")
Back to Journals » OncoTargets and Therapy » Volume 11
The CXCL12 rs1801157 polymorphism and risk of colorectal cancer: a meta-analysis
Authors Xu K , Dai H, Wang S, Zhang J, Liu T
Received 12 September 2017
Accepted for publication 5 March 2018
Published 1 May 2018 Volume 2018:11 Pages 2445—2452
DOI https://doi.org/10.2147/OTT.S151514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ingrid Espinoza
Ke Xu,1 Hong Dai,2 Shaolong Wang,1 Jie Zhang,1 Tao Liu1
1Department of Oncology, The First Affiliated Hospital of Chengdu Medical College, Chengdu, Sichuan, People’s Republic of China; 2Department of Preclinical and Forensic Medicine, Sichuan University, Chengdu, Sichuan, People’s Republic of China
Background: The CXCL12 rs1801157 polymorphism is putatively associated with the risk of malignancy. However, research results are inconsistent regarding particular cancers, especially colorectal cancer (CRC).
Methods: We conducted a meta-analysis via a comprehensive literature search of the databases PubMed and Embase. Odds ratios and their corresponding 95% confidence intervals were extracted to assess comprehensively the association between the CXCL12 rs1801157 polymorphism and the risk of CRC.
Results: According to the following models, the correlation between the presence of the CXCL12 rs1801157 polymorphism and the risk of CRC was not statistically significant: allelic (G cf. A), heterozygous (GG cf. GA), homozygous (GG cf. AA), dominant (GG cf. GA+AA), or recessive (AA cf. GA+GG) for pooled calculating. However, in subgroup analysis, elevated risk of CRC was found in the non-Caucasian group in four genetic models, while no connection was found in the Caucasian group. The sensitivity analysis confirmed that the result of the Caucasian group was stable and analyzed the heterogeneity of the non-Caucasian group.
Conclusion: This meta-analysis suggested that the CXCL12 rs1801157 polymorphism did not significantly confer a risk of CRC among Caucasians but may among non-Caucasians. These results warrant confirmation and further studies of different ethnic populations.
Keywords: CXCL12, rs1801157, polymorphism, CRC, meta-analysis
Introduction
Colorectal cancer (CRC) is one of the most common malignancies worldwide, ranking third in both the number of new cases and mortality rate. Approximately 55% of cases occur in developed countries.1 However, the incidence of CRC is also increasing in the developing world, as the westernized lifestyle is adopted, and the aging population.2 Thus, it is important to determine the risk factors that contribute to CRC, and in recent years, studies on the pathogenesis of CRC have increased greatly.
The risk of CRC is related to many factors, as with most other malignancies. Various epidemiological studies have suggested that the following increase the risk of CRC: family history of CRC,3 inflammatory bowel disease,4 diabetes,5 obesity,6 diet habits,7 smoking,8 drinking,9 and infection with Helicobacter pylori or Fusobacterium spp.10,11 Other studies suggest that calcium and fiber supplementation,12 aspirin use,13,14 and exercise may help prevent CRC.15 Because a family history of CRC is a strong risk factor,16 further analysis of the association between genetic factors and CRC is warranted.
The chemokine protein CXCL12 (also known as SDF1) and its receptor CXCR4 are involved in the proliferation, differentiation, and migration of specific cells in the body.17 The levels of CXCL12 are high in individual organs such as liver, brain, heart, and kidney.18 Recently, studies have linked the CXCL12/CXCR4 biological axis to malignancy,19 and elevated levels of SDF1 may be associated with an increased risk of malignancy.
The CXCL12 gene is located on chromosome 10q11.1. A single nucleotide polymorphism (SNP) in noncoding region 801 (G/A) of the CXCL12 gene upregulated the expression of SDF1.20,21 An increasing number of studies in recent years have confirmed an association between the CXCL12 rs1801157 polymorphism and the risk of malignancies.22,23 Nevertheless, whether it is associated specifically with the risk of CRC remains controversial. Therefore, this meta-analysis of relevant studies was conducted to investigate further an association between CXCL12 rs1801157 polymorphism and the risk of CRC.
Methods
Search strategy
A systematic search was performed in the PubMed and Embase databases for literature published in English up to June 1, 2017. The search involved combinations of the terms “colorectal” or “colon” or “rectal” and “cancer” or “carcinoma” or “tumor” or “neoplasms” and “C-X-C motif chemokine 12” or “CXCL12” or “SDF1” or “stromal cell-derived factor 1” or “G801A “or “rs1801157” and “polymorphism” or “variation” or “variant.”
