")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
The current status of culturally adapted mental health interventions: a practice-focused review of meta-analyses
Authors Rathod S, Gega L, Degnan A , Pikard J, Khan T, Husain N, Munshi T, Naeem F
Received 30 March 2017
Accepted for publication 11 July 2017
Published 4 January 2018 Volume 2018:14 Pages 165—178
DOI https://doi.org/10.2147/NDT.S138430
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Shanaya Rathod,1 Lina Gega,2 Amy Degnan,3 Jennifer Pikard,4 Tasneem Khan,5 Nusrat Husain,3 Tariq Munshi,4 Farooq Naeem4
1Southern Health NHS Foundation Trust, Southampton, UK; 2Department of Health Sciences, University of York, York, UK; 3Division of Psychology and Mental Health, University of Manchester, Manchester, UK; 4Department of Psychiatry, Queen’s University, Kingston, ON, Canada; 5Faculty of Applied Health Sciences, School of Public Health and Health Systems, University of Waterloo, Waterloo, ON, Canada
Abstract: In recent years, there has been a steadily increasing recognition of the need to improve the cultural competence of services and cultural adaptation of interventions so that every individual can benefit from evidence-based care. There have been attempts at culturally adapting evidence-based interventions for mental health problems, and a few meta-analyses have been published in this area. This is, however, a much debated subject. Furthermore, there is a lack of a comprehensive review of meta-analyses and literature reviews that provide guidance to policy makers and clinicians. This review summarizes the current meta-analysis literature on culturally adapted interventions for mental health disorders to provide a succinct account of the current state of knowledge in this area, limitations, and guidance for the future research.
Keywords: cultural adaptation, interventions, mental illness, meta-analysis, minority ethnic, psychotherapies
Introduction
Cultural differences are reported in the prevalence, clinical manifestation, diagnosis, treatment response, and outcomes for individuals with mental health problems. Globalization is making many countries culturally diverse,1 and this places an enormous responsibility on health care systems to ensure that practice is relevant to the variety of cultural backgrounds of the diverse populations,2 thereby reducing health disparities through cultural responsiveness, appropriateness, and effectiveness of clinical services. Lack of cultural competence and cultural adaptations in systems of care is a leading cause of disparity in services for minority cultures leading to poor uptake of available services, adverse outcomes, and increasing the cost to society.3
Despite availability of a number of interventions, studies in mental health have concluded that outcomes for minority cultural groups are not as good as for Caucasian people.4 The current criteria for judging good research designs may or may not be feasible for research on minority ethnic groups, and additionally, there are no paradigms for developing measures or interpreting existing measures to incorporate ethnicity and racialized experiences.5 Therefore, the generalization of findings of the effectiveness of therapeutic interventions to many cultural groups may not be valid or even appropriate.
Despite the potential for a cultural mismatch to render treatments ineffective, clinicians and researchers are disseminating interventions locally and globally across widely diverse cultures.6–9 Efforts to improve this gap remain piecemeal. To date, no comprehensive review of meta-analyses is available with a detailed summary of findings, guidance on the state of current evidence, and directions for future practice.
This review provides a summary and overview of findings across meta-analyses on culturally adapted interventions for mental health problems, describing the current state of affairs. The objectives of this review are to:
- Summarize findings from existing meta-analyses and literature reviews of culturally adapted psychosocial interventions for mental health problems;
- Gather knowledge regarding the nature and process of adaptation;
- Identify what specific elements of cultural adaptation may moderate or mediate the effectiveness of such interventions for mental health problems; and
- Discuss the way forward.
Method
The PICO model10 was used for this study.
Inclusion–exclusion criteria
We included all meta-analyses of 1) psychosocial interventions; 2) populations who belonged to a non-western cultural background, whether living in the west or outside the west; and 3) with mental health problems.
Population
Reviews of studies comprising samples with any type of mental health problem or diagnosis were included. Reviews with mixed diagnostic samples were not excluded.
Interventions
Reviews relating to all types and modalities of an intervention that incorporated a cultural adaptation – psychological and social – were included. We excluded meta-analyses that only incorporated faith and religion-adapted interventions.
Comparators
We reported all comparisons of psychosocial interventions, including standard interventions without cultural adaptation and other comparators such as usual care.
Outcomes
We included all health-related outcomes measured by standardized outcome measures, both generic (eg, quality of life, daily functioning, well-being, disability) and condition-specific (eg, symptoms, risk, recurrence).
Design
We included review papers with meta-analyses. There was no restriction on the types of studies included in the reviews, and no reviews were excluded based on their methodological quality.
Search strategy
We carried out a comprehensive literature search to identify relevant published meta-analyses. The following electronic research databases were searched: MEDLINE (via the Ovid platform); EMBASE (via Ovid); PsycINFO (via EBSCO platform); The Cumulative Index to Nursing and Allied Health Literature (CINAHL) (via EBSCO); the Cochrane Database of Systematic Reviews (CDSR); Database of Abstracts of Reviews of Effectiveness (DARE); Health Technology Assessment database and the NIHR Journals Library; Database of promoting health effectiveness reviews (DoPHER); and PROSPERO (international prospective register of systematic reviews). We searched databases indexing gray literature, such as Opengrey (www.opengrey.eu), which contained references to potentially relevant theses. Reference lists of reviews meeting the inclusion criteria were manually checked to identify any relevant meta-analyses.
We conducted preliminary searches using different terms to capture relevant literature for this review in relation to population (ethnic, minority, migrant); intervention (cultural adaptation, culturally sensitive, culturally appropriate); comparator (intervention, therapy, treatment, care); outcomes (mental health, mental illness, psychiatric disorder, behavior, depression, anxiety, schizophrenia, psychosis); and design (meta-analysis, systematic review).
