")
Back to Journals » Infection and Drug Resistance » Volume 13
The Coronavirus Disease 2019 (COVID-19) in Children: A Study in an Iranian Children’s Referral Hospital
Authors Mahmoudi S, Mehdizadeh M, Shervin Badv R, Navaeian A, Pourakbari B, Rostamyan M, Sharifzadeh Ekbatani M, Eshaghi H , Abdolsalehi MR, Alimadadi H, Movahedi Z, Mamishi S
Received 20 April 2020
Accepted for publication 16 July 2020
Published 31 July 2020 Volume 2020:13 Pages 2649—2655
DOI https://doi.org/10.2147/IDR.S259064
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Shima Mahmoudi,1 Mehrzad Mehdizadeh,2,3 Reza Shervin Badv,3 Amene Navaeian,4 Babak Pourakbari,1 Maryam Rostamyan,4 Meisam Sharifzadeh Ekbatani,3 Hamid Eshaghi,4 Mohammad Reza Abdolsalehi,4 Hosein Alimadadi,5 Zahra Movahedi,6 Setareh Mamishi1,4
1Tehran University of Medical Sciences, Tehran, Iran; 2School of Medicine, Tehran University of Medical Sciences, Tehran, Iran; 3Pediatrics Center of Excellence, Children’s Medical Center, Tehran University of Medical Sciences, Tehran, Iran; 4Department of Infectious Diseases, Pediatrics Center of Excellence, Children’s Medical Center, Tehran University of Medical Sciences, Tehran, Iran; 5Tehran University of Medical Sciences, Tehran, Iran; 6Department of Pediatric Infectious Disease, Faculty of Medicine, Qom University of Medical Sciences, Qom, Iran
Correspondence: Setareh Mamishi Department of Infectious Diseases
Pediatrics Center of Excellence, Children’s Medical Center Hospital, Keshavarz Boulevard, Tehran, Iran
Tel/ Fax +98- 21- 6642- 8996
Email [email protected]
Background: Despite the worldwide spread of the coronavirus disease 2019 (COVID-19), the epidemiological and clinical patterns of the COVID-19 infection remain largely unclear, particularly among children. In this study, we explored the epidemiological characteristics, clinical patterns, and laboratory and imaging findings of pediatric patients with COVID-19.
Materials and Methods: From March 7 to March 30, 2020, there were a total of 35 patients who had confirmed COVID-19 infection by laboratory virus nucleic acid test (RT-PCR) assay with throat swab samples or typical chest CT manifestation compatible with COVID-19, in addition to a history of close contact with suspected or confirmed SARS‐CoV‐2 in family members. Information recorded included demographic data, medical history, exposure history, underlying comorbidities, symptoms, signs, laboratory findings and radiologic assessments, severity of disease, treatment, and mortality.
Results: The median age of the patients was 7.5 years (IQR=4– 11; range=4 months to 15 years). A total of 63% were male. Cough was present in 80% of the patients, followed by fever (77%), nausea or vomiting (29%), diarrhea (26%), shortness of breath (29%), headache (20%), and myalgia (14%). Lymphopenia was present in 43% of the patients, thrombocytopenia in 9%, neutopenia in 8%, and leucopenia in 26%. We reported severe pneumonia in 40% of the hospitalized patients and 18 (51%) had underlying diseases. Of 35 patients, 11 had positive RT-PCR results (31%). The chest CT images of 24 patients (69%) suggested COVID-19, while their RT-PCR assays from throat swab samples were negative.
Conclusion: This study demonstrates different clinical findings of pediatrics compared to the previous reports of children. Since a high rate of false negative RT-PCR test was observed, early detection of children with COVID-19 infection by CT is conducive to reasonable management and early treatment.
Keywords: COVID-19, children, severe pneumonia, Iran
Introduction
The epidemic started in late December 2019 in Wuhan and swept across China and has spread through the world rapidly. According to the daily report of the World Health Organization, the epidemic of coronavirus disease 2019 (COVID-19) so far registered 7553182 cases and 423,349 deaths through the world. More than 182,545 cases of COVID-19 and 8659 deaths in Iran have been reported as of June 13, 2020.1 Genetic analyses of novel coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), showed that SARS-CoV-2 viruses evolved into two major types of L and S. Although L type newly evolved from the ancient S type, the L type (~70%) is more prevalent and aggressive than the S type (70% vs 30%) and transmits or replicates faster in human populations.2
Despite the worldwide spread, the epidemiological and clinical patterns of the COVID-19 remain largely unclear, particularly among children.3 Pediatric patients with COVID-19 have their own clinical features and therapeutic responses.4 However, in contrast to adult patients, clinical manifestations of children with COVID-19 infection might be less severe.3
Children might be less likely to become infected or, if infected, may show milder symptoms.5,6 It is suggested that children were less sensitive to COVID-19 due to several factors including the lower maturity and binding ability of Angiotensin converting enzyme II (ACE2), which is known as a cell receptor for SARS-CoV-2. In addition, higher levels of antibody against respiratory infection viruses including respiratory syncytial virus and different immune responses to pathogens than adults might be another possible explanation.3 However, the mechanisms for the differences in clinical manifestations between children and adults are unclear.
