")
Back to Journals » Infection and Drug Resistance » Volume 15
The Diagnosis of Severe Fever with Thrombocytopenia Syndrome Using Metagenomic Next-Generation Sequencing: Case Report and Literature Review
Authors Zhan L, Huang K, Xia W, Chen J, Wang L, Lu J, Wang J, Lin J , Wu W
Received 11 November 2021
Accepted for publication 21 December 2021
Published 11 January 2022 Volume 2022:15 Pages 83—89
DOI https://doi.org/10.2147/IDR.S345991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Liying Zhan,1,* Kai Huang,2,* Wenfang Xia,1 Jingdi Chen,3 Lu Wang,1 Jiaming Lu,4 Jing Wang,4 Jun Lin,2,4 Wei Wu1
1Department of Critical Care Medicine, Renmin Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China; 2Department of Gastroenterology, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China; 3Department of Orthopedics, The Airborne Military Hospital, Wuhan, Hubei, People’s Republic of China; 4Department of Gastroenterology, Renmin Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Wu; Jun Lin Email [email protected]; [email protected]
Background: Severe fever with thrombocytopenia syndrome (SFTS) is an infectious disease caused by a bunyaviridae virus. Its main clinical manifestation is fever with thrombocytopenia, which may be accompanied by other clinical symptoms. Here, we report a patient diagnosed with SFTS using metagenomic next‑generation sequencing (mNGS).
Case Presentation: A 56-year-old female patient was hospitalized with intermittent diarrhea and fever. She visited a local clinic for treatment, but instead of improving, the symptoms progressed to unconsciousness.
Diagnosis: Using mNGS, we isolated the bunyaviridae virus and several other pathogens from the patient’s blood samples to confirm the diagnosis.
Interventions: The patient was treated with symptomatic and supportive therapy, including intravenous human γ-globulin (20 g/d), platelet transfusion, platelet elevation (subcutaneous injection of recombinant human thrombopoietin, 15,000 IU), white blood cell elevation (subcutaneous injection of recombinant human granulocyte colony-stimulating factor, 200 ug, qd); and antibiotic (cefoperazone sodium and tazobactam sodium, 2 g, q8h), antiviral (ganciclovir, 250 mg, q12h), and antifungal therapy (voriconazole for injection, 0.2 g, q12h). After ten days of treatment, the patient’s condition gradually improved.
Conclusion: Compared to traditional detection methods, mNGS has many advantages. It can quickly identify the pathogen when the patient’s clinical manifestations are complex and difficult to diagnose, resulting in the formulation of an effective treatment.
Keywords: severe fever with thrombocytopenia syndrome, metagenomic next‑generation sequencing, bunyaviridae virus
Background
Severe fever with thrombocytopenia syndrome (SFTS) is an infectious disease characterized by decreases in white blood cells and platelets. The pathogenic virus is the severe fever with thrombocytopenia syndrome bunyavirus (SFTSV). Since 2006, a tick-borne disease named Human granulocytic anaplasmosis (HGA) has been reported in some rural areas in China. The SFTSV was first isolated from the blood in HGA patient in 2009.1 Japan and South Korea have reported similar SFTS cases.2,3
The incubation period of SFTS is unclear and may be 1–2 weeks. Its clinical manifestations are complex, and the lesions can involve organs and tissues of multiple systems, which can cause misdiagnoses and affect patient prognosis. The main clinical manifestations are fever, with body temperatures often greater than 38°C. The affected patient can have a continuous high fever reaching more than 40°C. Physical examinations often find that the neck, groin, and other superficial lymph nodes are enlarged and tender.
A few critical cases have been reported; patients may die from shock, respiratory failure, or disseminated intravascular coagulation. The severity and prognosis of SFTS are related to viral replication and the host immune response. The vast majority of patients have a good prognosis, but patients with prior basic diseases, psychoneurosis symptoms, bleeding tendencies, hyponatremia, and who are elderly may have poor prognosis.
