")
Back to Journals » Clinical Epidemiology » Volume 13
The Danish Diabetes Musculoskeletal Cohort: Non-Responder Analysis of an Electronic Survey Using Registry Data
Authors Boyle E , Folkestad L, Frafjord E, Koes BW, Skou ST , Hartvigsen J
Received 20 November 2020
Accepted for publication 29 April 2021
Published 31 May 2021 Volume 2021:13 Pages 397—405
DOI https://doi.org/10.2147/CLEP.S293186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 8
Editor who approved publication: Professor Vera Ehrenstein
Eleanor Boyle,1 Lars Folkestad,2– 5 Erik Frafjord,6 Bart W Koes,1,7 Soren Thorgaard Skou,1,8 Jan Hartvigsen1,6
1Center for Muscle and Joint Health, Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, Denmark; 2Department of Endocrinology and Metabolism, Odense University Hospital, Odense, Denmark; 3Department of Internal Medicine, Hospital of South West Denmark, Esbjerg, Denmark; 4Department of Clinical Research, University of Southern Denmark, Odense, Denmark; 5Open Patient Exploratory Network, University of Southern Denmark, Odense, Denmark; 6Chiropractic Knowledge Hub, Odense, Denmark; 7Department of General Practice, Erasmus MC, Rotterdam, the Netherlands; 8The Research Unit PROgrez, Department of Physiotherapy and Occupational Therapy, Næstved-Slagelse-Ringsted Hospitals, Slagelse, Denmark
Correspondence: Jan Hartvigsen
Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, Campusvej 55, Odense M, Odense, 5230, Denmark
Tel +45 65504522
Email [email protected]
Purpose: To conduct a non-responder analysis on a musculoskeletal (MSK) electronic questionnaire.
Methods: Individuals aged 18 years and older, diagnosed with diabetes mellitus (DM), and attended an ambulatory DM clinic formed the sample frame. They were invited to complete an electronic musculoskeletal (MSK) conditions and symptoms questionnaire booklet using a secured electronic email system. Individuals whose secured email box was not active at the time were discarded. Using the Central Person Registry number, a unique number assigned to all Danish residents, we linked the sample frame to different registries to learn more about non-responders. Non-responders were either individuals who did not respond to a single question and those who responded “No” to the first question about willing to participate. We calculated descriptive statistics for each characteristic. Univariate logistic regression models were conducted to determine the relationship between each characteristic and non-responder status.
Results: The response rate was 36% (n = 3812). Individuals with type 2 DM (OR 2.0 (95% CI 1.8– 2.2)), secondary DM (1.9 (1.3– 2.8)) or unspecified DM (2.1 (1.8– 2.4)) were more likely to be non-responders than individuals with Type 1 DM. Also, individuals aged 70– 79 (1.3 (1.1– 1.6)) and 80 years and older (5.9 (4.5– 7.7)) were more likely to be non-responders than 18– 29 years old individuals. However, individuals aged 40– 49 (1.5 (1.2– 1.8)), 50– 59 (1.5 (1.3– 1.8)) or 60– 69 (1.4 (1.1– 1.6)) were more likely to be responders than 18– 29 years old individuals. Individuals with Charlson Comorbidity Index (CCI) of 1 (2.0 (1.3.2.9) or CCI of 2 (1.7 (1.1– 2.5) were more likely to be responders than individuals with a CCI of 0. Lastly, individuals who were currently outside of the workforce (1.6 (2.4– 2.9) or had unknown/missing socioeconomic status (3.9 (2.8– 5.3) were more likely to be non-responders than individuals who were working.
Conclusion: Although we did find a non-response bias, this cohort will be an important source to determine the prevalence and consequences of MSK conditions in a secondary care DM population.
Keywords: diabetes, survey, non-participation analysis, musculoskeletal conditions
Introduction
Observational cohort studies can describe the prevalence and the incidence of diseases in whole or subgroups of populations. Additionally, they can identify factors that affect prognosis and identify potential targets for prevention and treatment. Because observational cohort studies are subject to biases that may affect the results of studies, it is recommended by the “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) statement that these potential sources of bias are examined.1
When administering targeted questionnaires to individuals enrolled in a clinical database, a leading source of bias is selection bias, also known as participation or non-responder bias. Rarely does everyone enrolled in a clinical database participate in additional data collection procedures. Ideally, researchers have enough information on the non-responders to determine if they differ systematically from the responders. However, it can be challenging to obtain information beyond age, sex, and where the non-responders live. In Denmark, all residents have a unique 10-digit identifying number, the Central Persons Registration Number (CPR). This number is linkable to all information in governmental databases and registries.2 Therefore, it is possible to learn more details on the non-responders.
