")
Back to Journals » Clinical Interventions in Aging » Volume 13
The effect of religious intervention on depressive symptoms and quality of life among Indonesian elderly in nursing homes: A quasi-experimental study
Authors Pramesona BA , Taneepanichskul S
Received 18 January 2018
Accepted for publication 16 February 2018
Published 23 March 2018 Volume 2018:13 Pages 473—483
DOI https://doi.org/10.2147/CIA.S162946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Bayu Anggileo Pramesona,1,2 Surasak Taneepanichskul1
1College of Public Health Sciences, Chulalongkorn University, Bangkok, Thailand; 2Mayjend HM Ryacudu General Hospital, Kotabumi, North Lampung, Indonesia
Purpose: This study aimed to investigate the effect of religious intervention on depressive symptoms and quality of life (QOL) among Indonesian elderly in nursing homes (NHs).
Patients and methods: This was a quasi-experimental study with repeated measures. Sixty elderly residents at three NHs in three districts in Yogyakarta, Indonesia, with the Geriatric Depression Scale (GDS) score of 5–11 were recruited and purposively assigned to the religious intervention group (combining 36 sessions of listening to Qur’anic recital and 3 sessions of attending a sermon by a preacher, n=30) and the control group (treatment as usual/TAU, n=30). The primary outcome was depression, measured by a short form GDS questionnaire. The QOL as the secondary outcome was assessed by the World Health Organization Quality of Life (WHOQOL)-BREF Indonesian version. Both groups were evaluated at the baseline, 4th, 8th, and 12th week after the interventions were performed.
Results: In both groups, there were statistically significant reductions in depression scores after the 12-week intervention (P<0.001). There was also a statistically significant improvement in QOL mean scores in both intervention and control groups at the 12-week post-intervention. However, the religious intervention group showed a greater decrease in depressive symptoms and a greater improvement in the QOL mean scores than those in the control group. There was a statistically significant difference in geriatric depression and QOL mean scores between groups at the 4th, 8th, and 12th week post-interventions.
Conclusions: It can be concluded that religious-based intervention has a greater impact on relieving depressive symptoms and increasing the QOL amongst elderly NH residents.
Keywords: geriatric depression, Indonesia, nursing home, quality of life, Qur’anic recital intervention, religious leader approach
Introduction
Population ageing is a worldwide issue, with around 22% of the total population projected to be aged ≥60 years in 2050.1 Indonesia is ranked as a nation with the eighth largest elderly population globally2 and was at third position amongst 25 Asia-Pacific countries in 2015.3 The prevalence of geriatric depression in Indonesia ranges between 7.2% and 33.8% in the community-dwelling settings.4,5
Depression is one of the most serious mental health disorders in older adults.1 It has an increasing impact on relatives and social dependence, healthcare services utilization,6,7 morbidity and mortality,8 risk of being hospitalized,9,10 and eventually erodes the quality of life (QOL) of older adults.11 Previous study revealed that the depressed elderly had a lower QOL compared to those with many other chronic medical disorders.12 Given these serious consequences, the World Health Organization (WHO) campaigned to focus on depression as a highlighted topic for the 2017 World Health Day.13
In addition, prevalence rates of depression both major, minor, and subsyndromal depressive symptoms, were found to be higher amongst nursing home (NH) residents than community dwellers.14 This mental health disorder is prevalent in NHs even though some evidence-based studies related prevention and treatment for depression have been provided.15,16 NH settings still present implementation challenges due to the special characteristics in this vulnerable population and confine evidence-based treatment utilization to the residents.16 Some psychological and behavioral alterations that correspond to depressive symptoms have been found such as loss of appetite, sleep disturbance, exsiccated libido, and psychomotor alterations.17 Thus, an applicable depression treatment should be initiated to overcome this mental health problem in these particular settings and subjects.
Some specific consequences of geriatric depression include an increased cognitive impairment and an increased burden both on residents and on NH staff who provide the care.18 Since medication-based treatment for depression was effective for relieving the symptoms of 60% of subjects,19 and has minimal effect for those who have mild and moderate depression,20 solid evidence emphasized the effectiveness of an integrated religion/spirituality approach for depression treatment.21
Previous evidence has further indicated that faith-based interventions were effective in preventing and treating depression and improving QOL.22,23 Furthermore, the effect of depression treatment will be more feasible when involving the values and beliefs into intervention in certain populations.24 Subjects from Muslim backgrounds show the greatest agreement compared to the other religious groups when considering the option of a religious approach to treat depression.25 However, evidence about the kind of methods used by Muslims as part of their spiritual coping methods in order to relieve depressive symptoms and improve the QOL is lacking. Hence, we tried to combine Qur’anic recital listening and preacher approach as a type of religious intervention for depressed elderly NH residents. This study aimed to investigate the effect of religious intervention on depressive symptoms and QOL amongst Indonesian elderly in an NH setting.
Patients and methods
Sample size, study design, and procedure
This study was a quasi-experimental study with repeated measures. Following a G-Power program, the required sample for each group was 30 (the total sample was 60), which could achieve 80% power at a 5% level of significance.26 All 273 elderly residents at 3 NHs in 3 districts in Yogyakarta province, Indonesia, were invited to participate. To be an eligible respondent, residents had to be aged 60 years and above, had to have a Geriatric Depression Scale (GDS) score in the range of 5–11 (presenting with mild to moderate levels of depression), could have, or not have any chronic diseases, and had to be living in an NH for at least one month. In all, 77 residents were eligible. Exclusions from this study included one resident who refused to participate, one bedridden patient suffering from severe physical health conditions, and 15 non-Muslim elderly NH residents who were ineligible for the purposes of this study. Thus, data for this study came from 60 elderly NH residents with complete GDS and QOL measurements at the baseline examination. These 60 elderly were purposively assigned into the religious intervention group (n=30) and the control group (n=30) (Figure 1).