Although the diagnosis of COVID-19 must be confirmed by reverse transcription polymerase chain reaction (RT-PCR), a total positive rate of RT-PCR for throat swab samples was about 30% to 60% at initial presentation. On the other hand, radiological characteristics can provide important evidence for the clinical diagnosis of COVID-19 and chest computed tomography (CT) might reveal pulmonary abnormalities consistent with COVID-19 even in patients with initial negative RT-PCR results.7,9
In the absence of specific therapeutic drugs or vaccines for COVID-19, early detection of children with SARS‐CoV‐2 infection is essential to decrease the risk of infecting a larger population. Sine clinical and imaging features of pediatric patients with COVID‐19 infection in Iran are limited, in this study, we explored the epidemiological characteristics, clinical patterns, and laboratory and imaging findings of pediatric patients with COVID-19. The aim of this study was to investigate the consistency of chest CT in comparison to RT-PCR assay in COVID-19 in children.
Materials and Methods
This study was approved by the Ethics Committee of Tehran University of Medical Sciences, Tehran, Iran (IR.TUMS.VCR.REC.1399.060) and signed informed consent was obtained from all patients who participated in the study or their parents/legal guardians. In cases that did not have the legal capacity or maturity to provide informed consent, their parents/legal guardians provided informed consent for themselves.
This study was performed in the Children’s Medical Center, the hub of excellence in pediatrics in Iran. Approximately, more than 35,000 outpatients and 2500 inpatients are admitted to our hospital monthly. From March 7 to March 30, 2020, a total of 35 patients were included in the study. The inclusion criteria were a patient who had a confirmed COVID-19 infection by laboratory virus nucleic acid test (RT-PCR assay) with throat swab samples or typical chest CT manifestation compatible with COVID-19 in addition to a history of close contact with suspected or confirmed SARS‐CoV‐2 in family members. If both radiologic assessments and RT-PCR test were not performed for a patient, they were excluded from the study.
Information recorded included demographic data, medical history, exposure history, underlying comorbidities, symptoms, signs, laboratory findings and radiologic assessments, severity of disease, treatment, and mortality.
The presence of SARS‐CoV‐2 was detected by the RT-PCR method, as previously described10 using nucleocapsid protein (N) 5′‐GACCCCAAAATCAGCGAA AT‐3′ (F) and 5′‐ TCTGGTTACTGCCAGTTGAATCTG‐3′ (R) primers, and 5′‐FAM‐ACCCCGCAT TACGTTTGGTGGACC‐3′ probe. Each sample was run duplicated with positive and negative controls. Throat swab samples were collected into a collection tube with 150 μL of virus preservation solution for extracting SARS‐CoV‐2 RNA from patients suspected of having SARS‐CoV‐2 infection. The RT-PCR assay was performed under the following conditions: at 50°C for 15 minutes and 95°C for 5 minutes, 40 cycles at 94°C for 15 seconds and at 55°C for 45 seconds. A cycle threshold value (Ct-value) of less than 37 was defined as a positive test result, and a Ct-value of 40 or more was defined as a negative result. Radiologic assessments including chest radiography or CT scan were performed, and all laboratory testing was performed according to the clinical care needs of the patient. Laboratory assessments consisted of a complete blood count, blood chemical analysis, coagulation testing, assessment of liver and renal function, and measures of electrolytes, C-reactive protein (CRP), procalcitonin, lactate dehydrogenase, creatine kinase, and erythrocyte sedimentation rate (ESR).
Severe pneumonia was defined by the presence of any of the following conditions:
- Hypoxia: SpO2≤93% (<90% in premature infants).
- Increased respiration rate: RR≥70/min (≤1 year), RR≥50/min (>1 year).
- Blood gas analysis: PaO2<60 mmHg, PaCO2>50 mmHg.
