")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
The Effect of Perceptual-Motor Training on Executive Functions in Children with Non-Verbal Learning Disorder
Authors Soltani Kouhbanani S, Arabi SM, Zarenezhad S, Khosrorad R
Received 5 March 2020
Accepted for publication 21 April 2020
Published 5 May 2020 Volume 2020:16 Pages 1129—1137
DOI https://doi.org/10.2147/NDT.S252662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Sakineh Soltani Kouhbanani,1 Seyedeh Manizheh Arabi,2 Somayeh Zarenezhad,1 Razieh Khosrorad3
1Department of Educational Sciences, Educational Sciences and Psychology Faculty, Ferdowsi University of Mashhad, Mashhad, Iran; 2Department of Motor Behavior, Faculty of Sport Sciences, Ferdowsi University of Mashhad, Mashhad, Iran; 3Department of Health Education, Educational Neuroscience Research Center, Sabzevar University of Medical Sciences, Sabzevar, Iran
Correspondence: Razieh Khosrorad
Department of Health Education, Educational Neuroscience Research Center, Sabzevar University of Medical Sciences, Sabzevar, Iran
Tel +98 930 668 1173
Fax +98 51 4401 8424
Email [email protected]
Purpose: Research shows an atypical cognitive process in children with nonverbal learning disorder (NLD) compared to typically developing children, but a wealth of information indicates that physical activity can influence cognitive processes. However, little is known about the effects of perceptual-motor training and its impact on the cognitive process of children with NLD. Thus, the major goals of this study are to compare the executive functions (EFs) in children with NLD with typically developing children and then to investigate the effect of perceptual-motor training on EFs of children with NLD.
Methods: To achieve the first goal, 400 typically developing (IQ > 80) and NLD children (7– 13 years old) were randomly selected in the city of Mashhad, Iran, during the period 2017– 2018. As for the second goal, 50 children with NLD were randomly assigned to an experimental or control group. To evaluate executive functions, Delis–Kaplan executive function system test was used at the pretest, posttest, and 3-month follow-up. The experimental group received the Werner and Reini’s perceptual-motor training program in sixteen 45-min sessions (three sessions per week), but the control group did not receive any intervention.
Results: The results showed that children with NLD were significantly weaker than typically developing children in London Tower Test (t (38) = − 4.662, p < 0.01), Trail Making Test (t (33.926) = − 3.11, p < 0.01), Card Sorting Test (t (38) = − 3.427, p < 0.01), and Stroop Color Test (t (30.035) = − 5.876, p < 0.01). The Pilates training had an obvious effect on enhancing the performance of participants in the experimental group (p< 0.001), but similar results were not observed in the control group.
Conclusion: Children with NLD have problems in EFs, but perceptual-motor training can be used as an effective intervention for these children.
Keywords: physical activity, cognitive processing, executive function, nonverbal learning disorder
Introduction
Non-verbal Learning Disorder (NLD), which is considered as a neurodevelopmental disorder by the International Classification System,1,2 refers to the disrupted processing of non-verbal information, especially in solving mathematical problems.3 The math learning disabilities usually giving rise to a plethora of problems related to conceptual understanding, counting sequences, symbol system of written numbers, math language, basic number facts, procedural steps of computation, application of arithmetic skills, and problem solving.4 Many reasons have been presented to explain problems of children with NLD, but most of studies have highlighted the role of executive functions (EFs) as one of the key aspects of NLD difficulties.5
EFs are cognitive-regulatory processes that support targeted thoughts and behaviors in two main brain networks.6 EF processes include planning, cognitive flexibility, problem-solving, reasoning functions, and working memory.7 Working memory is a system that integrates sub-systems and functions of short-term and long-term memory.8 Cognitive flexibility is another main component of EFs characterized by lagging behind, repetitive movements, difficulty in adjustment of motor activities and inability to regulate thoughts and actions in response to environmental changes.9 One important aspect of EFs is problem-solving, which is concerned with processes that facilitate the selection of appropriate responses to overcome barriers and reach a desirable position.10 These basic EF skills encompass “the cognitive system,” which controls and manages other cognitive process such as academic achievements at school.11 Given the important role of EFs in school achievements, they have received considerable attention. Many correlational studies have demonstrated the relationship between EFs and achievements in reading, writing, and mathematics in typically developing children.8,12,13 In addition, both cross-sectional and longitudinal correlation studies have demonstrated that EFs are significantly correlated with academic achievements, and physical activity in children.14–16 What we know about EFs in healthy children is based on correlational studies about EFs and school achievements, which have highlighted the need for designing intervention methods to affect EFs in children with NLD. Recently, growing attention has been paid to the effect of physical activities on EFs. Traditionally, it is believed that cardiovascular physical activities wield a positive effect on EFs in typically developing children due to structural and chemical changes induced in the central nervous system.14,17 Cardiovascular physical activities represent the quantitative aspect of physical activity that chiefly focus on heart rate