Eligibility criteria
For inclusion in this meta-analysis, the studies conformed to the following four major criteria: all CRCs were pathologically diagnosed; concerned an association between the rs1801157 polymorphism of CXCL12 and the risk of CRC; a case–control study design, with a control group in Hardy–Weinberg equilibrium (HWE). All basic experimental research, duplicated research, studies with unavailable experimental data, case reports or reviews or editorial articles, or non-English literature were excluded.
Data extraction
Two researchers extracted data from the included studies independently. All the data were then crosschecked. Differences arising during data extraction were discussed and resolved by consulting a third researcher. The following data were noted: name of the author, year of publication, country of origin, ethnicity of subjects, study design, genotyping method, sample size, and P-value of the HWE test for the control group. If the study did not specifically describe the ethnicity of enrolled patients or volunteers, they were considered the main ethnicity of the investigated area.
Quality evaluation
All eligible studies were evaluated by the Newcastle–Ottawa Quality Assessment Scale (NOS), which evaluates the quality of literature, mainly according to the standardization of selection, comparability, and exposure. All authors of this meta-analysis participated in quality assessment, and a consensus was reached on the score after discussion. Scores ranged from 0 to 9 points. Generally, studies scored >5 points were considered high-quality research.
Statistical analysis
The Chi-squared goodness-of-fit test was employed to examine whether the genotype distributions of the CXCL12 rs1801157 polymorphism in the controls were in HWE (P > 0.05 for genetic equilibrium). Each of five genetic models were compared and analyzed: the allele model (G cf A), heterozygous model (GG cf GA), homozygous model (GG cf AA), dominant model (GG cf GA+AA), and the recessive model (AA cf GA+GG). The strength of the association between the CXCL12 rs1801157 polymorphism and the risk of CRC was assessed by odds ratio (OR) with the corresponding 95% confidence interval (CI). Cochran’s Q statistic and the I-squared (I2) statistic were used to test the heterogeneity between studies. Heterogeneity was considered significant when P < 0.10 or I2 > 50%, where the random effects model was used.
In addition, subgroup analyses by ethnicity were conducted. Populations were stratified as Caucasian or non-Caucasian. Sensitivity analyses were performed by recalculating the pooled ORs in a random effects model, which replaced the fixed effects model, and by omitting one study each time to examine its effect on the entire OR value. Finally, the Harbord test was used to determine publication bias, where P < 0.05 indicated bias.24 All statistical analyses were performed in the STATA 13.0 program (StataCorp LP, College Station, TX, USA).
Results
Characteristics of the included studies
Twenty-eight potential articles were initially identified in the literature search (10 from PubMed, 18 from Embase; Figure 1). After applying the inclusion and exclusion criteria, 22 articles were disqualified, specifically nine each for duplicated publication or not associated with CXCL12 rs1801157 polymorphism and the risk of CRC; two for lacking a control group; and one each for being a review or basic research.
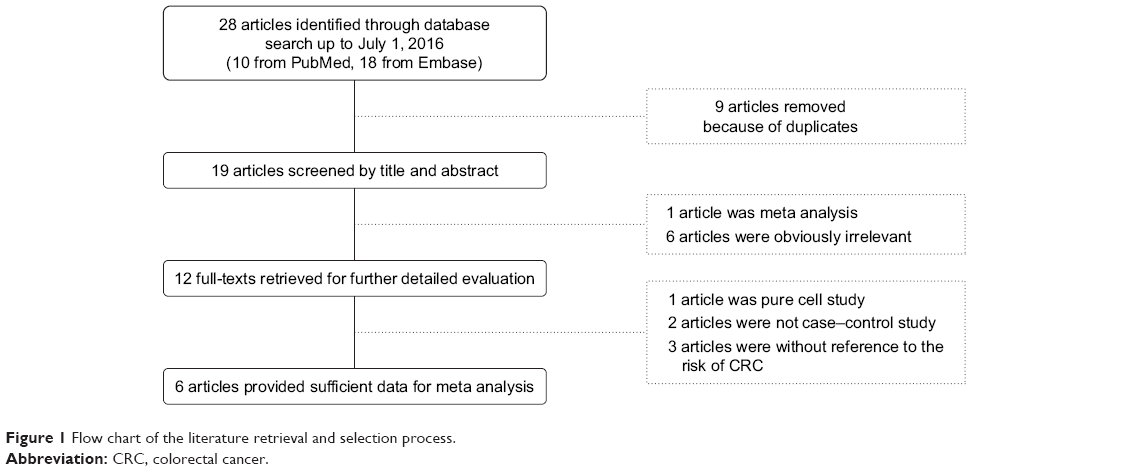 | Figure 1 Flow chart of the literature retrieval and selection process. |
Finally, the following six articles were included: Hidalgo-Pascual et al,25 Shi et al,26 Dimberg et al,27 Amara et al,28 Razmkhah and Ghaderi,29 and Ramzi et al.30 The studies of Hidalgo-Pascual et al, Dimberg et al, and Razmkhah and Ghaderi were conducted in Caucasian populations, and other studies were non-Caucasian (Table 1).