- Other manifestations.11
The CT features were evaluated as follows: ground‐glass opacities, consolidations, nodules, pleural effusion, lymphadenopathy, unilateral or bilateral, number of affected lobes, and opacity distribution. The analysis of chest radiographic findings was based on density (ground‐glass and consolidations), central to peripheral distribution, and lung involvements.
Statistical Analysis
All statistical analyses were performed using SPSS (Statistical Package for the Social Sciences) version 13.0 software (SPSS Inc). Categorical variables were described as frequency rates and percentages, and continuous variables were described using median and interquartile range (IQR) values. Normally distributed continuous variables were presented as means with standard deviations (SD). Comparison of the differences between the two groups was conducted using the t-test or Chi-square test. Variables with a two-tailed P-value<0.05 were considered statistically significant.
Results
The demographic and clinical characteristics of the patients are shown in Table 1. The median age of the patients was 7.5 years (IQR=4–11; range=4 months to 15 years). No differences by gender were observed, but there were more males in the study overall (63%).
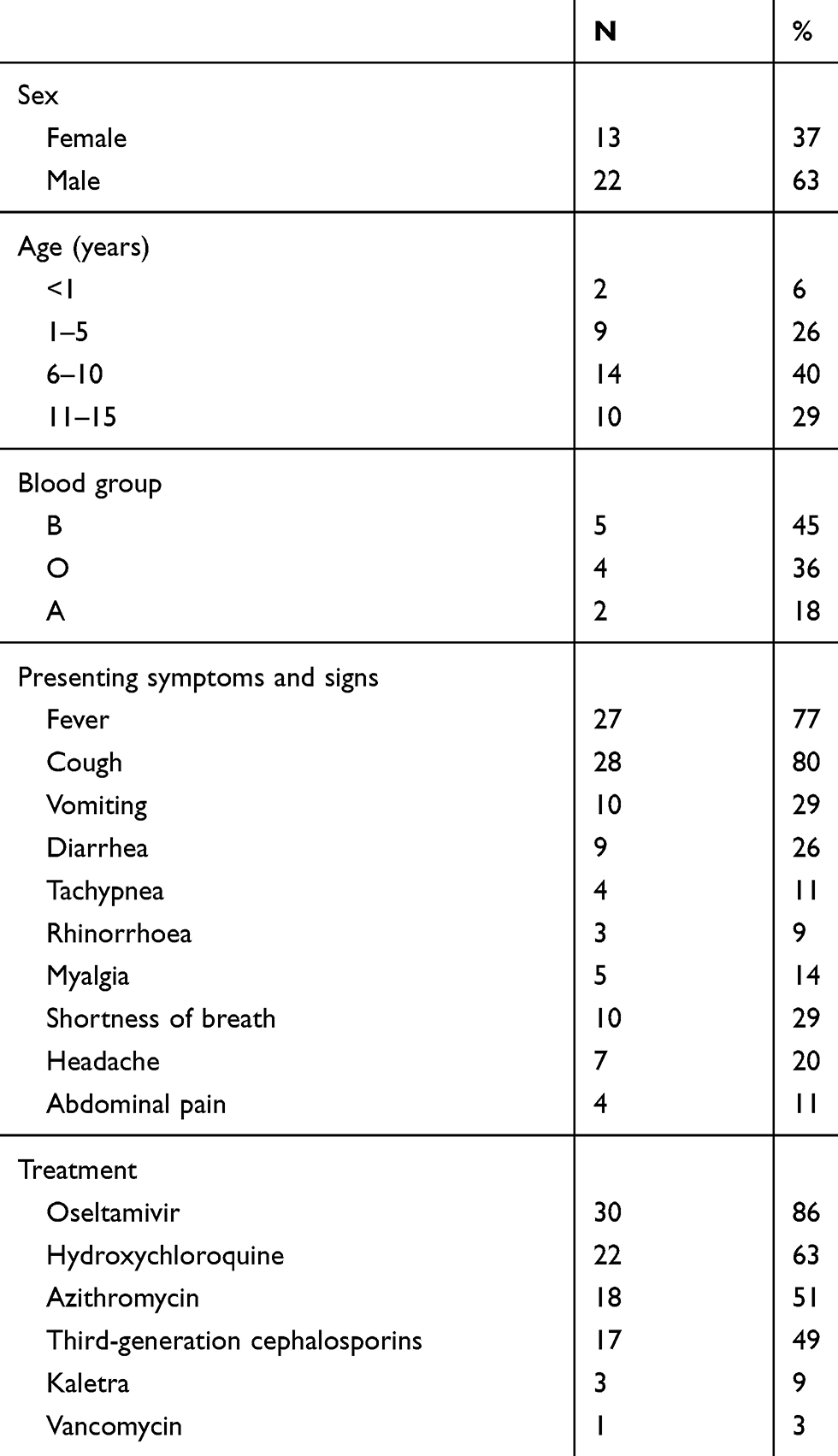 |
Table 1 Summary of Patient’s Characteristics (n=35) |
Twenty-nine patients (83%) had an identified history of close contact with suspected or confirmed COVID‐19 cases in family members. No patient had a history of international travel within 14 days before symptom onset. Seven patients (20%) required intensive care unit (ICU) admission. The median time to admission from development of symptoms was 7 days (interquartile range [IQR]=2–7 days). We reported severe pneumonia in 14 hospitalized patients (40%). The time from the onset of symptoms and the reference time to the hospital was higher in patients with severe disease than patients in the mild group (8.0±7.6 vs 5.3±4.5 days, P-value=0.19).
