal anti-inflammatory drugs or antiplatelets were excluded. The hospital pharmacy prepared placebo capsules and 150 mg pregabalin capsules. Capsules were introduced to patients in closed sealed envelopes by an anesthesia resident not participating in the study. The patients and the assessors were thus blind to the technique.
Patients were randomly allocated by computer-generated software (Random Allocation Software). Group A (placebo group) received the previously prepared placebo capsules 1 hr before surgery. Group B (pregabalin group) received 150 mg oral capsules of pregabalin 1 hr before surgery.
In the operating theatre, intravascular access was established by an 18-gauge peripheral venous cannula. Then, 7 mL/kg of lactated ringer solution was infused over 20 mins, as a preload. Once admitted to the operating room, patients were closely monitored using a pulse oximeter, non-invasive blood pressure monitor, and three-lead electrocardiogram.
Under complete aseptic conditions and in lateral position, the line connecting the two iliac crests (Tuffier’s line) was identified to detect the level of L3-L4 or L4-L5 inter-vertebral space. Three milliliters of lidocaine 2% were infiltrated at midline at the level space for local anesthesia. Spinal anesthesia was performed via midline approach using a 23-gauge sharp tip spinal needle, injecting 2.5 mL of hyperbaric bupivacaine (0.5%). The patients were then turned to supine position, with 15-degree head elevation. They were left in this position for 20 mins, during which hemodynamic parameters were closely monitored and sensory and motor block criteria assessed. Hemodynamic parameters were monitored every 3 mins during the first 30 mins after spinal anesthesia. Patients who showed a decrease in mean arterial pressure to less than 65 mmHg received intravenous ephedrine 5 mg. Those who showed a decrease in heart rate to less than 50 beats/min received atropine 0.5 mg intravenously.
Measurements
An assistant nurse not participating in the study helped in intraoperative and postoperative measurements. The surgeon was blinded to the patients’ group and did not participate in taking measurements.
Sensory block was assessed using pinprick test by a 26-gauge needle from caudal to cephalic direction on both sides, every minute, until the maximal sensory level was reached. This was repeated every 15 mins till two-segment regression of the sensory level. The sensory level should at least reach the 10th thoracic segment (T10). If not, the patient was excluded from the study.
The onset of sensory block was recorded to be the elapsed time between subarachnoid injection and reaching the sensory level of T10. Time to regression of sensory block was calculated to be the time interval between reaching the highest sensory level and two-segment regression of this level (like regression of sensory block from T8 to T10). The time interval between reaching the maximal sensory level and the level of the 2nd lumbar segment (L2) was also calculated and recorded (time to regression to L2).
Modified Bromage score10 was used to evaluate motor block (grade 3: no movement, grade 2: unable to flex knees but can flex ankle, grade 1: unable to raise an extended leg but able to move the knees and ankles, and grade 0: no paralysis). The onset of motor block represented the time interval between performing spinal anesthesia and reaching a Bromage score of 1. Bromage score was assessed postoperatively in the healthy limb till a score of 0 was reached. The duration of motor block was estimated to be the elapsed time between reaching the highest motor block score and regression of the motor score to 0.
During the postoperative period, all patients received 1000 mg paracetamol intravenously every 6 hrs as routine analgesia, according to local hospital policy. The visual analogue score (VAS) (score for assessment of the severity of pain with a 0–10 metric, where 0 = no pain and 10 = severe pain) was used to evaluate postoperative analgesia immediately after surgery, every 2 hrs for the first 6 hrs, and then every 6 hrs up to 24 hrs. Whenever VAS exceeded 4, 4 mg morphine was administered intravenously as rescue analgesia (according to local hospital policy), which could be repeated with a calculation of the time to the first request for rescue analgesia after surgery and quality of postoperative analgesia. The incidence of other postoperative complications was recorded, such as pruritus, drowsiness, nausea and vomiting, or urine retention.
Quality of sleep on the first night after surgery and 1 week later was determined by the patients to be very good, good, fair, bad, or very bad. Sleep was assessed using the Consensus Sleep Diary,11 a tool for gathering information about the quality of sleep. The sleep diary was explained to the patients in the preoperative period. They were asked to fill in the self-assessment questionnaire preoperatively, on the night following the surgery, and one week later, to be able to rate their sleep quality.
