")
Back to Journals » Drug Design, Development and Therapy » Volume 15
The Current Evidence for the Use of Safinamide for the Treatment of Parkinson’s Disease
Authors Abbruzzese G, Barone P, Lopiano L , Stocchi F
Received 8 April 2021
Accepted for publication 25 May 2021
Published 10 June 2021 Volume 2021:15 Pages 2507—2517
DOI https://doi.org/10.2147/DDDT.S302673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Giovanni Abbruzzese,1 Paolo Barone,2 Leonardo Lopiano,3 Fabrizio Stocchi4
1Department of Neuroscience, University of Genova, Genova, Italy; 2School of Medicine, University of Salerno, Salerno, Italy; 3Department of Neuroscience, University of Turin, AOU Città della Salute e della Scienza, Torino, Italy; 4Department of Neurology, University and Institute for Research and Medical Care, San Raffaele Roma, Rome, Italy
Correspondence: Fabrizio Stocchi
Department of Neurology, University and Institute for Research and Medical Care, San Raffaele Roma, Via della Pisana 235, Rome, 00163, Italy
Tel +390653352311
Fax +39066789158
Email [email protected]
Introduction: Parkinson’s therapeutic interventions are only symptomatic. An optimal treatment should therefore address the largest number of motor and non-motor symptoms, to manage patients at best. Safinamide is one of the most recent approved drugs for fluctuating patients, in add-on to levodopa, that remains the gold standard treatment. It has a unique mechanism of action, both dopaminergic (as MAO-B inhibitor) and glutamatergic (through Na+ channel blockade). Results from Phase III trials, post-hoc analyses and real-life experiences suggest a beneficial effect on motor (such as tremor, bradykinesia, rigidity and gait) and non-motor (pain, mood, sleep) symptoms.
Areas Covered: Here, the authors discuss clinical efficacy and safety of safinamide, identifying the patients’ profiles that could benefit most. A search in PubMed was performed in September 2020, with no time limits. Publications’ abstracts were reviewed.
Conclusion: Safinamide is peculiar due to its double mechanism of action. Its benefits in improving motor functions and fluctuations, and some non-motor symptoms, could have a valuable impact on patients’ quality of life (QoL), together with its safety profile.
Keywords: glutamate, motor fluctuations, Parkinson’s disease, safinamide
Introduction
Parkinson’s disease (PD) is the second neurodegenerative disorder for prevalence after Alzheimer’s disease, affecting 1–2% of the population over 60 years old and 3–5% of the population over 85 years old.1
The neurogenerative process underlying PD involves not only dopamine reduction, but also other non-dopaminergic neurotransmitters, such as acetylcholine, noradrenaline, serotonin, glutamate and adenosine.2 The dopamine loss induces the classical motor symptoms such as bradykinesia, rigidity and tremor but also some non-motor symptoms (NMS) (anxiety, depression, apathy). On the other end, other non-motor symptoms and complications seem to be related to other neurotransmitters impaired in PD.
In particular, glutamate overactivity in basal ganglia may participate in the development of dyskinesia and NMS such as pain, cognitive impairment and mood disorders.3,4 Decrease of serotonin activity has been described in depressed PD patients and decrease of acetylcholine in patients with cognitive impairment.5,6
Current therapeutic options are based on dopamine replacement to manage motor and non-motor symptoms, trying to avoid motor complications.
Levodopa (L-dopa) is the most effective drug and to date is considered as the “gold standard”.7
However, the positive motor response to levodopa gradually shortens over time (wearing-off) and dyskinesias increasingly compromise the so-called “ON Time”.7 Levodopa monotherapy is efficacious in controlling motor symptoms in early-stage patients, and may be optimized by adding dopamine agonists (DA) and other dopamine-potentiating agents such as monoamine oxidase inhibitors (MAOB-i), and catechol-O-methyl transferase (COMT) inhibitors1,4 to control motor complications which may emerge along with the progression of the disease. In addition to dopaminergic drugs, amantadine can be used to control dyskinesia.2
The therapeutic interventions differ about drug characteristics, mode of administration, safety, patients’ characteristics, and even if there are limited head-to-head comparisons, RCTs and clinical experience support different approaches to manage fluctuations.8 A comprehensive treatment of PD must also minimize the NMS negative impact on functionality and on patients’ quality of life.9
An approach to treat motor symptoms and non-levodopa-responsive symptoms is the use of non-dopaminergic drugs as add-on therapy2 to address the shortcomings of current dopamine-centered approaches.4
Safinamide is a compound with a dual mechanism of action recently approved for the treatment of fluctuations in PD patients. In this review, the pivotal trials and the study conducted with safinamide in a real-life setting are reported. Moreover, a profile of the best candidate for safinamide treatment is proposed.
Introduction to Safinamide
Chemistry and Pharmacodynamics
Safinamide [(S)-(+)-2-[4-(3-fluorobenzyloxy-benzylamino) propion-amide] belongs to the chemical class of α-aminoamides. It is a small molecule (molecular weight 302.34 g/mol), chemically and metabolically stable, water soluble, and acts through a dual mechanism of action: dopaminergic and non-dopaminergic.10,11
In particular, safinamide is a highly selective and fully reversible MAOB-i, determining an increase in extracellular levels of dopamine in the striatum.7 Its selectivity for MAOB is superior to selegiline and rasagiline.12
Moreover, it is associated with the concentration- and state-dependent blockade of voltage-gated Na+ channels, with consequent modulation of Ca2+ channels and inhibition of stimulated glutamate release.13,14 The dual mechanism of action of safinamide is, to date, a unique feature in the field of anti-Parkinson drugs. Its role in glutamate inhibition has recently been demonstrated in humans.15 This neurophysiological study showed that the dysfunction of circuits within M1 is restored by the anti-glutamatergic properties of safinamide 100 mg.
