")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 13
The Effect of Peer Support on Hope Among Patients Under Hemodialysis
Authors Pasyar N , Rambod M , Jowkar M
Received 2 December 2019
Accepted for publication 25 February 2020
Published 13 March 2020 Volume 2020:13 Pages 37—44
DOI https://doi.org/10.2147/IJNRD.S240756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Nilofar Pasyar,1,2 Masoume Rambod,1,2 Mostafa Jowkar3
1Community Based Psychiatric Care Research Center, Shiraz University of Medical Sciences, Shiraz, Iran; 2Nursing Department, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Shiraz, Iran; 3Student Research Committee, Shiraz University of Medical Sciences, Shiraz, Iran
Correspondence: Masoume Rambod
Nursing Department, School of Nursing and Midwifery, Shiraz University of Medical Sciences, Zand St., Nemazee Sq., Shiraz 7193613119, Iran
Tel +98 71 3647 4254
Fax +98 71 3647 4252
Email [email protected]
Introduction: Providing social support for patients under hemodialysis treatment can reduce their psychological, social, and physical problems. The present study aimed at determining the effect of peer support on hopefulness in patients under hemodialysis.
Methods: This clinical trial with a pre/posttest design was conducted on 128 patients who had referred to the hemodialysis centers of Shiraz University of Medical Sciences in 2019. The patients were randomly divided into an intervention and a control group. The patients in the intervention group were supported by their peers for eight weeks and were provided with the usual care, but the controls were only provided with the usual care. The data were collected using Snyder Hope Scale. Then, the data were entered into the SPSS software, version 18 and were analyzed using independent t-test and paired t-test.
Results: At baseline, the participants in both groups were similar with respect to the mean scores of hope and its subscales (p> 0.05). However, there was a significant difference between the two groups in terms of hope and its subscales eight weeks after the intervention (p< 0.001).
Conclusion: The results confirmed the effect of peer support on increasing hope among the patients under hemodialysis. Peer support in informational, emotional, instrumental, and spiritual forms could create a positive incentive and increase hope among the patients.
Clinical Trial Number: This clinical trial has been registered in the Iranian Registry of Clinical Trials (IRCT20190126042498N1).
Keywords: hope, chronic kidney failure, hemodialysis
Introduction
Chronic renal failure is considered a health issue in modern societies.1 In the past few years, much attention has been paid to this issue in developed countries.2 The final stage of chronic renal failure poses a clinical situation through which a kidney is not able to perform metabolic actions and keep balanced fluid and electrolytes in the body.3 This disease is one of the most common health problems, affecting 2–3% of people around the world.4
Patients under hemodialysis face problems, such as increase in blood urea nitrogen, serum potassium and phosphate levels, and even intradialytic weight gain due to the loss of both kidneys. Dietary and fluid non-adherence are other common issues among hemodialysis patients.5 These patients experience a lower Quality of Life (QoL) in family and health function dimensions compared to those undergoing kidney transplantation.6 They also suffer from insomnia,7 poor sleep quality,8 sexual dysfunction,9 and fatigue.10 Therefore, they have to change their daily life similar to the patients with other chronic diseases.11
Girija and Radha investigated elderly individuals under hemodialysis and stated that their hope levels were lower compared to the adults under the same circumstances.12 However, another study indicated that the hemodialysis patients’ hope levels were higher than the expected average, but the mean score of hope was moderate.13 Hope is a human preventive strategy for adjusting to problems and acute diseases.14 Hope can be a therapeutic, multi-dimensional, dynamic, and powerful factor, playing an important role in coping with disabilities.15 Different studies have shown a positive association between hope and positive emotions16 and self-respect.17 Additionally, negative associations have been revealed between hope and exhaustion18 and negative emotions.17 Snyder et al defined hope as “the capability to derive pathways to desired goals and motivate oneself via agency thinking to use those pathways”.19
Considering various issues in different aspects of QoL in hemodialysis patients and the presence of hope as an adjusting source, Complementary and Integrative Health (CIH) interventions can probably decrease these issues among hemodialysis patients. CIH types include reflexology,20 yoga,21 massage,22 coping skills training,23 and resilience training.24 For example, stress management training as a kind of CIH could enhance hope among patients under hemodialysis.25 Social support is one of the effective interventions in hope among hemodialysis patients, because social support and hope are mediated by symptom distress.26 Social support could be presented as psychological, emotional, and informational tangibility.27 People who received high levels of social support could adjust to life events more efficiently, but those who received low social support levels were more vulnerable.28 Social support also reduced psychological issues, such as anxiety, in chronic diseases.29 It has been stated that social support led to a better life, reduced depression, and resulted in more efficient coping with the disease in patients under hemodialysis, while weak social support could increase mortality.30 Indeed, social support was associated with the hemodialysis patients’ QoL,31 which not only protected them against tensions caused by the illness, but also increased their social-mental coping level.32 It has also been found that low levels of social support increased mortality and reduced QoL in patients under hemodialysis.33 Another study, too, revealed that hope and social support were closely associated with QoL among the patients who suffered from chronic diseases.34 Social interventions and hope could also be effective in the quick healing of the wounds caused by diabetes.35 The association between social support and hope has been approved, as well.36 Accordingly, increase in social support by families could reduce despair in patients with chronic diseases, such as cancer.37
As mentioned before, social support has been reported to be associated with health in patients with chronic diseases. Peer support was also associated with self-care in patients with diabetes.38 Review of the literature revealed no studies on the effect of social support, particularly peer support, on hope among patients under hemodialysis. Only one study investigated the effects of telephone follow-up and self-care education on hope among patients under hemodialysis.39 In another study, cognitive-existential group therapy led to an increase in hope among patients under hemodialysis.40 These two interventions are different from peer support, because peer support is done in the face-to-face manner by a person who is experiencing the disease and is not a healthcare worker, which seems to be more efficient. Thus, the present study aims to determine the effect of peer support on hope among patients under hemodialysis.