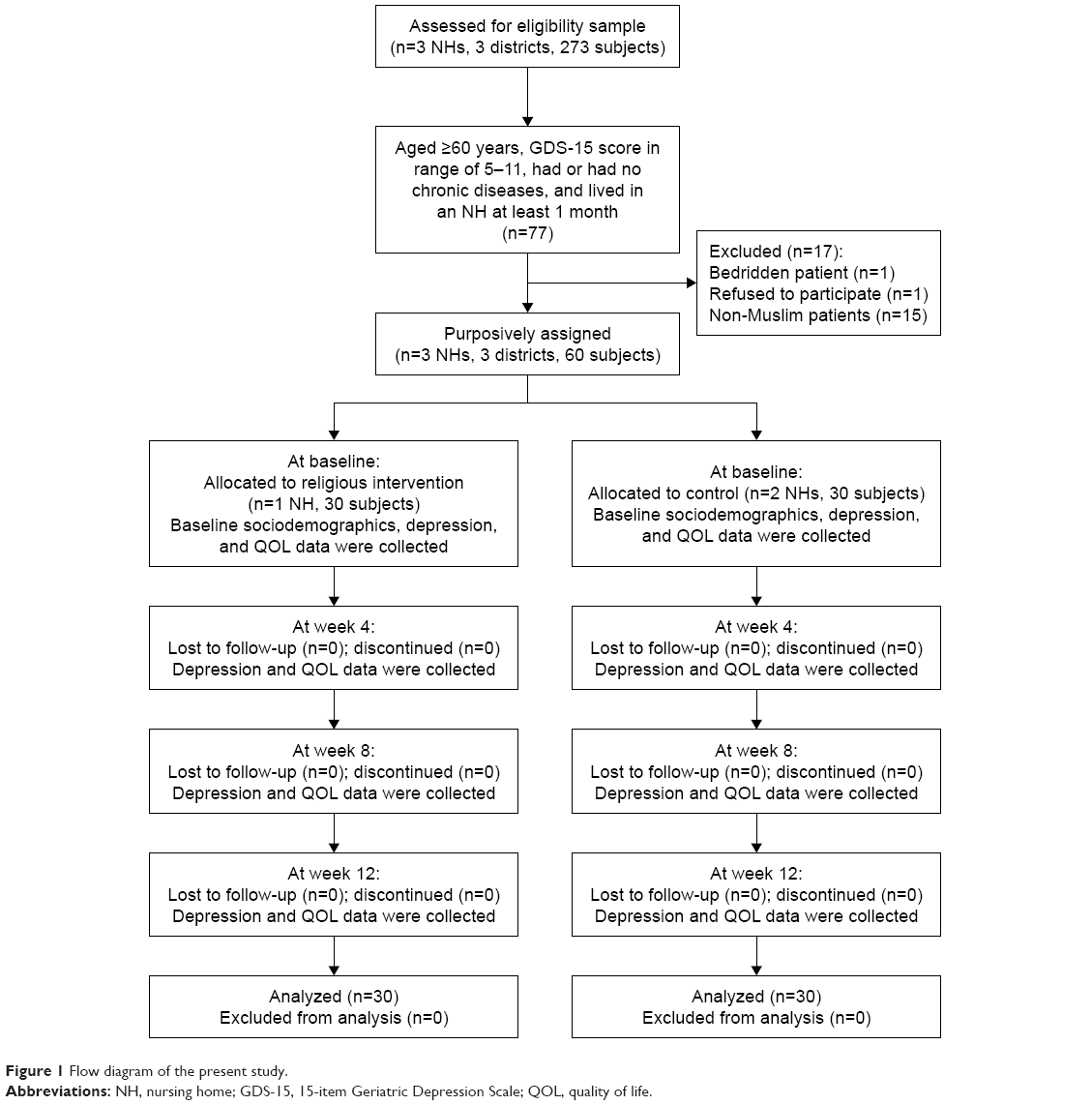 | Figure 1 Flow diagram of the present study. |
Respondents in the intervention group participated in the religious intervention which was a combination of 36 sessions of listening to Qur’anic recital plus 3 sessions of attending a sermon by a Muslim religious leader/preacher. Besides following the preachers’ advice as guidance is highly recommended, belief in the Qur’an as the final revelation book of Allah (God) is the third pillar of Iman (belief) in Islam which is compulsory for Muslims. The Qur’anic recital listening and preaching were chosen purposively over other Muslim spiritual practices due to the beneficial effects of these approaches being rarely investigated amongst the elderly NH residents. Furthermore, the Qur’anic recital listening and preaching sessions were deemed to be more feasibly implemented amongst this specific population.
Both interventions were completed within 12 weeks. Qur’anic recitation/listening sessions were scheduled 3 times a week, lasting between 20 and 25 min per session, using earphones with an MP3 player. 6,236 verses from 114 surah (chapters) in the Qur’an were randomly chosen for each session. The subjects were allowed to ask the researcher to control the MP3 at a comfortable volume and to choose the most comfortable place to listen to the Qur’anic recital, for example, in their bedroom, living room, or on the terrace. The researcher would stay with the subjects during intervention so that the researcher could be available for any unexpected responses.