We used the truncation symbol (*) to search for variable endings; for example, cultural* captured cultural and culturally; depress* captured depression, depressed, and depressive; adapt* captured adaptation and adapted; meta-only* captured meta-analysis, meta-analyses, and meta-analytic (al); therapy* captured therapy, therapeutic, and therapies. Wildcard symbols (? and $) were used to capture different spellings (behavio?r for behaviour and behavior) and different prefixes ($therapy for psychotherapy, physiotherapy, and therapy). We combined our search terms using Boolean AND/OR commands; for example, we searched for (psychiatr* OR mental OR behavio?r*) AND (minorit* OR ethnic* OR *migrant).
Following piloting of various search strategies to assess their sensitivity (ability to capture relevant well-known reviews in the field) and specificity (ability to filter out irrelevant literature so that we did not end up with overinflated number of returned reviews), the search strategy deemed to be the most efficient and sensitive search combined the terms (cultural* OR ethnic) AND (intervention* OR treatment* OR $therap*) and (meta-analy* OR metanaly*). The searches in Medline and CINHAL contained the same terms in all fields, whereas the searches in PsycIINFO searched for these terms only in “abstracts” and included the terms (adapt* OR sensitive OR appropriate OR competen*) to improve the specificity of the search and reduce the number of irrelevant returns.
Database searches were conducted over the past 10 years (2006–2016) of each of the databases, as we know that no relevant reviews have been published before then. We did not filter the results of our searches using only review articles because this returned irrelevant results (reviews without meta-analyses) and also failed to capture some meta-analyses that were not identified in the databases as “reviews.” Searches were restricted to literature published in the English language as we anticipated that most reviews of culturally adapted mental health interventions for nondominant ethnic or racial groups, even when conducted by non-native English-speaking research groups, would have a version published in English. Finally, experts in the field were contacted to identify meta-analyses and reviews of literature in this area.
Evidence selection and synthesis
There is no agreed methodology on reviewing and analyzing data from meta-analyses and literature reviews. We followed a similar method to that of PRISMA.11 We screened all titles and abstracts identified from our literature search against our inclusion criteria and retrieved the full texts of potentially relevant articles for more thorough screening. We selected meta-analyses that met our inclusion criteria regarding population, intervention, comparator, outcomes, and design (Figure 1).
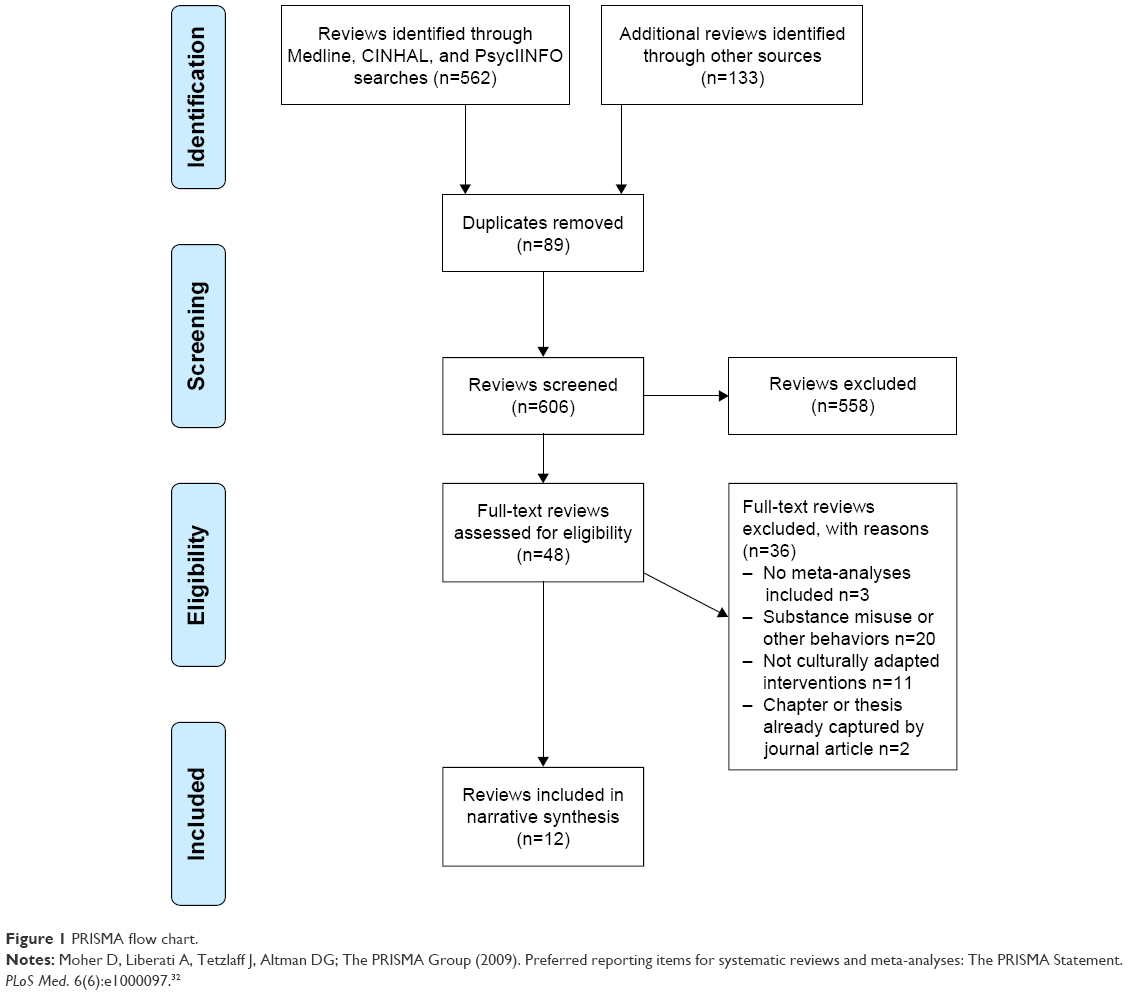 | Figure 1 PRISMA flow chart. |
The lead (SR) and senior author (LG) extracted data on study and participant characteristics, meta-analytic results, methodological quality, cultural adaptation, and potential moderators.
