")
Back to Journals » Psychology Research and Behavior Management » Volume 15
The Effect of Emotion Regulation on Non-Suicidal Self-Injury Among Adolescents: The Mediating Roles of Sleep, Exercise, and Social Support
Authors Lan Z , Pau K , Md Yusof H, Huang X
Received 25 February 2022
Accepted for publication 26 May 2022
Published 7 June 2022 Volume 2022:15 Pages 1451—1463
DOI https://doi.org/10.2147/PRBM.S363433
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Zhensong Lan,1,2 Kee Pau,3 Hapsah Md Yusof,3 Xuefang Huang4
1School of Public Administrations, Hechi University, Hechi, Guangxi, 546300, People’s Republic of China; 2National Child Development Research Centre, Sultan Idris Education University, Tanjong Malim Perak, 35900, Malaysia; 3Department of Psychology and Counseling, Faculty of Human Development, Sultan Idris Education University, Tanjong Malim Perak, 35900, Malaysia; 4College of Humanities & Social Sciences, Huazhong Agricultural University, Wuhan, Hubei, 430070, People’s Republic of China
Correspondence: Kee Pau, Director of Counseling Center, Bangunan Bitarasiswa, Tingkat Bawah, Kampus Sultan Abdul Jalil Shah Universiti Pendidikan Sultan Idris, Tanjong Malim Perak, 35900, Malaysia, Tel +60 167228023, Email [email protected]
Purpose: To explore the relationship between adolescents’ emotion regulation ability and non-suicidal self-injury (NSSI) behavior and the role of sleep, exercise, and social support in this relationship.
Methods: A total of 2573 adolescents were investigated with the Cognitive Emotion Regulation Scale, the Social Support Scale for Children and Adolescents, the Ottawa Self-Injury Questionnaire, and the Self-Made Living Condition Questionnaire, and path analysis was conducted based on the structural equation model (SEM).
Results: 1) There was a significant correlation between emotion regulation ability and NSSI behavior; 2) sleep and social support played a mediating role between emotion regulation ability and NSSI behavior; and 3) sleep modulated the direct effect of negative emotion regulation ability on NSSI, while exercise modulated the direct effect of positive emotion regulation ability on NSSI, which indicated that sleep and exercise could effectively alleviate NSSI behavior caused by the lack of emotion regulation in adolescents.
Keywords: emotion regulation ability, non-suicidal self-injury, NSSI, structural equation model, SEM
Introduction
Adolescence is a transitional period in one’s physical, cognitive, social, and emotional development.1 Adolescents are in a critical period of physical and psychological growth, turbulence, and chaos.2 During this period, they are faced with psychological and behavioral problems such as identity development, the desire to be accepted and recognized by a group, and adaptation to social life.3,4 Non-suicidal self-injury (NSSI) is an act in which an individual intentionally harms their own body tissue, but without suicidal intent.5 In western countries such as European nations, North America or Australia, the incidence of NSSI behavior of adolescents ranges from 6.2% to 45%.6–10 In China, the incidence of NSSI behavior among adolescents is 5.4%-57.4%.11–15 The NSSI problem of Chinese adolescents is serious and needs to be addressed urgently. Therefore, it is necessary to strengthen and widen research to provide support for the prevention and intervention of NSSI behavior of adolescents, and to promote the development of their mental health.
The Relationship Between Emotion Regulation Ability and NSSI
The experiential avoidance model believes that the main function of NSSI is to regulate negative emotional experience,16 or that individuals adopt NSSI behavior to avoid negative emotional experiences.17 Emotion regulation refers to the individual’s recognition, understanding, and acceptance of their own emotional experience, and flexible use of strategies for appropriate behavior.18 When encountered with stressful events, NSSI people have problems experiencing and expressing their emotions, and are more likely to produce a higher level of emotional arousal. They are not able to exercise effective strategies to adjust their behavioral responses, which produces NSSI behavior.
Victor and Klonsky (2013) found that individuals with NSSI behavior suffered greater negative emotions than those without NSSI behavior.19 In terms of problem avoidance behavior, people tend to use NSSI as an effective coping strategy due to the lack of other coping strategies.20 In terms of coping behavior, those with repetitive NSSI are highly likely to use avoidance or emotion-focused coping styles.21
Therefore, the following hypothesis is proposed:
H1: emotion regulation ability will affect adolescent NSSI behavior.
The Mediating Effect of Sleep
Sleep quality is often overlooked as a predictor of NSSI behavior. Nighttime sleep is a period when adolescents undergo many psychological and biological changes in their bodies, which may lead to sleep deprivation.22 The key mechanism by which sleep deprivation affects mental health is emotional dysregulation. Studies have shown that individual transformations occurring in the central nervous system of adolescents may not necessarily have a direct impact on sleep patterns, but are highly likely to alter or influence mood or emotion regulation activities, which are critical to the interaction of adolescent sleep patterns.23
Sleep deprivation may ultimately lead to psychological and emotional instability in adolescents,24 thereby limiting their ability to confront certain emotional weaknesses.25 Adolescents can regulate their moods or emotions in many ways, and sleep deprivation may make them vulnerable to various measures of adaptive regulation of emotional distress, such as deliberately regulating their emotions by engaging in NSSI or compensating for sleep deprivation through NSSI behavior.26 Sleep quality mediates the relationship between depressed mood and NSSI behavior.27
Multiple sleep variables, such as short sleep time, insomnia or frequent nightmares, are associated with and are important risk factors for NSSI behavior.28,29 Studies have found that most individuals with NSSI behavior have sleep difficulties.30,31 The researchers also demonstrated through logistic regression models that poor sleep quality was associated with NSSI (OR=2.18, 95% CI=1.37–3.47), and that it affected the mental health of adolescents.32–35 Park, Yoo and Kim also found that adolescents with sleep problems were highly likely to have NSSI than those who slept well (OR=1.58, p=0.03), and that less than four hours of sleep increased the likelihood of NSSI.36
NSSI may also be a complex and serious challenge that may not be only solved by nighttime sleep. Sleep deprivation in adolescents can impair mood or emotional regulation, which is a key role of NSSI. It is necessary to further explore whether there is a direct correlation between sleep quality and individual emotion regulation ability and NSSI behavior.
Therefore, the following hypotheses are proposed:
H2: sleep has an impact on adolescents’ NSSI behavior. H3: sleep is related to adolescents’ emotion regulation. H4: sleep quality plays a mediating role between emotion regulation and adolescents’ NSSI behavior.
The Mediating Effect of Exercise
Sports may affect emotional regulation, thereby affecting NSSI behavior.34,37–39 The level of physical exercise may affect an individual’s hormonal balance, and subsequently, their emotional state.40,41 A study explored the association between exercise and NSSI, and established that exercise is inversely related to NSSI frequency,42 and exercise interventions of different intensities can reduce physical and mental health problems.43 There may be an association between physical inactivity and depression, which, in turn, affects NSSI.42
Lack of exercise may be associated with NSSI behavior, and may affect sleep quality.41 Long-term sleep deprivation can lead to serious mental health problems.44 Kline pointed out that insufficient sleep may affect physical activity.45 Therefore, the relationship between sleep and exercise is bidirectional.46 The interaction between sleep and physical activity may regulate NSSI behavior in adolescents.47
Physical exercise is a non-pharmaceutical intervention for sleep disorders, which does not incur many costs.48 This approach is also readily available, and provides a complementary approach to improving sleep quality and NSSI behavior, which can be used as a reference for future interventions for adolescent NSSI behavior. Therefore, it is necessary to further analyze how physical exercise affects the relationship between emotion regulation ability and NSSI behavior.