Monthly sermons relating to depression and QOL from an Islamic perspective were delivered by a preacher for 50–60 min sessions. All subjects were gathered in one place during the intervention. The topics of the preacher’s sermons included themes such as the causes, signs and symptoms of depression, and how to prevent it according to Islamic perspectives, while lessons in reducing depression symptoms and increasing QOL amongst the elderly, based on Islamic perspectives were delivered through an LCD projector with PowerPoint. The sermons’ content was built and derived from Qur’an verses, then discussed together between researcher and preacher to ensure that the objective of this study had been addressed. The preacher selected to deliver the sermons for the purposes of this study was a Muslim religious leader recognized by the community and also a licensed psychiatric nurse.
Respondents in the control group were engaged in daily routine activities such as praying, watching television, counselling, and playing or listening to music. All the data collection, including the administration, intervention, and collecting of data, was carried out by the researcher.
Measurements
Sociodemographic variables
These included age, gender, marital status, education level, length of stay in the NH, social support resources, type of support, physical illness, reason for living in the NH, and perceived adequacy of care. Data gathering was completed through face-to-face interviews, lasting between 30 and 45 min for each respondent and considered as baseline information for all subjects.
Depressive symptoms
The primary outcome was depression (scores and levels), as measured by a short form GDS questionnaire comprising 15 questions that have been tested and extensively used in community, clinical, and NH settings amongst the older population.27–29 The English version of the GDS questionnaire was translated into Bahasa Indonesia. Forward-translations and panel back-translation from three experts were employed. Pearson’s correlation items total score was significant at 0.05 level (P-value <0.05) with Content Validity Index for Items (I-CVI) computation at 1.00. In terms of internal consistency, it was found that the Cronbach’s alpha for the Indonesian version of the GDS questionnaire was good (Cronbach’s alpha=0.80).
The 15-item questionnaire required participants to respond by answering yes or no in reference to how they felt over the past week. Of the 15 items, 10 indicated the presence of depression when answering positively, while the rest (question numbers 1, 5, 7, 11, 13) indicated depression when answering negatively. Scores of 0–4 are considered normal; 5–8 indicate mild depression; 9–11 indicate moderate depression; and 12–15 indicate severe depression.27 The questionnaire took 5–7 min to complete. A cut-off score of 5 was used to distinguish between presence of depression and non-depression.
Quality of life measurement
The QOL as the secondary outcome was assessed by the World Health Organization Quality of Life (WHOQOL)-BREF Indonesian version which consisted of 26 items, and consisted of four domains: physical health, psychological, social relationships, and environment. The Cronbach’s alpha value for each domain of this questionnaire ranges between 0.41 and 0.77, while the Pearson correlation coefficient ranges between 0.5 and 0.7.30 Analyses of internal consistency, item-total correlations, discriminant validity and construct validity through confirmatory factor analysis, indicated that the WHOQOL-BREF has good-to-excellent psychometric properties of reliability and performed well in preliminary tests of validity.31 The raw score in each domain was converted to a transformed score with the range of transformed scores being from 0 to 100.32 The mean score of items within each domain was used to calculate the domain score. Domain scores are scaled in a positive direction; a higher score denoted a higher QOL.
Both intervention and control groups were evaluated at the baseline, 4th, 8th, and 12th week after the intervention was performed. Ethical clearance was approved by the Medical and Health Research Ethics Committee (MHREC), Faculty of Medicine, Universitas Gadjah Mada, Indonesia (Ref KE/FK/0131/EC/2017). Written informed consent for data usage was obtained from all respondents. Verbal and written informed consent for intervention was obtained from all the respondents in the intervention arm. Data regarding cognitive impairment status or dementia was obtained from the medical record, information from healthcare workers, or NH staff.
Statistical analysis
Descriptive statistics were employed to describe the groups’ sociodemographic characteristics. The Shapiro–Wilk test was used to assess the normality of sample distribution for the depression and QOL scores at baseline data. Given that the P-value for depression score was <0.001 and the P-value for QOL score was 0.082, which suggested that the Mann–Whitney U-test was appropriately used to determine whether any statistically significant differences were found in depression mean scores between groups at baseline, 4th, 8th, and 12th week after intervention, and the independent t-test was used to examine the differences of QOL mean score between two groups at each time point. The Friedman test was used to test for any statistically significant changes for depression mean scores over time during intervention for each group. The repeated measurement ANOVA (analysis of variance) test was used to examine for any statistically significant changes in QOL mean scores among the four time points for each group. The Wilcoxon signed-rank test as the post-hoc analysis was performed for pairwise comparisons on depression mean scores in each group. Meanwhile, adjustment for multiple comparisons on QOL mean scores in each group was tested by using Bonferroni post-hoc analysis with statistical significance was set at P-value <0.05.33
Results
Sociodemographic, health-related characteristic, and social support variables
The data regarding sociodemographic, health-related characteristic, and social support variables for 60 respondents are presented in Table 1. The majority (76.7%) were aged <80 years, 76.7% were female, and 91.7% had no partner. A large number (88.3%) of elderly had no or low educational background, and 60% had <3 physical illness. More than half (51.7%) of the elderly still received social support from family or others, with the majority (60%) of support being psychological and/or financial. In addition, the majority (86.7%) of elderly lived in NHs due to compulsion and most of them (61.7%) stayed in an NH for <4 years, with near two-thirds of elderly NH residents (61.7%) having a perceived adequacy of care. It was identified that there was no difference in terms of those sociodemographic, health-related characteristic, and social support variables between the groups (Table 1).
