")
Back to Journals » Vascular Health and Risk Management » Volume 16
The Effect of CYP2C9 Genotype Variants in Type 2 Diabetes on the Pharmacological Effectiveness of Sulfonylureas, Diabetic Retinopathy, and Nephropathy
Authors Saberi M, Ramazani Z, Rashidi H, Saberi A
Received 11 September 2019
Accepted for publication 5 June 2020
Published 18 June 2020 Volume 2020:16 Pages 241—248
DOI https://doi.org/10.2147/VHRM.S230639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Meisam Saberi,1 Zahra Ramazani,1 Homeira Rashidi,2 Alihossein Saberi3
1Department of Medical Chemistry, School of Pharmacy, Ahvaz Jundishpur University of Medical Sciences, Ahvaz, Iran; 2Diabetic Research Center, Ahvaz Jundishpur University of Medical Sciences, Ahvaz, Iran; 3Department of Medical Genetics, School of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Correspondence: Alihossein Saberi
Department of Medical Genetics, School of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Tel +98-9161133488
Fax +98-6133332036
Email [email protected]
Aim: Type 2 diabetes (T2D), as a major cause of morbidity and mortality, is predicted to have a prevalence of 629 million by 2045. As diabetic patients show considerable inter-individual variation in response to antidiabetic treatment, this study aimed to investigate the gene polymorphism of cytochrome P450 as well as the effectiveness and safety of glibenclamide and gliclazide for different genotypes of CYP2C9. Besides, the chronic side effects of T2D including retinal microvasculature complications or retinopathy and renal dysfunction due to nephropathy in different genotypes were considered.
Patients and Methods: The participants including 80 T2D patients treated with glibenclamide or gliclazide were recruited from university hospitals of Ahvaz Jundishpur University of Medical Sciences, Ahvaz, in the southwest of Iran. Blood samples were collected from the patients at 2.5h after the morning dose of glibenclamide and 12h after the last dose of gliclazide. Genotyping from the extracted DNA was, then, performed using PCR-RFLP. The plasma level of glibenclamide and gliclazide was, in turn, measured by the reverse-phase high-pressure liquid chromatography.
Results: The results showed that the wild-type allele, i.e., CYP2C9*1, occurred in the highest frequency (0.8), while the frequency rates of the mutant allele, i.e., CYP2C9*2 and CYP2C9*3, were 0.15 and 0.05, respectively. Moreover, no significant association was found between any of the genotypes as well as the clinical and biochemical characteristics of the patients. The findings also showed that the plasma level of sulfonylureas (i.e., glibenclamide and gliclazide) was the highest in the patients with the CYP2C9*3 allele. It was also found that 75.9% of the patients with variant genotypes had experienced hypoglycemia events. Furthermore, in the absence of wild type allele, a significant increase was observed in retinopathy (p=0.039) and nephropathy (p=0.05).
Conclusion: The findings can provide guidelines for the optimal management of the treatment protocols with sulfonylurea intended to control the T2D complications.
Keywords: CYP2C9, glibenclamide, gliclazide, retinopathy, nephropathy
Introduction
Type 2 diabetes (T2D), as a metabolic disorder characterized by hyperglycemia, is reported to have a prevalence of 629 million by 2045.1 Genetic factors are, in turn, supposed to contribute to great inter-individual variation in response to antidiabetic treatment. Indeed, the importance of pharmacogenetics to reinforce therapeutic outcomes is widely acknowledged. Among others, sulfonylureas, as a group of antidiabetic drugs, are most widely used for the treatments of patients with T2D.2 In effect, the sulfonylurea receptor functions as a part of the ATP-dependent potassium channel in the beta cells of the pancreas (K-ATP).3 This way, channel function is inhibited due to the binding of the receptor to sulfonylurea. This, in turn, alters the resting potential of the cell, resulting in calcium influx and the stimulation of insulin secretion.
The net effect occurs when the beta cell response increases in both stimulants of glucose and non-glucose (e.g., amino acids), and insulin secrets at higher levels at all blood glucose concentrations. Having similar characteristics in their structure, glibenclamide and gliclazide, as the second generation sulfonylureas, are prescribed in much lower doses than the previous generation of sulfonylureas. However, the effectiveness of different sulfonylureas in lowering blood glucose concentration is reported to be the same.2 Although sulfonylureas are usually well-tolerated, they usually have serious side effects including hypoglycemia which is more common in the long-acting version of such drugs.4–6
Sulfonylurea is known to be metabolized by cytochrome P450, which is encoded by the CYP2C9 gene. Several studies have already reported medical evidence suggesting that in patients with CYP2C9*2 and CYP2C9*3 variant alleles, the metabolism of the substrate is significantly slower than that in the wild-type allele.7–10 For instance, in a Go-DART study by Zhou et al11, it was shown that sulfonylureas were metabolized mainly by the cytochrome P450 2C9 (15). Two CYP2C9* and CYP2C *3 genotypes were, indeed, found to be associated with impaired substrate metabolism. Furthermore, many reports have demonstrated that at least one variant allele causes a significant decrease in CYP2C9 activity, requiring dose adjustment for sulfonylureas.12–15 Therefore, CYP2C9 gene polymorphism is likely to affect the metabolism and the adverse drug reaction (ADR) of glibenclamide and gliclazide.