Therefore, the following hypotheses are proposed:
H5: exercise will affect adolescents’ NSSI behavior. H6: exercise is related to adolescents’ emotion regulation. H7: exercise level plays a mediating role between emotion regulation and adolescents’ NSSI behavior.
The Moderating Effect of Social Support
Social support may influence NSSI behavior, and increasing social support may decrease the likelihood of NSSI behavior.49 NSSI behavior may be influenced by peers, and peer relationships play an important role in the growth and development of adolescents. Positive peer relationships5 or negative events in peer relationship50 may influence the occurrence of NSSI behavior in adolescents. However, poor peer relationships may also contribute to increased NSSI behavior.51 For example, specific social behavior induction among peers,52 discussion or encouragement of this behavior with peers,53 and risk-taking behavior via imitation learning or ostentation54 may also lead to the occurrence of NSSI behavior.
School or social environment may affect social adaptability of adolescents, which may lead to NSSI behavior occurrence in adolescents.3,55,56 Positive school functioning has a protective effect on NSSI, while future NSSI behavior is highly likely in students who feel disconnected from or dissatisfied with school, and those who feel that teachers are unfair.57 Positive family relationships may form protective factors that prevent or buffer the effects of adolescents’ NSSI behaviors.58–61 Peer and family support may moderate interpersonal problems and mitigate NSSI behaviors. For example, Adrian et al established structural equation models (SEM) to show that emotional dysregulation is the underlying process that puts adolescents at risk for NSSI, and mediated the effects of interpersonal problems through home and peer domains.62 Parental bonding, bonding with non-parent adults, and school safety emerged as strong protective factors.61
Therefore, the following hypotheses are proposed:
H8: social support will impact adolescents’ NSSI behavior. H9: social support is significantly related to adolescents’ emotion regulation. H10: the level of social support plays a mediating role between emotion regulation and adolescents’ NSSI behavior.
Methods
Study Participants
A total of 2573 middle school students from 48 classes (24 junior high schools and 24 senior high schools) in 12 middle schools in Guangxi were selected by offline cluster stratified sampling. Questionnaires were distributed and collected by trained head teachers, psychological teachers and professional students on the spot. In this study, 2400 questionnaires were collected, and 2344 valid questionnaires were obtained after deleting the invalid questionnaires such as those with consistent responses and multiple missing answers, with an effective rate of 97.67%. There were 1142 boys and 1202 girls in the survey. The participants were between 11 and 19 years of age (15.76 ± 2.58). Of them, 411 were in the seventh grade, 427 in the eighth grade, 332 in the ninth grade, 466 in the tenth grade, 447 in the eleventh grade and 261 in the twelfth grade.
Before the questionnaire survey, the parents of the interviewees were informed of the contents of the survey by the investigator and their head teacher, and their consent was obtained. Simultaneously, the interviewees were briefed on the subject, content, and the use of the questionnaire, and informed consent was obtained (the survey could also be terminated at any time according to their wishes). All the interviewees were required to maintain anonymity to protect their privacy. This study was reviewed and approved by the Human Research Ethics Committee of the Sultan Idris University of Education, Malaysia.
Measuring Instrument
Cognitive Emotion Regulation Questionnaire (CERQ)
It was compiled by Granifski after synthesizing the previous literature related to emotional coping theory. Zhu et al revised and tested the reliability and validity of the Chinese version of Cognitive Emotion Regulation Questionnaire (CERQ).63 There are 36 items in the scale, including two dimensions of positive regulation (including five items of acceptance, positive refocusing, positive reappraisal, rational thinking, and refocus on planning, scored in the opposite direction) and negative regulation (four contents of rumination, self-censure, censure of others, and catastrophizing), scored on five points; the higher the score, the lower the level of regulation. In this study, the combined reliability (CR) of the negative cognitive emotion regulation subscale was 0.95, the convergent validity (AVE) was 0.56, and there was good fit index of the confirmatory factor test: χ2/DF = 12.24, CFI =0.94, TLI =0.92, RMSEA =0.069. The positive cognitive emotion regulation subscale had a combined reliability (CR) of 0.96, convergent validity (AVE) of 0.53, and good fit measures for confirmatory factor tests: χ2/DF = 15.03, CFI =0.90, TLI =0.88, RMSEA =0.077.
Child and Adolescent Social Support Scale
The Chinese version of the Child and Adolescent Social Support Scale was first compiled by Malecki and Demaray (updated in 2000) and revised by Luo, Chen and Mu.64 The scale consists of 60 items, including five sub-scales (parents, teachers, classmates, friends, and school people). A six-point score was used; the higher the score, the higher the degree of support. In this study, the combined reliability (CR) was 0.98, the convergent validity (AVE) was 0.73, and there was good fit index of the confirmatory factor test: χ2/DF = 14.88, CFI =0.95, TLI =0.94, RMSEA =0.077.
Ottawa Self-Injury Inventory
The Chinese version of the Ottawa Self-Injury Inventory was revised by Cloutier and Nixon on the basis of Epstein, and revised and tested by Zhang et al52,65 The questionnaire consists of 28 items, including the frequency of NSSI, the location of injury, the way of injury, impulse feeling, motivation, the role of releasing negative emotions, potential addiction characteristics and resistance strategies, and seeking treatment. Likert Level 2 (Yes, No) and Level 5 (0, 1, 2, 3, 4) assessment methods were adopted. In this study, the combined reliability (CR) was 0.91, the convergent validity (AVE) was 0.72, and there was good fit index of the confirmatory factor tests: χ2/df=14.23, CFI=0.99, TLI=0.99, RMSEA=0.075.
Living Condition Questionnaire
A self-designed Living Condition Questionnaire was used. Sleep status comprises sleep duration, sleep environment, sleep quality, and sleep effect, which is scored on five points, and the higher the score, the better the sleep quality. Physical exercise status consists of exercise duration, interest, exercise intensity, and exercise effect, which is scored on five points. The higher the score, the better the exercise level. In this study, the combined reliability of the sleep status questionnaire was 0.61, the convergent validity (AVE) was 0.32, and the confirmatory factor analysis fit index was good: χ2/df=4.31, CFI=0.99, TLI=0.98, RMSEA=0.038. The combined reliability of the physical exercise status questionnaire was 0.68, the convergent validity (AVE) was 0.34, and the confirmatory factor analysis fit index was good: χ2/df=17.87, CFI=0.98, TLI=0.93, RMSEA=0.085.
Data Analysis
SPSS 25.0 (IBM, Armonk, NY, USA) was used for descriptive statistics and correlation analysis. Amos 23.0, SPSS 25.0 and its plug-in Process v3.5 (Andrew F. Hayes) were used to test reliability and validity. Common method bias test, confirmatory factor analysis, mediating effect, and moderating effect tests were conducted.
Results
Common Method Bias Test
Harman’s single factor was used to test the common method bias of the questionnaire used in this study, and the remaining items were analyzed by factor analysis. The data results showed 18 common factors whose eigenvalues were greater than one, and the first common factor explained 21.90% of the total variance. It was significantly less than the critical value of 40%, so there was no common method bias effect in this study.