Pharmacokinetics and Metabolism
Safinamide absorption is rapid after single and multiple oral dosing, reaching Tmax in the time range 1.8–2.8 h after dosing under fasting conditions. Absolute bioavailability is high (95%), showing that safinamide is almost completely absorbed after oral administration and first pass metabolism is negligible.16
The volume of distribution (Vss) is approximately 165 L which is 2.5-fold of body volume, indicating extensive extravascular distribution of safinamide.11,16
In humans, safinamide is almost exclusively eliminated via metabolism (urinary excretion of unchanged safinamide was <10%). Substance-related radioactivity was largely excreted in urine (76%) and only to a low extent in faeces (1.5%) after 192 h.16
The elimination half-life of safinamide is 20–30 h. Steady-state is reached within one week. The pharmacokinetics of safinamide are linear after single and repeated doses. No time-dependency was observed.11,16
Clinical Efficacy
Safinamide proved to be efficacious in controlled clinical trials named 016–018, SETTLE, and a Japanese study.17–20
Study 01617 was a Phase III, multicenter, randomized, double-blind, placebo-controlled, parallel group trial with four phases: a 10-day screening period, a 4-week levodopa stabilization enrolled patients suffering from motor fluctuations. Patients with disabling peak dose or biphasic dyskinesias were excluded as well as patients with evidence of dementia, psychiatric complications or severe concomitant disease. The primary efficacy measure was change in mean daily on time with no or non-troublesome dyskinesias as detected by Hauser’s diaries. A number of other efficacy measures were also studied.
Six hundred and ninety-nine patients were randomized and equally divided into the three treatment groups; overall, 88% of enrolled subjects completed the study. At week 24 there were significant differences in the least squares (LS) mean change versus placebo in both the safinamide 50 mg/day and 100 mg/day groups. For off time, at week 24, LS mean differences versus placebo were significantly higher in both safinamide 50 mg/day and 100 mg/day groups. UPDRS III (motor) scores were significantly improved in both 50 and 100 mg/day groups compared to placebo. There were also significant improvements in CGI-C, CGI-S, and off time following the morning levodopa dose in both safinamide groups compared with placebo. There were no significant between-group differences in DRS scores during on time. Safinamide 100 mg/day improved UPDRS II (activities of daily living) scores compared to placebo (P=0.006: treatments were compared using an ANCOVA with baseline as a covariate and treatment and site as main effects); however, this was not noted for the 50 mg/day group. There were also improvements in PDQ-39 total score (P=0.0360; treatments were compared using an ANCOVA with baseline as a covariate and treatment and site as main effects) and subscale scores for emotional wellbeing (P=0.0116; treatments were compared using an ANCOVA with baseline as a covariate and treatment and site as main effects), communication (P=0.0361; treatments were compared using an ANCOVA with baseline as a covariate and treatment and site as main effects), and bodily discomfort (P=0.0159; treatments were compared using an ANCOVA with baseline as a covariate and treatment and site as main effects) for safinamide 100 mg/day versus placebo. Changes in GRID-HAM-D scores from baseline to week 24 were numerically greater for both safinamide groups versus placebo.17
Five hundred and forty-four patients who did not experience side effects, after completion of the core study, entered an 18-month double-blind, placebo-controlled parallel-group extension study (Study 018).18 Subjects that had discontinued from Study 016 but had completed efficacy evaluations at weeks 12 and 24 were also enrolled into this trial.
Interestingly, in this study the primary endpoint changed to mean change from baseline at Study 016 entrance in Dyskinesia Rating Scale (DRS) total score during on time while change in ON and OFF time were secondary.
Change in DRS was not significantly different in safinamide versus placebo groups, despite safinamide 50 and 100 mg/day being able to reduce mean DRS scores respectively by 31% and 27% from baseline compared with 3% observed in the placebo group. The mean total daily ON time without troublesome dyskinesia significantly improved from baseline at Study 016 to week 78 in Study 018 in both safinamide 50 and 100 mg/day groups (P=0.0031 and P=0.0002 respectively: treatments were compared with placebo using an ANCOVA with the model containing baseline, treatment and pooled center).
However, a post-hoc analysis conducted on patients with DRS baseline scores >4 showed a statistic significant improvement of dyskinesia in patients taking safinamide 100 mg versus baseline. The result was not achieved with 50 mg16 (Figure 1).