Generally, individuals who have diabetes mellitus (DM) have a higher prevalence of musculoskeletal (MSK) pain than individuals who do not have DM. For example, individuals with type 2 diabetes mellitus (T2DM) who were referred to a DM self-management education program reported MSK pain 1.7 (for shoulder/neck), 2.0 (for low back pain), and 2.1 (for arm, hand, knee or hip) times more frequently than their age- and sex-matched general population controls.3 But the association between DM and MSK pain is inconsistent across MSK pain sites. Carvalho-E-Silva et al found the association between DM and back pain was non-significant after adjusting for MSK risk factors, but remained for hip and neck/shoulder pain.4
The degree to which MSK pain interferes with the daily life of an individual who has DM differs across MSK pain sites. A higher proportion of individuals with both back pain and T2DM reported poorer general health, poor well-being, experienced restrictions in their usual activities, reported a sedentary lifestyle and had difficulties moving around when compared to age- and sex-matched general population controls.3 In individuals who had either neck or shoulder pain and T2DM, a higher proportion had poorer general health, had problems going up and down a flight of stairs, experienced restrictions in their usual activities (for women only), and were unable to walk 400 meters (for men only). Furthermore, walking disability from osteoarthritis might be an independent risk factor for diabetes complications. Therefore, research into obstacles for physical activity such as MSK pain is highly relevant. 5
Diagnostic codes are not submitted to the Danish National Health Service Registry, a health care administrative database used in primary care.6 Therefore, to determine the prevalence of MSK conditions and their impact on the individuals with DM, we decided to create an electronic questionnaire booklet (see Appendix 1) to collect this additional information. The booklet contained the following questionnaires: the Nordic Musculoskeletal Questionnaire, the quality-of-life and the osteoarthritis subscales of both the hip and knee disability and osteoarthritis outcomes, the 36-item short-form health survey and the Major Depressive Inventory.
This study’s objective was to conduct a non-responder analysis to determine if those who responded to the electronic questionnaire booklet differed from those who did not.
Methods
Design and Sample Frame
We conducted a census of patients registered in the Department of Endocrinology clinical databases from either the Odense University Hospital (OUH) or the Hospital South West Jutland (SVS). Generally, patients in the clinical databases are seen by a physician at least once a year.
According to current national guidelines, adult patients with type 1 diabetes mellitus (T1DM) are followed routinely via specialized diabetes ambulatory clinics for yearly consultations. Patients with T2DM are routinely followed via their family physician; however, if they develop complications to their treatment or diabetes, they are referred to the same specialized diabetes clinics that the patients with T1DM attend. Thus, the distribution of diabetes subtypes in secondary care does not follow the same distribution found in the general Danish population.
The Danish Board of Health and the Danish Patient Safety Authority approved access to the two clinical databases (file number 3–30132031/1). Patients aged 18 years and older who attended at least one of the clinics were included in the sample frame. The CPR number from the clinical databases was included in the sample frame. All participants provided informed consent to participate in the study. The study was conducted according to the Declaration of Helsinki.
Testing of the Electronic Questionnaire Booklet
The questionnaire booklet’s content validity was assessed by an endocrinologist and two nurses from the Department of Endocrinology at OUH. They were asked if the questions were suitable for the population and if any essential concepts were missing from the booklet’s inventory of questions. Ten patients attending the DM outpatient clinic at OUH and nine laypersons without DM were then asked to read over the questionnaire booklet and indicate anything unclear. Minor adjustments to layout and wording were performed.
Subsequently, the electronic questionnaire booklet was pilot tested. All patients who attended the DM outpatient clinic at OUH in August and September 2017 were given an information letter describing the study’s purpose and invited to participate in the project’s pilot testing via a link in the letter. One hundred and thirty-five patients received the information letter, and 73 (54%) completed the questionnaire booklet. No one indicated any errors, misunderstandings or problems accessing the electronic questionnaire booklet. Consequently, no changes were made to the electronic questionnaire booklet. (Appendix 1).