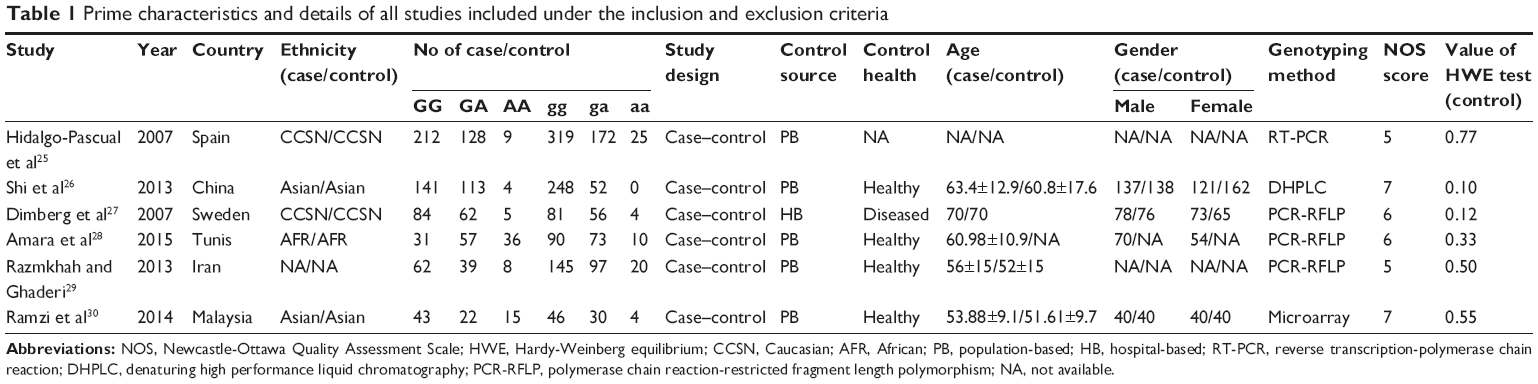 | Table 1 Prime characteristics and details of all studies included under the inclusion and exclusion criteria |
Overall data analysis
The present meta-analysis of the six included articles comprised pooled data of 1,071 CRC patients and 1,472 controlled volunteers. All of the five genetic models were used for random effects model, owing to significant heterogeneity. From comparisons using all five genetic models, no significant association was found between the rs1801157 polymorphism and the risk of CRC (Table 2).
 | Table 2 Prime result of subgroup analysis and pooled analysis for CXCL12 rs1801157 polymorphism on the risk of CRC |
Subgroup analysis
In all five genetic models specifically in the group of Caucasians, there was no correlation between the CXCL12 rs1801157 polymorphism and the risk of CRC. However, comparisons using the allele, homozygous, dominant, and recessive genetic models showed that non-Caucasians with the CXCL12 rs1801157 polymorphism had an elevated risk of CRC. However, according to the heterozygous model, there was no association between the rs1801157 polymorphism and the risk of CRC in these non-Caucasian subjects (Table 2 and Figure 2).