Diabetic retinopathy, a retinal vascular disorder, occurs as a complication of diabetes mellitus and causes blindness in diabetic patients. In effect, the associated vision loss results from several mechanisms, including neovascularization, macular edema, and retinal capillary nonperfusion.16 Likewise, a few studies have shown that diabetic retinopathy is influenced by CYP2C9 variants.17 Epoxyeicosatrienoic acids (EETs) produced by CYP2C8 and CYP2C9, which are hydrolyzed to dihydroxyeicosatrienoic acids (DHETs) by epoxide hydrolase, are known to play an important role in the diabetic retinopathy.18 Therefore, CYP2C9 genetic polymorphism is also likely to affect retinopathy, considering that renal dysfunction has been reported in patients with T2D. The severity and onset of nephropathy maybe thus influenced by genetic variants.
This study was, thus, intended to analyze the frequency of CYP2C9 genotypes in T2 diabetic patients, and also investigate the metabolism as well as safety (ADR) of glibenclamide and gliclazide in patients with different CYP2C9 genotypes to predict their response to sulfonylureas. Also, this study examined whether the CYP2C9 polymorphisms were associated with the risk of diabetic retinopathy and diabetic nephropathy.
Patients and Methods
Patient Selection and Clinical Study Design
Iranian patients with T2D who had received medical treatment with sulfonylureas (i.e., glibenclamide or gliclazide) at Golestan and Imam Khomeini Hospitals were recruited for this study. The participants included 80 T2D male and female patients who had to take 10 mg Glibenclamide and 160 mg Gliclazide for more than 3 months. Blood samples were collected from the patients at 2.5 h after the morning dose of glibenclamide15 and 12h after the last dose of gliclazide, corresponding to the time for the peak drug concentration.19
The plasma samples collected were used to estimate the levels of sulfonylureas, and the buffy coat fraction was used for DNA extraction and genotyping of variant alleles. The plasma levels of glibenclamide and gliclazide were, then, estimated by reverse-phase high-pressure liquid chromatography.20,21 The DNA was extracted from the buffy coat using the salting-out extraction procedure. The variant alleles CYP2C9*2 and *3 were genotyped by PCR– restriction fragment length polymorphism (RLFP).22 Fasting blood glucose (FBS), HbA1c, blood urea nitrogen (BUN), creatinine (Cr), microalbuminuria, LDL (Low-density lipoprotein), HDL (High-density lipoprotein), total cholesterol and retinopathy data were collected from the patients’ medical records. Nephropathy was, in turn, achieved by using an NKF KDOQI.
GUIDELINES.23 The cause of chronic kidney disease, glomerular filtration rate (GFR) and albuminuria, collectively referred to as CGA staging, was checked according to the guidelines. The GFR ≥ 90mL/min/1.73m2 (G1) was considered as normal or high GFR, while GFR≤ 15 (G5) was described as kidney failure. There are several categories between G1 and G5 (i.e., G2, G3a, G3b, and G4) meaning mildly to severely decreased as GFR. Increasing albuminuria from less than 30mg/g to more than 300mg/g was, in turn, categorized as A1 to A3 (normal to severely increased). We described the risk of nephropathy using the combination of GFR decreasing and albuminuria increasing ranges. For instance, the patients with GFR<15 mL/min/1.73m2 and albuminuria more than 300mg/g (G5-A3) were considered at very high risk for nephropathy.
This study was approved by the Medical Ethics Committee at Ahvaz Jundishapur University of Medical Sciences, Iran. Informed written consent was obtained from the patients after they were introduced to the research objectives and the procedure used.
Statistical Analysis
In the statistical analysis performed, all quantitative data were presented as mean ± standard deviation (SD), and the comparison between different genotype groups was conducted using an independent t-test and ANOVA test. The chi-square test was, in turn, used to compare the genotype and allelic frequency distribution of CYP2C9, as well as the distribution of sulfonylureas plasma level, ADRs (hypoglycemia), and the retinopathy and nephropathy between the genotype groups.
Results
A total of 80 patients with T2D were genotyped by PCR-RFLP method described previously (Table 1). The compound heterozygous genotypes were scored according to the Seng et al paper.22 In CYP2C9*1/CYP2C9*2 genotype, AvaII digestion produced 296b + 79bp and 375bp, while Kpn1 digestion created 105bp. In turn, in CYP2C9*1/CYP2C9*3 genotype, AvaII digestion produced 375bp and 296bp + 79bp, while Kpn1 digestion produced 85bp + 20bp. Likewise, in the CYP2C9*2/CYP2C9*3 genotype, AvaII digestion produced 375bp and 296bp + 79 bp, while Kpn1 digestion produced 105bp fragments.