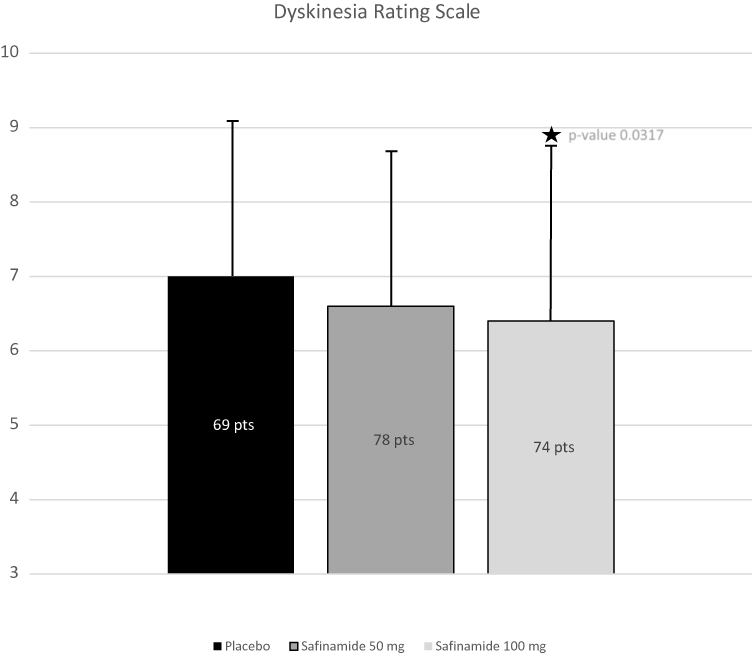 |
Figure 1 Study 018: safinamide reduced DRS scores in patients with baseline scores >4 (post-hoc analysis). |
Significant improvements were also reported in off time, on time without dyskinesia, CGI-S, CGI-C (for safinamide 50 mg/day), UPDRS part II, III and IV total scores, PDQ 39 and GRID-HAMD-D (safinamide 100 mg/day only). Overall, benefits observed during Study 016 in both groups treated with safinamide remained stable throughout the extension study; during the same period, the mean dose of levodopa increased in the placebo and the safinamide 50 mg group but decreased in the safinamide 100 mg group from 579.6±310.0 mg to 556.0±381.9 mg.18
The SETTLE study19 was a 6-month (24-week), randomized, double-blind, placebo-controlled international Phase III trial. It enrolled 549 fluctuating parkinsonian patients treated with optimized, stable doses of levodopa plus any other antiparkinsonian drug but MAOBI. The primary endpoint of the trial was the change in daily “ON” time, as assessed by the patient-completed daily diary cards (18 h/day). In this study, all the patients were administered safinamide 100 mg/day after two initial weeks with 50 mg/day. The SETTLE study confirmed the results of the 016 trial. In fact, safinamide significantly improved ON time (without worsening troublesome dyskinesia), OFF time, UPDRS III, CGI-S, CGI-C, PDQ-39 and OFF time following the first morning levodopa dose (ie, latency to ON) compared to placebo.
Hattori et al20 randomized 406 patients in 71 centers in Japan. The primary endpoint was mean daily ON time: changes from placebo were 1.39 h for the safinamide 50 mg/day group (p=0.0002; mixed model for repeated measures) and 1.66 h for safinamide 100 mg/day arm (p<0.0001; mixed model for repeated measures). Mean daily OFF time was significantly reduced in both arms compared to placebo (p=0.0003 and p<0.0001 respectively; mixed model for repeated measures). Even UPDRS II in OFF (p<0.0002 for both dosages; mixed model for repeated measures) and UPDRS III in ON were significantly improved in both arms (p<0.0001 for both dosages; mixed model for repeated measures).
In a recent review by MDS,21 016 and SETTLE were evaluated17,19 leading to the conclusion that safinamide is efficacious and clinically useful, without safety concerns.
Add on to Dopamine Agonist
Safinamide has been studied also as an add on to dopamine agonist monotherapy. Two study has been conducted. The 015 study22 was a double-blind controlled trial where safinamide 100 and 200 mg/day were added to a stable dose of dopamine agonist. The study demonstrated a significant improvement of the UPDRS III total score, UPDRS part II and CGI-C in the safinamide 100 mg group; the percentage of responders was higher in both safinamide groups compared to placebo. In this study, the dose of 200 mg failed to reach significance. The MOTION study23 was a 6-month (24-week), randomized, double-blind, placebo-controlled trial to evaluate the efficacy and safety of two fixed doses of SAF (50 and 100 mg/day). This trial enrolled patients with early idiopathic PD (less than five years of disease) treated with a single dopamine agonist. Six hundred and seventy-nine patients were randomized to receive safinamide 50 mg once daily, 100 mg, or placebo. Six hundred and seven patients completed the 24-week treatment period. Safinamide 100 mg/day significantly improved UPDRS III (mean change), and PDQ-39 compared to placebo. There was borderline significant improvement in ADL for the 100 mg/day, as well as UPDRS III (responders) for the 50 mg/day group.
Safinamide is not approved to be used in early patients or as an add-on therapy to dopamine agonist monotherapy, limiting its use in this population. Muller24 underlined that this is an important aspect; in fact, safety and tolerability of a MAO-B inhibitor, such as safinamide, is easier than therapy with dopamine agonists and could help to spare dopamine agonists and levodopa.
Post-hoc analyses of pooled data confirmed improvement in motor symptoms by UPRDS III and in cardinal symptoms with 100 mg/day.25
Safinamide has also shown to be effective in improving ON and OFF time in addition to levodopa alone or with any combination of antiparkinsonian therapies.25
Even UPDRS II score showed a significant reduction for safinamide 100 mg/day compared to placebo (p=0.0068; ANCOVA models with treatment and study as fixed effects and baseline value as continuous covariate), and quality of life (PDQ-39) improved significantly more with 100 mg/day in 352 patients treated for 2 years (-p=0.039; ANCOVA models with treatment and study as fixed effects and baseline value as continuous covariate).26
Post-hoc analysis of RCTs have shown that, without modifying the levodopa dose, 75% of patients on safinamide 100 mg/day showed “no deterioration” or an “improvement” of dyskinesias after 2 years of treatment, measured through the DRS score.27
Other post-hoc studies suggested it could act also on some non-motor symptoms (such as mood and pain) possibly because of its double mechanism of action.10,28–30 In more than 200 patients, safinamide 100 mg/day, compared to placebo, significantly improved the PDQ-39 “Emotional well-being” domain after 6 months (p=0.0067; ANCOVA models with treatment group and center as fixed dummy test and baseline values as continuous covariate) and 2 years (p=0.0006; ANCOVA models with treatment group and center as fixed dummy test and baseline values as continuous covariate) as well as the GRID-HAMD (p=0.048 and p=0.0027 respectively; ANCOVA models with treatment group and center as fixed dummy test and baseline values as continuous covariate). Significantly fewer patients in safinamide vs placebo group experienced depression as adverse event (p=0.0444 after 6 months and p=0.0057 after 2 years; two-sided Fisher’s exact test).29 Pain was measured indirectly through PDQ-39 items 37 and 39 after 6 months of safinamide 100 mg/day (p=0.0009 and p=0.006 respectively; ANCOVA model with PDQ-39 scores changes from baseline as dependent variable, with treatment and studies as fixed effects and with baseline values as covariate)28 and 24 months (p=0.0074 and p=0.0209 respectively; ANCOVA model with PDQ-39 scores changes from baseline as dependent variable, with treatment and studies as fixed effects and with baseline values as covariate) and through reduction of concomitant pain treatments (−26.2%; p=0.005; negative binomial regression model obtained with a Generalized Linear Model parameterized with logarithmic link function and negative binomial distribution and with treatment and studies as fixed effects).30 In a systematic review and meta-analysis on pain therapies in PD,31 the authors conclude that safinamide is the most effective among the therapies analyzed (cannabinoids, opioids, COMT inhibitors, Chinese medicine, surgery, pardoprunox and dopamine agonists, as well complementary therapies).