Administration of the Electronic Questionnaire Booklet
We contracted the Open Patient Data Explorative Network (OPEN) to electronically send the invitation letter and individualized link to the electronic questionnaire booklet to everyone in the sample frame using the e-Boks system via their CPR number. E-Boks is a mandatory method used by Danish public authorities in their communication to Danish residents. It was established in 2014 and is used by 91.7% of Danish residents for their secured digital mail. Individuals who did not have an active e-Boks account at the time of the first mailing were removed from the sample frame. Reminder letters were delivered to their e-Boks’ inbox at four weeks and at eight weeks after the first invitation.
The clinical staff (clinicians and administrative personnel) were informed about this study. If they received any questions or concerns about the study, they were asked to tell the individual to contact the responsible clinician (LF) or the student (AFS). These two individuals, along with one of the researchers (JH), signed the invitation letter.
Data Linkages
The sample frame was uploaded to Statistics Denmark’s Division of Research server (File number 707678), who then linked the records to the following registries: the Danish National Patient Register (DNPR), the National Prescription Register and the Employment Classification Module from Statistics Denmark. After uploading the completed electronic questionnaire booklets to the same server, all CPR numbers in the extract databases were scrambled by Statistics Denmark and renamed PNR. Only after pseudo-anonymization was completed did we receive access to our data.
Variables Used in the Analysis
Responder
Individuals who answered in the affirmative to the first question (about willingness to participate in the study) of the electronic questionnaire booklet by December 31, 2018, were classified as responders. Those who responded later, did not respond at all or responded in the negative to the first question of the electronic questionnaire booklet were classified as non-responders.
Age and Sex
The first six digits of a CPR number is an individual’s birthday. If the last digit in the 10-digit number is even, the individual is female. Statistics Denmark generated the age and sex of everyone in the sample frame before scrambling the CPR number.
Type of DM
The DNPR contains a record of all hospital, emergency room and ambulatory secondary care clinic encounters. Using the last discharge diagnosis recorded in the DNPR, we determined the type of DM using the following algorithm: E10.XX for type 1 diabetes mellitus (T1DM), E.11.XX for T2DM, E13.XX for secondary DM, and E14.XX for unspecified DM. The quality of the DNPR is high, the level of incorrect discharge diagnosis is below 3%.7
Charlson Comorbidity Index (CCI)
The CCI was created using the diagnoses registered in the DNPR from 1995 to 2017 using the same method described by Christensen et al8. The individuals’ CCI was categorized into four groups (CCI score of 0, 1, 2 or ≥3), where higher CCI scores indicated more severe burden of comorbidity.
Socioeconomic Status (SES)
Socioeconomic status was determined using the SOCIO13 variable that is assigned to all Danish residents each year by Statistics Denmark.9 The classification is based on a Danish resident’s main source of income or employment status during the past year. Individuals were categorized into the following socioeconomic categories using their 2018 (or 2017 if missing) status: working (ie, employed full-time, employed part-time, self-employed or student), outside of workforce (ie, unemployed, long-term sick-leave, leave of absence, social assistance, disability pension or retired) or unknown or missing.
Statistical Analysis
Simple descriptive statistics were calculated for the sample frame, for the responders and the non-responders. Odds ratios with 95% confidence intervals were computed for each characteristic to determine if there was a relationship between the characteristic and non-responder status. All statistical analyses were performed using Stata Statistical Software, Release 16.1 (25).
Results
Of the 10,615 individuals registered in the two clinical databases, 33 were excluded because they were <18 years of age (Figure 1). The sample frame contained CPR numbers of 10,582 individuals with active e-Boks accounts. Out of these, 3812 (36%) agreed to participate in the study and were defined as responders. The remaining 6770 (64%) individuals were defined as non-responders.