Results
We have summarized findings from existing meta-analyses and literature reviews of culturally adapted psychosocial interventions for mental health problems in tabular form (Table 1). Table 1 also presents specific elements of cultural adaptation that may moderate or mediate the effectiveness of such interventions for mental health problems.
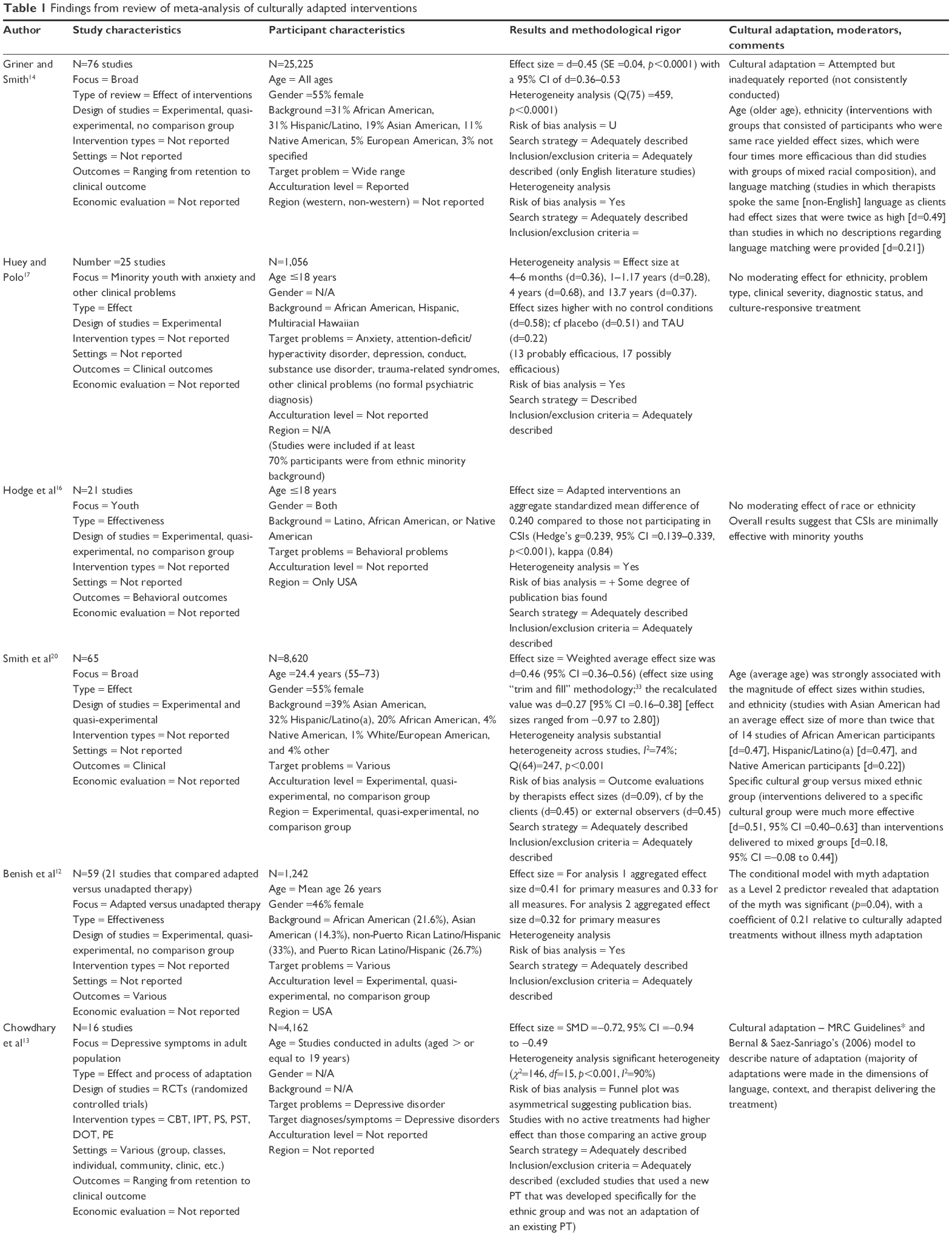 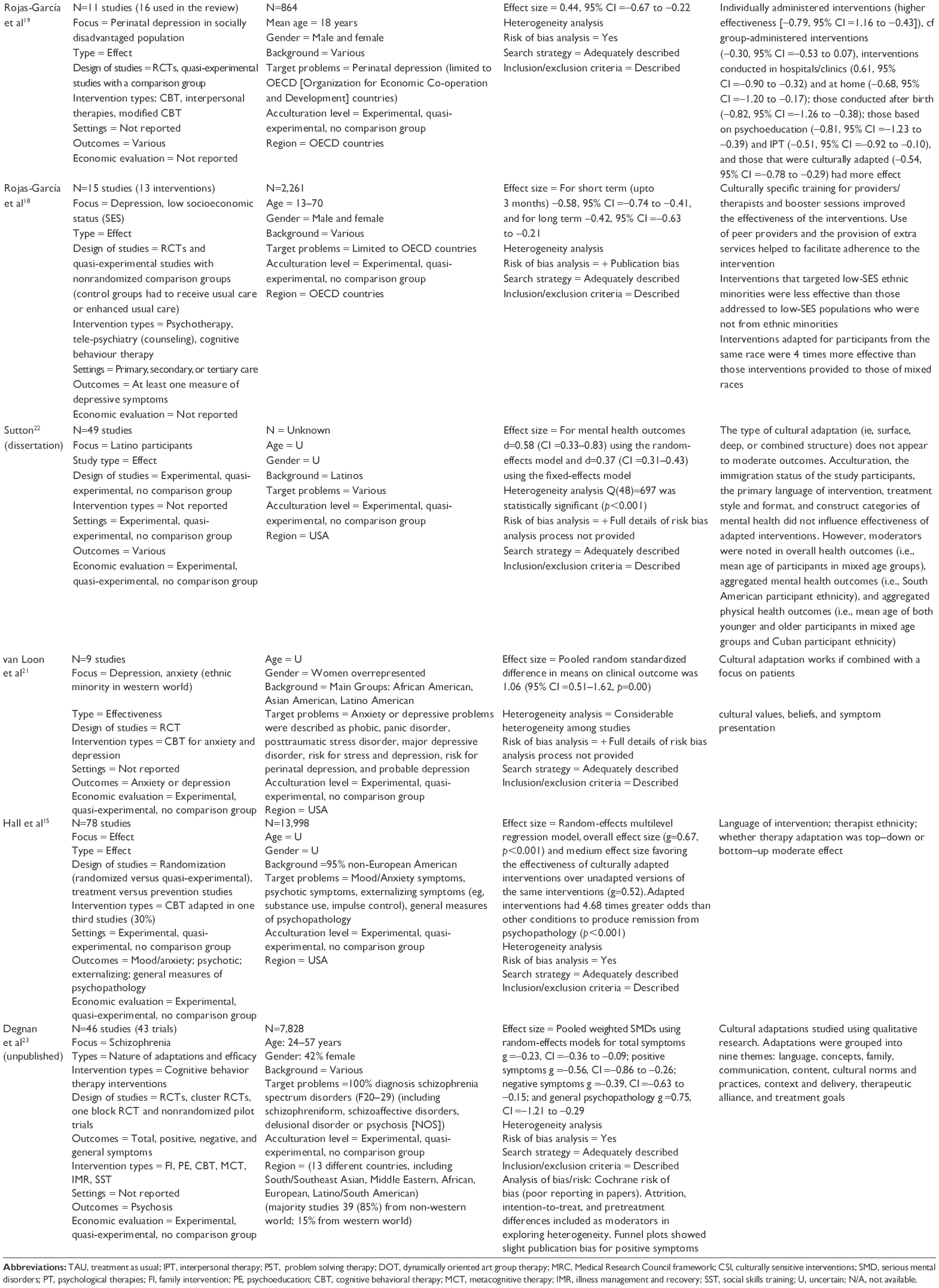 | Table 1 Findings from review of meta-analysis of culturally adapted interventions |
Due to methodological heterogeneity and nonindependence (with reviews including the same study samples), a narrative approach has been undertaken to synthesize the meta-analytic findings and discuss the nature and process of adaptation.
Characteristics of reviews
Our systematic search generated a total of 12 articles that met inclusion criteria. The overall approach in the studies of cultural adaptation appears to be western versus non-western cultures. These included 10 published reviews,12–21 one thesis,22 and one unpublished review (accepted for publication).23 We agreed that it would not be meaningful to calculate the total number of participants as a number of meta analyses looked at the same and previously published studies.
Most of the reviews focused on a variety of disorders and populations. One focused on schizophrenia23 while four focused on depressive symptoms.13,18,19,21 One review focused on a specific population, that is, Latinos,22 and another on Latino, African American, or Native American only,16 while the rest included studies of different ethnic and cultural groups. Two reviews focused on youth only (≤18 years).16,17 One review specifically focused on women – perinatal depression.19 Only one review compared adapted versus unadapted interventions.12 While most reviews attempted some description of cultural adaptation, only two of these described the nature and process in detail using a systematic approach.13,23 The latter two articles were also the only reviews that described and compared the different types of therapies adapted for culture. Two meta-analyses conducted by Rojas-Garcia et al18,19 focused on culturally adapted interventions for depressed persons from low socioeconomic status. Table 1 presents the study characteristics and results of each meta-analysis included in this review.
Effectiveness and quality of the reviews
The included reviews reported effect sizes ranging from 0.23 to 0.75, with the majority reporting moderate to large effect sizes. These are summarized in Table 1. Table 2 presents the quality assessment based on Assessment of Multiple SysTemAtic Reviews (AMSTAR) criteria.