Structural Equation Model Analysis
Path Analysis
Emotion experiential avoidance theory suggests that adolescents’ emotion regulation is related to NSSI behavior. In addition, research has demonstrated that parental support, sleep quality, and exercise level can affect the emotional regulation ability and NSSI behavior of adolescents. This study establishes an SEM to test the relationship between adolescent emotion regulation, parental support, sleep quality, exercise level, and NSSI behavior (see Figure 1). The results show that the fitting indexes of the SEM meet the standard: χ2/DF = 7.70, CFI = 0.90, TLI = 0.88, SRMR = 0.03, RMSEA = 0.053 (< 0.08). By observing the path coefficients CR and P among the variables in the SEM, the results showed that the 11 hypothetical paths in the model were supported (see Table 1).
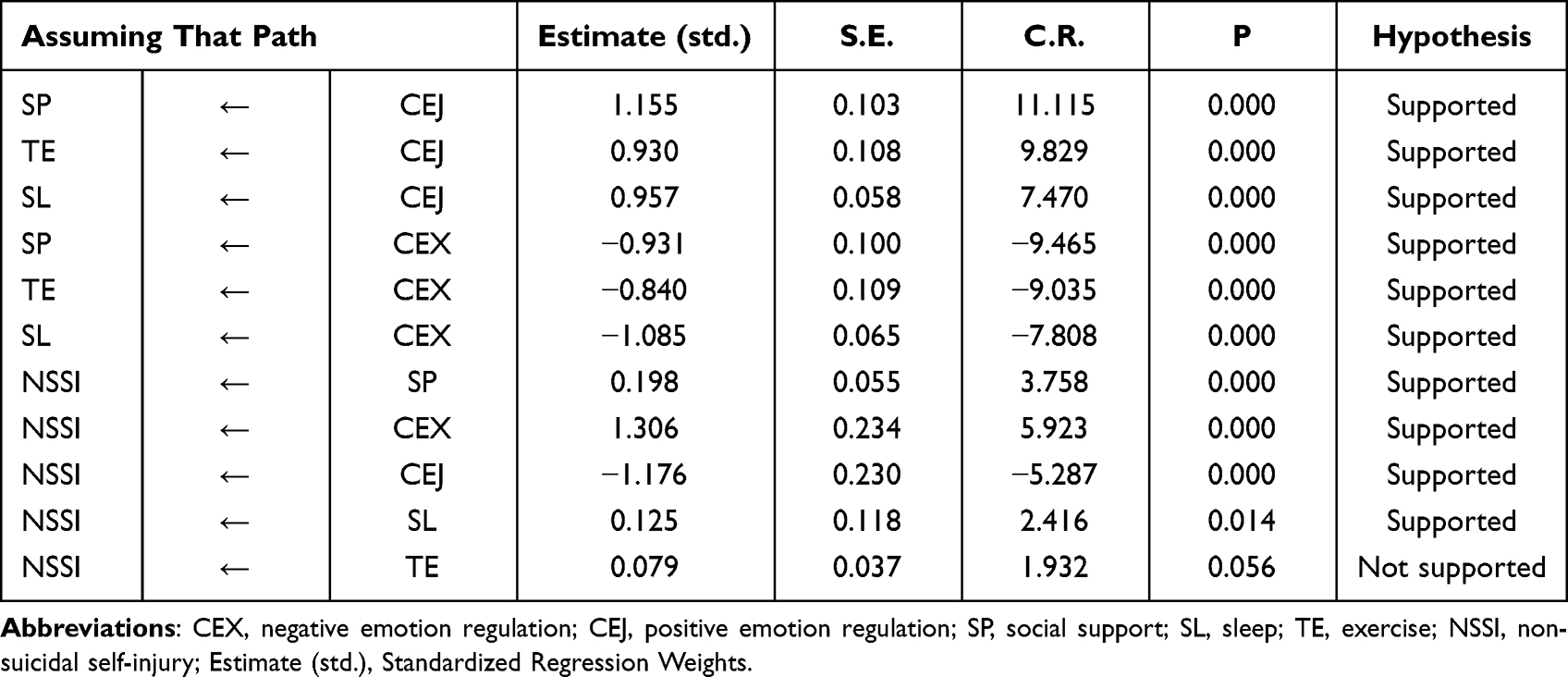 |
Table 1 Path Coefficient of Structural Equation Model |
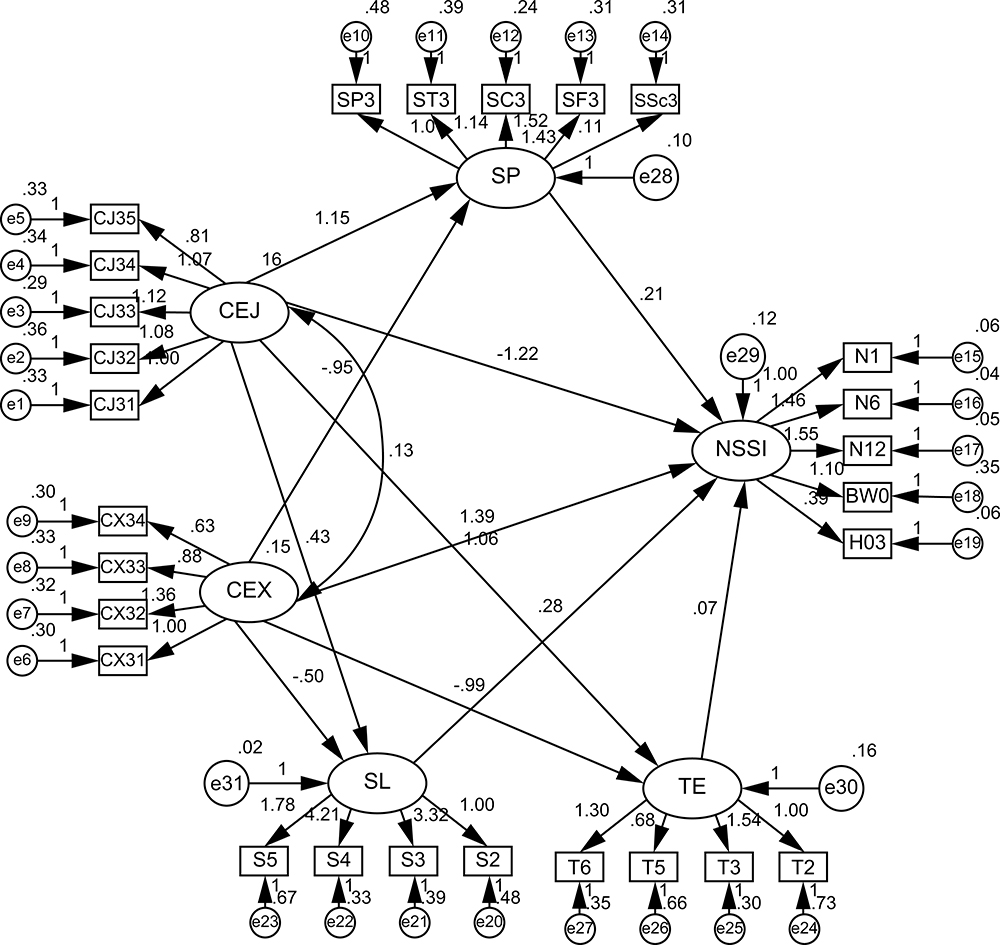 |
Figure 1 Structure path diagram. Abbreviations: CEX, negative emotion regulation; CEJ, positive emotion regulation; SP, social support; SL, sleep; TE, exercise; NSSI, non-suicidal self-injury. |
Among them, positive emotion regulation had a great influence on social support (β=1.155, P <0.001), exercise (β=0.930, P<0.001), sleep (β=0.957, P<0.001); negative emotion regulation influenced social support (β=−0.931, P<0.001), exercise (β=−0.840, P<0.001), and sleep (β=−1.085, P<0.001). Positive emotion regulation (β=−1.176, P<0.001), negative emotion regulation (β= 1.306, P <0.001), sleep (β=0.125, P<0.05), exercise (β=0.079, P<0.053), and social support (β=0.198, P<0.001) had a significant effect on NSSI.