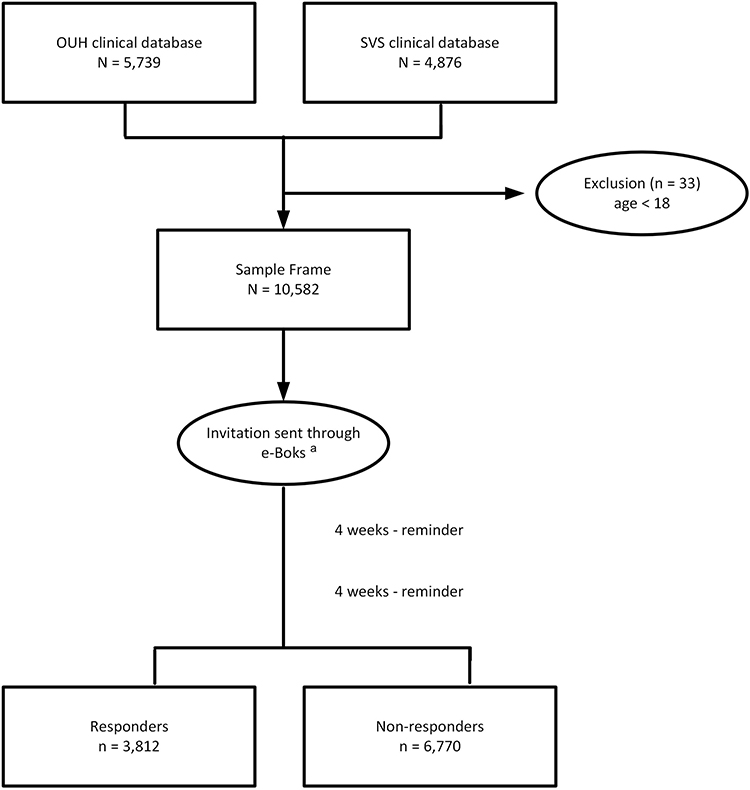 |
Figure 1 Study Flow Diagram. Abbreviations: OUH, Odense University Hospital; SVS, Hospital South West Jutland. Note: ae-Boks is a secure digital mail system that is used by the public authorities in Denmark. |
The sample frame’s mean age was 59.7 years, and 59.3% were males (Table 1). The majority were diagnosed with T2DM, and the majority had three or more comorbidities.
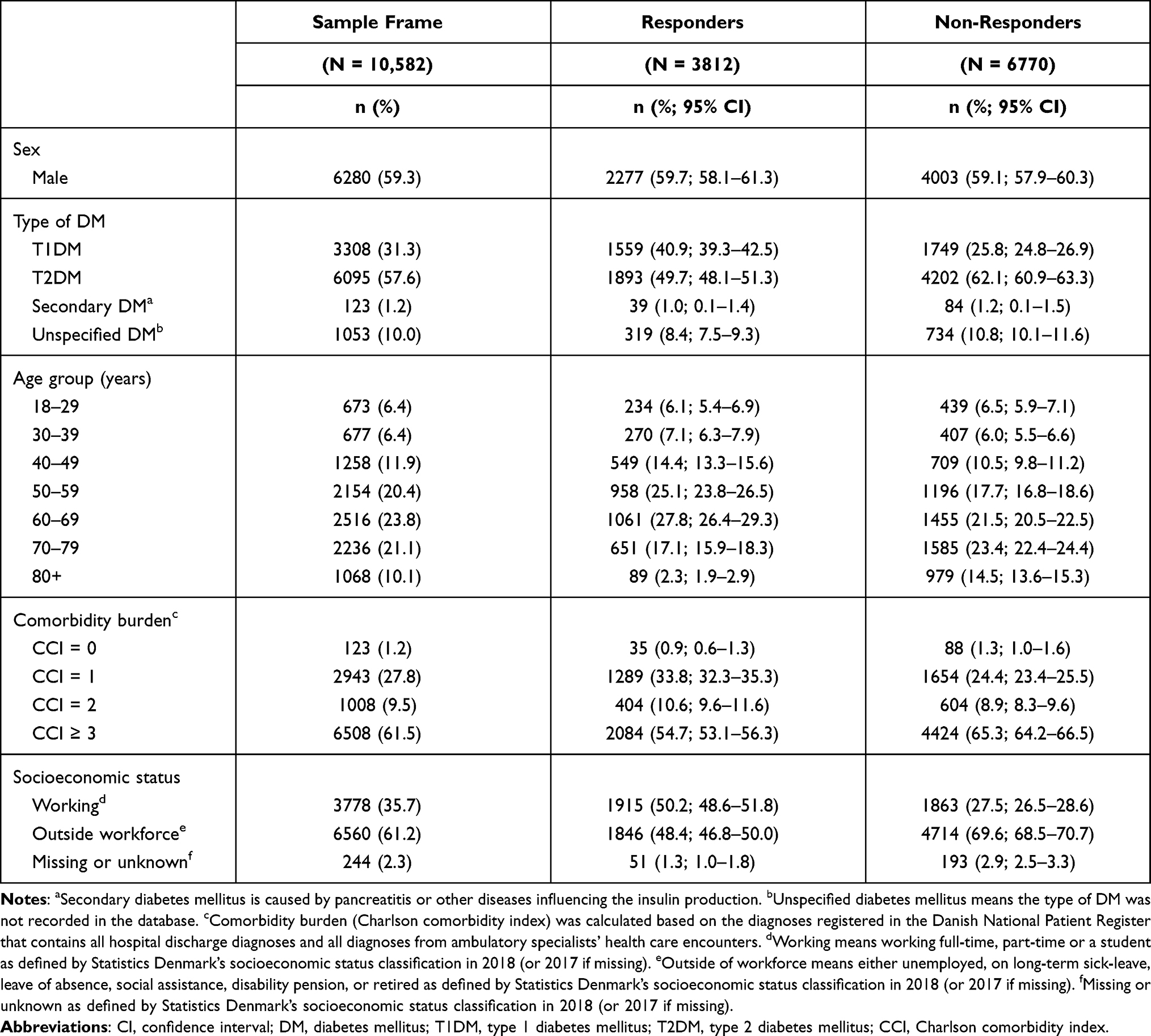 |
Table 1 Description of the Sample Frame, the Responders and the Non-Responders |
The non-responders were more likely to be classified as either having T2DM, secondary DM or unspecified DM than having T1DM (Figure 2). Additionally, the non-responders were more likely to be aged 70 years and older; however, the responders were more likely to be between age 40 and 69 years than being 18 to 29 years old. The responders were more likely to have one or two comorbidities than none; however, there was no difference in the response rate for individuals with three or more comorbidities although the