Data from RCT and post-hoc studies have been confirmed in real life experiences. A number of non-controlled open-label studies have been published reporting clinical experience with safinamide.32–35 The data reported are generally positive and are in line with the RCT trials. In particular, patients reported an improvement at CGI scale but also positive results were found using UPDRS evaluations and clinical diaries.
Interestingly, some small studies focused on non-motor symptoms. Geroin et al36 found a significant decrease in Kings Pain Scale, Brief Pain Inventory Intensity and Interference, and NRS scores from baseline (p<0.05: paired samples t-test) in 13 fluctuating patients being treated with safinamide 100 mg/day for 12 weeks.
A real-life experience on safinamide and sleep disorders was reported by Liguori et al.37 They examined 46 and 15 patients, treated with safinamide or rasagiline respectively, showing statistically significant improvement, from baseline, of nighttime sleep, daytime sleepiness and sleep daily dysfunction only with safinamide (p<0.05: Wilcoxon test).
Bianchi et al38 retrospectively evaluated 20 patients with PD complicated by motor fluctuations. These patients were administered safinamide 50 mg/day for 15 days, increased then to 100 mg/day for 3 months (no changes in other therapies). The total score of NMS scale significantly decreased from baseline (p=0.00031: non-parametric Friedman test). In particular, the reduction was significant in the cardiovascular, attention/memory, sleep/fatigue, mood/cognition, urinary, and sexual function domains (p<0.05 for all: non-parametric Friedman test).
Rinaldi et al39 enrolled 32 fluctuating PD patients, to assess the therapeutic potentials of safinamide (100 mg/day) on cognitive symptoms. Subjects received safinamide 50 mg/day for 2 weeks, then 100 mg/day for a further 10 weeks. Add-on with high-dose safinamide was accompanied by a significant increase of the Frontal Assessment Battery score and significant reduction of the “interference-time” score at the Stroop Word–Color Test (p<0.0001: paired t-test and Bonferroni correction for multiple comparisons). In particular, attention and inhibition of cognitive interference were significantly ameliorated by high-dose safinamide, suggesting increased modulatory performances of prefrontal cortical pathways. Findings on inhibitory control were opposite to those obtained with rasagiline,40 and this may depend on safinamide glutamatergic inhibition.
Safety and Tolerability
In RCT the percentages of patients in the safinamide groups, affected by adverse events, were similar to those observed in the placebo group,41 particularly for the dose of 100 mg/day (Table 1). The complete list of side effects is reported in Table 2.
 |
Table 1 Principal Safety Results of Safinamide from Clinical Trials 016, 018 and SETTLE |
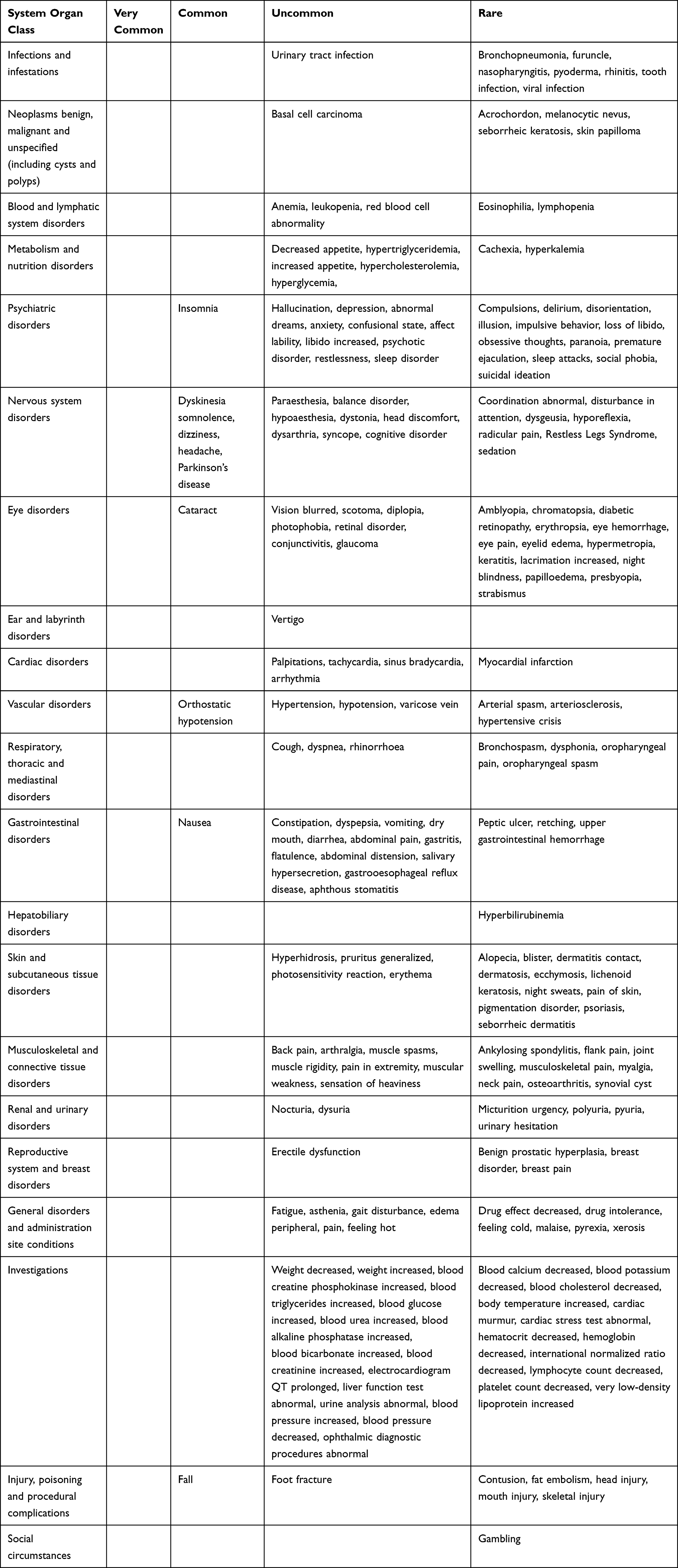 |
Table 2 Adverse Reactions Observed in Clinical Trials Where Adverse Events Were Considered Related |
Distinctive elements regarding the safety of safinamide are the following:
• Safinamide is a reversible MAO-B inhibitor (selegiline and rasagiline are irreversible);42,43 therefore, an adverse event attributable to safinamide regresses rapidly after stopping the drug. Within 5 days from withdrawal, there is a full recovery of enzyme activity,10 which allows to perform surgery under general anesthesia without the risk of strengthening the depressive effects of anesthetics on CNS;
• Safinamide is a powerful and highly selective MAO-B inhibitor. In human brain it is 1000-fold more selective for MAO-B than for MAO-A, avoiding the need for any food restriction;7,44
• Given the characteristics above, administration of antidepressants is possible, if administered at minimum doses needed;16
• In vitro metabolism studies indicated that there is no significant induction or inhibition
of cytochrome P450 in humans;16
• The lower safinamide dosage is permitted in moderate hepatic impairment, unlike other MAOB-i;16