The duration of hospital stay was significantly higher in patients with severe disease than patients in the mild group (14.9±14.4 vs 4.3±3.7 days, P-value=0.003).
Cough was present in 80% of the patients, followed by fever (77%), nausea or vomiting (29%), diarrhea (26%), shortness of breath (29%), headache (20%), and myalgia (14%). Less common symptoms were tachypnea (11%), abdominal pain (11%), and rhinorrhea (8%).
The majority of cases were ≥5 years old (n=24, 69%). No significant differences between the clinical features and outcome were found between children aged <5 years and ≥5 years with and without severe disease. Fever was observed in only around half of the children <5 years (54.5%) and that was less than children ≥5 years (87.5%).
The presence of preexisting underlying medical conditions was found in 18 (51%) patients. Chronic kidney diseases (n=4, 22%), neurological disorders (n=4, 22%), cardiovascular disease (n=2, 11%), liver cirrhosis (n=2, 11%), leukemia (n=2, 11%), polyarthritis (n=1, 6%), reactive airway disease, X-linked lymphoproliferative (XLP) syndrome (n=1, 6%), and human immunodeficiency virus (n=1, 6%) were the reported coexisting conditions.
Table 2 shows laboratory findings on admission. Lymphopenia was present in 43% of the patients, thrombocytopenia in 9%, neutopenia in 8%, and leucopenia in 26%. Most of the patients had elevated levels of ESR (83%). Most patients showed normal serum levels of procalcitonim (64%), and the CRP level was above the normal range in 59% of the cases. Lactate dehydrogenase and creatinine kinase were elevated in 31% and 9% of the cases, respectively, and anemia was found in 20% of the cases.
