")
Back to Journals » Clinical Epidemiology » Volume 8
The Danish Testicular Cancer database
Authors Daugaard G, Kier MGG, Bandak M, Mortensen MS, Larsson H, Søgaard M, Toft BG, Engvad B, Agerbæk M, Holm NV, Lauritsen J
Received 16 December 2015
Accepted for publication 8 January 2016
Published 25 October 2016 Volume 2016:8 Pages 703—707
DOI https://doi.org/10.2147/CLEP.S99493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Henrik Sørensen
Gedske Daugaard,1 Maria Gry Gundgaard Kier,1 Mikkel Bandak,1 Mette Saksø Mortensen,1 Heidi Larsson,2 Mette Søgaard,2 Birgitte Groenkaer Toft,3 Birte Engvad,4 Mads Agerbæk,5 Niels Vilstrup Holm,6 Jakob Lauritsen1
1Department of Oncology 5073, Copenhagen University Hospital, Rigshospitalet, Copenhagen, 2Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, 3Department of Pathology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, 4Department of Pathology, Odense University Hospital, Odense, 5Department of Oncology, Aarhus University Hospital, Aarhus, 6Department of Oncology, Odense University Hospital, Odense, Denmark
Aim: The nationwide Danish Testicular Cancer database consists of a retrospective research database (DaTeCa database) and a prospective clinical database (Danish Multidisciplinary Cancer Group [DMCG] DaTeCa database). The aim is to improve the quality of care for patients with testicular cancer (TC) in Denmark, that is, by identifying risk factors for relapse, toxicity related to treatment, and focusing on late effects.
Study population: All Danish male patients with a histologically verified germ cell cancer diagnosis in the Danish Pathology Registry are included in the DaTeCa databases. Data collection has been performed from 1984 to 2007 and from 2013 onward, respectively.
Main variables and descriptive data: The retrospective DaTeCa database contains detailed information with more than 300 variables related to histology, stage, treatment, relapses, pathology, tumor markers, kidney function, lung function, etc. A questionnaire related to late effects has been conducted, which includes questions regarding social relationships, life situation, general health status, family background, diseases, symptoms, use of medication, marital status, psychosocial issues, fertility, and sexuality. TC survivors alive on October 2014 were invited to fill in this questionnaire including 160 validated questions. Collection of questionnaires is still ongoing. A biobank including blood/sputum samples for future genetic analyses has been established. Both samples related to DaTeCa and DMCG DaTeCa database are included. The prospective DMCG DaTeCa database includes variables regarding histology, stage, prognostic group, and treatment.
Conclusion: The DMCG DaTeCa database has existed since 2013 and is a young clinical database. It is necessary to extend the data collection in the prospective database in order to answer quality-related questions. Data from the retrospective database will be added to the prospective data. This will result in a large and very comprehensive database for future studies on TC patients.
Keywords: testis cancer, clinical indicators, database research, DaTeCa, DMCG DaTeCa database, hypogonadism
Aim of database
Testicular cancer (TC) is a rare disease, with ~300 cases per year in Denmark. Nonetheless, TC is the most common cancer in men aged 20–40 years. Today, it represents the most curable solid tumor with a 10-year survival of 90%–95%.1
With the high cure rate and young age at diagnosis, posttreatment morbidity plays a central role. Previous studies have shown an increased risk of secondary cancers, and conditions including heart disease, diabetes, hypogonadism, decreased fertility, and psychosocial problems.2 Data regarding risk factors for long-term side effects of treatment are modest, and the precise risk of the various late side effects remains unresolved.
In Denmark, treatment of TC after orchiectomy has been increasingly centralized over the years, and is now performed only at three university hospitals. A common treatment and follow-up strategy has been developed across these centers (Table 1). National guidelines for treatment have been set by a multidisciplinary group. This group consists of representatives from all attending departments and from specialties relevant in the treatment of TC (www.ducg.dk). We have a large retrospective and a smaller prospective database, which will be merged in the coming years.
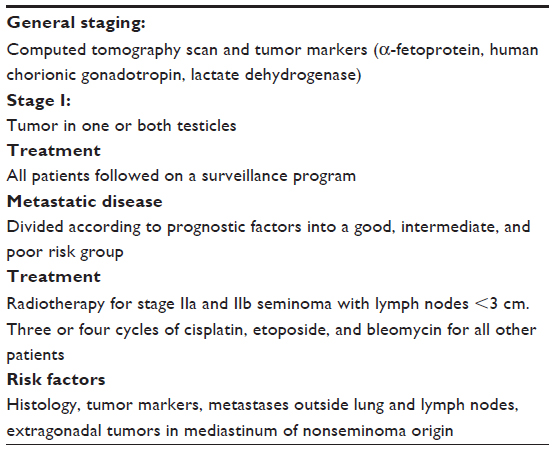 | Table 1 Testicular cancer – diagnosis and treatment |
The overall aim of both databases is to improve the quality of care for patients with TC in Denmark. Several important issues related to treatment and survivorship of TC patients such as prognostic factors for relapse, treatment, follow-up, and late effects may be described through analyses of data from the clinical databases. So far, the focus has been on the following areas:
- Analyses of quality indicators, benchmarking, quality audit, and feedback to departments.