SFTS is often misdiagnosed as hemorrhagic fever with renal syndrome or human granulocytic anaplasmosis.4 Patients come mainly from mountainous and hilly areas. Healthy people can become infected with the SFTSV after being bitten by a tick, and the disease can occur after contact with a patient’s blood or bodily fluids if protective measures are not taken. Aerosols can also cause human-to-human transmission.5–7 The diagnosis of SFTS requires one of the following conditions: SFTSV is isolated from a patient’s sample, SFTSV RNA is detected in the patient’s blood or serum, or SFTSV-specific antibodies are detected in the patient’s serum.8
Metagenomic next-generation sequencing (mNGS), also known as high-throughput or large-scale parallel sequencing, can independently sequence thousands to billions of DNA or RNA fragments simultaneously. It can detect pathogenic microorganisms in various body fluids and is valuable in the diagnosis of infectious diseases.9–11 mNGS may overcome the limitations of current diagnostic tests by directly detecting all pathogens in clinical samples regardless of microorganism type (ie, virus, bacteria, fungi, or parasite). It may even be applied to the discovery of new pathogens. Compared to traditional methods, such as microbial culturing, nucleic acid amplification, serological pathogen antibody detection, and polymerase chain reactions (PCRs) for specific pathogens, mNGS has many advantages in pathogen detection. Traditional PCR detection requires the pre-design of primers based on the sequence information of known pathogens, while mNGS can perform unbiased sequencing of all nucleic acid sequences in clinical samples. Notably, mNGS was used to quickly detect the SARS-CoV-2 coronavirus in patient alveolar lavage fluid and to sequence its entire genome.12 When patients are infected with multiple pathogens, mNGS can detect all pathogens, thereby allowing time for doctors to make a clear diagnosis. Furthermore, mNGS can detect differences between animal-derived and human-derived pathogens and explore the origins of zoonotic diseases.13 Etiological diagnosis is crucial in the diagnosis of infectious diseases. Critically ill patients often have severe infections, and many of them do not know the source of their infection. This lack of information makes it difficult for physicians to quickly establish a treatment for the patient. When appropriate, the use of mNGS can allow us to discover new or unexpected pathogens and quantitatively detect any portion of their genomes.
Case Presentation
On May 1, 2021, a 56-year-old female patient was hospitalized with intermittent diarrhea lasting for 6 d and fever lasting for 3 d. Six days earlier, the patient had unprovoked diarrhea with vomiting and fatigue, after which she visited a local clinic. The doctor’s treatment plan was unclear, but the patient still had diarrhea. Three days later, the patient developed fever where the highest temperature was 39.4°C. The patient visited another local hospital and was diagnosed with infectious diarrhea. The physicians there prescribed antibiotics and antivirals, protected the stomach, and treated the symptoms, but the patient’s symptoms remained unabated. The patient subsequently developed shock, cognitive decline, and abdominal pain. After treatment at the local hospital, she was transported to Renmin Hospital of Wuhan University. The patient had fever of unknown origin, so she was admitted to the intensive isolation ward.
Except for unexplained diarrhea and fever, the patient also had hypertension, hyperthyroidism, and type 2 diabetes mellitus.
On admission, she had a body temperature of 37.6 °C, heart rate of 95/min, respiratory rate of 24/min, and blood pressure of 111/77 mmHg. Heart and breathing sounds were generally normal; she had no swelling of the superficial lymph nodes. The laboratory tests indicated thrombocytopenia (platelet: 32 × 109/L) and leukocytopenia (WBC: 2.87 × 109/L). The lymphocyte ratio (34.30%) and lactate dehydrogenase levels were normal. However, alanine aminotransferase (64 IU/L), aspartate aminotransferase (140 IU/L), procalcitonin (0.45 ng/mL), creatine kinase-MB (9.15 ng/mL) and TnI-Ultra (0.367 ng/mL) levels were elevated.
After admission, the treatment plan was antibiotics (cefoperazone sodium and tazobactam sodium, 2 g, q8h; ganciclovir, 250 mg, q12h), recombinant human thrombopoietin (TPO, 15,000 IU, subcutaneous injection), recombinant human granulocyte colony-stimulating factor (200 ug, subcutaneous injection), nutritional support, and organ protection treatment.