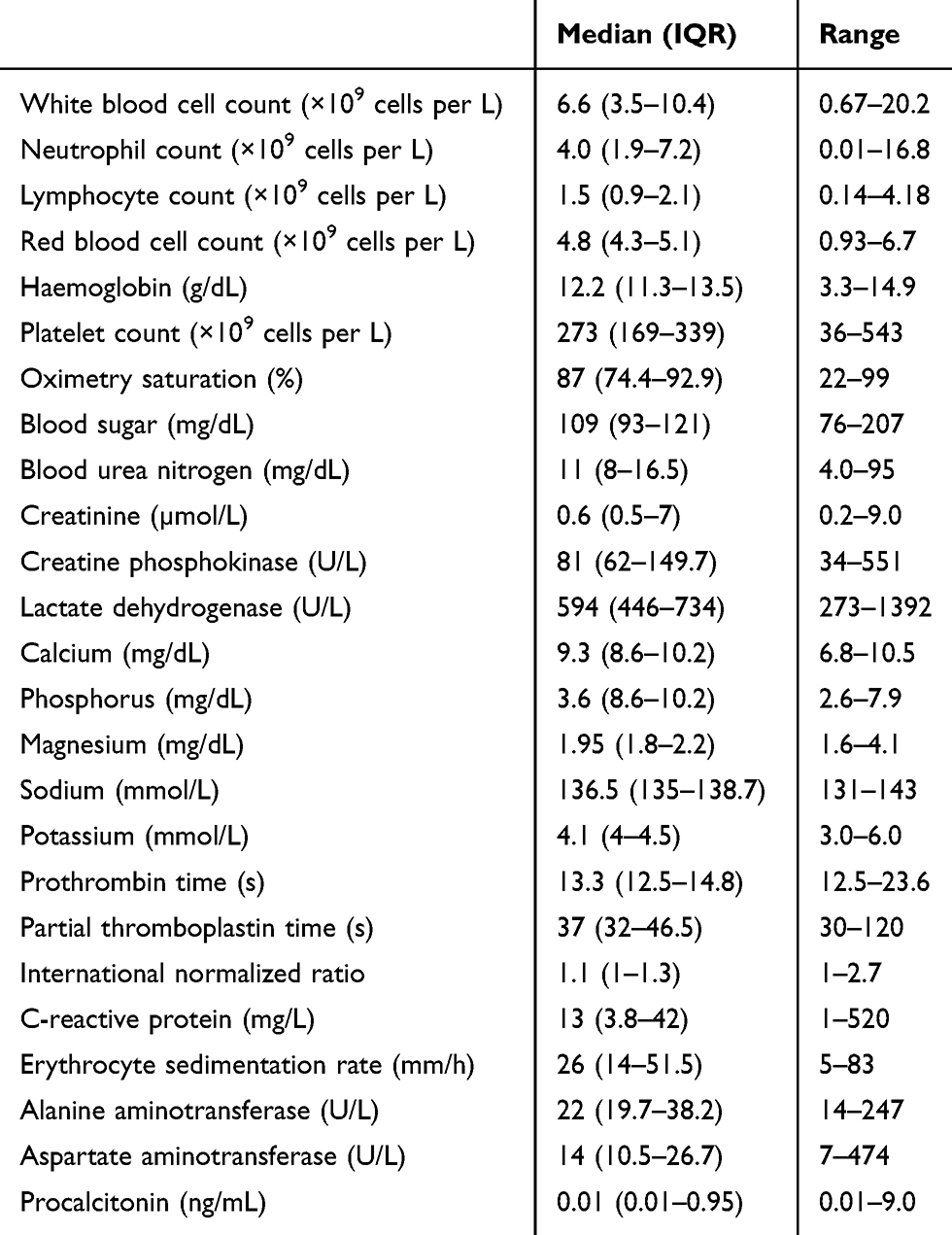 |
Table 2 Laboratory Findings of the Patients with COVID-19 Infection on Admission |
The white blood cell counts at admission did not differ significantly in patients with and without severe disease (median=7×109 cells per L vs 6.6×109 cells per L). Lymphopenia was observed at admission in 15 patients (43%), but did not differ significantly between those with and without severe disease (48% vs 36%, P-value=0.48).
Inflammatory markers (CRP: median=36 mg/dL vs 10 mg/dL; procalcitonin: median=0.7 ng/mL vs 0.15 ng/mL) were elevated at admission for patients with severe disease compared to patients with mild disease; however, the differences were not significant. Of 35 patients, 11 had positive RT-PCR results (31%). Of 35 CT scans that were performed at the time of admission, 91% revealed abnormal results (Table 3). The chest CT images of 24 patients (69%) suggested COVID-19, while their RT-PCR assays from throat swab samples were negative. A typical CT scan manifestation compatible with COVID-19 in addition to a history of close contact with suspected or confirmed cases in family members was considered as a decisive clue for pediatric COVID-19 in patients with a RT-PCR negative result.