Materials and Methods
Design
The present clinical trial with a pre/posttest design was conducted on 128 patients under hemodialysis who had referred to the hemodialysis centers affiliated to Shiraz University of Medical Sciences. The data were collected from April to June 2019. This study was registered in the Iranian Registry of Clinical Trials (approval No. IRCT20190126042498N1) in 4/20/2019.
Setting
This study was conducted in three hemodialysis centers in Namazi and Faghihi hospitals and the 24 hr Imam Reza clinic in Shiraz.
Sample
The target population included the patients under hemodialysis who had active records in the three aforementioned centers. The inclusion criteria were aging 18 years and above, having experienced hemodialysis for at least six months, being on hemodialysis at least twice and at most three times a week, and being willing to participate in the study. The patients suffering from advanced cardiovascular diseases such as heart failure and acute lung deficiency, those with neural sensory disorders such as hearing and visual impairments or cognitive disorders, those addicted to narcotics, and those who had experienced emotional traumas such death of their loved ones and divorce in the past six months were excluded from the study.
The peer support members were selected purposefully by reviewing the list of the patients under hemodialysis in the selected hemodialysis centers affiliated to Shiraz University of Medical Sciences. For this purpose, 13 patients in the peer group who were willing to participate in the study were voluntarily chosen. They had been under hemodialysis treatment for at least six months, were eligible according to the checklist’s criteria, and were able to overcome their disease successfully. The abovementioned checklist assessed skills, abilities, and personal attributes that were derived from the five characteristics of peer support workers, including lived experience of chronic renal failure and hemodialysis, interpersonal communication, critical thinking, teamwork and collaboration, and ethics and reliability.41
Randomization
In order to select the study participants, a table of random numbers was used based on the list of the patients. The participants were divided into an intervention and a control group using the systematic random method based on their referral on odd or even days.
Sample Size
Based on the research by Jadid Milani and Amiri,42 using the Med-Calc statistical software, and considering µ1-µ2=11, standard deviation=18.3, β=90%, α=0.05, and drop out=10%, the sample size was estimated as 128 patients (64 patients in each group).
During the study, four participants in the control group had to be removed due to death and four participants in the intervention group were excluded because they were hospitalized. Finally, 60 patients in the intervention group and 60 ones in the control group remained until the end of the study (Figure 1).
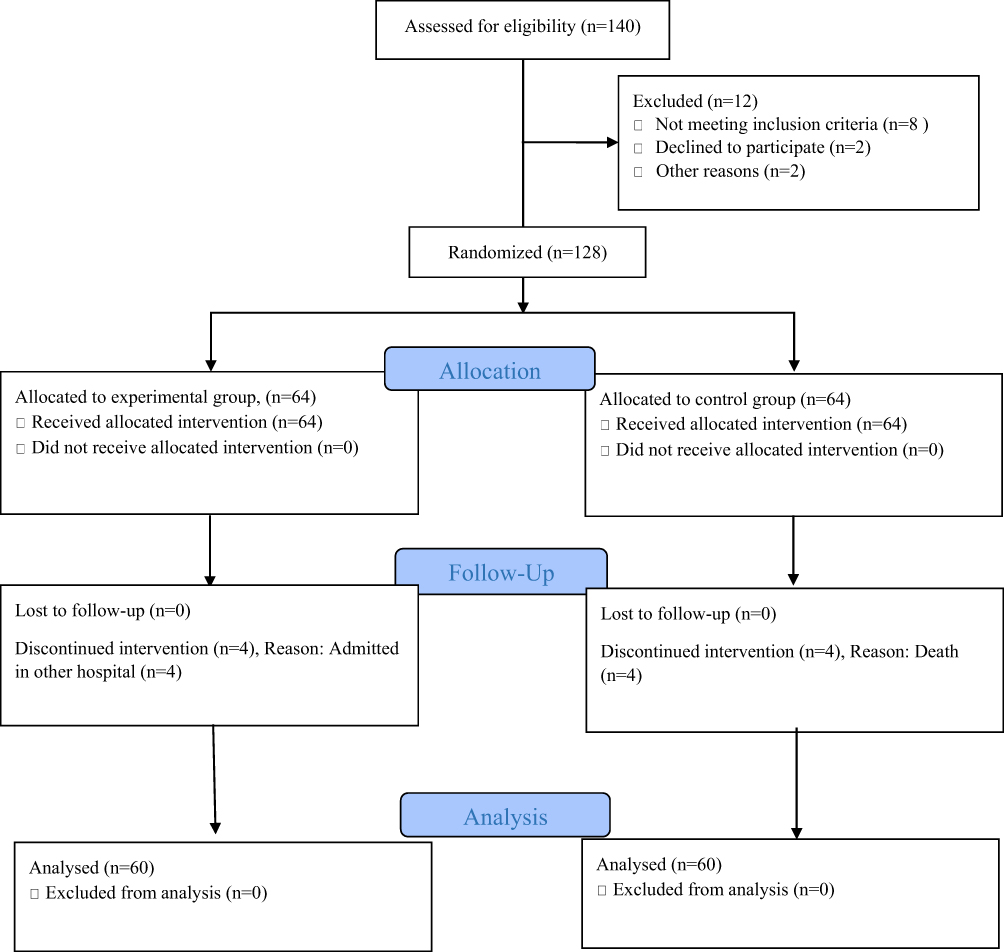 |
Figure 1 CONSORT flow diagram of hemodialysis’ subjects who participated in this study. |
Blinding
The participants’ evaluation was done by the researcher’s assistants who were blind to the intervention and control groups at baseline and immediately after the intervention. The person who did the data analysis also did not have any information regarding the study groups.
Intervention