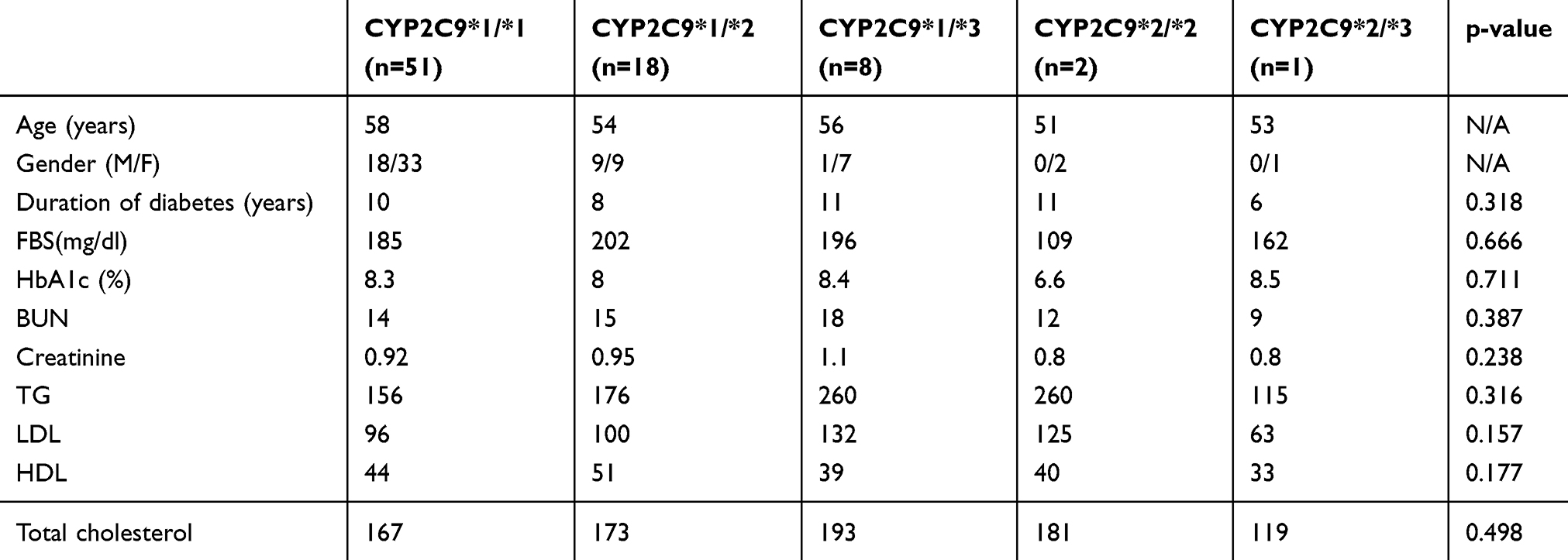 |
Table 1 The Demographic and Biochemical Factors in Different Genotypes of CYP2C9 |
The genotype and allelic frequencies obtained were consistent with those of Hardy-Weinberg Equilibrium. Indeed, CYP2C9*1 (wild type) was the predominant allele and occurred in high frequency in this study (0.8). Besides, the frequency of mutant alleles, CYP2C9*2 and CYP2C9*3, were 0.15 and 0.05, respectively.
The results also showed that there were 51 patients with CYP2C9*1/*1 genotype (63.57%), and CYP2C9*1/*2 (22.5%) was found to be the second most frequent genotype. Also, the percentage rates of the observed CYP2C9*1/*3 and CYP2C9*2/*3 genotypes were 10 and 2.5, respectively. Moreover, only one patient was observed with the CYP2C9*2/*3 compound heterozygous genotype. Though none of the patients was a homozygous mutant genotype for the CYP2C9*3 allele, two patients with CYP2C9*2 allele were found to be a homozygous mutant.
The demographic information and biochemical characteristics of the patients are summarized in Table 1. The parameters such as age, gender, duration of diabetes, FBS, HbA1c, BUN, TG, LDL, HDL, and total cholesterol were compared in different genotypes. The findings showed that there was no significant correlation between any of the genotypes as well as the clinical and biochemical characteristics of the patients. It was also found that 55 patients, out of 80 patients, underwent concomitant treatment with two drugs, namely sulfonylureas (glibenclamide or gliclazide) and metformin, 16 patients with three drugs (i.e., metformin, sulfonylureas, and another antidiabetic drug), 9 patients with monotherapy, 5 patients with gliclazide, and other 4 patients with glibenclamide.