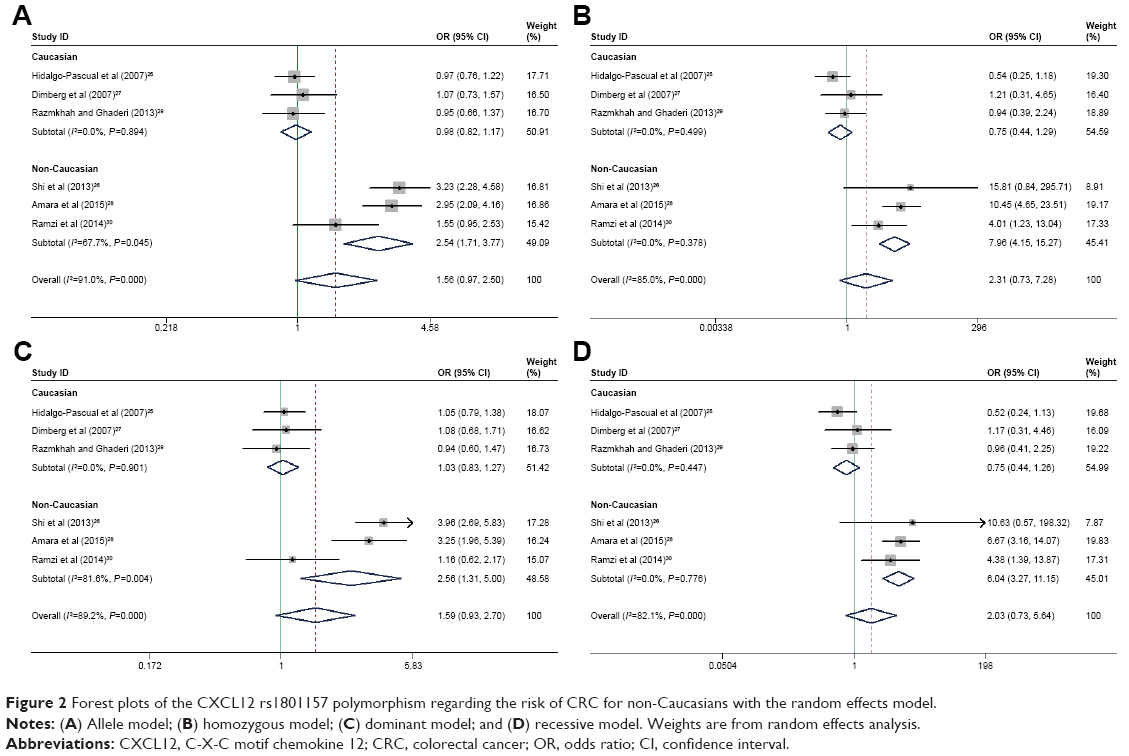 | Figure 2 Forest plots of the CXCL12 rs1801157 polymorphism regarding the risk of CRC for non-Caucasians with the random effects model. |
Sensitivity analysis
In the sensitivity analysis, the change from the fixed effects model to the random effects model did not substantially affect the results. However, in the dominant model among the non-Caucasians, the original OR of 2.556 (95% CI: 1.307–5.001) changed to 1.980 (95% CI: 0.724–5.417) after excluding Shi et al, and changed to 2.202 (95% CI: 0.664–7.297) after excluding Amara et al. Similar changes were found in the heterozygous model in the non-Caucasian group after excluding Ramzi et al (OR: 3.045, 95% CI: 1.833–5.059) (Figure 3). In the other genetic models applied to Caucasians and non-Caucasians, the ORs did not significantly change.
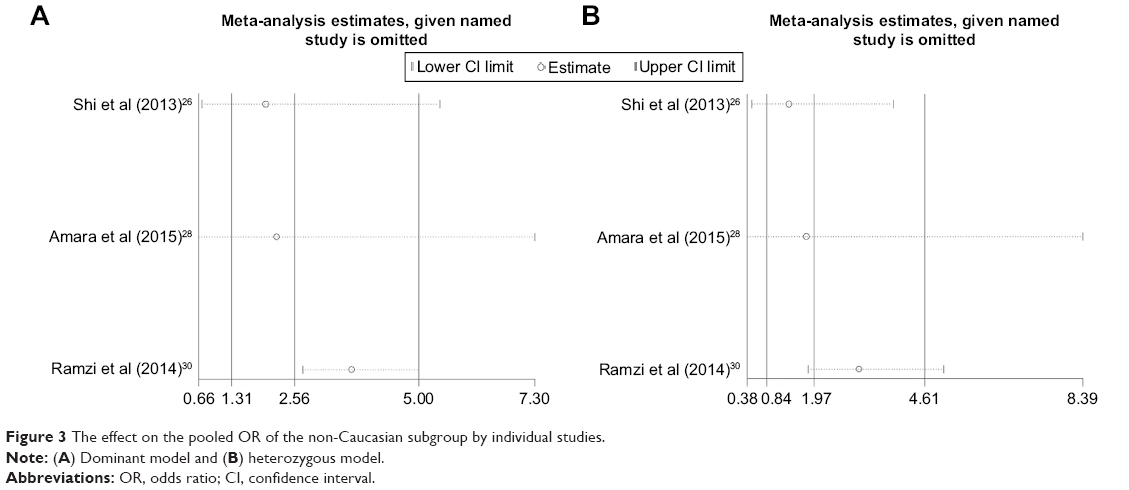 | Figure 3 The effect on the pooled OR of the non-Caucasian subgroup by individual studies. |
Publication bias
There was no publication bias via the Harbord tests (Figure 4). Specifically, results of the Harbord tests for the five genetic models were as follows: allele, P = 0.613, 95% CI: −14.969 to 22.314; heterozygous, P = 0.771, 95% CI: −14.323 to 11.432; homozygous, P = 0.780, 95% CI: −9.913 to 12.304; dominant, P = 0.880, 95% CI: −14.567 to 16.360; and recessive, P = 0.877, 95% CI: −9.259 to 10.431.