To provide peer support, 13 individuals were selected through three two-hour training sessions by the researchers. During the first session, concepts such as the importance and advantages of peer support, accurate communication skills, and techniques of tangible and instrumental support were presented. In the second session, a lecture was given on how to present informational support, such as preparation and required care before and after hemodialysis, home activities, and preventive measures for the physical and psychological side effects. Some information about adherence to dietary and fluid limitations in hemodialysis patients and how to care for vascular access, such as an arteriovenous fistula, was also provided in this session. In the third session, topics such as presenting techniques for emotional-psychological support and spiritual support, were explained. Considering emotional-psychological support, methods were described for living a happy life and enjoying life. In addition, in order to perform Benson’s relaxation technique, the participants were asked to sit calmly, close their eyes, entirely relax all their body muscles starting from the sole of their feet upward to head, breath in and out through the nose, listen carefully to the breath sounds, quietly say “one” to themselves, and continue for 20 mins.43 In this session, some information regarding spiritual support, such as relationship with God, praying for oneself and others, reading Quran, hope in God, trust in God, spiritual satisfaction, and thanking the divine blessing, was also given to the peers.44 The participants’ questions were answered during the sessions and their wrong beliefs were corrected by referring to scientific resources. After all, the booklet of the presented information was given to the peers.
The support sessions for the intervention group were held for two hours before the initiation of the dialysis session once a week, which lasted for eight weeks (a total of 16 hrs). For each member of the intervention group, a peer was selected randomly based on their genders. The peers taught and supported the patients in their groups via face-to-face group discussions, question and answer, and lecture method. The misconceptions regarding the contents of the intervention were corrected, as well. Considering the sample size, 12 groups were made each containing five people.
In the first session, the peers asked the patients about their health problems and arranged the next seven sessions based on the priorities of the topics. The topics were different types of social support (emotional, informational, and tangible/instrumental support), the physical and psychological changes and side effects associated with the disease and hemodialysis, such as muscle spasms, insomnia, and itching, and a proper diet. In each session, the attitudes towards coping with the changes and difficulties related to the disease, coping with the present situation, forming a new concept for life, and using others’ experiences and viewpoints were emphasized. Benson’s relaxation technique, training about the disease and the methods for controlling it, and planning for pleasant activities were also pointed in these sessions.
In the peer group, the researcher (the third author of this manuscript) was a facilitator who could enhance the efficiency of the group. He had the duty of facilitating the group discussions, presenting accurate scientific information, and presenting feedbacks to the members by monitoring their obedience. To prevent the disclosure of information, the control and intervention groups were categorized in separate shifts of hemodialysis, so that they could not meet each other. After the intervention, all participants were required to fill out the demographic and clinical characteristics questionnaires and Snyder Hope Scale.
At the end of the study when data analysis was finished, the control group participants were provided with the booklet of the intervention.
Outcome Measures
The outcome measure in this study was hope, which was evaluated at the beginning of the study and eight weeks after the intervention.
Measures
The demographic features questionnaire consisted of five questions about age, gender, education level, marital status, and length of hemodialysis.