To examine the effects of CYP2C9 genotypes on the plasma level of sulfonylureas, the drug concentration was investigated using HPLC 2.5 hours after glibenclamide and 12 hours after gliclazide administration. The results showed that a relatively higher plasma level of sulfonylureas was observed in the CYP2C9*3 allele in comparison to those of other alleles. Besides, it was found that there was no steady-state in the plasma level of the drugs in patients with wild-type alleles (Table 2). Furthermore, the distributions of various alleles in two groups of patients, namely, steady-state and non-steady-state, were significantly different (p=0.001).
 |
Table 2 Plasma Level of Glybenclamid and Glyclaside as Well as the Number of Patients Reached Steady State in Different Genotype of CYP2C9 |
Additionally, the occurrence of hypoglycemic ADRs to sulfonylureas was compared between the wild-type and variant genotypes. The results showed that 75.9% of the patients with variant genotypes had experienced hypoglycemia status, whereas this was not observed in the wild-type genotypes. Overall, these data showed that hypoglycemia status increased significantly in the patients with variant genotypes. The retinopathy was, in turn, checked in all samples, and a significant association was identified between the duration of diabetes and retinopathy (p=0.002).
To investigate the association between the variant genotypes and retinopathy, we initially checked the average duration of diabetes between various genotypes. As the findings showed, no significant difference was observed (p=0.318). However, the association between the different genotypes and retinopathy was found to be significant (p=0.039). In the patients with CYP2C9*1/*3 genotype 50%, while in CYP2C9*2/*2 and *2/*3 genotypes, 100% of the patients were affected by retinopathy (Figure 1).
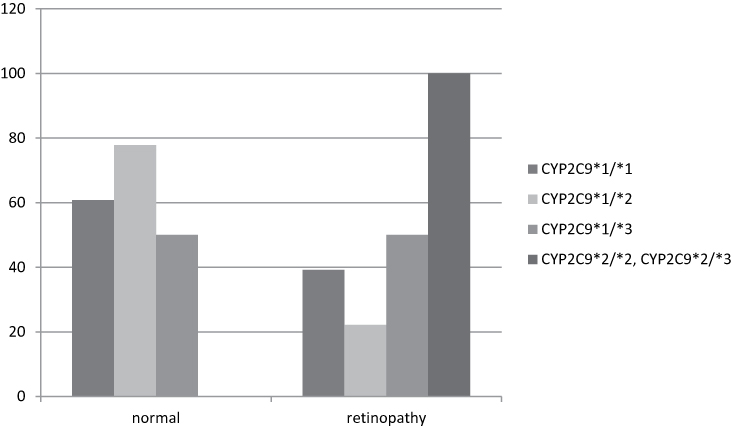 |
Figure 1 Association of retinopathy and different genotypes of CYP2C9. |
In turn, to evaluate the impact of the duration of diabetes on the renal function, the correlation between nephropathy and the duration of diabetes was investigated. As the results showed, no significant correlation was found (p=0.404). However, patients with variant genotypes were found to be significantly affected by nephropathy (p=0.05). Besides, 50% of the patients with CYP2C9*1/*3 and 67% of the patients with CYP2C9*2/*2 and CYP2C9*2/*3 genotypes were identified to be affected (Figure 2).
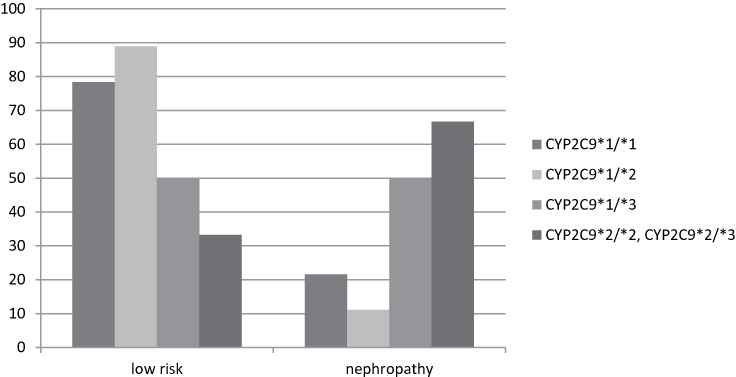 |
Figure 2 Association of nephropathy and different genotypes of CYP2C9. |
Discussion
This study was, initially, intended to investigate the frequency of variant genotypes in 80 patients with T2D. Then, the effect of variant genotypes of CYP2C9 on responses to sulfonylureas including glibenclamide and gliclazide was examined. The association between hypoglycemic ADRs and variant genotypes in T2 diabetics who were treated with sulfonylureas (glibenclamide or gliclazide) was also sought. Finally, the influence of variant genotypes on diabetic nephropathy and retinopathy was studied.