• Pooled analyses of adverse events data from placebo-controlled studies in patients with PD indicate that concomitant administration of safinamide with a broad category of commonly used medicines in this patient population (antihypertensives, beta-blockers, proton pump inhibitors, non-steroidal anti-inflammatory drugs, antidepressants etc) is not associated with an increase in risk for adverse events;16
• Safinamide can be associated with any other antiparkinsonian drug. The best drug association is levodopa alone;25
• The use of safinamide in patients with albinism, retinal degeneration, uveitis, inherited retinopathy or severe progressive diabetic retinopathy is contraindicated.16 Preclinical studies with safinamide have shown induction of retinal degeneration in rats, as happened with other anti-Parkinson drugs (pramipexole) which, unlike safinamide, also require regular ophthalmologic controls.45 However, none of these drugs has been associated with retinal degeneration in humans.
A recent real-life experience46 evaluated frail patients (>60 years old with other chronic comorbidities for which they were being treated since at least 2 years). Over 47 patients treated with safinamide, 68% was still in treatment after 1 year. Efficacy and safety in older people were also confirmed in another retrospective study with 53 patients,47 improving WOQ-19 in 60% of them after 6 months of treatment, with a withdrawal in only 11% of cases.
Stocchi et al48 evaluated safety and tolerability of an overnight switch from rasagiline to safinamide (50 mg/day for 2 weeks, then 100 mg/day) in 20 consecutive PD fluctuating patients, through blood pressure (BP) monitoring with 24-h Holter recording. Patients were followed for 6 weeks. The study showed that BP did not increase by ≥10 mmHg and no serotonin-related symptoms were observed during the study. The overnight switch was safe and well tolerated by the patients.
Regulatory Affairs
Safinamide is indicated in the EU since 2015 for the treatment of adult patients with idiopathic PD as add-on therapy to a stable dose of levodopa alone or in combination with other anti-PD drugs in mid to late stage fluctuating patients.16
Treatment with safinamide should be started at a dose of 50 mg/day, that may be increased to 100 mg/day based on individual clinical need.16 The response to treatment already occurs at 219 or 4 weeks.17,18
Conclusion and Clinical Use Suggestions
Fluctuation in motor and non-motor symptoms remains one of the most important challenges in the treatment of Parkinson’s disease. Recent clinical trials showed that levodopa response and fluctuations can be improved adding other drugs to levodopa. Indeed, the administration of DA-agonist, COMTI, MAOBI and adenosine receptor antagonists together with levodopa was shown to improve motor and non-motor function even when one drug was administered on top of all the others. Therefore, the ability to combine drugs with different mechanism of action is fundamental for a successful treatment of PD.
The peculiarity of safinamide is the dual mechanism of action, modulating both dopaminergic and glutamatergic systems and it is the only available reversible MAOBI.
Safinamide 50 and 100 mg demonstrated efficacy in the treatment of motor fluctuations and motor symptoms in RCTs. Interestingly the effect of safinamide was maintained stable for 2 years in a double-blind situation (Study 016–018). Moreover, post-hoc analysis indicate that safinamide may improve other motor complications (dyskinesia), and some non-motor symptoms (pain, mood), and this was associated with a good tolerability profile.
Taking into account the characteristics of the drug and the results of the studies, we can make some practical considerations.
Best Patient’s Profile
A patient showing wearing OFF for the first-time taking levodopa monotherapy or in combination with a DA agonist is the best candidate for safinamide. In these patients, fluctuations can be improved maintaining levodopa dose and frequency unchanged.