Intermediary Model Test
Zhao, Lynch and Chen suggested that the SEM method is the best framework for the analysis of mediation effects.66 The bootstrapping method is used to generate the empirical sample distribution of the statistic (mediating effect), from which the confidence interval and standard error are obtained to judge the statistical significance of the mediating effect.67 Based on the research hypothesis in this study, a self-compiled code was inserted to calculate the mediating effect values of parental support, sleep quality, and exercise level between emotion regulation type and NSSI. Table 2 shows the results.
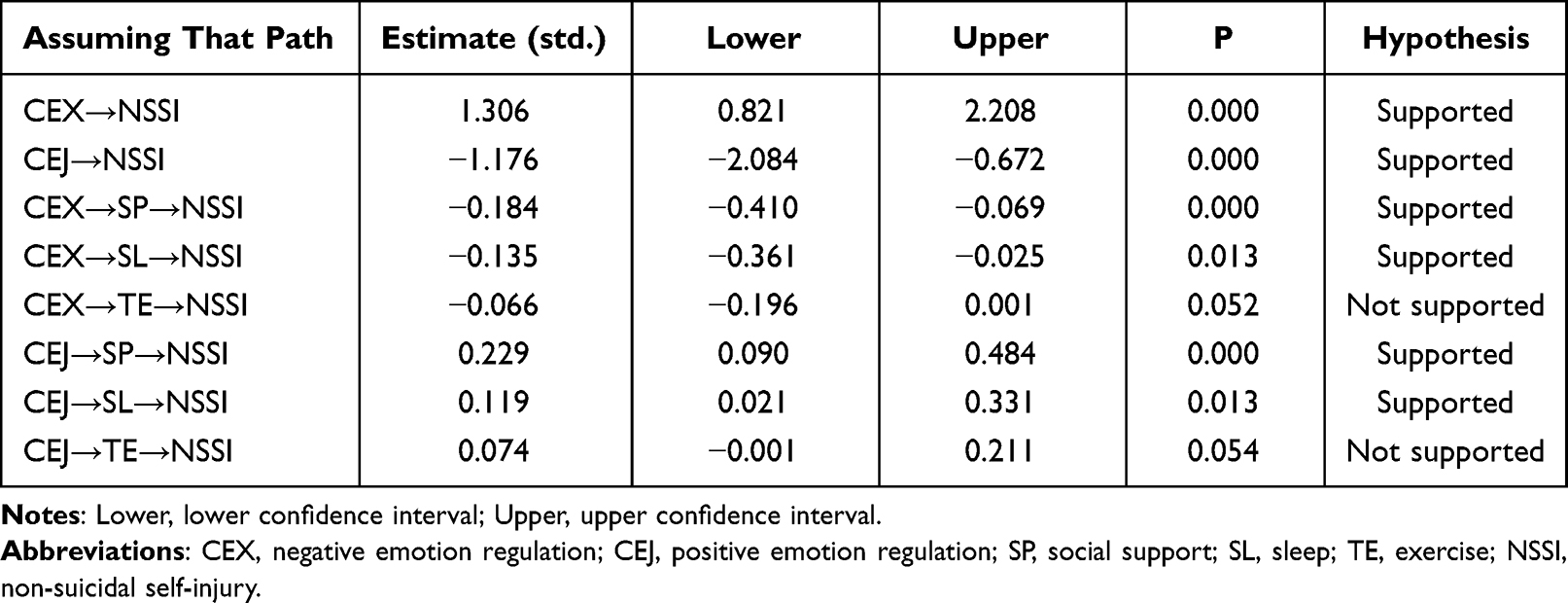 |
Table 2 Intermediary Effect Test |
Mediating effects of three variables were seen between negative emotion regulation and NSSI. First, the mediating effect of sleep on NSSI (β=−0.135, p<0.05), and the effect of negative emotion regulation on sleep (β=−1.085, p<0.001) were significant. Second, after adding exercise, the mediating effect of exercise on NSSI was not significant (β=−0.066, p>0.05), while the effect of negative emotion regulation on exercise (β=−0.840, p<0.001), and the total effect of negative emotion regulation on NSSI (β=1.306, p<0.001) were significant. Finally, when social support was added, the mediating effect of social support on NSSI (β= −0.184, p<0.001), and the effect of negative emotion regulation on social support (β=−0.931, p<0.001) were significant.
Mediating effects of three different variables were seen between positive emotion regulation and NSSI. First, the mediating effect of sleep on NSSI (β=0.119, p< 0.05), and the effect of positive emotion regulation on sleep (β=0.957, p<0.001) were significant. Second, after adding exercise, the mediating effect of exercise on NSSI was not significant (β= 0.074, p>0.05), while the effect of positive emotion regulation on exercise (β=0.930, p< 0.001), and the total effect of positive emotion regulation on NSSI (β=−1.176, p< 0.001) were significant; Finally, social support had a significant mediating effect on NSSI (β=0.229, p<0.001), and positive emotion regulation had a significant effect on social support (β=1.155, p<0.001).
In addition, the upper and lower limits of the confidence intervals of the direct and mediating effects of social support and sleep on negative emotion regulation, positive emotion regulation, and NSSI do not contain 0 (see Table 2), thus indicating that positive and negative emotion regulation can not only directly affect NSSI, but also affect NSSI through the mediating effects of social support and sleep.
Adjustment Model Fitting Test
To test the moderating effect of parental support, sleep quality, and exercise on the relationship between two emotion regulation styles and NSSI, this study established multiple regression analysis models. In these models, negative and positive emotion regulation were independent variables; parental support, sleep quality, and exercise were moderators; and NSSI was the dependent variable. Therefore, 13 multiple regression models were established. The specific analysis steps are as follows: first, the model introduces a control variable (M1); second, the model introduces a control variable, an independent variable, and an adjustment variable (M2, M4, M6, M8, M10, M12); third, the model introduces control variables, independent variables, moderators, and interaction terms between independent and moderators (M3, M5, M7, M9, M11, M13).
First, the influence of control variables on NSSI was analyzed. The results showed that the regression coefficients of the control variables in Model M1 were significant, indicating that the effects of sex (Gen), class type (Key), age (Age), and academic achievement (Ace) on NSSI were significant (see Model M1 in Table 3).
