")
Back to Journals » Local and Regional Anesthesia » Volume 14
The Current Practice of Spinal Anesthesia in Anesthetists at a Comprehensive Specialized Hospital: A Single Center Observational Study
Authors Hunie M , Fenta E , Kibret S, Teshome D
Received 1 January 2021
Accepted for publication 17 March 2021
Published 31 March 2021 Volume 2021:14 Pages 51—56
DOI https://doi.org/10.2147/LRA.S300054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Stefan Wirz
Metages Hunie, Efrem Fenta, Simegnew Kibret, Diriba Teshome
Department of Anesthesia, School of Medicine, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia
Correspondence: Metages Hunie
Department of Anesthesia, School of Medicine, College of Health Sciences, Debre Tabor University, PO. Box 272, Debre Tabor, Ethiopia
Email [email protected]
Background: Spinal anesthesia block is the most widely practiced anesthesia technique due to its safety margin. It is an invasive procedure that could be associated with a variety of complications like total spinal, cardiovascular collapse, meningitis, paralysis, and even death. The aim of this study to assess the current practice of spinal anesthesia.
Methods: A Cross-sectional study design was conducted in Debre Tabor Comprehensive Specialized Hospital from November 01 to December 15, 2020. All anesthesia professionals who are working in the study Hospital were surveyed by the Purposive sampling technique. A standardized structured checklist prepared from recommendations of New York school of regional anesthesia guideline regarding the current Practice of spinal anesthesia was used to collect the data after taking written informed consent. Descriptive statistics were employed to summarize the results.
Results: A total of 24 anesthetists were observed of their practice before, during, and after administer of spinal anesthesia. All of the anesthetists were practicing the preparation and assembling of all necessary anesthesia equipments, resuscitation drugs, and basic monitors while all of the anesthetists did not wash their hands, wore a sterile gown, and draped the back of the patient with fenestrated drapes in a sterile fashion.
Conclusion: Most of the anesthesiology professionals in our setting have a good preparation of all necessary anesthesia equipments, and resuscitation drugs, while the assessment of patient’s emotional reaction and pain during injection, the skin preparation allowed to being dry and assessment of the degree of sensory and motor block of the patient were insufficient.
Keywords: spinal anesthesia, standards, Ethiopia
Introduction
Spinal anesthesia is a type of regional anesthesia in which a local anesthetic is injected directly into the cerebrospinal fluid that surrounds the spinal cord and nerve roots.1,2 It blocks pain from an entire region of the body, such as the hips, the belly, the pelvis, and the legs.2
Spinal anesthesia is part of the modern practice of anesthesia because of its proven success, predictability, increased patient satisfaction, low complication rate, better pain control than intravenous narcotics, earlier recovery of bowel function, less need for systemic Opioids, easier breathing resulting from better pain control, Easier participation in physical therapy.3,4
A spinal anesthetic is used for orthopedic surgery on joints or bones of the leg and is also commonly used for any surgery bellow the umbilicus like groin hernia repair, hemorrhoid surgery, hysterectomy, cesarean section, prostate surgery, genital surgery.5–9 Spinal anesthesia has indicated for surgery below the umbilicus but it has contraindication which ranges from absolute to relative. Patient refusal, infection at the site of injection, a true allergy to local anesthetic drugs, coagulopathy, and increased intracranial pressure are absolute while neurological disease, fixed cardiac output states, uncooperative, and aortic stenosis are the relative contraindications.5,10–13
A spinal anesthesia block is an invasive procedure that could be associated with a variety of complications.7,14–16
These complications could be classified as minor, moderate, and major. A minor complication includes nausea, vomiting, mild hypotension, shivering, and urinary retention. Postdural puncture headache and failed spinal blockade are classified as moderate complications, and vertebral canal hematoma, direct needle trauma, total spinal, cardiovascular collapse, meningitis, paralysis, and even death are the major complications.15,17–21
To minimize these complications National guidelines have been developed by the Joint Commission of different associations.22–25
Now a day experts are recommending spinal anesthesia over general anesthesia to have better patient outcome.26 They are recommending regional anesthesia as compared to general anesthesia during pandemic like the current crisis COVID-19.27 But, it is not without complications especially in a resource limited setting, when standards of performing regional anesthesia is not maintained throughout the procedure.28
The aim of this study to assess the current practice of spinal anesthesia at Debre Tabor Comprehensive specialized Hospital.