confidence interval was wide indicating lack of precision of this estimate. Lastly, individuals outside of the workforce or had unknown or missing SES were more likely to not have responded to the electronic questionnaire booklet than individuals who were working.
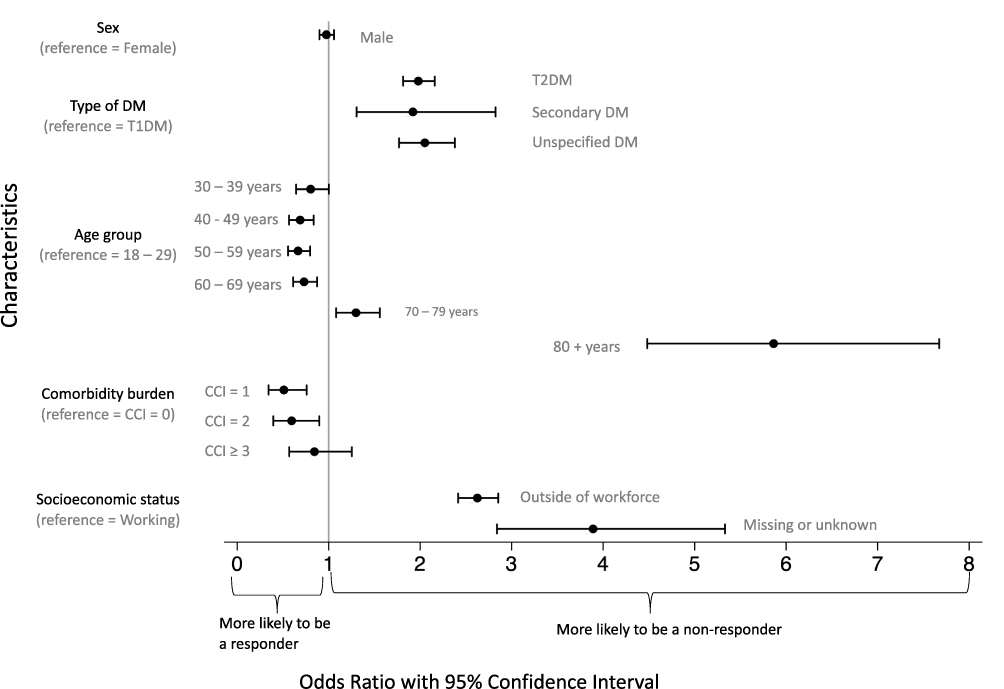 |
Figure 2 The odds of being a non-responder for each of the characteristics. Abbreviations: DM, diabetes mellitus; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; CCI, Charlson comorbidity index. |
Discussion
Our study found responder bias for age, but it did not exist for sex. Linking our sample frame to different national data registries, we determined that the characteristics of our non-responders were different from our responders on type of DM, CCI and SES. Several of the confidence intervals for the characteristics were wide. This may be due to the heterogeneity of the individuals within each characteristic and not the sample size given there was a 95% chance that the true proportion falls within 0.7% of the estimated proportion.