Statistical Analysis
A pilot study was conducted on 10 patients not included in the final study and undergoing internal fixation of femoral fracture under spinal anesthesia. The patients were randomly divided into two groups (five each).
The time to the first request for rescue analgesia was significantly prolonged from 208.8 ± 44.4 mins to 399.1 ± 98.2 mins with the preemptive administration of oral pregabalin. At least 27 patients were required in each group to detect prolongation of the time to the first request of rescue analgesia by 90 mins at an α value of 0.05 and 90% power of study. The statistically analyzed data were presented as mean and standard deviation or as a number and percent. Non-parametric data were analyzed by Fisher’s exact test, while numerical data were analyzed by unpaired T-test. Mann–Whitney test was used for the statistical evaluation of the postoperative visual analogue score and the Consensus Sleep Diary. Levels were considered significant whenever the P value was less than 0.05. The computer program SPSS (SPSS Inc., Chicago, IL, USA) was used for statistical analysis of the collected data.
Results
In total, 79 patients were thought to be eligible for the study. However, 19 were excluded due to refusal to participate (8 patients) or not meeting the inclusion criteria (11 patients; five diagnosed with coagulopathy, three morbidly obese, two receiving antiplatelet therapy, and one on routine nonsteroidal anti-inflammatory drugs).
The remaining 60 patients were randomly allocated into two equal groups. No patients were excluded as a result of failure of spinal anesthesia to reach the level of T10. Data of all patients were successfully collected (Figure 1).
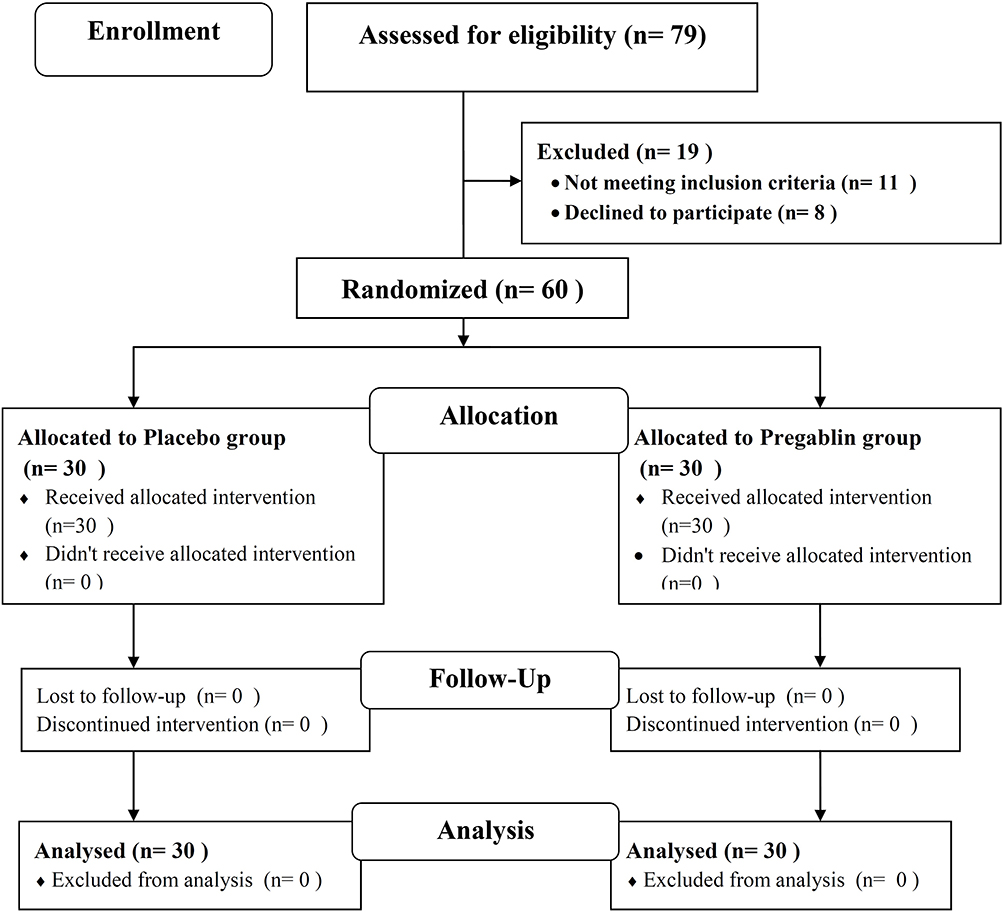 |
Figure 1 CONSORT flow chart of the study. |
Patients’ characteristics, including age, gender, body weight, and American Society of Anesthesiologists physical status, were comparable between the two groups. Differences in the type and duration of surgery between the two groups were statistically insignificant (Table 1).