Methods
Study Design, Setting, and Period
This single center observational study was conducted in Debre Tabor Comprehensive Specialized Hospital which is found in the north-central part of Ethiopia. It is located in the Debub Gondar Zone of the Amhara Region of Ethiopia, about 100 kilometers northeast of Bahir Dar city and 50 kilometers east of Lake Tana, with a latitude and longitude of 11°51′N 38°1′E and an elevation of 2706 meters (8878 ft) above sea level.29 The Hospital has 6 operation tables and 24 anesthetists. It provides more than 2000 surgical cases annually. The study was conducted from November 01 to December 15, 2020. Our study was conducted in accordance with the Declaration of Helsinki.
Sampling Technique
We have employed a survey-based study so that all anesthetists who are available during the study period have been observed.
Study Population
All anesthesia professionals who are working in the operation theatres of Debre Tabor Comprehensive Specialized Hospital were observed.
Data Collection Technique
A standardized structured checklist regarding the current Practice of spinal anesthesia among anesthetists in the operation theater was used to collect the data. A checklist was prepared from recommendations of the New York school of regional anesthesia (NYSORA) guideline.25 After taking written informed consent, study participants were observed based on the checklist about their routine practice of spinal anesthesia.
Data Analysis
Data were checked manually for completeness and then coded by using SPSS version 23 computer program for analysis. Descriptive statistics (counts, and percentages) were employed to summarize the results.
Data Quality Control
The training was given to data collectors (to understand and to clarify ambiguity data collection tool if any); supervision was made throughout the data collection period. Consistency, and completeness of the collected data are also checked.
Results
A total of 24 (19 male and 5 female) anesthetists were observed of their practice before, during, and after administration of spinal anesthesia. From those standards of spinal anesthesia practice, all of the anesthetists did not wash their hands, wore a sterile gown, and draped the back of the patient with fenestrated drapes in a sterile fashion. All of the anesthetists were practicing the preparation and assembling of all necessary anesthesia equipment like Endotracheal tubes, laryngeal mask airways, Laryngoscopes, and monitoring before giving spinal anesthesia and including a wide bore intravenous cannula securing before administration spinal anesthesia achieved (Table 1).
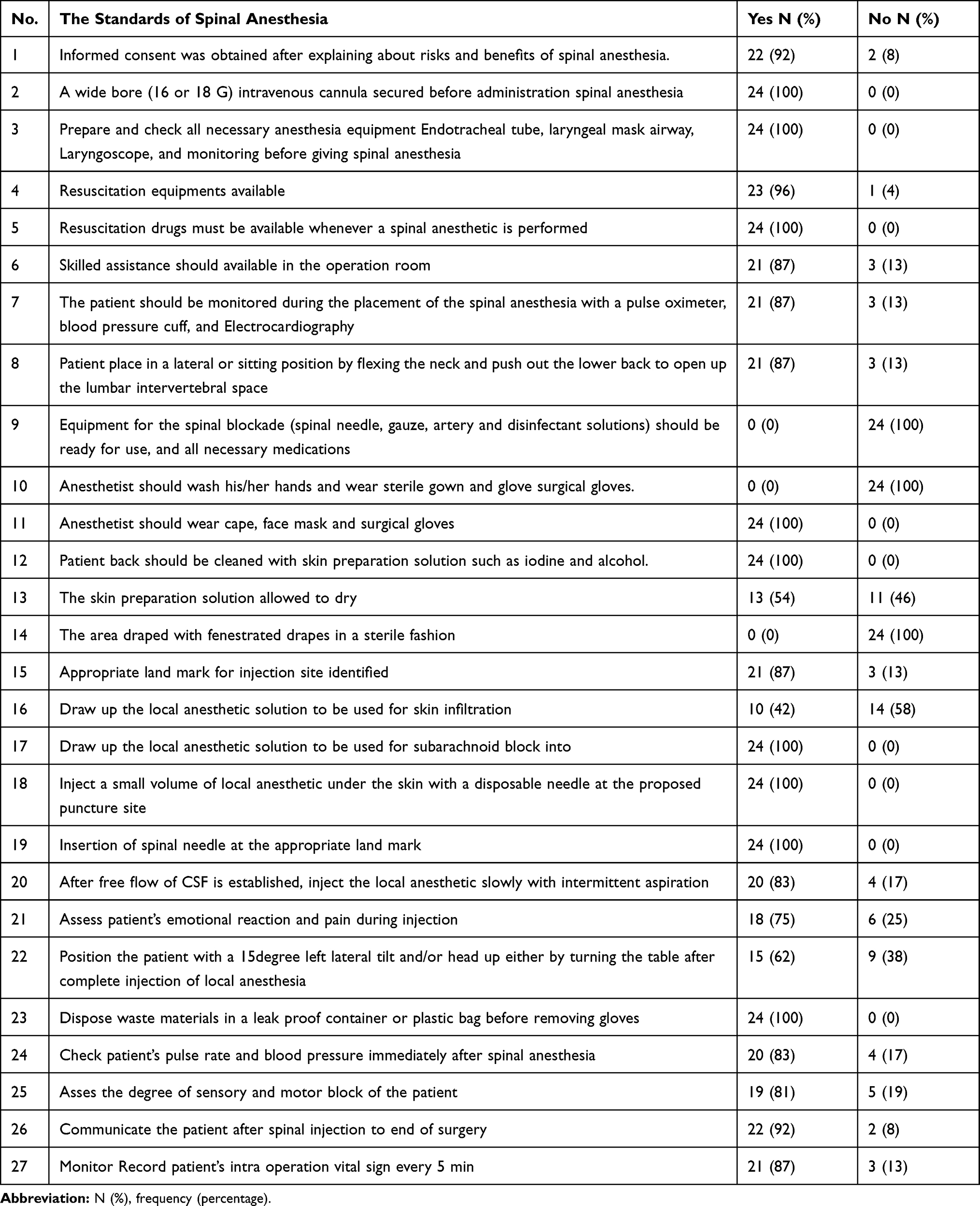 |
Table 1 The Current Practice of Spinal Anesthesia in Anesthetists at a Comprehensive Specialized Hospital |
Discussion