However, the patient’s condition gradually deteriorated. She developed disturbances in consciousness, mixed aphasia, and could not answer questions. On physical examination, she had equally large bilateral pupils (3.5 mm), obvious stiff-neck, and bilateral positive Kernig symptoms. We continued to improve our inspection. The Widal reaction was negative, and the echocardiogram, electroencephalogram, and chest X-rays showed no abnormalities. The brain magnetic resonance imaging, magnetic resonance venography, and diffusion weighted imaging displayed abnormal signal in the centrum semiovale and parietal and occipital lobes, indicating possible inflammatory lesions (Figure 1). The neurologist recommended a lumbar puncture, but it was refused by the patient’s family due to her low platelet count and consequent high risk of bleeding.
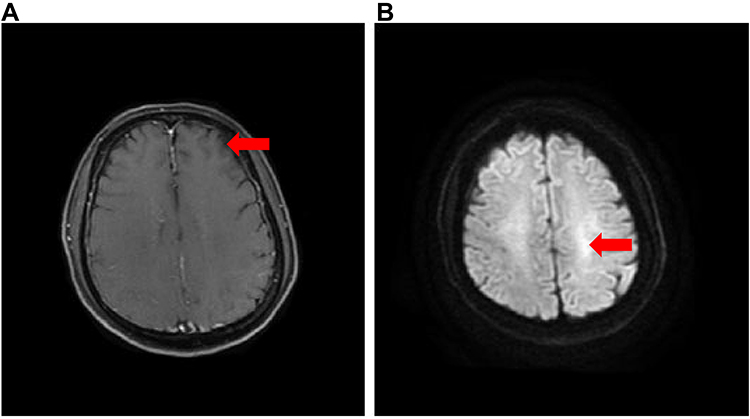 |
Figure 1 Brain magnetic resonance imaging (MRI) The red arrows in Figure 1 indicate the possible location of the lesion. (A) left parietal lobe and occipital lobe. (B) left centrum semiovale abnormal signal, considering the possibility of inflammation. |
At this point, the patient’s diagnosis remained unclear. We followed up on her medical history. Before the onset of her symptoms, she had traveled to a mountainous area to pick tea leaves and may have been bitten by ticks. Tick bites had been reported in the local area. Therefore, combined with the patient’s clinical manifestations and biochemical results, we suspected that she had SFTS.
We took blood and sputum samples for pathogenic microorganism culturing. As SFTS is an infectious disease, we also sent the blood sample to the Center for Disease Control and Prevention (CDC) of Hubei province.
Given that the disease may be caused by atypical pathogens, the low detection rate of conventional detection methods, and the patient’s critical condition, we proceeded with mNGS. Two days later, Aspergillus flavus/A. oryzae and SFTSV were detected in the blood mNGS, and A. flavus/A. oryzae and Epstein-Barr virus were detected in the sputum mNGS. We ultimately established a diagnosis of SFTS and reported it to the CDC. In addition, before the onset of illness, the patient was consuming soaked black fungus long term and so the possibility of aflatoxin poisoning was considered. After platelet-boosting therapy (TPO, 15,000 IU) and platelet transfusion, her platelet count increased. In combination with antibiotics (cefoperazone sodium and tazobactam sodium, 2 g, q8h; ganciclovir, 250 mg, q12h; voriconazole for injection, 0.2 g, q12h), we also gave the patient human γ-globulin (20 g, qd) infusions to strengthen her immunity.
On the fifth day after admission, the patient gradually regained consciousness and was able to intermittently vocalize. While her blood and sputum culture results were negative, based on her medical history and the mNGS results, her diagnosis was clear. With treatment, her condition gradually improved. The patient’s temperature returned to normal and by day 10, she could properly communicate with doctors. The results from the laboratory examination indicated normal platelet counts (149 × 109/L). All indicators returned to normal except for mild anemia (Figure 2). Accordingly, the patient was transferred out of the intensive care unit, recovered, and was ultimately discharged from the hospital on day 18.