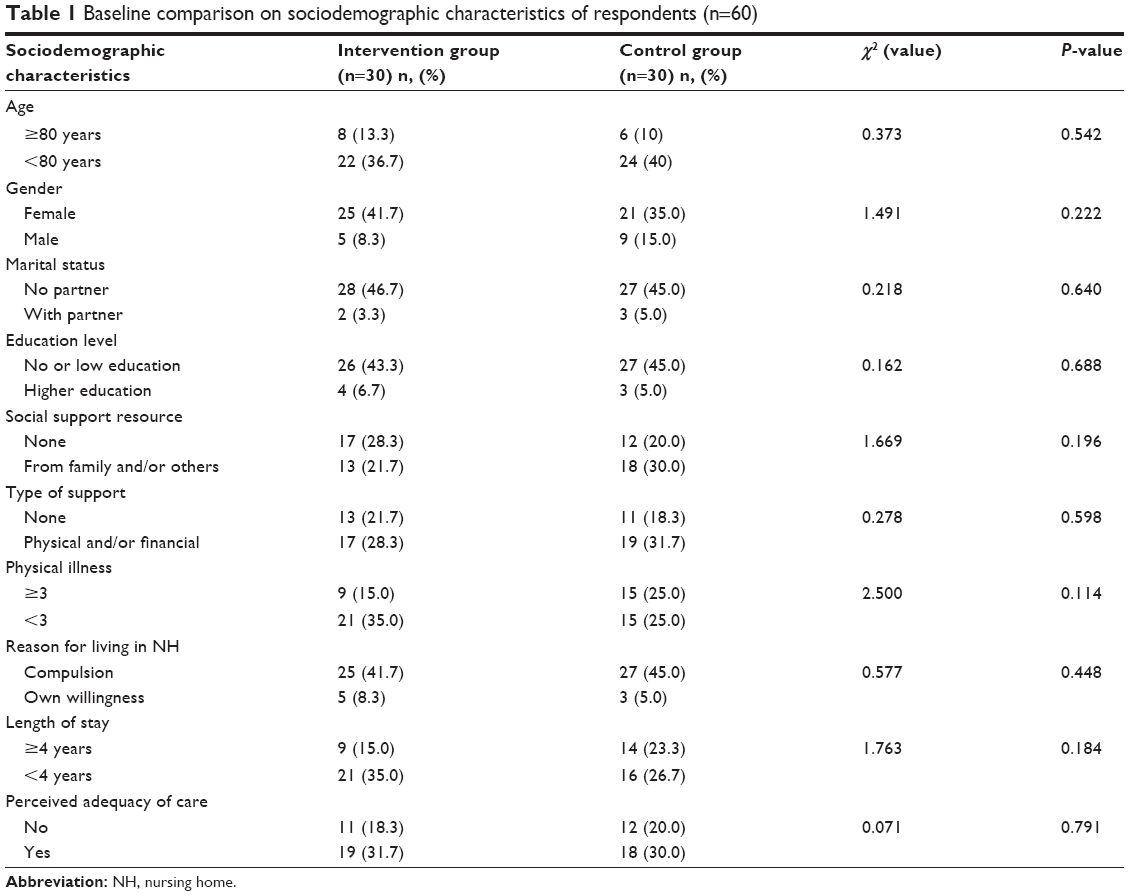 | Table 1 Baseline comparison on sociodemographic characteristics of respondents (n=60) |
Depressive symptoms measures
In both groups, there were statistically significant reductions in depression scores after the 12-week intervention (P<0.001). However, the religious intervention group showed a greater decrease in depressive symptoms after the 12-week intervention. Furthermore, statistically significant difference reductions in depression scores were only revealed in the intervention group after the 4-week intervention. In contrast, in the control group, there were no statistically significant difference reductions in depressive symptoms after the usual 4-week care intervention. In addition, there was a statistically significant difference in GDS scores between groups at the 4th, 8th, and 12th week post-intervention (Table 2). Finally, there was statistically significant difference in depression mean scores between the intervention and control groups at the week 12 post-intervention (Figure 2).
 | Table 2 Multiple comparisons on depression and QOL mean scores within and between groups (n=60) |
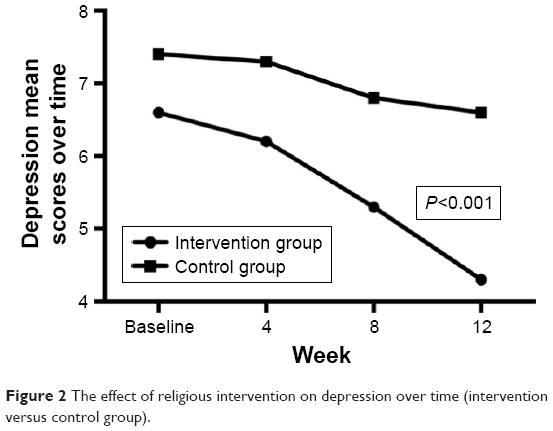 | Figure 2 The effect of religious intervention on depression over time (intervention versus control group). |
Quality of life measures
There was statistically significant improvement in QOL mean scores in both intervention and control groups at the 12-week post-intervention (P<0.001). However, the religious intervention group had a greater improvement in the QOL mean scores than those in the control group after the 12-week intervention (14.7 versus 9.1). There was a statistically significant difference in QOL mean scores between groups at the 4th, 8th, and 12th week post-intervention (Table 2). In addition, there was statistically significant difference in QOL mean scores between intervention and control groups at week 12 post-intervention (Figure 3).