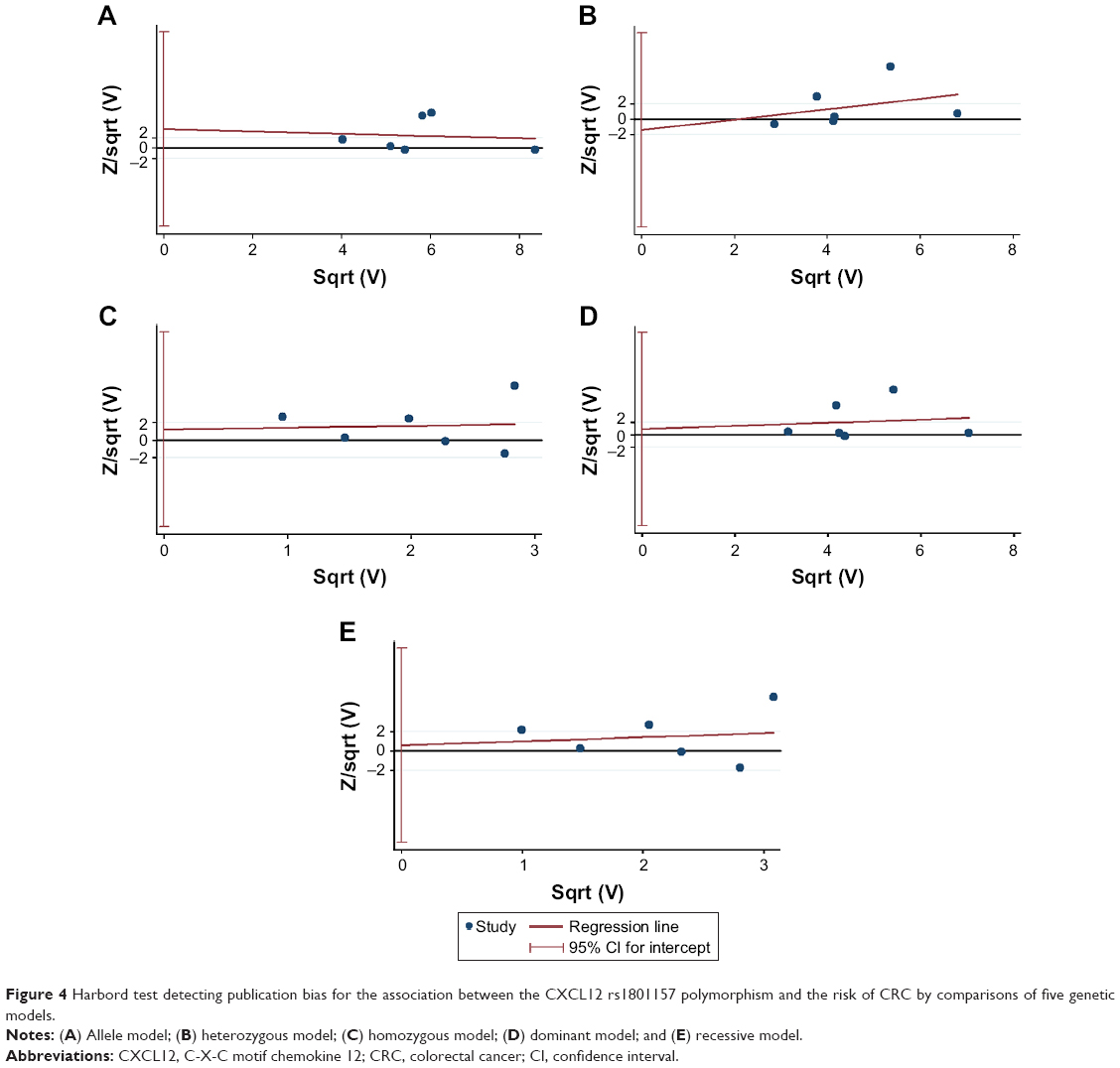 | Figure 4 Harbord test detecting publication bias for the association between the CXCL12 rs1801157 polymorphism and the risk of CRC by comparisons of five genetic models. |
Discussion
Like most malignancies, many factors contribute to a risk of CRC. Lichtenstein et al found that 35% of the risk of CRC was determined by genetic factor.31 However, there is much about the underlying genetics of CRC that lacks elucidation. SNPs directly take variation of the genetic sequence as marker, are closely associated with human phenotypic differences, disease susceptibility, and drug reactions. Genome-wide association studies (GWAS) have reported that 14 SNPs are associated with the risk of CRC and could explain ~6% of the excess familial risk.32,33 Theodoratou et al in a meta-analysis extracted data from 635 studies regarding SNP and CRC and found 16 independent variants at 13 loci linked to the risk of CRC.34 However, none of the abovementioned studies have investigated an association specifically between the CXCL12 rs1801157 polymorphism and risk of CRC.