The response rates to surveys have generally been decreasing over time. The overall response rate for the European Social Survey (ESS) went from 62% in 2002 to 57% in 2014.10 The Danish response rate for the ESS declined from around 68% in 2002 to 52% in 2014. In Finland, the Finnish Adults’ Health Behavior Survey is mailed to a random sample of the population aged 15 to 64 years every year.11 The response rates for that survey changed from 84% for men and 85% for women in 1978 to 59% and 71%, respectively. There was a slight decline in the Danish Health and Morbidity Surveys’ response rate from 61% in 2010 to 56% in 2017.12 But, the survey mode did change over time from being 100% mailed to 74% being web-based in 2017.
Response rate is impacted by survey mode. A meta-analysis of 114 studies that compared response rates to web-based surveys over the other modes (ie, postal mail, telephone, email) response rates were on average 12% (95% CI 9–16%) lower.13 When considering studies published between 2005 and 2016, the authors found the response rate was 15% (11–19%) lower.
It is difficult to compare our response rate of 36% against other web-based surveys’ response rates. We had several additional steps that needed to be completed before initiating the survey. The invitation and the personal link to the electronic questionnaire booklet were sent through the e-Boks system. Users of e-Boks are first notified by email that they have a new message in their secure e-Boks’ mailbox and who the message is from. Then, the individual is required to log onto the e-Boks system and open their secure mail. Unfortunately, we do not know how many individuals read the invitation in their secure mailbox and decided not to click the survey link.
When focusing on surveys that have solely used e-Boks as their means of survey recruitment, participation rates are similar to ours. For example, a recent study of individuals included in the inflammatory rheumatoid disease registry had a participation rate of 35%.14 Another study about seeking health care outside of regular clinical hours reported a participation rate of 36% for the random sample.15 When examining their response rate by age groups, the response rate for individuals aged 50 to 59 years was the same as ours (44%), whereas, for individuals aged 30 to 39 years, it was lower than ours (23% versus 40%). A study dealing with mothers’ decisions for not allowing their adolescent children to be vaccinated against human papillomavirus (HPV) reported an overall response rate of 54%.16 Their higher response rate may be explained by the topic, which had extensive media coverage in Denmark at that time. Their response rates for the 20–29 years old and 30–39 years old were 14% and 17% larger than ours for these age groups, but their response rate for mothers who were working was 5% higher than the response rate for our working individuals. Lastly, a study examining the prevalence and impact of knee pain among 60- to 69-year-olds living in Copenhagen had a response rate of 52%, which is higher than ours of 42%.17
A major strength of this non-participation analysis is that we could link to different Danish data registries and learn more about non-responders than their age and sex. Another strength is using the e-Boks system because we know the invitation did indeed reach everyone in the sample frame. Therefore, individuals’ not up-dating home addresses and telephone numbers in the clinical database were eliminated. However, it is possible during the data collection phase some of the e-Boks accounts were terminated due to death, emigration or unable to access it anymore.