changes, duration and intensity of training in each training session, while the qualitative aspect of training is characterized with coordinative demands and cognitive engagement that place a premium on perception-motor activities like bimanual coordination and eye-hand/foot coordination. Koutsandreou et al (2016) have reported that 10 weeks of an afterschool perceptual-motor training exercise regimen containing three 45-min sessions of physical activities per week has a positive effect on working memory in typically developing children compared to a simple cardiovascular training.17 Similarly, Beck et al found that 6 weeks of fine and gross motor training had a significant effect on arithmetic performance of healthy children.18 It is generally acknowledged that motor exercises consisting of gross and fine motor activities are basically perceptual-motor activities that influence the cognitive process of central nervous system.19 Research shows that the significant effect of perceptual-motor training on cognitive processes is related to brain electrophysiological measures, including increased amplitudes and shorter latencies of P3 event relate to potential component, which demonstrate a more efficient and faster cognitive processing.18
However, according to above studies, cognitively challenging physical activities have a greater effect on EFs in healthy children than the cardiovascular physical training. There is ongoing debate about the best strategies to improve EFs in children with NLD and the types of cognitively demanding exercises have not been precisely determined. To date, this method has not been used for children with NLD. In view of this, this study attempts to explore the effectiveness of perceptual-motor intervention in children with NLD. In particular, this study sets out to compare EFs in healthy children with NLD, and investigates the effect of perceptual-motor training on EFs in children with NLD. It is hypothesized that measures of EFs will be improved in participants in the motor- perceptual group at the post-test and follow-up.
Materials and Methods
Participants
First phase: 400 children (200 children with NLD and 200 typically developing children) participated in this study. Children with NLD who met the following criteria were included in the study: 1) at least two subtests on Wechsler Intelligence Scale for Children (WISC), vocabulary, similarities, and information, obtaining the highest result, which shows reading skills superior to the mathematical achievement; 2) at least two of WISC subtests – block design, object assembly, and coding – earning the lowest results, which is indicative of deficit in the visuospatial working memory;2 3) a verbal intelligence quotient (VIQ) at least 10 points higher than the performance intelligence quotient (PIQ) on WISC; 4) less than two errors on simple tactile perception and suppression vs finger agnosia and finger dysgraphesthesia, as well as an astereognosis composite greater than 1 standard deviation below the mean; 5) grip strength within or above one standard deviation of the mean vs Grooved Pegboard test; 6) Progressive decline of right, left, and both hands in Tactual Performance Test; and 7) obtaining a Wide Range Achievement Test’s standard score in reading at least 8 points higher than standard score of arithmetic. While five or six of these traits suggest the probability of NLD in older children (9–15 years old), in younger children (7–8 years old), three criteria are sufficient to confirm the diagnosis. Accordingly, 200 children diagnosed with NLD, including 96 females and 104 males (7–13 years of age, a mean age of 10.6 years) were selected for the study. We decided to study children in this age range as most of previous research has explored EFs at this age group. Further, it is postulated that brain development is greater at this age, and can exert a sizable effect on the cognitive level.20 Exclusion criteria for the NLD group consisted of a diagnosis of Attention Deficit/Hyper Activity Disorder (indicated by scores below 14 and 22 for females and males on ADHD rating scale, respectively), high function autism disorder (defined by Autism Diagnostic Observation Schedule (ADOS), Autism Diagnostic Interview (ADI-R), and full IQ > 80), seizure and fragile X.
Also, 200 participants who shared the same chronological age and sex (100 females and 100 males, aged 7–13 with a mean age of 10.4 years) were enrolled in the study as the typically developing control group. We selected typically developing children from the city of Mashhad via e-mail and advertisement throughout the city. The children that exhibited symptoms of ADHD, had a history of academic or psychiatric difficulties, or were on psychiatric medications (as reported by parents), were excluded from the study. Only children whose cognitive functioning was close to or above the average range, assessed by Wechsler Abbreviated Scale of Intelligence, or had high performance on IQ scale were included in this study.21 None of the children participating in this study used any prescribed medications that affected motor functions (eg, Risperdal), or reported a history of head injury or organic brain disorder.
Second phase: To examine the effect of intervention on EFs, 50 children with NLD (25 males, aged 7–13 years, mean (M) =10.67, SD = 0.542 as well as 25 females, aged 7–13 years, M=10.37, SD = 0.463) were selected from the first phase of the study. The children with NLD were assigned randomly to the experimental (13 males, aged 7–13 years, M = 10.43, SD = 0.46 as well as 12 females, aged 7–13 years, (M) = 10.56, SD = 0.42) and control groups (11 males, aged 7–13 years, M=10.37, SD=0.42 and 14 females, aged 7–13 years, M=10.61, SD=0.34). Participants were controlled for age, gender and intelligence quotient. Demographic information is shown in Table 1.