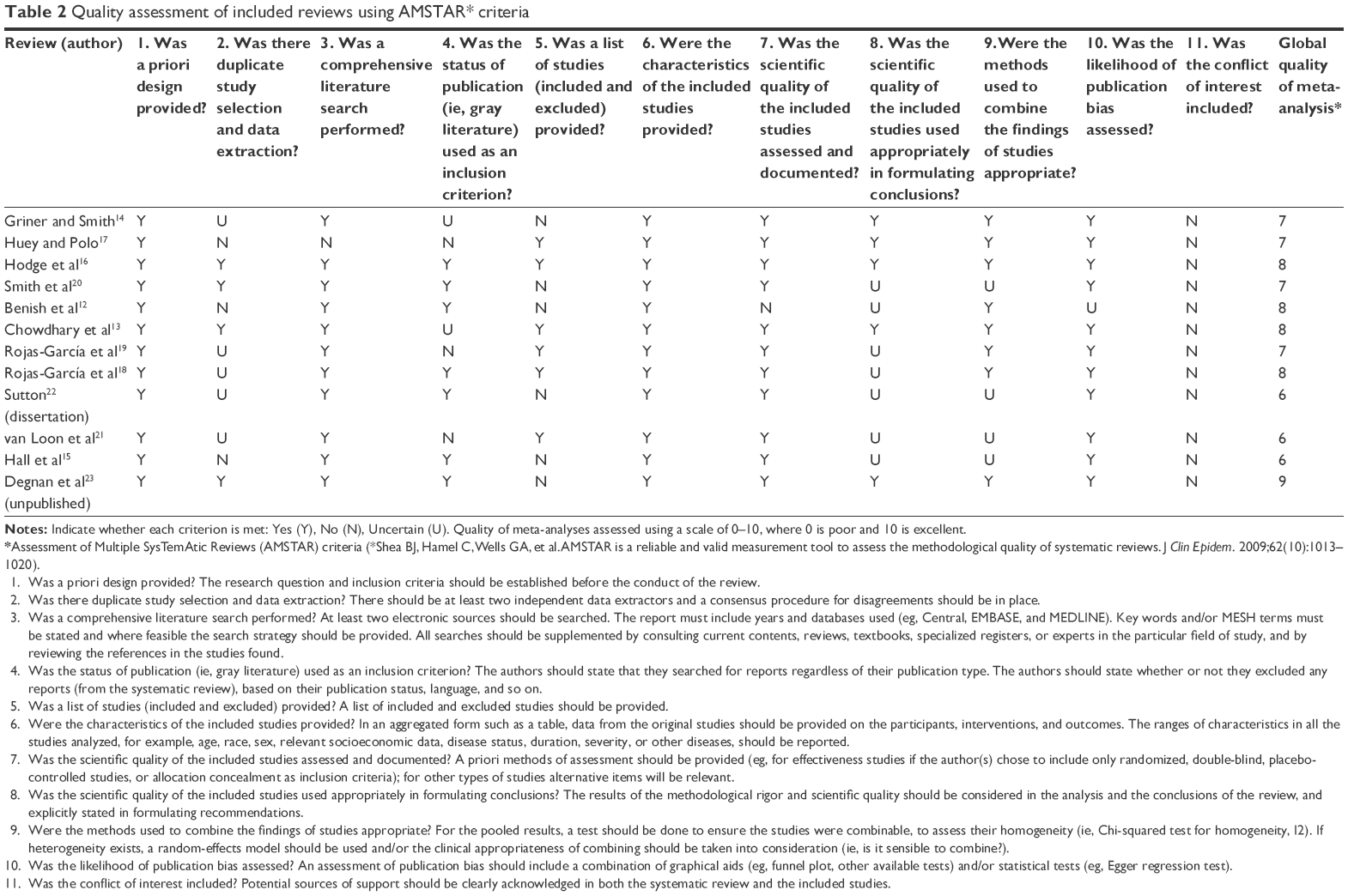 | Table 2 Quality assessment of included reviews using AMSTAR* criteria
|
Griner and Smith14 conducted the first meta-analysis of culturally adapted interventions and included the majority of retrieved studies as part of their strategy. The overinclusiveness was also a quality-limiting factor of the meta-analysis. The inclusion criteria were that the studies were written in English and provided quantitative data on evaluation of culturally adapted mental health interventions. The authors categorized cultural adaptation based on whether the treatments included components like explicit statement of culture, matched race or ethnicity between the client and the therapist, use of client’s preferred language, incorporation of cultural values and worldview into sessions, collaborated with cultural others, and localized services appropriately and included relevant discussion of spirituality.
Huey and Polo17 analyzed published randomized trials comparing active treatment with no treatment and placebo or treatment as usual control groups for ethnic minority youth. They described treatment efficacy as “well-established,” “probably efficacious,” and “possibly efficacious.” In their review, none of the studies met the criteria for well-established therapies, 13 studies were considered probably efficacious, and 17 as possibly efficacious. This meta-analysis was limited by the small number of studies with inconsistent quality.
Smith et al20 used quasi-experimental or experimental designs and included adaptations to aspects of content, format, or delivery. They excluded substance abuse treatments and prevention programs. The authors acknowledged limitations in the low number of studies, researcher allegiance to culturally adapted interventions, the heterogeneity, and lack of systematic measurement of adapted treatments.
Benish et al12 conducted a multilevel direct comparison meta-analysis of published and unpublished studies prior to 2010, in the English language, that contained quantitative data. They compared culturally adapted treatments to a heterogeneous control group and then conducted a meta-analysis comparing culturally adapted treatments to a bonafide evidence-based treatment. In the third part of their meta-analysis, they studied whether adapting the explanation of the mental illness symptoms to a person’s cultural belief (myth) produced better results. The authors recognized that very few studies in their analysis acknowledged the clients’ ecological context and the underreporting of implicit adaptations in the comparison groups.
Christina Sutton22 conducted a meta-analysis of studies that reported culturally adapted interventions in Latino populations in the USA. The author rationalized that Latino individuals have less access to mental health care resources although they are the largest and fastest-growing minority population, estimated to reach 132.8 million by 2015. There were limitations through the reliability of individual studies in terms of control groups, adaptations, and outcomes.
Hodge et al16 conducted a random-effects model meta-analysis of studies from the USA where research employed an intervention that incorporated a measurable and modifiable outcome and the intervention incorporated surface or deep structure strategies to determine the effectiveness of culturally sensitive interventions on health and behavioral outcomes. Quality issues were highlighted around the use of passive control groups in some of the studies.
Chowdhary et al13 conducted a review of adaptations of psychological therapies for depressive disorder to describe the process, extent, nature, and effectiveness in ethnic minority communities in western countries and for any populations in non-western countries. Incompleteness of information in some studies compromised quality.
Rojas-Garcia et al19 conducted a systematic review and meta-analysis of 16 articles assessing 15 interventions (psychotherapeutic) to decrease depressive symptoms in socially disadvantaged women with or at risk of perinatal depression. Adaptations consisted of providing information in languages other than the dominant one, adjusting the content of the interventions to the cultural background of the women, providing additional information, or increasing the accessibility to the intervention. The interventions were mainly provided in group settings.