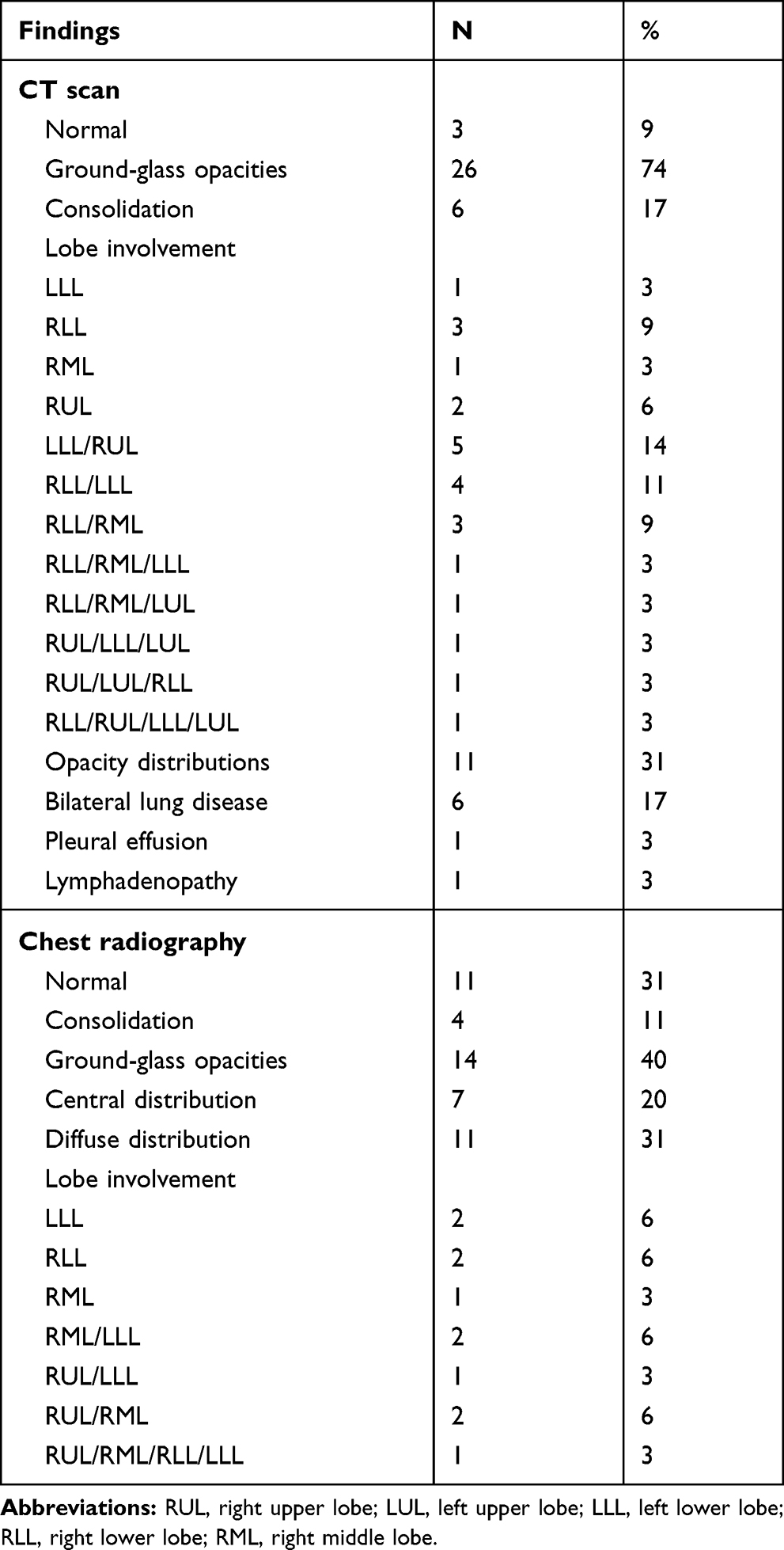 |
Table 3 Findings at Initial Chest CT and Radiographic Examination |
The most common pattern on chest CT was ground-glass opacity (74%). Opacity and bilateral distribution were seen in 31% and 17% of cases, respectively; and 17 (49%) had involvement of two or more lobes at chest CT. The right lower lobe was involved in 14 (40%), the left lower lobe was involved in 13 (37%), the right upper lobe in 10 (29%), the right middle lobe was involved in six (1%), and the left upper lobe in four (11%) patients at initial CT scan.
Normal chest radiographic findings were found in 31% of patients; diffuse and central distribution was seen in 31% and 20% of cases, respectively (Table 3).
Most patients received antiviral therapy (oseltamivir, 30 [86%]), and many received antibacterial therapy including azithromycin (n=18, 51%), cefotaxime (n=11, 31%), and ceftriaxone (n=6, 17%). More than half of the patients (63%) received hydroxychloroquine therapy.
Most patients were discharged (31 [89%]) with a median length of stay of 4 days (range=12–46 days). Four deaths (11%) were reported among the pediatric cases included in this analysis.
In a patient with XLP syndrome infected with COVID-19 after bone marrow transplantation, his condition deteriorated in spite of treatment. Despite steady improvement being seen in a patient with Wilson disease and a patient with congenital heart defect, their COVID-19 RT-PCR was positive several times; however, finally in a patient with congenital heart defect the result of COVID-19 RT-PCR changed to negative, in a patient with Wilson disease it remained positive.
Discussion
This report, to our knowledge, is the largest study to date of hospitalized children with COVID-19 infection in Iran.