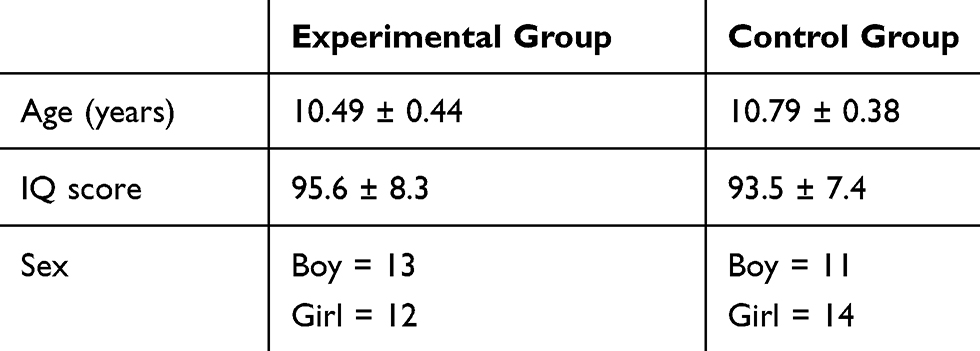 |
Table 1 Characteristics of Study Participants are Stated as Means (Standard Deviations) |
Materials
Delis–Kaplan Executive Function System
It is a valid instrument used to evaluate critical components of EFs in childhood and adolescence. As a neuropsychological test, it measures verbal and non-verbal EFs in children and adults aged 9 to 90 years. This test is used to assess variables of working memory, response inhibition, cognitive flexibility and problem-solving. It consists of 9 subtests that measure each component of EFs, but we used only 4 subtests to assess the non-verbal aspect of EFs. The first subscale is London Tower Test that measures planning and inhibition by manipulating prefabricated building blocks to develop a specific program in accordance with a set of instructions.7 The second subscale is the Trail Making Test that assesses cognitive flexibility and visuospatial working memory. The third subscale is the Stroop Color Test that evaluates response inhibition. The Stroop card contains three phases where participants need to name the color in Phase 1, read the printed color in Phase 2, and detect the color of the printed ink in Phase 3. The fourth subscale is Card Sorting that tests set-shifting. In this test, the examiner asks children to arrange cards into three possible groups (shapes, colors, or numbers) and identify sorting rules after a certain number of arrangements.22
Procedure
This study was approved by the Review Board of Ferdowsi University of Mashhad (IR.UM.REC. 1398.149). The study was conducted in compliance with the principles of the Declaration of Helsinki.
The First Phase of the Study
This phase involved a pretest and a posttest with two groups (typically developing children and children with NLD) with identical age and IQ score. We made an appointment with parents of participants, during which the goals and protocols of the study were explained. A written informed consent was obtained from parents and the participants, if they were old enough to read and sign the consent form. Also, they were informed that they could withdraw from the study at any stage. We also explained the goals and procedure of the study to participants. Then, we performed Wechsler intelligence test. To evaluate EFs, we used Delis–Kaplan Executive Functions System.23 This test was conducted in a quiet room in a psychology institute in Mashhad.
The Second Phase of Study
The second phase of the study involved a pretest, 16 sessions of training, a posttest, and a three-month follow-up, with one experimental and one control group. Fifty children with NLD were randomly selected from the first phase of the study. Parents were invited to an orientation session that described the goals and protocols of the second phase of the study. Then, a written consent form along with the child assent for participation in the study was gathered from parents. They were also given assurance regarding the possibility of withdrawing from research at any time. A random assignment was completed to determine the experimental and control groups. The control group did not receive any physical training, while experimental group participated in Werner and Reini’s perceptual-motor training for sixteen 45-min sessions that were held three times a week. Posttest assessment was conducted at the end of the intervention sessions. Follow-up assessments were carried out 3 months after the intervention. In addition to the intervention, both experimental and control groups received routine care in their institution. The routine care consisted of services such as an educational program that were not part of the study. Thus, the control group represented as a passive group. After data were collected from the posttest and follow-up, identical intervention was presented to the control group.
Perceptual-Motor Training
The perceptual-motor skills training is a cognitively challenging exercise based on the Werner-Reini’s training program,24 which was conducted for the experimental group. It consisted of sixteen 45-min sessions over a 6-week period (three sessions per week). Three motor skill instructors with at least 5 years of experience in working with children conducted the intervention program. Before the perceptual-motor training intervention, the goals of the study were explained to instructors in a briefing session. All participants in the experimental group attended the group training session in the morning (10–11 am). The intervention was performed in a gym equipped with balance ladders, mats, balls, tubs, mirrors, and a white board. Also, some necessary materials such as sand, clay and finger color, puzzle, paper, balloon, and handy bubble makers were brought to the gym. All children had their own space and equipment during the intervention.