We acknowledge there are several limitations in our study. Some potential respondents may have received an invitation to participate in another study during the same period. Notably, individuals from OUH are asked to participate in different studies. Unfortunately, it was not possible to remove the individuals who were invited to participate in the pilot study from the sample frame as we did not know who they were. Therefore, the potential respondents may be experiencing a participation burden and decided not to participate. It has been shown that if respondents perceive there is a benefit from participating not only to themselves but also to other people like themselves, they are more likely to participate.18 However, there is a point where saturation may occur when too many requests are asked upon the same group of people, which ultimately affects the response rate.19
Another limitation was that we could only send two reminders out using the e-Boks system due to time constraints. We did not have the means to post paper-based questionnaires to the non-responders, nor was there an option for individuals to ask for a paper-based questionnaire to be mailed to them. In addition, the time constraints of double-data entering paper-based questionnaires into the database made the option unreasonable. It has been suggested using different delivery modes, also called mixed modes, may increase the response rate.20 However, using mixed modes of survey distribution does not guarantee an increase in the response rate. A meta-analysis found that adding a web-based option to a mail survey resulted in lower response rates.21
Our electronic questionnaire booklet was quite long. The booklet could have taken around 30 minutes to complete. Several studies have determined the ideal time to complete a survey should be less than 20 minutes.22,23 To reduce the time needed, the electronic questionnaire booklet did contain several skip patterns. Thus, the respondents could skip over an entire section if they had never experienced pain and/or discomfort in a specific area. Also, a status bar stated what question the respondent was currently answering and how many questions there were in total.
Lastly, we cannot distinguish between individuals who clicked the survey link and stated they were not interested from those who did not respond at all due to how the data was saved in the system.
The electronic questionnaire booklet was developed to study the prevalence of MSK conditions and their consequences in a cohort of individuals who attended an ambulatory DM clinic in two acute care hospitals in Denmark. Our goal is to elaborate how MSK fits into the DM clinical presentation (eg is MSK related to the severity of DM complications). Our long-term goal would be to include a closer screening of MSK in DM as part of the clinical routine check-ups. As it has been found, health care providers do not raise this issue during a diabetic consultation. In a survey of Dutch primary care physicians and nurse practitioners, it was found that a majority did not know that limited joint mobility of the upper extremities was a complication to DM.24 In addition, around 63% of nurse practitioners believed that screening for this complication should be done regularly, but a quarter of primary care physicians thought it was worthwhile.
In conclusion, our response rate was similar to other surveys that used the same survey mode. Although we did find a non-response bias where the characteristics of the non-responders differed from the responders, it is still important to determine the prevalence and consequences of MSK conditions in a secondary care DM population.
Acknowledgments
We want to acknowledge Amalie Frost Stammerjohan, who was responsible for assembling the electronic questionnaire booklet and conducting the pilot study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. Have drafted or written, or substantially revised or critically reviewed the article. Have agreed on the journal to which the article will be submitted. Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. Agree to take responsibility and be accountable for the contents of the article.
Funding
Erik Frafjord was funded by a grant from the Danish Foundation for Chiropractic Research and Postgraduate Education.Søren Skou is currently funded by a grant from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation program (grant agreement No 801790) and a program grant from Region Zealand (Exercise First).The Department of Endocrinology, Odense University Hospital, funded expenses related to study administration and expenses related to Statistics Denmark.
Disclosure
Mr Erik Frafjord report grants from Foundation for Advancement of Chiropractic Research and Postgraduate Education, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61:344–349. doi:10.1016/j.jclinepi.2007.11.008
2. Pedersen CB. The Danish Civil Registration System. Scand J Public Health. 2011;39(7 Suppl):22–25. doi:10.1177/1403494810387965
3. Molsted S, Tribler J, Snorgaard O. Musculoskeletal pain in patients with type 2 diabetes. Diabetes Res Clin Pract. 2012;96:135–140. doi:10.1016/j.diabres.2011.12.022
4. Carvalho-E-Silva AP, Ferreira ML, Ferreira PH, Harmer AR. Does type 2 diabetes increase the risk of musculoskeletal pain? Cross-sectional and longitudinal analyses of UK biobank data. Semin Arthritis Rheum. 2020;50:728–734. doi:10.1016/j.semarthrit.2020.05.007
5. Smith AD, Crippa A, Woodcock J, Brage S. Physical activity and incident type 2 diabetes mellitus: a systematic review and dose-response meta-analysis of prospective cohort studies. Diabetologia. 2016;59:2527–2545. doi:10.1007/s00125-016-4079-0
6. Andersen JS, Olivarius Nde F, Krasnik A. The Danish National Health Service Register. Scand J Public Health. 2011;39(7 Suppl):34–37. doi:10.1177/1403494810394718
7. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
8. Christiansen CF, Moller MH, Nielsen H, Christensen S. The Danish Intensive Care Database. Clin Epidemiol. 2016;8:525–530. doi:10.2147/CLEP.S99476
9. Stattistics Dennmark SOCIO2013; 2020. Available from: https://www.dst.dk/da/Statistik/dokumentation/Times/personindkomst/socio13.