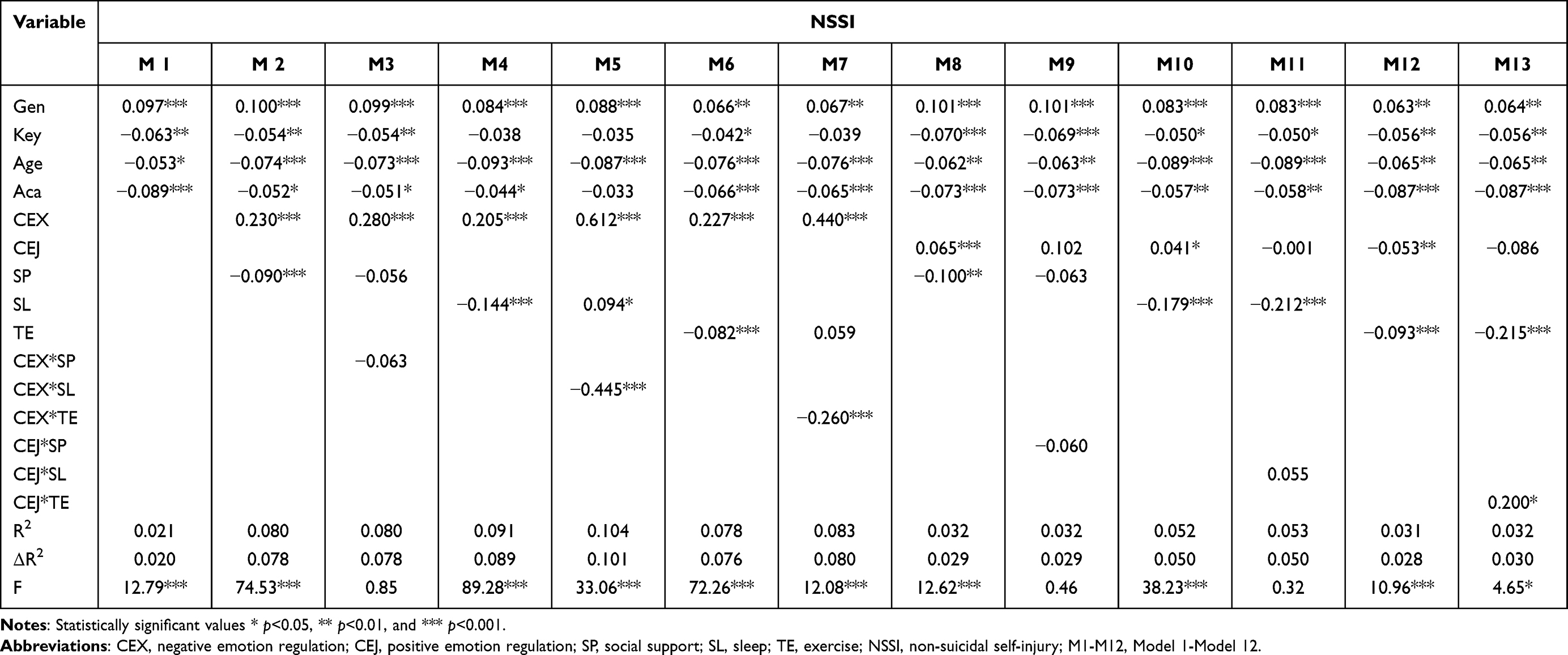 |
Table 3 Regulation Effect Test |
Second, moderating effects of different independent variables were found between negative emotion regulation and NSSI (see Table 3):
In Model M3, the interaction of the independent variables (social support and negative emotion regulation) had no significant effect on NSSI (β=−0.063, p>0.05).
In Model M5, the independent variables of negative emotion regulation (β=0.612, P<0.001), and sleep (β=0.094, P<0.05) had a significant effect on NSSI and the regression coefficient of independent variable interaction term (β=−0.445, P<0.001), indicating that the interaction term has a significant impact on NSSI. Further analysis found that the R2 of Models M4 and M5 are 0.091 and 0.089, respectively, indicating that the explanatory ability of the model has been improved (P<0.001). Therefore, sleep has a significant regulatory effect on the relationship between negative emotion regulation ability and NSSI.
In Model M7, the independent variable of negative emotion regulation had a significant effect on NSSI (β=0.440, P<0.001), but exercise had no significant effect on NSSI (β=0.059, P>0.05).
The moderating effects of different independent variables were found between positive emotion regulation and NSSI (see Table 3).
In Model M9, the interaction of independent variables social support and positive emotion regulation had no significant effect on NSSI (β=−0.060, p>0.05).
In Model M11, the interaction of independent variable sleep and positive emotion regulation had a marginal significant effect on NSSI (β=−0.055, p>0.05).
In Model M13, the independent variable of positive emotion regulation had no significant effect on NSSI (β=−0.086, P>0.05), exercise had a significant effect on NSSI (β=−0.215, P<0.001), but the regression coefficient of independent variable interaction term (β=0.200, P<0.05), had a significant impact on NSSI. Further analysis found that the R2 of Models M12 and M13 are 0.031 and 0.032, respectively, thus indicating that the explanatory ability of the model has been improved (P<0.05). Therefore, the exercise of regulatory variables has a significant regulatory effect on the relationship between positive emotion regulation ability and NSSI.
Finally, according to the regulation results in the significant regulation effect model, the regulation effect trend of different independent variables between emotion regulation and NSSI will be analyzed by drawing a simple regulation effect diagram.
In Model M5, sleep quality had a significant moderating effect between negative emotion regulation and NSSI behavior. As seen in the regulation effect diagram (Figure 2), in the case of high sleep quality (95% confidence interval [0.120, 0.206], excluding 0), the positive effect of negative emotion regulation on NSSI behavior is weak, while in the case of moderate sleep quality (95% confidence interval [0.149, 0.241], excluding 0), or low sleep quality (95% confidence interval [0.164, 0.292], excluding 0), the positive effect of negative emotion regulation on NSSI behavior gradually increased.
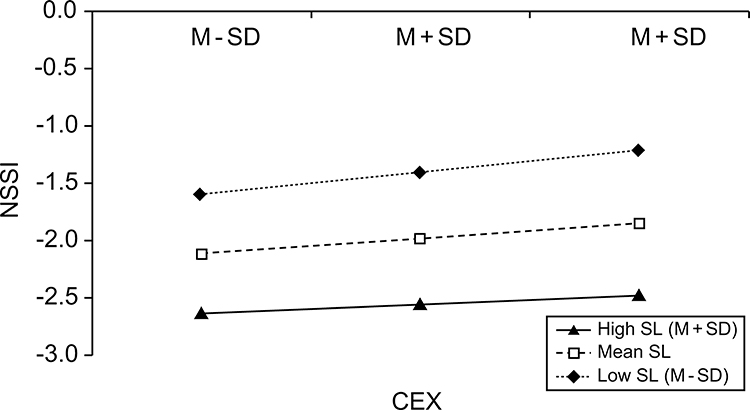 |
Figure 2 Regulatory effect of sleep on negative emotion and NSSI. Abbreviations: CEX, negative emotion regulation; SL, sleep; NSSI, non-suicidal self-injury. |
In Model M13, exercise had a significant moderating effect between positive emotion regulation and NSSI behavior. It can be seen in the regulation effect diagram (Figure 3) that the effect of positive emotion regulation ability on NSSI behavior is weak under the condition of high exercise level (95% confidence interval [−0.067, 0.028], including 0), while under the condition of moderate exercise level (95% confidence interval [−0.124, −0.032], excluding 0) or low exercise level (95% confidence interval [−0.179, −0.054], excluding 0), the effect of positive emotion regulation on NSSI behavior gradually weakened.