The Snyder Adult Hope Scale is used to evaluate a person’s hope status. This scale is based on the Snyder’s cognitive model of hope defining hope as “a positive motivational state that is based on an interactively derived sense of successful agency (goal-directed energy) and pathways (planning to meet goals)”. This scale consists of 12 maxims and two subscales of agency and pathways thinking.17 The test-taker should identify the amount of agreement and disagreement on an eight-point Likert scale ranging from totally agree to totally disagree. The score of the test can range from 8 to 64. The internal consistency of the Hope Scale was reported as 0.84 and its test-retest reliability was 0.80. Higher values were obtained in periods more than eight to ten weeks. The internal consistency of the agency subscale was 0.71–0.76 and that of the pathways subscale was 0.63–0.80.45 In a study by Sadat Kiafar et al, the Cronbach’s alpha coefficient was found to be 0.80 for the whole scale, 0.78 for the agency subscale, and 0.61 for the pathways subscale.46
Ethical Considerations
All research procedures were done based on Helsinki Declaration after being approved by the Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.REC.1398.93). Written informed consent forms for taking part in the research were obtained from all participants. Accordingly, the participants were provided with explanation about the advantages of the study and were assured that they could withdraw from the study at any time. In order to keep the confidentiality of the participants’ information, the questionnaires were encoded.
Data Analysis
All data analyses were carried out using the SPSS software, version 18. Descriptive statistics were used. Paired t-test was employed to compare the two groups regarding the mean score of hope before and after the intervention. Independent t-test was also used to compare the mean score of hope in the two groups before and after the intervention.
Results
The majority of the participants in the intervention and control groups were male and married. Additionally, most of the participants in both groups had secondary and high school degrees. The mean age of the participants was 54.93 years, ranging from 29 to 70 years. The mean age of the patients was 56.57 years (SD=9.54) in the intervention group and 53.30 years (SD=10.01) in the control group. Moreover, the length of dialysis was 30.60 months (SD=15.53) in the intervention group and 36.13 months (15.23) in the control group. The results showed no significant difference between the two groups regarding gender, marital status, education level, age, and length of dialysis (p>0.05) (Table 1).
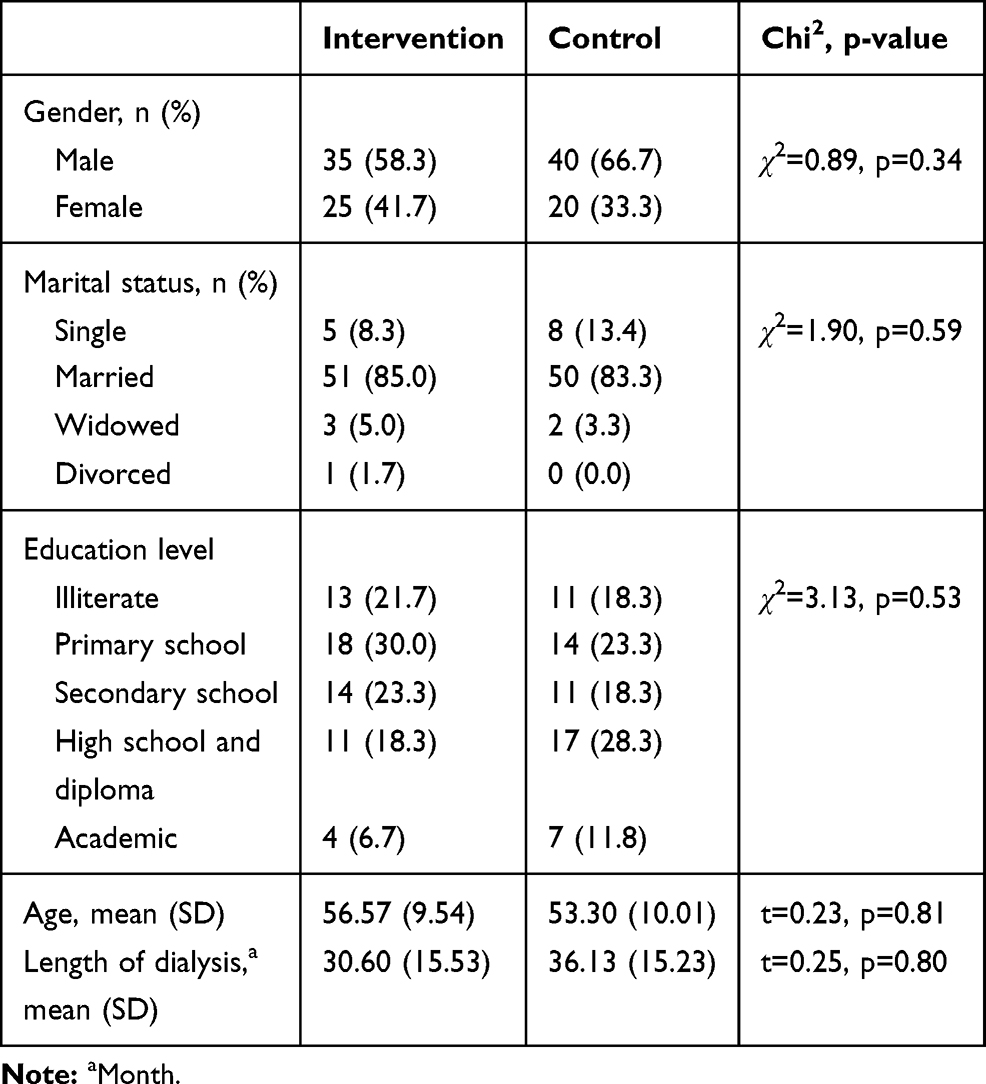 |
Table 1 The Demographic and Clinical Characteristics of the Participants in the Intervention and Control Groups |
Before the intervention, the mean score of hope was 62.4 (SD=6.13) in the intervention group and 62.03 (SD=4.38) in the control group. The results revealed no significant difference between the two groups regarding the mean scores of hope and its subscales before the intervention. However, a significant difference was observed between the two groups concerning the mean scores of hope and its subscales after the intervention (Table 2). The effect size was measured by Cohen’s d, which was equal to 1.74. According to Cohen, d=0.2, 0.5, and 0.8 represented small, medium, and large effect sizes, respectively.47 Therefore, the effect size of this study was large enough.