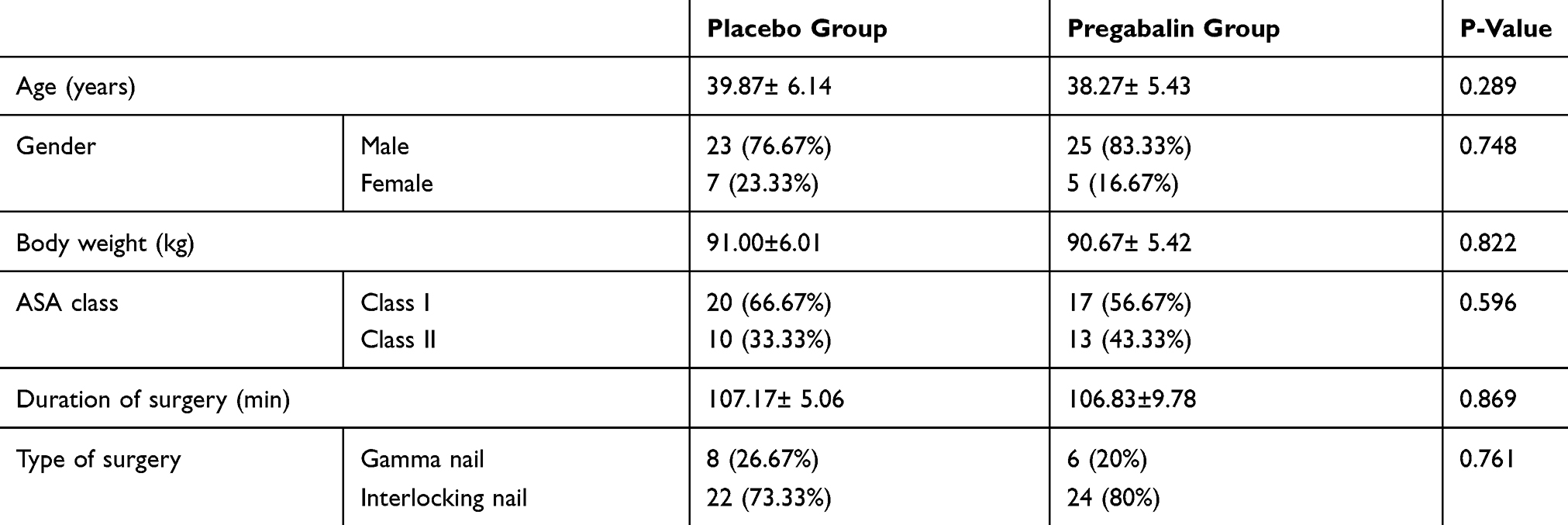 |
Table 1 Demographic Data In The Studied Groups |
The time to the first request for rescue analgesia (primary outcome) was significantly longer in the pregabalin group than in the placebo group (P = 0.0001). The total dose consumed of morphine was significantly lower in the pregabalin group than in the placebo group (P = 0.003) (Table 2).