- Prognostic factors for relapse in stage I seminoma and nonseminoma patients.3,4
- Rational follow-up of stage I patients in a surveillance program.3,4
- Screening for contralateral carcinoma in situ testis.5
- National treatment results for patients with metastatic disease including reanalysis of international risk factors published in 1997.6
- Patients treated with more than one line of therapy for disseminated disease.7
- Second primary cancer and cause of death.
- Long-term morbidity in the form of cardiovascular disease, metabolic syndrome, neurotoxicity, nephrotoxicity, pulmonary toxicity, hypogonadism, decreased fertility, and psychosocial problems.8,9
Study population
There are two TC databases in Denmark. Initially, the retrospective Danish Testicular Cancer (DaTeCa) database was constructed (Danish data protection agency J.nr. 2012-41-0751). This is a research database comprising ~6,000 Danish male patients with TC diagnosed from January 1, 1984 to December 31, 2007. Subsequently, the prospective Danish Multidisciplinary Cancer Group (DMCG) DaTeCa database was initiated in 2013 with prospective data collection of key clinical variables. The databases include cancers of both gonadal and extragonadal origin.
Patients in the retrospective DaTeCa database have been identified through the Danish National Patient Registry10 and hospital files. The diagnoses have been confirmed through manual review of pathology reports. The prospective DMCG DaTeCa database includes all incident TCs of both gonadal and extragonadal origin in Denmark recorded in the Danish National Patient Registry and/or the Danish Pathology Registry11 from 2013 onward. At present, ~650 patients have been included in the database, with 300 new cases added every year. Up to now, the main focus has been on optimizing the validity of the algorithm for patient identification in the central registries, and validation of pathology data from three larger hospitals diagnosing and treating patients have revealed 100% coverage of histologically verified cancers. Further validation will ensure an even higher validity and completeness of data in the future.
Main variables
The retrospective DaTeCa database contains detailed information with more than 300 variables related to histology, stage, treatment, relapses, pathology, tumor markers, kidney function, lung function, etc. Information about cause of death has been obtained from the Danish Registry of Causes of Death and cross-checked against journal files. Through linkage with national central registries, medical history after 5 years of standard follow-up program has been obtained, including vital status. A questionnaire related to late effects has been prepared, which includes issues on social relationships, life situation, general health status, family background, diseases, symptoms, use of medication, marital status, psychosocial issues, fertility, and sexuality. Patients have been asked to fill this questionnaire, and to deliver relevant blood/sputum tests to a biobank for future genetic analyses. These data will be included in the retrospective database. In the longer term, the same data will be collected in the prospective database.
The prospective DMCG DaTeCa database includes variables regarding histology, stage, prognostic group, and treatment. These variables are obtained by data linkage to the Danish Pathology Registry (eg, histology and stage), the Danish National Patient Register (eg, medical history, surgical procedures, chemotherapy, and radiation therapy), and the Civil Registration System (data on vital status and migration). Additional key clinical variables are registered online in a web-based form by the treating clinicians at the oncological departments. These online registration forms are partly uniform for the five uro-oncological databases in Denmark. In 2013 and 2014, ~98% of all newly diagnosed patients identified in the central registries have had an online registration form filled in.
Seven clinical quality indicators (four result indicators and three process indicators) are derived from the prospective database in order to monitor and improve the quality of care for patients with TC. These quality indicators include both indicators describing remission after treatment (indicator 1a–c), surgery (indicator 2), occurrence of relapse (indicator 3a–b, 4), prognosis, and the completeness of the pathological coding (indicator 5–7) (Table 2).