Dyskinesia
Cumulative evidence supports the idea that hyperactivity of striatal projection neurons (SPNs), which express DA D1 or D2 receptors, has a prominent role in the abnormal responses to DA replacement leading to the development of dyskinesia in PD patients. A key driver of this overactivity is represented by a dysregulated neurotransmission mediated by glutamate which is released from cortical and thalamic terminals in the striatum and evokes excitatory synaptic events in SPNs.49,50 Safinamide through use-dependent sodium channel blockade reduces overactive glutamatergic transmission in basal ganglia, which play an important role in the development of dyskinesia. Sciaccaluga et al demonstrated that in experimental animals, safinamide was able to delay the onset of dyskinesia but not their severity once induced.49 Gardoni et al reached a similar conclusion.50 They investigated the effects of safinamide on the development of dyskinesia in 6-hydroxydopamine (6-OHDA)-lesioned rats and they found that the drug did not halt or delay the priming to levodopa, which underlies the development of dyskinesia, in the rat. However, safinamide did not worsen dyskinesia severity. Consistent with its antiglutamatergic activity, safinamide inhibited different parameters of corticostriatal glutamatergic transmission, an effect that might correlate with its antiakinetic activity. Overall, the experiment suggests that the striatal Glu-modulating component of safinamide’s activity may contribute to its clinical effects of improving motor function and increasing “on” time without troublesome dyskinesia.18,19
In human, safinamide cannot be considered an anti-dyskinetic drug as it does not have any acute effect on dyskinesias. However, at the dosage of 100 mg/day and administered over the long term, safinamide can improve dyskinesias.27
Regarding dyskinesias, two different kinds of patients could benefit from safinamide administration:
- Those starting treatment without having experienced any dyskinesias.
- Those starting treatment with pre-existing mild dyskinesias.
In the first case, it is suggested to begin with safinamide 50 mg/day and modulate dopaminergic therapy, decreasing the total load, due to the dopaminergic effect of safinamide.7 The increase of safinamide to 100 mg/day can be postponed when motor functions deteriorate, due to PD progression or in case of dyskinesias development.
In the second case, two approaches are suggested contemporaneously:
- Begin with safinamide 50 mg/day16 and increase rapidly to 100 mg/day (even after 2 weeks). The increase to safinamide 100 mg/day will allow to exploit at most the non-dopaminergic mechanism of action. We learned from clinical practice that the effects may take about 3–6 months to be detectable.
- Reduce levodopa/dopaminergic drug dose.
Dose
The results from RCT showed that the effect of 50 and 100 mg/day of safinamide are similar looking at improvement in time ON and OFF. However, safinamide 100 mg/day only showed a significative improvement in UPDRS part II, UPDRS part IV and quality of life (PDQ39). Therefore, it can be argued that the non-dopaminergic effect of the drug is better expressed when it is administered at the dose of 100 mg and at this dose the drug is different from the other MAOBI.
Switch
In case motor complications are not well controlled, non-motor symptoms such as pain or depression are present or dyskinesia are disabling, the switch from another MAOBI to safinamide could be considered. Open-label real life studies reported an improvement after switching from rasagiline to safinamide.32–34 This switch could result in an improvement in motor function and even in non-motor symptoms.32–34
In this case, it is better to increase the dose up to 100 mg/day, that has been shown to produce the greatest benefits in different scales/symptoms (UPDRS II-III-IV, PDQ-39, ADL, pain and mood), also in the long term.17–19,25–30
In case the switch is a possible therapeutic option, the best way to do it should be considered. If for any reason physicians want to switch from one MAOB-i to another, patients should remain without MAOB-is for 2 weeks before starting the other, as advised in the leaflets of both drugs.16,43
However, this indication results in a major inconvenience for PD patients because of the worsening of their clinical condition. On the other hand, the main concern when switching between MAOIs are the occurrence of hypertensive crisis and serotonin syndrome (SS).51 To investigate the possible risk of switching overnight from rasagiline to safinamide, Stocchi et al performed a safety study. In this study the possible occurrence of SS was strictly monitored. Each patient participating in the trial was monitored at site for 6 h after the administration of safinamide 50 mg and then at home blood pressure was recorded with a 24-h Holter recording (ABPM). No cases of serotonin syndrome were reported during the study. The ABPM study revealed a trend toward an increase of all parameters evaluated, which was not significant, and it was way below the 10-mmHg interval set as a primary endpoint. Similarly, blood pressure variability remained unchanged.48
Non-Motor Symptoms
The therapeutic effect of safinamide, observed at the lower dose of 50 mg/day and reinforced at 100 mg/day, on some non-motor symptoms (such as pain, sleep disorders, mood), linked or independent from motor fluctuations, is of particular interest.
Further investigations on its effect on NMS are still needed.
Safety
Safinamide has an optimum tolerability profile,43 confirming the conclusions contained in the recent review from Movement Disorder Society,19 which indicates safinamide as an efficacious drug and useful in clinical practice, without safety problems.
Safinamide dosing is relatively simple, with a low risk of drug–drug interactions, little need for dose adjustment and no need for dietary tyramine restrictions, even in older patients.37,38
Safinamide, in clinical practice, confirms good results obtained in clinical trials and post-hoc.
Disclosure
Prof. Dr Paolo Barone reports grants from Zambon, during the conduct of the study. Prof. Dr Fabrizio Stocchi reports personal fees from Zambon pharma, outside the submitted work. The authors report no other potential conflicts of interest for this work.