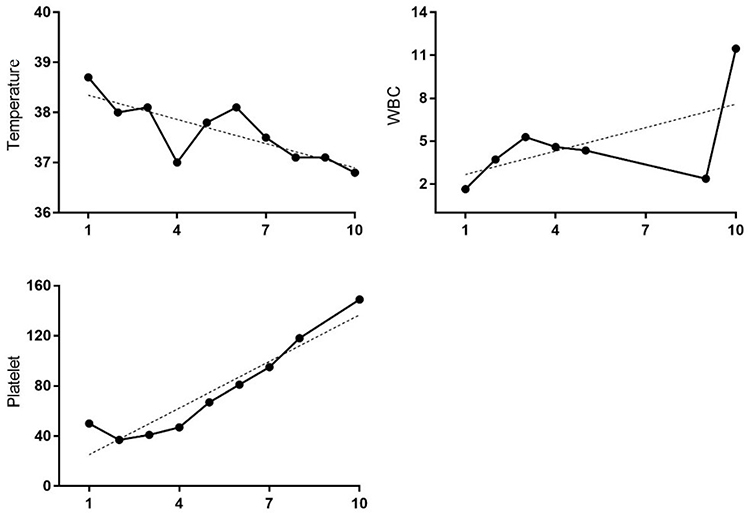 |
Figure 2 Clinical course: Horizontal axis represents the days after admission. Ordinate of each graph: Temperature (°C), WBC (10*9/L), Platelet (10*9/L). Dashed line represents the trend. The patient’s body temperature fluctuates up and down, but generally decreases until the body temperature returns to normal. With platelet transfusions and leukocyte promoting therapy, the patient’s platelet levels and white blood cell count increased. |
Discussion and Conclusions
Here, we describe the case of a 56-year-old woman suffering from SFTS. Using mNGS, we were able to quickly diagnose the disease and develop an effective treatment plan, ultimately saving her life.
When the patient is in critical condition and infected with rare pathogens, routine blood or sputum culture may fail to detect the pathogen. In this case, via the use of mNGS, we found co-infection with multiple pathogens. This information allowed us to create an etiological treatment. Due to the timely and correct treatment, the patient’s condition gradually improved, and she eventually recovered. mNGS is already being used in clinical practice to help doctors identify disease pathogens. However, no reports have yet been published regarding its use in diagnosing SFTS. Previously, a 63-year-old Japanese woman was diagnosed with SFTS based on a positive serum test for SFTSV RNA and the changes of electroencephalogram (EEG).14 Another 62-year-old previously healthy woman diagnosed as having SFTS by real-time reverse transcription polymerase chain reaction.15 Here, we report for the first time a case of serologically negative SFTS diagnosed via mNGS.
This case demonstrates the advantage of mNGS in the diagnosis of unexplained infections, especially for those that are severe. Timely diagnosis can help quickly develop an effective treatment. However, some doubts persist regarding the present case. On one hand, the patient’s fever, diarrhea, and other clinical manifestations could be caused by SFTS. On the other, several other pathogens can cause similar clinical manifestations. A. flavus produces aflatoxins, which can give rise to nausea, vomiting, diarrhea, and even intracranial infections. If we had found other pathogens in the cerebrospinal fluid, we could have located the patient’s source of infection. Her family refused a lumbar puncture; thus, we collected blood samples for the mNGS tests. Even if other pathogens were detected, we still cannot confirm if the results are due to the patient’s own infection or to contaminated blood samples. The patient’s medical history is needed, a disadvantage of mNGS. However, combined with the patient’s characteristics and examination results, we can make a definite diagnosis of SFTS. While there is no specific treatment for SFTS, symptomatic treatment is mainly used. In that case, we use platelet-boosting therapy, platelet transfusion, several antibiotics and human γ-globulin to treat patients. Thrombopoietin is often used to treat thrombocytopenia, but a new therapy has recently been reported to boost patients’ platelets. In a retrospective multicenter study, eltrombopag is thought to increase platelet counts. Moreover, platelets can be elevated in early stage of treatment without the need for a combination of other drugs. Although further studies are needed to assess the long-term efficacy of eltrombopag, it may play a key role in a quick therapy.16
SFTS is a rare clinical disease that in many cases cannot be detected and diagnosed early. When the diagnosis is unclear, symptomatic treatment would only delay the treatment. After the rapid diagnosis of SFTS by mNGS, the early and accurate treatment saved the patient’s life. Pediatric patients with SFTS have less vague subjective complaints and sometimes the clinical course is not obvious. At this time, the application of mNGS is very important for the early diagnosis of SFTS in children.17 mNGS not only has a fast detection speed, but it can also detect the simultaneous infection of multiple pathogens. In addition to the timely treatment of patients, mNGS can also reduce average hospital stay and patient mortality. With the continuous improvement of mNGS technology, its clinical application is increasing.