Investigating the prevalence of different CYP2C9 genotypes, it was found that the wild-type allele (CYP2C9*1) was the highest. This result is similar to the allelic frequency reported in the study conducted by Ataby et al in the north of Iran, involving patients from Turkman and Fars ethnic groups.24
Similarly, several other studies showed that the most prevalent allele of CYP2C9*1 was the wild-type allele.9,25-36 Also, it was reported that the second most prevalent allele was the CYP2C9*2 allele (15 %), which is consistent with the previous reports in Caucasian populations.37 However, the lowest frequency of this allele was observed in the Africans (0.46%), East Asians (0.56%) and Native Americans (1.25%).37 CYP2C9*3 allele in our study was found to be 5%, similar to the allelic frequency observed in Ataby for Turkman and Fars ethnic groups.24 In contrast, CYP2C9*3 showed the highest frequency among the South Asians (11.7%).37 Moreover, the frequency of the CYP2C9*3/*3 homozygous genotype was not identified in our study as well as in the Caucasian ethnic groups,38,39 whereas it was detected frequently in the Malay and Indian ethnic groups.22 Overall, these data show that the allelic frequency of the Iranian ethnic groups is similar to that of the Caucasian population.
To find out the different responses of glibenclamide treatment in the patients with various CYP2C9 genotypes, the plasma level of glibenclamide in T2 diabetic patients with CYP2C9*1/*1, CYP2C9*1/*2, CYP2C9*1/*3, CYP2C9*2/*2, and CYP2C9*2/*3 genotypes was measured 2.5 hours after the treatment. The plasma concentration of gliclazide was also measured for the same genotypes 12 hours after the treatment. Given that the peak of plasma concentration in the previous studies reached a maximum of 2 hours after the glibenclamide treatment,15 the plasma level was measured 2.5 hours after the administration in our study. However, as gliclazide remains in plasma for a longer time, the measurement was, thus, done 12 hours after the administration. Consistent with the previous studies, the highest plasma level of glibenclamide was observed in the CYP2C9*1/*3 (0.8µg/mL). Moreover, the plasma level of gliclazide was higher not only in the CYP2C9*1/*3 genotype but also in CYP2C9*2/*3 genotypes (2.46µg/mL). In contrast, the lowest level of glibenclamide and gliclazide concentration in the plasma was observed in the wild-type CYP2C9*1/*1 genotype. Therefore, this result implies that the elimination of plasma glibenclamide and gliclazide in patients with CYP2C9*1/*3 may be slower than that in patients with CYP2C9*1/*1. This, in turn, indicates that the higher concentration of glibenclamide and gliclazide may cause stronger pharmacological effects. Moreover, it was found that the plasma concentration of glibenclamide and gliclazide in other variant genotypes, namely CYP2C9*1/*2 and CYP2C9*2/*2 was higher than that in the wild-type genotype (Table 2). However, the plasma level of gliclazide in CYP2C9*2/*2 was similar to that in the wild-type CYP2C9*1/*1 genotypes. Overall, these data showed that in the patients with wild-type genotypes, the elimination of glibenclamide and gliclazide was likely to be faster than that invariant genotypes, as a lower concentration of such drugs is needed for the patients with wild-type genotypes.
The association of variant genotypes with hypoglycemic ADRs in T2 diabetic patients treated with the sulfonylureas glibenclamide or gliclazide was, in turn, investigated. The results showed that the presence of variant genotypes predisposes sulfonylurea-treated patients to hypoglycemia. It was found that in individuals with variant genotypes (CYP2C9*1/*2, CYP2C9*1/*3, CYP2C9*2/*2, CYP2C9*2/*3) when treated with sulfonylureas, the risk of suffering a hypoglycemic event significantly increased. Similarly, in a study with a limited number of patients (i.e., 20 patients), Holstein et al reported that CYP2C9*2/*3 and CYP2C9*1/*3 genotypes correlated with severe hypoglycemia.40 By contrast, in the study conducted by Surendiran et al, there was no significant difference in the occurrence or severity of hypoglycemia.41 Accordingly, since hypoglycemia can significantly cause morbidity and mortality, the treatment protocol for diabetes should be geared to the patients’ individual needs to reduce the occurrence of hypoglycemic episodes. It is suggested that, particularly at the beginning of the treatment by sulfonylurea, genotype analysis is likely to prevent overdose in patients with CYP2C9 genotypes, causing lower activity.42 In effect, identifying the genotype of the patient might help the physician adjust the regimen protocol accordingly, and therefore reduce the possibility of the patient’s experiencing a hypoglycemic event. This approach to CYP2C9 genotyping of patients before the treatment by glimepiride has already been adopted in Korea and Russia.43,44 Our data also provide evidence supporting the use of such an approach.
Limitations
There are several limitations to consider in this study, including the small sample size, compared to Go-DART trials11 studies, limiting the generalizability of the findings. Indeed, despite registering180 patients for the research purpose, we could only include data from 82 patients in the final analysis as some of the patients did not cooperate to be compatible with our inclusion criteria. However, the association of plasma level of sulfonylurea with CYP2C9 genotypes was statistically significant (p-value less than 0.05). Moreover, future studies using large mega studies seem necessary to confirm our findings.