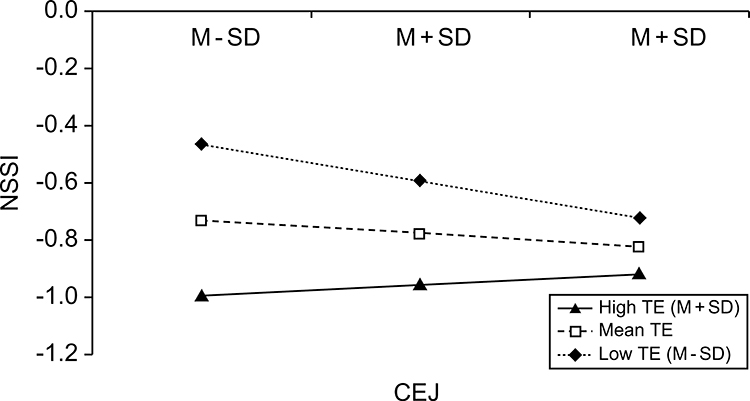 |
Figure 3 Regulation of exercise on positive emotion and NSSI. Abbreviations: CEJ, positive emotion regulation; TE, exercise; NSSI, non-suicidal self-injury. |
Discussion
Relationship Between Emotion Regulation and NSSI
The results showed a significant correlation between emotion regulation and adolescents’ NSSI behavior. Negative emotion regulation was positively correlated with NSSI behavior (β = 1.306, p < 0.001), while positive emotion regulation was negatively correlated with NSSI behavior (β = −1.176, p < 0.001). Hypothesis H1 was established. This result shows a significant correlation between emotion regulation and adolescent NSSI behavior, and from the correlation value, negative emotion regulation has a greater impact than positive emotion regulation, which indirectly proves that NSSI is a strategy and way for adolescents to cope with emotions or behaviors.20
Relationship of Sleep with Emotion Regulation and NSSI
The results showed a significant correlation between sleep and adolescent NSSI behavior (β=0.125, P<0.05), and the hypothesis H2 was established, which was consistent with the results of the previous studies.26,28,29 Second, there was a significant positive correlation between positive emotion regulation and sleep (β=0.957, P<0.001). There was a significant negative correlation between negative emotion regulation and sleep (β=−1.085, P<0.001), assuming that H3 is true, which shows that sleep affects adolescents’ emotional regulation.24 In addition, it was found that sleep had significant mediating effects on negative emotion regulation (β=−0.135, P<0.05), positive emotion regulation (β=0.119, P<0.05) and NSSI, indicating that sleep mediates between emotion regulation and adolescent NSSI behavior.27 However, in terms of the regulatory effect of sleep on emotion regulation and adolescent NSSI behavior, it played a greater regulatory role in negative emotion regulation and NSSI behavior (β=−0.445, P<0.001), and the regulatory effect was significant in different levels of sleep quality. Therefore, sleep plays a mediating role between emotion regulation and adolescent NSSI behavior, and the hypothesis H4 holds.
Relationship of Exercise with Emotion Regulation and NSSI
The results show that exercise has a certain correlation with adolescent NSSI behavior, showing a marginal significant effect (β=0.079, P<0.053), assuming H5 holds, which is similar to the results of Boone and Brausch.42 Second, through the path analysis of exercise and emotion regulation, it was found that exercise has a significant correlation with positive emotion regulation (β=0.930, P<0.001) and negative emotion regulation exercise (β=−0.840, P<0.001). It is assumed that H6 is established, which is consistent with the results of previous studies.40,41 Due to the necessity for fitting the SEM, there is no direct relationship between exercise and sleep. Using the total score of exercise and sleep, there is a significant positive correlation between exercise and sleep in adolescents (r=0.248, P<0.001), which is consistent with the results of O’Connor, Rasmussen and Hawton.41 Further analysis of the mediating effect of exercise on emotion regulation and adolescent NSSI behavior shows that while exercise can regulate negative (β=−0.066, P>0.05) and positive emotions (β=0.074, P>0.05), the mediating effect of NSSI is not significant, and the hypothesis H7 is not tenable. However, further examination of the regulatory effect of exercise on emotion regulation and adolescent NSSI behavior shows that exercise has a significant regulatory effect on positive emotion regulation and adolescent NSSI behavior (β=0.200, P<0.05), and positive emotion regulation plays a highly significant role in adolescents with low and medium level of exercise. Thus, there is a difference in the moderating effect of exercise level between positive emotion regulation and adolescent NSSI behavior. Therefore, while intervening in adolescents’ behavior by adjusting their exercise level, attention must be given to identify adolescents with different exercise levels and highlight the prevention and intervention of adolescents’ NSSI in practice.
Relationship of Social Support with Emotion Regulation and NSSI
The results showed a significant correlation between social support and adolescent NSSI behavior (β=0.198, P<0.001), assuming that H8 holds. Second, positive emotion regulation had a positive correlation with social support (β=1.155, P<0.001), and negative emotion regulation had a negative correlation with social support (β=−0.931, P<0.001). It illustrates the impact of social support on emotion regulation, assuming that H9 is true. Further analysis of the intermediary relationship between social support in emotion regulation and adolescent NSSI behavior found that social support in negative emotion regulation (β=−0.184, P<0.001), positive emotion regulation (β=0.229, P<0.001), and NSSI, has significant mediating effects, indicating that sleep mediates between emotion regulation and adolescent NSSI behavior, which supports the view of Christoffersen et al.49 However, verifying the independent variables of social support, negative emotion regulation (β=−0.063, P>0.05), and positive emotion regulation (β=−0.060, P>0.05) indicated that social support has no regulatory effect on emotion regulation and adolescent NSSI behavior. Therefore, the hypothesis H10 is partially true. Thus, the relationship between social support in different ways of emotion regulation and NSSI behavior is still unclear, and a higher amount of in-depth discussion is needed to find a highly authentic relationship.
Conclusion
There is a significant correlation between emotion regulation and NSSI behavior in adolescents. Negative emotion regulation is negatively correlated with NSSI behavior, while positive emotion regulation is positively correlated with NSSI behavior. The direct effect of negative emotion regulation on adolescent NSSI behavior is regulated by sleep, and high sleep quality can effectively alleviate the negative effect of negative emotion regulation on NSSI behavior. The direct effect of positive emotion regulation on adolescents’ NSSI behavior is regulated by exercise, and exercise can effectively promote the effect of positive emotion regulation on adolescents’ NSSI behavior. Therefore, for middle schools in China, especially those in underdeveloped rural areas, in the absence of systematic guidance on NSSI crisis intervention strategies, appropriate intervention on adolescents’ sleep state and exercise levels may serve to resolve their emotional state and NSSI behavior.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki, and it has been approved by the Human Research Ethics Committee of Sultan Idris University of Education (No. 2022-0465-01).
Author Contributions
Dr.Pau and Dr. Hapsah focus on the conception and design of the study; Dr. Lan and Mrs. Huang focus on the acquisition of data, and drafting the article or revising it critically for important intellectual content; Dr. Lan focus on the analysis and interpretation of data.