Since the early days of a COVID‐19 infection outbreak, it has been thought that pediatric patients were not susceptible to COVID‐19. However, along with widespread spread of the virus, the number of infected children has gradually increased.7 In a recent report, among 1099 laboratory-confirmed cases, only nine patients (0.9%) were younger than 15 years of age.12 Males seemto be more susceptible to COVID-19 infection, which is similar to the recent epidemiological studies.3,5,12 A higher incidence rate of COVID-19 infection in males and in Asia might be due to the higher expression level of ACE‐2.13,14
Our study is similar to previous reports indicating that the main clinical manifestations of COVID-19 are fever and cough.3,12,15 Although fever was the most common symptoms at onset of illness in children, it was reported less than in adults.10 Moreover, fever was more prevalent in children aged ≥5 years compared to the patients aged <5 years.
Diarrhea and vomiting were reported as uncommon symptoms in previous studies of children;3,12,15 however, in our study nearly one third of our patients experiences diarrhea and/or vomiting.
It has been reported that clinical symptoms in pediatric patients are relatively milder compared with those in adults; however, there are limited data on the epidemiological and clinical patterns of COVID-19 in children. In contrast to previous reports of pediatrics in China,3,11,12 we reported severe pneumonia in 40% of the hospitalized patients in the COVID-19 outbreak in Iran.
In laboratory examination results, most patients (80%) had normal or decreased white blood cell counts. In contrast to adults where lymphopenia is found in the majority of cases with COVID-19,10 it was found in only 43% of cases. Nearly half of the patients (46%) had underlying diseases. Immunocompromised patients may be at high risk of developing a severe COVID-19 pneumonia.16
It has been reported that patients with chronic comorbidities are at higher risk of severe acute respiratory syndrome.4 The underlying and chronic diseases may be linked to the pathogenesis of COVID-19, which might make individuals more susceptible to severe disease complications, probably due to the attenuation of the innate immune response, low immune function, and proinflammatory responses.17
Eighty-three percent of our cases had close contact with family members suspected or confirmed with COVID-19; therefore, family prevention is highly recommended to prevent the transmission of COVID-19 to children.
COVID‐19 has not been described in organ transplant recipients or donors.18 Although identifying of COVID-19 before donation in transplant donors for the consequent exclusion of positive cases was introduced, no specific indications for recipients of transplants in epidemic areas are available.19 To our knowledge, this is a first report of COVID‐19 in organ transplant recipients in children. We described COVID‐19 in a liver transplant candidate that had no fever and did not meet the case definition for COVID‐19 and she was tested before transplantation.
Chest CT is a sensitive tool to detect COVID‐19 infection, especially in areas with a shortage of RT-PCR testing.5 Since the diagnosis of COVID-19 must be confirmed by RT-PCR for respiratory specimens, pharyngeal swab COVID‐19 nucleic acid has a low detection rate.7 In addition, sampling errors and low virus load, and kit performance, might lead to negative results, especially in an early stage of disease.8,20
In our study only 31% of the cases had a positive RT-PCR result. The total positive rate of 30–60% for throat swab RT-PCR was reported at initial presentation of patients with COVID-19 infection.21
It has been reported that chest CT has a high sensitivity for diagnosis of COVID-19.7 We observed that 69% of cases with COVID-19 infection had a false negative RT-PCR result of throat swab samples, so chest CT may be considered as a primary tool for the current COVID-19 detection in epidemic areas.7 The sensitivity of chest CT based on positive RT-PCR results in suggesting COVID-19 was 97% (95% CI=95–98%) and 75% of patients with negative RT-PCR results had positive chest CT findings.7
Since COVID-19 is a novel disease and little has been described about the clinical course, risk factors for severity of disease and reappearance of SARS‐CoV, especially in children,22,23 plans should be made at local and regional levels for preventing transmission and slowing the rate of new infections.
On the other hand, reducing the risk of nosocomial outbreak by infection prevention and control precautions are of critical importance. Maintaining of appropriate distancing of at least 2 meters between patients with suspected or confirmed COVID-19 with other patients and health care workers as well as use of relevant personal protective equipment is highly recommended.
Several limitations have been observed in this paper. First, the sample size included in the study was small and the results cannot be really generalized on the whole child population in Iran. Moreover, prioritization of SARS‐CoV‐2 RT-PCR testing for symptomatic patients would result in overestimation of the percentage of patients with COVID-19 severe infection. The RT-PCR assay was performed on throat swab samples and the sensitivity of throat swab samples was not high enough and repeated RT-PCR tests on other samples including nasopharyngeal swab samples with higher sensitivity and compliance in children was not performed. Besides, although RT-PCR assay is considered as a confirmatory test for COVID-19, typical CT scan manifestation compatible with COVID-19 in addition to a history of close contact with suspected or confirmed cases in family members was a decisive clue of pediatric COVID-19 in patients with a RT-PCR negative result.