CXCL12 is closely related to invasion and metastasis of CRC through the CXCL12/CXCR4 axis, but it is unclear whether there is a risk associated with CRC. Recently, studies have been conducted concerning the link between the CXCL12 rs1801157 polymorphism and the risk of malignancies. For example, in an Asian population the polymorphism was associated with malignancies, but in a Caucasian population this was uncertain.23 Xia et al found individuals with the A allele of the G801A polymorphism in the CXCL12 gene are under a higher risk for breast carcinoma.35 Zhang et al demonstrated that SDF1-3′A polymorphism may be associated with increased risk of hematological malignancy, especially for chronic myeloid leukemia, Hodgkin’s lymphoma, multiple myeloma and the non-Caucasian population.36 Studies have also investigated the association between the CXCL12 rs1801157 polymorphism and CRC risk regarding the site of occurrence,25,27 degree of tumor invasion,28,37 and prognosis.25,38 However, the role of this polymorphism in the development and progression of CRC remains uncertain. The present meta-analysis was performed to obtain a more accurate and objective conclusion through strict evaluation and analyses of similar research. To our best knowledge, the present meta-analysis is the first to assess the association between the CXCL12 rs1801157 polymorphism and the risk of CRC. In this study, in five genetic models, upon calculating the pooled ORs no association between the CXCL12 rs1801157 polymorphism and the risk of CRC was found. It should be noted that the heterogeneity among each model was obvious, yet to analyze the source of the heterogeneity, we successively conducted subgroup and sensitivity analyses. In the subgroup analysis, ethnicity was identified as a factor responsible for heterogeneity. The heterogeneity was acceptable in the Caucasian group, and the result was stable. This suggested that there was no significant association between the CXCL12 rs1801157 polymorphism and the risk of CRC among the Caucasian population. This reconfirmed and complemented the published meta-analysis by Tong et al concerning various malignancies,23 although it should be noted that the study did not specifically address CRC in detail because it was published early and included only three CRC-related studies. On the other hand, the present meta-analysis found obvious heterogeneity within some genetic model comparisons among the non-Caucasians. Two studies in this meta-analysis were very different from the others, as Shi et al only included CRC patients at stage T2 in the test group, and Ramzi et al used gene chip technology for gene analysis. These two factors were identified as the main source of heterogeneity after deep analysis for the three studies of this group. Finally, through comparisons of the allele, homozygous, dominant, and recessive genetic models, we found that in the non-Caucasian population, the CXCL12 rs1801157 polymorphism may be associated with a risk of CRC, and the A allele increased the risk of CRC. Whereas the study of Razmkhah and Ghaderi29 did not report the ethnicity of the samples and the heterogeneity in non-Caucasian subgroup, a sensitivity analysis was conducted to improve the reliability and stability of these results. The pooled ORs were not significantly affected except for the comparison of heterozygous model and dominant model in the non-Caucasian population. It implied that the results concerning the Caucasian group were more reliable, but the result of the non-Caucasian group should be understood with caution. This may be due to the heterogeneity of the non-Caucasian group. Thus, further randomized controlled studies with a large sample size are needed to confirm the association among non-Caucasian subjects. In particular, it is necessary to stratify non-Caucasian populations by specific ethnicities.
Why should we persist in publishing this meta-analysis although the abovementioned results and analysis need to be further studied? All meta-analyses about CXCL12 polymorphism and the risk of malignancies were fully consulted before we did this research. Various cancers were mixed together to analysis by most of the studies and got the statistically significant results of the correlation. Deeper research was bound by the lack of single disease studies. Recently, the related literature were published increasingly in the study of breast cancer, CRC, and hematological malignancies with the research advance of this aspect. Scholars have completed the meta-analysis of breast cancer and hematological malignancies about this respectively.35,36 The result of CRC is still controversial. More credible and acceptable results are expected based on the method of evidence-based medicine. Only in this way can researchers carry out further studies on the connection between CXCL12 polymorphism and the clinicopathology of CRC.