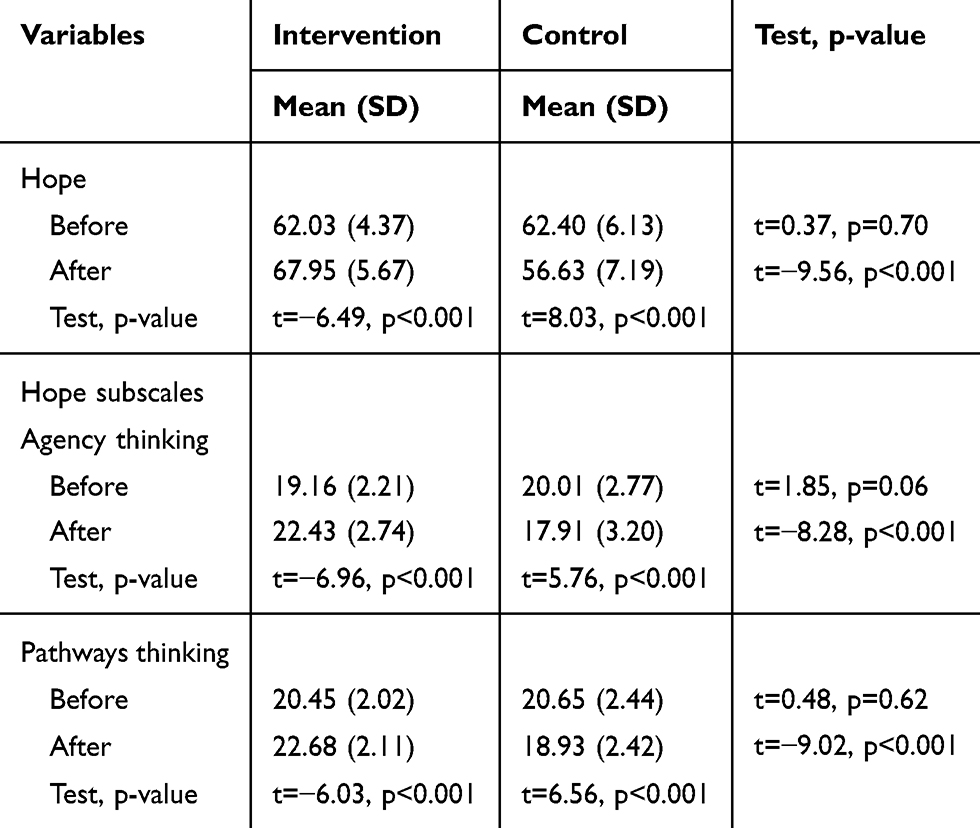 |
Table 2 Comparison of the Mean Scores of Hope and Its Subscales in the Two Groups Before and After the Intervention |
Discussion
This study aimed to determine the effect of peer support on hope in patients under hemodialysis. The results revealed a significant difference between the two groups regarding the mean score of hope after the intervention. Accordingly, the hemodialysis patients who had received the peer support had a significantly higher level of hope after the intervention. In another study, social support and coping style were found to be associated with symptom distress.26 Social support can help a patient select a positive coping strategy. This enhances the hope status by reducing symptom distress. It was also indicated that if an individual received peer and network support, s/he could deal with the difficult situations caused by the disease and, consequently, enjoy an enhanced emotional condition, which could in turn increase one’s hope level.48
Ruston et al stated that hope could be effective in the psychological characteristics of the patients with cancer.49 Therefore, hope is a powerful coping mechanism in patients with chronic diseases, and people who are hopeful can tolerate the trauma caused by the disease more easily. Hope is also a necessary and crucial element of survival and life expectancy.50
The effect size of the present study was 1.74, which was large enough. However, the effects size of a hope-based intervention for colorectal cancer was small in a previous study.51 Based on the results, utilizing peer groups as an educational-supportive human resource and strong intervention is warranted in addition to the treatment team. This is of particular importance due to the tangibility of hemodialysis in the peers’ personal life, effective control of the disease, convenient communication, and the powerful effect of training. All these can encourage the patients to discuss their concerns in groups and obtain the required information more easily. Moreover, the patients learn strategies on how to cope with the disease from their peers and their hope level increases as their knowledge expands. Furthermore, the use of peer support groups provides a powerful and cost-effective human resource for managing the disease.