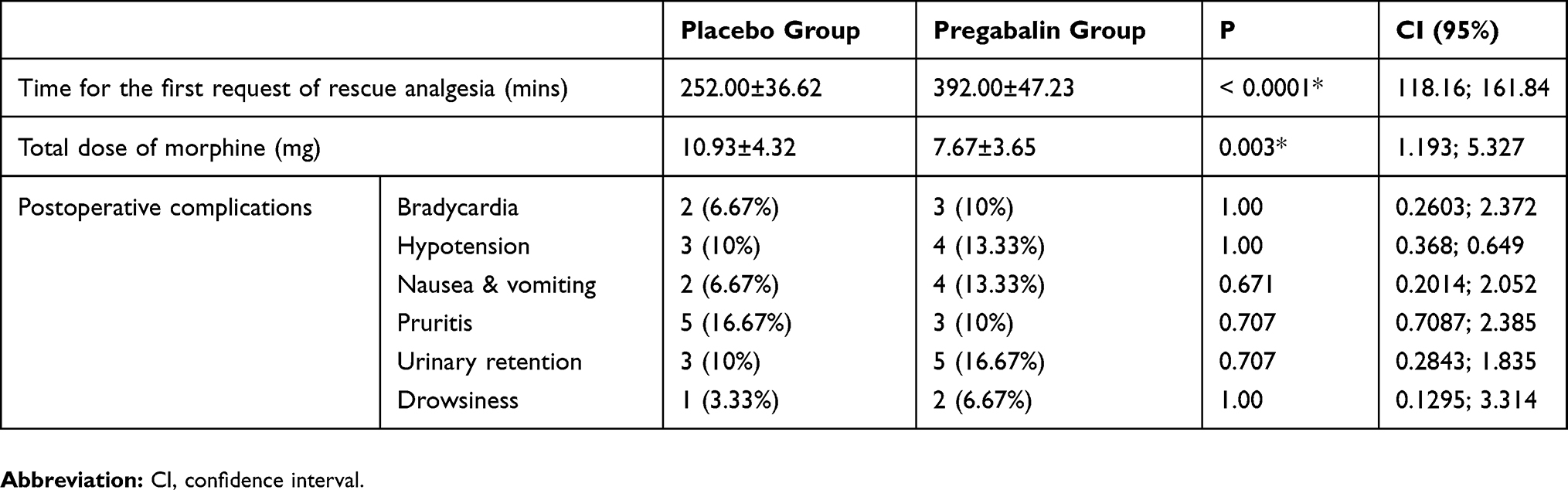 |
Table 2 Postoperative Criteria In The Two Studied Groups |
VAS scores were significantly lower 4, 6, and 12 hrs after surgery in the pregabalin group than in the placebo group (P = 0.0002, 0.0001, and 0.0004, respectively). However, it was comparable between the two groups in the immediate postoperative period and 2 hrs, 18 hrs, and 24 hrs postoperatively (P = 0.431, 0.363, 0.273, 0.476, respectively) (Table 3).
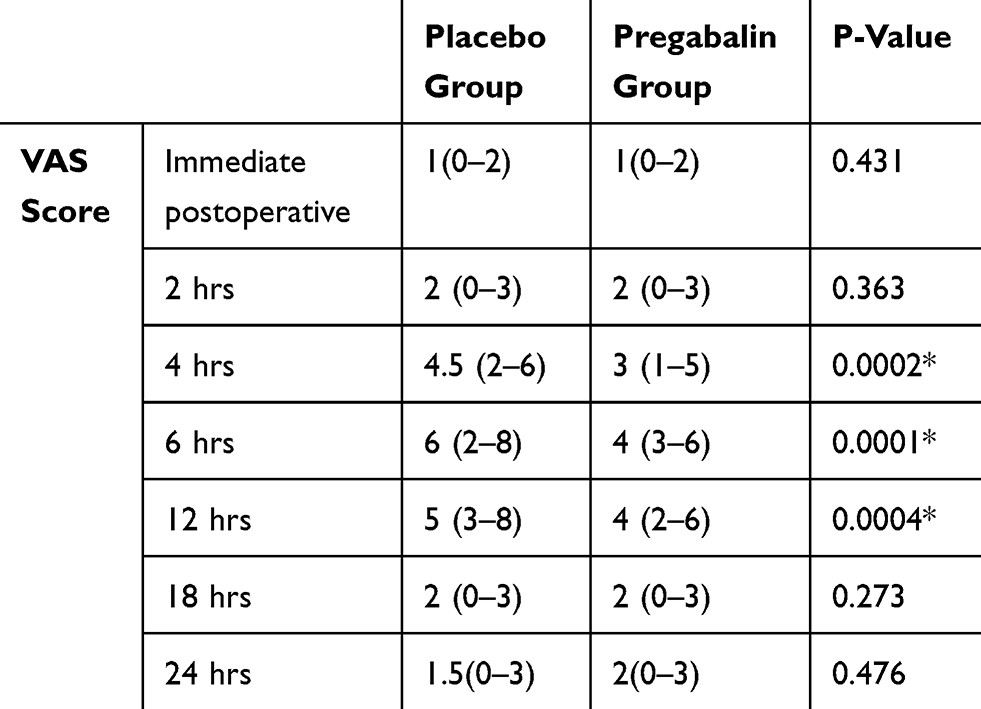 |
Table 3 Postoperative VAS Score In The Two Groups |
The use of oral pregabalin did not significantly change the onset of sensory block (P = 0.602) (4.6 ± 1.7 mins) or the onset of motor block (P = 0.620) (6.3 ± 2.4 mins) of spinal anesthesia as compared to the placebo group (4.8 ± 1.7 mins and 6.6 ± 2.3 mins, respectively). However, there was statistically significant prolongation in the time required to two-segment regression of the sensory level, from 72.3 ± 16.5 mins in the placebo group to 86.7 ± 17.9 mins in the pregabalin