Funding
Supported by Basic Ability Improvement Project of Young and Middle-aged Teachers in Universities of the Education Department of Guangxi Zhuang Autonomous Region, China (No.2021KY0604).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Choudhury S, Blakemore S-J, Charman T. Social cognitive development during adolescence. Soc Cogn Affect Neurosci. 2006;1(3):165–174. doi:10.1093/scan/nsl024
2. Thorndike EL. Adolescence; its psychology and its relations to physiology, anthropology, sociology, sex, crime, religion and education. Science. 1904;20(500):142–145. doi:10.1126/science.20.500.142
3. Kroger J. Identity, regression and development. J Adolesc. 1996;19(3):203–222. doi:10.1006/jado.1996.0020
4. Carlson NR, Miller HL, Heth SD, Donahoe JW, Martin GN. Psychology: The Science of Behaviour. Ontario: Pearson Education Canada; 2010:20–22.
5. Hilt LM, Cha CB, Nolen-Hoeksema S. Nonsuicidal self-injury in young adolescent girls: moderators of the distress-function relationship. J Consult Clin Psychol. 2008;76(1):63. doi:10.1037/0022-006X.76.1.63
6. Muehlenkamp JJ, Swanson JD, Brausch AM. Self-objectification, risk taking, and self-harm in college women. Psychol Women Q. 2005;29(1):24–32. doi:10.1111/j.1471-6402.2005.00164.x
7. Greydanus DE, Shek D. Deliberate self-harm and suicide in adolescents. Keio J Med. 2009;58(3):144–151. doi:10.2302/kjm.58.144
8. Duggan J, Heath N, Hu T. Non-suicidal self-injury maintenance and cessation among adolescents: a one-year longitudinal investigation of the role of objectified body consciousness, depression and emotion dysregulation. Child Adolesc Psychiatry Ment Health. 2015;9(1):1–12. doi:10.1186/s13034-015-0052-9
9. Plener PL, Schumacher TS, Munz LM, Groschwitz RC. The longitudinal course of non-suicidal self-injury and deliberate self-harm: a systematic review of the literature. Borderline Personal Disord Emot Dysregulation. 2015;2(1):1–11. doi:10.1186/s40479-014-0024-3
10. Zubrick SR, Hafekost J, Johnson SE, et al. Self-harm: prevalence estimates from the second Australian child and adolescent survey of mental health and wellbeing. Aust N Z J Psychiatry. 2016;50(9):911–921. doi:10.1177/0004867415617837
11. Zheng Y An epidemiological survey and functional model of self-harm behavior among middle school students in Wuhan. [dissertation]. Central China Normal University; 2006.
12. Yan J, Zhu CZ, Situ MJ, Na DU, Huang Y. The detection rate of non-suicidal self-injury behavior and its risk factors among 1312 middle school students in Sichuan Province. Chin J Epidemiol. 2012;33(1):46–49.
13. Lei W, Yuan L, Xin J, Jie L, Guoqing X, Chengqing Z. Epidemiological survey of non-suicidal self-injury behavior of 1463 junior high school students in Dalian. Chin J Behav Med Brain Sci. 2016;02:177–180.
14. Wan Y, Liu W, Hao J, Tao F. Development and evaluation on reliability and validity of adolescent non-suicidal self-injury assessment questionnaire. Chin J School Health. 2018;39(2):170–173. doi:10.16835/j.cnki.1000-9817.2018.02.005
15. Tang H, Chen X, Lu F, et al. Meta-analysis of the relationship between bullying and non-suicidal self-harm in adolescents. Chin J Evid-Based Med. 2018;07:707–714.
16. Klonsky ED. The functions of deliberate self-injury: a review of the evidence. Clin Psychol Rev. 2007;27(2):226–239. doi:10.1016/j.cpr.2006.08.002
17. Chapman AL, Gratz KL, Brown MZ. Solving the puzzle of deliberate self-harm: the experiential avoidance model. Behav Res Ther. 2006;44(3):371–394. doi:10.1016/j.brat.2005.03.005
18. Yu F The relationship between adolescent self-harm behavior and individual emotional factors and family environment factors. [dissertation]. Central China Normal University; 2008.
19. Victor SE, Klonsky ED. Daily emotion in non‐suicidal self‐injury. J Clin Psychol. 2014;70(4):364–375. doi:10.1002/jclp.22037
20. Haines J, Williams CL. Coping and problem solving of self‐mutilators. J Clin Psychol. 2003;59(10):1097–1106. doi:10.1002/jclp.10202
21. Nock MK, Mendes WB. Physiological arousal, distress tolerance, and social problem-solving deficits among adolescent self-injurers. J Consult Clin Psychol. 2008;76(1):28. doi:10.1037/0022-006X.76.1.28
22. Carskadon MA. Sleep in adolescents: the perfect storm. Pediatr Clin. 2011;58(3):637–647. doi:10.1016/j.pcl.2011.03.003
23. Campbell IG, Grimm KJ, De Bie E, Feinberg I. Sex, puberty, and the timing of sleep EEG measured adolescent brain maturation. PNAS. 2012;109(15):5740–5743. doi:10.1073/pnas.1120860109
24. Gau SS-F, Shang C-Y, Merikangas KR, Chiu Y-N, Soong W-T, Cheng -AT-A. Association between morningness-eveningness and behavioral/emotional problems among adolescents. J Biol Rhythms. 2007;22(3):268–274. doi:10.1177/0748730406298447
25. Schmidt RE, Van der Linden M. The relations between sleep, personality, behavioral problems, and school performance in adolescents. Sleep Med Clin. 2015;10(2):117–123. doi:10.1016/j.jsmc.2015.02.007
26. Talbot LS, McGlinchey EL, Kaplan KA, Dahl RE, Harvey AG. Sleep deprivation in adolescents and adults: changes in affect. Emotion. 2010;10(6):831. doi:10.1037/a0020138
27. Zhao Y, Jiang MM, Wang J, Ai D, Jin YL. Effects of depression on NSSI in college students: the mediating role of sleep quality and the moderating role of gender. Chin J Health Psychol. 2021;06:922–926.
28. Liu X, Chen H, Bo Q-G, Fan F, Jia C-X. Poor sleep quality and nightmares are associated with non-suicidal self-injury in adolescents. Eur Child Adolesc Psychiatry. 2017;26(3):271–279. doi:10.1007/s00787-016-0885-7
29. Shi X, Zhu Y, Ma X, Xiao S, Wang S, Cai Y. Relationship between sleep problems and non-suicidal self-injury behavior among college students. Chin J Sch Health. 2020;41(6):918–921.
30. McGlinchey EL, Courtney-Seidler EA, German M, Miller AL. The role of sleep disturbance in suicidal and nonsuicidal self-injurious behavior among adolescents. Suicide Life Threat Behav. 2017;47(1):103–111. doi:10.1111/sltb.12268
31. Sami H, Danielle L, Lihi D, Elena S. The effect of sleep disturbances and internet addiction on suicidal ideation among adolescents in the presence of depressive symptoms. Psychiatry Res. 2018;267:327–332. doi:10.1016/j.psychres.2018.03.067
32. Franić T, Kralj Z, Marčinko D, Knez R, Kardum G. Suicidal ideations and sleep‐related problems in early adolescence. Early Interv Psychiatry. 2014;8(2):155–162. doi:10.1111/eip.12035
33. Gomes GC, Passos MHPD, Silva HA, et al. Sleep quality and its association with psychological symptoms in adolescent athletes. Rev Paul Pediatr. 2017;35:316–321. doi:10.1590/1984-0462/;2017;35;3;00009
34. Bernert RA, Nadorff MR. Sleep disturbances and suicide risk. Sleep Med Clin. 2015;10(1):35–39. doi:10.1016/j.jsmc.2014.11.004
35. Owens J, Au R, Carskadon M; Adolescent Sleep Working Group, Committee on Adolescence. Insufficient sleep in adolescents and young adults: an update on causes and consequences. Pediatrics. 2014;134(3):e921–e932. doi:10.1542/peds.2014-1696
36. Park JH, Yoo JH, Kim SH. Suicidal ideations and sleep‐related problems in early adolescence. Psychiatry Clin Neurosci. 2013;67(1):28–34. doi:10.1111/j.1440-1819.2012.02394.x