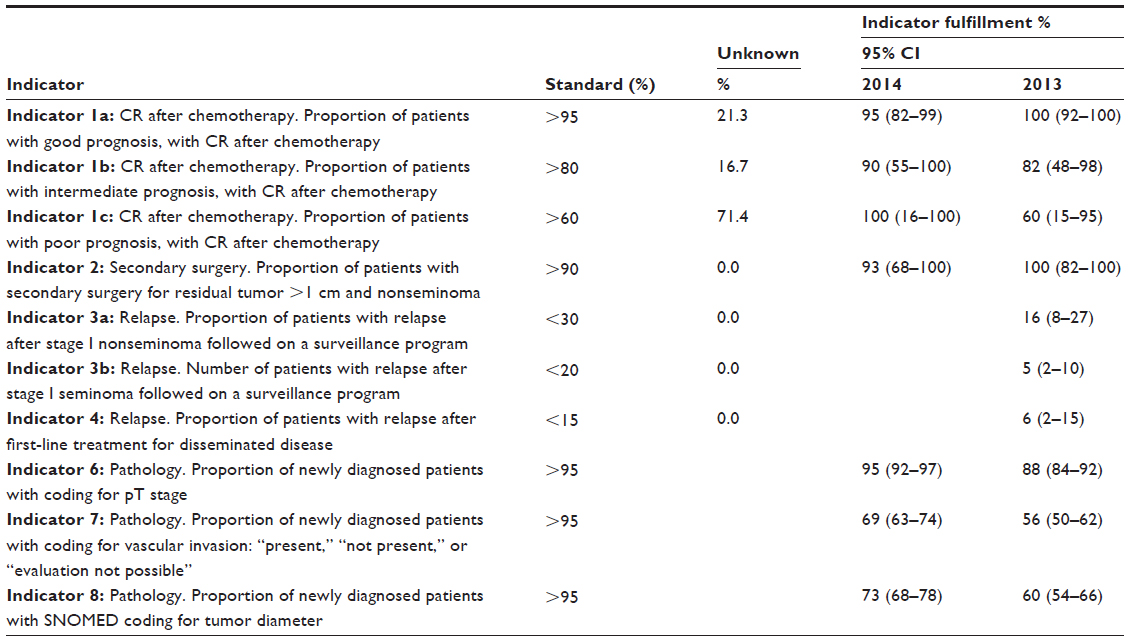 | Table 2 Clinical quality indicators in the prospective DaTeCa database and indicator fulfillment in 2013 and 2014 |
The relevant pathological codes used to identify prognosis and risk of relapse are important, and from 2013 to 2014, a significant improvement of coding practice was observed.12 With continuous attention, also regarding coding of other clinical and paraclinical parameters, we found it possible to meet the expected quality standards.
Follow-up
Patients are followed by uniform national follow-up schedules, usually for 5 years. After that, survival and possible relapse can be followed in national registries.
Examples of research
Patients with stage I TCs are followed for 5 years in a surveillance program. It is demanded that follow-up programs are effective and relevant for the survival of the patient. We have used the retrospective database to obtain detailed information about relapses including risk factors for relapse both in seminoma and nonseminoma patients.3,4 Furthermore, we have been able to suggest a timetable for follow-up.
The relapse rate after orchiectomy in stage I nonseminoma was 30.6% after 5 years. Presence of vascular invasion together with embryonal carcinoma and rete testis invasion in the testicular primary identified a group of patients with a relapse risk of 50%. Without risk factors, the relapse risk was 12%. With a median follow-up of 15 years in the seminoma group, we found the relapse risk was 18.9%. Tumor size was an important risk factor for relapse. Either vascular invasion or invasion of epididymis was significant, if the other factor was excluded from analysis. For a patient with seminoma, and characterized by a tumor diameter of 8 cm and vascular invasion, the 5-year risk of recurrence was 40%.
Preventive treatment of recurrences of high-risk stage I patients with chemotherapy or radiation therapy is practiced at many centers worldwide. Based on our data, the risk factors underlying the selection of patients for treatment is incorrect. The newly defined risk factors identified through use of the DaTeCa database needs to be confirmed prospectively before deciding on adjuvant treatment in high-risk patients. As Denmark is one of the few countries worldwide in which all stage I patients are followed with surveillance, the confirmation of risk factors will be performed on patients in the prospective DMCG DaTeCa database. Data completeness concerning histology in the prospective DMCG database is expected to be better compared with the retrospective database, and we aim to validate the risk factors mentioned above and possibly identify additional factors.
In 2015, the first annual report from the prospective DMCG DaTeCa database was published online at www.Sundhed.dk. The report contained detailed analyses on indicator fulfillment in 2013 and 2014 at the hospital level, regional level, and national level.
Administrative issues and funding
The retrospective DaTeCa database was created as a research database and analyses from this database have received support from various funding and already created several publications.3–5,7–9
The prospective DMCG DaTeCa database is under the auspices of the Danish Multidisciplinary Cancer Groups (DMCG.dk), which is an umbrella organization comprising 24 national cancer groups and clinical databases in Denmark.13 The urological cancer groups and databases are further organized under the subgroup for Danish Urological Cancer Groups.14
The prospective DMCG DaTeCa database is publicly funded by the Danish Regions15 and under the administration of the Danish Clinical Registries (RKKP).16 Technical support and data management is provided by the Registry Support Centres of Clinical Quality and Health Informatics (West) (KCKS-Vest)17 and epidemiological and statistical support to the annual reports is provided by the Registry Support Centre of Epidemiology and Biostatistics (North) (KCEB-Nord).18 The Danish Clinical Registries (RKKP) is a nationwide initiative for monitoring and improving the quality of clinical care in Denmark.