10. Beullens K, Loosveldtt G, Vamdemplas C, Stoop I. Response raes in the European Social Survey: increasing, descreasing, or a matter of fieldwork efforts? 2018. Available from: https://www.surveyinsights.org/?p=9673.
11. Tolonen H, Helakorpi S, Talala K, Helasoja V, Martelin T, Prattala R. 25-year trends and socio-demographic differences in response rates: finnish adult health behaviour survey. Eur J Epidemiol. 2006;21:409–415. doi:10.1007/s10654-006-9019-8
12. Jensen HAR, Ekholm O, Davidsen M, Christensen AI. The Danish health and morbidity surveys: study design and participant characteristics. BMC Med Res Methodol. 2019;19:91. doi:10.1186/s12874-019-0733-9
13. Daikeler J, Bosnjak M, Manfreda KL. Web versus otther survey modes: an updated and extended meta-analysis comparing response rattes. J Survey Stat Methodol. 2019;8:36.
14. Glintborg B, Jensen DV, Engel S, et al. Self-protection strategies and health behaviour in patients with inflammatory rheumatic diseases during the COVID-19 pandemic: results and predictors in more than 12 000 patients with inflammatory rheumatic diseases followed in the Danish DANBIO registry. RMD Open. 2021;7:e001505. doi:10.1136/rmdopen-2020-001505
15. Ebert JF, Huibers L, Christensen B, Christensen MB. Paper- or web-based questionnaire invitations as a method for data collection: cross-sectional comparative study of differences in response rate, completeness of data, and financial cost. J Med Internet Res. 2018;20:e24. doi:10.2196/jmir.8353
16. Baumann A, Andersen B, Ostergaard L, Larsen MB. Sense & sensibility: decision-making and sources of information in mothers who decline HPV vaccination of their adolescent daughters. Vaccine X. 2019;2:e100020. doi:10.1016/j.jvacx.2019.100020
17. Ginnerup-Nielsen E, Christensen R, Heitmann BL, et al. Estimating the Prevalence of Knee Pain and the Association between Illness Perception Profiles and Self-Management Strategies in the Frederiksberg Cohort of Elderly Individuals with Knee Pain: a Cross-Sectional Study. J Clin Med. 2021;10:668. doi:10.3390/jcm10040668
18. Singer E, Couper MP, Fagerlin A, et al. The role of perceived benefits and costs in patients’ medical decisions. Health Expect. 2014;17:4–14. doi:10.1111/j.1369-7625.2011.00739.x
19. Leeper TJ. Where have the respondents gone? Perhaps we ate them all. Public Opin Q. 2019;83(S1):1. doi:10.1093/poq/nfz010
20. DeLeeuw ED. Mixed-medthods: past, present, and future. Surv Res Methods. 2018;12(2):14.
21. Medway RL, Fulton J. When more gets you less: a meta-analysis of the effect of concurrent web options on mail survey response rattes. Public Opin Q. 2012;76:13. doi:10.1093/poq/nfs047
22. Saleh A, Bista K. Examinning factors impactting online survey response rates in educaion research: perceptions of graduate students. J Multidiscip Eval. 2017;13:11.
23. Revilla M, Achoa C. Ideal and maximum length for a web survey. Int J Market res. 2017;59:9.
24. Alabdali LAS, Jaeken J, Dinant GJ, Ottenheijm RPG. Awareness of limited joint mobility in type 2 diabetes in general practice in the Netherlands: an online questionnaire survey. BMC Fam Pract. 2019;20:98. doi:10.1186/s12875-019-0987-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.