This meta-analysis is limited by the obvious insufficient quantity and depth of the included studies, especially for non-Caucasian subjects. We were unable to conduct an in-depth subgroup analysis, because of the incompleteness and incomprehensiveness of specific data such as gender, age, and lifestyle, which were difficult to collect. HWE testing was not routinely and appropriately performed in most of the included studies. Only Ramzi et al reported on HWE and others had to be recalculated. In addition, studies that have investigated an association between the CXCL12 rs1801157 polymorphism and the occurrence and development of CRC are still rare, and much remains unknown regarding primary site, invasion, metastasis, and prognosis.
Conclusion
The present meta-analysis did not find a significant association between the CXCL12 rs1801157 polymorphism and risk of CRC. However, this result may be belied in some populations because of the existence of the heterogeneity in overall calculation process. In summary, this meta-analysis indicated that the CXCL12 rs1801157 polymorphism had no significant association with the risk of CRC among Caucasians but may contribute to the risk of CRC among non-Caucasians. Nevertheless, studies should be conducted to reconfirm these conclusions among different ethnic populations.
Disclosure
The authors report no conflicts of interest in this work.
References
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):359–386. | ||
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. | ||
Taylor DP, Burt RW, Williams MS, Haug PJ, Cannon-Albright LA. Population-based family history-specific risks for colorectal cancer: a constellation approach. Gastroenterology. 2010;138(3):877–885. | ||
Jess T, Rungoe C, Peyrin-Biroulet L. Risk of colorectal cancer in patients with ulcerative colitis: a meta-analysis of population-based cohort studies. Clin Gastroenterol Hepatol. 2012;10(6):639–645. | ||
Jiang Y, Ben Q, Shen H, Zhang Y, Zhu J. Diabetes mellitus and incidence and mortality of colorectal cancer: a systematic review and meta-analysis of cohort studies. Eur J Epidemiol. 2011;26(11):863–876. | ||
Ma Y, Yang Y, Wang F, et al. Obesity and risk of colorectal cancer: a systematic review of prospective studies. PLoS One. 2013;8(1):e53916. | ||
Chan DS, Lau R, Aune D, et al. Red and processed meat and colorectal cancer incidence: meta-analysis of prospective studies. PLoS One. 2011;6(6):e20456. | ||
Liang PS, Chen TY, Giovannucci E. Cigarette smoking and colorectal cancer incidence and mortality: systematic review and meta-analysis. Int J Cancer. 2009;124(10):2406–2415. | ||
Fedirko V, Tramacere I, Bagnardi V, et al. Alcohol drinking and colorectal cancer risk: an overall and dose-response meta-analysis of published studies. Ann Oncol. 2011;22(9):1958–1972. | ||
Sonnenberg A, Genta RM. Helicobacter pylori is a risk factor for colonic neoplasms. Am J Gastroenterol. 2013;108(2):208–215. | ||
Kostic AD, Gevers D, Pedamallu CS, et al. Genomic analysis identifies association of Fusobacterium with colorectal carcinoma. Genome Res. 2012;22(2):292–298. | ||
Bonithon-Kopp C, Kronborg O, Giacosa A, Räth U, Faivre J. Calcium and fibre supplementation in prevention of colorectal adenoma recurrence: a randomised intervention trial. European Cancer Prevention Organisation Study Group. Lancet. 2000;356(9238):1300–1306. | ||
Bosetti C, Rosato V, Gallus S, Cuzick J, La Vecchia C. Aspirin and cancer risk: a quantitative review to 2011. Ann Oncol. 2012;23(6):1403–1415. | ||
Rothwell PM, Fowkes FG, Belch JF, Ogawa H, Warlow CP, Meade TW. Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomised trials. Lancet. 2011;377(9759):31–41. | ||
Boyle T, Keegel T, Bull F, Heyworth J, Fritschi L. Physical activity and risks of proximal and distal colon cancers: a systematic review and meta-analysis. J Natl Cancer Inst. 2012;104(20):1548–1561. | ||