A spinal anesthesia block is a safe and effective form of anesthesia performed by anesthesiology professionals which can be used as an alternative to general anesthesia commonly in surgeries involving the lower extremities and surgeries below the umbilicus.30 If it is appropriately practiced it has associated with better pain relief immediately after surgery, reduced need for strong opioids, less nausea, and vomiting, earlier return to drinking and eating after surgery, less impact on the cardiovascular and respiratory system, less risk of chest infections.3,31,32
Complete spinal nerve block documentation is vital for the quality of patient care.33 Ensuring patient safety is a core component of our professional practice. While performing this spinal nerve block, it is vital to observe the practice before, during, and after administer spinal anesthesia to ensure patient safety and enhance a better outcome.34
In the current study a wide bore (16 or 18 G) intravenous cannula, all necessary anesthesia equipment like Endotracheal tubes, laryngeal mask airways, Laryngoscopes, application of basic monitors, resuscitation drugs, personnel protective equipments like wearing a cap, face mask, and surgical gloves, and patient back cleaning with skin solution such as iodine and alcohol to prevent infection was practiced 100%.
On the other hand, the assessment of patient’s emotional reaction and pain during injection, position the patient with a 15degree left lateral tilt and/or head up after complete injection of local anesthesia, skin preparation with solution allowed being dry and used skin infiltration in about 75%, 62% 54%, and 42% respectively.
Similarly, a study done at the University of Gondar by Ferede YA et al, 2020 found the assessment of patient’s emotional reaction and pain during injection, check patient’s pulse rate and blood pressure immediately after spinal anesthesia, and appropriate positioning of the patient was not completely practiced and they recommend for improvements.35
Another study conducted at the University of Gondar by Chekol W et al, 2018 found as all anesthetists did not wash their hands and wear sterile gowns throughout the procedure which is inline with our study.36
In conflicting with our finding’s various literature and clinical practice guidelines reported and recommended that while performing this spinal nerve block, it is vital to completely practice the standards of spinal anesthesia to ensure patient safety and enhance the better outcome.23,24,37
Conclusion
Most of the anesthesiology professionals in our setting have a good preparation of all necessary anesthesia equipments, and resuscitation drugs, while the assessment of patient’s emotional reaction and pain during injection, the skin preparation allowed to being dry and assessment of the degree of sensory and motor block of the patient were insufficient. The absence of local practice guideline, availability of spinal kits with drapes and anesthetists adherence to internationally available guidelines could be the barriers to perform safe spinal anesthesia for patients requiring it.
Ethics and Consent Statement
Ethical clearance was obtained from Debre Tabor University Ethical Review Committee. Written informed consent was secured from each study participant after the aim of the study is disclosed.