Rojas-Garcia et al18 conducted another meta-analysis, for assessing both the short- (n=11) and long-term effectiveness (n=12) of interventions in depression. Strategies used to culturally adapt the interventions included adaptation of the content, training to providers in delivering the intervention in a culturally appropriate manner, use of peer providers, and the provision of extra services to facilitate adherence to the intervention.
Hall et al15 set out to reconcile the differences of the previous meta-analyses, and, therefore, used studies from each of the previous meta-analysis on cultural adaptations and new studies completed since the earlier meta-analyses to conduct a meta-analysis of 78 studies. They used a random-effects multilevel regression model, which accounts for nonindependence of effect size because of multiple effect sizes obtained from a single sample. van Loon et al21 focused on depression and anxiety in ethnic minority of the western world. They themselves commented that they had only identified a small number of US studies, so generalization of the findings to other western countries needed discussion.
Degnan et al23 recently conducted a systematic review of studies to examine the nature and effectiveness of culturally adapted psychosocial interventions in schizophrenia. To reduce heterogeneity, they adopted stringent inclusion criteria, including only controlled trials with 100% diagnosis of schizophrenia spectrum disorders (F20–29) (including schizophreniform, schizoaffective disorders, delusional disorder or psychosis [NOS]), and interventions targeting specific ethnic populations. Akin to Chowdhary et al,13 they were interested in interventions that were adapted for minority groups in western (Europe and USA) countries and majority groups in non-western countries.
Most of the meta-analyses reported limitations related to the included studies. For example, the inclusion of studies ranging from randomized controlled trials (RCTs) to observational or quasi-experimental research designs. The review authors highlighted limitations of individual trials including the lack of a systematic approach to cultural adaptation, limited description of the adaptation process, incomplete data, small sample sizes, and mixed diagnostic and ethnic samples. One review by Benish et al12 compared adapted with unadapted therapies, which is considered to be the “gold standard” design to test whether adapted interventions are more effective. Most studies used usual care control groups leading to lack of systematic measurement of adapted treatments. Again, most studies reported either a short-term follow-up or none at all.
Limitations of the reviews themselves included methodological heterogeneity, including studies with diverse designs and contexts (eg, intervention model, adaptation process, ethnic/cultural group, adapted for majority versus minority populations, type of control). Reviews often conducted meta-analyses on studies that focused on participants from a variety of ethnic background, with multiple problems who lived in different countries. Only one review reported outcomes in one ethnic group, that is, Latinos.22 Only two reviews13,23 reported different types of interventions in detail and grouped therapies from various theoretical backgrounds together. As mentioned, all except a few studies combined papers that used a variety of experimental designs. Similarly, studies with various control conditions were combined. At least some of these factors could be controlled for through sensitivity, subgroup, or moderator analyses. However, most of the meta-analyses did not report subgroup analyses. These methodological issues in part might explain a wide variety of conclusions and a wide range of effect sizes reported by these studies (ie, 0.23–0.75). The meta-analyses used a variety of methods to calculate the effect sizes (eg, aggregated mean, fixed-, and random-effect size models). As the literature is limited in this area, and the reviews were not very focused, it was not surprising that most meta-analyses included the same papers. Finally, none of the studies reported economic evaluations.
Most authors recognized a selection of studies published only in the English language. Authors highlighted the effect of risk biases, including publication bias, blinding of outcome assessors, and attrition bias. Publication bias was calculated in some studies, but its influence on effect size was not calculated. Other factors reported to influence the effect were the choice of control group and measurements by therapists versus self-reports and external observers.
Evaluation of nature and process of cultural adaption in reviews
The meta-analyses in this review used a variety of methods to assess the nature, process, and quality of cultural adaptation. For example, in their review of adapted interventions for mental health problems, Griner and Smith14 categorized cultural adaptation based on whether the treatments included components like explicit statement of culture; matched race or ethnicity between the client and therapist; use of client’s preferred language; incorporation of cultural values and worldview into sessions; collaborated with cultural others; localized services appropriately and included relevant discussion of spirituality. Chowdhary et al13 evaluated cultural adaptation using Medical Research Council framework and Bernal and Saez-Sanriago25 existing model and found that the majority of adaptations were made in the dimensions of language, context, and therapist delivering the treatment. In another meta-analysis of culturally adapted interventions for schizophrenia, the authors23 used qualitative methodology to evaluate the nature of cultural adaptations reported in the included studies. The authors thematically analyzed the adaptations to generate nine themes: language, concepts, family, communication, content, cultural norms and practices, context and delivery, therapeutic alliance, and treatment goals.
Cultural factors as moderators of effect of adapted interventions
Some of the meta-analyses attempted to look into the factors that predicted a larger effect of culturally adapted interventions. These include certain characteristics of the intervention, design, sample, and context that may have made a difference to effectiveness.
Rojas-Garcia et al19 reported that individually administered interventions (cf group-administered interventions), interventions conducted in hospitals/clinics and at home, those based on psychoeducation and interpersonal therapy, and those that were culturally adapted had more effect. Degnan et al23 reported little difference in symptomatic effect based on intervention type but that interventions were more effective when participants attended with relatives versus alone.
The review by Degnan et al23 found larger effect sizes for psychotic symptoms in RCTs with usual care control groups versus those with active controls. They also reported that studies with higher risk of bias (ie, open trials with unblinded outcome assessors, “as treated” analyses and high levels of attrition) had reduced effect sizes for symptomatic outcomes in schizophrenia compared to those studies with lower risk of bias.
Multiple studies14,20,22 found age as a predictor of the effect of culturally adapted interventions. Of these, two reviews14,20 specifically found older age to be a moderator of the effect of interventions. Other studies14,15 reported language match to influence the effectiveness of the interventions. Sutton22 failed to find the effect of language on effectiveness.