group (P = 0.002), and the time required to regression of the sensory level till the level of L2, from 134.7 ± 32 mins in the placebo group to 155.3 ± 34.7 mins in the pregabalin group (P = 0.012). The duration of the motor block was also significantly prolonged in the pregabalin group (138 ± 23.5 mins) compared to the placebo group (123.3 ± 16.9 mins) (P = 0.007) (Table 4).
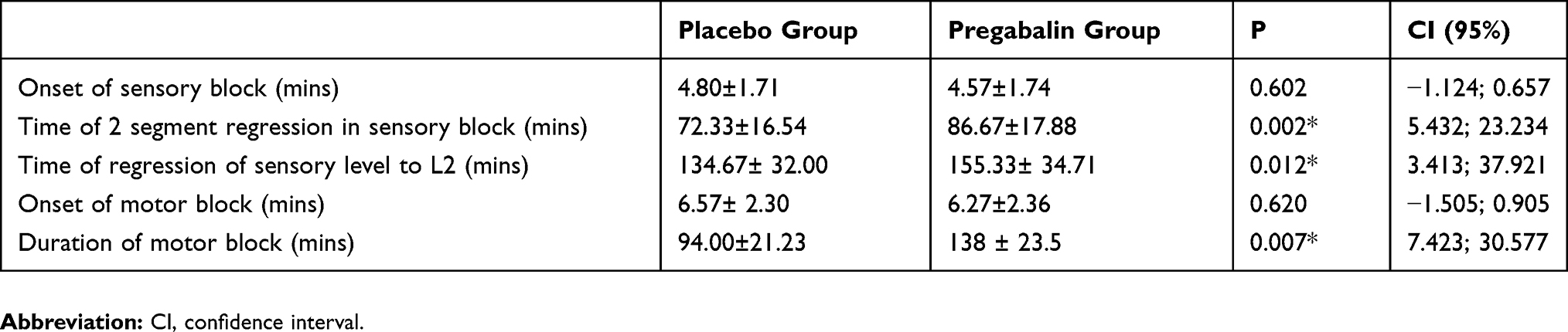 |
Table 4 Sensory And Motor Criteria Of The Spinal Anesthesia In The Studied Groups |
Patients in the pregabalin group showed a significantly better quality of sleep on the first night after surgery than patients in the placebo group (P ˂ 0.001). However, quality of sleep 1 week after surgery was comparable between the two groups (Figure 2). The incidence of postoperative complications, including bradycardia, hypotension, nausea and vomiting, pruritus, urinary retention, and drowsiness, was not significantly higher in one group than the other (P = 1.00, 1.00, 0.671, 0.707, 0.707, and 1.00) (Table 2).