Intervention plans were developed based on key elements of perceptual-motor skills. It aimed to develop balance, tone awareness, space awareness, shape perception, visual and auditory perceptions, kinesthetic-tactile perception, and eye-hand/foot coordination. Each intervention sessions commenced with some warm-up activities and games such as jumping and tagging for about 10 min. Children were randomly assigned to three stations with one instructor per station. Each station’s activities lasted for 15 min. Then, children were switched to a different station. Overall, children spent 45 min on the perceptual-motor training. The intervention sessions were ended by cool-down activities such as stretching for about 5 min. Table 2 shows the perceptual-motor activities performed in each session as well as the objectives of each session.
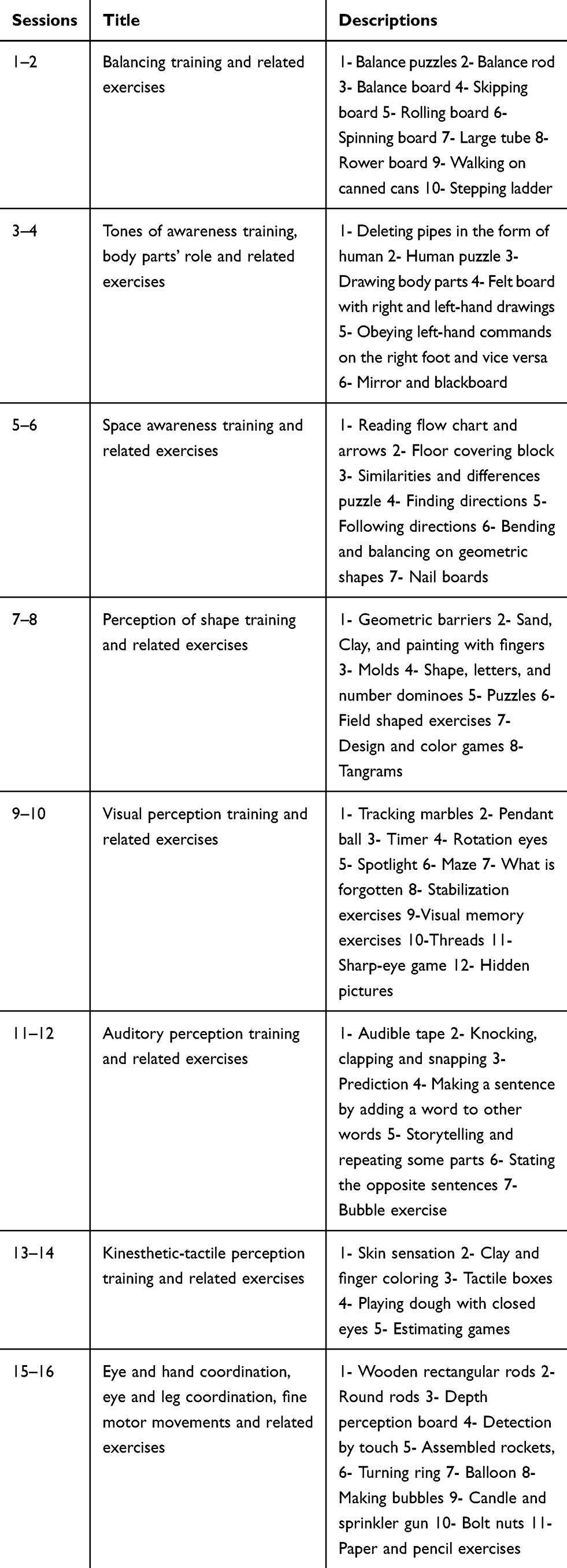 |
Table 2 Exercise Training in Each Session of Intervention |
Data Analysis
The descriptive statistics used in data analysis consisted of means (M) and standard deviations (SD) of both groups. To compare the difference between typically developing children and children with NLD, the independent t-test was employed. The effect of perceptual-motor intervention on dependent variables was evaluated using repeated measures ANCOVA, and MANCOVA. Age and intelligence were considered as covariates to control their effects on dependent variables. We also checked typical assumptions of ANCOVA, and MANCOVA tests including normality and homogeneity of variance using Boxplot and Q-Q plot (residuals vs fitted values). The Bonferroni’s post hoc test was used to detect inter-group differences at different times. The analyses were performed using SPSS 25 software, and a significance level of p < 0.05 was considered.
Results
Comparison of EFs in Typically Developing Children and Children with NLD
Table 3 shows the descriptive information of EFs for children with NLD and typically developing children.