Conclusion
The retrospective DaTeCa database is the most detailed database concerning TC worldwide. The strength of the database is the complete and detailed information relating to treatment and that the treatment is consistent with today’s international standards, both in terms of stage I disease and chemotherapy for metastatic disease. We have focused on patients treated between 1984 and 2007 to ensure at least 5-year follow-up of all patients. It is the intention to use the prospective DMCG DaTeCa database to validate findings in the retrospective database and to expand the database to include a larger amount of data from public registries. The quality indicators will be used to improve quality of treatment. It is a challenge to identify and ensure the use of correct diagnosis codes so that all relevant patients are included in the database. Furthermore, data from the retrospective database will be added to the prospective data. This will result in a large and comprehensive database for future studies on TC patients. In the long term, the main variables in the prospective database should be expanded to cover results from relevant laboratory analyses, and results from specialized tests, that is, single nucleotide polymorphism analysis.
Data regarding the factors leading to long-term side effects of treatment are scarce. The introduction of new molecular testing methods allows us to use these tools to identify patients at high risk for therapy-related complications and thus the opportunity to develop risk-adapted screening and intervention strategies. The available database along with the biobank is optimal for this purpose.
Acknowledgments
This paper was funded by the Program for Clinical Research Infrastructure established by the Lundbeck Foundation and the Novo Nordisk Foundation and administered by the Danish Regions.
Disclosure
The authors report no conflicts of interest in this work.
References
Verdecchia A, Francisci S, Brenner H, et al. Recent cancer survival in Europe: a 2000–2002 period analysis of EUROCARE-4 data. Lancet Oncol. 2007;8:784–796. | |
Travis LB, Beard C, Allan JM, et al. Testicular cancer survivorship: research strategies and recommendations. J Natl Cancer Inst. 2010; 102:1114–1130. | |
Mortensen MS, Lauritsen J, Gundgaard MG, et al. A nationwide cohort study of stage I seminoma patients followed on a surveillance program. Eur Urol. 2014;66(6):1172–1178. | |
Daugaard G, Gundgaard MG, Mortensen MS, et al. Surveillance for stage I non-seminomatous testicular cancer – outcomes and long-term follow-up in a population based cohort. J Clin Oncol. 2014;32(34):3817–3823. | |
Kier MG, Lauritsen J, Almstrup K, et al. Screening for contralateral carcinoma in situ testis in patients with testicular cancer: a population based study. DaTeCa 03 study. Ann Oncol. 2015;26(4):737–742. | |
International Germ Cell Cancer Collaborative Group: International Germ Cell Consensus Classification: a prognostic factor-based staging system for metastatic germ cell cancer. J Clin Oncol. 1997;15:594–596. | |
Lauritsen J, Kier MGG, Mortensen MS, et al. Germ cell cancer and multiple relapses – toxicity and survival. J Clin Oncol. 33:3116–3123. | |
Bandak M, Aksglaede L, Juul A, Rørth M, Daugaard G. The pituitary-Leydig cell axis before and after orchiectomy in patients with stage I testicular cancer. Eur J Cancer. 2011;47(17):2585–2591. | |
Lauritsen J, Mortensen MS, Kier MG, et al. Renal impairment and late toxicity in germ-cell cancer survivors. Ann Oncol. 2015; 26(1):173–178. | |
Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. | |
Bjerregaard B, Larsen OB. The Danish Pathology Register. Scand J Public Health. 2011;39(7 Suppl):72–74. | |
Kliniske databaser [homepage on the Internet]. Sundhed.dk [updated 2014 Dec 31]. Available from: https://www.sundhed.dk/content/cms/86/15686_dateca-%C3%A5rsrapport_2014_kommenteret_ 20150328.pdf. Accessed February 15, 2016. | |
Danish Multidisciplinary Cancer Groups (DMCG.dk). Available from: http://dmcg.dk/. Accessed August 1, 2015. | |
Danish Urological Cancer Groups (DUCG). Available from: http:// ducg.dk/. Accessed August 1, 2015. | |
Danish Regions. Available from: http://www.regioner.dk/. Accessed August 1, 2015. | |
Danish Quality Improvement Program (RKKP). Available from: http://www.rkkp.dk/. Accessed August 1, 2015. | |
Competence Centre for Health Quality and Informatics (KSKS-Vest). Available from: http://www.kcks-vest.dk/kliniske-kvalitetsdatabaser/. Accessed August 1, 2015. | |
Competence Centre for Clinical Epidemiology and Biostatistics, North (KCEB-Nord). Available from: http://www.kea.au.dk/en/ClinicalQuality/CentreClinEpiBiostatNorth.html. Accessed August 1, 2015. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.