Most of the reviews14,15,18,22 that explored the effect of ethnicity as a moderator found it to be an influential factor. Interestingly, some of the reviews14,18,20 also found that culturally adapted interventions work better when they are provided to a homogenous group of participants than when provided to persons from mixed racial or cultural backgrounds. Rojas-Garcia et al18 also found that culturally adapted interventions were twice more effective with Asian Americans compared with other ethnic minority groups in the USA. Degnan et al23 reported interventions adapted for Chinese and majority populations to be less effective at reducing overall symptoms in schizophrenia than non-Chinese and minority populations.
Two meta-analyses12,21 have probed deeper into the nature of the adaptation and its effect on moderating intervention effects. Benish et al12 found that adaptation using illness myth had a strong moderating effect relative to culturally adapted treatments without illness myth adaptation. Similarly, van Loon et al21 discovered that cultural adaptation works better if combined with a focus on patients’ cultural values, beliefs, and symptom presentation. However, Sutton22 reported that the type of cultural adaptation (ie, surface, deep, or combined structure) does not appear to moderate outcomes.
Three reviews failed to find the moderating effect of any factors. Huey and Polo17 found no moderating effect for ethnicity, problem type, clinical severity, diagnostic status, and culture-responsive treatment. Similarly, Hodge et al16 found no moderating effect of race or ethnicity. Finally, Sutton22 reported that acculturation, the immigration status of the study participants, the primary language of intervention, treatment style and format, and construct categories of mental health did not influence the effectiveness of adapted interventions.
Discussion
This is the first review of meta-analyses of culturally adapted interventions. The majority of meta-analyses showed a moderate to large effect for culturally adapted interventions. However, we can only conclude that adapting interventions for culture is better than usual care because of limited studies including active controls and very few with nonadapted treatment arms. Moreover, caution is warranted in interpreting these results as most of these meta-analytic reviews lacked methodological rigor and were plagued with other problems, such as poor consideration of theoretical underpinning and cultural issues. The overall approach in the studies of cultural adaptation appears to be western versus non-western cultures, without realizing the diversity in the non-western cultures.
Although not all the studies focused on content and process of adaptation, the limited evidence13,23 suggests that majority of adaptations were made in the dimensions of language, context, concepts, family, communication, content, cultural norms and practices, context and delivery, therapeutic alliance, and treatment goals. Chowdhary et al13 evaluated cultural adaptation using the Medical Research Council framework24 and Bernal and Saez-Sanriago’s model25 to describe nature of adaptation, while Degnan et al23 used qualitative methodology to evaluate the nature of cultural adaptations. Degnan et al23 review used robust methodology to evaluate the process and components of adaptation. However, both studies extracted data from the RCTs that might have limited the identification of themes, as authors often did not report the adaptations or the adaptation process was described separately.7,9,26 This might have led to difficulty in building a comprehensive picture of the process of adaptation.
A review of the moderators in the studies confirmed different factors that were statistically significant in the different studies, for example, age, language, ethnicity, use of homogenous groups instead of mixed race groups, and a focus on illness myths and cultural values and beliefs. There were, however, studies that failed to confirm some of the moderators as described earlier. Again, many of the articles did not describe the complete details of the process of adaptation, and therefore, some moderators may have been missed.
A review of the studies highlighted a lack of standardized frameworks for cultural adaptation of interventions that have been universally accepted, evaluated, and applied routinely in research and practice. Therefore, the meta-analyses have been limited by the diverse criteria used to adapt interventions in the included studies, with each author group often developing their own criteria. Most adaptation frameworks have been developed in North America27–30 and Western Europe9 for immigrant populations, and therefore might not work for indigenous populations. The number of adaptation frameworks developed outside the western world is limited.7,26,31 Most of these frameworks are for general therapeutic principles, with few exceptions5,7,9,26 for cognitive therapy.
The way forward
There is a growing evidence base to suggest that culturally adapted interventions are effective. However, there are a number of recommendations for future work in the field. There needs to be further research into the process of adaptation to find out what works. There is also a need for further studies evaluating the effectiveness of adapted interventions when compared with nonadapted interventions as opposed to usual care.
Currently, there is no review on frameworks of adaptation, and there is a need for one. Such a review can assimilate data from existing literature and provide a common evidence-based framework that could guide clinicians and researchers in adapting different types of therapies. Future papers should provide detailed accounts of potential moderators of cultural adaptation on outcome that can be tested in future meta-analyses. The lessons learnt from this exercise will also provide criteria against which meta-analyses can evaluate the adaptation of interventions.
The authors suggest that in addition to following the basic rules of meta-analysis, future meta-analyses should focus on specific ethnic and diagnostic populations, with intervention types sub-analyzed, instead of combining participants from a variety of backgrounds and analyzing different types of interventions together regardless of their varied theoretical underpinning. The studies in this area should be conducted using robust RCT designs, preferably three-armed trials comparing the adapted intervention to usual care versus the unadapted intervention, with strict eligibility criteria to see whether adapting interventions is more effective for specific populations. Finally, there is a need for economic evaluation of interventions to convince policy makers of the need through a sound financial argument.
Conclusion
The present review suggests that there is value in cultural adaptation. Current evidence does not offer a solution to the issue of which components of cultural adaptation are effective, for what population, and whether cultural adaptation works better than noncultural adaption. Well-defined and standardized frameworks for adaptation are needed, and further research in testing the application of these frameworks to evaluate the effectiveness of adapted interventions is essential. There is also a need to further refine the criteria and process of RCTs and meta-analyses in this field.
Disclosure
SR, FN, NH have received grants to conduct research in cultural adaptations of interventions. The authors report no other conflicts of interest in this work.