References
1. Kalia LV, Lang AE. Parkinson’s disease. Lancet. 2015;386(9996):896–912. doi:10.1016/S0140-6736(14)61393-3
2. Fox S. Non-dopaminergic treatments for motor control in parkinson’s disease. Drugs. 2013;73(13):1405–1415. doi:10.1007/s40265-013-0105-4
3. Jenner P, Caccia C. The role of glutamate in the healthy brain and in the pathophysiology of parkinson’s disease. Eur Neurol Rev. 2019;14(Suppl. 2):2–12.
4. Calabresi P, Kulisevsky J. Safinamide as add-on therapy – moving beyond dopamine for a multifaceted approach in parkinson’s disease. Eur Neurol Rev. 2017;12(Suppl. 5):2–6.
5. Politis M, Niccolini F. Serotonin in parkinson’s disease. Behav Brain Res. 2015;277:136–145. doi:10.1016/j.bbr.2014.07.037
6. O’Callaghan C, Lewis SJG. Cognition in parkinson’s disease. Int Rev Neurobiol. 2017;133:557–583. doi:10.1016/bs.irn.2017.05.002
7. Olanow CW, Stocchi F. Safinamide – a new therapeutic option to address motor symptoms and motor complications in mid-to-late-stage parkinson’s disease. Eur Neurol Rev. 2016;11(Suppl. 2):2–15.
8. Fabbri M, Rosa MM, Ferreira JJ. Adjunctive therapies in parkinson’s disease: how to choose the best treatment strategy approach. Drugs Aging. 2018;35(12):1041–1054. doi:10.1007/s40266-018-0599-2
9. Opara JA, Brola W, Leonardi M, et al. Quality of life in Parkinson’s disease. J Med Life. 2012;5(4):375–381.
10. Blair HA, Dhillon S. Safinamide: a review in parkinson’s disease. CNS Drugs. 2017;31(2):169–176. doi:10.1007/s40263-017-0408-1
11. Wasan H, Singh D, Reeta KH. Safinamide in neurological disorders and beyond: evidence from preclinical and clinical studies. Brain Res Bull. 2021;168:165–177. doi:10.1016/j.brainresbull.2020.12.018
12. Alborghetti M, Nicoletti F. Different generations of type-B monoamine oxidase inhibitors in parkinson’s disease: from bench to bedside. Curr Neuropharmacol. 2018;16:1–13. doi:10.2174/1570159X1601171214093100
13. Kulisevsky J. Emerging role of safinamide in parkinson’s disease therapy. Eur Neurol Rev. 2014;9(2):108–112. doi:10.17925/ENR.2014.09.02.108
14. Reichmann H, Barone P, Poewe W. Progression of parkinson’s disease and unmet needs in mid- to late-stage patients. Eur Neurol Rev. 2015;10:182–188. doi:10.17925/ENR.2015.10.02.182
15. Guerra A, Suppa A, D’Onofrio V, et al. Abnormal cortical facilitation and L-dopa-induced dyskinesia in parkinson’s disease. Brain Stimul. 2019;12(6):1517–1525. doi:10.1016/j.brs.2019.06.012
16. Xadago® - summary of product characteristics, approved by EMA on 24/02/15. Summary of product characteristics. Available from: https://www.medicines.org.uk/emc/product/2159/smpc.
17. Borgohain R, Szasz J, Stanzione P, et al. Randomized trial of safinamide add-on to levodopa in parkinson’s disease with motor fluctuations. Mov Disord. 2014;29(2):229–237. doi:10.1002/mds.25751
18. Borgohain R, Szasz J, Stanzione P, et al. Two-year, randomized, controlled study of safinamide as add-on to levodopa in mid to late parkinson’s disease. Mov Disord. 2014;29(10):1273–1280. doi:10.1002/mds.25961
19. Schapira AHV, Fox S, Hauser RA, et al. Assessment of safety and efficacy of safinamide as a levodopa adjunct in patients with parkinson disease and motor fluctuations. JAMA Neurol. 2017;74(2):216–224. doi:10.1001/jamaneurol.2016.4467
20. Hattori N, Tsuboi Y, Yamamoto A, Sasagawa Y, Nomoto M. Efficacy and safety of safinamide as an add-on therapy to L-DOPA for patients with parkinson’s disease: a randomized, double-blind, placebo-controlled, phase II/III study. Park Rel Dis. 2020;75:17–23. doi:10.1016/j.parkreldis.2020.04.012
21. Fox SH, Katzenschlager R, Lim S-Y, et al. International parkinson and movement disorder society evidence-based medicine review: update on treatments for the motor symptoms of parkinson’s disease. Mov Dis. 2018;33(8):1248–1266. doi:10.1002/mds.27372
22. Stocchi F, Borgohain R, Onofrj M, et al. A randomized, double-blind, placebo-controlled trial of safinamide as add-on therapy in early parkinson’s disease patients. Mov Dis. 2012;27:106–112. doi:10.1002/mds.23954
23. Dézsi L, Vécsei L. Safinamide for the treatment of parkinson’s disease. Expert Opin Investig Drugs. 2014;23:729–742. doi:10.1517/13543784.2014.897694
24. Muller T. Safinamide in the treatment of parkinson’s disease. Neurodegener Dis Manag. 2020;10:195–204. doi:10.2217/nmt-2020-0017
25. Cattaneo C, Sardina M, Bonizzoni E. Safinamide as add on therapy to levodopa in mid- to late-stage parkinson’s disease fluctuating patients. Post hoc analyses of studies 016 and SETTLE. Parkinsons Dis. 2016;6(1):165–173. doi:10.3233/JPD-150700
26. Cattaneo C, Jost WH, Bonizzoni E. Long-term efficacy of safinamide on symptoms severity and quality of life in fluctuating parkinson’s disease patients. J Park Dis. 2020;10:89–97.