Brenner H, Kloor M, Pox CP. Colorectal cancer. Lancet. 2014;383(9927):1490–1502. | ||
Li L, Jiang K, Tan P, et al. Prognosis and clinicopathology of CXCR4 in colorectal cancer patients: a meta-analysis. Asian Pac J Cancer Prev. 2015;16(9):4077–4080. | ||
Horuk R. Chemokines beyond inflammation. Nature. 1998;393(6685):524–525. | ||
Balkwill F. Chemokine biology in cancer. Semin Immunol. 2003;15(1):49–55. | ||
Winkler C, Modi W, Smith MW, et al. Genetic restriction of AIDS pathogenesis by an SDF1 chemokine gene variant. ALIVE Study, Hemophilia Growth and Development Study (HGDS), Multicenter AIDS Cohort Study (MACS), Multicenter Hemophilia Cohort Study (MHCS), San Francisco City Cohort (SFCC). Science. 1998;279(5349):389–393. | ||
Watanabe MA, de Oliveia Cavassin GG, Orellana MD, et al. SDF1 gene polymorphisms and syncytia induction in Brazilian HIV-1 infected individuals. Microb Pathog. 2003;35(1):31–34. | ||
Zhu K, Jiang B, Hu R, et al. The CXCL12 G801A polymorphism is associated with cancer risk: a meta-analysis. PLoS One. 2014;9(9):e108953. | ||
Tong X, Ma Y, Deng H, et al. The SDF-1 rs1801157 polymorphism is associated with cancer risk: an update pooled analysis and FPRP test of 17,876 participants. Sci Rep. 2016;6:27466. | ||
Harbord RM, Egger M, Sterne JA. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat Med. 2006;25(20):3443–3457. | ||
Hidalgo-Pascual M, Galan JJ, Chaves-Conde M, et al. Analysis of CXCL12 3′UTR G>A polymorphism in colorectal cancer. Oncol Rep. 2007;18(6):1583–1587. | ||
Shi MD, Chen JH, Sung HT, et al. CXCL12-G801 A polymorphism modulates risk of colorectal cancer in Taiwan. Arch Med Sci. 2013;9(6):999–1005. | ||
Dimberg J, Hugander A, Löfgren S, Wågsäter D. Polymorphism and circulating levels of the chemokine CXCL12 in colorectal cancer patients. Int J Mol Med. 2007;19(1):11–15. | ||
Amara S, Chaar I, Khiari M, et al. Relationship between SDF1G801A polymorphism and its expression in Tunisian patients with colorectal cancer. J Immunoassay Immunochem. 2015;36(2):182–194. | ||
Razmkhah M, Ghaderi A. SDF1alpha G801A polymorphism in Southern Iranian patients with colorectal and gastric cancers. Indian J Gastroenterol. 2013;32(1):28–31. | ||
Ramzi NH, Chahil JK, Lye SH, et al. Role of genetic & environment risk factors in the aetiology of colorectal cancer in Malaysia. Indian J Med Res. 2014;139(6):873–882. | ||
Lichtenstein P, Holm NV, Verkasalo PK, et al. Environmental and heritable factors in the causation of cancer – analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med. 2000;343(2):78–85. | ||
COGENT Study, Houlston RS, Webb E, Broderick P, et al. Meta-analysis of genome-wide association data identifies four new susceptibility loci for colorectal cancer. Nat Genet. 2008;40(12):1426–1435. | ||
Houlston RS, Cheadle J, Dobbins SE, et al. Meta-analysis of three genome-wide association studies identifies susceptibility loci for colorectal cancer at 1q41, 3q26.2, 12q13.13 and 20q13.33. Nat Genet. 2010;42(11):973–977. | ||
Theodoratou E, Montazeri Z, Hawken S, et al. Systematic meta-analyses and field synopsis of genetic association studies in colorectal cancer. J Natl Cancer Inst. 2012;104(19):1433–1457. | ||
Xia Y, Guo X, Ji T. The G801A polymorphism in the CXCL12 gene and risk of breast carcinoma: evidence from a meta-analysis including 2931 subjects. Asian Pac J Cancer Prev. 2014;15(6):2857–2861. | ||
Zhang X, Fan Y, Li Z. SDF1-3’A polymorphism is associated with increased risk of hematological malignancy: a meta-analysis. Onco Targets Ther. 2017;10:1575–1583. | ||
Allami RH, Graf C, Martchenko K, et al. Analysis of the expression of SDF1 splicing variants in human colorectal cancer and normal mucosa tissues. Oncol Lett. 2016;11(3):1873–1878. | ||
Chang SC, Lin PC, Yang SH, Wang HS, Li AF, Lin JK. SDF1a G801A polymorphism predicts lymph node metastasis in stage T3 colorectal cancer. Ann Surg Oncol. 2009;16(8):2323–2330. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.