In conclusion, this study demonstrated different clinical findings of pediatrics compare to the previous reports of children. Since a high rate of false negative RT-PCR test was observed, early detection of children with COVID-19 infection by CT is conducive to reasonable management and early treatment of pediatric patients.
Acknowledgments
This study was supported by a grant (grant number: 99-1-149-47172) from Tehran University of Medical Sciences to Dr. Setareh Mamishi.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World health organization. Coronavirus disease 2019 (COVID-19): situation report, 145. June 13, 2020.
2. Tang X, Wu C, Li X, et al. On the origin and continuing evolution of SARS-CoV-2. Natl Sci Rev. 2020;7(6):1012–1023. doi:10.1093/nsr/nwaa036
3. Dong Y, Mo X, Hu Y, et al. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics. 2020.
4. Sun D, Li H, Lu -X-X, et al. Clinical features of severe pediatric patients with coronavirus disease 2019 in Wuhan: a single center’s observational study. World J Pediatrics. 2020;1–9.
5. He F, Deng Y, Li W. Coronavirus disease 2019: what we know? J Med Virol. 2020;92(7):719–725. doi:10.1002/jmv.25766
6. Fang Y, Zhang H, Xie J, et al. Sensitivity of chest CT for COVID-19: comparison to RT-PCR. Radiology. 2020;200432.
7. Ai T, Yang Z, Hou H, et al. Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases. Radiology. 2020;200642.
8. Xie X, Zhong Z, Zhao W, Zheng C, Wang F, Liu J. Chest CT for typical 2019-nCoV pneumonia: relationship to negative RT-PCR testing. Radiology. 2020;200343.
9. Lan L, Xu D, Xia C, Wang S, Yu M, Xu H. Early CT Findings of Coronavirus Disease 2019 (COVID-19) in Asymptomatic Children: A Single-Center Experience. Korean J Radiol. 2020;21(7):919–924. doi:10.3348/kjr.2020.0231
10. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061. doi:10.1001/jama.2020.1585
11. Chen Z-M, Fu J-F, Shu Q, et al. Diagnosis and treatment recommendations for pediatric respiratory infection caused by the 2019 novel coronavirus. World J Pediatrics. 2020;1–7.
12. Guan W-J, Ni Z-Y, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
13. Lu Q, Shi Y. Coronavirus disease (COVID‐19) and neonate: what neonatologist need to know. J Med Virol. 2020.
14. Del Rio C, Malani PN. COVID-19—new insights on a rapidly changing epidemic. JAMA. 2020;323(14):1339. doi:10.1001/jama.2020.3072
15. Guo Y-R, Cao Q-D, Hong Z-S, et al. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak–an update on the status. Military Med Res. 2020;7(1):1–10. doi:10.1186/s40779-020-00240-0
16. D’Antiga L. Coronaviruses and immunosuppressed patients. The facts during the third epidemic. Liver Transplant. 2020;26(6):832–834. doi:10.1002/lt.25756
17. Yang J, Zheng Y, Gou X, et al. Prevalence of comorbidities in the novel Wuhan coronavirus (COVID-19) infection: a systematic review and meta-analysis. Int J Infect Dis. 2020;94:91–95. doi:10.1016/j.ijid.2020.03.017
18. Michaels MG, La Hoz RM, Danziger Isakov L, et al. Coronavirus disease 2019: implications of emerging infections for transplantation. Am J Transplant. 2020;20(7):1768–1772. doi:10.1111/ajt.15832
19. Andrea G, Daniele D, Barbara A, et al. Coronavirus disease 2019 and transplantation: a view from the inside. Am J Transplant. 2020.
20. Zu ZY, Jiang MD, Xu PP, et al. Coronavirus disease 2019 (COVID-19): a perspective from China. Radiology. 2020;200490.
21. Yang Y, Yang M, Shen C, et al. Laboratory diagnosis and monitoring the viral shedding of 2019-nCoV infections. medRxiv. 2020.
22. Murthy S, Gomersall CD, Fowler RA. Care for critically ill patients with COVID-19. JAMA. 2020;323(15):1499. doi:10.1001/jama.2020.3633
23. Li G, Fan Y, Lai Y, et al. Coronavirus infections and immune responses. J Med Virol. 2020;92(4):424–432. doi:10.1002/jmv.25685
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.