")
Back to Journals » Clinical Epidemiology » Volume 8
The Danish Vascular Registry, Karbase
Authors Eldrup N, Cerqueira C, de la Motte L, Rathenborg LK, Hansen AK
Received 8 January 2016
Accepted for publication 29 February 2016
Published 25 October 2016 Volume 2016:8 Pages 713—718
DOI https://doi.org/10.2147/CLEP.S99506
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Henrik Sørensen
Nikolaj Eldrup,1,2 Charlotte Cerqueira,3 Louise de la Motte,2,4 Lisbet Knudsen Rathenborg,2,4 Allan K Hansen2,5
1Department of Cardiothoracic and Vascular Surgery, Aarhus University Hospital, 2Karbase, The Danish Vascular Registry, Aarhus, 3Registry Support Centre (East) – Epidemiology and Biostatistics, Research Centre for Prevention and Health, Capital Region of Denmark, 4Department of Vascular Surgery, Rigshospitalet, Copenhagen University Hospital, Copenhagen, 5Department of Vascular Surgery, Aalborg University Hospital, Aalborg, Denmark
Aim: The Danish Vascular Registry (DVR), Karbase, is monitoring arterial and advanced vein interventions conducted at all vascular departments in Denmark. The main aim of the DVR is to improve the quality of treatment for patients undergoing vascular surgery in Denmark by using the registry for quality assessment and research.
Study population: All patients undergoing vascular interventions (surgical and endovascular) at any vascular department in Denmark are registered in the DVR. The DVR was initiated in 1989, and each year, ~9,000 procedures are added. By January 2016, .180,000 procedures have been recorded. Since 2001, data completeness has been .90% (compared to the Danish National Patient Register).
Main variables: Variables include information on descriptive patient data (ie, age, sex, height, and weight) and comorbidity (ie, previous cardiovascular disease and diabetes). Process variable includes waiting time (time from event to medical contact and treatment) and the type of procedures conducted. Outcome variables for in-hospital complications (ie, wound complications, myocardial infarction, stroke, amputation, respiratory complications, and renal insufficiency) and 30-day patency are submitted. Variables for medical treatment (antithrombotic and statin treatment), amputation, and survival are extracted from nationwide, administrative registers.
Conclusion: The DVR reports outcome on key indicators for monitoring the quality at all vascular departments in Denmark for the purpose of quality improvement. Furthermore, data are available for research and are being used in international collaborations on changes in clinical practices.
Keywords: vascular surgery, quality of care, clinical registry
Background
The Danish Vascular Registry (DVR), Karbase, was initiated in 1989 for monitoring the results and complications of the vascular surgery, and equally important for creating a nationwide database for research in vascular surgery. Today, 27 years later, the database contains >180,000 procedures (both surgical and endovascular), has nationwide coverage, and is being integrated with other registries to automatically generate predefined outcome data.
Aim of the database
The main aim of the DVR is to improve the quality of procedures and treatment for patients undergoing vascular surgery in Denmark. By describing variation in clinical practice across the country, the aim is to stimulate the quality improvement initiatives, to standardize the excellence in practice, and thus to improve the outcomes. Also, the DVR aims to monitor and support the implementation of evidence-based treatment for patients undergoing vascular procedures, both surgical and endovascular.
Data are collected by the vascular surgeon who is responsible for the treatment. Data are entered to the DVR by the surgeon, but at some departments, paper forms are still completed by the surgeon and then entered to the database by the secretaries.
Study population
The DVR includes data on all reconstructive arterial and advanced vein procedures performed at the seven vascular surgical departments in Denmark. Patient consent is not required for the entry of data in the DVR, because Danish legislation allows data collection for nationwide clinical quality databases. Patients must possess a Danish unique personal identification number (central person registration number [CPR]) that links to health registers as well as to nationwide administrative registers. Each year, ~9,000 procedures are added. The main procedures are ~450 carotid endarterectomies, 500 open repair for aortic aneurysm, 250 endovascular aortic repairs, 1,500 open peripheral arterial reconstructions, 2,500 endovascular arterial interventions for atherosclerosis, and 700 arteriovenous fistulas for renal insufficiency.