To the best of our knowledge, this may be the first study on the impact of CYP2C9 genotype variants on retinopathy in patients with T2D. The data showed that in the absence of wild-type alleles, all patients were affected by retinopathy, while the presence of wild-type allele delayed the microvascular complications (Figure 1). However, it is not clear how CYP2C9 variant alleles (*2 and *3) influenced the retinal microvasculatures, but a few studies have reported the influence of CYP2C9 and their products, namely the epoxyeicosatrienoic acids (EETs), in the hypoxia-induced VEGF production and pathologic retinal angiogenesis.45 Also, comparing the risk of nephropathy in the patients with different CYP2C9 alleles, based on the marked increase in microalbuminuria and the decrease observed in the glomerular filtration rate (GFR), 66.7% of the patients with CYp2C9*2/*2 and CYP2C9*2/*3 genotypes were identified to be affected by nephropathy (Figure 2). It seems that the presence of wild-type alleles (*1/*1, *1/*2 and *1/*3) protected the normal function of the kidney in patients with T2D. However, the precise mechanism of CYP2C9 in diabetic retinopathy and nephropathy is still unclear.
It is concluded that the genotype analysis of CYP2C9 in patients with T2D can provide guidelines for the optimal management of the treatment protocol with sulfonylurea by physicians so that they can make sound decisions to regulate the treatment protocol accordingly before the initiation of sulfonylurea therapy, and thus prevent the hypoglycemic events.
Ethics Approval and Consent to Participate
In this clinical experimental study, all peripheral blood samples were collected and used by the ethical rules confirmed by the ethics committee of Ahvaz Jundishapur University of Medical Sciences (Code no: IR.AJUMS.REC.139.221). Ethical issues (including plagiarism, informed consent, misconduct, data fabrication and/or falsification, double publication and/or submission, redundancy, etc.) have been completely observed by the authors. Written informed consent was also obtained from all patients. Data were anonymously and confidentially retrieved with compliance with the Declaration of Helsinki.
Acknowledgments
We thank the patients and nurses in diabetic specific clinics at Imam Khomeini and Golestan Hospitals affiliated to Ahvaz Jundishpur University of Medical Sciences, Ahvaz, Iran for their contribution to the research. The study was supported by the grant provided by the Deputy of Research Affairs at Ahvaz Jundishpur University of Medical Sciences.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest.
References
1. Federation ID, editor. IDF Diabetes Atlas Update Poster. Brussels, Belgium: International Diabetes Federation; 20152015.
2. Bressler R, Johnson DG. Pharmacological regulation of blood glucose levels in non—insulin-department diabetes mellitus. Arch Intern Med. 1997;157(8):836–848. doi:10.1001/archinte.1997.00440290014001
3. Aguilar-Bryan L, Nichols CG, Wechsler SW, Clement JP
4. Tessier D, Dawson K, Tetrault J, Bravo G, Meneilly G. Glibenclamide vs gliclazide in type 2 diabetes of the elderly. Diabet Med. 1994;11(10):974–980. doi:10.1111/j.1464-5491.1994.tb00256.x
5. Holstein A, Plaschke A, Egberts EH. Lower incidence of severe hypoglycemia in patients with type 2 diabetes treated with glimepiride versus glibenclamide. Diabetes Metab Res Rev. 2001;17(6):467–473. doi:10.1002/dmrr.235
6. Gangji AS, Cukierman T, Gerstein HC, Goldsmith CH, Clase CM. A systematic review and meta-analysis of hypoglycemia and cardiovascular events. Diabetes Care. 2007;30(2):389–394. doi:10.2337/dc06-1789
7. Lee CR, Goldstein JA, Pieper JA. Cytochrome P450 2C9 polymorphisms: a comprehensive review of the in-vitro and human data. Pharmacogenet Genomics. 2002;12(3):251–263. doi:10.1097/00008571-200204000-00010
8. Takanashi K, Tainaka H, Kobayashi K, Yasumori T, Hosakawa M, Chiba K. CYP2C9 Ile359 and Leu359 variants: enzyme kinetic study with seven substrates. Pharmacogenet Genomics. 2000;10(2):95–104. doi:10.1097/00008571-200003000-00001
9. Sullivan-Klose TH, Ghanayem BI, Bell DA, et al. The role of the CFP2C9-Leu 359 allelic variant in the tolbutamide polymorphism. Pharmacogenet Genomics. 1996;6(4):341–349. doi:10.1097/00008571-199608000-00007