Limitations
One of the limitations of this study was that the third author of the manuscript participated as a facilitator. This might have yielded interventional bias, resulting in better outcomes than expected.
Conclusion
The results of this study showed that offering social support by peers could increase the hope level among the patients under hemodialysis. Hence, this intervention could be effective in promoting the individuals’ internal forces and hope levels.
Suggestions for Future Studies
Future studies are recommended to be conducted on other chronic diseases, such as cancer and diabetes.
Data Sharing Statement
Another study-related document will be made available in the format of SPSS software. As the data were unlinked, the data will be available by contact to email of Pasyar N ([email protected]).
Acknowledgment
The present study was extracted from Mostafa Jowkar’s M.Sc. thesis in Nursing. The researchers wish to express their gratitude to the Vice-Chancellor for Research Affairs at Shiraz University of Medical Sciences for providing financial support for this research project (grant No. 18651). They would also like to thank Ms. A. Keivanshekouh at the Research Improvement Center of Shiraz University of Medical Sciences for improving the use of English in the manuscript. Finally, they would like to thank all participants for taking part in the research.
Disclosure
The authors declare no conflicts of interest in this project.
References
1. Pasyar N, Rambod M, Sharif F, Rafii F, Pourali-Mohammadi N. Improving adherence and biomedical markers in hemodialysis patients: the effects of relaxation therapy. Complement Ther Med. 2015;23(1):38–45. doi:10.1016/j.ctim.2014.10.011
2. Viazzi F, Bonino B, Cappadona F, Pontremoli R. Renin–angiotensin–aldosterone system blockade in chronic kidney disease: current strategies and a look ahead. Intern Emerg Med. 2016;11(5):627–635. doi:10.1007/s11739-016-1435-5
3. Givi M. Durability of effect of massage therapy on blood pressure. Int J Prev Med. 2013;4(5):511.
4. Hill NR, Fatoba ST, Oke JL, et al. Global prevalence of chronic kidney disease–a systematic review and meta-analysis. PLoS One. 2016;11(7):e0158765. doi:10.1371/journal.pone.0158765
5. Rambod M, Peyravi H, Shokrpour N, Sareban MT. Dietary and fluid adherence in Iranian hemodialysis patients. Health Care Manag (Frederick). 2010;29(4):359–364. doi:10.1097/HCM.0b013e3181fa0691
6. Rambod M, Shabani M, Shokrpour N, Rafii F, Mohammadalliha J. Quality of life of hemodialysis and renal transplantation patients. Health Care Manag (Frederick). 2011;30(1):23–28. doi:10.1097/HCM.0b013e3182078ab6
7. Rambod M, Pourali-Mohammadi N, Pasyar N, Rafii F, Sharif F. The effect of Benson’s relaxation technique on the quality of sleep of Iranian hemodialysis patients: a randomized trial. Complement Ther Med. 2013;21(6):577–584. doi:10.1016/j.ctim.2013.08.009
8. Otaghi M, Bastami M, Borji M, Tayebi A, Azami M. The effect of continuous care model on the sleep quality of hemodialysis patients. Nephrourol Mon. 2016;8(3):35467. doi:10.5812/numonthly.35467
9. Edey MM. Male sexual dysfunction and chronic kidney disease. Front Med. 2017;4:1–10. doi:10.3389/fmed.2017.00032
10. Zyga S, Alikari V, Sachlas A, et al. Assessment of fatigue in end stage renal disease patients undergoing hemodialysis: prevalence and associated factors. Med Arh. 2015;69(6):376–380. doi:10.5455/medarh.2015.69.376-380
11. Pasyar N, Sharif F, Rakhshan M, Nikoo MH, Navab E. Changes in daily life of Iranian patients with implantable cardioverter defibrillator: a qualitative study. Int J Community Based Nurs Midwifery. 2017;5(2):134–143.