Main variables
The main variables recorded in the DVR are patient characteristics (sex, height, weight, age, tobacco use, level of self-care, hemoglobin, creatinine, total cholesterol, and high-density lipoprotein), comorbidity (previous cerebrovascular or cardiac disease, hypertension, diabetes, and pulmonary disease), indication for intervention (claudication, rest pain, wound, necrosis, aneurysm, stroke, bleeding, and infection), the International Classification of Diseases-tenth revision code for the surgical/endovascular procedure performed, and outcome variables on complications (infection, bleeding, thrombosis, nerve lesions, pulmonary complication, myocardial infarction, stroke, renal insufficiency, dialysis, stay at intensive care >3 days, deep venous thrombosis, pulmonary embolism, compartment syndrome in the extremities, and multiorgan failure). Process variables include waiting time from event to examination and intervention, length of hospital stay, and time from preintervention angiography to intervention. Outcome variables include mortality, myocardial infarction, stroke, and amputation rate.
Depending on the disease, information on distal blood pressure, degree of carotid stenosis, or size of arterial aneurysm is recorded. Furthermore, follow-up information on patency is noted for 1 month, 3 months, and 12 months.
Registration in the DVR is mandatory for all procedures performed in public Danish hospitals by vascular surgeons. Data variables have been adjusted to conform to the international Vascunet recommended standard for carotid, aortic, and peripheral arterial diseases1 and for the purpose of processing national quality analysis. Existing data from administrative registers are used, when deemed valid.
The key outcome and performance indicators for monitoring and improving the quality of care are mainly objective endpoints such as mortality, cardiovascular events, amputation, reoperations, infections, medical treatment, waiting time, and length of stay (Table 1). These endpoints are gathered from data entered by the surgeons of events occurring during admission as well as from data extracted from administrative registers after discharge.
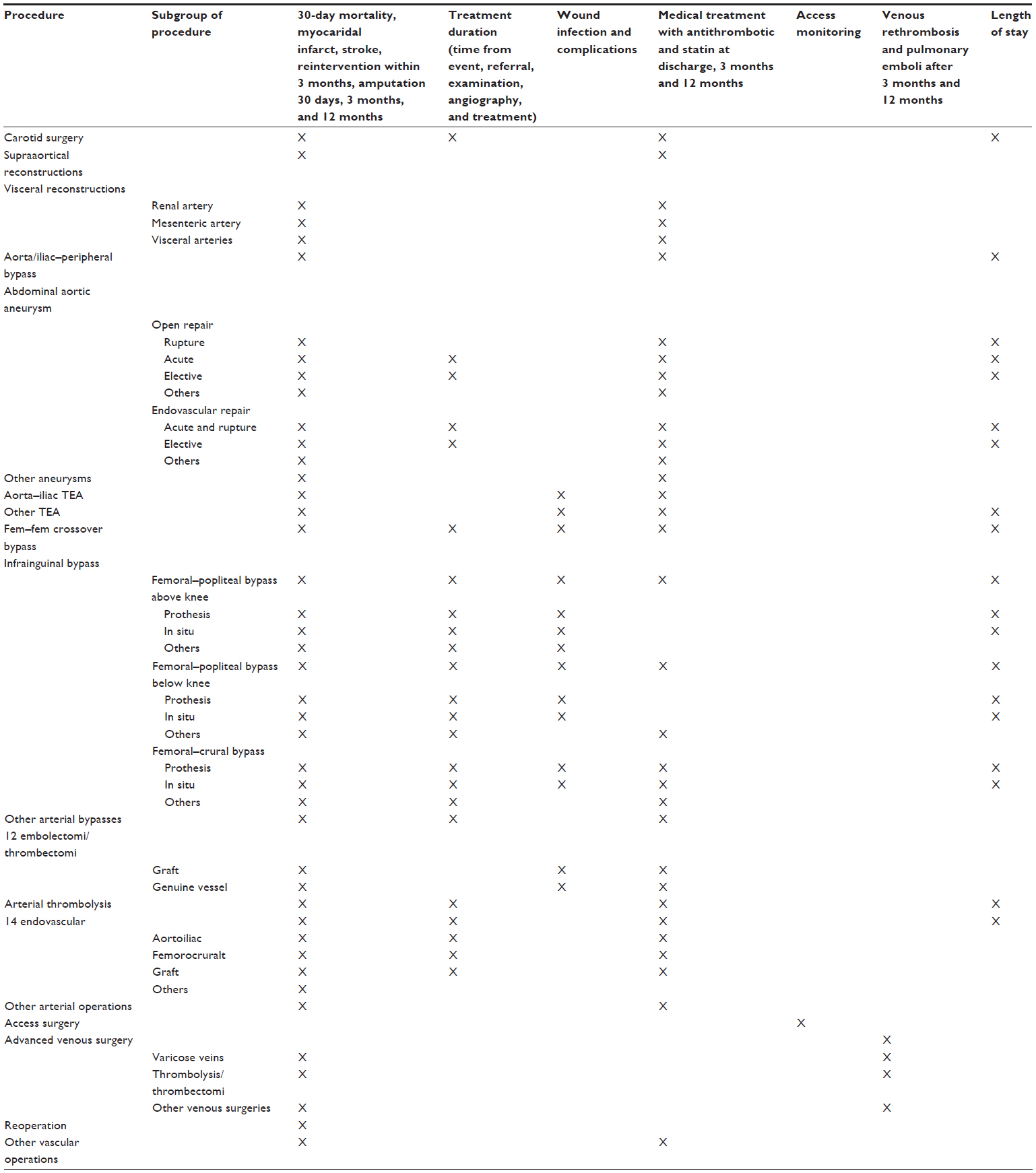 | Table 1 Indicators of Danish Vascular Registry from 2016–2017 |
The coverage of the DVR is routinely evaluated by matching data to the administrative data in the Danish National Patient Register, which has kept record of all hospital contacts in Denmark since 1977. These analyses show a high completeness of data in the DVR with 95% of procedures of carotid surgery, abdominal aortic aneurysms, and lower limb bypass being recorded. Data completeness for all procedures has been >90% in the DVR compared to the Danish National Patient Register since 2001. The coverage of the register is to a large extent due to the continuous effort by the surgical departments, and the time allocated, to review the patient lists for missing or incorrect information.
Follow-up