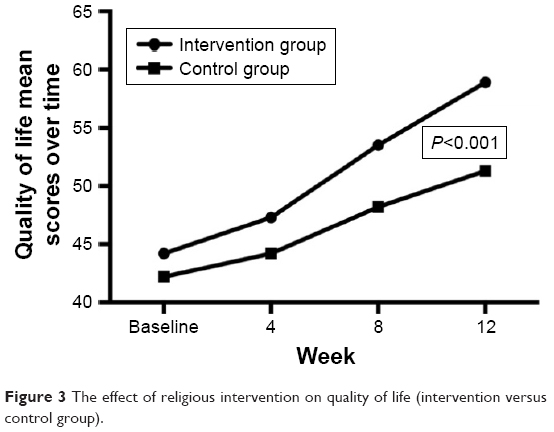 | Figure 3 The effect of religious intervention on quality of life (intervention versus control group). |
In both groups, the statistically significant difference improvement also revealed in both physical health, psychological, social relationship, and environment QOL domain mean scores (P<0.001). However, there was no statistically significant difference between groups at the 4th week post-intervention in the physical health, social relationship, nor environment QOL domain mean scores (P>0.05) (Table 2).
Discussion
In this present study, we provide preliminary evidence that religious intervention such as listening to Qur’anic recitals combined with a Muslim religious leader’s sermon approach could probably help reduce depressive symptoms as well as improve the QOL amongst the elderly.
Listening to Qur’anic recital appeared to have a similar result as listening to relaxing music therapy in terms of the pathophysiology of auditory stimuli mechanisms. The cerebral limbic system (hypothalamic–pituitary–adrenal axis and amygdaloid complex) mediates the audio involvement in steroid production via the pathway from the auditory system to the auditory area, particularly the neural pathway (emotion circuit).34 Audio stimuli evoke psychophysiological responses because of its influences on the limbic system which might stimulate the secretion of some hormones such as serotonin, dopamine, and/or norepinephrine at the synapse, eventually releasing the stress that leads to depression. The audio stimuli intervention in our study was derived from Qur’anic recital that serves as guidance for living as Muslims. It was surmised that this might have an effect in secreting those hormones that could relieve depression amongst respondents.
In fact, around 60%–70% depressive disorders are attributed to non-genetic factors such as past adverse events. For instance, experiencing sexual abuse, recent stress due to interpersonal difficulties, lifetime trauma, lack of social support, marital problems, and divorce were found to be contributors to depression.35,36 Sensitivity toward stress in depression is also unique by gender. Women are more responsive to stress compared to men, which is in line with the greater incidence of depression in women.37 In men, some conditions such as divorce, separation, and work difficulties are more likely to affect their developing depression, while women are more sensitive towards difficulty in socializing, developing a serious illness, or a response to death.38 This finding shows the gender-sensitive psychosocial approaches are important in preventing and treating depressive disorder cases, so the clinician should be aware that family background history and personal life experiences could continue to be the most solid source of information to estimate the risk of depressive disorders.
Delivering audio stimuli also effects the cardiovascular system.39 Specific musical phrases can synchronize inherent cardiovascular rhythms, thus modulating cardiovascular control,40 inducing the skin vasodilatation, and resulting in reduced blood pressure.41 Listening to Qur’anic recitals which consist of many rules of Tajwid (science of recitation) in the sound production such as the beats (harakat), segment quality, and single-breath phrase42 seems to have similar role to the musical phrases in alleviating stress that may lead to depression. One of the modern Qur’anic recitation styles, called the Murattal was selected for this study for its straightforward, speech-bound style of recitation. Its intent is the clear rendering of the text whether practiced for instructional or devotional purposes.43
Some supportive studies related to Qur’anic intervention have been conducted in various settings or subjects. A study amongst university faculty members found the effective role of reading the Qur’an in reducing depression.44 Learning Qur’anic recitation is also effective in relieving stress amongst adolescents and youngsters.45 Another clinical study in Pakistan indicated that the most significant reduction of depression levels amongst hospitalized patients were from those who listened to rhythmic Qur’anic recitation.46 While Qur’anic-related interventions show beneficial effects particularly on the psychological aspect in human beings, a Cochrane meta-analysis study indicated that music therapy only provides short-term beneficial effects for people with depression when compared to TAU (treatment as usual) alone. Furthermore, music therapy and TAU was not more effective than TAU alone for improving QOL.47
Considering the limitation of music therapy above, our study findings propose the notion that involving religious beliefs and faith-based intervention has a greater impact on relieving depressive symptoms and eventually resulting in improved QOL among elderly NH residents. Indeed, both groups in our study had reduced depression and increased QOL which may be because there were members in both groups who might be engaged in other Islamic rituals and practices such as daily prayers or salat, fasting, reading the Qur’an, or the other daily routine activities such as watching television, counselling, and playing or listening to music. These types of activities might affect the measurement outcomes in our study findings. However, it should be underlined that statistically significant difference reductions in depression scores only revealed in the intervention group after the 4-week intervention, whereas the statistically significant difference reductions in depression scores in the control group were revealed at the 8-week post-intervention. This suggests that the intervention group had a faster impact in lessening depressive symptoms than those in the control group.