Clinical manifestations and laboratory examinations of central nervous system (CNS) infection include fever, headache, meningeal irritation, vomiting, convulsions, and increased white blood cell count and protein levels in the cerebrospinal fluid. Many new and rare pathogens have been successfully detected in CNS infections via the use of mNGS, such as Brucella melitensis, Candida tropicalis, and Leptospira santarosai.18 In addition, mNGS have a high detection rate of pathogenic bacteria in tuberculous meningitis patients.11
Previous reports have demonstrated the advantages of mNGS application over traditional bacterial methods in blood samples.19 In terms of diagnostic efficacy, mNGS had a greater than six-fold higher positivity rate than blood culture in a 28-day study.20 Chen et al used routine microbiological tests and mNGS to detect potential pathogens in blood samples of patients with severe pneumonia. mNGS-positive results were found in 10 of the blood samples, but only one was found using conventional blood culture.19 Moreover, bloodstream infection has been shown to be an important predictor of poor outcome in patients with severe pneumonia.21 For severe infections, timely identification of bloodstream infection guides accurate therapy. Speed of detection is also an advantage of mNGS. It takes only about 30 h from sample preparation to the identification report, thereby providing a promising diagnostic platform for critically ill patients with blood-borne infections.22
In respiratory infections, pneumonia is a common infection. In most cases, empirical antibiotic therapy works well. However, in a few cases, especially in those with severe infections, finding the source of the infection is essential for effective treatment. Besides sputum and alveolar lavage fluid, mNGS can also detect pathogens in lung biopsy specimens, with potential advantages in terms of speed and sensitivity. Chen et al used routine microbiological tests and mNGS to detect potential pathogens in bronchoalveolar lavage fluid (BALF) from patients with severe pneumonia. In these patients, the mNGS test demonstrated an 85% (17/20) positive rate. By contrast, conventional microbiological tests displayed a 50% (10/20) positive rate. Moreover, mNGS of the BALF can reveal dynamic alterations in microbial species parameters after treatment.23 In a retrospective study, Zhang et al used various human clinical specimens to evaluate mNGS in the diagnosis of focal infection. The clinical diagnosis coincidence rate of mNGS (86.30%) was substantially higher than the culture method (45.21%), which is noteworthy given that 85.00% of patients with culture-negative focal infections have additional pathogen diagnoses.24 Compared to conventional diagnostics, mNGS improved pathogen detection in BALF from hematopoietic cellular transplant patients. Finally, one study reported the use of mNGS in the investigation of putative nosocomial outbreaks.25
Many colorectal cancers are difficult to diagnose at an early stage because their clinical manifestations are not obvious. Using mNGS and metabolomic analyses, researchers found that the microbiome and metabolome begins to change in the early stages of colorectal cancer, thereby providing a new direction for its early diagnosis.26
As a revolutionary technology, mNGS surpasses traditional detection techniques in many ways. Compared with traditional pathogen detection methods, mNGS has more detection types, does not need cultures, is unaffected by antibiotics, and can simultaneously identify bacteria, fungi, viruses, and protozoa in samples. Furthermore, mNGS can help clinicians quickly diagnose unknown infections, thus reducing the use of empirical antibiotics and helping to develop accurate treatment plans. However, mNGS has some shortcomings. For example, RNA degrades easily, and the transcription process is complex. Accordingly, it is difficult to detect RNA viruses using mNGS. Similar problems exist with testing for drug-resistant genes. Additionally, before using mNGS, the human host background must be sequenced, and not all genomes are available. Also, specimens are susceptible to contamination by environmental species, which can lead to false results. The cost of testing is another disadvantage.27 At present, due to sampling standards, testing costs, testing methods, and other limitations, mNGS cannot replace traditional microbial testing methods.