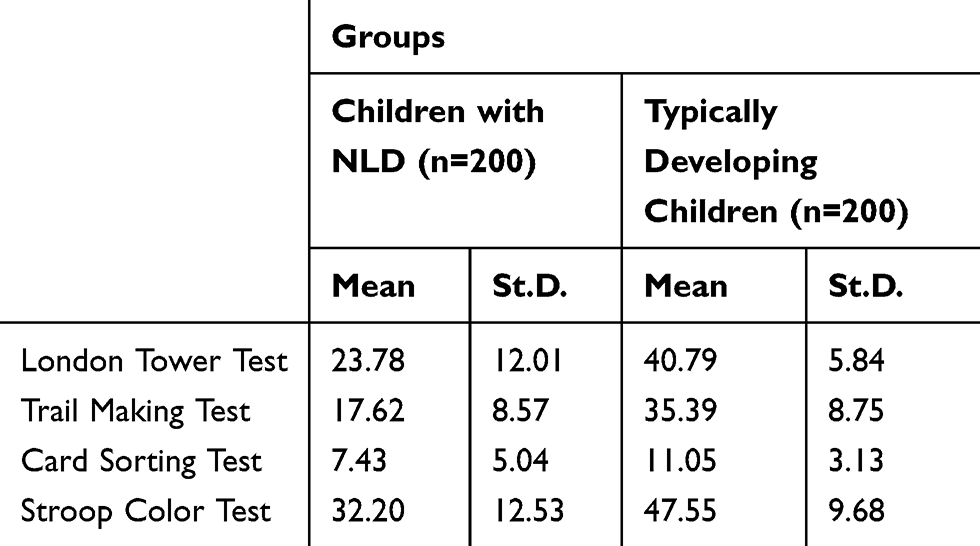 |
Table 3 Descriptive Information on EFs in Each Group |
The results of independent t-test (Table 4) showed a significant difference between typically developing children and children with NLD with respect to London Tower Test at the significance level of 0.99 (t (286.05) = −17.96, p < 0.001). According to the descriptive indicators, typically developing children excelled at the London Tower Test (M = −17.002). The results of independent t-test for the Trail Making Test revealed a significant difference between typically developing children and children with NLD scores at a significance level of 0.99 (t (398) = −20.51, p<0.001). With regard to the descriptive indices, we observed that students in the typically developing group gained higher scores on the Trail Making Test (M = −76/17).
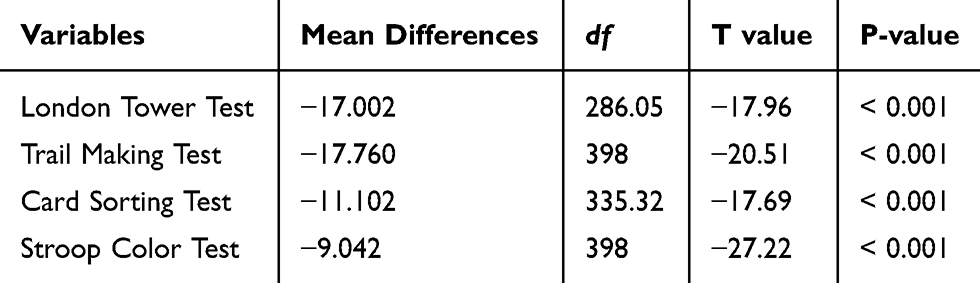 |
Table 4 The Results of t-Test for the Difference of Students in Study Variables |
Besides, the results of independent t-test exhibited a significant difference between the scores of typically developing children and children with NLD in Card Sorting Test at a significance level of 0.99 (t (335.32) = −17.96, p < 0.001). As for the descriptive indicators, it can be seen that students in the typically developing group obtained higher scores on the Card Sorting Test (M = −11.10). The results of independent t-test exhibited a significant difference between typically developing children and children with NLD with respect to performance on Stroop Color Test at a significance level of 0.99 (t (398) = −27.22, p < 0.001). According to the descriptive indices, typically developing children gained higher scores on the Stroop Color Test (M = −0.49).