Noticeably, the holy Qur’an provides a complete code of living for Muslims. It guides in all moral matters and offers the best values and methods of dealing with all aspects of human life. In the Qur’an, Surah Al-Israa:82 states that “And We send down of the Qur’an that which is a healing and a mercy to those who believe (in Islamic Monotheism and act on it), and it increases the zalimun (polytheists and wrongdoers) in nothing but loss”.48 It encourages believers to refer the Qur’an as healing when they face problems. Furthermore, the holy Qur’an also guides believers to put their trust in Allah’s plan (tawakkul). Surah At-Tawba:51 states, “Say: Nothing shall ever happen to us except what Allah has ordained for us. He is our Maula (Lord, Helper and Protector). And in Allah let the believers put their trust”.48 This Islamic concept of reliance on God and belief that He has the best intentions for humans more than they are capable of affecting for themselves seems to have an effect in achieving the expected outcomes amongst respondents in this present study.
Besides using the Qur’anic recital listening, a preacher’s approach was also applied simultaneously and considered as an additional religious intervention in our study. Previous studies that support this claim revealed the potential roles of religious leaders in influencing certain faith community members on health education and promotion programs, eventually resulting in positive health outcomes.49 In Islam, the primary source of guidance and advice is also derived from religious leaders, Imams, or preachers. Religious leaders who have been trained and briefed by health workers will become powerful agents of social change and are therefore able to change their followers and community’s health behaviors.50
In Nigeria, religious leaders have an important role in taking up reproductive health services,51 while in Malaysia, play a part in shaping health polices relating to HIV prevention.52 However, these Islamic religious leaders that have great influence on communities are rarely involved in health projects. A religious leader’s credibility, strong long-term relationships with followers, as well as excellent communication skills should be considered key factors in influencing the health behavior alterations amongst targeted groups. This is the underlying reason why a preacher with a licensed psychiatric nursing background was selected to deliver the sermon and speech in our study.
In terms of QOL, a systematic review found the stable significant association between depression severity and poorer QOL amongst elderly over time, regardless of which QOL assessment tools were used.53 This suggests that when individuals suffer from depression, their QOL tends to be lower, and vice versa. So by relieving depressive symptoms, it would also effect the QOL improvement among respondents. As a multidimensional and multilevel concept, generic health-related QOL (HQOL) has a more comprehensive concept than the current individuals’ health status due to its covering physical, psychological, social, and environmental domains as the life evaluations, with both positive and negative aspects.54,55
There are 57 countries with a dominant Muslim population,56 with more than 1.8 billion or 24% of the total population globally, placing Muslims as the world’s second largest religious group in 2015, and also projected to be the fastest growing major religious group in the decades ahead.57 Given that Indonesia has the largest Muslim population in the world58 and because of its rapidly growing elderly population, Indonesia should appropriately consider and anticipate the projected problems related to the elderly population growth in the years ahead.
Strengths, limitations, and practical recommendations
The first strength of our study is that we provided the 12-week intervention with a 100% follow-up rating on all follow-up sessions with no participants in either group withdrawing. The second strength was the use of widely validated and reliable questionnaires to screen geriatric depression and measure the QOL in various study site settings. Third, we randomized the Qur’an verses while delivering the Qur’anic recital listening intervention sessions in order to minimize the bias. Fourth, we chose the preacher with a licensed psychiatric nursing background to deliver the sermons to ensure the study goals were obtained.
Despite these strengths, the first limitation included the inability to distinguish between the comparative success of the Qur’anic recitations vs the sermons in reducing depressive symptoms for the intervention group. Future researchers might separate those interventions into 3 arms (Qur’anic recital listening, preacher’s approach, and TAU) in order to reduce the bias. The second limitation is that there were members in both groups who might be engaged in other Islamic rituals such as daily prayers or salat, fasting, reading the Qur’an, etc., which could affect the outcome measurements of this present study. Another limitation is that nonparametric tests to analyze the depression variable were used but it is advisable to use parametric methods to examine the effects on the outcome measures in future studies.
The growing trend of studies on the effect of the Qur’an and religious leader approaches in multi-dimensions and functions of human beings indicates that the researchers are paying more attention and interest toward this new basis of complementary therapy in their clinical practice. This is a great opportunity for Islamic states in the world to involve Muslims religious leaders and to make caregiving policies based on Qur’an issues and then implementing the findings in decision-making. The health care providers such as psychiatrists, nurses, and psychologists could probably also consider using faith-based therapy as part of their intervention in reducing depression and eventually improving QOL.
Conclusion
This present study shows the positive effects of relieving depressive symptoms and increasing the QOL amongst elderly NH residents by Qur’anic recital listening combined with a preacher approach.