10. Inoue K, Yamazaki H, Imiya K, Akasaka S, Guengerich FP, Shimada T. Relationship between CYP2C9 and 2C19 genotypes and tolbutamide methyl hydroxylation and S-mephenytoin 4ʹ-hydroxylation activities in livers of Japanese and Caucasian populations. Pharmacogenet Genomics. 1997;7(2):103–113. doi:10.1097/00008571-199704000-00003
11. Zhou K, Donelly L, Burch L, et al. Loss–off-functionCYP2C9 variants improve therapeutic response to sulfonylureas in type 2 diabetes: a go-DARTS study. Clin Pharmacol Ther. 2010;87(1):52–56. doi:10.1038/clpt.2009.176
12. Kirchheiner J, Bauer S, Meineke I, et al. Impact of CYP2C9 and CYP2C19 polymorphisms on tolbutamide kinetics and the insulin and glucose response in healthy volunteers. Pharmacogenet Genomics. 2002;12(2):101–109. doi:10.1097/00008571-200203000-00004
13. Shon J-H, Yoon Y-R, Kim K-A, et al. Effects of CYP2C19 and CYP2C9 genetic polymorphisms on the disposition of and blood glucose lowering response to tolbutamide in humans. Pharmacogenet Genomics. 2002;12(2):111–119. doi:10.1097/00008571-200203000-00005
14. Suzuki K, Yanagawa T, Shibasaki T, Kaniwa N, Hasegawa R, Tohkin M. Effect of CYP2C9 genetic polymorphisms on the efficacy and pharmacokinetics of glimepiride in subjects with type 2 diabetes. Diabetes Res Clin Pract. 2006;72(2):148–154. doi:10.1016/j.diabres.2005.09.019
15. Niemi M, Cascorbi I, Timm R, Kroemer HK, Neuvonen PJ, Kivistö KT. Glyburide and glimepiride pharmacokinetics in subjects with different CYP2C9 genotypes. Clin Pharmacol Ther. 2002;72(3):326–332. doi:10.1067/mcp.2002.127495
16. American Academy of Ophthalmology. Preferred Practice Pattern: Diabetic Retinopathy. September 20; 2014; San Francisco, Calif: American Academy of Ophthalmology.
17. Capozzi ME, McCollum GW, Penn JS. The role of cytochrome P450 epoxygenases in retinal angiogenesis cytochrome P450 epoxygenases. Invest Ophthalmol Vis Sci. 2014;55(7):4253–4260. doi:10.1167/iovs.14-14216
18. Suzuki S, Oguro A, Osada-Oka M, Funae Y, Imaoka S. Epoxyeicosatrienoic acids and/or their metabolites promote hypoxic response of cells. J Pharmacol Sci. 2008;108(1):79–88. doi:10.1254/jphs.08122FP
19. Shao H, Ren X, Liu N, et al. Influence of CYP2C9 and CYP2C19 genetic polymorphisms on pharmacokinetics and pharmacodynamics of gliclazide in healthy Chinese Han volunteers. J Clin Pharm Ther. 2010;35(3):351–360. doi:10.1111/j.1365-2710.2009.01134.x
20. Rajendran S, Philip B, Gopinath R, Suresh B. RP-HPLC method for the estimation of glibenclamide in human serum. Indian J Pharm Sci. 2007;69(6):796. doi:10.4103/0250-474X.39436
21. Venkatesh P, Harisudhan T, Choudhury H, Mullangi R, Srinivas NR. Simultaneous estimation of six anti‐diabetic drugs—glibenclamide, gliclazide, glipizide, pioglitazone, repaglinide and rosiglitazone: development of a novel HPLC method for use in the analysis of pharmaceutical formulations and its application to human plasma assay. Biomed Chromatogr. 2006;20(10):1043–1048. doi:10.1002/bmc.635
22. Seng KC, Gin GG, Sangkar JV, Phipps ME. Frequency of cytochrome P450 2C9 (CYP2C9) alleles in three ethnic groups in Malaysia. Asia Pac J Mol Biol Biotechnol. 2003;11(2):83–91.
23. Levey AS, Coresh J, Balk E, et al. National kidney foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003;139(2):137–147. doi:10.7326/0003-4819-139-2-200307150-00013
24. Ataby OA, Tabari RG, Mansourian AR, Samai NM, Marjani A. Genetic polymorphism of cytochrome P450 2C9 (CYP2C9) in two ethnic groups in Iran. Am J Biomed Sci. 2013;5(3):177–187. doi:10.5099/aj130300177
25. Wang S-L, Huang J-D, Lai M-D, Tsai -J-J. Detection of CYP2C9 polymorphism based on the polymerase chain reaction in Chinese. Pharmacogenet Genomics. 1995;5(1):37–42. doi:10.1097/00008571-199502000-00004
26. Stubbins MJ, Harries LW, Smith G, Tarbit MH, Wolf CR. Genetic analysis of the human cytochrome P450 CYP2C9 locus. Pharmacogenet Genomics. 1996;6(5):429–439. doi:10.1097/00008571-199610000-00007
27. Nasu K, Kubot T, Ishizaki T. Genetic analysis of CYP2C9 polymorphism in a Japanese population. Pharmacogenet Genomics. 1997;7(5):405–409. doi:10.1097/00008571-199710000-00011
28. Ackermann E, Cascorbi I, Sachse C, Brockmoller J, Mrozikiewiza P, Roots I. Frequencies and the allelic linkage of CYP2C9 mutations in a German population and the detection of a C/T mutation in intron 2. Eur J Clin Pharmacol. 1997;52:A71.