The Effect of Intervention on EFs in Children with NLD
Table 5 shows descriptive statistics of EF tasks for each group at different stages of the study.
 |
Table 5 Descriptive Statistics of EF Tasks |
We used a 3 (time: pretest, posttest, and follow-up) * 2 (groups: experimental and control) repeated measures analysis of covariance (MANCOVA) to evaluate each participant’s function on London Tower Test, Trail Making Test, Card Sorting Test, and Stroop Color Test. According to the results, the main stage effect (F (2, 58) = 44.07, p < 0.001, ŋ2 = 0.2) was significant and London Tower scores in the posttest and follow-up were significantly higher than the pretest. Also, the main group effect (F (1, 58) = 48.68, p = 0.004, ŋ2 = 0.6) was found to be significant. The results of post hoc comparisons exhibited that experimental group outperformed the control group in London Tower tasks. In addition, stage and group interactions were significant (F (1, 58) = 53.95, p < 0.001, ŋ2 = 0.4). Although training had a prominent effect on improving performance in the experiment group (p < 0.001), comparable results were not observed in the control group. Also, the results of Trail Making tasks illustrated that the main stage effect (F (2, 58) = 9.32, p = 0.005, ŋ2 = 0.6) was significant and Trail Making scores were significantly higher in the posttest and follow-up than in the pretest. Moreover, the main group effect (F (1, 58) = 8.34, p = 0.01, ŋ2 = 0.6) was found to be significant. The results of post hoc comparisons revealed that the experimental group excelled the control group in Trail Making tasks. In addition, stage and group interactions were significant (F (1, 58) = 6.61, p = 0.016, ŋ2 = 0.5). Although training had a remarkable effect on boosting the performance of participants in the experiment group (p < 0.001), comparable results were not observed in the control group.
According to the results of Card sorting tasks, the main stage effect (F (2, 58) = 28.24, p < 0.001, ŋ2 = 0.1) was significant, and Card sorting scores in posttest and follow-up were significantly higher than the pretest. Also, the main group effect (F (1, 58) = 13.59, p = 0.002, ŋ2 = 0.6) was significant. The results of post hoc comparisons suggested that the experimental group outperformed control group in Card Sorting tasks. In addition, stage and group interactions were significant (F (1, 58) = 23.82, p<0.001, ŋ2 = 0.5). Although training had an obvious effect on enhancing the performance of participants in the experiment group (p<0.001), similar results were not observed in the control group. According to the results of Stroop Color tasks, the main stage effect (F (2, 58) = 41.93, p<0.001, ŋ2 = 0.03) was significant and Stroop Color scores in the posttest and follow-up were significantly higher than the pretest. Also, the main group effect (F (1, 58)=45.62, p = 0.004, ŋ2 = 0.3) was significant. The results of post hoc comparisons demonstrated that the experimental group outstripped the control group in Stroop Color tasks. In addition, stage and group interactions were significant (F (1, 58) = 48.42, p<0.001, ŋ2 = 0.1). Although training wielded a significant effect on improving the performance of participants in the experiment group (p < 0.001), comparable results were not observed in the control group.
Discussion
This study was conducted to compare EFs in two groups of typically developing children and children with NLD. We also examined whether perceptual-motor intervention produced any effect on planning, inhibition, cognitive flexibility, switching attention of children with NLD. The results manifested that children with NLD had weaker EFs in all domains of planning, inhibition, cognitive flexibility, switching attention compared to typically developing children. These findings align well with literature in this field. NLD is a neurodevelopmental disorder that affects cognitive functions like spatial and abstract processing, which are primarily located in the right brain hemisphere.25,26 The results demonstrated the slower responses of participants in the NLD group in classifying space (for a visual object or sound frequency change) in comparison with the control group. This suggests that individuals with NLD have difficulty in spatial processing.27 Neural networks involved in controlling activities are primarily located in the frontal area of the brain. These children are postulated to suffer from neurodevelopmental disorders that may be induced by delayed frontal development.28 The importance of white matter connections in left and right hemispheres in behavioral and cognitive deficits of individuals with NLD disorders is important.29 In fact, EF skills are concerned with the performance of the cognitive-motor external coordinator associated with the frontal or lateral parts of the forehead, which are coordinated with other neural circuits. As a result, targeted behaviors are executed in a planned, flexible, relevant, timely, and appropriate manner.30 Also, experimental and clinical studies offer evidence that cerebellum plays various roles during development including sequencing purposes, behavioral aspects, and EFs.
As for the perceptual-motor training, our results exhibited improvement in all aspects of EFs in the experimental group compared to the control group. This results are aligned with those reported in earlier studies on typically developing children. Beck et al revealed that fine and gross motor enrichment has a positive effect on mathematical problem solving in typically developing children. Similarly, our results showed that perceptual motor activity containing fine and gross motor training could improve EFs in children with NLD. In addition, these findings support the idea that cognitively demanding physical exercises can improve cognitive processing.17 The motor-cognition connection is reinforced by the engagement of neural regions during motor tasks, which are classically pertained to cognitive functions.17 Training EFs through motor tasks generates positive changes in EFs, which could be linked to the growth of prefrontal and parietal activity. Serrien et al and Olesen et al demonstrated that identical brain regions seem to be engaged in both complex motor tasks and EFs tasks.31 Additionally, this positive effect may be linked to electrophysiological measures of the brain, including increased amplitude and shorter latency of the P3 event-related potentials (ERPs) component, which exhibit more efficient and faster cognitive processing.32 Accordingly, perceptual – motor activities seem to be effective physical activities in reinforcing attention, which is critical to the reinforcement of short and long-term memory due to the role of cerebellum and frontal lobe in perceptual motor tasks and cognition.33
Moreover, according to the embodied cognition theory, cognitive processing is grounded in bodily experience. According to this perspective, cognition is a product of brain, body, and environmental interactions when individuals engage in an action. Hence, it may vary by changing the activity. Cognitively demanding motor tasks can alter EFs and consequently learning. The results are in agreement with those reported by Picard and Strick (1996) according to which cognitively demanding motor tasks co-vary with the pattern of brain activation, and therefore the extent of information processing.34 A greater cognitive demand for motor tasks requires more prefrontal and cerebellum activities during perceptual motor training task.31 Thus, it seems that this type of motor training requires more diversified frontal-dependent cognitive processes.