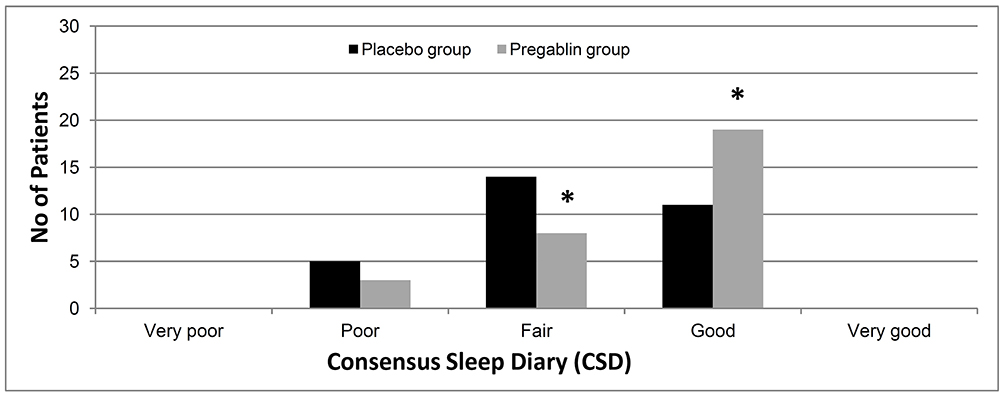 |
Figure 2 The consensus sleep diary of the first night in the two groups. Data were presented as patients number. *Denotes significant change. |
Discussion
The results of this clinical study reveal that oral pregabalin administered an hour before subarachnoid bupivacaine anesthesia significantly alters sensory and motor block characteristics. Its use was associated with significant prolongation in the time to two-segment regression of sensory blockade, an increase in the time to regression of the sensory level to L2, prolongation in the duration of sensory and motor blockade, improvement in the score of postoperative analgesia, and a decrease in the consumption of postoperative analgesics. However, there was an insignificant change in the onset of sensory and motor block. Oral administration of pregabalin improved quality of sleep in the night following surgery, without a significant increase in the incidence of complications.
The mechanism by which premedication using gabapentinoid compounds can affect the sensory and motor block characteristics of subarachnoid anesthesia is not quite obvious. These compounds are r-aminobutyric acid analogs that can bind to the a2-d subunit of the presynaptic voltage-gated calcium channels. This leads to a decrease in potassium-evoked excitatory transmitter release, which decreases postsynaptic excitability. They also exert a modulating effect on GABA neurotransmission and calcium influx.12,13 Gabapentinoid compounds have an anxiolytic, antiepileptic, and analgesic effect. These compounds significantly improve preoperative anxiety scores and have euphorigenic effects that may be useful.13,14
Many published trials evaluate the effect of preemptive oral gabapentinoid compounds with regional anesthesia. However, results are conflicting.
There is no universally accepted dose or regimen of preemptive gabapentinoids. The time of administration, the frequency, the indications, and the pitfalls are also not well established. The systematic review of Tiippana et al reveals the effectiveness of gabapentinoids in reducing the degree of postoperative pain and opioid consumption. However, the trials were heterogenous and could not determine the optimal dose or duration of treatment.15
Buvanendran et al16 conducted a study that assessed the effect of oral administration of 300 mg pregabalin preoperatively on continuous spinal anesthesia in patients presented for total knee replacement. They found that the central nervous system (CSF) concentration of pregabalin after 6 hrs was high enough to reduce the hypersensitivity of the CNS. The median time of the peak concentration of pregabalin in cerebrospinal fluid (CSF) was 8 hrs.
Bafna et al17 studied 90 adult patients undergoing gynecological surgeries under spinal anesthesia. The patients were randomly classified into 3 groups: a placebo group, where patients received identical placebo capsules, a gabapentin group, where patients received 600 mg oral gabapentin, and a pregabalin group, where patients received 150 mg oral pregabalin. They showed that the oral use of either pregabalin or gabapentin prolonged the mean duration of effective analgesia of spinal bupivacaine block, prolonged the mean duration of motor block, and improved postoperative analgesia without a significant increase in the incidence of side effects or complications. Pregabalin showed a significantly longer duration of effective analgesia than gabapentin.