References
Leung K, Lin Q, Chiu C. Psychological science of globalization. In: The Oxford Handbook of Multicultural Identity. Oxford, NY: Oxford University Press; 2014. (Oxford Library of Psychology). | ||
Rathod S, Kingdon D. Case for cultural adaptation of psychological interventions for mental healthcare in low and middle income countries. BMJ. 2014;349:g7636. | ||
Kirmayer LJ. Rethinking cultural competence. Transcult Psychiatry. 2012;49(2):149–164. | ||
Bhugra D. Setting up psychiatric services: cross-cultural issues in planning and delivery. Int J Soc Psychiatry. 1997;43(1):16–28. | ||
Helms JE. An examination of the evidence in culturally adapted evidence-based or empirically supported interventions. Transcult Psychiatry. 2015;52(2):174–197. | ||
Li ZJ, Guo ZH, Wang N, et al. Cognitive–behavioural therapy for patients with schizophrenia: a multicentre randomized controlled trial in Beijing, China. Psychol Med. 2015;45(9):1893–1905. | ||
Naeem F, Phiri P, Munshi T, et al. Using cognitive behaviour therapy with South Asian Muslims: findings from the culturally sensitive CBT project. Int Rev Psychiatry. 2015;27(3):233–246. | ||
Husain N, Afsar S, Ara J, et al. Brief psychological intervention after self-harm: randomised controlled trial from Pakistan. Br J Psychiatry. 2014;204(6):462–470. | ||
Rathod S, Kingdon D, Phiri P, Gobbi M. Developing culturally sensitive cognitive behaviour therapy for psychosis for ethnic minority patients by exploration and incorporation of service users’ and health professionals’ views and opinions. Behav Cogn Psychother. 2010;38(5):511–533. | ||
Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak. 2007;7:16. | ||
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. | ||
Benish SG, Quintana S, Wampold BE. Culturally adapted psychotherapy and the legitimacy of myth: a direct-comparison meta-analysis. J Couns Psychol. 2011;58(3):279–289. | ||
Chowdhary N, Jotheeswaran AT, Nadkarni A, et al. The methods and outcomes of cultural adaptations of psychological treatments for depressive disorders: a systematic review. Psychol Med. 2014;44(6):1131–1146. | ||
Griner D, Smith TB. Culturally adapted mental health intervention: a meta-analytic review. Psychotherapy (Chic). 2006;43(4):531–548. | ||
Hall GCN, Ibaraki AY, Huang ER, Marti CN, Stice E. A meta-analysis of cultural adaptations of psychological interventions. Behav Ther. 2016;47(6):993–1014. | ||
Hodge DR, Jackson KF, Vaughn MG. Culturally sensitive interventions and health and behavioral health youth outcomes: a meta-analytic review. Soc Work Health Care. 2010;49(5):401–423. | ||
Huey S Jr, Polo AJ. Evidence-based psychosocial treatments for ethnic minority youth. J Clin Child Adolesc Psychol. 2008;37(1):262–301. | ||
Rojas-García A, Ruiz-Perez I, Rodríguez-Barranco M, Gonçalves Bradley DC, Pastor-Moreno G, Ricci-Cabello I. Healthcare interventions for depression in low socioeconomic status populations: a systematic review and meta-analysis. Clin Psychol Rev. 2015;38:65–78. | ||
Rojas-García A, Ruíz-Pérez I, Gonçalves DC, Rodríguez-Barranco M, Ricci-Cabello I. Healthcare interventions for perinatal depression in socially disadvantaged women: a systematic review and meta-analysis. Clin Psychol Sci Pract. 2014;21(4):363–384. | ||
Smith TB, Rodríguez MD, Bernal G. Culture. J Clin Psychol. 2011;67(2):166–175. | ||
van Loon A, van Schaik A, Dekker J, Beekman A. Bridging the gap for ethnic minority adult outpatients with depression and anxiety disorders by culturally adapted treatments. J Affect Disord. 2013;147(1–3):9–16. | ||
Sutton C. Culturally adapted interventions for Latinos: a meta-analysis. School of Graduate Psychology [Internet]. Available from: http://commons.pacificu.edu/spp/1134. Accessed May 28, 2015. | ||
Degnan A, Baker S, Edge D, et al. The nature and efficacy of culturally-adapted psychosocial interventions for schizophrenia: a systematic review and meta-analysis. Psychol Med. 2017;1–14. | ||
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337:a1655. | ||
Bernal G, Sáez-Santiago E. Culturally centered psychosocial interventions. J Community Psychol. 2006;34(2):121–132. | ||
Naeem F, Habib N, Gul M, et al. A qualitative study to explore patients’, carers’ and health professionals’ views to culturally adapt CBT for psychosis (CBTp) in Pakistan. Behav Cogn Psychother. 2014;44(1):43–55. | ||
Bernal G, Jiménez-Chafey MI, Domenech Rodríguez MM. Cultural adaptation of treatments: a resource for considering culture in evidence-based practice. Prof Psychol Res Pract. 2009;40(4):361–368. | ||
Castro FG, Barrera M Jr, Holleran Steiker LK. Issues and challenges in the design of culturally adapted evidence-based interventions. Annu Rev Clin Psychol. 2010;6(1):213–239. | ||
Hwang WC. The psychotherapy adaptation and modification framework: application to Asian Americans. Am Psychol. 2006;61(7):702–715. | ||
Stirman SW, Miller CJ, Toder K, Calloway A. Development of a framework and coding system for modifications and adaptations of evidence-based interventions. Implement Sci. 2013;8:65. | ||
Naeem F, Ayub M, Gobbi M, Kingdon D. Development of Southampton Adaptation Framework for CBT (SAF-CBT): a framework for adaptation of CBT in non-western culture. J Pak Psych Soc. 2009;6(2):79–84. | ||
Moher D, Liberati A, Tetzlaff J, Altman DG. The PRISMAGroup (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMAStatement. PLoS Med. 6(7):e1000097. | ||
Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2): 455–463. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.