Conclusion
In conclusion, our results support the effect of perceptual-motor training on EFs in children with NLD. Given the improvement of EFs and its lasting effect in children with NLD (about 3 months), it seems that conducting perceptual-motor trainings can improve cognitive processes. Overall, the main strength of this study lies in the ecological value of its design, which involves the selection of participants from all over the city. Moreover, since a regular teacher and framework were used for students during the intervention, these factors are unlikely to have influenced the results. In addition, the results exhibited the lasting effect of intervention, which persisted for about 3 months after the intervention. The present study had a number of limitations that should be noted. We had a passive control group in our study that did not participate in any physical activities. Accordingly, we suggest future studies to compare an active control group that do cardiovascular trainings or any other kind of physical training, so that perceptual-motor training could be compared to other kind of physical exercise. Also, it is suggested that future studies assess the neural aspect of perceptual motor training effect like brain event-related potentials after the intervention to confirm the neural effect of perceptual-motor training on EF.
Acknowledgments
All expenses of this research project were funded by the author and we did not receive any financial grant from a specific entity. We would like to thank the Welfare Organization of Khorasan Razavi and its branches. We are also grateful to the families who took part in our research. We also wish to thank teachers, coaches, and specialists who help us in the course of this study.
Disclosure
The authors have no conflicts of interest to report in this work.
References
1. Mammarella IC, Cardillo R, Zoccante L. Differences in visuospatial processing in individuals with nonverbal learning disability or autism spectrum disorder without intellectual disability. Neuropsychology. 2019;33(1):123.
2. Mammarella IC, Cornoldi C. An analysis of the criteria used to diagnose children with Nonverbal Learning Disability (NLD). Child Neuropsychol. 2014;20(3):255–280. doi:10.1080/09297049.2013.796920
3. Zhang N, Kong Y. A cognitive therapy intervention programme increases working memory in students with learning disabilities. NeuroQuantology. 2018;16(2). doi:10.14704/nq.2018.16.2.1177
4. Garnett K. Developing fluency with basic number facts: intervention for students with learning disabilities. Learn Disabil Res Pract. 1992;7(4):210–216.
5. Liddell GA, Rasmussen C. Memory profile of children with nonverbal learning disability. Learn Disabil Res Pract. 2005;20(3):137–141. doi:10.1111/j.1540-5826.2005.00128.x
6. Kim-Spoon J, Deater-Deckard K, Calkins SD, King-Casas B, Bell MA. Commonality between executive functioning and effortful control related to adjustment. J Appl Dev Psychol. 2019;60:47–55. doi:10.1016/j.appdev.2018.10.004
7. Delis DC, Kramer JH, Kaplan E, Holdnack J. Reliability and validity of the Delis-Kaplan executive function system: an update. J Int Neuropsychol Soc. 2004;10(2):301–303. doi:10.1017/S1355617704102191
8. Bull R, Espy KA, Wiebe SA. Short-term memory, working memory, and executive functioning in preschoolers: longitudinal predictors of mathematical achievement at age 7 years. Dev Neuropsychol. 2008;33(3):205–228. doi:10.1080/87565640801982312
9. Hill EL. Evaluating the theory of executive dysfunction in autism. De Rev. 2004;24(2):189–233. doi:10.1016/j.dr.2004.01.001