27. Cattaneo C, La Ferla R, Bonizzoni E, et al. Long-term effects of safinamide on dyskinesia in mid- to late-stage parkinson’s disease: a post-hoc analysis. J Parkinsons Dis. 2015;5(3):475–481. doi:10.3233/JPD-150569
28. Cattaneo C, Barone P, Bonizzoni E, et al. Effects of safinamide on pain in fluctuating parkinson’s disease patients: a post-hoc analysis. J Parkinsons Dis. 2017;7(1):95–101. doi:10.3233/JPD-160911
29. Cattaneo C, Muller T, Bonizzoni E, Lazzeri G, Kottakis I, Keywood C. Long-term effects of safinamide on mood fluctuations in parkinson’s disease. J Parkinsons Dis. 2017;7(4):629–634. doi:10.3233/JPD-171143
30. Cattaneo C, Kulisevsky J, Tubazio V, et al. Long-term efficacy of safinamide on parkinson’s disease chronic pain. Adv Ther. 2018;35(4):515–522. doi:10.1007/s12325-018-0687-z
31. Qureshi AR, Rana AQ, Malik SH, et al. Comprehensive examination of therapies for pain in parkinson’s disease: a systematic review and meta-analysis. Neuroepidemiology. 2018;51(3–4):190–206. doi:10.1159/000492221
32. Mancini F, Di Fonzo A, Lazzeri G, et al. Real life evaluation of safinamide effectiveness in parkinson’s disease. Neurol Sci. 2018;39(4):733–739. doi:10.1007/s10072-018-3272-y
33. Pagonabarraga J, Kulisevsky J. Safinamide from daily clinical practice: first clinical steps. Rev Neurol. 2017;65(10):433–438.
34. Martí-Andrés G, Jiménez-Bolaños R, Arbelo-González JM, et al. Safinamide in clinical practice: a Spanish Multicenter Cohort Study. Brain Sci. 2019;9:272. doi:10.3390/brainsci9100272
35. Tsuboi Y, Hattori N, Yamamoto A, Sasagawa Y, Nomoto M. Long-term safety and efficacy of safinamide as add-on therapy in levodopa-treated Japanese patients with parkinson’s disease with wearing-off: results of an open-label study. J Neurol Sci. 2020;416:117012. doi:10.1016/j.jns.2020.117012
36. Geroin C, Di Vico IA, Squintani GM, Segatti A, Bovi T, Tinazzi M. Effects of safinamide on pain in parkinson’s disease with motor fluctuations: an exploratory study. J Neural Transm. 2020;127(8):1143–1152. doi:10.1007/s00702-020-02218-7
37. Liguori C, Stefani A, Ruffini R, et al. Safinamide effect on sleep disturbances and daytime sleepiness in motor fluctuating Parkinson’s disease patients: a validated questionnaires-controlled study. Parkinsonism Relat Disord. 2018;57:80–81. doi:10.1016/j.parkreldis.2018.06.033
38. Bianchi MLE, Riboldazzi G, Mauri M, Versino M. Efficacy of safinamide on non-motor symptoms in a cohort of patients affected by idiopatic parkinson’s disease. Neurol Sci. 2019;40:275–279. doi:10.1007/s10072-018-3628-3
39. Rinaldi D, Sforza M, Assogna F, et al. Safinamide improves executive functions in fluctuating parkinson’s disease patients: an exploratory study. J Neural Transm. 2020. doi:10.1007/s00702-020-02259-y
40. Rinaldi D, Assogna F, Sforza M, et al. Rasagiline for dysexecutive symptoms during wearing-off in parkinson’s disease: a pilot study. Neurol Sci. 2018;39(1):141–143. doi:10.1007/s10072-017-3123-2
41. EPAR Xadago. Available from: http://www.ema.europa.eu/ema/index.jsp?curl=/pages/medicines/human/medicines/002396/human_med_001847.jsp.
42. Jumex®. Summary of product characteristics.
43. Azilect® summary of product characteristics. Available from: https://www.medicines.org.uk/emc/product/74/smpc.
44. Caccia C, Maj R, Calabresi M, et al. Safinamide: from molecular targets to a new anti-parkinson drug. Neurology. 2006;67(7Suppl. 2):S18–S23.44. doi:10.1212/WNL.67.7_suppl_2.S18
45. Mirapexin® 2008. Summary of product characteristics.
46. Lo Monaco MR, Petracca M, Vetrano DL, et al. Safinamide as an adjunct therapy in older patients with parkinson’s disease: a retrospective study. Aging Clin Exp Res. 2020;32:1369–1373. doi:10.1007/s40520-020-01469-4
47. Rinaldi D, Bianchini E, Sforza M, et al. The tolerability, safety and efficacy of safinamide in elderly parkinson’s disease patients: a retrospective study. Aging Clin Exp Res. 2020. doi:10.1007/s40520-020-01648-3
48. Stocchi F, Vacca L, Grassini P. Overnight switch from rasagiline to safinamide in Parkinson’s disease patients with motor fluctuations: a tolerability and safety study. Eur J Neurol. 2021;28(1):349–354. doi:10.1111/ene.14552
49. Sciaccaluga M, Mazzocchetti P, Bastioli G, et al. Effects of safinamide on the glutamatergic striatal network in experimental parkinson’s disease. Neuropharmacology. 2020;170:108024. doi:10.1016/j.neuropharm.2020.108024
50. Gardoni F, Morari M, Kulisevsky J, et al. Safinamide modulates striatal glutamatergic signaling in a rat model of levodopa-induced dyskinesia. J Pharmacol Exp Ther. 2018;367(3):442–451. doi:10.1124/jpet.118.251645
51. Francescangeli J, Karamchandani K, Powell M, Bonavia A. The serotonin syndrome: from molecular mechanisms to clinical practice. Int J Mol Sci. 2019;20(9):2288. doi:10.3390/ijms20092288
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.