Acknowledgment
The authors acknowledge Debre Tabor University for their support with this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors reported no funding for this work.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Hood DD, Curry R. Spinal versus epidural anesthesia for cesarean section in severely preeclamptic patients a retrospective survey. Anesthesiology. 1999;90(5):1276–1282. doi:10.1097/00000542-199905000-00009
2. Riley ET, Cohen SE, Macario A, Desai JB, Ratner EF. Spinal versus epidural anesthesia for cesarean section: a comparison of time efficiency, costs, charges, and complications. Anesth Analg. 1995;80(4):709–712.
3. McLain RF, Kalfas I, Bell GR, Tetzlaff JE, Yoon HJ, Rana M. Comparison of spinal and general anesthesia in lumbar laminectomy surgery: a case-controlled analysis of 400 patients. J Neurosurg Spine. 2005;2(1):17–22. doi:10.3171/spi.2005.2.1.0017
4. Sinha R, Gurwara A, Gupta S. Laparoscopic surgery using spinal anesthesia. JSLS. 2008;12(2):133.
5. Kokki H. Spinal blocks. Paediatr Anaesth. 2012;22(1):56–64. doi:10.1111/j.1460-9592.2011.03693.x
6. Bors E, Comarr AE, Moulton SH. The role of nerve blocks in management of traumatic cord bladders: spinal anesthesia, subarachnoid alcohol injections, pudendal nerve anesthesia and vesical neck anesthesia. J Urol. 1950;63(4):653–666. doi:10.1016/S0022-5347(17)68810-4
7. Olawin AM, Das JM. Spinal anesthesia. StatPearls [Internet]. StatPearls Publishing; 2019.
8. Tuohy CEB. Costinuous spinal anesthesia: its usefitiisess and technic involved. Anesthesiology. 1944;5(2):142–148. doi:10.1097/00000542-194403000-00003
9. Obi VO, Umeora OUJ. Anesthesia for emergency cesarean section: a comparison of spinal versus general anesthesia on maternal and neonatal outcomes. Afr J Med Health Sci. 2018;17(1):31. doi:10.4103/ajmhs.ajmhs_33_18
10. Hodgson PS, Liu SS. New developments in spinal anesthesia. Anesthesiol Clin North Am. 2000;18(2):235–249. doi:10.1016/S0889-8537(05)70162-0
11. Mets B, Broccoli E, Brown AR. Is spinal anesthesia after failed epidural anesthesia contraindicated for cesarean section? Anesth Analg. 1993;77(3):629–631. doi:10.1213/00000539-199309000-00034
12. Kee WDN, Khaw KS, Tan PE, Ng FF, Karmakar MK. Placental transfer and fetal metabolic effects of phenylephrine and ephedrine during spinal anesthesia for cesarean delivery. Anesthesiology. 2009;111(3):506–512. doi:10.1097/ALN.0b013e3181b160a3
13. Heesen M, Klimek M, Hoeks SE, Rossaint R. Prevention of spinal anesthesia-induced hypotension during cesarean delivery by 5-hydroxytryptamine-3 receptor antagonists: a systematic review and meta-analysis and meta-regression. Anesth Analg. 2016;123(4):977–988. doi:10.1213/ANE.0000000000001511
14. Horlocker TT, Wedel DJ. Neurologic complications of spinal and epidural anesthesia. Reg Anesth Pain Med. 2000;25(1):83–98.
15. Horlocker TT. Complications of spinal and epidural anesthesia. Anesthesiol Clin North Am. 2000;18(2):461–485. doi:10.1016/S0889-8537(05)70172-3
16. Wedel DJ, Horlocker TT. Regional anesthesia in the febrile or infected patient. Reg Anesth Pain Med. 2006;31(4):324–333. doi:10.1016/j.rapm.2006.04.003
17. Tarkkila PJ, Kaukinen S. Complications during spinal anesthesia: a prospective study. Reg Anesth Pain Med. 1991;16(2):101–106.
18. Kilpatrick ME, Girgis NI. Meningitis—a complication of spinal anesthesia. Anesth Analg. 1983;62(5):513–515. doi:10.1213/00000539-198305000-00009
19. Kelsaka E, Sarihasan B, Baris S, Tur A. Subdural hematoma as a late complication of spinal anesthesia. J Neurosurg Anesthesiol. 2003;15(1):47–49. doi:10.1097/00008506-200301000-00008
20. Sonras SA, Komplikasyon GNB. Spinal subdural hematoma: a rare complication of spinal anesthesia: a case report. Turk Neurosurg. 2008;18(3):324–326.