The DVR reports annually, based on data submitted by the vascular departments in Denmark. Reporting is based on the national and departmental data.
The reported results are discussed at annual meetings with the aim of improvement, rather than criticism. In case of outlier results (positive as well as negative), local audits are performed. The results of the audits are published in the final annual report. Audits are essential to the maintenance of good clinical practice within the field of vascular surgery, where outcomes are dependent on the careful selection of patients, the skills of the surgical, endovascular, and anesthetic teams, and the medical care.
Periodic assessments of the quality indicators are published on a monthly basis in the regional information systems where hospital departments have access to their own results, both to ensure the real-time registration and to show the results for the further development and quality assurance in the units, respectively. These results are of interest to practicing vascular surgeons and a useful guide for health care administrative workers and managers to help allocate maximum value for the limited resources available.
Examples of research
Based on the DVR, several different types of studies have been conducted, for example,
- Impact of β-blockers on patients treated for peripheral arterial disease:2 this study showed a reduced risk of amputation but increased risk of myocardial infarction or stroke.
- Influence of type of anesthesia on the patency of peripheral bypass:3 hypothesizing that epidural anesthesia could positively affect 30-day patency because of an increased regional blood flow; the study showed that the choice of anesthesia does not affect the 7-day patency.
- Benefit of open repair versus endovascular repair for electively asymptomatic abdominal aortic aneurysm repair was investigated during a 4-year period:4 this (national) study showed that the results found in the previous randomized studies of a benefit in 30-day survival with endovascular repair were also seen in daily Danish practice. Furthermore, it showed that after 20 months, there was no difference in survival between the two treatment modalities.
- Cardiovascular risk in patients suffering from aortic aneurysm disease, who had undergone open aortic aneurysm repair compared to the normal Danish population:5 this study found that patients with abdominal aortic aneurysm had a twofold increased risk of myocardial infarction and stroke compared to the general population, emphasizing the need for cardiovascular preventive treatment and lifestyle intervention.
- The DVR has also provided data for the evaluation of national initiatives for quality improvement in decreasing the treatment time after stroke or transient ischemic attack due to carotid stenosis6 in collaboration with the Danish Stroke Registry: the study showed that implementation of national time limits, for time from event to ultrasound examination and surgical treatment, decreased the time from referral to operation by 40%.