29. Kimura M, Ieiri I, Mamiya K, Urae A, Higuchi S. Genetic polymorphism of cytochrome P450s, CYP2C19, and CYP2C9 in a Japanese population. Ther Drug Monit. 1998;20(3):243–247. doi:10.1097/00007691-199806000-00001
30. Yasar Ü, Eliasson E, Dahl M-L, Johansson I, Ingelman-Sundberg M, Sjöqvist F. Validation of methods for CYP2C9 genotyping: frequencies of mutant alleles in a Swedish population. Biochem Biophys Res Commun. 1999;254(3):628–631. doi:10.1006/bbrc.1998.9992
31. Brockmöller J, Bauer S, Sachse C, et al. Frequency of cytochrome P450 CYP2C9 variants in a Turkish population and functional relevance for phenytoin. Br J Clin Pharmacol. 1999;48(3):409–415. doi:10.1046/j.1365-2125.1999.00012.x
32. Gaedigk A. Interethnic differences of drug-metabolizing enzymes. Int J Clin Pharmacol Ther. 2000;38(2):61–68. doi:10.5414/CPP38061
33. Kim J, Gaedigk A, Leeder J, Kearns G, Bertino J. Cyp2c9 mutant alleles frequencies in a rural us Caucasian population. Clin Pharmacol Ther. 2000;67(2):120.
34. Choo E, Dresser G, Stein C, et al. Identification of a new CYP2C9 variant in African-Americans. Clin Pharmacol Ther. 2000;67(2):169.
35. Jittikoon J, Mahasirimongkol S, Charoenyingwattana A, et al. Comparison of genetic variation in drug ADME-related genes in Thais with Caucasian, African and Asian HapMap populations. J Hum Genet. 2016;61(2):119–127. doi:10.1038/jhg.2015.115
36. Villegas-Torres B, Sánchez-Girón F, Jaramillo-Villafuerte K, Soberón X, Gonzalez-Covarrubias V. Genotype frequencies of VKORC1 and CYP2C9 in native and Mestizo populations from Mexico, potential impact for coumarin dosing. Gene. 2015;558(2):235–240. doi:10.1016/j.gene.2014.12.068
37. Céspedes-Garro C, Fricke-Galindo I, Naranjo MEG, et al. Worldwide interethnic variability and geographical distribution of CYP2C9 genotypes and phenotypes. Expert Opin Drug Metab Toxicol. 2015;11(12):1893–1905. doi:10.1517/17425255.2015.1111871
38. Aithal GP, Day CP, Kesteven PJ, Daly AK. Association of polymorphisms in the cytochrome P450 CYP2C9 with warfarin dose requirement and risk of bleeding complications. Lancet. 1999;353(9154):717–719. doi:10.1016/S0140-6736(98)04474-2
39. Gaedigk A, Casley WL, Tyndale RF, Sellers EM, Jurima-Romet M, Leeder JS. Cytochrome P4502C9 (CYP2C9) allele frequencies in Canadian Native Indian and Inuit populations. Can J Physiol Pharmacol. 2001;79(10):841–847. doi:10.1139/y01-065
40. Holstein A, Plaschke A, Ptak M, et al. Association between CYP2C9 slow metabolizer genotypes and severe hypoglycemia on medication with sulphonylurea hypoglycaemic agents. Br J Clin Pharmacol. 2005;60(1):103–106. doi:10.1111/j.1365-2125.2005.02379.x
41. Surendiran A, Pradhan S, Agrawal A, et al. Influence of CYP2C9 gene polymorphisms on response to glibenclamide in type 2 diabetes mellitus patients. Eur J Clin Pharmacol. 2011;67(8):797–801. doi:10.1007/s00228-011-1013-8
42. Kirchheiner J, Roots I, Goldammer M, Rosenkranz B, Brockmöller J. Effect of genetic polymorphisms in cytochrome P450 (CYP) 2C9 and CYP2C8 on the pharmacokinetics of oral antidiabetic drugs. Clin Pharmacokinet. 2005;44(12):1209–1225. doi:10.2165/00003088-200544120-00002
43. Kim YM, Yoo SH, Kang RY, et al. Identifying drugs needing pharmacogenetic monitoring in a Korean hospital. Am J Health Syst Pharm. 2007;64(2):166–175. doi:10.2146/ajhp050490
44. Mosikian A, Dolgorukova A, Zalevskaya A. Possible approaches to CYP2C9-guided prescription of sulfonylureas in Russia. Pharmacogenomics. 2016;17(18):2115–2126. doi:10.2217/pgs-2016-0121
45. Tacconelli S, Patrignani P. Inside epoxyeicosatrienoic acids and cardiovascular disease. Front Pharmacol. 2014;5:239. doi:10.3389/fphar.2014.00239
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.