In summary, as a comprehensive direct detection technology, mNGS is expected to become a first-line clinical diagnostic technique in the future.
Patient Consent and Ethics Statement
The patient provided informed consent for publication of the case. No ethical committee approval was required for this study as the data had been analyzed in a retrospective manner.
Acknowledgment
We thank American Journal Experts for language editing.
Funding
This work was supported by “the Fundamental Research Funds for the Central Universities” (2042020kf0057).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Yu XJ, Liang MF, Zhang SY, et al. Fever with thrombocytopenia associated with a novel bunyavirus in China. N Engl J Med. 2011;364(16):1523–1532. doi:10.1056/NEJMoa1010095
2. Kato H, Yamagishi T, Shimada T, et al. Epidemiological and clinical features of severe fever with thrombocytopenia syndrome in Japan, 2013–2014. PLoS One. 2016;11(10):e0165207. doi:10.1371/journal.pone.0165207
3. Shin J, Kwon D, Youn SK, Park JH. Characteristics and factors associated with death among patients hospitalized for severe fever with thrombocytopenia syndrome, South Korea, 2013. Emerg Infect Dis. 2015;21(10):1704–1710. doi:10.3201/eid2110.141928
4. Qi R, Qin XR, Wang L, et al. Severe fever with thrombocytopenia syndrome can masquerade as hemorrhagic fever with renal syndrome. PLoS Negl Trop Dis. 2019;13(3):e0007308. doi:10.1371/journal.pntd.0007308
5. Chen Y, Jia B, Liu Y, Huang R, Chen J, Wu C. Risk factors associated with fatality of severe fever with thrombocytopenia syndrome: a meta-analysis. Oncotarget. 2017;8(51):89119–89129. doi:10.18632/oncotarget.19163
6. Hu J, Li Z, Hong L, et al. Preliminary fast diagnosis of severe fever with thrombocytopenia syndrome with clinical and epidemiological parameters. PLoS One. 2017;12(7):e0180256. doi:10.1371/journal.pone.0180256
7. Huang D, Jiang Y, Liu X, et al. A cluster of symptomatic and asymptomatic infections of severe fever with thrombocytopenia syndrome caused by person-to-person transmission. Am J Trop Med Hyg. 2017;97(2):396–402. doi:10.4269/ajtmh.17-0059