12. Orlandi FD, Pepino BG, Pavarini SC, Santos DA, Mendiondo MS. The evaluation of the level of hope of elderly chronic kidney disease patients undergoing hemodialysis. Rev Esc Enferm USP. 2012;46(4):900–905. doi:10.1590/S0080-62342012000400017
13. Ottaviani AC, Souza ÉN, Drago ND, Mendiondo MS, Pavarini SC, Orlandi FD. Hope and spirituality among patients with chronic kidney disease undergoing hemodialysis: a correlational study. Rev Lat Am Enfermagem. 2014;22(2):248–254. doi:10.1590/0104-1169.3323.2409
14. Scioli A, Scioli-salter ER, Sykes K, Anderson C, Fedele M. The positive contributions of hope to maintaining and restoring health: an integrative, mixed-method approach. J Posit Psychol. 2016;11(2):135–148. doi:10.1080/17439760.2015.1037858
15. Erdley-kass SD, Kass DS, Gellis ZD, Bogner HA, Berger A, Perkins RM. Using problem-solving therapy to improve problem-solving orientation, problem-solving skills and quality of life in older hemodialysis patients. Clin Gerontol. 2018;41(5):424–437. doi:10.1080/07317115.2017.1371819
16. Esen B, Kahvecioglu S, Atay AE, et al. Evaluation of relationship between sexual functions, depression and quality of life in patients with chronic kidney disease at predialysis stage. Ren Fail. 2015;37(2):262–267. doi:10.3109/0886022X.2014.990348
17. Snyder CR, Sympson SC, Ybasco FC, Borders TF, Babyak MA, Higgins RL. Development and validation of the state hope scale. J Pers Soc Psychol. 1996;70(2):321. doi:10.1037//0022-3514.70.2.321
18. Snyder CR. Hope theory: rainbows in the mind. Psychol Inq. 2002;13(4):249–275. doi:10.1207/S15327965PLI1304_01
19. Snyder CR, Harris C, Anderson JR, et al. The will and the way: development and validation of an indivitual-differences measure of hope. J Pers Soc Psychol. 1991;60:570–585. doi:10.1037/0022-3514.60.4.570
20. Rambod M, Pasyar N, Shamsadini M. The effect of foot reflexology on fatigue, pain, and sleep quality in lymphoma patients: a clinical trial. Eur J Oncol Nurs. 2019;43:101678. doi:10.1016/j.ejon.2019.101678
21. Pasyar N, Tashnizi NB, Mansouri P, Tahmasebi S. Effect of yoga exercise on the quality of life and upper extremity volume among women with breast cancer related lymphedema: a pilot study. Eur J Oncol Nurs. 2019;42:103–109. doi:10.1016/j.ejon.2019.08.008
22. Pasyar N, Rambod M, Kahkhaee FR. The effect of foot massage on pain intensity and anxiety in patients having undergone a tibial shaft fracture surgery: a randomized clinical trial. J Orthop Trauma. 2018;32(12):e482–6. doi:10.1097/BOT.0000000000001320
23. Edraki M, Rambod M, Molazem Z. The effect of coping skills training on depression, anxiety, stress, and self-efficacy in adolescents with diabetes: a randomized controlled trial. Int J Community Based Nurs Midwifery. 2018;6(4):324.
24. Torabizadeh C, Asadabadi Poor Z, Shaygan M. The Effects of resilience training on the self-efficacy of patients with type 2 diabetes: a randomized controlled clinical trial. Int J Community Based Nurs Midwifery. 2019;7(3):211–221. doi:10.30476/IJCBNM.2019.44996
25. Poorgholami F, Abdollahifard S, Zamani M, Jahromi MK, Jahromi ZB. The effect of stress management training on hope in hemodialysis patients. Glob J Health Sci. 2016;8(7):165. doi:10.5539/gjhs.v8n7p165
26. Gao Y, Zhou Y, Guo CX, Zhao JF. The relationship among hope, symptom distress, social support, coping style and monthly income in maintenance hemodialysis patients: a structural equation model. Int J Clin Exp Med. 2016;9(10):19717–19724.