Cegin et al13 evaluated the effect of preemptive oral administration of different doses of pregabalin (75, 150, or 300 mg) on sensory and motor block characteristics of infraclavicular nerve block. They showed a significant prolongation of sensory and motor blockade with the use of pregabalin. However, they found that oral pregabalin decreased the onset of sensory and motor block.
Moreover, Park et al18 evaluated the effect of oral pregabalin on the intrathecal block in 44 patients presented for urogenital surgeries. They suggested that 150 mg oral pregabalin administrated 2 hrs preoperatively improved the duration of sensory and motor block, with a significant decrease in postoperative pain and request for analgesia.
On the contrary, Short et al19 did not observe any significant difference in postoperative analgesia after cesarean section delivery with the use of oral gabapentin, either 300 mg or 600 mg. Monks et al20 did not reveal better postoperative pain scores in cesarean section delivery under spinal anesthesia with the preemptive oral intake of 600 mg gabapentin. The use of gabapentin instead of pregabalin may explain the difference between their results and the results of the current study. Moreover, increased perioperative anxiety in the parturient presented for cesarean section delivery may limit the anxiolytic effect of gabapentinoid, which may be responsible for its analgesic effect. Multimodal analgesia used in this study may also be a factor causing the indifference in postoperative analgesia.
The use of a single dose regimen of pregabalin (150 mg twice) was a limitation in this study, as it caused lack of comparison with other dose regimens of pregabalin (75 and 300 mg). Moreover, preoperative pain or anxiety was not assessed and recorded. Pregabalin can affect patients’ mood and anxiety scores.
Conclusion
It can be concluded that 150 mg pregabalin orally administered 1 hr before spinal anesthesia in patients undergoing orthopedic surgery was effective in delaying the first request for postoperative analgesics and decreasing postoperative pain. In addition, it was associated with prolongated duration of sensory and motor block and improvement in sleep quality in the first night after surgery. It had no effect on the onset of sensory or motor block, nor the incidence of complications.
Data Sharing
The authors do not intend to share individual deidentified participant data. No specific data or study-related document will be shared. Only the mentioned data in the manuscript will be available.
Disclosure
The authors declare no competing interests in this work.
References
1. Rathmell JP, Wu CL, Sinatra RS, et al. Acute post-surgical pain management: a critical appraisal of current practice. Reg Anesth Pain Med. 2006;31(4):1–42. doi:10.1016/j.rapm.2006.05.002
2. Arcioni R, Palmisani S, Tigano S, et al. Combined intrathecal and epidural magnesium sulfate supplementation of spinal anesthesia to reduce post‐operative analgesic requirements: a prospective, randomized, double‐blind, controlled trial in patients undergoing major orthopedic surgery. Acta Anaesthesiol Scand. 2007;51(4):482–489. doi:10.1111/j.1399-6576.2007.01263.x
3. Liu SS, Strodtbeck WM, Richman JM, Wu CL. A comparison of regional versus general anesthesia for ambulatory anesthesia: a meta-analysis of randomized controlled trials. Anesth Analg. 2005;101(6):1634–1642. doi:10.1213/01.ANE.0000180829.70036.4F
4. Kaya FN, Yavascaoglu B, Turker G, et al. Intravenous dexmedetomidine, but not midazolam, prolongs bupivacaine spinal anesthesia. Can J Anaesth. 2010;57(1):39–45. doi:10.1007/s12630-009-9231-6