21. Pugely AJ, Martin CT, Gao Y, Mendoza-Lattes S, Callaghan JJ. Differences in short-term complications between spinal and general anesthesia for primary total knee arthroplasty. J Bone Joint Surg. 2013;95(3):193–199. doi:10.2106/JBJS.K.01682
22. Midia M, Dao D. The utility of peripheral nerve blocks in interventional radiology. Am J Roentgenol. 2016;207(4):718–730. doi:10.2214/AJR.16.16643
23. Mulroy MF, Weller RS, Liguori GA. A checklist for performing regional nerve blocks. Reg Anesth Pain Med. 2014;39(3):195–199. doi:10.1097/AAP.0000000000000075
24. de Araújo Azi LMT, Fonseca NM, Linard LG. BSA 2020: regional anesthesia safety recommendations update. Braz J Anesthesiol. 2020.
25. Zundert ACaAv. Spinal anesthesia: NYSORA; 2020. Available from: https://www.nysora.com/techniques/neuraxial-and-perineuraxial-techniques/spinal-anesthesia/.
26. Memtsoudis SG, Cozowicz C, Bekeris J, et al. Anaesthetic care of patients undergoing primary hip and knee arthroplasty: consensus recommendations from the International Consensus on Anaesthesia-Related Outcomes after Surgery group (ICAROS) based on a systematic review and meta-analysis. Br J Anaesth. 2019;123(3):269–287. doi:10.1016/j.bja.2019.05.042
27. Singleton MN, Soffin EM. Daring discourse: are we ready to recommend neuraxial anesthesia and peripheral nerve blocks during the COVID-19 pandemic? A pro-con. Reg Anesth Pain Med. 2020;45(10):831–834. doi:10.1136/rapm-2020-101653
28. Neal JM, Barrington MJ, Brull R, et al. The second ASRA practice advisory on neurologic complications associated with regional anesthesia and pain medicine: executive summary 2015. Reg Anesth Pain Med. 2015;40(5):401–430. doi:10.1097/AAP.0000000000000286
29. Halefom A, Teshome A, Sisay E, Ahmad I. Dynamics of land use and land cover change using remote sensing and GIS: a case study of Debre Tabor Town, South Gondar, Ethiopia. J Geogr Inf Syst. 2018;10(02):165. doi:10.4236/jgis.2018.102008
30. Liu SS, McDonald SB. Current issues in spinal anesthesia. Anesthesiology. 2001;94(5):888–906. doi:10.1097/00000542-200105000-00030
31. Tetzlaff JE, Dilger JA, Kodsy M, Al-Bataineh J, Yoon HJ, Bell GR. Spinal anesthesia for elective lumbar spine surgery. J Clin Anesth. 1998;10(8):666–669. doi:10.1016/S0952-8180(98)00112-3
32. Bridenbaugh PO, Greene NM, Brull SJ. Spinal (subarachnoid) neural blockade. In: Cousins MJ, Bridenbaugh PO, editors. Neural Blockade in Clinical Anesthesia and Management of Pain. Third edition. Lippincott - Raven Publishers; 1998:203–242.
33. Mathioudakis A, Rousalova I, Gagnat AA, Saad N, Hardavella G. How to keep good clinical records. Breathe. 2016;12(4):369–373. doi:10.1183/20734735.018016
34. Moran PJ, Fennessy P, Johnson MZ. Establishing a new national standard for the documentation of regional anaesthesia in Ireland. BMJ Open Qual. 2017;6(2):e000210. doi:10.1136/bmjoq-2017-000210
35. Ferede YA, Nigatu YA, Agegnehu AF, Mustofa SY. Practice of spinal anesthesia among anesthetists in the operation room of referral hospital: cross-sectional study. Int J Surg Open. 2020;27:145–148. doi:10.1016/j.ijso.2020.11.002
36. Chekol W, Denu Z, Tawuye H. Audit on documentation completeness after regional nerve blocks at University of Gondar referral hospital, 2018. J Anesth Crit Open Access. 2018;10(6):208–211.
37. Hebl JR. The importance and implications of aseptic techniques during regional anesthesia. Reg Anesth Pain Med. 2006;31(4):311–323. doi:10.1016/j.rapm.2006.04.004
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.