Beyond this, the DVR is a major contributor in providing data to research-year and PhD students.
It is of major interest to determine to which extent the differences in health care systems influence clinical practice and results. Therefore, the DVR participates in the international collaboration, Vascunet, which is established to compare the practice between countries for common vascular interventions. The Vascunet collaboration has published comparative data on carotid endarterectomy,7 abdominal aortic aneurysms, lower limb revascularization, and rare conditions where national data are too limited to conduct studies.1 These analyses have revealed slight differences in practices and outcomes between countries and have supported local quality improvement initiatives. The DVR has also entered the International Consortium of Vascular Registries, which aim to collect the international follow-up data on vascular devices in order to improve the safety of patients.
Administrative issues and funding
The first local initiative toward a nationwide vascular database was taken by a group of enthusiastic vascular surgeons in 1989. The DVR was approved by the Danish Health Authority in 1993. The registry is run by a steering committee and representatives from each department of vascular surgery.
Each year, the steering committee and the local representatives meet to discuss the recent annual report and decide which departments will need to do an audit due to performance outside the expected limits (good or bad). Audits are followed up at the DVR annual meeting and published in a final version of the annual report, including plans for either optimizing treatment at other departments or optimizing treatment locally.
The steering committee meets four to six times a year to plan the development of the database content and the quality indicators.
The DVR is a part of the Danish Clinical Registries (RKKP), which is funded by the Danish Regions.
Access to data can be obtained by applying to the Danish Clinical Registries, after obtaining the necessary official approval from the Danish Data Protection Agency as well as from the (local) ethical committee.
Conclusion
The DVR (Karbase) is monitoring all arterial and advanced vein interventions for quality improvement as well as for research and contains information about baseline characteristics, comorbidity, procedures conducted, complications, and medical treatment status.
Acknowledgments
The existence of the DVR (Karbase) is only possible due to the continued contributions in the collection of data from the staff of the hospital departments caring for patients undergoing vascular surgery. The publication costs for this article were funded by the Program for Clinical Research Infrastructure (PROCRIN) established by the Lundbeck Foundation and the Novo Nordisk Foundation and administered by the Danish Regions.
Disclosure
The authors report no conflicts of interest in this work.
References
Lees T, Troëng T, Thomson IA, et al. International variations in infrainguinal bypass surgery – a VASCUNET report. Eur J Vasc Endovas Surg. 2012;44(2):185–192. | |
Hogh A, Lindholt JS, Nielsen H, Jensen LP, Johnsen SP. Beta-blocker use and clinical outcomes after primary vascular surgery: a nationwide propensity score-matched study. Eur J Vasc Endovasc Surg. 2013; 46(1):93–102. | |
Wiis JT, Jensen-Gadegaard P, Altintas U, Seidelin C, Martusevicius R, Mantoni T. One-week postoperative patency of lower extremity in situ bypass graft comparing epidural and general anesthesia: retrospective study of 822 patients. Ann Vasc Surg. 2014;28(2):295–300. | |
de la Motte L, Jensen LP, Vogt K, Kehlet H, Schroeder TV, Lonn L. Outcomes after elective aortic aneurysm repair: a nationwide Danish cohort study 2007–2010. Eur J Vasc Endovasc Surg. 2013;46(1):57–64. | |
Eldrup N, Budtz-Lilly J, Laustsen J, Bibby BM, Paaske WP. Long-term incidence of myocardial infarct, stroke, and mortality in patients operated on for abdominal aortic aneurysms. J Vasc Surg. 2012;55(2):311–317. | |
Witt AH, Johnsen SP, Jensen LP, Hansen AK, Hundborg HH, Andersen G. Reducing delay of carotid endarterectomy in acute uschemic stroke patients: a nationwide initiative. Stroke. 2013;44(3):686–690. | |
Vikatmaa P, Mitchell D, Jensen LP, et al. Variation in clinical practice in carotid surgery in nine countries 2005–2010. Lessons from VASCUNET and recommendations for the future of national clinical audit. Eur J Vasc Endovasc Surg. 2012;44(1):11–17. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.