5. Clarke H, Pagé GM, McCartney CJL, et al. Pregabalin reduces postoperative opioid consumption and pain for 1 week after hospital discharge, but does not affect function at 6 weeks or 3 months after total hip arthroplasty. Br J Anaesth. 2015;115(6):903–911. doi:10.1093/bja/aev363
6. Akhavanakbari G, Entezariasl M, Isazadehfar K, Mirzarahimi T. The effects of oral pregabalin on post-operative pain of lower limb orthopedic surgery: a double-blind, placebo-controlled trial. Perspect Clin Res. 2013;4(3):165–168. doi:10.4103/2229-3485.115376
7. Reuben SS, Buvanendran A. Preventing the development of chronic pain after orthopaedic surgery with preventive multimodal analgesic techniques. J Bone Joint Surg Am. 2007;89(6):1343–1358. doi:10.2106/00004623-200706000-00025
8. Katz J, Clarke H, Seltzer ZE. Preventive analgesia: quo vadimus? Anesth Analg. 2011;113(5):1242–1253. doi:10.1213/ANE.0b013e31822c9a59
9. Basavareddy A, Meher B, Rajendran I, Srinivasan S. Prospective, randomised, double blinded controlled trial of gabapentin and pregabalin as pre emptive analgesia in patients undergoing lower abdominal and limb surgery under spinal anaesthesia. Indian J Pain. 2014;28(3):155–159. doi:10.4103/0970-5333.138450
10. Graham A, McClure J. Quantitative assessment of motor block in labouring women receiving epidural analgesia. Anaesthesia. 2001;56(5):470–476. doi:10.1046/j.1365-2044.2001.01524-6.x
11. Carney CE, Buysse DJ, Ancoli-Israel S, et al. The consensus sleep diary: standardizing prospective sleep self-monitoring. Sleep. 2012;35(2):287–302. doi:10.5665/sleep.1642
12. Ben-Menachem E. Pregabalin pharmacology and its relevance to clinical practice. Epilepsia. 2004;45(s6):13–18. doi:10.1111/j.0013-9580.2004.455003.x
13. Cegin M, Soyoral L, Yuzkat N, Baydi V, Goktas U. Pregabalin administered as an anxiolytic agent in ultrasound-guided infraclavicular block: a controlled, double-blind, dose-ranging trial. Eur Rev Med Pharmacol Sci. 2016;20(3):568–574.
14. Shimony N, Amit U, Minz B, et al. Perioperative pregabalin for reducing pain, analgesic consumption, and anxiety and enhancing sleep quality in elective neurosurgical patients: a prospective, randomized, double-blind, and controlled clinical study. J Neurosurg. 2016;125(6):1513–1522. doi:10.3171/2015.10.JNS151516
15. Tiippana EM, Hamunen K, Kontinen VK, Kalso E. Do surgical patients benefit from perioperative gabapentin/pregabalin? A systematic review of efficacy and safety. Anesth Analg. 2007;104(6):1545–1556. doi:10.1213/01.ane.0000261517.27532.80
16. Buvanendran A, Kroin JS, Kari M, Tuman KJ. Can a single dose of 300 mg of pregabalin reach acute antihyperalgesic levels in the central nervous system? Reg Anesth Pain Med. 2010;35(6):535–538. doi:10.1097/AAP.0b013e3181fa6b7a
17. Bafna U, Rajarajeshwaran K, Khandelwal M, Verma A. A comparison of effect of preemptive use of oral gabapentin and pregabalin for acute post-operative pain after surgery under spinal anesthesia. J Anaesthesiol Clin Pharmacol. 2014;30(3):373. doi:10.4103/0970-9185.137270
18. Park M, Jeon Y. Preoperative pregabalin prolongs duration of spinal anesthesia and reduces early postoperative pain: a double-blind, randomized clinical CONSORT study. Medicine. 2016;95(36). doi:10.1097/MD.0000000000004864
19. Short J, Downey K, Bernstein P, Shah V, Carvalho JCA. A single preoperative dose of gabapentin does not improve postcesarean delivery pain management: a randomized, double-blind, placebo-controlled dose-finding trial. Surv Anesthesiol. 2013;57(4):186–187. doi:10.1097/01.sa.0000431212.11836.26
20. Monks DT, Hoppe DW, Downey K, Shah V, Bernstein P, Carvalho JCA. A perioperative course of gabapentin does not produce a clinically meaningful improvement in analgesia after cesarean delivery. A randomized controlled trial. Anesthesiology. 2015;123(2):320–326. doi:10.1097/ALN.0000000000000722
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.