27. Sousa H, Ribeiro O, Paúl C, et al. Social support and treatment adherence in patients with end‐stage renal disease: a systematic review. Semin Dial. 2019;32(6):562–574. doi:10.1111/sdi.12831
28. Yu HD, Petrini MA. The HRQoL of Chinese patients undergoing haemodialysis. J Clin Nurs. 2010;19(5‐6):658–665. doi:10.1111/j.1365-2702.2009.03071.x
29. Torabizadeh C, Bostani S, Yektatalab S. Comparison between the effects of muscle relaxation and support groups on the anxiety of nursing students: a randomized controlled trial. Complement Ther Clin Pract. 2016;25:106–113. doi:10.1016/j.ctcp.2016.09.001
30. Hamilton AJ, Caskey FJ, Casula A, Inward CD, Ben-shlomo Y. Associations with wellbeing and medication adherence in young adults receiving kidney replacement therapy. Clin J Am Soc Nephrol. 2018;13(11):1669–1679. doi:10.2215/CJN.02450218
31. Rambod M, Rafii F. Perceived social support and quality of life in Iranian hemodialysis patients. J Nurs Scholarsh. 2010;42(3):242–249. doi:10.1111/j.1547-5069.2010.01353.x
32. Jiang H, Wang L, Zhang Q, et al. Family functioning, marital satisfaction and social support in hemodialysis patients and their spouses. Stress Health. 2015;31(2):166–174. doi:10.1002/smi.2541
33. Pan K-C, Hung S-Y, Chen C-I, Lu C-Y, Shih M-L, Huang C-Y. Social support as a mediator between sleep disturbances, depressive symptoms, and health-related quality of life in patients undergoing hemodialysis. PLoS One. 2019;14(4):e0216045. doi:10.1371/journal.pone.0216045
34. Li MY, Yang YL, Liu L, Wang L. Effects of social support, hope and resilience on quality of life among Chinese bladder cancer patients: a cross-sectional study. Health Qual Life Outcomes. 2016;14(1):73. doi:10.1186/s12955-016-0481-z
35. Peker A, Karaöz S. The effects of social support and hope in the healing of diabetic foot ulcers treated with standard care. Popul Health Manag. 2017;20(6):507. doi:10.1089/pop.2017.0010
36. Denewer A, Farouk O, Mostafa WA, Elshamy K. Social support and hope among Egyptian women with breast cancer after mastectomy. Breast Cancer (Auckl). 2011;5:93–103. doi:10.4137/BCBCR.S6655
37. Madani H, Pourmemari M, Moghimi M, Rashvand F. Hopelessness, perceived social support and their relationship in Iranian patients with cancer. Asia Pac J Oncol Nurs. 2018;5(3):31. doi:10.4103/apjon.apjon_5_18
38. Doe E. An analysis of the relationships between peer support and diabetes outcomes in adolescents with type 1 diabetes. J Health Psychol. 2018;23(10):1356–1366. doi:10.1177/1359105316656228
39. Poorgholami F, Mansoori P, Montaseri Z, Najafi K. Effect of self care education with and without telephone follow-up on the level of hope in renal dialysis patients: a single-blind randomized controlled clinical trial. Int J Community Based Nurs Midwifery. 2016;4(3):256.
40. Bahmani B, Najjar MM, Sayyah M, Shafi-abadi A, Kashani HH. The effectiveness of cognitive-existential group therapy on increasing hope and decreasing depression in women-treated with haemodialysis. Glob J Health Sci. 2016;8(6):219. doi:10.5539/gjhs.v8n6p219
41. Mahajan S, Sunderland K, Mishkin W. Peer Leadership Group, Mental Health Commission of Canada. Guidelines for the Practice and Training of Peer Support. Calgary, AB: Mental Health Commission of Canada; 2013. Retrieved from: http://www.mentalhealthcommission.ca.
42. Jadid Milani M, Amiri P. The effects of peer support groups on mental health of hemodialysis patients. Iran J Nurs. 2015;28(96):40–49. doi:10.29252/ijn.28.96.40
43. Rambod M, Sharif F, Pourali-mohammadi N, Pasyar N, Rafii F. Evaluation of the effect of Benson’s relaxation technique on pain and quality of life of haemodialysis patients: a randomized controlled trial. Int J Nurs Stud. 2014;51(7):964–973. doi:10.1016/j.ijnurstu.2013.11.004
44. Rambod M, Sharif F, Molazem Z, Khair K. Spirituality experiences in hemophilia patients: a phenomenological study. J Relig Health. 2019;58(3):992–1002. doi:10.1007/s10943-018-0621-3
45. Snyder CR, Lopez SJ. Oxford Handbook of Positive Psychology. Oxford library of psychology; 2009.
46. Sadat Kiafar M, Kareshki H, Hashemi F. The role of hope components and optimism on academic motivation of graduate students of Ferdowsi University and Mashhad University of Medical Sciences. Iran J Med Educ. 2014;14(6):517–526.
47. Sullivan GM, Feinn R. Using effect size—or why the P value is not enough. J Grad Med Educ. 2012;4(3):279–282. doi:10.4300/JGME-D-12-00156.1
48. Karadag E, Kilic SP, Metin O. Relationship between fatigue and social support in hemodialysis patients. Nurs Health Sci. 2013;15(2):164–171. doi:10.1111/nhs.12008
49. Rustøen T, Cooper BA, Miaskowski C. The importance of hope as a mediator of psychological distress and life satisfaction in a community sample of cancer patients. Cancer Nurs. 2010;33(4):258–267. doi:10.1097/NCC.0b013e3181d6fb61
50. Bergerot CD, Battle D, Bergerot PG, et al. Sources of frustration among patients diagnosed with renal cell carcinoma. Front Oncol. 2019;9:11. doi:10.3389/fonc.2019.00011
51. Ho SM, Ho JW, Pau BK, Hui BP, Wong RS, Chu AT. Hope-based intervention for individuals susceptible to colorectal cancer: a pilot study. Fam Cancer. 2012;11(4):545–551. doi:10.1007/s10689-012-9545-3
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.