10. Riley MS. Development of Children’s Problem-Solving Ability in Arithmetic. 1984.
11. Watson SM, Gable RA, Morin LL. The role of executive functions in classroom instruction of students with learning disabilities. Int J Sch Cogn Psychol. 2016;3:167. doi:10.4172/2469-9837.1000167
12. Alloway TP, Alloway RG. Investigating the predictive roles of working memory and IQ in academic attainment. J Exp Child Psychol. 2010;106(1):20–29. doi:10.1016/j.jecp.2009.11.003
13. Clark CA, Pritchard VE, Woodward LJ. Preschool executive functioning abilities predict early mathematics achievement. Dev Psychol. 2010;46(5):1176. doi:10.1037/a0019672
14. Diamond A. Activities and programs that improve children’s executive functions. Curr Dir Psychol Sci. 2012;21(5):335–341. doi:10.1177/0963721412453722
15. Donnelly JE, Hillman CH, Castelli D, et al. Physical activity, fitness, cognitive function, and academic achievement in children: a systematic review. Med Sci Sports Exerc. 2016;48(6):1197. doi:10.1249/MSS.0000000000000901
16. Pesce C, Ben-Soussan TD. “Cogito ergo sum” or “ambulo ergo sum”? New perspectives in developmental exercise and cognition research. In: T. McMorris, editor, Exercise-Cognition Interaction: Neuroscience Perspectives. Elsevier Academic Press; 2016:251–282.
17. Koutsandreou F, Wegner M, Niemann C, Budde H. Effects of motor versus cardiovascular exercise training on children’s working memory. Med Sci Sports Exerc. 2016;48(6):1144–1152. doi:10.1249/MSS.0000000000000869
18. Beck MM, Lind RR, Geertsen SS, Ritz C, Lundbye-Jensen J, Wienecke J. Motor-enriched learning activities can improve mathematical performance in preadolescent children. Front Hum Neurosci. 2016;10:645. doi:10.3389/fnhum.2016.00645
19. Thelen E. Motor development as foundation and future of developmental psychology. Int J Behav Dev. 2000;24(4):385–397. doi:10.1080/016502500750037937
20. Iglesias-Sarmiento V, López NC, Rodríguez JLR. Updating executive function and performance in reading comprehension and problem solving. An Psicología. 2015. doi:10.6018/analesps.31.1.158111
21. Frey HP, Molholm S, Lalor EC, Russo NN, Foxe JJ. Atypical cortical representation of peripheral visual space in children with an autism spectrum disorder. Euro J Neurosci. 2013;38(1):2125–2138. doi:10.1111/ejn.12243
22. Delis DC, Kaplan E, Kramer JH, Delis D, Kramer J Delis-Kaplan executive function system (D-KEFS). Examiner’s manual. 2001.
23. Ghawami H, Raghibi M, Tamini BK, Dolatshahi B, Rahimi-Movaghar V. Cross-cultural adaptation of executive function tests for assessments of traumatic brain injury patients in southeast Iran1. Psicología Conductual. 2016;24(3):513.
24. Werner PH, Rini L. Perceptual-Motor Development Equipment: Inexpensive Ideas and Activities. Wiley; 1976.
25. Mammarella IC, Cornoldi C. Sequence and space: the critical role of a backward spatial span in the working memory deficit of visuospatial learning disabled children. Cogn Neuropsychol. 2005;22(8):1055–1068. doi:10.1080/02643290442000509
26. Garcia RB, Mammarella IC, Tripodi D, Cornoldi C. Visuospatial working memory for locations, colours, and binding in typically developing children and in children with dyslexia and non‐verbal learning disability. Br J Health Psychol. 2014;32(1):17–33. doi:10.1111/bjdp.12019
27. Fernández-Prieto I, Caprile C, Tinoco-González D, et al. Pitch perception deficits in nonverbal learning disability. Res Dev Disabil. 2016;59:378–386. doi:10.1016/j.ridd.2016.09.011
28. Alahmadi NA. Cognitive control in children with learning disabilities: neuromarker for deficient executive functions. Neuroreport. 2017;28(11):638–644. doi:10.1097/WNR.0000000000000805
29. Kegel NE. Executive Functioning in Asperger’s Disorder and Nonverbal Learning Disabilities: A Comparison of Developmental and Behavioral Characteristics; 2010.
30. Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cogn Psychol. 2000;41(1):49–100. doi:10.1006/cogp.1999.0734
31. Serrien DJ, Ivry RB, Swinnen SP. Dynamics of hemispheric specialization and integration in the context of motor control. Nat Rev Neurosci. 2006;7(2):160. doi:10.1038/nrn1849
32. Polich J. Updating P300: an integrative theory of P3a and P3b. Clin Neurophysiol. 2007;118(10):2128–2148. doi:10.1016/j.clinph.2007.04.019
33. Budde H, Voelcker-Rehage C, Pietraßyk-Kendziorra S, Ribeiro P, Tidow G. Acute coordinative exercise improves attentional performance in adolescents. Neurosci Lett. 2008;441(2):219–223. doi:10.1016/j.neulet.2008.06.024
34. Picard N, Strick PL. Motor areas of the medial wall: a review of their location and functional activation. Cereb Cortex. 1996;6(3):342–353. doi:10.1093/cercor/6.3.342
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.