Acknowledgment
This study was fully funded by the Indonesia Endowment Fund for Education (LPDP Scholarship), Ministry of Finance, Republic of Indonesia. The authors thank Mrs Marina Moore for proofreading this paper.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization (WHO). Mental health and older adults. WHO; 2016. Available from: http://www.who.int/mediacentre/factsheets/fs381/en/#. Accessed June 22, 2016. | ||
United Nations Department of Economic and Social Affairs. Population Division. World population ageing 2015. United Nations; 2015. Available from: http://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2015_Report.pdf. Accessed July 12, 2017. | ||
Teerawichitchainan B, Knodel J. Data mapping on ageing in Asia and the Pacific. HelpAge International; 2015. Available from: https://www.researchgate.net/profile/Bussarawan_Teerawichitchainan/publication/276204522_Data_mapping_on_ageing_in_Asia_and_the_Pacific/links/5552195b08ae980ca606a8a7.pdf. Accessed June 22, 2016. | ||
Wada T, Ishine M, Sakagami T, et al. Depression, activities of daily living, and quality of life of community-dwelling elderly in three Asian countries: Indonesia, Vietnam, and Japan. Arch Gerontol Geriatr. 2005;41(3):271–280. | ||
Mahwati Y. The relationship between spirituality and depression among the elderly in Indonesia. Makara J Health Res. 2017;21(1):13–19. | ||
Penninx BW, Deeg DJ, Van Eijk JT, Beekman AT, Guralnik JM. Changes in depression and physical decline in older adults: A longitudinal perspective. J Affect Disord. 2000;61(1–2):1–12. | ||
Cronin-Stubbs D, de Leon CF, Beckett LA, Field TS, Glynn RJ, Evans DA. Six-year effect of depressive symptoms on the course of physical disability in community-living older adults. Arch Int Med. 2000;160(20):3074–3080. | ||
Mitchell AJ, Subramaniam H. Prognosis of depression in old age compared to middle age: A systematic review of comparative studies. Am J Psychiatry. 2005;162:1588–1601. | ||
Ingold BB, Yersin B, Wietlisbach V, Burckhardt P, Bumand B, Büla CJ. Characteristics associated with inappropriate hospital use in elderly patients admitted to a general internal medicine service. Aging (Milano). 2000;12(6):430–438. | ||
Huang BY, Cornoni-Huntley J, Hays JC, Huntley RR, Galanos AN, Blazer DG. Impact of depressive symptoms on hospitalization risk in community-dwelling older persons. J Am Geriatr Soc. 2000;48(10):1279–1284. | ||
Cuijpers P, Schoevers RA. Increased mortality in depressive disorders: A review. Curr Psychiatry Rep. 2004;6(6):430–437. | ||
Unützer J. Top cited papers in International Psychogeriatrics: 2. Quality adjusted life years in older adults with depressive symptoms and chronic medical disorders. International Psychogeriatrics. 2009;21(2):265–266. | ||
World Health Organization (WHO). World Health Day – 7 April 2017. Depression: Let’s talk. WHO; 2017. Available from: http://www.who.int/campaigns/world-health-day/2017/en/. Accessed 29 October, 2017. | ||
Teresi J, Abrams R, Homes D, Ramirez M, Eimicke J. Prevalence of depression and depression recognition in nursing homes. Soc Psychiatry Psychiatr Epidemiol. 2001;36(12):613–620. | ||
Lok N, Lok S, Canbaz M. The effect of physical activity on depressive symptoms and quality of life among elderly nursing home residents: Randomized controlled trial. Arch Gerontol Geriatr. 2017;70:92–98. | ||
Meeks S, Van Haitsma K, Schoenbachler B, Looney SW. BE-ACTIV for depression in nursing homes: Primary outcomes of a randomized clinical trial. J Gerontol B Psychol Sci Soc Sci. 2015;70(1):13–23. | ||
Nemeroff CB. The corticotropin-releasing factor (CRF) hypothesis of depression: New findings and new directions. Mol Psychiatry. 1996;1(4):336–342. | ||
Cody RA, Drysdale K. The effects of psychotherapy on reducing depression in residential aged care: A meta-analytic review. Clin Gerontol. 2012;36(1):46–69. | ||
Gartlehner G, Hansen RA, Morgan LC, et al. Second-generation antidepressants in the pharmacologic treatment of adult depression: An update of the 2007 comparative effectiveness review. Vol 46. Rockville, MD: Agency for Healthcare Research and Quality (US); 2011. | ||
Fournier JC, DeRubeis RJ, Hollon SD, Dimidjian S, Amsterdam JD, Shelton RC, Fawcett J. Antidepressant drug effects and depression severity a patient-level meta-analysis. JAMA. 2010;303(1):47–53. | ||
Worthington EL Jr, Hook JN, Davis DE, McDaniel MA. Religion and spirituality. J Clin Psychol. 2011;67(2):204–214. | ||
Pargament KI, Tarakeshwar N, Ellison CG, Wulff KM. Religious coping among the religious: The relationships between religious coping and well-being in a national sample of Presbyterian clergy, elders, and members. J Sci Study of Relig. 2001;40:497–513. | ||
Lee CC, Czaja SJ, Schulz R. The moderating influence of demographic characteristics, social support, and religious coping on the effectiveness of a multicomponent psychosocial caregiver intervention in three racial ethnic groups. J Gerontol B Psychol Sci Soc Sci. 2010;65B(2):185–194. | ||
van Loon A, van Schaik A, Dekker J, Beekman A. Bridging the gap for ethnic minority adult outpatients with depression and anxiety disorders by culturally adapted treatments. J Affect Disord. 2013;147(1–3):9–16. | ||
Cinnirella M, Loewenthal KM. Religious and ethnic group influences on beliefs about mental illness: A qualitative interview study. Br J Med Psychol. 1999;72(Pt 4):505–524. | ||