37. Zhao Y. The positive effect of sports on optimizing middle school students’ emotions. World Sports. 2012;07:114–115.
38. Stanley B, Sher L, Wilson S, Ekman R, Huang Y-Y, Mann JJ. Non-suicidal self-injurious behavior, endogenous opioids and monoamine neurotransmitters. J Affect Disord. 2010;124(1–2):134–140. doi:10.1016/j.jad.2009.10.028
39. Song Y. The influence mechanism of exercise on negative emotions. Sports Sci Technol Lit Bull. 2017;4:136–137.
40. Wallenstein MB, Nock MK. Physical exercise as a treatment for non-suicidal self-injury: evidence from a single-case study. Am J Psychiatry. 2007;164(2):350–351. doi:10.1176/ajp.2007.164.2.350a
41. O’Connor RC, Rasmussen S, Hawton K. Distinguishing adolescents who think about self-harm from those who engage in self-harm. Br J Psychiatry. 2012;200(4):330–335. doi:10.1192/bjp.bp.111.097808
42. Boone SD, Brausch AM. Physical activity, exercise motivations, depression, and nonsuicidal self-injury in youth. Suicide Life Threat Behav. 2016;46(5):625–633. doi:10.1111/sltb.12240
43. Ahn S, Fedewa AL. A meta-analysis of the relationship between children’s physical activity and mental health. J Pediatr Psychol. 2011;36(4):385–397. doi:10.1093/jpepsy/jsq107
44. Dolezal B, Neufeld E, Boland D, Martin J, Cooper C. The interrelationship between sleep and exercise: a systematic review. Adv Prev Med. 2017;2017:1364387. doi:10.1155/2017/1364387
45. Kline CE. The bidirectional relationship between exercise and sleep: implications for exercise adherence and sleep improvement. Am J Lifestyle Med. 2014;8(6):375–379. doi:10.1177/1559827614544437
46. Wang F, Boros S. The effect of physical activity on sleep quality: a systematic review. Eur J Physiother. 2021;23(1):11–18. doi:10.1080/21679169.2019.1623314
47. Vancampfort D, Hallgren M, Firth J, et al. Physical activity and suicidal ideation: a systematic review and meta-analysis. J Affect Disord. 2018;225:438–448. doi:10.1016/j.jad.2017.08.070
48. Kelley GA, Kelley KS. Exercise and sleep: a systematic review of previous meta-analyses. J Evid Based Med. 2017;10(1):26–36. doi:10.1111/jebm.12236
49. Christoffersen MN, Møhl B, DePanfilis D, Vammen KS. Non-suicidal self-injury–does social support make a difference? An epidemiological investigation of a Danish national sample. Child Abuse Negl. 2015;44:106–116. doi:10.1016/j.chiabu.2014.10.023
50. Peng Z, Klomek AB, Li L, et al. Associations between Chinese adolescents subjected to traditional and cyber bullying and suicidal ideation, self-harm and suicide attempts. BMC Psychiatry. 2019;19(1):1–8. doi:10.1186/s12888-019-2319-9
51. Heath NL, Ross S, Toste JR, Charlebois A, Nedecheva T. Retrospective analysis of social factors and nonsuicidal self-injury among young adults. Can J Behav Sci. 2009;41(3):180. doi:10.1037/a0015732
52. Gould MS, Greenberg T, Velting DM, Shaffer D. Youth suicide risk and preventive interventions: a review of the past 10 years. J Am Acad Child Adolesc Psychiatry. 2003;42(4):386–405. doi:10.1097/01.CHI.0000046821.95464.CF
53. Nock MK, Prinstein MJ, Sterba SK. Revealing the form and function of self-injurious thoughts and behaviors: a real-time ecological assessment study among adolescents and young adults. J Abnorm Psychol. 2009;118(4):816. doi:10.1037/a0016948
54. Lixia Y The same self-injury and two kinds of people: a classification study of self-injury teenagers [dissertation]. Central China Normal University; 2013.
55. Nansel TR, Overpeck M, Pilla RS, Ruan WJ, Simons-Morton B, Scheidt P. Bullying behaviors among US youth: prevalence and association with psychosocial adjustment. JAMA. 2001;285(16):2094–2100. doi:10.1001/jama.285.16.2094
56. Keenan K, Hipwell AE, Stepp SD, Wroblewski K. Testing an equifinality model of nonsuicidal self-injury among early adolescent girls. Dev Psychopathol. 2014;26(3):851–862. doi:10.1017/S0954579414000431
57. Kidger J, Heron J, Leon DA, Tilling K, Lewis G, Gunnell D. Self-reported school experience as a predictor of self-harm during adolescence: a prospective cohort study in the South West of England (ALSPAC). J Affect Disord. 2015;173:163–169. doi:10.1016/j.jad.2014.11.003
58. Au AC, Lau S, Lee MT. Suicide ideation and depression: the moderation effects of family cohesion and social self-concept. Adolescence. 2009;44(176):851–868.
59. Shek DT, Sun RC. Positive youth development programs for adolescents with greater psychosocial needs: subjective outcome evaluation over 3 years. J Pediatr Adolesc Gynecol. 2014;27:S17–S25. doi:10.1016/j.jpag.2014.02.008
60. Jiang Y, You J, Hou Y, et al. Buffering the effects of peer victimization on adolescent non-suicidal self-injury: the role of self-compassion and family cohesion. J Adolesc. 2016;53:107–115. doi:10.1016/j.adolescence.2016.09.005
61. Taliaferro LA, McMorris BJ, Eisenberg ME. Connections that moderate risk of non-suicidal self-injury among transgender and gender non-conforming youth. Psychiatry Res. 2018;268:65–67. doi:10.1016/j.psychres.2018.06.068
62. Adrian M, Zeman J, Erdley C, Lisa L, Sim L. Emotional dysregulation and interpersonal difficulties as risk factors for nonsuicidal self-injury in adolescent girls. J Abnorm Child Psychol. 2011;39(3):389–400. doi:10.1007/s10802-010-9465-3
63. Zhu X, Luo F, Yao S, Auerbach RP, Jr ZA. Reliability and validity of the Chinese version of the Cognitive Emotion Regulation Questionnaire (CERQ-C). Chin J Clin Psychol. 2007;02:
64. Luo X, Chen Q, Mu S. Revision and preliminary application of the Chinese version of the social support scale for children and adolescents. Chin J Clin Psychol. 2017;04(25):671–674.
65. Zhang F, Cheng W-H, Xiao Z-P. Study on reliability and validity of Chinese version of Ottawa self-injury inventory. J Shanghai Jiaotong Univ. 2015;35(3):460.
66. Zhao X, Lynch JG
67. Iacobucci D, Saldanha N, Deng X. A meditation on mediation: evidence that structural equations models perform better than regressions. J Consum Psychol. 2007;17(2):140–154. doi:10.1016/S1057-7408(07)70020-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.