8. Li D. A highly pathogenic new bunyavirus emerged in China. Em Microbes Infect. 2013;2(1):e1.
9. Ai JW, Li Y, Cheng Q, et al. Diagnosis of local hepatic tuberculosis through next-generation sequencing: smarter, faster and better. Clin Res Hepatol Gastroenterol. 2018;42(3):178–181. doi:10.1016/j.clinre.2018.04.007
10. Miao Q, Ma Y, Wang Q, et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin Infect Dis. 2018;67(suppl_2):S231–s240. doi:10.1093/cid/ciy693
11. Wang S, Chen Y, Wang D, et al. The feasibility of metagenomic next-generation sequencing to identify pathogens causing tuberculous meningitis in cerebrospinal fluid. Front Microbiol. 2019;10:1993. doi:10.3389/fmicb.2019.01993
12. Wu F, Zhao S, Yu B, et al. A new coronavirus associated with human respiratory disease in China. Nature. 2020;579(7798):265–269. doi:10.1038/s41586-020-2008-3
13. Harrison EM, Paterson GK, Holden MT, et al. Whole genome sequencing identifies zoonotic transmission of MRSA isolates with the novel mecA homologue mecC. EMBO Mol Med. 2013;5(4):509–515. doi:10.1002/emmm.201202413
14. Fujikawa K, Koga T, Honda T, et al. Serial analysis of cytokine and chemokine profiles and viral load in severe fever with thrombocytopenia syndrome: case report and review of literature. Medicine. 2019;98(42):e17571. doi:10.1097/MD.0000000000017571
15. Miyamoto S, Ito T, Terada S, et al. Fulminant myocarditis associated with severe fever with thrombocytopenia syndrome: a case report. BMC Infect Dis. 2019;19(1):266. doi:10.1186/s12879-019-3904-8
16. Giordano P, Lassandro G, Barone A, et al. Use of eltrombopag in children with chronic Immune Thrombocytopenia (ITP): a real life retrospective multicenter experience of the Italian association of pediatric hematology and oncology (AIEOP). Front Med. 2020;7:66. doi:10.3389/fmed.2020.00066
17. Wang LY, Cui N, Lu QB, et al. Severe fever with thrombocytopenia syndrome in children: a case report. BMC Infect Dis. 2014;14:366. doi:10.1186/1471-2334-14-366
18. Brown JR, Bharucha T, Breuer J. Encephalitis diagnosis using metagenomics: application of next generation sequencing for undiagnosed cases. J Infect. 2018;76(3):225–240. doi:10.1016/j.jinf.2017.12.014
19. Brooks D, Smith A, Young D, Fulton R, Booth MG. Mortality in intensive care: the impact of bacteremia and the utility of systemic inflammatory response syndrome. Am J Infect Control. 2016;44(11):1291–1295. doi:10.1016/j.ajic.2016.04.214
20. Li H, Gao H, Meng H, et al. Detection of pulmonary infectious pathogens from lung biopsy tissues by metagenomic next-generation sequencing. Front Cell Infect Microbiol. 2018;8:205. doi:10.3389/fcimb.2018.00205
21. Zhou X, Wu H, Ruan Q, et al. Clinical evaluation of diagnosis efficacy of active mycobacterium tuberculosis complex infection via metagenomic next-generation sequencing of direct clinical samples. Front Cell Infect Microbiol. 2019;9:351. doi:10.3389/fcimb.2019.00351
22. Langelier C, Zinter MS, Kalantar K, et al. Metagenomic sequencing detects respiratory pathogens in hematopoietic cellular transplant patients. Am J Respir Crit Care Med. 2018;197(4):524–528. doi:10.1164/rccm.201706-1097LE
23. Chen J, Zhao Y, Shang Y, et al. The clinical significance of simultaneous detection of pathogens from bronchoalveolar lavage fluid and blood samples by metagenomic next-generation sequencing in patients with severe pneumonia. J Med Microbiol. 2021;70(1). doi:10.1099/jmm.0.001259
24. Zhang HC, Ai JW, Cui P, et al. Incremental value of metagenomic next generation sequencing for the diagnosis of suspected focal infection in adults. J Infect. 2019;79(5):419–425. doi:10.1016/j.jinf.2019.08.012
25. Greninger AL, Waghmare A, Adler A, et al. Rule-out outbreak: 24-hour metagenomic next-generation sequencing for characterizing respiratory virus source for infection prevention. J Pediatric Infect Dis Soc. 2017;6(2):168–172. doi:10.1093/jpids/pix019
26. Yachida S, Mizutani S, Shiroma H, et al. Metagenomic and metabolomic analyses reveal distinct stage-specific phenotypes of the gut microbiota in colorectal cancer. Nat Med. 2019;25(6):968–976. doi:10.1038/s41591-019-0458-7
27. Gu W, Miller S, Chiu CY. Clinical metagenomic next-generation sequencing for pathogen detection. Annu Rev Pathol. 2019;14:319–338. doi:10.1146/annurev-pathmechdis-012418-012751
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.