Chiang K-J, Chen T-H, Hsieh H-T, Tsai J-C, Ou K-L, Chou K-R. One-year follow-up of the effectiveness of cognitive behavioral group therapy for patients’ depression: A randomized, single-blinded, controlled study. ScientificWorldJournal. 2015:1–11. | ||
Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. In Brink TL, editor. Clinical Gerontologist. New York: Haworth Press; 1986:165–173. | ||
McGivney SA, Mulvihill MM, Taylor B. Validating the GDS depression screen in the nursing home. J Am Geriatr Soc. 1994;42(5):490–492. | ||
Lesher EL. Validation of Geriatric Depression Scale among nursing home residents. Clin Gerontol. 1986;4(4):21–28. | ||
Salim OC, Sudharma NI, Hidayat A. Validitas dan reliabilitas World Health Organization Quality of Life-BREF untuk mengukur kualitas hidup lanjut usia. Universa Medicina. 2007;26(1):27–38. | ||
Skevington SM, Lotfy M, O’Connell KA; WHOQOL Group. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A Report from the WHOQOL Group. Qual Life Res. 2004;13(2):299–310. | ||
World Health Organization (WHO). WHOQOL-BREF Introduction, Administration, Scoring and Generic Version of The Assessment; 1996. Available from: http://www.who.int/mental_health/media/en/76.pdf. Accessed June 23, 2016. | ||
Peacock JL, Peacock PJ. Oxford handbook of medical statistics. New York, USA: Oxford University Press; 2011. | ||
Fukui H, Toyoshima K. Music facilitate the neurogenesis, regeneration and repair of neurons. Med Hypotheses. 2008;71(5):765–769. | ||
Kendler KS, Gardner CO, Prescott CA. Toward a comprehensive developmental model for major depression in men. Am J Psychiatry. 2006;163(1):115–124. | ||
Kendler KS, Gardner CO, Prescott CA. Toward a comprehensive developmental model for major depression in women. Am J Psychiatry. 2002;159(7):1133–1145. | ||
Young EA. Sex differences and the HPA axis: Implications for psychiatric disease. J Gend Specif Med. 1998;1(1):21–27. | ||
Kendler KS, Thornton LM, Prescott CA. Gender differences in the rates of exposure to stressful life events and sensitivity to their depressogenic effects. Am J Psychiatry. 2001;158(4):587–593. | ||
Trappe HJ. Music and medicine: The effects of music on the human being. Appl Cardiopulm Pathophysiol. 2012;16:133–142. | ||
Grewe O, Nagel F, Kopiez R, Altenmüller E. How does music arouse “chills”? Investigating strong emotions, combining psychological, physiological, and psychoacoustical methods. Ann NY Acad Sci. 2005;1060(1):446–449. | ||
Bernardi L, Porta C, Casucci G, Balsamo R, Bernardi NF, Fagari R, Sleight P. Dynamic interactions between musical, cardiovascular, and cerebral rhythms in humans. Circulation. 2009;119(25):3171–3180. | ||
Al-Tawil A. Fannu al-Tartil wa ‘Ulumuhu. Medina: Mujamma’ al-Malik Fahd; 1999. | ||
Nelson K. The Art of Reciting the Qur’an. Cairo; New York: The American University in Cairo Press; 1987. | ||
Mohammadi Laeini MB, Azadbakht M, Hosayni SH, Pezeshkan P. Knowledge and attitudes of some faculty members of Mazandaran university of medical sciences about the Quran, 2007 to 2008. Mazandaran Univ Med Sci J. 2009;1(69):73–78. | ||
Taghiloue S. Effect on reducing stress in the Quran reading among youth. Gilan Univ Med Sci J. 2009;18(17):72–81. | ||
Rana SA, North AC. The effect of rhythmic Quranic recitation on depression. Journal of Behavioural Sciences. 2007;17(1–2). | ||
Aalbers S, Fusar-Poli L, Freeman RE, et al. Music therapy for depression. Cochrane Database Syst Rev. 2017;11:CD004517. | ||
Khan MM, Al-Hilali MT. Interpretation of the meanings of the Noble Qur’an in the English language. Revised edition. Riyadh, Kingdom of Saudi Arabia: Darussalam; 2011. | ||
Toni-Uebari TK, Inusa BPD. The role of religious leaders and faith organisations in haemoglobinopathies: A review. BMC Hematol. 2009;9(6). | ||
Freij LS. Muslim religious leaders as partners in fostering positive reproductive health and family planning behaviors in Yemen: A best practice. Washington, DC: USAID; 2009. | ||
Maiwada AM, Rahman NAA, Abdurrahaman S, Mamat NM, Walker J-A. The Islamic religious leaders as health promoters: Improving maternal health in selected communities of Zamfara State, Nigeria. J Reprod Infertil. 2016;7(1):8–14. | ||
Barmania S, Aljunid SM. Navigating HIV prevention policy and Islam in Malaysia: Contention, compatibility or reconciliation? Findings from in-depth interviews among key stakeholders. BMC Public Health. 2016;16(524):1–8. | ||
Sivertsen H, Bjørkløf GH, Engedal K, Selbæk G, Helvik A-S. Depression and quality of life in older persons: A review. Dement Geriatr Cogn Disord. 2015;40(5–6):311–339. | ||
Bowling A. Measuring health. 3 ed. Maidenhead: Open University Press; 2005. | ||
The WHOQOL Group. The World Health Organization quality of life assessment (WHOQOL). Position paper from the World Health Organization. Soc Sci Med. 1995;41(10):1403–1409. | ||
Bukhari A, Rafique M, Aziz R. The role of religious leaders in the prevention of HIV/AIDS. First ed. Pakistan: UNICEF-Ministry of Health of Pakistan-National AIDS Control Program; 2004. | ||
Pew Research Center. The changing global religious landscape. 2017. Available from: http://www.pewforum.org/2017/04/05/the-changing-global-religious-landscape/. Accessed 8 January, 2018. | ||
Pew Research Center. The future of world religions: Population growth projections, 2010–2050. Appendix C: Religious composition by country and territory, 2010 and 2050. 2017:234. Available from: http://www.pewforum.org/files/2015/04/PF_15.04.02_ProjectionsAppendixC.pdf. Accessed January 8, 2018. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.